Embed Size (px)
Citation preview

Scand J Haematol( l983) 30,289-296
Internal Distribution of Excess Iron and Sources of Serum Ferritin in Patients with Thalassaemia
MARIO CAZZOLA , l CATERINA BORGNA-RGNA~I ,' RERO DE STEFANO ,2 GAETANO BERGAMASCHI , I
k D E G. BONGO,' LAURA DEZZA' & FRANCO AVAT03
' Istituto di Patologia Medica I , Dipartimento di Pediatria and .7 Istituto di Medicina Legale, University of Pavia, Pavia, Italy
Liver and spleen iron concentrations, serum ferritin level and binding of S-ferritin to concanavalin A (Con A) were measured in 12 patients with thalassaemia major or inter- media at the time of splenectomy. All these subjects had increased liver iron concentration, most of them had hepatic fibrosis but none of them had histological evidence of chronic hepatitis. No patient had ascorbic acid deficiency. Serum ferritin concentration was increased in all cases, ranging from 266 to 5 504 pg/l. In all but 2 subjects most of the protein did not bind to Con A, thus behaving as tissue ferritin. There were highly significant correlations between serum ferritin concentration, amount of blood transfused and liver iron concen- tration. On the average, iron concentration in the liver was about 3 times that in the spleen. The findings obtained suggest that in patients with thalassaemia major or intermedia most of the iron is deposited in parenchymal tissues and most of the S-ferritin derives by leakage from the cytosol of iron-loaded parenchymal cells. S-ferritin is a valid index of liver iron overload in thalassaemic patients without complications such as viral hepatitis and/or ascorbic acid deficiency.
Key wordst ferritin - iron overload - serum ferritin - thalassaemia
Accepted for publication October 12, 1982
Correspondence to: Dr. Mario Cazzola, Patologia Medica 1, Policlinico S. Matteo, 1-27100 Pavia, Italy
Measurement of S-ferritin is a convenient method of assessing the amount of storage iron in patients with transfusional iron over- load (Wonvood 1980). However, the origin of S-ferritin in these subjects is far from clear. In particular, it is yet unknown which fraction of the ferritin that we measure in the serum derives from the reticuloendo- thelial system (RES) and which derives from the parenchymal tissue (Hoffbrand 1980). This issue has considerable clinical
relevance since it is the accumulation of iron in parenchymal cells that is harmful to the patient.
Worwood et a1 (1979) have shown that binding of S-ferritin to concanavalin A (Con A) may be a useful way of distinguish- ing between the ferritin secreted by the RES cells and that released from iron-loaded parenchymal tissues. Ferritin which binds to Con A is glycosylated and is thought to derive by secretion from RES, whereas

290 CAZZOLA ET AL
non-binding ferritin would be directly re- leased into the serum by parenchymal cells, e.g. hepatocytes. Such a method has al- ready been employed for studying the source of serum ferritin during infection (Birgegird 1980).
The purpose of the present study was to investigate the origin of S-ferritin in pa- tients with thalassaemia major or inter- media who had various degrees of iron overload but no complication such as viral hepatitis and/or ascorbic acid deficiency. Thus, at the time of splenectomy, we mea- sured liver and spleen-iron concentrations, S-ferritin concentration and binding of S- ferritin to Con A.
MATERIAL AND METHODS
Patients 8 patients with thalassaemia major and 4 patients with thalassaemia intermedia were studied (Table 1). All were negative for hepatitis B viral markers (HBsAg, anti-HBc and anti-HBs antibodies).
All the patients with thalassaemia had been treated with i.m. desferrioxamine from the beginning of trans- fusional therapy. Patients nos. 1-6 had received des- ferrioxamine subcutaneously for about 6 to 12 months prior to splenectomy. All the patients with thalassaemia major were supplemented with ascorbic acid. Patients with thalassaemia intermedia did not receive supple- mentary ascorbic acid; none of them had clinical evi- dence of ascorbic acid deficiency.
Patients were splenectomized because of a sustained increase in blood consumption and/or hypersplenism. Haematological and other routine investigations were carried out in the week preceding splenectomy. The amount of blood administered by transfusion was cal- culated from medical records.
Serum ferritin S-ferritin concentration was measured by a radio- immunoassay (Liso-phase RIA System Ferritin Kit, Gruppo Lepetit, Milan, Italy) based on human liver ferritin standards and antibodies raised in the rabbit against human liver ferritin. The sensitivity of the assay
method was increased up to 1 pg/l by appropriate dilution of labelled ferritin and antiserum.
Binding of S-ferritin to Con A was measured as described by Wonvood et al (1979). Con A-Sepharose and Sepharose 4B were purchased from Pharmacia Fine Chemicals, Uppsala, Sweden. Both gels were prepared as a suspension of particles in acetate buffer solution (sodium acetate solution, 50 mmol/l, adjusted to pH 6.0 with acetic acid, and containing sodium chloride, 500 mmol/l, and CaC12, MgS04 and MnS04, all at 1 mmol/l and the vol. was adjusted to twice the vol. of the packed particles. Of these suspensions, 0.8 ml was incubated with 1.1 ml of the same acetate buffer and 100 pI of the test sample during slow rotation for 2 h at room temp. All samples were prepared in duplicate; for serum specimens with a total ferritin concentration lower than 200 pg/l, different vol. of buffer, test sample and packed gel (e.g. 1.0, 0.2 and 0.8 ml, respectively) were also employed in order to determine the ferritin concentration in the best portion of the working range.
After incubation, the mixtures were centrifuged at 3000 rpm/min for 15 min and the supernatant was sucked off with a pipette. The ferritin concentration was estimated in each supernatant by the afore-men- tioned RIA. After adjustment for dilution, the assay of the Sepharose 4B sample provided the total S- ferritin concentration, and that of the Con A-Sepha- rose 4B sample provided the concentration of serum ferritin which does not bind to Con A. From the difference, the Con A-binding S-ferritin was cal- culated. Preliminary studies showed no significant dif- ference in S-ferritin concentration before and after incubation with Sepharose 4B, thus excluding non- specific binding to the gel.
Measurement of iron concentration in liver and spleen At the time of splenectomy, samples of liver and spleen were weighed and preserved in a sterile plastic iron-free container. Fresh samples were lyophilized and the dry weight was recorded; the dry samples were transferred into a polyethylene tube without any chem- ical treatment. Tissue iron was determined by activa- tion analysis. Nuclear irradiation took place in the TRIGA Mark I1 250 kW reactor of the University of Pavia. Under appropriate conditions of irradiation, 58Fe was converted to 59Fe and this radioactive isotope was then determined by gamma counting. NBS 1577 bovine liver was used as standard reference material throughout the entire process.
TA
BL
E 1
C
linic
al a
nd la
bora
tory
dat
a in
eig
ht p
atie
nts
with
thal
assa
emia
maj
or a
nd fo
ur pa
tient
s w
ith th
alas
saem
ia in
term
edia
Pa
tie
nt,
se
x/a
ge
(yr)
NO
. of
units
Ser
um f
err
itin
(pg/l)
Liv
er
iro
n
Sp
leen
iro
n
AL
T
ac-
of
blo
od
co
ncn
co
ncn
ti
vit
y
rec
eiv
ed
to
tal
no
n-b
ind
ing
b
ind
ing
to
( 4
1
) (m
g/g
of
dry
tissue)
to C
on A
Con
A
(%)
1,
tha
l.
maj
or,
M
/11
2,
tha
l.
maj
or,
F/
9
3,
tha
l.
maj
or,
M
/6
4,
tha
l.
maj
or,
M
/11
5,
tha
l.
maj
or,
M
/16
6,
tha
l.
maj
or,
F/
5
7,
tha
l.
maj
or,
F
/14
8,
tha
l.
maj
or,
F/
12
9,
tha
l.
int.
, F
/~O
10
, th
al.
in
t.,
F/11
11
, th
al.
in
t.,
M/9
12
, th
al.
in
t.,
M/6
Nor
mal
range
254
16
0
12
0
15
0
10
0
59
200
13
0
48 0 0
0
v1 2 2
55
;;3
5 33
0 3
358
1 97
2 (3
7)
31 .I
18
.5
10
8
4 30
5 3
025
1 28
0 (3
0)
n.d.
8
e4
96
**
4 0
00
2
400
1 60
0 (4
0)
23.3
8
.I
7.1
95
f 4
715
3 34
8 1
367
(29
) 17
.3
3 36
0 2
752
608
(18
) 18
.3
n.d.
6
0
4 30
5 3
075
1 23
0 (2
9)
5 5
04
3
584
1 92
0 (3
5)
38.0
19
.0
80
3 28
0 2
427
853
(26
) 15
.9
4.9
48
1 40
8
**
P z 20
.8
7.0
87
z z 2 7 0
4
70
4 (
50
) 2.
7 4.
7 5
3
F 51
2
328
18
4 (
36
) 3
-2
1.5
15
% s
266
12
8
13
8 (
52
) 5.
0 1
1.4
5
> 77
9
748
31
(4)
0.4
3 -1
1
6
E
20-1
1 0
7-35
12
-75
< 0.
2 <
0.2
5-1
5 (5
9-80
) ~
~~
* 1
unit
= 3
00 m
l of
bloo
d **
n.d
. =
not
det
erm
ined
292 CAZZOLA ET AL
4000
2000
0
RESULTS
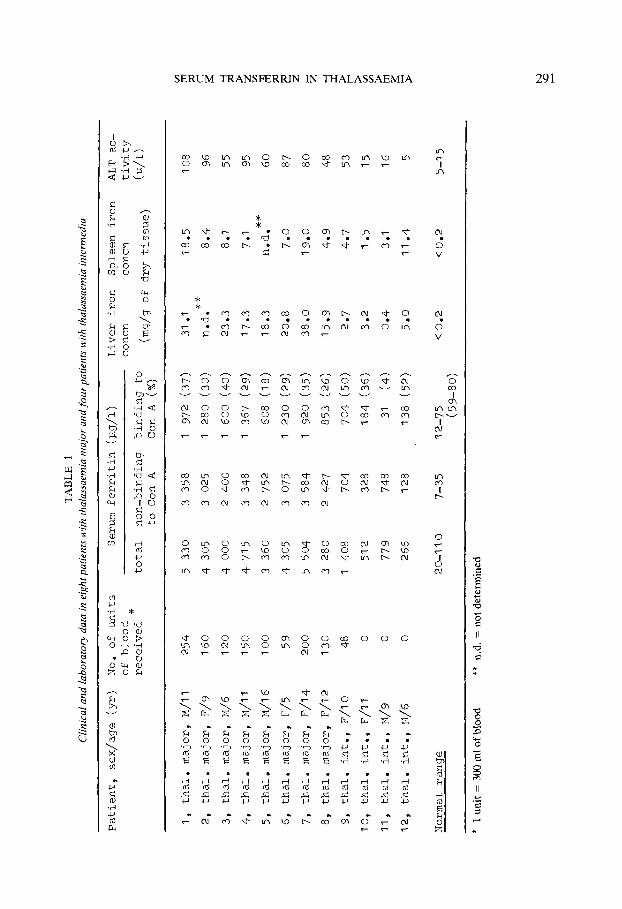
The results obtained in the present study are reported in Table 1. The total S-ferritin concentration was increased to a variable degree in subjects with thalassaemia. While in normal subjects 59 to 80% of S-ferritin bound to Con A, most of the protein did not bind in all but 2 thalassaemic patients. Both liver and spleen iron concentrations were consistently increased in the patients studied. Histological studies of the liver biopsies showed siderosis and fibrosis; no inflammatory changes compatible with a diagnosis of chronic hepatitis were found.
As shown in Figure 1, there were signi- ficant correlations between the amount of blood transfused and total S-ferritin, non- glycosylated ferritin and glycosylated ferri- tin.
- -
-
A
A -A
6ooo[
I Total ferr i t in ]
r = 0.90 r: P < 0.001
0 I. I I I I I
0 100 200
Correlations were also found between the amount of blood transfused and both liver and spleen iron concentrations (Figure 2) although increased tissue iron was found even in 3 subjects with thalassaemia inter- media who had received no blood trans- fusions. On average, 1 unit of blood (300 ml) was found to produce an increase in iron concentration of 0.128 mg/g dry weight in the liver as against 0.048 mg/g in the spleen. Since liver size was greater than spleen size in all subjects, the above data indicate that a large part of the iron contained in each blood unit transfused was found in the liver at the time of study. Liver and spleen iron concentrations were correlated ( r = 0.80, P < 0.01), the mean iron concentration of the spleen being only 38 % of that of the liver.
A consistent direct relationship was found between liver iron concentration and all of
A A A
A A A
r = 0.87 P. 0.001
A A
fer r i t in
A
A A
A r,o.go A P.0.001
A Ai-l I A A I ferritin I -
I 1 I 1 I
100 200
0 1) 0
Units of blood transfused
Figure 1. The relationships between total S-ferritin concentration or its fractions and number of units of blood transfused. Con A binding ferritin is indicated as glycosylated ferritin; non-binding ferritin is indicated as
non-glycosylated ferritin.

SERUM TRANSERRIN IN THALASSAEMIA
C : 3000- L L
c m
E 2 In
0 -
293
0 1- 0.90 P < 0.001
0
0
a
r = 0.88 P <0.001
a .. I I I 1 I
0 100 200
40 - e,
c D Q .- P
P
s E - 5 20 c 0
C
2 c lo .-
Q
v)
- n
0
r = 0.72 ’ P< 0.01
. I I I I I
0 100 200
Units of blood transfused
Figure 2. The relationship between liver iron concentration (left) and spleen iron concentration (right) and number of units of blood transfused.
the following: total S-ferritin ( r = 0.90, P < 0.001, Figure 3), non-glycosylated S-ferritin ( r = 0.89, P < 0.001) and glycosylated S - ferritin ( r = 0.90, P < 0.001). Spleen iron concentration was closely related to glyco- sylated ferritin only ( r = 0.71, P < 0.01).
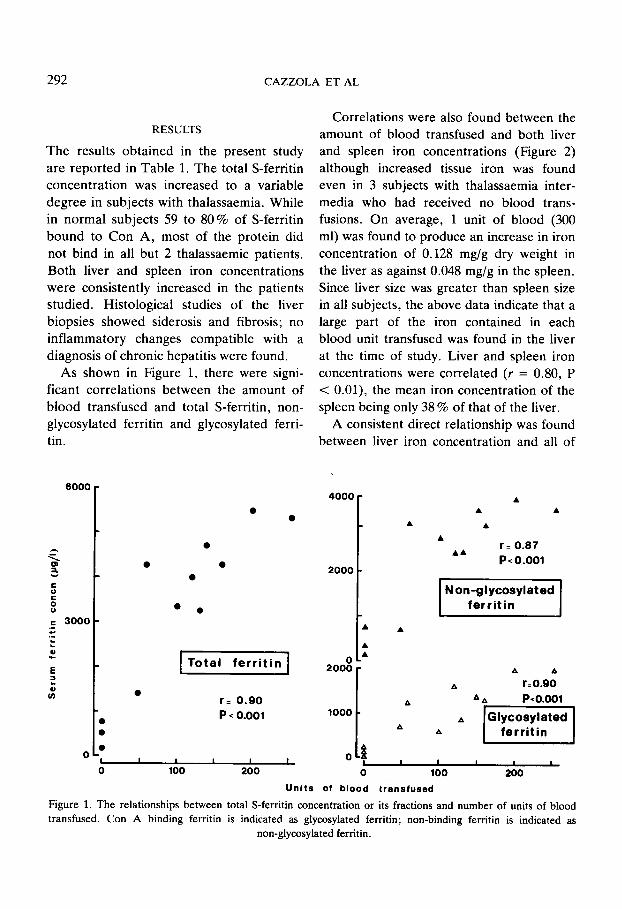
As shown in Figure 4, alanine aminotrans- ferase (ALT) activity was directly related to
6000 r
L i v e r i ron concn h g / g dry weight)
Figure 3. The relationship between S-ferritin and liver iron concentration.
both liver iron concentration and total S- ferritin. There was a weak correlation be- tween liver iron concentration and the S - ferritin to ALT ratio ( r = 0.62, P <0.005).
DISCUSSION
A number of clinical studies recently re- viewed by Wonvood (1982) have shown that there are at least 2 factors controlling the level of ferritin in the serum of patients with iron overload: (1) the amount of storage iron and (2) tissue damage. The first factor would involve secretion of ferritin from RES with the addition of carbohydrate residues in this process (glycosylated fer- ritin, binding to Con A). The second factor, tissue damage, would lead to release of fer- ritin through the membranes of damaged parenchymal cells (non-glycosylated ferri- tin, non-binding to Con A), and would also
294 CAZZOLA ET AL
100
50
m e
r = 0.78 r= 0.92
PcO.001 P c 0.001
I I I
3000 6000
t,eme1 I I I 0 2 O L t e e 0
0 10 20 30 40 0
Liver iron concn(rng/g dry weight) Serum ferr i t in concn(pg/l)
Figure 4. The relationship between alanine aminotransferase (ALT) activity and liver iron concentration (left) and S-ferritin (right).
interfere with the rate of clearance of fer- ritin from the circulation (Worwood 1980).
It is clear that iron overload due to repeated blood transfusions, such as is observed in patients with thalassaemia major, will elevate S-ferritin through both the above quoted mechanisms. Moreover, other factors may play a r81e in the me- tabolism of S-ferritin in patients with thalassaemia. Chronic viral hepatitis which is a frequent complication in these patients, at least in Italy (Masera et al 1976, De Vergiliis et a1 1981), may produce leakage of ferritin from the cytosol of damaged hepatocytes (Prieto et a1 1975). Patients with thalassaemia major may have a re- duced body content of ascorbic acid and this may affect S-ferritin concentration, probably through a reduction in iron re- lease and ferritin synthesis by the RES (Cohen et a1 1981, Roeser et a1 1980, Chap- man et a1 1982b).
In the present work, we have studied the relationship between internal distribution of excess iron and S-ferritin measurements in
a selected group of patients with thalassae- mia major or intermedia who had various degrees of iron overload without complica- tions. Our data on iron distribution are in accord with the accumulating evidence (Schafer et a1 1981, Cazzola & Barosi 1982) that, irrespective of plasma iron turnover and erythroid activity, the iron given with the transfused blood does not remain in the RES but is rapidly redistributed to paren- chymal tissue. As a matter of fact, liver iron concentration was tightly related to the amount of blood transfused, and largely ex- ceeded spleen iron concentration. Liver iron was also increased in the 4 subjects with thalassaemia intermedia, probably as a con- sequence of increased iron absorption (Pip- pard et al 1979), but the values were con- sistently lower than those found in the pa- tients regularly transfused.
The findings of our studies on S-ferritin suggest that in patients with thalassaemia major or intermedia the largest part of S- ferritin derives by leakage from the cytosol of iron-loaded parenchymal tissues. In 10
SERUM TRANSFERRIN IN THALASSAEMIA 295
out of 12 thalassaemic subjects, more than 50% of S-ferritin did not bind to Con A , thus behaving as tissue ferritin. The connection between S-ferritin and parenchymal tissues was also supported by the strong correlation between S-ferritin and liver iron concentra- tion. Although liver tissue contains both RES and parenchymal cells, the latter are predominant and liver iron concentration essentially reflects hepatocyte iron. On the other hand, whereas the liver iron concen- tration showed good correlation with all the S-ferritin measurements, the spleen iron concentration was closely related only to the glycosylated ferritin. This appears to be in favour of the hypothesis that glycosylated ferritin arises from RES (Worwood et a1 1979, Birgeghd 1980).
We have confirmed that total S-ferritin is a valid index of liver iron overload in pa- tients with thalassaemia who are not as- corbic acid deficient (Letsky et al 1974, Chapman et a1 1982b), and that measuring the fraction of S-ferritin which binds to Con A does not provide any advantage for such purpose (Chapman et a1 1982a). By analysis of our data and those of Letsky et a1 (1974) and Chapman et al (1982b), it may be cal- culated that 200 pg/l of S-ferritin are equiv- alent to about 1 mglg (dry weight) of liver iron, although such an equation should not be applied to a single ferritin value. In single patients, in fact, more useful infor- mation can be derived from the trend of serial ferritin concentrations (Hoffbrand et al 1979, Cohen et a1 1981b) than by a single ferritin value.
The close correlation between liver iron, S-ferritin and ALT activity (Figure 4) may suggest that the iron accumulated in the hepatocytes caused an increased leakage of both ferritin and ALT in our patients. In our group of subjects, the S-ferritin to ALT
ratio was less useful than measurement of S-ferritin alone in evaluating the liver iron load. This seems to be not valid in patients who also have chronic hepatitis (De Vir- giliis et al 1982). In these cases, liver biopsy with quantification of liver iron is probably necessary to reliable evaluate parenchymal iron overload. Computed tomography might be a useful alternative technique (Houang et a1 1979).
ACKNOWLEDGEMENTS
We are indebted to Dr. M. Worwood for having taught one of us (MC) the method of measuring the binding of S-ferritin to Con A.
REFERENCES
Birgegird G (1980) The source of serum ferritin dur- ing infection. Studies with concanavalin A-Sepha- rose absorption. Clin Sci 59,38547.
Cazzola M & Barosi G (1982) Non-erythroid iron kinetics in iron loading anaemias. In D J Weather- all, G Fiorelli & S Gorini (eds) Advances in red blood cell biology, p 95. Raven Press, New York.
Chapman R W G, Gorman A, Laulicht M, Hussain M A M, Sherlock S & Hoffbrand A V (1982a) Binding of serum ferritin to concanavalin A in patients with iron overload and with chronic liver disease. J Clin
Chapman R W G, Hussain M A M, Gorman A, Laulicht M, Politis D, Flynn D M, Sherlock S & Hoffbrand A V (1982b) Effect of ascorbic acid defi- ciency on serum ferritin concentration in patients with P-thalassaemia major and iron overload. J Clin Pathol35,487-91.
Cohen A, Cohen I J & Schwartz E (1981a) Scurvy and altered iron stores in thalassemia major. N Engl J Med 304, 158-60.
Cohen A, Martin M & Schwartz E (1981b) Response to long-term desferoxamine therapy in thalassemia. J Pediatr 99, 689-94.
De Virgiliis S, Cornacchia G , Sanna G, Argiolu F, Galanello R, Fiorelli G, Rais M, Cossu P, Bertolino F & Cao A (1981) Chronic liver disease in trans-
Path01 35,481-86.

296 CAZZOLA ET AL
fusion-dependent thalassemia: liver iron quantitation and distribution. Acta Haematol (Basel) 65, 32-39.
De Virgiliis S, Cossu P, Sanna G , Frau F, Loi E, Lobrano R, Nucaro A, Toccafondi C, Cornacchia G, Loi A & Cao A (1982) Iron chelation in transfusion- dependent thalassemia with chronic hepatitis. Acta Haematol (Basel) 67,49-56.
Hoffbrand A V (1980) Transfusion siderosis and chela- tion therapy. In A Jacobs & M Worwood (eds) Iron in biochemistry and medicine, 11, p 499. Academic Press, London.
Hoffbrand A V, Gorman A, Laulicht M, Garidi M, Economidou J, Georgipoulou P, Hussain M A M & Flynn D M (1979) Improvement in iron status and liver function in patients with long-term subcutaneous desferrioxamine. Luncer i, 94749.
Houang M T W, Arozena X, Skalicka A, Huehns E R & Shaw D G (1979) Correlation between computed tomographic values and liver iron content in thalas- saemia major with iron overload. Lancer i , 1322-23.
Letsky E A, Miller F, Worwood M & Flynn D M (1974) Serum ferritin in children with thalassaemia regularly transfused. J Clin Pathol 27, 652-55.
Masera G, Jean G, Gazzola G & Novakova M (1976) Role of chronic hepatitis in development of thalas- saemic liver disease. Arch Dis Child 51,680-85.
Pippard M J , Callender S T, Warner G T & Weatherall D J (1979) Iron absorption and loading in P-thalas- saemia intermedia. Lancet ii, 819-21.
Prieto J , Barry M & Sherlock S (1975) Serum ferritin in patients with iron overload and with acute and chronic liver disease. Gastroenterology 68,525-33.
Roeser H P, Halliday J W, Sizemore D J, Nikles A & Willgoss D (1980) Serum ferritin in ascorbic acid deficiency. Br J Haematol45,459-66.
Schafer A I, Cheron R G , Dluhy R, Cooper 8 , Glea- son R E, Soeldner J S & Bunn H F (1981) Clinical consequences of acquired transfusional iron overload in adults. N Engl J Med 304, 319-24.
Worwood M (1980) Serum ferritin. In A Jacobs & M Worwood (eds) Iron in biochemistry and medicine, 11, p 204. Academic Press, London.
Worwood M (1982) Serum ferritin and iron overload . In D J Weatherall, G Fiorelli & S Gorini (eds) Advances in red blood cell biology, p 49. Raven Press, New York.
Worwood M, Cragg S J, Jacobs A , McLaren C, Ric- ketts C & Economidou J (1980) Binding of serum fgrritin to concanavalin A: patients with homozygous p thalassaemia and transfusional iron overload. Br J Haematol46,409-16.
Worwood M, Cragg S J, Wagstaff M & Jacobs A (1979) Binding of serum ferritin to concanavalin A. CIin Sci 56, 83-87.