Embed Size (px)
Citation preview

The Knee xxx (2014) xxx–xxx
THEKNE-01871; No of Pages 8
Contents lists available at ScienceDirect
The Knee
Internal derangement of the knee in fibular hemimelia: Radiographic andMRI findings
Philip Yoong ⁎, Ramy MansourDepartment of Radiology, Nuffield Orthopaedic Centre, Oxford, UK
⁎ Corresponding author at: Nuffield Orthopaedic CentrOxford OX3 7LD, UK. Tel.: +44 1865 741 155; fax: +44 1
E-mail address: [email protected] (P. Yoong).
http://dx.doi.org/10.1016/j.knee.2014.02.0170968-0160/© 2014 Elsevier B.V. All rights reserved.
Please cite this article as: Yoong P, Mansou(2014), http://dx.doi.org/10.1016/j.knee.201
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 2 December 2013Received in revised form 3 February 2014Accepted 17 February 2014Available online xxxxKeywords:Fibular hemimeliaDysplasiaMRI
Background: Fibular hemimelia is a rare bone dysplasia with partial or complete absence of the fibula. There aremany associated lower limb deformities.Methods:Wedescribe the commonly associated bone and soft tissue abnormalities in the knee joint in a case se-ries of six knees in five patients with fibular hemimelia who underwent both radiographic and MR imaging.Results: In all knees, there was an elongated conjoint tendon of the lateral collateral ligament and biceps femoris.In five out of six knees, there was trochlear dysplasia. In four out of six, there was complete absence of the ante-rior cruciate ligament. In four out of six, therewas an abnormal lateral meniscus (threewere hypoplastic and oneabsent).Conclusion: These associations in fibular hemimelia, although unpredictable, have relevance in the guidance of
further orthopaedic management in this complex condition.© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Fibular hemimelia, also known as congenital fibular deficiency, isdefined as the complete or partial absence of the fibula. It is thecommonest long bone deficiency with an estimated incidence of 7.4and 20 cases per million live births [1,2]. Most cases are unilateral andthere is a slight male predominance [3]. There is a very wide spectrumof abnormality ranging from a mildly shortened fibula with no symp-toms in adulthood, to an absent fibula with multiple other lower limbabnormalities, presenting at birth [4]. Associated osseous lower limbfind-ings include talipes equinovarus, tarsal coalition, shortening of the femur,bowing of the tibia and absent lateral metatarsal rays [5]. Treatment infibular hemimelia is related to the extent of leg length discrepancy andfunction in the foot. The greater the deformity, the more the balance isshifted towards amputation over leg lengthening procedures [6].
In addition, there are several associated abnormal findings in theknee joint in fibular hemimelia, involving both bone and soft tissues.These abnormalities may influence ongoing orthopaedic treatment inthis complex condition.
In this pictorial review, we will describe the characteristic findingson radiography and magnetic resonance imaging (MRI) in the kneejoint in this unusual condition using a case series of patients from ourdepartment.
e, Windmill Road, Headington,865 738 199.
r R, Internal derangement of4.02.017
2. Materials and methods
A search was performed on all MRI scans between August 2006and August 2013 using our departmental radiology information da-tabase (RIS). The key phrase “fibular hemimelia” were used to iden-tify patients with this condition. The plain film and MRI of thesepatients were reviewed by two musculoskeletal radiologists of two(PY) and eight years experience (RM). A standard departmentalMRI knee protocol was used: fat-saturated proton density (FSPD)sagittal, coronal and axial and T2* sagittal sequences. In each patient,observations were made with regard to the severity of fibularhemimelia based on the Achterman and Kalamchi classification [7],as well as the appearance of bone, menisci, cartilage, cruciate andcollateral ligament complexes, posterolateral corner and tendon at-tachments around the knee joint. Basic demographic informationwas also recorded.
3. Results
There were a total of five patients with fibular hemimelia and MRI of theknee joint. In one knee, concurrent MRI of the lower limb was also performed.In one patient, there was bilateral fibular deficiency. The mean age at the timeof scan was 21 years (range 14–31). Three patients were male, two female. Inthree patients (four knees) the fibula was completely absent since birth, in onepatient there was a vestigial fibula just proximal to the ankle mortise joint andin one patient there was a hypoplastic proximal fibula with a normal distal fib-ula (Fig. 1).
The findings relating to the soft tissues of the knee in the six knees are documented inthe table.
the knee in fibular hemimelia: Radiographic and MRI findings, Knee
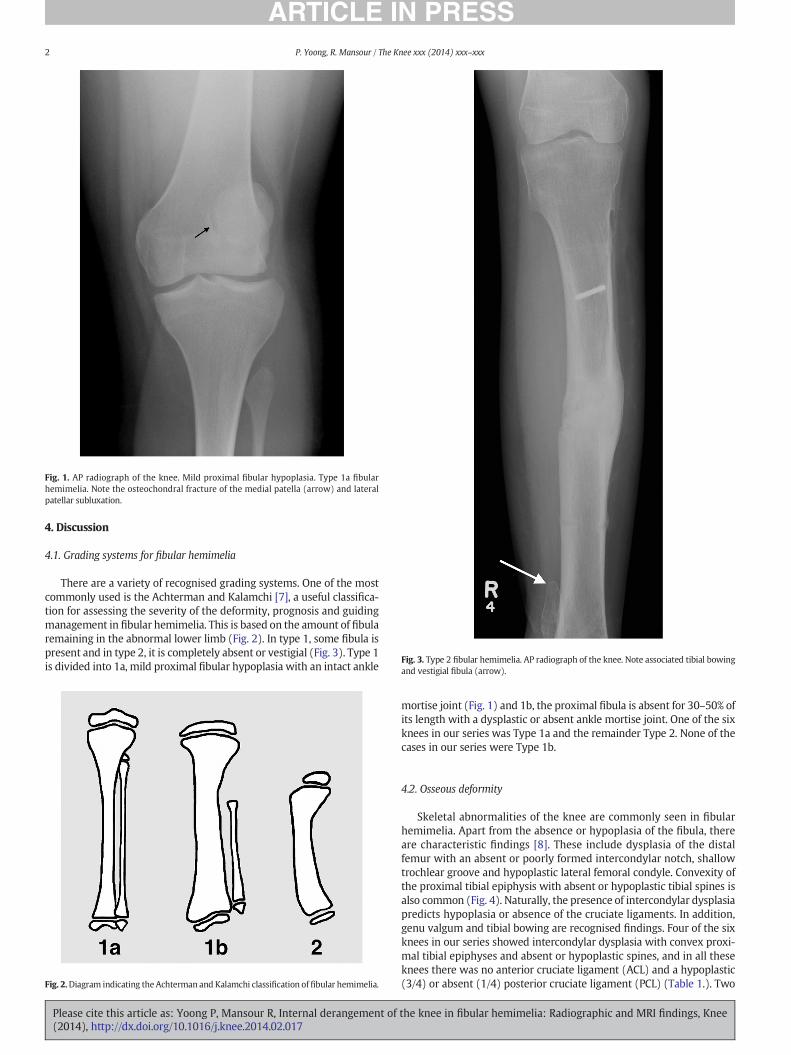
Fig. 1. AP radiograph of the knee. Mild proximal fibular hypoplasia. Type 1a fibularhemimelia. Note the osteochondral fracture of the medial patella (arrow) and lateralpatellar subluxation.
Fig. 3. Type 2 fibular hemimelia. AP radiograph of the knee. Note associated tibial bowingand vestigial fibula (arrow).
2 P. Yoong, R. Mansour / The Knee xxx (2014) xxx–xxx
4. Discussion
4.1. Grading systems for fibular hemimelia
There are a variety of recognised grading systems. One of the mostcommonly used is the Achterman and Kalamchi [7], a useful classifica-tion for assessing the severity of the deformity, prognosis and guidingmanagement in fibular hemimelia. This is based on the amount of fibularemaining in the abnormal lower limb (Fig. 2). In type 1, some fibula ispresent and in type 2, it is completely absent or vestigial (Fig. 3). Type 1is divided into 1a, mild proximal fibular hypoplasia with an intact ankle
Fig. 2.Diagram indicating theAchterman and Kalamchi classification offibular hemimelia.
Please cite this article as: Yoong P, Mansour R, Internal derangement of(2014), http://dx.doi.org/10.1016/j.knee.2014.02.017
mortise joint (Fig. 1) and 1b, the proximal fibula is absent for 30–50% ofits length with a dysplastic or absent ankle mortise joint. One of the sixknees in our series was Type 1a and the remainder Type 2. None of thecases in our series were Type 1b.
4.2. Osseous deformity
Skeletal abnormalities of the knee are commonly seen in fibularhemimelia. Apart from the absence or hypoplasia of the fibula, thereare characteristic findings [8]. These include dysplasia of the distalfemur with an absent or poorly formed intercondylar notch, shallowtrochlear groove and hypoplastic lateral femoral condyle. Convexity ofthe proximal tibial epiphysis with absent or hypoplastic tibial spines isalso common (Fig. 4). Naturally, the presence of intercondylar dysplasiapredicts hypoplasia or absence of the cruciate ligaments. In addition,genu valgum and tibial bowing are recognised findings. Four of the sixknees in our series showed intercondylar dysplasia with convex proxi-mal tibial epiphyses and absent or hypoplastic spines, and in all theseknees there was no anterior cruciate ligament (ACL) and a hypoplastic(3/4) or absent (1/4) posterior cruciate ligament (PCL) (Table 1.). Two
the knee in fibular hemimelia: Radiographic and MRI findings, Knee
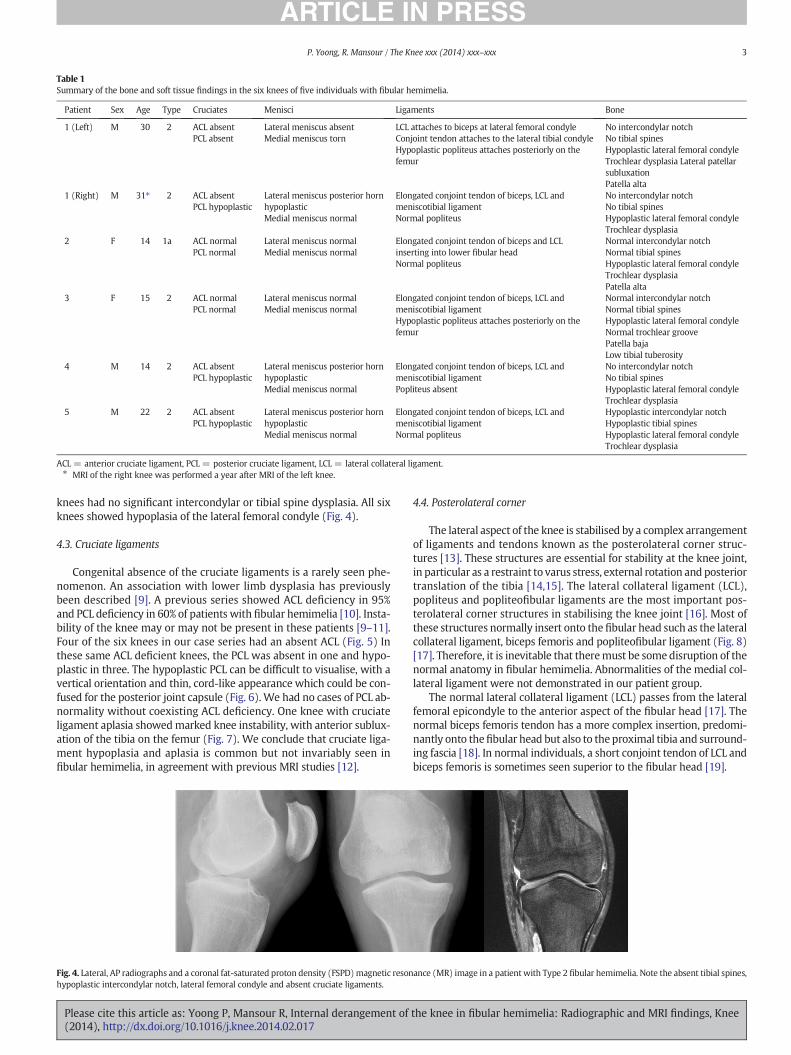
Table 1Summary of the bone and soft tissue findings in the six knees of five individuals with fibular hemimelia.
Patient Sex Age Type Cruciates Menisci Ligaments Bone
1 (Left) M 30 2 ACL absentPCL absent
Lateral meniscus absentMedial meniscus torn
LCL attaches to biceps at lateral femoral condyleConjoint tendon attaches to the lateral tibial condyleHypoplastic popliteus attaches posteriorly on thefemur
No intercondylar notchNo tibial spinesHypoplastic lateral femoral condyleTrochlear dysplasia Lateral patellarsubluxationPatella alta
1 (Right) M 31⁎ 2 ACL absentPCL hypoplastic
Lateral meniscus posterior hornhypoplasticMedial meniscus normal
Elongated conjoint tendon of biceps, LCL andmeniscotibial ligamentNormal popliteus
No intercondylar notchNo tibial spinesHypoplastic lateral femoral condyleTrochlear dysplasia
2 F 14 1a ACL normalPCL normal
Lateral meniscus normalMedial meniscus normal
Elongated conjoint tendon of biceps and LCLinserting into lower fibular headNormal popliteus
Normal intercondylar notchNormal tibial spinesHypoplastic lateral femoral condyleTrochlear dysplasiaPatella alta
3 F 15 2 ACL normalPCL normal
Lateral meniscus normalMedial meniscus normal
Elongated conjoint tendon of biceps, LCL andmeniscotibial ligamentHypoplastic popliteus attaches posteriorly on thefemur
Normal intercondylar notchNormal tibial spinesHypoplastic lateral femoral condyleNormal trochlear groovePatella bajaLow tibial tuberosity
4 M 14 2 ACL absentPCL hypoplastic
Lateral meniscus posterior hornhypoplasticMedial meniscus normal
Elongated conjoint tendon of biceps, LCL andmeniscotibial ligamentPopliteus absent
No intercondylar notchNo tibial spinesHypoplastic lateral femoral condyleTrochlear dysplasia
5 M 22 2 ACL absentPCL hypoplastic
Lateral meniscus posterior hornhypoplasticMedial meniscus normal
Elongated conjoint tendon of biceps, LCL andmeniscotibial ligamentNormal popliteus
Hypoplastic intercondylar notchHypoplastic tibial spinesHypoplastic lateral femoral condyleTrochlear dysplasia
ACL = anterior cruciate ligament, PCL = posterior cruciate ligament, LCL = lateral collateral ligament.⁎ MRI of the right knee was performed a year after MRI of the left knee.
3P. Yoong, R. Mansour / The Knee xxx (2014) xxx–xxx
knees had no significant intercondylar or tibial spine dysplasia. All sixknees showed hypoplasia of the lateral femoral condyle (Fig. 4).
4.3. Cruciate ligaments
Congenital absence of the cruciate ligaments is a rarely seen phe-nomenon. An association with lower limb dysplasia has previouslybeen described [9]. A previous series showed ACL deficiency in 95%and PCL deficiency in 60% of patients with fibular hemimelia [10]. Insta-bility of the knee may or may not be present in these patients [9–11].Four of the six knees in our case series had an absent ACL (Fig. 5) Inthese same ACL deficient knees, the PCL was absent in one and hypo-plastic in three. The hypoplastic PCL can be difficult to visualise, with avertical orientation and thin, cord-like appearance which could be con-fused for the posterior joint capsule (Fig. 6). We had no cases of PCL ab-normality without coexisting ACL deficiency. One knee with cruciateligament aplasia showedmarked knee instability, with anterior sublux-ation of the tibia on the femur (Fig. 7). We conclude that cruciate liga-ment hypoplasia and aplasia is common but not invariably seen infibular hemimelia, in agreement with previous MRI studies [12].
Fig. 4. Lateral, AP radiographs and a coronal fat-saturated proton density (FSPD)magnetic resonhypoplastic intercondylar notch, lateral femoral condyle and absent cruciate ligaments.
Please cite this article as: Yoong P, Mansour R, Internal derangement of(2014), http://dx.doi.org/10.1016/j.knee.2014.02.017
4.4. Posterolateral corner
The lateral aspect of the knee is stabilised by a complex arrangementof ligaments and tendons known as the posterolateral corner struc-tures [13]. These structures are essential for stability at the knee joint,in particular as a restraint to varus stress, external rotation and posteriortranslation of the tibia [14,15]. The lateral collateral ligament (LCL),popliteus and popliteofibular ligaments are the most important pos-terolateral corner structures in stabilising the knee joint [16]. Most ofthese structures normally insert onto the fibular head such as the lateralcollateral ligament, biceps femoris and popliteofibular ligament (Fig. 8)[17]. Therefore, it is inevitable that theremust be somedisruption of thenormal anatomy in fibular hemimelia. Abnormalities of the medial col-lateral ligament were not demonstrated in our patient group.
The normal lateral collateral ligament (LCL) passes from the lateralfemoral epicondyle to the anterior aspect of the fibular head [17]. Thenormal biceps femoris tendon has a more complex insertion, predomi-nantly onto thefibular head but also to the proximal tibia and surround-ing fascia [18]. In normal individuals, a short conjoint tendon of LCL andbiceps femoris is sometimes seen superior to the fibular head [19].
ance (MR) image in a patient with Type 2 fibular hemimelia. Note the absent tibial spines,
the knee in fibular hemimelia: Radiographic and MRI findings, Knee

Fig. 5. Sagittal T1 midline MR image. Both cruciate ligaments are absent.
4 P. Yoong, R. Mansour / The Knee xxx (2014) xxx–xxx
The popliteus muscle passes obliquely upwards from the posterioraspect of the tibia, with the tendon running deep to the LCL, inseparablefrom the posterior horn of the lateralmeniscus, inserting into the poste-rior aspect of the lateral condyle of the femur. The popliteofibular liga-ment passes between the posteromedial fibular styloid and popliteustendon [20] but is not consistently seen on MRI [19].
Fig. 6. Sagittal FSPD MR image. A vertical orientated, hypoplastic, cord-like PCL (arrows).The ACL is absent.
Fig. 7. Large field of view sagittal T1 MR image of the knee and lower leg. There is asubluxed ACL and PCL deficient knee in Type 2 fibular hemimeliawith anterior translationof the tibia. Note the vestigial fibula (arrow).
Please cite this article as: Yoong P, Mansour R, Internal derangement of(2014), http://dx.doi.org/10.1016/j.knee.2014.02.017
In our patient group, an elongated conjoint tendon of biceps femorisand LCL is seen (Fig. 9) to descend into the lower leg in the plane be-tween the peroneal musculature anteriorly and lateral gastrocnemiusmuscle posteriorly (Fig. 10). In four of the six knees, there is a furtherthickened ligamentous structure, which also joins the conjoint tendon,arising from the posterior horn of the lateralmeniscus (Fig. 11). This ap-pears to be a thickening of the normal meniscotibial ligament. In oneknee, there was a prominent ligamentous attachment to the lateral as-pect of the proximal tibia from the biceps femoris, more prominentthan that normally seen (Fig. 12).
In three of six knees, the popliteus musculotendinous complex wasabnormal. In two knees, the popliteal tendon was hypoplastic andthere was an anomalous insertion, more posteroinferiorly on the tibia(Fig. 13). In one knee, there was no popliteus muscle or tendon.
The popliteofibular, fabellofibular and arcuate ligaments complexeswere not seen in any of our patients, although they are often not visibleon a normal MRI scan [19]. The iliotibial band was intact in all six knees.Therewas a normal insertion of the lateral head of gastrocnemius tendonin all six knees. The recently described anterolateral ligament of the knee[21], running between the lateral femoral condyle and the anterolateraltibia, anterior to the LCL,was not convincingly seen in any of the six cases.
In the context of acute knee trauma, undiagnosed injury to the pos-terolateral corner structures and resultant instability in associated withearly osteoarthritis [19]. We cannot be sure whether a congenital pos-terolateral corner deficiency is associated with long-term functionaldeficit in fibular hemimelia. We do not have long-term data on our
the knee in fibular hemimelia: Radiographic and MRI findings, Knee
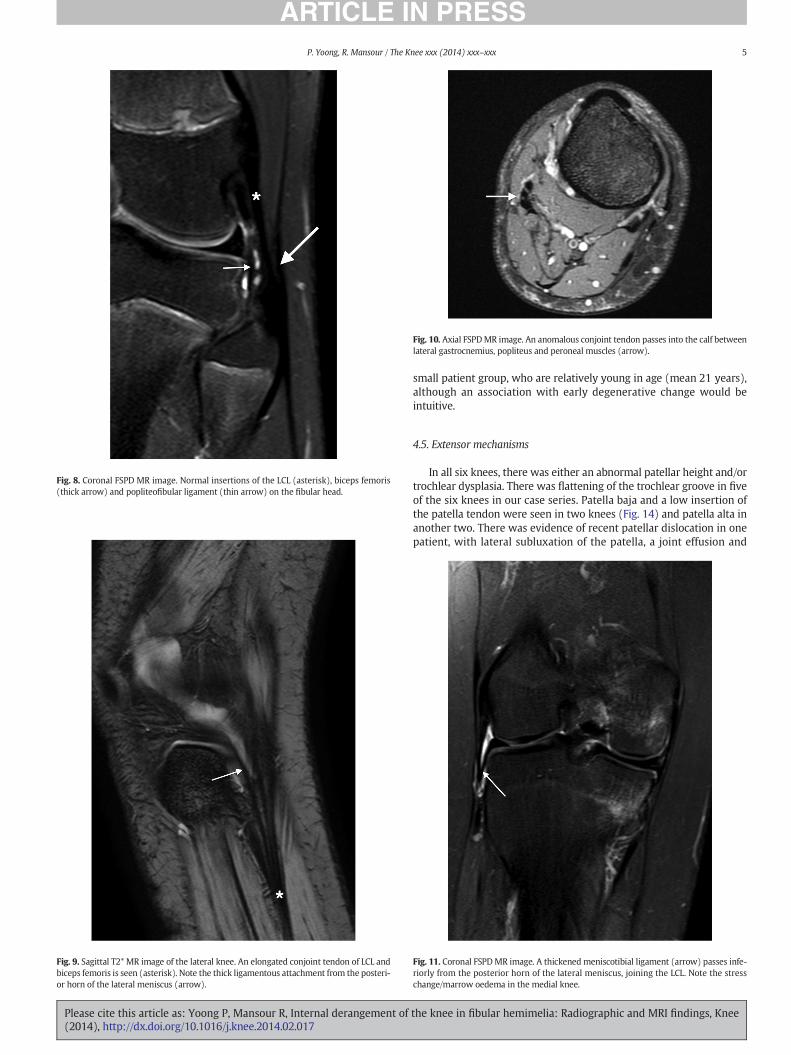
Fig. 8. Coronal FSPD MR image. Normal insertions of the LCL (asterisk), biceps femoris(thick arrow) and popliteofibular ligament (thin arrow) on the fibular head.
Fig. 9. Sagittal T2* MR image of the lateral knee. An elongated conjoint tendon of LCL andbiceps femoris is seen (asterisk). Note the thick ligamentous attachment from the posteri-or horn of the lateral meniscus (arrow).
Fig. 10. Axial FSPDMR image. An anomalous conjoint tendon passes into the calf betweenlateral gastrocnemius, popliteus and peroneal muscles (arrow).
5P. Yoong, R. Mansour / The Knee xxx (2014) xxx–xxx
Please cite this article as: Yoong P, Mansour R, Internal derangement of(2014), http://dx.doi.org/10.1016/j.knee.2014.02.017
small patient group, who are relatively young in age (mean 21 years),although an association with early degenerative change would beintuitive.
4.5. Extensor mechanisms
In all six knees, there was either an abnormal patellar height and/ortrochlear dysplasia. There was flattening of the trochlear groove in fiveof the six knees in our case series. Patella baja and a low insertion ofthe patella tendon were seen in two knees (Fig. 14) and patella alta inanother two. There was evidence of recent patellar dislocation in onepatient, with lateral subluxation of the patella, a joint effusion and
Fig. 11. Coronal FSPDMR image. A thickenedmeniscotibial ligament (arrow) passes infe-riorly from the posterior horn of the lateral meniscus, joining the LCL. Note the stresschange/marrow oedema in the medial knee.
the knee in fibular hemimelia: Radiographic and MRI findings, Knee
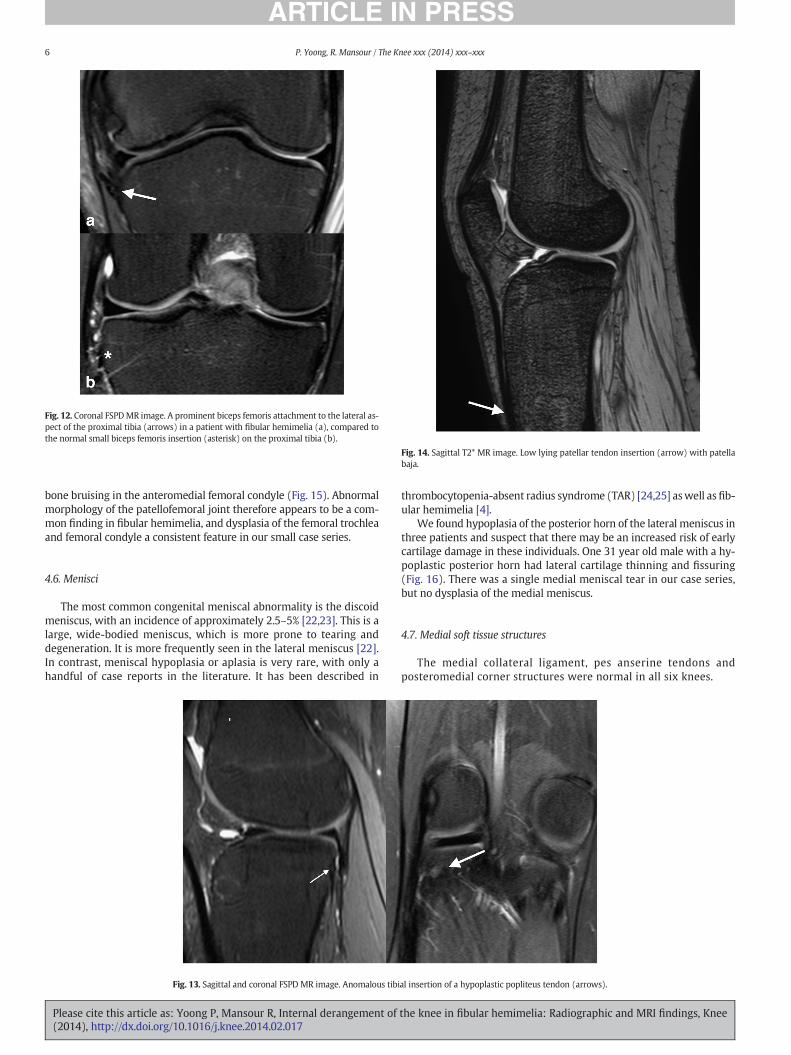
Fig. 12. Coronal FSPDMR image. A prominent biceps femoris attachment to the lateral as-pect of the proximal tibia (arrows) in a patient with fibular hemimelia (a), compared tothe normal small biceps femoris insertion (asterisk) on the proximal tibia (b).
Fig. 14. Sagittal T2* MR image. Low lying patellar tendon insertion (arrow) with patellabaja.
6 P. Yoong, R. Mansour / The Knee xxx (2014) xxx–xxx
bone bruising in the anteromedial femoral condyle (Fig. 15). Abnormalmorphology of the patellofemoral joint therefore appears to be a com-mon finding in fibular hemimelia, and dysplasia of the femoral trochleaand femoral condyle a consistent feature in our small case series.
4.6. Menisci
The most common congenital meniscal abnormality is the discoidmeniscus, with an incidence of approximately 2.5–5% [22,23]. This is alarge, wide-bodied meniscus, which is more prone to tearing anddegeneration. It is more frequently seen in the lateral meniscus [22].In contrast, meniscal hypoplasia or aplasia is very rare, with only ahandful of case reports in the literature. It has been described in
Fig. 13. Sagittal and coronal FSPD MR image. Anomalous tibi
Please cite this article as: Yoong P, Mansour R, Internal derangement of(2014), http://dx.doi.org/10.1016/j.knee.2014.02.017
thrombocytopenia-absent radius syndrome (TAR) [24,25] aswell asfib-ular hemimelia [4].
We found hypoplasia of the posterior horn of the lateral meniscus inthree patients and suspect that there may be an increased risk of earlycartilage damage in these individuals. One 31 year old male with a hy-poplastic posterior horn had lateral cartilage thinning and fissuring(Fig. 16). There was a single medial meniscal tear in our case series,but no dysplasia of the medial meniscus.
4.7. Medial soft tissue structures
The medial collateral ligament, pes anserine tendons andposteromedial corner structures were normal in all six knees.
al insertion of a hypoplastic popliteus tendon (arrows).
the knee in fibular hemimelia: Radiographic and MRI findings, Knee
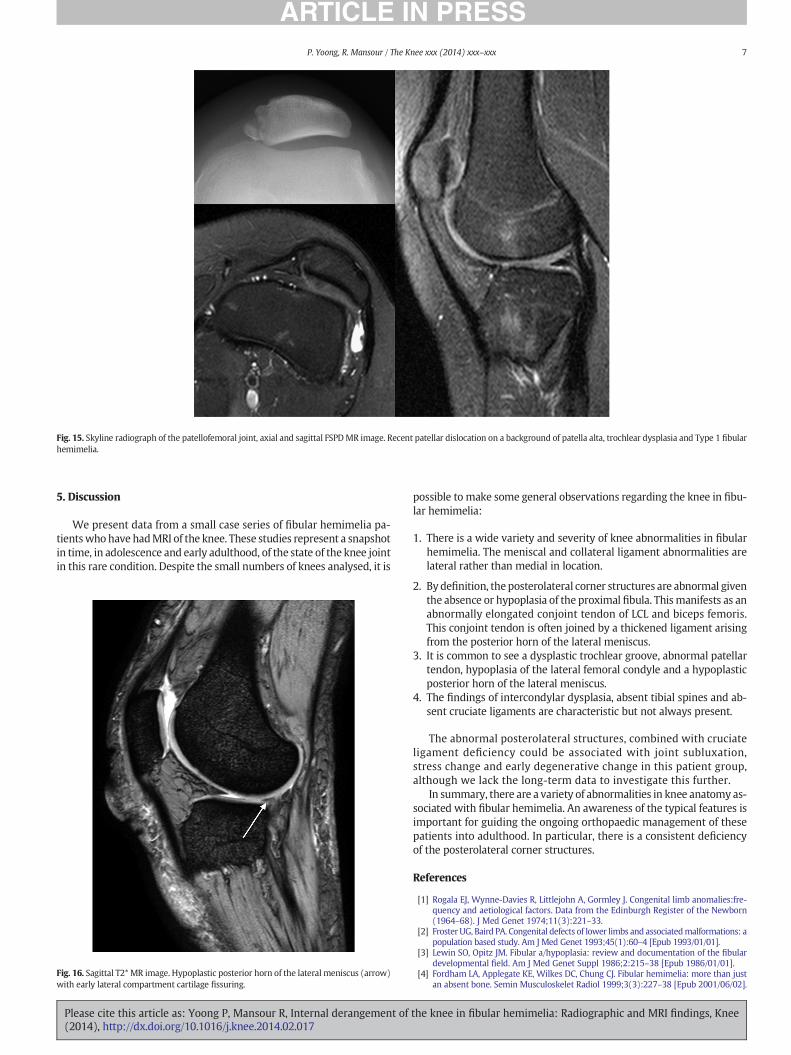
Fig. 15. Skyline radiograph of the patellofemoral joint, axial and sagittal FSPDMR image. Recent patellar dislocation on a background of patella alta, trochlear dysplasia and Type 1 fibularhemimelia.
7P. Yoong, R. Mansour / The Knee xxx (2014) xxx–xxx
5. Discussion
We present data from a small case series of fibular hemimelia pa-tientswhohave hadMRI of the knee. These studies represent a snapshotin time, in adolescence and early adulthood, of the state of the knee jointin this rare condition. Despite the small numbers of knees analysed, it is
Fig. 16. Sagittal T2* MR image. Hypoplastic posterior horn of the lateral meniscus (arrow)with early lateral compartment cartilage fissuring.
Please cite this article as: Yoong P, Mansour R, Internal derangement of(2014), http://dx.doi.org/10.1016/j.knee.2014.02.017
possible to make some general observations regarding the knee in fibu-lar hemimelia:
1. There is a wide variety and severity of knee abnormalities in fibularhemimelia. The meniscal and collateral ligament abnormalities arelateral rather than medial in location.
2. By definition, theposterolateral corner structures are abnormal giventhe absence or hypoplasia of the proximal fibula. Thismanifests as anabnormally elongated conjoint tendon of LCL and biceps femoris.This conjoint tendon is often joined by a thickened ligament arisingfrom the posterior horn of the lateral meniscus.
3. It is common to see a dysplastic trochlear groove, abnormal patellartendon, hypoplasia of the lateral femoral condyle and a hypoplasticposterior horn of the lateral meniscus.
4. The findings of intercondylar dysplasia, absent tibial spines and ab-sent cruciate ligaments are characteristic but not always present.
The abnormal posterolateral structures, combined with cruciateligament deficiency could be associated with joint subluxation,stress change and early degenerative change in this patient group,although we lack the long-term data to investigate this further.
In summary, there are a variety of abnormalities in knee anatomy as-sociated with fibular hemimelia. An awareness of the typical features isimportant for guiding the ongoing orthopaedic management of thesepatients into adulthood. In particular, there is a consistent deficiencyof the posterolateral corner structures.
References
[1] Rogala EJ, Wynne-Davies R, Littlejohn A, Gormley J. Congenital limb anomalies:fre-quency and aetiological factors. Data from the Edinburgh Register of the Newborn(1964–68). J Med Genet 1974;11(3):221–33.
[2] Froster UG, Baird PA. Congenital defects of lower limbs and associatedmalformations: apopulation based study. Am J Med Genet 1993;45(1):60–4 [Epub 1993/01/01].
[3] Lewin SO, Opitz JM. Fibular a/hypoplasia: review and documentation of the fibulardevelopmental field. Am J Med Genet Suppl 1986;2:215–38 [Epub 1986/01/01].
[4] Fordham LA, Applegate KE, Wilkes DC, Chung CJ. Fibular hemimelia: more than justan absent bone. Semin Musculoskelet Radiol 1999;3(3):227–38 [Epub 2001/06/02].
the knee in fibular hemimelia: Radiographic and MRI findings, Knee

8 P. Yoong, R. Mansour / The Knee xxx (2014) xxx–xxx
[5] Rodriguez-Ramirez A, Thacker MM, Becerra LC, Riddle EC, Mackenzie WG. Limblength discrepancy and congenital limb anomalies in fibular hemimelia. J PediatrOrthop B 2010;19(5):436–40 [Epub 2010/05/26].
[6] Oberc A, Sulko J. Fibular hemimelia — diagnostic management, principles, and re-sults of treatment. J Pediatr Orthop B 2013;22(5):450–6 [Epub 2013/06/29].
[7] Achterman C, Kalamchi A. Congenital deficiency of the fibula. J Bone Joint Surg Br1979;61-B(2):133–7 [Epub 1979/05/01].
[8] Chelli-Bouaziz M, Bouaziz N, Bianchi-Zamorani MP, Fritschy D, Bianchi S. Knee trauma:cruciate ligament dysplasia associated with fibular hemimelia (2003:7b). Eur Radiol2003;13(10):2402–4 [Epub 2003/10/29].
[9] Thomas NP, Jackson AM, Aichroth PM. Congenital absence of the anterior cruciate liga-ment. A common component of knee dysplasia. J Bone Joint Surg Br 1985;67(4):572–5[Epub 1985/08/01].
[10] RouxMO, Carlioz H. Clinical examination and investigation of the cruciate ligamentsin childrenwith fibular hemimelia. J Pediatr Orthop 1999;19(2):247–51 [Epub 1999/03/24].
[11] Crawford SN, Waterman BR, Lubowitz JH. Long-term failure of anterior cruciate lig-ament reconstruction. Arthroscopy 2013;29(9):1566–71 [Epub 2013/07/04].
[12] Laor T, Jaramillo D, Hoffer FA, Kasser JR. MR imaging in congenital lower limb defor-mities. Pediatr Radiol 1996;26(6):381–7 [Epub 1996/01/01].
[13] Pacholke DA, Helms CA. MRI of the posterolateral corner injury: a concise review. JMagn Reson Imaging 2007;26(2):250–5 [Epub 2007/07/12].
[14] Veltri DM, Deng XH, Torzilli PA, Maynard MJ, Warren RF. The role of thepopliteofibular ligament in stability of the human knee. A biomechanical study.Am J Sports Med 1996;24(1):19–27 [Epub 1996/01/01].
[15] Veltri DM, Deng XH, Torzilli PA, Warren RF, Maynard MJ. The role of the cruciate andposterolateral ligaments in stability of the knee. A biomechanical study. Am J SportsMed 1995;23(4):436–43 [Epub 1995/07/01].
Please cite this article as: Yoong P, Mansour R, Internal derangement of(2014), http://dx.doi.org/10.1016/j.knee.2014.02.017
[16] LaPrade RF, Resig S, Wentorf F, Lewis JL. The effects of grade III posterolateral kneecomplex injuries on anterior cruciate ligament graft force. A biomechanical analysis.Am J Sports Med 1999;27(4):469–75 [Epub 1999/07/29].
[17] Brinkman JM, Schwering PJ, Blankevoort L, Kooloos JG, Luites J, Wymenga AB. Theinsertion geometry of the posterolateral corner of the knee. J Bone Joint Surg Br2005;87(10):1364–8 [Epub 2005/09/29].
[18] Vieira RL, Rosenberg ZS, Kiprovski K. MRI of the distal biceps femoris muscle: normalanatomy, variants, and association with common peroneal entrapment neuropathy.AJR Am J Roentgenol 2007;189(3):549–55 [Epub 2007/08/24].
[19] Vinson EN, Major NM, Helms CA. The posterolateral corner of the knee. AJR Am JRoentgenol 2008;190(2):449–58 [Epub 2008/01/24].
[20] Shahane SA, Ibbotson C, Strachan R, Bickerstaff DR. The popliteofibular ligament. Ananatomical study of the posterolateral corner of the knee. J Bone Joint Surg Am1999;81(4):636–42 [Epub 1999/08/27].
[21] Claes S, Vereecke E, MaesM, Victor J, Verdonk P, Bellemans J. Anatomy of the antero-lateral ligament of the knee. J Anat 2013;223(4):321–8 [Epub 2013/08/03].
[22] Nathan PA, Cole SC. Discoid meniscus. A clinical and pathologic study. Clin OrthopRelat Res 1969;64:107–13 [Epub 1969/05/01].
[23] Rohren EM, Kosarek FJ, Helms CA. Discoid lateral meniscus and the frequency ofmeniscal tears. Skeletal Radiol 2001;30(6):316–20 [Epub 2001/07/24].
[24] Tolo VT. Congenital absence of themenisci and cruciate ligaments of the knee. A casereport. J Bone Joint Surg Am 1981;63(6):1022–4 [Epub 1981/07/01].
[25] Heron D, Bonnard C, Moraine C, Toutain A. A genesis of cruciate ligaments and me-nisci causing severe knee dysplasia in TAR syndrome. J Med Genet 2001;38(8):E27[Epub 2001/08/03].
the knee in fibular hemimelia: Radiographic and MRI findings, Knee





























