Embed Size (px)
Citation preview

8/3/2019 Intermittent Cyclical Etidronate in the Prevention of Corticoids Induced Bone Loss
http://slidepdf.com/reader/full/intermittent-cyclical-etidronate-in-the-prevention-of-corticoids-induced-bone 1/3
British Journal of Rheumatology 1994;33:348-350
INTERMITTENT CYCLICAL ETIDRONATE IN THE PREVENTION OF
CORTICOSTEROID-INDUCED BONE LOSS
H. MULDER* and A. STRUYSt
*Gezondheidscentrum Zuidplein, Metroplein 50 , 3083 BB Rotterdam, and fSint Clara Hospital,Olympiaweg 350, 3075 HT Rotterdam, The Netherlands
SUMMARY
We conducted a prospective study of etidronate's effects on corticosteroid-induced bone loss in postmenopausal womenwith temporal arteritis for whom high-dose prednisone therapy was indicated. Group A (n=10) received etidronate (400mg/day for 2 weeks, then 11 weeks off etidronate; four cycles total) and prednisone; Group B (/i=10) received onlyprednisone. Vertebral bone mineral density (BMD ) was measured blinded by dual X-ray absorptiometry.
At 3,6 and 12 months, vertebral BM D was significantly (P<0.01 ) increased in Group A and decreased in Group B, based onmean actual and percent changes in BMD and mean changes in BMD Z-score from baseline. Between-group comparisonswere also significant (P<0.002) at each time point. No adverse events related to etidronate treatment were reported.
Our results suggest that corticosteroid-induced bone loss may be prevented by instituting intermittent cyclicaletidronate therapy when high-dose prednisone therapy is begun. Further research into bisphosphonate use incorticosteroid-induced bone loss (with larger patient populations, longer follow-up and fracture assessment) is warranted.
KEY WORDS: Bone loss, Corticosteroids, Etidronate, P rednisone, Temporal arteritis.
TH E concept that excess endogenous glucocorticoidcan lead to an increased tendency to fracture was firstdescribed by C ushing in 1932 [1]. Soo n after the intro-duction of cortisone as a therapeutic agent, it becameclear that exogen ous h ypercortisolism was also delete-rious to the skeleton [2]. Both b one quantity and bonequality are decreased with the use of corticosteroids.Prospective studies of bon e mass during corticosteroidtreatm ent have confirmed that their use can cause pro-gressive bon e loss [2]. Da ta suggest that up to 50% ofpatients tak ing glucocorticoids lon g-term will developosteoporosis and experience atraumatic fractures dueto the resultant comp romised bon e quality [2-4].
The pathogenesis of corticosteroid-induced bone
loss is associated with decreased bone formation andincreased bon e resorptio n [2]. Decreased intestinalcalcium absorption and increased urinary calciumexcretion are also attributable to corticosteroid useand contribute to a negative calcium balance [2]. Thisnegative balance in turn leads to secondary hy perpara-thyroidism that results in increased bone resorptiveactivity [2]. Th ese effects a re man ifested by acceler-ated bo ne loss early in treatm ent (within the first 6-12months), followed by continuing losses and slowerrates in subsequent ye ars [2,5].
Althoug h the effects of steroids on bone and calciumbalance are well described, no fully safe and effectivetherap eutic or proph ylactic regimen for corticosteroid-
induced bo ne loss has been established. H owever, anti-resorptive agents such as oestrogen [6], calcitonin(given either parenterally and nasally) [7], and the bis-phosph onate pa midron ate [8,9] have been reported tobe effective in preventing or reversing co rticosteroid-induced bon e loss. In ad dition, the prophylactic use ofcalcitriol and calcium, with or without calcitonin hasbeen shown to prevent corticosteroid-induced boneloss [10].
Subm itted 20 May; revised version accep ted 4 October 1993.
0263-7103/94/040348 + 03 $08.00/0
The bisphosphonate etidronate, given in an inter-mittent cyclical regimen, has been demonstrated toincrease vertebral bone mass significantly and reducethe incidence of vertebral fractures in patients withpostmenopausal osteoporosis [9,11]. The objective ofthe current study was to determine whether this anti-resorptive agent, when administered in a similar man-ner and at the outset of corticosteroid therapy, couldprevent the early accelerated bone loss associated withpharmacologic doses of prednisone.
. MATERIALS AND METH ODSStudy design
This study was conducted as a prospe ctive 1-yr clini-
cal trial according to the guidelines of the H elsinki dec-laration for physician-initiated studies. Patients wererecruited from one investigational site (IJsselland H os-pital, The Netherlands) from April 15 1990 toFebruary 1 1991. The study enrolled postm enopausalwomen with a biopsy-confirmed diagnosis of temporalarteritis for whom high-dose prednisone therapy wasindicated. Patients were excluded from the study ifthey had any disease or were receiving any medication,with the exception of the study d rugs, that w ould inter-fere with calcium or bone metabolism. A completehistory and physical examination including haemato-logic, serum chemistry, and urinalysis evaluations w ereperformed before treatment.
Patients were alternately assigned to one of twotreatmen t groups. Group A received interm ittent cycli-cal oral etidronate disodium 400 mg (Didronel®,Procter & Gamble Pharmaceuticals, Norwich, NewYork) once daily for 2 weeks, followed by 11 weeks oftherapy (four cycles total) in conjunction with appro -priate prednison e therapy. Grou p B received only pre-dnisone therapy. The daily prednisone dosage in bothgroups was 60 mg once daily for 4 weeks, followed bydose adjustment (decrease) to maintain an ESR sedi-
© 1994 British Society for Rheumatology
348

8/3/2019 Intermittent Cyclical Etidronate in the Prevention of Corticoids Induced Bone Loss
http://slidepdf.com/reader/full/intermittent-cyclical-etidronate-in-the-prevention-of-corticoids-induced-bone 2/3
MULDER AND STRUYS: ETIDRONATE PREVENTS STEROID-INDUCED BONE LOSS 349
mentation rate below 30 mm/h. Patients had a dailydietary calcium intak e of 400-800 mg; no supplementalcalcium was administered.
AssessmentVertebral (L1-L4) BMD was measured by dual
X-ray absorptiometry (H ologic QD R1 000) at baselineand at 3, 6 and 12 months by a technician blinded totreatment assignment. Serum alkaline phosphatase (abiochemical marker of bone turnover) was measuredat baseline and 12 months. Patients were judgedeligible for evaluation if they followed the prescribedregimens and had the scheduled BMD determinationsduring the 12-month study.
StatisticsVertebral BMD data, serum alkaline phosphatase,
and the respective actual and percent changes frombaseline in these clinical variables are displayed asmean ± S.E.M. Statistical comparisons (Minitab,Release 5.1, Minitab, Inc., State College, Pennsyl-vania) were performed by one-sample f-tests forbetween-groups changes, respectively. Z-scores (com-paring individual patients' BMDs with the mean ofBM D of age-matched normal w omen) w ere calculatedat baseline and at 3,6 and 12 months; f-scores (compar-ing individual patients ' BM Ds with the m ean BM D ofyoung normal women) were calculated only at base-line. Statistical significance was assigned as P<0.05.Ninety-five per cent confidence intervals were calcu-lated by a two-sample t procedure.
RESULTS
Ten women received intermittent cyclical etidronateconcurrently with the prescribed prednisone regimen(Group A); 10 women received only the prednisoneregimen (Group B). The mean age of the patientsreceiving etidronate and prednisone treatment was 74yr (range, 62-82 yr), and the mean age of the controlpatients was 72 yr (range 58-84 yr). Baseline BMD
(Table I) was not statistically significantly differentbetween the groups. At baseline, Z-scores were0.00±0.33 in Grou p A and 0.21 ±0.20 in G roup B (95%CI: -1.02, 0.61); /-scores were -2.26±0.45 and-1.80±0.32 in Group B.
Each of the patients responded to the prednisone
therapy for temporal arteritis. Mean prednisone dos-ages of the 12 month study period were 11.0 mg/day inGroup A and 10.7 mg/day in Group B.
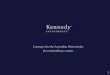
At 3, 6 and 12 months, vertebral BMD was signifi-cantly (/><0.01) increased in Group A and decreasedin Group B, based on mean actual and percent changesfrom baseline in BMD and mean changes from base-line BMD Z-score (Table I). Between-group compari-sons were also significant (P<0.002) at each timepoint. At 12 months, the mean percent change frombaseline in BMD was 1.42±0.45% in Group A and-4.95±0.64% in Group B; the 95 % CI showed that thedifference between the two treatment groups was atleast 4.71% and as much as 8.03%. Nine of the 10patients treated with etidronate and prednisone hadincreases in bone m ass, whereas all 10 patients treatedwith only predn isone had decreases (Fig. 1).
At 12 months, the change from baseline in serumalkaline phosphatase was 6.2±3.9% in Group A and-5.3± 3.0% in Group B (P<0.05, between groups). Noclinically significant changes in routine clinical andlaboratory evaluations were noted. Etidronate waswell tolerated, and no adverse events related to etidro-nate treatment were reported.
DISCUSSION
Our study demonstrated that intermittent cyclicaletidronate can prevent the negative effects of continu-ous prednisone use on bone mass. The study patients
were at high risk of developing osteoporosis, beingelderly postmenopausal women requiring first-timehigh-dose prednisone treatment for 6 months orlonger. The significant and progressive decreas es frombaseline in BM D in the group treated with pred nisone
TABLE IVertebral bone mineral density
Measurement
Length oftreatment(months) G roup A G roup B 95% CI*
BMD (g/cm2)
Change from baseline (g/cm 2)
Percentage change from baseline (%)
Change from baseline (Z-score)
Baseline36
1236
1236
1236
12
0.798±0.0500.802±0.0500.807±0.050
0.809±0.0500.005±0.001 t t0.009±0.003tt0.011±0.003tt0.58 ±0.14 n
l . io ±0.31 n1.42 ±0.45 n0.06 ±0.01 tt0.11 ±0.02 t*0.16 ±0.03 n
0.850±0.0350.829±0.0340.815±0.033
0.807±0.032-0.020±0.002+--0.035±0.004+--0 .042±0.006t
-2.36 ±0.25 %-4.09 ±0.45 t-4.95 ±0.64 t
0.01 ±0.00 t0.10 ±0.03 t
-0.15 ±0.04 t
-0.180,-0.155,-0.136,
-0.125,0.02,0.034,0.040,2.33,4.02,4.71,0.02,0.14,0.20,
0.076
0.1010.121
0.1290.030
0.054
0.068
3.576.368.030.070.290.41
Group A (n=10) received intermittent cyclicla etidronate in conjunction with high-dose prednisone; Group B (/i=10) received high-dose prednisone only. Vertebral BMD.
•95% CI applies to the difference between treatment groups and was calculated by a two-sample /-procedure. t/ '<0.002, comparedwith Goup B; two-sample /-test. t / ' < 0 . 0 1 , compared with baseline; one-sample /-test.

8/3/2019 Intermittent Cyclical Etidronate in the Prevention of Corticoids Induced Bone Loss
http://slidepdf.com/reader/full/intermittent-cyclical-etidronate-in-the-prevention-of-corticoids-induced-bone 3/3
350 BRITISH JOURNAL OF RH EUMATOLOGY VOL. 33 NO. 4
4.0 ,
2.0
0.0
m
1 - 2 . 0
ES -40
a.u
b
-8.0 .
-10.0
8
- § -
Et idronale & Prednisone Prednisone
FIG. 1.—Percent change from baseline in vertebral B MD after 12months of treatment with intermittent cyclical etidronate in con-junction with high-dose prednisone (/i=10) or high dose pre-dnisone only (n=10). Means are shown as horizontal bars.*/><0.001, compared with high-dose prednisone; two-sampleMest .
alone confirmed a continued loss of bon e mass inducedby prednisone in excess of losses due to age or meno-pause. In contrast, the patients who received con-current etidronate exhibited significant increases inbone mass that were comparable to those seen in stud-ies of etidronate in the treatment of postmenopausalosteoporosis [11,12]. The significant increases frombaseline in BM D Z -scores in this gro up further suggesta beneficial protection from or prevention of theseprogressive corticosteroid-induced and age-relatedlosses in bone mass. This is especially importantbecause of the recognized strong inverse relationshipbetween low bone mass and an increased risk of atrau-matic verteb ral fractures [13].
Controversy currently exists about the overall influ-ence of clinical factors (such as age, sex, underlyingdisease, dose, treatment duration etc.) on costicoste-roid-induced bone loss. Studies in heterogenouspatient populations have shown variable results as tothe contribu tion of these and other factors. H owever,because we studied a highly uniform population, the
conclusions drawn from our results can be interpretedindependent of other possibly confounding clinicalinfluences.
The result of this study of etidronate and those ofReid et al. [8,9] in their study of another bisphospho-nate, pam idron ate, suggest that this class of antiresorp-tive drugs can counteract corticosteroid-induced boneloss by producing an ov erall increase in bone mass. It isalso important to note that, in our study, etidronatetreatment was initiated at the same time as thepatients' first exposure to prednisone. This is in con-trast with the Reid et al. investigations, in which all
patients had already received long-term corticosteroidtreatment and likely experienced bone loss beforepamidronate intervention was begun [8,9]. Our resultssuggest that this drug-induced bone loss can be effec-tively prevented by instituting intermittent cyclical eti-dronate therapy as soon as high-dose prednisone
therapy is begun . H owever, because our studyinvolved a limited num ber of patients and was restric-ted to only those with temporal arteritis, further stud-ies to confirm the efficacy of bisphosphonates incorticosteroid-induced bone loss (i.e. with largerpatient populations, longer follow-up, and assessmentof fractures) is warranted.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the valuable con-tribution of Mrs H . A. A. Snelder, Director of ClinicalResearch, Good Clinical Practice, Bergweg 66, Rotter-dam, for performing bone mass measurements.
REFERENCES
1. Cushing H . The basophil adenom as of the pituitary
body and their clinical manifestations (p ituitary baso-philism). Bull Johns Hopkins Hosp 1932;l:137-92.2. Lukert BP, Raisz LG. Glucocorticoid-induced osteo-
porosis: Pathogenesis and management. Ann InternMed 1990;112:352-64.
3. Adinoff AD, H olister JR . Steroid-induced fracturesand bone loss in patients with asthma. New Engl JMed 1983 ;309:265-8.
4. Ruegsegger, P, Medici TC , Anliker M. Corticosteroid-induced bone loss. A longitudinal study of alternateday therapy in patients with bronchial asthma usingquantitative computed tomography. Eur J Clin Phar-
macol 1983;25:615-20.5. Silverman SL. Management of corticosteroid-induced
osteoporosis: A clinician's perspective (editorial).Calcif Tissue Int 1992;50:101-3.
6. Lukert BP, Johnson B E, Robinson RG. Estrogen andprogesterone replacement therapy reduces glucocor-ticoid-induced bone loss. / Bone Min Res 1992;7:1063-9.
7. Mo ntem urro L, Schiraldi G, Fraioli P, Tosi G, RiboldiA, Rissato G. Prevention of corticosteroid-inducedosteoporosis with salmon calcitonin in sarcoidpatients Calcif Tissue In t 1991;49:71-6.
8. Reid IR, King AR, Alexan der CJ, Ibbertson H K. Pre-vention of steroid-induced osteoporosis with(3-amino-l-hydroxypropylidene)-l, 1-bisphospho-nate (APD). Lancet 1988;i:143-6.
9. Reid IR, H eap SW, King AR, Ibber tson H K. Twoyear follow-up of bisphosphonate (APD) treatmentin steroid osteoporosis. Lancet 1988;ii:1144.
10. Sambrook P, Birmingham J, Kelly P, Kempler S,Ngnyen T, Pocock N, Eism an J. Prevention of cortico-steroid o steoporosis. N EngU Med 1993;328:1747-52.
11 . Storm T, Tham sborg G, Steiiche T, Genant H , Soren-sen OH . Effect of intermittant cyclical etidronatetherapy on bone mass and fracture rate in womenwith postmenopausal osteoporosis. N Engl J Med1990;322:1265-71.
12. Watts NB, H arr is ST, Genant H K et al. Intermittentcyclical etidronate treatment of postmenopausalosteoporosis. N EngU Med 1990;323:73-9.
13. Ross PD, Wasnich RD, Vogel JM. Detection of pre-fracture spinal osteoporosis using bone mineralabsorptiometry. J Bone Min Res 1988;3:1-11.