Embed Size (px)
Citation preview

Transplant Immunology 21 (2009) 13–17
Contents lists available at ScienceDirect
Transplant Immunology
j ourna l homepage: www.e lsev ie r.com/ locate / t r im
Interleukin 8 −251TNA and Interferon gamma +874ANT polymorphism: Potentialpredictors of allograft outcome in renal transplant recipients from north India☆
Ranjana Singh, Pravin Kesarwani, Dinesh K. Ahirwar, Rakesh Kapoor, Rama D. Mittal ⁎Department of Urology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareli Road, Lucknow 226014, Uttar Pradesh, India
☆ Grant support: The study was supported by grant froIndustrial Research (CSIR) New Delhi, India (No. 27(018⁎ Corresponding author. Department of Urology, SGPG
226014, India. Tel.: +91 522 2668004 8x2116; fax: +91E-mail addresses: [email protected], rmittal@s
0966-3274/$ – see front matter © 2009 Published by Edoi:10.1016/j.trim.2009.01.001
a b s t r a c t
a r t i c l e i n f oArticle history:
Background: Episodes of ac Received 12 August 2008Received in revised form 26 December 2008Accepted 9 January 2009Keywords:IL8IFNGARMS-PCRRenal transplantationImmunosuppressantsAllograft rejection
ute rejection represent an important risk factor for the development of chronicallograft nephropathy. We explored whether certain cytokine gene polymorphisms in renal transplantrecipients may be useful markers for susceptibility to allograft rejection. Interleukin 8 (IL8) −251 TNA andinterferon gamma (IFNG) +874ANT gene polymorphisms were correlated with allograft outcome in renaltransplant recipients.Methods: Genotyping was done by amplification refractory mutational system-polymerase chain reaction(ARMS-PCR) in 264 healthy controls and 296 renal transplant recipients categorized into 235 non-rejectersand 61 rejecters.Results: IL8 −251AA genotype was associated with 2.7-folds increased risk for allograft rejection in recipientsexperiencing rejection episodes as compared to non-rejecters (OR=2.70, P=0.032). Cox proportional analysisrevealed N2-folds increased susceptibility for allograft rejection (HR=2.38, P=0.010) in IL8 −251AA recipients.Kaplan–Meier analysis also demonstrated lower mean time to first rejection episode for IL8 −251AA recipients(23 months) as compared to TT recipients (30 months) (log rank P=0.022). No association of IFNG+874ANT wasobserved with allograft rejection, however, an increasing trend towards immunosuppressant toxicity wasobserved in patients with +874TT genotype at one month post transplantation.Conclusion: Thus, IL8 −251AA genotype may serve as potential predictor of allograft outcome in our NorthIndian cohort of renal transplant recipients.
© 2009 Published by Elsevier B.V.
1. Introduction
Renal transplantation is the preferred treatment of choice for mostpatients with end stage renal failure. The recent advent of novelimmunosuppressive agents and new formulations has significantlyimproved the clinical outcome of renal transplant recipients. However,acute rejection episodes still occur in ~20–40% of organ transplantrecipients, while chronic rejection and allograft dysfunction remain themost common causes of long-term graft loss [1]. Thus, identification ofmarkers associated with or predictive of chronic allograft nephropathyshould prove clinically useful.
Chemokines and cytokines are potent inflammatory mediatorsdirectly involved in immunologic mechanisms mediating alloimmuneresponses. Interleukin 8 (IL8; CXCL8) belongs to the superfamily of CXC
m the Council of Scientific and5)/08/EMR-II).IMS, Raebareli Road, Lucknow-522 2668 017.gpgi.ac.in (R.D. Mittal).
lsevier B.V.
chemokines attracting neutrophils and macrophages and manifests awide rangeof proinflammatoryeffects [2,3]. It is reported tobe associatedwithThelper1 (Th1) typeof immune response in renal allograft rejection[4]. The IL8 gene is located on chromosome 4q13–21 and consists of fourexons, three introns, and a proximal promoter region [5]. The T/Apolymorphism located at−251nucleotides relative to the transcriptionalstart site of the gene is known to affect its expression [6]. Hull et al.suggested mutant A allele of the (−251) TNA polymorphism to beassociated with increased IL8 production by lipo-polysaccharide stimu-lated whole blood [7].
Interferon gamma (IFNG), another pro-inflammatory cytokine,produced by activated CD4+ T cells, defines the development of Th1response and promotes cell mediated immunity [8]. Several groups havepresented data that link Th1 cytokine pattern to allograft rejection [9,10].Amirzargar et al. reported significantlyhigher IFNGserumconcentrationsat 2 weeks post transplantation in group with acute rejection versusthose without acute rejection [11].
The human IFNG gene is located on chromosome 12q24.1. A singlenucleotidepolymorphism(SNP) inthefirst intronof IFNGgene(+874TNA)can putatively influence the secretion of IFNG [12]. Analysis of thebiological role of this SNP suggested that+874A carriers are low IFNGproducers [13]. In renal transplantation, the IFNG+874 TTgenotypewas
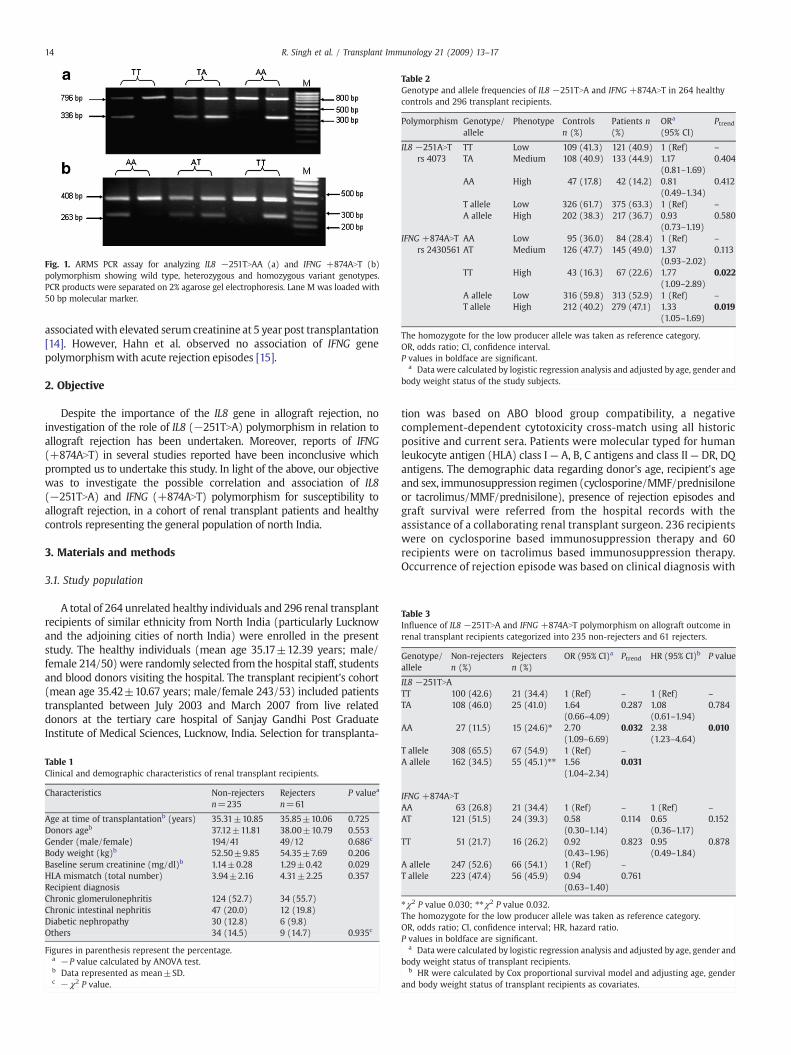
Fig. 1. ARMS PCR assay for analyzing IL8 −251TNAA (a) and IFNG +874ANT (b)polymorphism showing wild type, heterozygous and homozygous variant genotypes.PCR products were separated on 2% agarose gel electrophoresis. Lane M was loaded with50 bp molecular marker.
Table 2Genotype and allele frequencies of IL8 −251TNA and IFNG +874ANT in 264 healthycontrols and 296 transplant recipients.
Polymorphism Genotype/allele
Phenotype Controlsn (%)
Patients n(%)
ORa
(95% CI)Ptrend
IL8 −251ANTrs 4073
TT Low 109 (41.3) 121 (40.9) 1 (Ref) –
TA Medium 108 (40.9) 133 (44.9) 1.17(0.81–1.69)
0.404
AA High 47 (17.8) 42 (14.2) 0.81(0.49–1.34)
0.412
T allele Low 326 (61.7) 375 (63.3) 1 (Ref) –
A allele High 202 (38.3) 217 (36.7) 0.93(0.73–1.19)
0.580
IFNG +874ANTrs 2430561
AA Low 95 (36.0) 84 (28.4) 1 (Ref) –
AT Medium 126 (47.7) 145 (49.0) 1.37(0.93–2.02)
0.113
TT High 43 (16.3) 67 (22.6) 1.77(1.09–2.89)
0.022
A allele Low 316 (59.8) 313 (52.9) 1 (Ref) –
T allele High 212 (40.2) 279 (47.1) 1.33(1.05–1.69)
0.019
The homozygote for the low producer allele was taken as reference category.OR, odds ratio; CI, confidence interval.P values in boldface are significant.
a Data were calculated by logistic regression analysis and adjusted by age, gender andbody weight status of the study subjects.
Table 3Influence of IL8 −251TNA and IFNG +874ANT polymorphism on allograft outcome inrenal transplant recipients categorized into 235 non-rejecters and 61 rejecters.
Genotype/allele
Non-rejectersn (%)
Rejectersn (%)
OR (95% CI)a Ptrend HR (95% CI)b P value
IL8 −251TNATT 100 (42.6) 21 (34.4) 1 (Ref) – 1 (Ref) –
TA 108 (46.0) 25 (41.0) 1.64(0.66–4.09)
0.287 1.08(0.61–1.94)
0.784
AA 27 (11.5) 15 (24.6)⁎ 2.70(1.09–6.69)
0.032 2.38(1.23–4.64)
0.010
14 R. Singh et al. / Transplant Immunology 21 (2009) 13–17
associatedwith elevated serumcreatinine at 5 year post transplantation[14]. However, Hahn et al. observed no association of IFNG genepolymorphismwith acute rejection episodes [15].
2. Objective
Despite the importance of the IL8 gene in allograft rejection, noinvestigation of the role of IL8 (−251TNA) polymorphism in relation toallograft rejection has been undertaken. Moreover, reports of IFNG(+874ANT) in several studies reported have been inconclusive whichprompted us to undertake this study. In light of the above, our objectivewas to investigate the possible correlation and association of IL8(−251TNA) and IFNG (+874ANT) polymorphism for susceptibility toallograft rejection, in a cohort of renal transplant patients and healthycontrols representing the general population of north India.
3. Materials and methods
3.1. Study population
A total of 264 unrelated healthy individuals and 296 renal transplantrecipients of similar ethnicity from North India (particularly Lucknowand the adjoining cities of north India) were enrolled in the presentstudy. The healthy individuals (mean age 35.17±12.39 years; male/female 214/50) were randomly selected from the hospital staff, studentsand blood donors visiting the hospital. The transplant recipient's cohort(mean age 35.42±10.67 years; male/female 243/53) included patientstransplanted between July 2003 and March 2007 from live relateddonors at the tertiary care hospital of Sanjay Gandhi Post GraduateInstitute of Medical Sciences, Lucknow, India. Selection for transplanta-
Table 1Clinical and demographic characteristics of renal transplant recipients.
Characteristics Non-rejectersn=235
Rejectersn=61
P valuea
Age at time of transplantationb (years) 35.31±10.85 35.85±10.06 0.725Donors ageb 37.12±11.81 38.00±10.79 0.553Gender (male/female) 194/41 49/12 0.686c
Body weight (kg)b 52.50±9.85 54.35±7.69 0.206Baseline serum creatinine (mg/dl)b 1.14±0.28 1.29±0.42 0.029HLA mismatch (total number) 3.94±2.16 4.31±2.25 0.357Recipient diagnosisChronic glomerulonephritis 124 (52.7) 34 (55.7)Chronic intestinal nephritis 47 (20.0) 12 (19.8)Diabetic nephropathy 30 (12.8) 6 (9.8)Others 34 (14.5) 9 (14.7) 0.935c
Figures in parenthesis represent the percentage.a −P value calculated by ANOVA test.b Data represented as mean±SD.c −χ2 P value.
tion was based on ABO blood group compatibility, a negativecomplement-dependent cytotoxicity cross-match using all historicpositive and current sera. Patients were molecular typed for humanleukocyte antigen (HLA) class I — A, B, C antigens and class II— DR, DQantigens. The demographic data regarding donor's age, recipient's ageand sex, immunosuppression regimen (cyclosporine/MMF/prednisiloneor tacrolimus/MMF/prednisilone), presence of rejection episodes andgraft survival were referred from the hospital records with theassistance of a collaborating renal transplant surgeon. 236 recipientswere on cyclosporine based immunosuppression therapy and 60recipients were on tacrolimus based immunosuppression therapy.Occurrence of rejection episode was based on clinical diagnosis with
T allele 308 (65.5) 67 (54.9) 1 (Ref) –
A allele 162 (34.5) 55 (45.1)⁎⁎ 1.56(1.04–2.34)
0.031
IFNG +874ANTAA 63 (26.8) 21 (34.4) 1 (Ref) – 1 (Ref) –
AT 121 (51.5) 24 (39.3) 0.58(0.30–1.14)
0.114 0.65(0.36–1.17)
0.152
TT 51 (21.7) 16 (26.2) 0.92(0.43–1.96)
0.823 0.95(0.49–1.84)
0.878
A allele 247 (52.6) 66 (54.1) 1 (Ref) –
T allele 223 (47.4) 56 (45.9) 0.94(0.63–1.40)
0.761
⁎χ2 P value 0.030; ⁎⁎χ2 P value 0.032.The homozygote for the low producer allele was taken as reference category.OR, odds ratio; CI, confidence interval; HR, hazard ratio.P values in boldface are significant.
a Data were calculated by logistic regression analysis and adjusted by age, gender andbody weight status of transplant recipients.
b HR were calculated by Cox proportional survival model and adjusting age, genderand body weight status of transplant recipients as covariates.
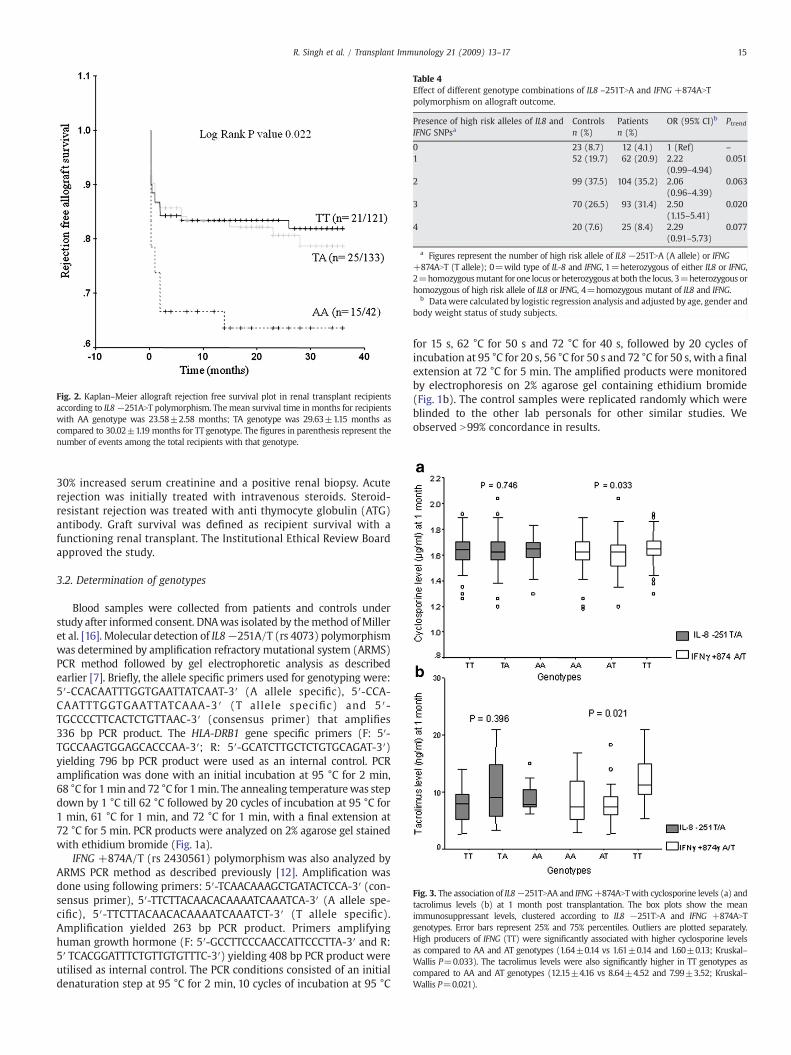
Fig. 2. Kaplan–Meier allograft rejection free survival plot in renal transplant recipientsaccording to IL8−251ANT polymorphism. The mean survival time in months for recipientswith AA genotype was 23.58±2.58 months; TA genotype was 29.63±1.15 months ascompared to 30.02±1.19 months for TT genotype. The figures in parenthesis represent thenumber of events among the total recipients with that genotype.
Table 4Effect of different genotype combinations of IL8 –251TNA and IFNG +874ANTpolymorphism on allograft outcome.
Presence of high risk alleles of IL8 andIFNG SNPsa
Controlsn (%)
Patientsn (%)
OR (95% CI)b Ptrend
0 23 (8.7) 12 (4.1) 1 (Ref) –
1 52 (19.7) 62 (20.9) 2.22(0.99–4.94)
0.051
2 99 (37.5) 104 (35.2) 2.06(0.96–4.39)
0.063
3 70 (26.5) 93 (31.4) 2.50(1.15–5.41)
0.020
4 20 (7.6) 25 (8.4) 2.29(0.91–5.73)
0.077
a Figures represent the number of high risk allele of IL8 −251TNA (A allele) or IFNG+874ANT (T allele); 0=wild type of IL-8 and IFNG, 1=heterozygous of either IL8 or IFNG,2=homozygousmutant for one locus or heterozygous at both the locus, 3=heterozygous orhomozygous of high risk allele of IL8 or IFNG, 4=homozygous mutant of IL8 and IFNG.
b Data were calculated by logistic regression analysis and adjusted by age, gender andbody weight status of study subjects.
Fig. 3. The association of IL8−251TNAA and IFNG+874ANT with cyclosporine levels (a) andtacrolimus levels (b) at 1 month post transplantation. The box plots show the meanimmunosuppressant levels, clustered according to IL8 −251TNA and IFNG +874ANTgenotypes. Error bars represent 25% and 75% percentiles. Outliers are plotted separately.High producers of IFNG (TT) were significantly associated with higher cyclosporine levelsas compared to AA and AT genotypes (1.64±0.14 vs 1.61±0.14 and 1.60±0.13; Kruskal–Wallis P=0.033). The tacrolimus levels were also significantly higher in TT genotypes ascompared to AA and AT genotypes (12.15±4.16 vs 8.64±4.52 and 7.99±3.52; Kruskal–Wallis P=0.021).
15R. Singh et al. / Transplant Immunology 21 (2009) 13–17
30% increased serum creatinine and a positive renal biopsy. Acuterejection was initially treated with intravenous steroids. Steroid-resistant rejection was treated with anti thymocyte globulin (ATG)antibody. Graft survival was defined as recipient survival with afunctioning renal transplant. The Institutional Ethical Review Boardapproved the study.
3.2. Determination of genotypes
Blood samples were collected from patients and controls understudy after informed consent. DNAwas isolated by themethod ofMilleret al. [16]. Molecular detection of IL8−251A/T (rs 4073) polymorphismwas determined by amplification refractory mutational system (ARMS)PCR method followed by gel electrophoretic analysis as describedearlier [7]. Briefly, the allele specific primers used for genotyping were:5′-CCACAATTTGGTGAATTATCAAT-3′ (A allele specific), 5′-CCA-CAATTTGGTGAATTATCAAA-3 ′ (T allele specific) and 5′-TGCCCCTTCACTCTGTTAAC-3′ (consensus primer) that amplifies336 bp PCR product. The HLA-DRB1 gene specific primers (F: 5′-TGCCAAGTGGAGCACCCAA-3′; R: 5′-GCATCTTGCTCTGTGCAGAT-3′)yielding 796 bp PCR product were used as an internal control. PCRamplification was done with an initial incubation at 95 °C for 2 min,68 °C for 1min and 72 °C for 1min. The annealing temperaturewas stepdown by 1 °C till 62 °C followed by 20 cycles of incubation at 95 °C for1 min, 61 °C for 1 min, and 72 °C for 1 min, with a final extension at72 °C for 5 min. PCR products were analyzed on 2% agarose gel stainedwith ethidium bromide (Fig. 1a).
IFNG +874A/T (rs 2430561) polymorphism was also analyzed byARMS PCR method as described previously [12]. Amplification wasdone using following primers: 5′-TCAACAAAGCTGATACTCCA-3′ (con-sensus primer), 5′-TTCTTACAACACAAAATCAAATCA-3′ (A allele spe-cific), 5′-TTCTTACAACACAAAATCAAATCT-3′ (T allele specific).Amplification yielded 263 bp PCR product. Primers amplifyinghuman growth hormone (F: 5′-GCCTTCCCAACCATTCCCTTA-3′ and R:5′ TCACGGATTTCTGTTGTGTTTC-3′) yielding 408 bp PCR product wereutilised as internal control. The PCR conditions consisted of an initialdenaturation step at 95 °C for 2 min, 10 cycles of incubation at 95 °C
for 15 s, 62 °C for 50 s and 72 °C for 40 s, followed by 20 cycles ofincubation at 95 °C for 20 s, 56 °C for 50 s and 72 °C for 50 s, with a finalextension at 72 °C for 5 min. The amplified products were monitoredby electrophoresis on 2% agarose gel containing ethidium bromide(Fig. 1b). The control samples were replicated randomly which wereblinded to the other lab personals for other similar studies. Weobserved N99% concordance in results.

16 R. Singh et al. / Transplant Immunology 21 (2009) 13–17
3.3. Statistical analysis
Each polymorphism was tested for Hardy–Weinberg equilibriumvia chi-square goodness of fit. The transplant outcome measures interms of rejection episodes were cross-tabulated against each poly-morphic genotype and differences among rejecters versus non-rejecterswere determined by chi-square analysis. Power of study was calculatedusing Quanto program version 1.1 (http://hydra.usc.edu/gxe) with inputof following variables, case–control study design, significancelevelb0.05 (2 sided), model of inheritance=log additive, minor allelefrequency=0.15, genetic effect (odds ratio)≤0.6 or≥1.6. Present studyachieved 80% of power which was sufficient to consider OR of ≤0.6 or≥1.6. Multiple logistic regression analysis was used to predict theassociation of IL8−252TNA and IFNG +874ANT SNPs with the allograftoutcome and risk was expressed as odds ratios (OR) with 95%confidence intervals (95% CI). ORs were adjusted for age, gender andbody weight status of the subjects. The mean immunosuppressantlevels at one month post transplantation were compared among thedifferent genotype groups by Kruskal–Wallis U test. Time-to-eventanalysis was performed using Kaplan–Meier estimates and log-ranktest. Time of occurrence of first rejection episode has been defined as anevent. Cox regression analysis was performed to calculate the hazardassociated with different genotypes. P values b0.05 (two-sided) wereconsidered significant. The statistical software package (SPSS 11.5 forWindows) was used for the calculations.
4. Results
A total of 264 unrelated healthy individuals and 296 renal transplant recipientswere included in the present study. The transplant recipients were further categorizedinto rejecters and non-rejecters based on biopsy proven allograft rejection. The overallincidence of rejection episode was 20.6% in our patient group. The relevantdemographic characteristics of transplant recipients are summarized in Table 1. Asexpected, the mean baseline serum creatinine (mg/dl) differed significantly amongnon-rejecters and rejecters (1.14±0.28 vs 1.29±0.42; P=0.029).
4.1. Genotype and allele frequency distribution of IL8−251TNA and IFNG+874ANT SNPs instudy population
We genotyped IL8 −251TNA and IFNG +874ANT polymorphisms in all the 560 studysubjects. Table 2 shows the genotype and allele frequencies in patients and healthy controls.Thegenotypedistribution instudied subjects followed theHardy–Weinbergequilibrium.Nosignificant differences in genotype or allele frequencies, between cases and controls, wereobserved for IL8−251TNApolymorphism. TheTTgenotypeof IFNG+874ANTpolymorphismwasmore prevalent in cases than in controls (OR=1.77, 95% CI,1.09–2.89, P=0.022). The Tallele of IFNG+874ANTwas alsomore prevalent in cases than in controls (OR=1.33, 95% CI,1.05–1.69, P=0.019).
On categorizing transplant recipients into non-rejecters and rejecters, the AA genotypeof IL8 −251TNA demonstrated significantly higher prevalence in rejecters as compared tonon-rejecters (OR=2.70, 95% CI, 1.09–6.69, P=0.032). The A allele of IL8 −251TNA alsodemonstrated higher prevalence in rejecters (OR=1.56, 95% CI,1.04–2.34,P=0.031) (Table3). No significant differences in genotype or allele frequencies, between rejecters and non-rejecters, were observed for IFNG +874ANT polymorphism.
4.2. Cox proportional and Kaplan–Meier analysis of time to first rejection episode
The Cox proportional hazardsmodel was used to analyze the influence of IL8−251TNAand IFNG +874ANT polymorphism and allograft outcome using months to initial rejectionepisode as the dependent variable and genotypes as independent variables. The resultsshow a similar trend as observed in logistic regression model. We observed higher risk forearlyallograft rejection inrecipientswith IL8−251AAgenotype(HR=2.38,95%CI,1.23–4.64,P=0.010)(Table3).Kaplan–Meier survival analysiswasconducted toassess themeantimeofrejection-free graft survival between different genotype groups of patients. Results showthat patients with the IL8 −251 AA genotype had the shortest mean time to first rejectionepisode(23.58±2.58months)whileTTgenotypehadthe longest (30.02±1.19months)withlog rank P value of 0.022 (Fig. 2). The IFNG +874ANT polymorphism was not significantlyassociated with time to rejection (log rank PN0.05, data not shown).
4.3. Influence of IL8 −251TNA and IFNG +874ANT genotype combinations on allograftoutcome
Wefurther studied the influence of different genotype combinations of IL8−251TNAandIFNG+874ANTon allograft outcome. Five combinationsweremade on the basis of presence/absence of high producer (risk) allele of either polymorphism. The four combinations withthe presence of either one, two, three or four risk allele of IL8 (−251-A) or IFNG (+874-T)
were compared with the combination having homozygous low risk genotype at bothpolymorphism (IL8 −251 TT and IFNG +874 AA) as reference category. As expected, all thecombinations having at least one risk allele were associated with more than 2-foldsincreased risk in transplant patients as compared to controls (Table 4). However, thesecombinations were not significantly associated with allograft outcome when transplantpatients were categorized into rejecters and non-rejecters group (data not shown).
4.4. IL8−251TNA and IFNG+874ANT SNPs and immunosuppressant levels at 1 month posttransplant
We then examined the relationship between IL8 −251TNA and IFNG +874ANTpolymorphism and cyclosporine C2 level (cyclosporine level 2 h post morning dose)/tacrolimus C0 levels (tacrolimus levels just before the morning dose) at 1 month posttransplantation. The recipients categorized on the basis of genotypewere compared for themean immunosuppressant levels by Kruskal–Wallis U test. High producers of IFNG (TT)were associated with significantly higher mean cyclosporine and tacrolimus levels at1 month post transplantation (Kruskal–Wallis P=0.033 and 0.021 respectively) (Fig. 3).
5. Discussion
Cellular invasion and cytokine release are important steps in theinitiation of rejection. The migration of inflammatory cells into theparenchyma of transplanted kidneys is an important feature oftransplant rejection. When activated, these cells release a series ofcytokines that bear the messages for mediating the ensuinginflammatory reaction associated with rejection. The chemokine IL8has been implicated in the pathogenesis of acute rejection inconjunction with other chemokines such as RANTES and MCP-1 [17].Our results suggested variant genotype of IL8−251TNA to be associatedwith allograft rejection.
In the present study, we evaluated whether IL8 and IFNG genepolymorphismswere associatedwith allograft outcome in North Indianrenal transplant recipients. Our results showed that IL8 −251TNApolymorphism was significantly associated with risk of allograftrejection. The IL8 −251 AA genotype (high producer) was associatedwith 2.7 folds increased risk for allograft rejection as compared to TTgenotype (low producer) (OR=2.70, 95% CI, 1.09–6.69, P=0.032). Coxproportional and Kaplan–Meier survival analysis also suggested N2-folds increased risk and lower mean time to first rejection episode inpatientswith−251AAgenotype ascompared to−251TTgenotype (Logrank P=0.022) further confirming IL8−251 AA genotype to be a potentrisk factor in allograft rejection. Recent studies have shown that renaltubular and mesangial cells are able to produce IL8. Schmouder et al.opined that after renal transplantation, the expression of IL8 wasincreased in tubular cells, suggesting an important role for theseproteins in the ongoing allograft rejection [18]. Tilg et al. reportedincreased serum levels during graft rejection in liver transplant patients,further suggesting the participation of IL8 in allograft rejection [19].Although these studies suggest elevated IL8 serum levels duringallograft rejection no genetic studies till date describe the associationof IL8 gene polymorphism and susceptibility to allograft rejection inrenal transplant patients.
IFNG orchestrates the trafficking of specific immune cells to sites ofinflammation through up-regulating expression of adhesion moleculesand various chemokines [20]. In the present study, the IFNG +874ANTpolymorphism was not associated with allograft outcome in ourtransplant cohort. A recent study by Nikolova et al. also observedsimilar results showing no significant association of IFNG (+874ANT)between recipients with stable graft functioning and chronic allograftnephropathy [21]. On the contrary, Hoffmann et al. reported IFNG+874polymorphism to be associatedwith renal transplant rejection [22]. Theinconsistency observed in these studies may be due to the ethnicvariation of the study cohort.
Calcineurin inhibitors (cyclosporine and tacrolimus) have revolu-tionised the organ transplantation by selectively suppressing T cellactivation by blocking IL2 gene expression and thereby minimisingallograft rejection. However, the immunosuppressive activities ofthese drugs extend far beyond the sole IL2-mediated responsesinvolved in the immune response. Cyclosporine and tacrolimus have

17R. Singh et al. / Transplant Immunology 21 (2009) 13–17
been reported to inhibit the transcription of IL3, IL4, IFNG, TNFA orGM-CSF by activated T cells [23]. Therefore, in the present study, weattempted to correlate the influence of IL8 and IFNG genotypes onmean cyclosporine/tacrolimus levels at 1 month post transplantation.Though IFNG +874 TT recipients demonstrated higher levels ofcyclosporine and tacrolimus at 1 month as compared to AA and ATrecipients, but due to non-availability of sufficient data regardingtoxicity, the findings cannot be regarded as conclusive of immuno-suppressant toxicity. Therefore, further studies will be required tovalidate the results.
In the present study, we also compared different genotype combina-tions of IL8 −251TNA and IFNG +874 ANT polymorphism and observed2.5-folds increased risk in individuals carrying homozygous IL8 −251Aallele and one IFNG +874T allele in comparison to low producinggenotypes at both the polymorphisms.
It is well documented that cytokine gene polymorphism in humansplays an important role in graft rejection [24–26]. The high producerphenotype of IL8 and IFNG leading to increase in the pro-inflammatoryactivity in kidney graft recipients could thus be a key factor indetermination of early rejection.Wang et al. have shown cells to becomeresistant to CsA therapy and produce higher amount of TH-1 cytokineslike IL2, IFNG and IL12 [27]. Therefore, it can be predicted that theseindividuals would have different rejection patterns and thus variablesusceptibility to certain immunosuppressive drugs.
Further, in view of the interactions between graft cells and graft-infiltrating leukocytes, it is likely that donor-derived cytokines caninfluence recipient derived cells and influence susceptibility torejection. Therefore, in an extension to this study, donor cytokinegenotyping of IL-8will be performed which might further support thefindings as observed by different groups for other cytokines [28,29].
Based on the results from the present study, it can be concluded thathigh producer IL8−251AA genotype is associatedwith increased risk forallograft rejection and lowermean survival time tofirst rejection episode.In combination, the high producers of IL8 and IFNG posed an increasedrisk for allograft rejection. Thus, down regulation of IL8 and IFNGsynthesis resulting in reduced trafficking of leukocytes may proveimportant in preventing chronic inflammation and progressive tissuedestruction. Therefore, these polymorphisms may serve as a valuablemarker for characterization of group of patients at increased risk forallograft rejection.
To our knowledge, this is the first study reporting association of theIL8 −251TNA and IFNG +874ANT gene with transplant rejection risk in aNorth Indian renal transplant cohort. However, the numbers of cases andcontrols were relatively small in our study, so additional multicentricstudies with larger sample size and diverse ethnic populations will beneeded to validate the genetic effects of IL8 and IFNG gene polymorphismsand susceptibility to allograft rejection. Thus, further studies of IL8and IFNG gene sequence variants and their biologic functions aresuggested, whichmay help to identify those individualsmost susceptibleto transplant rejection. Hence, the present results in association withother supportive functional studies may allow immunosuppressiveregimens and cytokine mediated antibody therapy to be tailored tomeet the needs of patients at risk for allograft rejection after renaltransplantation.
Acknowledgements
RS is thankful to the Council of Scientific and Industrial Research,New Delhi for Senior Research Fellowship. Assistance of hospitaltransplant unit in blood collection and the relevant clinical informationof the patients is duly acknowledged. DKS is thankful to theDepartment of Biotechnology for Senior Research Fellowship. Theauthors are also thankful to Dr. Aneesh Srivastava for criticalsuggestions during the preparation of the manuscript.
References
[1] Milford EL. Chronic renal allograft loss. Curr Opin Nephrol Hypertens 1994;3:475–9.[2] Matsushima K, Oppenheim JJ. Interleukin 8 and MCAF: novel inflammatory
cytokines inducible by IL 1 and TNF. Cytokine 1989;1:2–13.[3] Matsushima K, Baldwin ET, Mukaida N. Interleukin-8 and MCAF: novel leukocyte
recruitment and activating cytokines. Chem Immunol 1992;51:236–65.[4] Stasikowska O, Wagrowska-Danilewicz M. Chemokines and chemokine receptors
in glomerulonephritis and renal allograft rejection. Med Sci Monit 2007;13:RA31–6.
[5] Fey MF, Tobler A. An interleukin-8 (IL-8) cDNA clone identifies a frequent HindIIIpolymorphism. Hum Genet 1993;91:298.
[6] Ross OA, O'Neill C, Rea IM, Lynch T, Gosal D, Wallace A, et al. Functional promoterregion polymorphism of the proinflammatory chemokine IL-8 gene associates withParkinson's disease in the Irish. Hum Immunol 2004;65:340–6.
[7] Hull J, Thomson A, Kwiatkowski D. Association of respiratory syncytial virusbronchiolitis with the interleukin 8 gene region in UK families. Thorax 2000;55:1023–7.
[8] Morinobu A, Kumagai S. Cytokine measurement at a single-cell level to analyzehuman Th1 and Th2 cells. Rinsho Byori 1998;46:908–14.
[9] Hancock WW, Sayegh MH, Kwok CA, Weiner HL, Carpenter CB. Oral, but notintravenous, alloantigen prevents accelerated allograft rejection by selectiveintragraft Th2 cell activation. Transplantation 1993;55:1112–8.
[10] Binder J, Hancock WW, Wasowska B, Gallon L, Watschinger B, Sayegh MH, et al.Donor-specific transplantation unresponsiveness in sensitized rats followingtreatment with a nondepleting anti-CD4 MAb is associated with selectiveintragraft sparing of Th2-like cells. Transplant Proc 1995;27:114–6.
[11] Amirzargar A, Lessanpezeshki M, Fathi A, Amirzargar M, Khosravi F, Ansaripour B,et al. TH1/TH2 cytokine analysis in Iranian renal transplant recipients. TransplantProc 2005;37:2985–7.
[12] Pravica V, Perrey C, Stevens A, Lee JH, Hutchinson IV. A single nucleotidepolymorphism in the first intron of the human IFN-gamma gene: absolute correlationwith a polymorphic CA microsatellite marker of high IFN-gamma production. HumImmunol 2000;61:863–6.
[13] López-Maderuelo D, Arnalich F, Serantes R, González A, Codoceo R, Madero R, et al.Interferon-gamma and interleukin-10 gene polymorphisms in pulmonary tuber-culosis. Am J Respir Crit Care Med 2003;167:970–5.
[14] Asderakis A, Sankaran D, Dyer P, Johnson RW, Pravica V, Sinnott PJ, et al.Association of polymorphisms in the human interferon-gamma and interleukin-10gene with acute and chronic kidney transplant outcome: the cytokine effect ontransplantation. Transplantation 2001;71:674–7.
[15] Hahn AB, Kasten-Jolly JC, Constantino DM, Graffunder E, Singh TP, Shen GK, et al.TNF-alpha, IL-6, IFN-gamma, and IL-10 gene expression polymorphisms and the IL-4receptor alpha-chain variant Q576R: effects on renal allograft outcome. Transplanta-tion 2001;72:660–5.
[16] Miller SA, Dykes DD, Polesky HF. A simple salting out procedure for extracting DNAfrom human nucleated cells. Nucleic Acids Res 1988;16:1215.
[17] Budde K, Waiser J, Ceska M, Katalinic A, Kürzdörfer M, Neumayer HH. Interleukin-8expression in patients after renal transplantation. Am J Kidney Dis 1997;29:871–80.
[18] Schmouder RL, Stricter RM, Wiggins RC, Chensue SW, Kunkel SL. In vitro and invivo interleukin-8 production in human renal cortical epithelia. Kidney Int1992;41:191–8.
[19] Tilg H, Ceska M, Vogel W, Herold M, Margreiter R, Huber C. Interleukin 8 serumconcentrations after liver transplantation. Transplantation 1992;53:800–3.
[20] SchröderM, Kroeger KM, Volk HD, Eidne KA, Grütz G. Preassociation of nonactivatedSTAT3 molecules demonstrated in living cells using bioluminescence resonanceenergy transfer: a new model of STAT activation? J Leukoc Biol 2004;75:792–7.
[21] Nikolova PN, Ivanova MI, Mihailova SM, Myhailova AP, Baltadjieva DN,Simeonov PL, et al. Cytokine gene polymorphism in kidney transplantation—impact of TGF-beta 1,TNF-alpha and IL-6 on graft outcome. Transpl Immunol2008;18:344–8.
[22] Hoffmann S, Park J, Jacobson LM, Muehrer RJ, Lorentzen D, Kleiner D, et al. Donorgenomics influence graft events: the effect of donor polymorphisms on acuterejection and chronic allograft nephropathy. Kidney Int 2004;66:1686–93.
[23] Quesniaux VF. Immunosuppressants: tools to investigate the physiological role ofcytokines. Bioessays 1993;15:731–9.
[24] Thakkinstian A, Dmitrienko S, Gerbase-DelimaM, McDaniel DO, Inigo P, Chow KM,et al. Association between cytokine gene polymorphisms and outcomes in renaltransplantation: a meta-analysis of individual patient data. Nephrol DialTransplant Apr 17 2008 [Electronic publication ahead of print].
[25] Manchanda PK, Bid HK, Kumar A, Mittal RD. Genetic association of interleukin-1beta and receptor antagonist (IL-1Ra) gene polymorphism with allograft functionin renal transplant patients. Transpl Immunol 2006;15:289–96.
[26] Pawlik A, Domanski L, Rozanski J, Florczak M, Dabrowska-Zamojcin E,Dutkiewicz G, et al. IL-2 and TNF-alpha promoter polymorphisms in patientswith acute kidney graft rejection. Transplant Proc 2005;37:2041–3.
[27] Wang H, Hosiawa KA, MinW, Yang J, Zhang X, Garcia B, et al. Cytokines regulate thepattern of rejection and susceptibility to cyclosporine therapy in different mouserecipient strains after cardiac allografting. J Immunol 2003;171:3823–36.
[28] Hoffmann S, Park J, Jacobson LM, Muehrer RJ, Lorentzen D, Kleiner D, et al. Donorgenomics influence graft events: the effect of donor polymorphisms on acuterejection and chronic allograft nephropathy. Kidney Int 2004;66:1686–93.
[29] Wong WK, Robertson H, Carroll HP, Ali S, Kirby JA. Tubulitis in renal allograftrejection: role of transforming growth factor-beta and interleukin-15 in develop-ment and maintenance of CD103+ intraepithelial T cells. Transplantation2003;75:505–14.