Embed Size (px)
Citation preview

Human Cancer Biology
Interleukin-7 Inhibits Tumor-Induced CD27�CD28� SuppressorT Cells: Implications for Cancer Immunotherapy
Yue Zhang3,4, Lukas W. Pfannenstiel2, Elzbieta Bolesta3, Carolina L. Montes4, Xiaoyu Zhang4,Andrei I. Chapoval4, Ronald B. Gartenhaus5, Scott E. Strome4, and Brian R. Gastman1,2
AbstractPurpose: We have previously reported that many types of tumors can induce changes in human T cells
that lead to the acquisition of suppressive function and phenotypic alterations resembling those found in
senescent T cells. In the present study, we find a role for interleukin 7 (IL-7) in protecting T cells from these
changes and further define involved signaling pathways.
Experimental Design: We evaluated the ability of IL-7 treatment to prevent the gain of suppressive
function andphenotypic alterations inhumanT cells after a short coculturewith tumor cells in vitro.We then
used inhibitors of components of the phosphoinositide 3-kinase (PI3K)/AKT pathway and short interfering
RNA knockdown of Mcl-1 and Bim to evaluate the role of these signaling pathways in IL-7 protection.
Results: We found that IL-7 inhibits CD27/CD28 loss and maintains proliferative capacity, IL-2
production, and reduced suppressive function. The protective ability of IL-7 depended on activation of
the PI3K/AKT pathway, which inhibited activation of glycogen synthase kinase 3b, which, in turn,
prevented the phosphorylation and loss of Mcl-1. We further showed a key role for Mcl-1 in that its
knockdown or inhibition abrogated the effects of IL-7. In addition, knockdown of the Mcl-1 binding
partner and proapoptotic protein Bim protected T cells from these dysfunctional alterations.
Conclusion: These observations confirm the role for Bcl-2 family members in cytokine signaling and
suggest that IL-7 treatment in combination with other immunotherapies could lead to new clinical
strategies to maintain normal T-cell function and reduce tumor-induced generation of dysfunctional and
suppressor T cells. Clin Cancer Res; 17(15); 4975–86. �2011 AACR.
Introduction
The immune response plays an important role in detect-ing and killing tumor cells, and the use of immunothera-pies to take advantage of this process has been a major goalof medical research. Despite some successes, obstacles suchas multiple processes of T-cell regulation and dysfunctionremain unresolved. Recent studies have identified signifi-cantly increased populations of T cells in human patientsthat display many characteristics of senescent T cells nor-mally associated with aging (1–3). Although the hallmark
of these cells is the loss of CD27 and CD28 expression, theyalso possess other features of senescence, including shor-tened telomeres (4) and reduced proliferative capacity andcytokine production (5), as well as suppressor activity notassociated with traditional senescence. These findings sug-gest that increased numbers of dysfunctional, senescent-like T cells directly support the local and systemic immu-nosuppression observed in cancer patients (3, 6). Indeed,increased numbers of these cells correlates with a poorprognosis and contributes to general immune hyporespon-siveness (7–9), making these patients poor candidates forimmunotherapy (2, 3, 10).
Working from the hypothesis that the tumors themselveswere capable of inducing these dysfunctional changes in Tcells, we have previously characterized an in vitro model inwhich normal human T cells were induced to becomedysfunctional suppressors after a brief interaction withtumor cell lines of multiple origins (1). This model mimicsa process in patients where normal T cells travel to thetumor microenvironment, are altered by tumor-generatedfactors, and then reenter the periphery where phenotypicalterations can be used to track them. We found that a briefcoincubation with tumor cells was sufficient to induce asignificant loss of CD27 and CD28 expression in bothCD4þ and CD8þ T cells as well as other senescence-related
Authors' Affiliations: 1Institutes of Head and Neck, Dermatology andPlastic Surgery, Taussig Cancer Center and 2Department of Immunology,Lerner Research Institute, Cleveland Clinic, Cleveland, Ohio; Departmentsof 3Surgery and 4Otorhinolaryngology, and the 5Marlene and StewartGreenebaum Cancer Center, University of Maryland School of Medicine,Baltimore, Maryland
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Y. Zhang and L.W. Pfannenstiel contributed equally to this work.
Corresponding Author: Brian R. Gastman, Cleveland Clinic, 9500 EuclidAve/NE60, NE6-303, Cleveland, OH 44195. Phone: 216-445-2103; Fax:216-444-9329; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-10-3328
�2011 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 4975
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

markers including telomere shortening, nuclear hetero-chromatization, and increased expression of p53, p21,and p16. Most significantly, we found that this processinvolved a soluble factor secreted by tumor cells (but notuntransformed fibroblasts) and that both CD4þ and CD8þ
populations gained a potent suppressive ability. These datasuggest that this process of tumor-induced suppressioncould be a mechanism by which tumors could not onlyblunt T-cell responses against them directly but alsoenhance systemic hyporesponsiveness by redirecting effec-tors to become regulatory.
Several recentstudies suggest thatcytoprotectivecytokinessuch as interleukin (IL)-7 and IL-12may prevent the induc-tion of altered T-cell function. For instance, IL-7 and IL-12can induce telomerase activity, a key enzyme inmaintainingtelomere length (11–13). IL-12 has been found to restoreCD28 expression in CD4þCD28null T cells sorted fromhuman peripheral blood mononuclear cells (PBMC; ref.13). Furthermore, in a recent clinical trial of cancer patients,exogenous IL-7 maintained CD27 expression in peripheralblood T cells (14). Therefore, we hypothesized that thiscytokine could have the capacity to prevent the dysfunc-tional alterations thatwe observed in tumor-exposed T cells.
Using our previously described in vitro model of tumor-induced T-cell dysfunction, we now show that IL-7 preventsthe development of both phenotypic alterations and sup-pressive function in tumor-exposed T cells. We furthershow that this protection relies on the phosphoinositide3-kinase (PI3K)/AKT signaling pathway. Once activated,AKT inhibits the more downstream molecule glycogensynthase kinase 3b (GSK3b), preventing it from phosphor-ylating the cell survival molecule Mcl-1. Finally, we showthat Mcl-1 plays a nonapoptotic role as a key downstreameffector of IL-7 signaling by preventing tumor-induceddysfunction of T cells through well-known prosurvivalpathways. These findings suggest that IL-7 is a potentadjuvant for preventing the development of tumor-inducedsuppressor T cells andmay assist in cancer treatment, eitheralone or in combination with other immunotherapies.
Materials and Methods
Cell culturePeripheral blood T cells from healthy donors were iso-
lated as described previously (1). CD45RAþ T cells wereenriched from purified donor T cells by positive magneticbead selection (Miltenyi). Human solid tumor cell linesMCF7, 624mel, and Tu167were cultured for 24 hours up toa 90% confluence. To induce suppressor T cells, purified,naive, human T cells were added to wells containing solidtumor cells at a ratio of 1:1 for 6 hours. T cells were thencollected, washed, and cultured for 7 days in a completemedium with or without each of recombinant humanIL-2 (rIL-2; 100 U/mL; NCI BRB Preclinical Repository),IL-7 (rIL-7; 20 ng/mL; BD Pharmingen), IL-12 (rIL-12;20 ng/mL; R&D Systems), and IL-15 (rhIL-15; 10 ng/mL;eBioscience).
The following inhibitors at the indicated concentrationswere used: 20 mmol/L LY294002 (Sigma); 0.5 mmol/L AKTinhibitor IV (Cal Biochem); 20 and 2 mmol/L GSK3binhibitor X; and 5 mmol/L rapamycin (Calbiochem);20 nmol/L TW37 was a gift from Shaomeng Wang (Uni-versity of Michigan, Ann Arbor, MI), and 10 mmol/LABT737 was provided by Abbott Laboratories.
Flow cytometryDysfunctional phenotypic markers were evaluated by
CD27/CD28 staining and telomere length as describedpreviously (1). CD3þCD27þCD28þ subsets were collectedby fluorescence-activated cell-sorting (FACS) sorting. Forthe intracellular Mcl-1 staining, cells were incubated withMcl-1 antibody or IgG control (Sigma) followed by fluor-escein isothiocyanate (FITC)-labeled secondary antibody(Jackson ImmunoResearch). For IL-2 staining, tumor-exposed cells with or without IL-7 were washed and sti-mulated with 1 mg/mL anti-CD3 monoclonal antibody(mAb) overnight; BD Golgi Stop (0.7 mL/mL) was addedfor 4 hours followed by intracellular staining with APC-anti-IL-2 and APC-anti-rabbit IgG (BD Pharmingen). ForCFSE staining, T cells were labeled with 2 mmol/L carboxy-fluorescein succinimidyl ester (CFSE;Molecular Probes) for8minutes at 37�C and thenwashed 3 times with 10%RPMI1640 at room temperature. A total of 2� 105 CFSE-labeledfresh responder cells were placed in 96-well plates withcoated anti-CD3 mAb (1 mg/mL; BD Pharmingen) andcocultured with tumor-exposed cells with or without IL-7 for 48 hours (T cell� IL-7:responder¼ 1:3). Apoptosis inresponder cells was assessed by staining FITC-AnnexinV and 7-aminoactinomysin D (7-AAD; BD Phamingen)per the manufacturer’s instructions. All samples were ana-lyzed on a BD LRSII flow cytometer with FACS Diva Soft-ware (BD Bioscience). PBMCs from head and neck cancerpatients were collected and frozen under an InstitutionalReview Board approved protocol at the University of Mary-land (Baltimore, MD). Informed consent was obtainedfrom all subjects. Expression of T-cell surface markerswas evaluated by staining with PerCP-anti-CD3 (BDBioscience), PEcy7-anti-CD4 (BD Bioscience), APC-eFluor
Translational Relevance
In this study, we provide compelling data that IL-7, acytoprotective cytokine, is also a potent inhibitor oftumor-induced suppressive activity and phenotypicalterations observed in human T cells. We further showthat protective activities of IL-7 require involvement ofthePI3K/AKTpathwayandshowthe importanceofMcl-1as a key regulator of these dysfunctional changes.Together these data provide new insights into the mole-cular action of IL-7. Perhaps of greater importance is theobservation that T-cell alterations similar to thosereported here are found in cancer patients and have beenshown to be associated with poor prognosis and candi-dacy for immunotherapy. IL-7 may now have a broaderappealasanadjuvanttoimmune-basedcancertreatment.
Zhang et al.
Clin Cancer Res; 17(15) August 1, 2011 Clinical Cancer Research4976
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

780-anti-CD8 (eBioscience), PE-anti-CD127 (BDBioscience), APC-anti-CD28 (BD Bioscience), and FITC-anti-CD27 (BD Bioscience).
Western blot analysis and coimmunoprecipitationWestern blot analysis was carried out as previously
described (1) by using the following antibodies: anti-AKT1, anti-phospho-AKT Ser473, and Thr308, anti-Mcl-1, anti-phospho-Mcl-1 (Ser159/Thr163), anti-GSK3b, anti-phospho-GSK3b (Ser9), anti-Bim, anti-STAT5, and anti-phospho-STAT5 (Cell Signaling Biotechnology). For coim-munoprecipitation, cell lysates were precleared with pro-tein G beads and incubated overnight at 4�C with 1 mg ofanti-Mcl-1 (Santa Cruz Biotechnology) or anti-Bim (AlexisBiochemicals). Immunoprecipitates were collected by add-ing 30 mL protein G agarose beads (Sigma Aldrich) andincubated for 1 hour at 4�C.
Proliferation suppression assayAutologous T cells (responder cells) were plated at a
density of 2 � 105 cells per well in a flat-bottomed 96-wellplate coated with 1 mg/mL of anti-CD3 mAb (BD Pharmin-gen). The next day, tumor-exposed T cells with or withoutIL-7 were washed and added to the cultures of respondercells for an additional 72 hours, 1 mCi (0.037MBq) per well[3H]thymidine was pulsed overnight, and incorporationwas measured with a scintillation counter.
RNAi transfectionThe short interfering RNAs (siRNA) for Mcl-1, Bim, and
nontargeting were purchased from Dharmacon and SantaCruz Biotechnology. Purified primary T cells were trans-fected using the Amaxa Nucleofector Kit (Amaxa Biosys-tem) and analyzed 36 hours after transfection.
Statistical analysisStudent’s t test was used to evaluate the significance of
differences between sample means. Statistical significancewas defined at P < 0.05. All experiments were repeated atleast 3 times, with error bars representing the SD.
Results
IL-7 protects human T lymphocytes from tumor-induced T-cell suppressionWe have previously reported that tumor cells can directly
induce suppressor T cells in vitro, which could be amechan-ism that contributes to the ability of a tumor to evadeimmune recognition and killing (1). The cytokines IL-2, IL-7, or IL-12, which are known for their cytoprotective effectson T cells and are currently in clinical trials, were used todetermine whether they can prevent these phenotypic andfunctional alterations. Initially, we treated human periph-eral blood T cells with IL-2, IL-7, or IL-12 before andconcomitantly with different tumor cell lines, which werechosen on the basis of our previous study (1). T cells werethen recovered from coculture, washed, and plated incomplete media in the presence or absence of cytokines
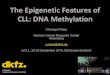
for 7 days. Dysfunctional suppressor T cells were identifiedby the loss of CD27 and CD28 or telomere shortening.Prior research had found that tumor-exposed T cellsundergo a 40% to 60% greater decrease in CD27 andCD28 expression than control T cells not exposed to tumor(1). The new findings show that IL-7 treatment (and to alesser degree IL-2 but not IL-12) consistently protectstumor-exposed T cells from CD27/CD28 loss (Fig. 1A
B60
40
RPMI
IL-2
IL-7
IL-12
IL-12IL-7IL-2RPMIA
14.9%2.2%4.8%12.1%
T cell
+ Tumor
CD
27
57% 17.4% 3.6% 36.7%
CD28
0
20
CD
27/C
D28 lo
ss%
T cell 624melMCF7Tu167
C
6
8
10
12
*
NS
0
2
4
IL-12IL-7IL-2RPMIIL-12IL-7IL-2RPMIRPMI
Telo
mere
len
gth
(kb
)
T cell (day 0) T cell (day 7) +TUMOR (day 7)
Figure 1. IL-7 prevents tumor-induced T-cell CD27/28 loss and telomereshortening induced by both hematopoietic and solid tumors in vitro.Purified T cells were incubated with various tumor cell lines (Tu167, MCF7,and 624mel) at a ratio of 1:1 for 6 hours and then washed and cultured foranother 7 days with or without cytokines (100 U/mL IL-2, 20 ng/mL IL-7,and IL-12). On day 7, T-cell controls and tumor-exposed cells wereevaluated for the loss of CD27 and CD28. A, representative dot plotsdepicting CD27�CD28� T cells induced by Tu167 are shown. B, tumor-exposed T cells incubated with different tumor cells (from at least 3independent experiments) in the presence or absence of differentcytokines are shown; error bars represent SD. C, analysis of telomerelength with freshly isolated T cells, T cells on day 7, and tumor-exposed Tcells on day 7 (with or without IL-2, IL- 7, or IL-12). The bar chart shows theSEM relative telomere length in cells from 3 independent experiments.*, P ¼ 0.027 versus control tumor–exposed cells. NS, no statisticalsignificance between IL-7–treated, tumor-exposed cells, and untreatedT cells alone.
IL-7 Inhibits Tumor-Induced Human Suppressor T cells
www.aacrjournals.org Clin Cancer Res; 17(15) August 1, 2011 4977
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

and B). However, only IL-7–treated, tumor-exposed T cellsmaintained a telomere length comparable with unexposedcontrols (Fig. 1C). We then established that the best timefor IL-7 treatment is immediately after coincubation withtumor (Supplementary Fig. S1), and for this reason, allsubsequent experiments used this time point. We alsodetermined that the combination of IL-7 with other com-mon receptor g-chain cytokines IL-2 and IL-15 did notresult in any additive effect over IL-7 alone (SupplementaryFig. S2). To test whether IL-7 treatment could equallybenefit naive versus memory T cells, naive CD45RAþ Tcells were enriched with purified T cells by positive mag-netic bead selection before both CD45RA-enriched and-depleted T cells were incubated with tumor and cultured inIL-7 (Supplementary Fig. S3). We found that the degree ofCD27/CD28 loss was greater in naive CD45RAþ T cellsthan in CD45ROþ memory T cells but that IL-7 treatmentwas protective in both. These results suggest that naive
T-cell populations may be more susceptible to tumor-induced alterations.
Our data also show that IL-7 alone promoted T-cellsurvival (Supplementary Fig. S4A) and did not induce pro-liferation of tumor-exposed T cells (Fig. 2A) or T cells alone(data not shown). These findings suggest that IL-7 protectsagainst T-cell dysfunction by inhibiting its developmentrather than causing the proliferation of nondysfunctionalT cells. To address whether IL-7 treatment can reverse thedysfunctional phenotype, we evaluated tumor-exposedT cells (untreated) 7 days after coincubation and addedIL-7. CD27/CD28 expression was checked at several timepoints after the introduction of IL-7, but only minorincreases in expression of both markers was observed (datanot shown). To determine whether loss of the IL-7 receptor(IL-7R) could account for this finding, we examined theexpression of this receptor (CD127) on tumor-exposedT cells. We observed that the loss of CD27 and CD28
BADay 7Day 4Day 1
+ Tumor
Isotype control
+ Tumor
+ Tumor + IL-7
Anti-CD3
Anti-CD3+IL-7
IL-2
Untreated
IL-7
250,000
80
60
40
20
0
60
50
40
30
20
10
0
200,000
150,000
100,000
50,000
R Tumor Tumor+ IL-7
R Tumor Tumor+ IL-7
Tumor Tumor+ IL-7
0
Tht
mis
inw
upt
ake
(cpm
)
% o
f sup
pres
sion
% A
nnex
in V
17-A
AD
-pos
itive
cel
ls
CFSE
DC
Figure 2. IL-7 enhances the proliferation of CD3-activated, tumor-exposed T cells and restores proliferation of responder cells in coculture with tumor-exposed cells. A, T cells were stained with 2 mmol/L CFSE and then cocultured with Tu167 at a ratio of 1:1 for 6 hours, washed, and cultured in anti-CD3mAb–coated plates with or without IL-7 (20 ng/mL). Cell proliferation was examined by flow cytometry on days 1, 4, and 7. Tumor-exposed T cellscultured without anti-CD3 in medium alone (untreated) with IL-7 served as negative controls. B, tumor-exposed cells cultured with or without IL-7 for 7 dayswere washed and stimulated with anti-CD3 mAb for 24 hours and then IL-2 expression was detected by intracellular cytokine staining and FACS. C, tumor-exposed T cells were incubated with or without IL-7 for 7 days and then washed and placed into the cultures of normal donor responder cells prestimulated for24 hours with anti-CD3 antibody at tumor-exposed cell:responder cell ratio of 1:3. Responder T-cell proliferation was evaluated by [3H]thymidine incorporationafter 72 hours and represented as the mean � SD of cpm from 3 independent experiments (left). The percentage of proliferation inhibition of responder T cellsby tumor-exposed T cells and IL-7–treated, tumor-exposed T ells was calculated from 3 independent experiments (*, P¼ 0.027). Each bar represents mean�SD of triplicate values. D, tumor-exposed T cells cultured 7 days with or without IL-7 were added to CFSE-labeled responder cells at a ratio of 1:3 andstimulated with anti-CD3 mAb for 48 hours. Apoptosis of the CFSE-labeled responder cells was evaluated by Annexin V and 7-AAD staining. The bar graphshows the percentage of double-positive staining cells from 3 independent experiments. Error bars represent the SD. R, responder cells.
Zhang et al.
Clin Cancer Res; 17(15) August 1, 2011 Clinical Cancer Research4978
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

correlated with significantly lower CD127 expression (Sup-plementary Fig. S5). To testwhether the observed decrease inCD127 expression after tumor exposure has clinical rele-vance, we obtained peripheral blood from human head andneck cancer patients collected under an Institutional ReviewBoard–approved protocol before chemotherapy treatmentand examined CD127 expression on CD27�/CD28� T cellsamong the total CD8þ population as compared withhealthy, age-matched donor controls. We chose to focuson the CD8þ T-cell population, as these cells display greaterlevelsofCD27/CD28 loss in vivo thanCD4þ cells (9). Similarto our in vitro observations, the CD27/CD28 double-nega-tive CD8þ T-cell population in these patients had very lowCD127 expression (Supplementary Fig. S6). These resultssuggest that the benefit of IL-7 therapy would be the protec-tion of CD127þ T cells from tumor-induced dysfunctionrather than the reversal of already dysfunctional cells due totheir lack of CD127 expression. Overall, our results showthat IL-7 protects against tumor-induced phenotypic altera-tions, but that once T cells lose CD27 and CD28 expression,further IL-7 exposure is unlikely to have any effect.
IL-7 prevents the functional changes associated withtumor-induced dysfunctionIn addition to the loss of CD27 and CD28 expression, we
have also found that tumor-exposed T cells are hypopro-liferative when stimulated with anti-CD3. To evaluatewhether IL-7 treatment could affect this aspect of tumor-induced dysfunction, we evaluated the proliferative capa-city of tumor-exposed T cells after 7 days in vitro culturewith or without IL-7. Using CFSE-labeling and plate-boundanti-CD3 antibody, we observed an increase in the pro-liferation of tumor-exposed, IL-7–treated cells, but not intumor-exposed T cells stimulated with anti-CD3 Ab or IL-7alone (Fig. 2A).To further validate this observation, we repeated the
experiment using [3H]thymidine incorporation as a read-out for proliferation. Initially, we did not observe prolif-eration in any of the treatment groups (data not shown).Because IL-7–treated T cells contain small numbers ofCD27/CD28 double-negative T cells, we hypothesized thatthe lack of proliferation could be due to suppression bythese cells. To evaluate this possibility, CD27þCD28þ Tcells were electronically sorted from IL-7–treated oruntreated groups 7 days after tumor exposure and stimu-lated with plate-bound anti-CD3 antibody for 72 hours(Supplementary Fig. S2B). Interestingly, we observed thatCD27þCD28þ T cells not receiving IL-7 treatment werehypoproliferative. This observation could be due to the factthat tumor-induced dysfunction is a process and that theloss of proliferative capacity precedes the loss of CD27 andCD28 expression. Tumor-exposed CD27/CD28 double-positive cells treated with IL-7 displayed proliferationsimilar to control T lymphocytes not exposed to tumor.As expected, the CD27�CD28� population from bothuntreated and IL-7–treated, tumor-exposed T cells didnot proliferate (data not shown). These observations indi-cate that IL-7 prevents tumor-induced dysfunction in
most, but not all, T cells and IL-7–treated CD27þCD28þ
T cells have normal proliferative capacity.Another distinguishing characteristic of both senescent
and dysfunctional T-cell populations in cancer patients andthose generated by our tumor-exposure model is reducedproduction of IL-2 upon stimulation (15). We discoveredIL-7 treatment can significantly increase IL-2 production intumor-exposed T cells after anti-CD3 stimulation (Fig. 2B)
Perhaps the most significant functional alteration oftumor-exposed T cells is their ability to suppress the pro-liferation of normal T lymphocytes in response to anti-CD3and mixed lymphocyte reaction stimulation in vitro (1).Thus, we examined whether IL-7 treatment could reduce orprevent this suppression. Fresh allogenic T lymphocytes(responder cells) were pretreated with plate-bound anti-CD3 Ab for 24 hours. Tumor-exposed T cells cultured withor without IL-7 were then added to the responder cells at aratio of 1:3. We observed that IL-7–treated cells had lesssuppressive function than their untreated counterparts(Fig. 2C). We then evaluated whether tumor-exposed, T-cell–mediated suppression occurs through induction ofapoptosis in responder T cells by labeling them with CFSEprior to coincubation. After 2 days, responder cell apop-tosis was measured by 7-AAD and Annexin V staining. The20% baseline level of apoptosis was expected because anti-CD3 stimulation induces proliferation and activation-induced cell death. In the presence of tumor-exposed Tcells, however, apoptosis in responder T lymphocytesnearly doubles, whereas coincubation with IL-7–treated,tumor-exposed cells did not significantly increase respon-der apoptosis (Fig. 2D). Taken together, these results showthat IL-7 inhibits the functional alterations seen in tumor-induced dysfunctional T cells.
PI3K/AKT is required for IL-7 protection againsttumor-induced T-cell dysfunction
To better understand the effects IL-7 treatment has onprotecting T cells from tumor-induced dysfunction, we nextinvestigated the role of several pathways known to beinvolved in IL-7 signaling, namely, JNK/STAT5 andPI3K/AKT (16). We found that though inhibition of STAT5(17) could block its phosphorylation during IL-7 treatment,the blockade had little effect on the protective ability ofIL-7 (Supplementary Fig. S7). We next evaluated the PI3K/AKT pathway, which has been shown to be involved inmediating IL-7–driven T-cell survival (16, 18). AKT is akey downstream target of PI3K and is activated by dualphosphorylation at Thr308 and Ser473. As shown in Figure3A and B, IL-7 cannot protect T cells from tumor-inducedCD27/CD28 loss when cultured with PI3K (LY294002) orAKT inhibitors (AKT inhibitor IV). We then analyzedwhether AKT is activated by IL-7 in tumor-exposed cells.As shown inFigure3C, IL-7 can induceAKTphosphorylationat Ser473 and Thr308 within 30 minutes, with phosphory-lation increasing for at least 12 hours. The PI3K and AKTinhibitors, as expected,blocked IL-7–inducedAKTactivationin tumor-exposed cells. Similar results occurredwithanotherinhibitor of PI3K, wortmannin (data not shown).
IL-7 Inhibits Tumor-Induced Human Suppressor T cells
www.aacrjournals.org Clin Cancer Res; 17(15) August 1, 2011 4979
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

IL-7 prevents tumor-induced T-cell dysfunctionthrough inhibition of GSK3b
We next evaluated downstream cell survival moleculesrelated to the PI3K/AKT pathway by examining the effectormolecular complex, mTOR (19, 20). Using the mTORinhibitor rapamycin, we did not observe any reductionin the protective function of IL-7 (Supplementary Fig. S8),suggesting that mTOR is dispensable for IL-7 effects. Wenext studied GSK3b, one of the downstream substrates ofPI3K/AKT, which is inactivated by direct phosphorylationon the Ser9 residue, promoting cytokine-driven cell survi-val (21). These previous reports suggested that GSK3bmight effect IL-7–mediated protection through PI3K/AKTpathway activation. We observed that the development oftumor-induced CD27/CD28 loss was prevented by theGSK3b inhibitor X (20 mmol/L) even without IL-7(Fig. 4A and B). We also tested the GSK3b inhibitor at alower dose (2 mmol/L) and observed less protection. With alower GSK3b inhibitor dose, IL-7 could prevent CD27/CD28 loss (data not shown). We also observed that IL-7causes a time-dependent increase in phosphorylation ofGSK3b, which suggests that this process is part of itsprotective signaling (Fig. 4C).
IL-7 upregulates Mcl-1 expression bydephosphorylation in tumor-exposed T cells
Studies indicate that Mcl-1 levels are highly regulated byGSK3b phosphorylation at Ser159 in cytokine-deprivedcells, which causes Mcl-1 degradation (22). We observed
via Western blot analysis that Mcl-1 phosphorylationoccurs in tumor-exposed cells (tumor 0 hour; Fig. 5A).IL-7 addition reduced Mcl-1 phosphorylation and upregu-lated total Mcl-1 in a time-dependent manner. Both PI3Kand AKT inhibitors can prevent IL-7–inducedMcl-1 depho-sphorylation, whereas GSK3b inhibitor with IL-7 preventedalmost completely Mcl-1 phosphorylation (Fig. 5A). Tofurther evaluate Mcl-1 expression, we used FACS analysis oftumor-exposed T cells in a 3-period time course over 1week. Our data show that fluorescence intensity of Mcl-1increased and was maintained throughout this course aftera single IL-7 administration. As control, we investigatedMcl-1 levels in tumor-exposed cells treatedwith IL-2 and IL-12 (Fig. 5B), concluding that IL-7 had the greatest impacton Mcl-1 expression. These experiments show that IL-7increases Mcl-1 levels by inhibiting its phosphorylationinduced by GSK3b, further elucidating the role of IL-7 inprotecting T cells from tumor-induced dysfunction.
Depletion of Mcl-1 abrogates IL-7 protection againsttumor-induced dysfunction
To determine whetherMcl-1 plays a role inmediating theprotective activity of IL-7, we reduced Mcl-1 levels throughsiRNA-mediated knockdown and examined the resultinginfluence on cell survival. T cells were transfected with Mcl-1 siRNA or a control siRNA. Transfection with Mcl-1–specific siRNA produced a profoundly decreased Mcl-1expression that IL-7 did not upregulate. Importantly, pro-tective activity of IL-7 was significantly abrogated in T cells
ATumor + AKT INHTumor + LY + IL-7Tumor + LYTumor + IL-7Tumor Tumor + AKT INH + IL-7
CD
27
64.7%74.4%80%19.2%55.1% 62.8%CD28
B C
Tumor+IL-7
0 0.5 h 1 h 12 h LY (12 h) AKTinh (12 h)T
AKT-T308
AKT-S473
AKT
Tumor Tumor LY
% l
os
s o
f e
xp
res
sio
no
f C
D2
7/2
8
TumorAKT inh
70
60
50
40
30
20
10
0
RPMI
IL07 (20 ng/mL)
Figure 3. IL-7–mediated protection from tumor-induced phenotypic alterations depends on PI3K and AKT. A and B, tumor-exposed T cells werecultured with or without IL-7 and with LY294002 (LY) or AKT inhibitor IV (AKT INH). On day 7, cells were stained with CD27 and CD28 antibodies. Onerepresentative of 3 experiments is shown (A) and data from 3 independent experiments are shown (B), with each bar representing mean � SD of triplicatevalues. C, T cells alone or tumor-exposed T cells treated with IL-7 or together with LY294002 (LY) or AKT inhibitor IV (AKT INH) were cultured for theindicated periods. Cell lysates were resolved with 10% SDS-PAGE and immunoblotted with indicated antibodies. Total AKT was used as a loading control.T, control T cells.
Zhang et al.
Clin Cancer Res; 17(15) August 1, 2011 Clinical Cancer Research4980
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

with reduced Mcl-1 levels. IL-7 still had a small effect inMcl-1 knockdown of T cells; however, this may be due tothe fact that the siRNA transfection is not absolute. Tofurther verify the lack of off-target effects, we used a distinctMcl-1 siRNA from another company and obtained similarexpression and functional results (Supplementary Fig. S9).Notably, downregulation of Mcl-l in T cells can inducemoderate losses of CD27/CD28 compared with controls(Fig. 5C). To confirm the specific role of Mcl-1 in IL-7–mediated protection, we introduced 2 pharmacologicdrugs, TW37 (a nonpeptide pan small-molecule inhibitorof Bcl-2, Mcl-1, and Bcl-xL) and ABT737 (a small-moleculeBH3 mimetic that binds to and antagonizes Bcl-2/Bcl-xL).Figure 5D illustrates that IL-7 can reduce CD27/CD28loss with ABT737 but not with TW37 treatment. Collec-tively, these results indicate the involvement of Mc1-1 inIL-7–mediated protection from tumor-induced T-celldysfunction.
The importance of the Mcl-1 binding partner Bim inIL-7 protectionAfter examining the role of Mcl-1 in IL-7–mediated
protection from tumor-induced T-cell dysfunction, weexplored its well-known binding partner Bim, whose inhi-bition is essential in IL-7–mediated lymphocyte survival(23–25). To assess the role of Bim in IL-7–mediated signal-
ing, we acutely knocked down its expression by usingsiRNA (from 2 different sources) in tumor-exposed cellswith and without IL-7 (Fig. 6A and SupplementaryFig. S9B). Bim loss abrogated tumor-induced CD27/CD28 loss, and IL-7 addition could not provide furtherprotection (Fig. 6A). Finally, to assess whether the functionof IL-7 was dependent on binding of Mcl-1 with Bim, wecarried out immunoprecipitation (IP) experiments forthese proteins. Interestingly, when we carried out IP forMcl-1, almost all Bim was pulled down in tumor-exposed Tcells whether or not IL-7 was administered. In contrast,after the IP for Bim, the level of free Mcl-1 was significantlyincreased by IL-7 in tumor-exposed cells (Fig. 6B and C).These data suggest that IL-7–driven Mcl-1 expression pre-vents tumor-induced T-cell dysfunction and that the levelof free (unbound to Bim) Mcl-1 is key to this process.
Discussion
The link between senescence and tumor-induced T-cellsuppression has yet to be completely understood. Manystudies have found elevated levels of T cells bearing thecharacteristics of replicative senescence normally asso-ciated with aged individuals in peripheral blood andtumor-infiltrating lymphocytes of cancer patients (3, 9).Other studies have focused on phenotypically similar
Tumor + GSK3 INHTumor + IL-7Tumor Tumor + GSK3 INH + IL-7A
CD
27
45% 3%4%21%CD28
B C
T cellsIL-7+
LY294002IL-7+
AKT Inh
T cells + tumor + IL-7
T cells1 min 30 min 60 min alone 12 h12 h 12 h+ tumor
GSK3ββ-Ser-9
GSK3β
β-Actin
Tumor Tumor+GSK3 inh
% l
os
s o
f e
xp
res
sio
no
f C
D2
7/2
8
80
70
60
50
40
30
20
10
0
RPMI
IL-7
Figure 4. Inactivation of GSK3b protects against CD27/CD28 loss. A and B, tumor-exposed T cells were cultured with medium, IL-7, GSK3b inhibitorX (GSK INH), or IL-7þGSK3b inhibitor X (GSK INHþ IL-7) for 7 days before staining for CD27/CD28 expression. One representative of 3 experiments is shown(A) and data from 3 independent experiments are shown (B), with each bar representing mean � SD of triplicate values. C, T cells alone or tumor-exposedT cells cultured with IL-7 and LY294002 (LY) or AKT inhibitor IV (AKT INH) were harvested at the indicated time points. GSK3b phosphorylation was detectedby immunoblotting with anti-phospho-GSK3b (Ser9) antibody. Blots were reprobed with an anti-GSK3b and anti-b-actin antibodies.
IL-7 Inhibits Tumor-Induced Human Suppressor T cells
www.aacrjournals.org Clin Cancer Res; 17(15) August 1, 2011 4981
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

populations that exhibit suppressor function (3). Ourprevious data suggest that the answer may be more com-plex. Specifically, we observe in appropriate coincubationconditions that tumor cells can induce senescent-likechanges in T cells, with strongly associated gain of sup-pressor function, in the absence of activation and prolif-eration (1). Interaction with tumors has been shown toinduce a large array of changes in T cells in addition to thesenescent-like dysfunctional changes reported here, includ-ing the induction of preapoptotic features such as the loss
of z chain and CCR7 expression (26). Our previous workhas found that the T-cell alterations we observe are aprocess distinct from tumor-induced apoptosis, thoughwe report here that the protection conferred by IL-7 treat-ment involves several signaling pathways known to beantiapoptotic. Thus, the signaling relationship betweentumor-induced apoptosis and dysfunction remains to becompletely resolved.
The presence of tumor-induced dysfunctional T-cellpopulations in cancer patients is associated with systemic
54 8% 87 9% 71 9%
BA
Tumor + IL-7 Tumor + IL-7 (12 h)
MFI = 8,135 MFI = 33,075 MFI = 8,556
Tumor
Day2 Day4 Day7
T Tumor Tumor AKT GSK0 h 0 h 0.5 h 1 h 12 h 12 h LY Inh Inh
p-Mcl-1
Mcl-1
β-
MFI = 18,276 MFI = 43,143 MFI = 17,175
Tumor + IL-2
βMFI = 27,891
MFI = 15,319
MFI = 53,363
MFI = 24,383
MFI = 20,272
MFI = 11,868
Tumor + IL-7
TllT
Mcl-1
Tumor + IL-12
D
Cctrl RNAi ctrl RNAi ctrl RNAi
CD
27
T cell Tumor Tumor + IL-7
D
11%
RPMI
RPMI
IL-7
IL-7
37.5% 75.8% 30.4%
Mcl-1 RNAi Mcl-1 RNAiMcl-1 RNAi
65%
Tumor Tumor+ TW37 Tumor Tumor
+ ABT737
72%73%
Medium IL-7 Medium IL-7
CD28. . .
Mcl-1 RNAictrl RNAi
Mcl-1
β-Actin
% L
oss o
f exp
ressio
n o
f C
D27/C
D28
% L
oss o
f exp
ressio
n o
f C
D27/C
D28
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0
Actin
Figure 5. Mcl-1 is upregulated and dephosphorylated at Ser159/Thr163 by IL-7 in tumor-exposed T cells. A, T cells or tumor-exposed T cells harvestedimmediately (0 hour) and 12 hours after coincubation with Tu167 tumor cells were harvested. Tumor-exposed T cells þ IL-7 were harvested 0.5, 2, or12 hours after coincubation with tumor. Tumor-exposed T cells þ IL-7 and LY294002 (LY), AKT inhibitor IV (AKT INH), or GSK3b inhibitor X (GSK INH) for12 hours were harvested. Total Mcl-1, pSer159/Thr163-Mcl-1, and b-actin (loading control) in all samples were analyzed by Western blotting. B, T cells werecoincubated with Tu167 tumor cells, washed, and cultured in media with or without a single dose of IL-2 (100 U/mL), IL-7 (20 ng/mL), or IL-12 (20 ng/mL).The expression of Mcl-1 was assessed by flow cytometry on days 2, 4, and 7; the mean fluorescence intensity (MFI) of Mcl-1 is shown. C, control (ctrl)and Mcl-1 siRNA–transfected T cells were cultured for 36 hours, coincubated with Tu167 for 6 hours at a ratio of 1:1, and then cultured with or without IL-7.Mcl-1 expression was examined by Western blotting (bottom). On day 5, we evaluated loss of CD27 and CD28 by flow cytometry. Representative dataare shown (top). D, TW37 but not ABT737 abrogates IL-7 protection. Tumor-exposed T cells with or without IL-7 and with and without TW37 or ABT737were cultured for 7 days before staining for loss of CD27 and CD28 expression. Data from 3 independent experiments are shown (D), with each barrepresenting mean � SD of triplicate values. T, control T cells.
Zhang et al.
Clin Cancer Res; 17(15) August 1, 2011 Clinical Cancer Research4982
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

immunosuppression and poor prognosis. Therefore, reg-ulating their formation could improve clinical outcomes(8, 27). Although cytokines are an attractive option forimmunomodulation, little is understood about their effectson natural and induced suppressor cell populations. Forinstance, some cytoprotective cytokines, such as IL-15,induce immunosuppressive cellular responses includingincreases in senescence-associated markers on T cells(28, 29). Our in vitro model, in which tumor cells caninduce similar changes in normal donor T cells, provides aplatform to identify cytokines that regulate formation ofdysfunctional T cells and dissect the molecular pathwaysresponsible for these effects. Using this model, we observedthat IL-7 is a potent inhibitor of tumor-induced dysfunc-tional T-cell phenotypic and functional changes. Further-more, we show that IL-7 exerted its protective functionthrough commonmolecular pathways involved in prevent-ing apoptosis.We initially began with 3 cytokines currently used in
clinical trials, namely, IL-2, IL-7, and IL-12. IL-2 and IL-7share the same g-chain receptor but seem to have disparateeffects on the immune system (30). For instance, whereas
both IL-2 and IL-7 promote T-cell survival, IL-2 also causesexpansion of natural regulatory T cells. IL-12, a non–g-chain cytokine, not only promotes antitumor immunitybut has also been shown to increase CD28 expression inCD28null T cells (13, 31). We found a striking differencebetween these cytokines in that only IL-7 consistentlyprotects against tumor-induced T-cell phenotypic and func-tional changes and that combination with other IL-2 familycytokines (IL-2 and IL-15) does not produce an additiveeffect over IL-7 alone. This observation is notable in thatboth IL-2 and IL-15 have been shown to enhance thesurvival of effector and memory T-cell populations similarto IL-7 (30). Several phase I clinical trials have beenconduced with IL-7 in the context of cancer (14, 32, 33)and HIV infection (34, 35). In total, these trials show thatIL-7 can be well tolerated by patients with minimal toxi-cities and it induces the expansion of naive and memoryCD4þ and CD8þ T-cell populations. However, overallantitumor efficacy was nominal whether used alone orin combination with vaccine. Our data showing that induc-tion of a suppressive, dysfunctional phenotype is accom-panied by the loss of IL-7R suggests that the timing of
A ctrl RNAi Tumor
ctrl RNAi Tumor + IL-7
Bim RNAi Tumor
Bim RNAi Tumor + IL-7
CD2838.9%40.3%32.9%75.1%
CD
27
Bim RNAictrl RNAi
Medium
Bim
β-Actin
Medium IL-7 IL-7
CB
Input Depleted IP Input Depleted IP
IP-Mcl-1
Tumor + IL-7Tumor
IP-Bim
Tumor + IL-7Tumor
Input Depleted IP Input Depleted IP
Mcl-1
Bim
Mcl-1
Bim
sup pellet sup pellet sup pellet sup pellet
β-Actin β-Actin
Figure 6. Free Mcl-1 is important for IL-7 protection and is upregulated by IL-7 treatment. A, T cells were transfected with either control (ctrl) siRNA orBim siRNA for 36 hours, coincubated with Tu167 for 6 hours at a ratio of 1:1, and cultured in fresh medium with or without IL-7 for 5 days. The loss of CD27/CD28 was determined by FACS (top). Bim expression was examined by Western blotting (bottom). One representative of 3 experiments is shown. B and C,tumor-exposed T cells with and without IL-7 were lysed in IP buffer and immunoprecipitated with anti-Mcl-1 and Bim antibody. The immunoprecipitatedproteins, total extracts, and depleted supernatant (sup) were analyzed by SDS-PAGE and immunoblotted with indicated antibodies.
IL-7 Inhibits Tumor-Induced Human Suppressor T cells
www.aacrjournals.org Clin Cancer Res; 17(15) August 1, 2011 4983
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

administration would be important not only in the deple-tion of existing dysfunctional suppressors but also in pro-tecting subsequent waves of effector T cells induced eitherendogenously by vaccine or injected via adoptive transfer.Indeed, preclinical mouse models have indicated that IL-7can successfully be combined with a vaccine to significantlyboost antitumor immunity (36).
IL-7 is known to activate cell survival signaling pathways,including the JAK/STAT and the PI3K/AKT pathways (37).However, these pathways may work in concert or bemutually exclusive (38). In addition, consequences of IL-7 signaling can differ depending on the T-cell lineage. Wehypothesized that the protective effects of IL-7 may bemediated through these known cytoprotective pathwaysand identified only the PI3K/AKT pathway as significant.Our data show that PI3K and AKT are required for IL-7–mediated protection from dysfunctional changes and, indoing so, causes phosphorylation of AKT at both possiblesites, indicating full activation of this molecule. Finally, ourfindings show that telomere length is maintained with IL-7administration, which is consistent with the reported abil-ity of AKT to activate telomerase (39).
A number of recent studies have shown that in cancer,constitutive AKT expression promotes cellular senescence(40). Others have shown, however, that AKT can promoteproliferation through inhibition of RAF (41). This discre-pancy may be a cell-type–dependent phenomenon and, atleast in mouse and human T cells, AKT seems to maintainnormal function. Thus, our data implicating the PI3K/AKTpathway may represent changes in lymphocytes only, ormay be related to its function in combination with other IL-7–induced pathways. Ultimately, these findings describe anovel IL-7–mediated T-cell–protective pathway dependenton PI3K and AKT.
The AKT molecule has many downstream targets. Twoof the most studied are the mTOR complex and GSK3b,which are both involved in promoting T-cell proliferation(42, 43). We observe that inhibition of mTOR usingrapamycin did not affect protective activities of IL-7. Thisobservation is interesting because it has been recentlyreported that AKT induces cellular senescence throughmTOR and may also explain why AKT in IL-7 signaling isantisenescent (44). As a result, we then tested the impor-tance of GSK3b. Our data show that chemical inhibitionof GSK3b was sufficient to almost completely inhibittumor-induced phenotypic alterations in T cells evenwithout IL-7. We further show that IL-7 causes the phos-phorylation and inhibition of GSK3b. Overall, our dataillustrate that during IL-7 signaling, AKT is activated,which then prevents GSK3b signaling and leads toreduced CD27/CD28 loss.
One of the main targets of phosphorylation by GSK3b isthe antiapoptotic Bcl-2 family member Mcl-1 (22).Although there is significant data regarding the role ofMcl-1 in apoptosis, there are no data about its ability tomodulate function and phenotypic changes in T cells.Other antiapoptotic Bcl-2 molecules, however, were shownto inhibit (Bcl-xL) or promote (Bcl-2) similar processes
associated with senescence (45, 46). We observe that IL-7consistently causes the phosphorylation of AKT (activa-tion) and GSK3b (inhibition) and prevents the increase inphosphorylation of Mcl-1. These findings seem to occur asearly as 30 to 60 minutes after administration of IL-7,indicating their temporal proximity. Although the increasein Mcl-1 expression could be due to lack of phosphoryla-tion and degradation, others have shown that AKT caninduce increases in Mcl-1 expression via a translationalmechanism (47). Regardless, the importance of these find-ings was confirmed through knockdown and chemicalinhibition of Mcl-1 in tumor-exposed T cells, showing itsimportance in preventing dysfunctional phenotypicchanges and indicating a novel nonapoptotic role.
Given that Mcl-1 has important function in resisting thetumor-induced T-cell phenotypic changes in our model, wedecided to investigate whether a related proapoptoticmole-cule, Bim, also played a role. Other and we have alreadyshown that Bim binds to and is inhibited by Mcl-1 inapoptosis (24). Our data show that not only does IL-7reduce the phosphorylation and increase the overall expres-sion of Mcl-1 but also causes an increase in free Mcl-1protein (not bound to Bim), resulting in a protective effect.
In summary, we present the novel conclusion that thecytokine IL-7 can prevent the formation of dysfunctionalT cells that display suppressor function and senescentphenotype. We further show novel data indicating that amajor IL-7–induced antiapoptotic pathway is also pro-tective (see Supplementary Fig. S10 for a diagrammaticoverview). Despite recent advances in immunotherapy,successful clinical outcomes remain limited (27, 48) andtumor-induced immunosuppression could be a majorcontributing factor (49). As a result, there is new enthu-siasm for cytoprotective strategies that are designed toovercome these processes (50). Cytokines such as IL-7reduce many aspects of cancer immunosuppression,including induction of dysfunctional phenotypic andfunctional immune changes, such as those elucidatedin this study. Therefore, future approaches to treat cancerusing immunotherapies will require the incorporation ofcytoprotective strategies, such as IL-7, to bring them toclinical reality.
Disclosure of Potential Conflicts of Interest
S.E. Strome is a cofounder and major stockholder in Gliknik Inc., abiotechnology company. He also receives royalties through the Mayo ClinicCollege of Medicine for licensure of intellectual property related to B7-H1(PD-L1) and 4-1BB (CD137) to third parties.
Grant Support
This work was sponsored by an award from the Charlotte Geyer Founda-tion and the National Cancer Institute, NIH (grant #5R01CA132796).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received January 4, 2011; revised May 26, 2011; accepted May 26, 2011;published OnlineFirst June 28, 2011.
Zhang et al.
Clin Cancer Res; 17(15) August 1, 2011 Clinical Cancer Research4984
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

References1. Montes CL, Chapoval AI, Nelson J, Orhue V, Zhang X, Schulze DH,
et al. Tumor-induced senescent T cells with suppressor function: apotential form of tumor immune evasion. Cancer Res 2008;68:870–9.
2. Zhou J, Shen X, Huang J, Hodes RJ, Rosenberg SA, Robbins PF.Telomere length of transferred lymphocytes correlates with in vivopersistence and tumor regression in melanoma patients receiving celltransfer therapy. J Immunol 2005;175:7046–52.
3. Filaci G, Fenoglio D, FravegaM, Ansaldo G, Borgonovo G, Traverso P,et al. CD8þ CD28� T regulatory lymphocytes inhibiting T cell pro-liferative and cytotoxic functions infiltrate human cancers. J Immunol2007;179:4323–34.
4. Vallejo AN. CD28 extinction in human T cells: altered functions and theprogram of T-cell senescence. Immunol Rev 2005;205:158–69.
5. Effros RB. Role of T lymphocyte replicative senescence in vaccineefficacy. Vaccine 2007;25:599–604.
6. Karagoz B, Bilgi O, Gumus M, Erikci AA, Sayan O, Turken O, et al.CD8þCD28� cells and CD4þCD25þ regulatory T cells in the peripheralblood of advanced stage lung cancer patients. Med Oncol 2009;27:29–33.
7. Martinez-Escribano JA, Hernandez-Caselles T, Campillo JA, Cam-pos M, Frias JF, Garcia-Alonso A, et al. Changes in the number ofCD80(þ), CD86(þ), and CD28(þ) peripheral blood lymphocyteshave prognostic value in melanoma patients. Hum Immunol2003;64:796–801.
8. Tsukishiro T, Donnenberg AD, Whiteside TL. Rapid turnover of theCD8(þ)CD28(�) T-cell subset of effector cells in the circulation ofpatients with head and neck cancer. Cancer Immunol Immunother2003;52:599–607.
9. Effros RB, Dagarag M, Spaulding C, Man J. The role of CD8þ T-cellreplicative senescence in human aging. Immunol Rev 2005;205:147–57.
10. Powell DJ Jr, Dudley ME, Robbins PF, Rosenberg SA. Transition oflate-stage effector T cells to CD27 þCD28þ tumor-reactive effectormemory T cells in humans after adoptive cell transfer therapy. Blood2005;105:241–50.
11. Rathmell JC, Farkash EA, Gao W, Thompson CB. IL-7 enhances thesurvival and maintains the size of naive T cells. J Immunol2001;167:6869–76.
12. Soares MV, Borthwick NJ, Maini MK, Janossy G, Salmon M, AkbarAN. IL-7-dependent extrathymic expansion of CD45RAþ T cellsenables preservation of a naive repertoire. J Immunol 1998;161:5909–17.
13. Warrington KJ, Vallejo AN, Weyand CM, Goronzy JJ. CD28 loss insenescent CD4þ T cells: reversal by interleukin-12 stimulation. Blood2003;101:3543–9.
14. Sportes C, Hakim FT,Memon SA, ZhangH, Chua KS, BrownMR, et al.Administration of rhIL-7 in humans increases in vivo TCR repertoirediversity by preferential expansion of naive T cell subsets. J Exp Med2008;205:1701–14.
15. Henson SM, Franzese O, Macaulay R, Libri V, Azevedo RI, Kiani-Alikhan S, et al. KLRG1 signaling induces defective Akt (Ser473)phosphorylation and proliferative dysfunction of highly differentiatedCD8þ T cells. Blood 2009;113:6619–28.
16. Pallard C, Stegmann AP, van Kleffens T, Smart F, Venkitaraman A,Spits H. Distinct roles of the phosphatidylinositol 3-kinase and STAT5pathways in IL-7-mediated development of human thymocyte pre-cursors. Immunity 1999;10:525–35.
17. Muller J, Sperl B, Reindl W, Kiessling A, Berg T. Discovery of chro-mone-based inhibitors of the transcription factor STAT5. Chembio-chem 2008;9:723–7.
18. Li WQ, Jiang Q, Khaled AR, Keller JR, Durum SK. Interleukin-7inactivates the pro-apoptotic protein Bad promoting T cell survival.J Biol Chem 2004;279:29160–6.
19. Hahn-Windgassen A, Nogueira V, Chen CC, Skeen JE, Sonenberg N,Hay N. Akt activates the mammalian target of rapamycin by regulatingcellular ATP level and AMPK activity. J Biol Chem 2005;280:32081–9.
20. Geginat J, Sallusto F, Lanzavecchia A. Cytokine-driven proliferationand differentiation of human naive, central memory, and effectormemory CD4(þ) T cells. J Exp Med 2001;194:1711–9.
21. Delcommenne M, Tan C, Gray V, Rue L, Woodgett J, Dedhar S.Phosphoinositide-3-OH kinase-dependent regulation of glycogensynthase kinase 3 and protein kinase B/AKT by the integrin-linkedkinase. Proc Natl Acad Sci U S A 1998;95:11211–6.
22. Maurer U, Charvet C, Wagman AS, Dejardin E, Green DR. Glycogensynthase kinase-3 regulates mitochondrial outer membrane permea-bilization and apoptosis by destabilization of MCL-1. Mol Cell2006;21:749–60.
23. Han J, Goldstein LA, Gastman BR, Rabinovitz A, Rabinowich H.Disruption of Mcl-1.Bim complex in granzyme B-mediated mitochon-drial apoptosis. J Biol Chem 2005;280:16383–92.
24. Han J, Goldstein LA, Gastman BR, RabinowichH. Interrelated roles forMcl-1 and BIM in regulation of TRAIL-mediated mitochondrial apop-tosis. J Biol Chem 2006;281:10153–63.
25. Huntington ND, Labi V, Cumano A, Vieira P, Strasser A, Villunger A,et al. Loss of the pro-apoptotic BH3-only Bcl-2 family member Bimsustains B lymphopoiesis in the absence of IL-7. Int Immunol2009;21:715–25.
26. Whiteside TL. Immune responses to malignancies. J Allergy ClinImmunol 2010;125:S272–83.
27. Morgan RA, Dudley ME, Wunderlich JR, Hughes MS, Yang JC, SherryRM, et al. Cancer regression in patients after transfer of geneticallyengineered lymphocytes. Science 2006;314:126–9.
28. Imamichi H, Sereti I, Lane HC. IL-15 acts as a potent inducer of CD4(þ)CD25(hi) cells expressing FOXP3. Eur J Immunol 2008;38:1621–30.
29. Yamada H, Kaibara N, Okano S, Maeda T, Shuto T, Nakashima Y,et al. Interleukin-15 selectively expands CD57þ CD28� CD4þ T cells,which are increased in active rheumatoid arthritis. Clin Immunol2007;124:328–35.
30. RochmanY,SpolskiR, LeonardWJ.New insights into the regulationofTcells by gamma(c) family cytokines. Nat Rev Immunol 2009;9:480–90.
31. van Herpen CM, van der Laak JA, de Vries IJ, van Krieken JH, deWildePC, Balvers MG, et al. Intratumoral recombinant human interleukin-12administration in head and neck squamous cell carcinoma patientsmodifies locoregional lymph node architecture and induces naturalkiller cell infiltration in the primary tumor. Clin Cancer Res 2005;11:1899–909.
32. Rosenberg SA, Sportes C, Ahmadzadeh M, Fry TJ, Ngo LT, SchwarzSL, et al. IL-7 administration to humans leads to expansion of CD8þ
and CD4þ cells but a relative decrease of CD4 þT-regulatory cells. JImmunother 2006;29:313–9.
33. Moller P, Sun Y, Dorbic T, Alijagic S, Makki A, Jurgovsky K, et al.Vaccination with IL-7 gene-modified autologous melanoma cells canenhance the anti-melanoma lytic activity in peripheral blood ofpatients with a good clinical performance status: a clinical phase Istudy. Br J Cancer 1998;77:1907–16.
34. Levy Y, Lacabaratz C, Weiss L, Viard JP, Goujard C, Lelievre JD, et al.Enhanced T cell recovery in HIV-1-infected adults through IL-7 treat-ment. J Clin Invest 2009;119:997–1007.
35. Sereti I, Dunham RM, Spritzler J, Aga E, ProschanMA, Medvik K, et al.IL-7 administration drives T cell-cycle entry and expansion in HIV-1infection. Blood 2009;113:6304–14.
36. Pellegrini M, Calzascia T, Elford AR, Shahinian A, Lin AE, DissanayakeD, et al. Adjuvant IL-7 antagonizes multiple cellular and molecularinhibitory networks to enhance immunotherapies. Nat Med2009;15:528–36.
37. Jiang Q, Li WQ, Aiello FB, Mazzucchelli R, Asefa B, Khaled AR, et al.Cell biology of IL-7, a key lymphotrophin. Cytokine Growth Factor Rev2005;16:513–33.
38. Kittipatarin C, Khaled AR. Interlinking interleukin-7. Cytokine2007;39:75–83.
39. Plunkett FJ, Franzese O, Finney HM, Fletcher JM, Belaramani LL,Salmon M, et al. The loss of telomerase activity in highly differentiatedCD8þCD28�CD27� T cells is associated with decreased Akt (Ser473)phosphorylation. J Immunol 2007;178:7710–9.
40. Nogueira V, Park Y, Chen CC, Xu PZ, Chen ML, Tonic I, et al. Aktdetermines replicative senescence and oxidative or oncogenic pre-mature senescence and sensitizes cells to oxidative apoptosis. Can-cer Cell 2008;14:458–70.
IL-7 Inhibits Tumor-Induced Human Suppressor T cells
www.aacrjournals.org Clin Cancer Res; 17(15) August 1, 2011 4985
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

41. Zimmermann S, Moelling K. Phosphorylation and regulation of Raf byAkt (protein kinase B). Science 1999;286:1741–4.
42. Mitsiades CS,Mitsiades N, Koutsilieris M. The Akt pathway: moleculartargets for anti-cancer drug development. Curr Cancer Drug Targets2004;4:235–56.
43. Breslin EM, White PC, Shore AM, Clement M, Brennan P. LY294002and rapamycin co-operate to inhibit T-cell proliferation. Br J Pharma-col 2005;144:791–800.
44. Wang CY, Kim HH, Hiroi Y, Sawada N, Salomone S, Benjamin LE,et al. Obesity increases vascular senescence and susceptibility toischemic injury through chronic activation of Akt and mTOR. SciSignal 2009;2:ra11.
45. Jung MS, Jin DH, Chae HD, Kang S, Kim SC, Bang YJ, et al. Bcl-xLand E1B-19K proteins inhibit p53-induced irreversible growth arrestand senescence by preventing reactive oxygen species-dependentp38 activation. J Biol Chem 2004;279:17765–71.
46. Nelyudova A, Aksenov N, Pospelov V, Pospelova T. By blockingapoptosis, Bcl-2 in p38-dependent manner promotes cell cycle arrestand accelerated senescence after DNA damage and serum with-drawal. Cell Cycle 2007;6:2171–7.
47. Woodland RT, Fox CJ, Schmidt MR, Hammerman PS, Opferman JT,Korsmeyer SJ, et al. Multiple signaling pathways promote B lympho-cyte stimulator dependent B-cell growth and survival. Blood2008;111:750–60.
48. Hunder NN, Wallen H, Cao J, Hendricks DW, Reilly JZ, Rodmyre R,et al. Treatment of metastatic melanomawith autologous CD4þ T cellsagainst NY-ESO-1. N Engl J Med 2008;358:2698–703.
49. Rosenberg SA. Progress in human tumour immunology and immu-notherapy. Nature 2001;411:380–4.
50. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, HaanenJB, et al. Improved survival with ipilimumab in patients with metastaticmelanoma. N Engl J Med 2010;363:711–23.
Zhang et al.
Clin Cancer Res; 17(15) August 1, 2011 Clinical Cancer Research4986
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328

2011;17:4975-4986. Published OnlineFirst June 28, 2011.Clin Cancer Res Yue Zhang, Lukas W. Pfannenstiel, Elzbieta Bolesta, et al. Cells: Implications for Cancer Immunotherapy
Suppressor T−CD28−Interleukin-7 Inhibits Tumor-Induced CD27
Updated version
10.1158/1078-0432.CCR-10-3328doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2011/07/26/1078-0432.CCR-10-3328.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/17/15/4975.full#ref-list-1
This article cites 49 articles, 22 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/17/15/4975.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/17/15/4975To request permission to re-use all or part of this article, use this link
on June 19, 2018. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 28, 2011; DOI: 10.1158/1078-0432.CCR-10-3328