Embed Size (px)
Citation preview

Interferences with Interferences with VentilationVentilationObjectivesObjectives
Describe causes, pathophysiology, clinical Describe causes, pathophysiology, clinical manifestations, therapeutic interventions, & manifestations, therapeutic interventions, & nursing management of patients with restrictive nursing management of patients with restrictive & obstructive pulmonary disease of the upper & obstructive pulmonary disease of the upper and lower airwayand lower airway Sleep apnea, asthma in child & adult, emphysema, Sleep apnea, asthma in child & adult, emphysema,
chronic bronchitis, COPDchronic bronchitis, COPD Describe the nursing process for patients who Describe the nursing process for patients who
experiences accidental interferences to experiences accidental interferences to ventilationventilation Chest traumaChest trauma

Interferences with Interferences with VentilationVentilation
Restrictive / Obstructive Restrictive / Obstructive Airway DiseaseAirway Disease Restrictive DisordersRestrictive Disorders::
Decreased compliance of the lungs or chest Decreased compliance of the lungs or chest wall or bothwall or both
Extrapulmonary – CNS, Neuromuscular, Chest WallExtrapulmonary – CNS, Neuromuscular, Chest Wall Intrapulmonary – Pleural, ParenchymalIntrapulmonary – Pleural, Parenchymal
Obstructive DisordersObstructive Disorders:: Increased resistance to airflowIncreased resistance to airflow
Asthma, Emphysema, Chronic Bronchitis, COPDAsthma, Emphysema, Chronic Bronchitis, COPD

Obstructive Sleep Apnea Obstructive Sleep Apnea (OSA)(OSA)

Obstructive Sleep Apnea Obstructive Sleep Apnea (OSA)(OSA)
Clinical ManifestationsClinical Manifestations: insomnia, daytime : insomnia, daytime sleepiness; witnessed apneic episodes; snoring; sleepiness; witnessed apneic episodes; snoring; morning headaches; impaired concentration & morning headaches; impaired concentration & memorymemory
DxDx: Polysomnography (sleep study) – multiple : Polysomnography (sleep study) – multiple episodes of apnea or hypopnea (airflow diminished episodes of apnea or hypopnea (airflow diminished 30-50% with respiratory effort)30-50% with respiratory effort)
TXTX: Avoid sedatives & alcohol 2-4 hrs prior to sleep; : Avoid sedatives & alcohol 2-4 hrs prior to sleep; compliance with nCPAP / BiPAPcompliance with nCPAP / BiPAP nCPAP nCPAP – continuous + airway pressure + 5-15 cm H2O – continuous + airway pressure + 5-15 cm H2O
pressurepressure BiPAP BiPAP – bilevel + airway pressure – delivers higher pressure – bilevel + airway pressure – delivers higher pressure
during inspiration & lower pressure during expirationduring inspiration & lower pressure during expiration Surgery Surgery
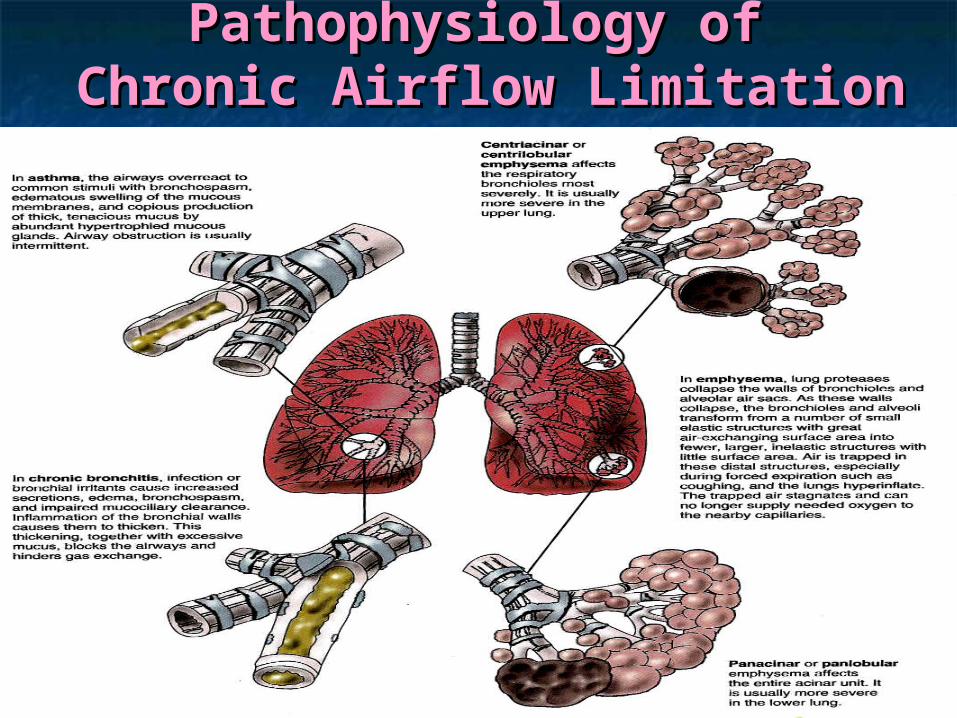
Pathophysiology of Pathophysiology of Chronic Airflow LimitationChronic Airflow Limitation

Interferences with VentilationInterferences with VentilationAsthmaAsthma
Chronic inflammatory disorder of the Chronic inflammatory disorder of the airwaysairways Causes varying degrees of obstruction in the Causes varying degrees of obstruction in the
airwaysairways Recurrent episodes of wheezing, breathlessness, Recurrent episodes of wheezing, breathlessness,
chest tightness, and cough, particularly at night and chest tightness, and cough, particularly at night and in early morningin early morning
Associated with hyperresponsiveness to a variety of Associated with hyperresponsiveness to a variety of stimuli stimuli
Affects 1 in 20 AmericansAffects 1 in 20 Americans 10 millions absences per year10 millions absences per year 5,000 deaths per year5,000 deaths per year

Recurrent and reversible shortness of breathRecurrent and reversible shortness of breath
Airways become narrow as a result of:Airways become narrow as a result of: BronchospasmBronchospasm InflammationInflammation & & EdemaEdema of the bronchial mucosa of the bronchial mucosa Production of viscid mucusProduction of viscid mucus
Alveolar ducts/alveoli remain open, but airflow to them is Alveolar ducts/alveoli remain open, but airflow to them is obstructedobstructed
SymptomsSymptoms WheezingWheezing Difficulty breathingDifficulty breathing
Respiratory System DrugsRespiratory System DrugsAsthmaAsthma

Interferences with Interferences with VentilationVentilation
AsthmaAsthma Triggers of Asthma AttacksTriggers of Asthma Attacks
AllergensAllergens ExerciseExercise Respiratory Infections Respiratory Infections Nose & sinus problemsNose & sinus problems Drugs and food additivesDrugs and food additives Gastroesophageal reflux disease (GERD)Gastroesophageal reflux disease (GERD) Emotional StressEmotional Stress

Interferences with Interferences with VentilationVentilation
Asthma - PathophysiologyAsthma - PathophysiologyHallmarks of Asthma:Hallmarks of Asthma: Airway inflammation & nonspecific Airway inflammation & nonspecific
hyperirritabilityhyperirritability Early phase Early phase
Characterized by bronchospasmCharacterized by bronchospasm Induces inflammatory sequelae of the late phase responseInduces inflammatory sequelae of the late phase response Allergen or irritant cross-links IgE receptors on mast cells Allergen or irritant cross-links IgE receptors on mast cells
beneath the basement membrane of the bronchial wallbeneath the basement membrane of the bronchial wallOROR
Hyperresponsiveness of the Hyperresponsiveness of the tracheobronchial treetracheobronchial tree Caused by bronchoconstriction in response to Caused by bronchoconstriction in response to
physical, chemical and pharmacological agentsphysical, chemical and pharmacological agents

Early & Late Responses in Early & Late Responses in AsthmaAsthma

Classification of Asthma Classification of Asthma SeveritySeverity

Pathophysiology of Pathophysiology of Acute Asthma AttackAcute Asthma Attack

Stepwise Approach for Stepwise Approach for Managing AsthmaManaging Asthma

Interferences with Interferences with VentilationVentilation
Asthma – MedicationAsthma – Medication

Interferences with Interferences with VentilationVentilation
Asthma - MedicationAsthma - Medication

Drug Therapy Drug Therapy Asthma & COPDAsthma & COPD

Drug Therapy – Asthma & Drug Therapy – Asthma & COPDCOPD

How to Use Metered-Dose How to Use Metered-Dose InhalerInhaler

Metered-Dose InhalerMetered-Dose Inhaler

Pair SharePair Share
A client who has been newly diagnosed with A client who has been newly diagnosed with asthma is admitted to the acute care unit for asthma is admitted to the acute care unit for evaluation. The nurse provides the client evaluation. The nurse provides the client with an Albuterol (Proventil, Ventolin) with an Albuterol (Proventil, Ventolin) metered-dose inhaler. The nurse will plan to metered-dose inhaler. The nurse will plan to monitor the client very closely for which of monitor the client very closely for which of the following side effects of Albuterol? the following side effects of Albuterol?
A. Tachycardia and nervousness A. Tachycardia and nervousness B. Nasal congestion and dry mouth B. Nasal congestion and dry mouth C. Sedation and lethargy C. Sedation and lethargy D. Joint pain and unstable gait D. Joint pain and unstable gait

Pair SharePair Share
When exercising, a client with asthma should When exercising, a client with asthma should be taught to monitor for which of the following be taught to monitor for which of the following problems? problems?
A. Increased peak expiratory flow ratesA. Increased peak expiratory flow rates B. Wheezing from bronchospasmB. Wheezing from bronchospasm C. Wheezing from atelectasisC. Wheezing from atelectasis D. Dyspnea from pulmonary hypertensionD. Dyspnea from pulmonary hypertension
What would the nurse recommend to prevent What would the nurse recommend to prevent future episodes of this problem?future episodes of this problem?

Status AsthmaticusStatus Asthmaticus Severe, life-threatening asthma attackSevere, life-threatening asthma attack
Refractory to the usual treatmentRefractory to the usual treatment
““The longer it lasts, the worse it gets, and The longer it lasts, the worse it gets, and the worse it gets, the longer it lasts”the worse it gets, the longer it lasts”
CausesCauses: : viral illnesses, ASA or NSAID viral illnesses, ASA or NSAID ingestion, allergen exposure, abrupt ingestion, allergen exposure, abrupt discontinuation of therapy, B-adrenergic discontinuation of therapy, B-adrenergic blocker ingestion, poorly controlled asthmablocker ingestion, poorly controlled asthma
ResultsResults: increased airway resistance – : increased airway resistance – edema, mucous plugging, bronchospasmedema, mucous plugging, bronchospasm

Status AsthmaticusStatus Asthmaticus Clinical ManifestationsClinical Manifestations::
Wheezing, forced exhalation, neck vein Wheezing, forced exhalation, neck vein distention, HTN, sinus tachycardia, distention, HTN, sinus tachycardia, ventricular dysrhythmiasventricular dysrhythmias
Initial hypoxemia & hypocapniaInitial hypoxemia & hypocapnia Late – hypoxemia & hypercapniaLate – hypoxemia & hypercapnia
Medical ManagementMedical Management:: Medications: Corticosteroids, B2-Medications: Corticosteroids, B2-
adrenergic agonists via MDI, IV adrenergic agonists via MDI, IV AminophyllineAminophylline
HydrationHydration Oxygen – Humidified; Oxygen – Humidified;
Intubation/Mechanical Ventilation 10% of Intubation/Mechanical Ventilation 10% of the timethe time

Chronic Obstructive Lung Chronic Obstructive Lung DiseaseDisease
Chronic Bronchitis Chronic Bronchitis Presence of chronic productive cough for Presence of chronic productive cough for
3 months in 2 successive years in a 3 months in 2 successive years in a patient in whom other causes of chronic patient in whom other causes of chronic cough have been excludedcough have been excluded Frequent respiratory infectionsFrequent respiratory infections Hx of cigarette smoking for many yearsHx of cigarette smoking for many years Hypoxemia & Hypercapnia Hypoxemia & Hypercapnia result from result from
hypoventilationhypoventilation Bluish-red color of skinBluish-red color of skin
Polycythemia – body’s attempt to compensate for Polycythemia – body’s attempt to compensate for chronic hypoxemia by increasing production of red chronic hypoxemia by increasing production of red blood cells blood cells

Chronic Obstructive Lung Chronic Obstructive Lung DiseaseDisease
Chronic Bronchitis Chronic Bronchitis A client with chronic bronchitis often A client with chronic bronchitis often
shows signs of hypoxia. The nurrse shows signs of hypoxia. The nurrse would observe for which of the would observe for which of the following clinical manifestations of this following clinical manifestations of this problem?problem?
A. Increased capillary refillA. Increased capillary refill B. Clubbing of fingersB. Clubbing of fingers C. Pink mucous membranesC. Pink mucous membranes D. Overall pale appearanceD. Overall pale appearance

Chronic Obstructive Lung Chronic Obstructive Lung DiseaseDisease
Chronic Bronchitis Chronic Bronchitis In chronic bronchitis, impaired gas exchange occurs as a In chronic bronchitis, impaired gas exchange occurs as a
result of which of the following?result of which of the following?
A. Chronic inflammation, thin secretions, and chronic A. Chronic inflammation, thin secretions, and chronic infectioninfection
B. Respiratory alkalosis, decreased PaCOB. Respiratory alkalosis, decreased PaCO2, 2, and increased and increased PaOPaO22
C. Chronic inflammation and decreased surfactant in the C. Chronic inflammation and decreased surfactant in the alveoli and atelectasisalveoli and atelectasis
D. Thickening of the bronchial walls, large amounts of D. Thickening of the bronchial walls, large amounts of thick thick
secretions, and repeated infectionssecretions, and repeated infections

Chronic Obstructive Lung Chronic Obstructive Lung DiseaseDisease
Emphysema Emphysema Abnormal permanent enlargement of the Abnormal permanent enlargement of the
airspaces distal to the terminal airspaces distal to the terminal bronchioles, accompanied by destruction bronchioles, accompanied by destruction of their walls and without obvious fibrosisof their walls and without obvious fibrosis
Risk FactorsRisk Factors:: Cigarette SmokingCigarette Smoking
Irritation - > 4,000 chemicals inhaledIrritation - > 4,000 chemicals inhaled Hyperplasia – reduces airway diameterHyperplasia – reduces airway diameter Abnormal dilatation of distal airspacesAbnormal dilatation of distal airspaces
Destruction of alveolar wallsDestruction of alveolar walls

Chronic Obstructive Lung Chronic Obstructive Lung DiseaseDisease
Emphysema Emphysema Risk Factors (cont’dRisk Factors (cont’d):):
Recurring respiratory tract infectionsRecurring respiratory tract infections H. flu, Strep pneumoniae, Moraxella catarrhalisH. flu, Strep pneumoniae, Moraxella catarrhalis
HeredityHeredity – alpha 1 – – alpha 1 –Antitrypsin (ATT) deficiencyAntitrypsin (ATT) deficiency Accounts for <1% of COPD in USAccounts for <1% of COPD in US AAT is a serum protein produced by the liver and normally AAT is a serum protein produced by the liver and normally
found in the lungsfound in the lungs IV or nebulized AAT (Prolastin) slows COPD progressionIV or nebulized AAT (Prolastin) slows COPD progression
Aging Aging – Changes in lung structure – Changes in lung structure Gradual loss of elastic recoil – thin alveolar wall – thoracic Gradual loss of elastic recoil – thin alveolar wall – thoracic
cage changes from osteoporosis & calcificationcage changes from osteoporosis & calcification

Comparison of Comparison of Emphysema & Chronic Emphysema & Chronic
Bronchitis Bronchitis Alveolar Problem Alveolar Problem Airway ProblemAirway Problem

COPDCOPDPulmonary Blebs & BullaePulmonary Blebs & Bullae

COPD -- Interaction of COPD -- Interaction of Chronic Bronchitis & Chronic Bronchitis &
EmphysemaEmphysema

Pathophysiology of Chronic Pathophysiology of Chronic Bronchitis and EmphysemaBronchitis and Emphysema

Interferences with Interferences with VentilationVentilation
Medical Management GoalsMedical Management Goals Improve ventilationImprove ventilation Promote removal of secretionsPromote removal of secretions Prevent complications & Prevent complications &
progression of symptomsprogression of symptoms Promote patient comfort & Promote patient comfort &
participation in careparticipation in care Improve quality of life as much Improve quality of life as much
as possibleas possible

Interferences with Interferences with VentilationVentilation
Medical TreatmentMedical Treatment Patients are treated primarily as Patients are treated primarily as
outpatientsoutpatients HospitalizationsHospitalizations
Acute exacerbationsAcute exacerbations ComplicationsComplications
Respiratory failure, pneumonia, Respiratory failure, pneumonia, congestive heart failurecongestive heart failure

Interferences with Interferences with VentilationVentilation
COPDCOPDA high-liter flow of oxygen is contraindicated in the A high-liter flow of oxygen is contraindicated in the
client with COPD because of which of the following?client with COPD because of which of the following?
A. The client depends often on a hypercapnic drive A. The client depends often on a hypercapnic drive to breatheto breathe
B. The client depends on a hypoxic drive to breatheB. The client depends on a hypoxic drive to breathe
C. Receiving too much oxygen over a short time C. Receiving too much oxygen over a short time results in a headacheresults in a headache
D. Response to high doses needed later will be D. Response to high doses needed later will be ineffectiveineffective

Interferences with Interferences with VentilationVentilation
COPDCOPD When teaching a client to use aerosol When teaching a client to use aerosol
treatments, the following is the correct sequence treatments, the following is the correct sequence for administering aerosol tx?for administering aerosol tx?
A. Steroid should be given immediately after the A. Steroid should be given immediately after the bronchodilatorbronchodilator
B. Steroid should be given 5 to 10 minutes after the B. Steroid should be given 5 to 10 minutes after the bronchodilatorbronchodilator
C. Bronchodilator should be given immediately after the C. Bronchodilator should be given immediately after the steroidsteroid
D. Bronchodilator should be given 5 to 10 minutes after the D. Bronchodilator should be given 5 to 10 minutes after the steroidsteroid

Interferences with Interferences with VentilationVentilation
Medical ManagementMedical Management Smoking cessationSmoking cessation Treatment of respiratory infectionsTreatment of respiratory infections Bronchodilator therapyBronchodilator therapy
Beta2-adrenergic agonistsBeta2-adrenergic agonists Anticholinergic agentsAnticholinergic agents Long-acting theophyllineLong-acting theophylline
CorticosteroidsCorticosteroids PEFR monitoring (peak expiratory flow rate)PEFR monitoring (peak expiratory flow rate) Chest physiotherapy / Breathing exercises & Chest physiotherapy / Breathing exercises &
retrainingretraining Hydration 3L/day (unless contraindicated)Hydration 3L/day (unless contraindicated) Rest - Progressive plan of exerciseRest - Progressive plan of exercise Patient & family educationPatient & family education Influenza / Pneumovax immunizationInfluenza / Pneumovax immunization Low flow oxygen rate (if indicated)Low flow oxygen rate (if indicated) Pulmonary rehabilitation programPulmonary rehabilitation program

Interference with Interference with VentilationVentilation
Oxygen TherapyOxygen Therapy IndicationsIndications::
TreatTreat: Respiratory; CV; CNS disturbances: Respiratory; CV; CNS disturbances Oxygen AdministrationOxygen Administration: High or low flow systems: High or low flow systems
High FlowHigh Flow — delivers fixed concentrations independent — delivers fixed concentrations independent of the patient’s respiratory patternof the patient’s respiratory pattern
Venturi Mask – up to 50%Venturi Mask – up to 50% Low FlowLow Flow — amount delivered varies with patient’s — amount delivered varies with patient’s
respiratory pattern respiratory pattern Nasal cannula 2L/min = 28% oxygenNasal cannula 2L/min = 28% oxygen Face tent or trach collar – Increased humidityFace tent or trach collar – Increased humidity Non-re-breathing mask – delivers 60-90% Non-re-breathing mask – delivers 60-90%
HumidityHumidity: : 1-4L low flow – use of “bubble-through” 1-4L low flow – use of “bubble-through”
controversialcontroversial NebulizedNebulized

Interferences with Interferences with VentilationVentilation
Oxygen Therapy- Oxygen Therapy- ComplicationsComplications CO2 NarcosisCO2 Narcosis – –
two chemoreceptors – O2 CO2two chemoreceptors – O2 CO2 CO2 accumulation – major stimulusCO2 accumulation – major stimulus COPD patient –COPD patient –
Develops tolerance to high CO2Develops tolerance to high CO2 Respiratory Center loses sensitivity to elevated CO2Respiratory Center loses sensitivity to elevated CO2
O2 Drive “Hypoxemia” O2 Drive “Hypoxemia” Concern about administering O2 to COPD patients ??Concern about administering O2 to COPD patients ?? Bigger Concern: not providing adequate O2Bigger Concern: not providing adequate O2
Goal: Titrate O2 to the lowest effective dose Goal: Titrate O2 to the lowest effective dose based on arterial blood gas monitoringbased on arterial blood gas monitoring

Interferences with VentilationInterferences with VentilationOxygen Therapy- Oxygen Therapy-
ComplicationsComplications O2 ToxicityO2 Toxicity
Prolonged exposure to high level O2Prolonged exposure to high level O2 Determined by patient tolerance, exposure Determined by patient tolerance, exposure
time, and effective dosetime, and effective dose High level Manifestations – High level Manifestations –
Initial -- Inactivate surfactant and lead to ARDS : Initial -- Inactivate surfactant and lead to ARDS : reduced vital capacity, cough, substernal chest pain, reduced vital capacity, cough, substernal chest pain, N&V, paresthesia, nasal stuffiness, sore throat, N&V, paresthesia, nasal stuffiness, sore throat, malaise malaise
Later – affects alveolar-capillary gas exchange: Later – affects alveolar-capillary gas exchange: pulmonary edema with copious sputumpulmonary edema with copious sputum
End Stage – lung fibrosisEnd Stage – lung fibrosis O2 Administration Goal: enough O2 to maintain O2 Administration Goal: enough O2 to maintain
PaO2 within normal or acceptable limitPaO2 within normal or acceptable limit O2 administration > 50% for > 24 hours potentially O2 administration > 50% for > 24 hours potentially
toxic toxic

Chronic Obstructive Lung Chronic Obstructive Lung Disease ComplicationsDisease Complications

Pair SharePair Share The nurse should report what unexpected The nurse should report what unexpected
findings in a client with emphysema? findings in a client with emphysema? A. Decreased breath sounds and dyspnea A. Decreased breath sounds and dyspnea
onon
exertionexertion B. Sputum with gram negative rods an B. Sputum with gram negative rods an
periods of apneaperiods of apnea C. Vesicular breath sounds and decreased C. Vesicular breath sounds and decreased
thoracic expansionthoracic expansion D. Increased anteroposterior chest D. Increased anteroposterior chest
measurementmeasurement

Nursing Care ManagementNursing Care ManagementIneffective airway Ineffective airway
clearanceclearance AssessAssess: Normal breath sounds; effective : Normal breath sounds; effective
coughingcoughing
Nsg ActionNsg Action: Elevate head of bed; sitting : Elevate head of bed; sitting up; hydration 2-3L/d; chest physiotherapy; up; hydration 2-3L/d; chest physiotherapy; Meds: inhaled bronchodilators Meds: inhaled bronchodilators
Pt EducationPt Education: Effective breathing & : Effective breathing & coughing techniques; Medications & coughing techniques; Medications & administrationadministration

Chest PercussionChest PercussionCupped Hand TechniqueCupped Hand Technique

Chest PhysiotherapyChest Physiotherapy

Postural DrainagePostural Drainage

Nursing Care ManagementNursing Care ManagementImpaired Gas ExchangeImpaired Gas Exchange
AssessAssess: Mental status; VS with Pulse : Mental status; VS with Pulse oximetry; ABGsoximetry; ABGs
Nsg ActionNsg Action: Position – Tripod-supported : Position – Tripod-supported extremities; Administer O2 to effective extremities; Administer O2 to effective level;level;
Pt EducationPt Education: Pursed-lip breathing; signs, : Pursed-lip breathing; signs, symptoms & consequences of hypercapnia; symptoms & consequences of hypercapnia; avoidance of CNS depressants; Medication avoidance of CNS depressants; Medication action; smoking cessationaction; smoking cessation

Orthopnea Positions to Orthopnea Positions to Decrease the Work of Decrease the Work of
BreathingBreathing

Nursing Care ManagementNursing Care ManagementImbalanced NutritionImbalanced Nutrition
AssessAssess: : Weight within normal range for height and Weight within normal range for height and
age; appetite; caloric intact; energy level; age; appetite; caloric intact; energy level; gastric distention; sputum production; affect; gastric distention; sputum production; affect; lack of interest in foods; serum albumin levellack of interest in foods; serum albumin level
Nsg ActionNsg Action: : Hi PRO, HI Calorie foods & liquid Hi PRO, HI Calorie foods & liquid
supplements; small frequent feedings; supplements; small frequent feedings; periods of rest after food intake; Referral—periods of rest after food intake; Referral—financial & nutritional support (Meals-on-financial & nutritional support (Meals-on-wheels; food stamps) wheels; food stamps)
Pt EducationPt Education: : Referrals / Importance of rest / digestion / Referrals / Importance of rest / digestion /
high protein & calorie foods – menu planninghigh protein & calorie foods – menu planning

Nursing Care ManagementNursing Care ManagementDisturbed Sleep PatternDisturbed Sleep Pattern
AssessAssess: : Identify usual patterns; explore reasons for Identify usual patterns; explore reasons for
discomfort, wakefulness, or difficulty sleeping; discomfort, wakefulness, or difficulty sleeping; sleep apneasleep apnea
Nsg ActionNsg Action: : Identify pt-specific relaxation methods; Identify pt-specific relaxation methods;
environment conducive to restenvironment conducive to rest
Pt EducationPt Education: : Balance activity (ADL’s) / rest; avoidance of Balance activity (ADL’s) / rest; avoidance of
alcoholic beverages, caffeine products, & other alcoholic beverages, caffeine products, & other stimulants before bedtime; include family; stimulants before bedtime; include family; sexual activity—positions of comfort; sexual activity—positions of comfort; psychosocial issuespsychosocial issues

Nursing Care ManagementNursing Care ManagementRisk for Infection Risk for Infection
AssessAssess: : Change in color, consistency, quantity, odor & viscosity Change in color, consistency, quantity, odor & viscosity
of sputum; difficulty mobilizing secretions; foul oral of sputum; difficulty mobilizing secretions; foul oral odor; increased dyspnea; fever; chills; diaphoresis; odor; increased dyspnea; fever; chills; diaphoresis; changes in respiratory rate & quality; breath sounds; changes in respiratory rate & quality; breath sounds; hypoxemia; hypercapnia – VS & pulse oximetry hypoxemia; hypercapnia – VS & pulse oximetry
Nsg ActionNsg Action: : Humidification; specimen collection; medication Humidification; specimen collection; medication
administrationadministration
Pt EducationPt Education: : Hand-washing; avoid contact with infected individuals; Hand-washing; avoid contact with infected individuals;
care & cleaning of home respiratory equipment; when to care & cleaning of home respiratory equipment; when to seek medical attention; steroid use; medication useseek medical attention; steroid use; medication use

Breathing ExercisesBreathing Exercises

Pair Share Pair Share The client with chronic obstructive pulmonary The client with chronic obstructive pulmonary
disease (COPD) has been hospitalized in the disease (COPD) has been hospitalized in the respiratory intensive care unit due to an acute respiratory intensive care unit due to an acute exacerbation of COPD. The client’s arterial exacerbation of COPD. The client’s arterial blood gas analysis of 3 samples earlier in the blood gas analysis of 3 samples earlier in the day are demonstrating a trending of increasing day are demonstrating a trending of increasing hypoxemia and hypercapnia. The nurse will hypoxemia and hypercapnia. The nurse will observe the client closely for a sign which would observe the client closely for a sign which would indicate impending respiratory failure, which indicate impending respiratory failure, which would be would be
A. increased expectoration of sputum A. increased expectoration of sputum B. decreased heart rate B. decreased heart rate C. increased respiratory rate C. increased respiratory rate D. decreased level of consciousnessD. decreased level of consciousness