Embed Size (px)
Citation preview
Interesting Case
Chrissy ZoonDecember 11th 2014
Pediatric Surgery
• 6 yo AAF• PMH: hemihypertrophy,
asthma, eczema• FH: none• SH: lives at home with
mom, siblings• US/MRI at 3 mo left kidney
mass – nephroblastomatosis• Plan for Q3mo US/MRIs
alternating but lost to follow up
• Presented 8/2014 to OSH with right abdominal pain, nausea, vomiting
• AF VSS• On physical exam was
felt to have abdominal mass
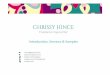
• CT scan performed
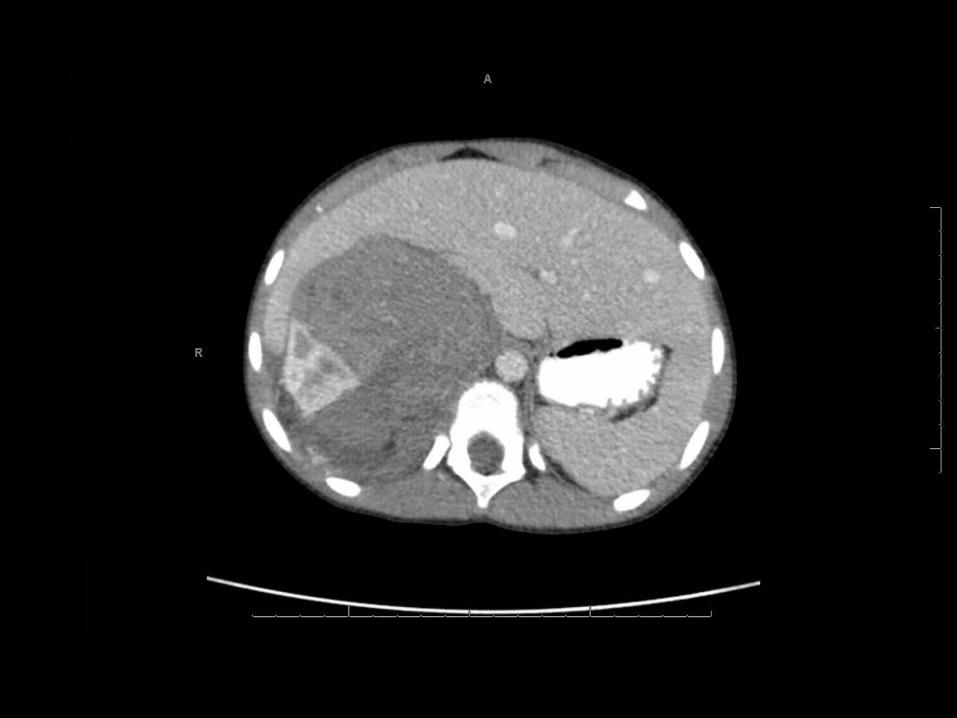

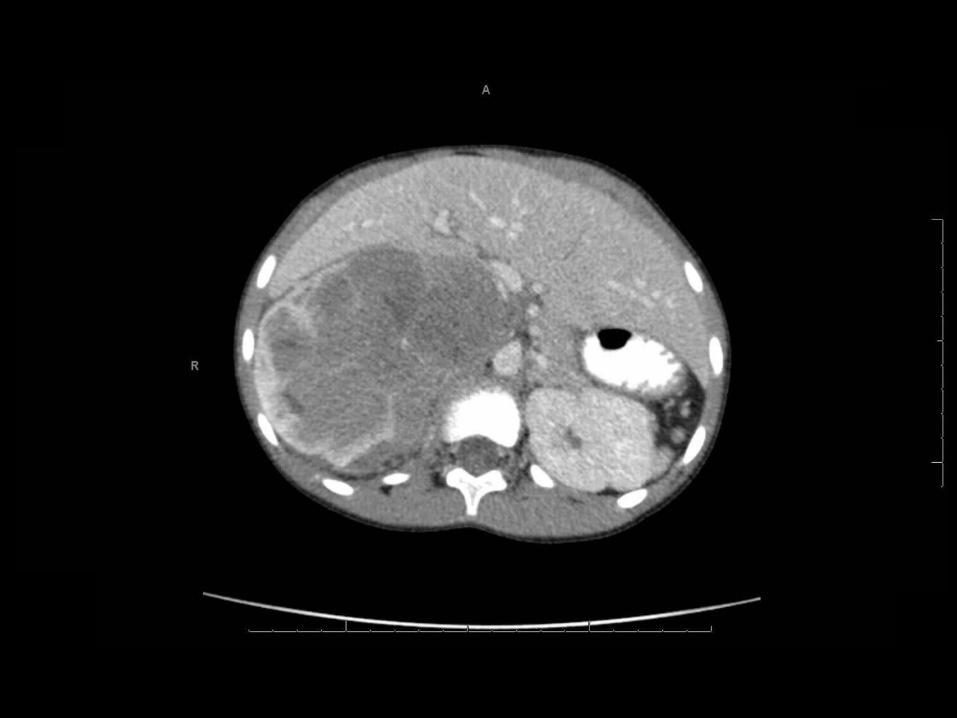
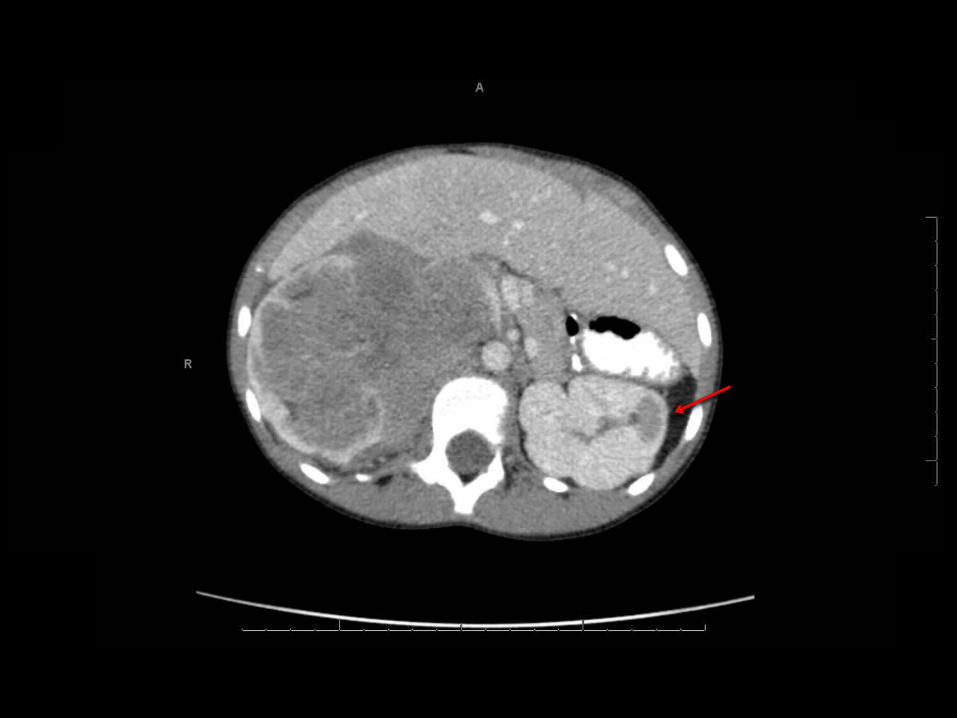
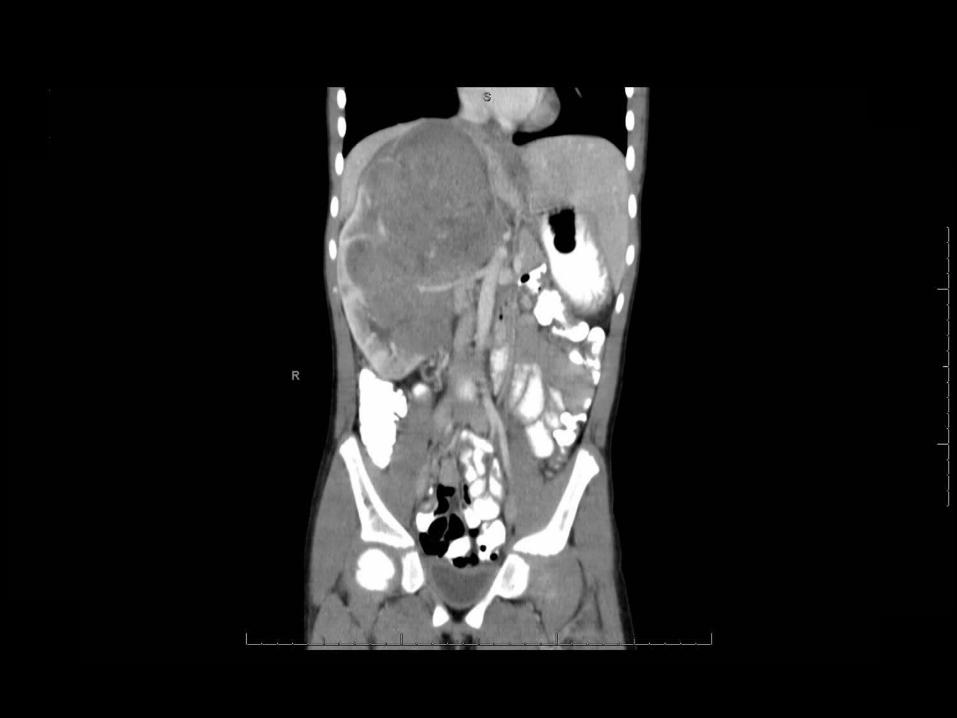
• Concern for bilateral Wilms tumors• Started on neoadjuvant protocol
COG protocol for the treatment of bilateral Wilms tumor, on Aug 2, 2014.

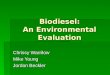
After ~ 1 month chemotherapy


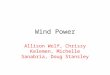
After ~ 3 months chemotherapy

Definitive surgery
• Right radical nephrectomy• Nephrectomy, lymph node sampling (hilar, pericaval,
periaortic), ureter
• Intraoperative US of left kidney (peds urology assisting)
• No gross or US abnormalities seen
• Pathology• Wilms tumor with prominent treatment effects• 0/7 nodes positive for metastatic disease• Stage III – tumor(changes) present at margins and h/o
biopsy before definitive surgery
Epidemiology
• 2nd most common pediatric solid abdominal tumor and most common renal malignancy
• Incidence is 8 cases per million in children <15yo– 500 new cases annually– 6% all childhood malignant tumors
• Most present between ages 1-5 – 66% before 5, 95% before 10
• Survival has increased dramatically over the years– 1930s: 30%– 2010s: >90%
• Multidisciplinary approach
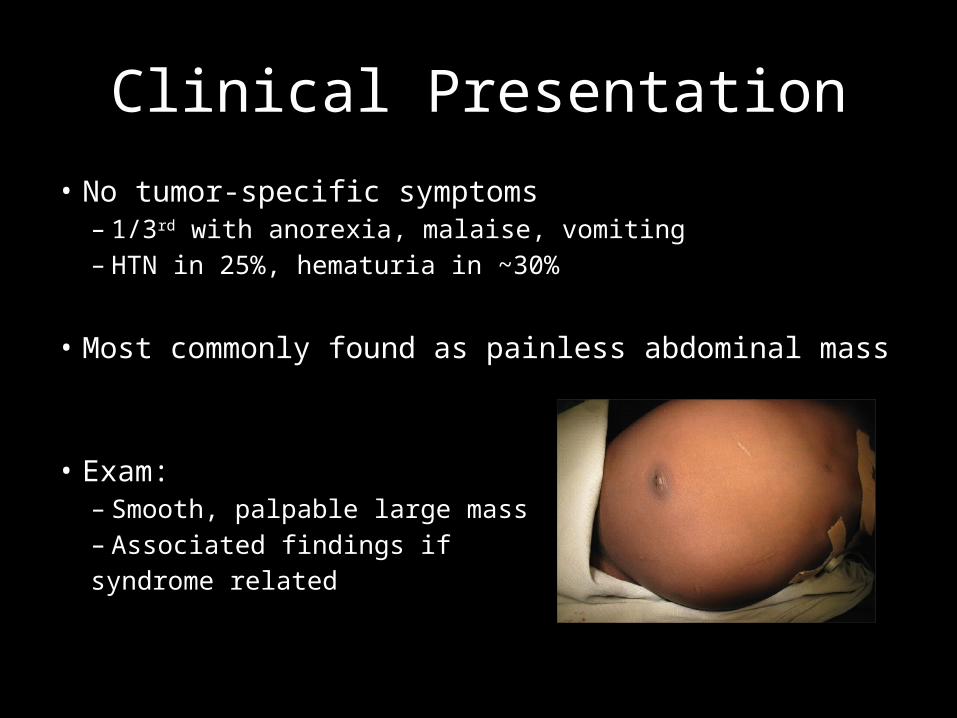
Clinical Presentation
• No tumor-specific symptoms– 1/3rd with anorexia, malaise, vomiting– HTN in 25%, hematuria in ~30%
• Most commonly found as painless abdominal mass
• Exam:– Smooth, palpable large mass– Associated findings if syndrome related
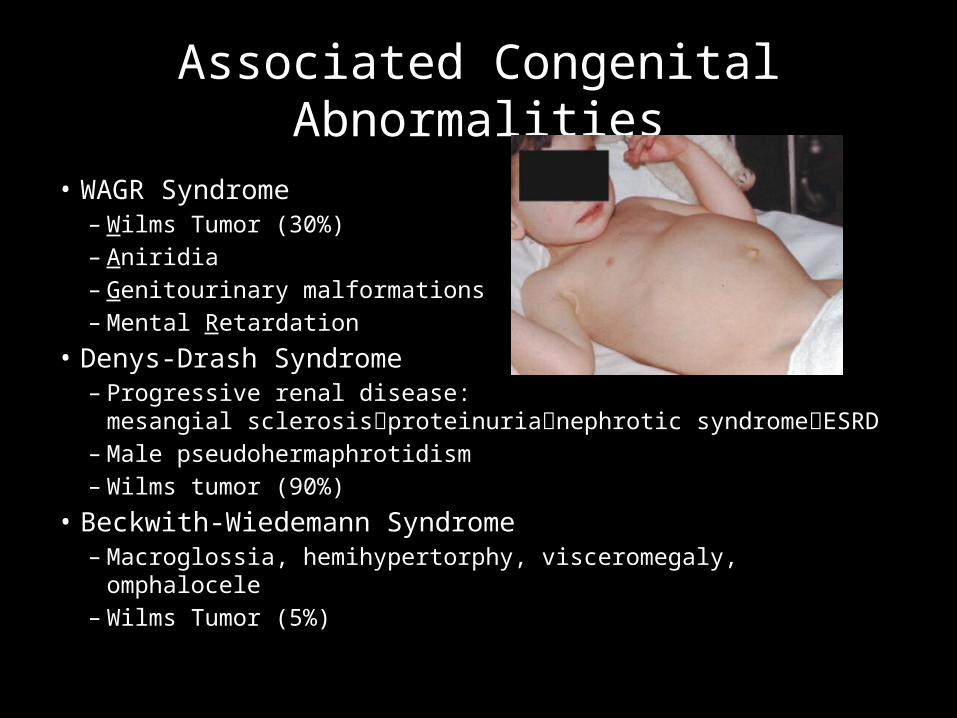
Associated Congenital Abnormalities
• WAGR Syndrome – Wilms Tumor (30%)– Aniridia– Genitourinary malformations– Mental Retardation
• Denys-Drash Syndrome– Progressive renal disease:
mesangial sclerosisproteinurianephrotic syndromeESRD– Male pseudohermaphrotidism– Wilms tumor (90%)
• Beckwith-Wiedemann Syndrome– Macroglossia, hemihypertorphy, visceromegaly, omphalocele– Wilms Tumor (5%)
• Majority of Wilms tumors are solitary.– 5-7% bilateral kidney involvement. – 10% multifocal loci within a kidney.
• Favorable histo contains 3 cell types– Blastemal (undifferentiated cells)– Stromal (immature spindle cells)– Epithelial cells (glomeruli and tubules)
• Unfavorable histo contains – anaplastic cells
Pathology
• Neuroblastoma• Clear cell sarcoma of kidney• Rhabdoid tumor of kidney• Congenital mesoblastic sarcoma of kidney• Renal medullary carcinoma
• Wilms v. Neuroblastoma: contrast enhanced CT• Wilms v. other renal cell tumors: histology
Differential Dx
• Tumor histology (increased anaplasia)• Tumor stage• Molecular and genetic markers
Prognostic factors
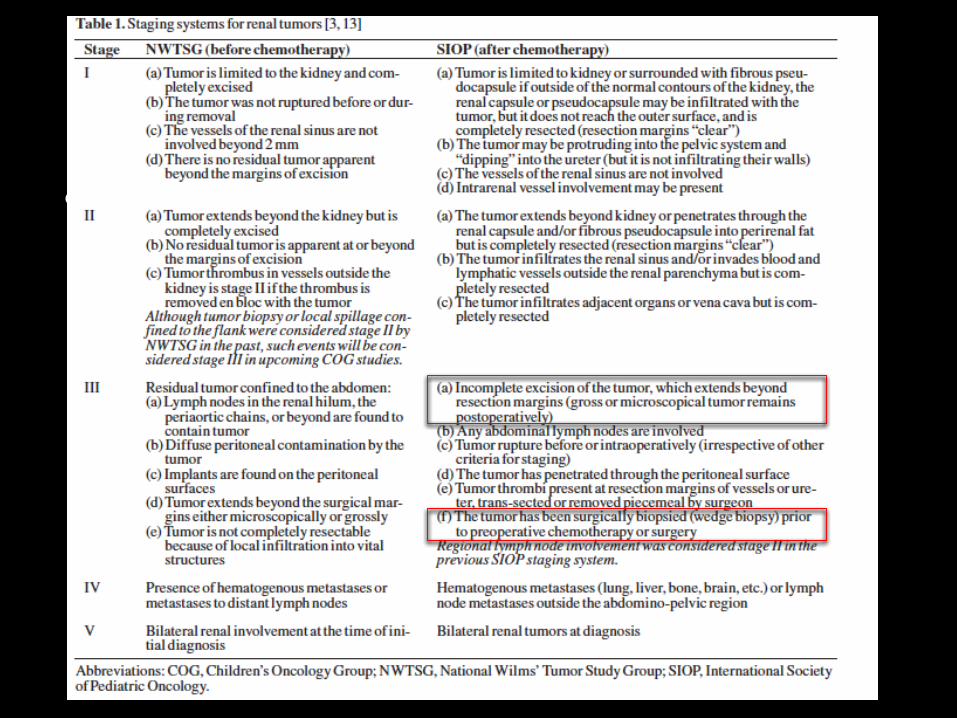
NWTSG vs SIOP• Two major approaches and therefore staging systems are
used
– National Wilms’ Tumor Study Group (NWTSG)• Surgery first approach • Staging is based off of surgical findings• Postoperative chemoradiation
– International Society of Pediatric Oncology (SIOP)• “Societe Internationale D'oncologie Pediatrique”• Staging after chemotherapy
• Ultimately, staging based on tumor extent
Combined Efforts
• Only 500 cases diagnosed annually• Single or small groups of institutions do
not provide enough patients to study• Investigators and institutions agreed to combine efforts• Goal was to get answers in a short period of time– Improve survival– Study long-term outcomes– Epidemiology and biology of the tumors
• Multimodal approach with varying physicians
• National Wilms’ Tumor Study Group– North American group, started in 1969 – 5 NWTSG trials to improve outcomes in Wilms’
patients– First four randomized, whereas last was used more
for biologic prognostic factors– More than 400 children entered in these studies
annually (70% of all Wilms’ cases in US)– In 2001, NWTS merged with other pediatric oncology
groups to create Children’s Oncology Group (COG)– Enrollment in NWTSG ended in 2002, now COG
NWTS
• #1: To determine effect of surgical technique• #2: Prognosis• #3: Reduce treatment for low-risk patients and
improve chemotherapy regimens • #4: Evaluate toxicity, efficacy, cost• #5: Identify biologic prognostic factors
NWTS
• NWTS #1 Conclusions: – Radiation not to be given in low risk Stage I diagnosis– Treatment combining two drugs more effective– Identified favorable/unfavorable histologic classifications
• NWTS #2 Conclusions: – Group I can be treated for 6 mo (instead of 15)– Adriamycin for stages II and III– Smaller babies can be treated with 50% reduction in CTx doses– Histology coincided with clinical outcome (favorable did better)– Updated staging- lymph nodes now increased to Stage III
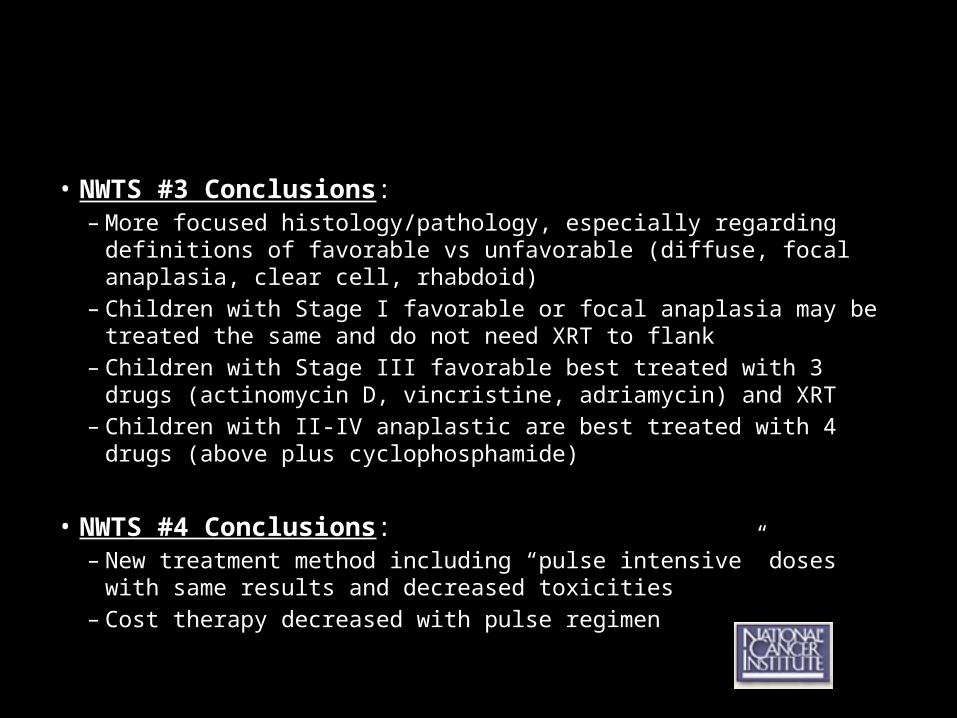
• NWTS #3 Conclusions:– More focused histology/pathology, especially regarding definitions of
favorable vs unfavorable (diffuse, focal anaplasia, clear cell, rhabdoid)– Children with Stage I favorable or focal anaplasia may be treated the same
and do not need XRT to flank– Children with Stage III favorable best treated with 3 drugs (actinomycin D,
vincristine, adriamycin) and XRT– Children with II-IV anaplastic are best treated with 4 drugs (above plus
cyclophosphamide)
• NWTS #4 Conclusions:– New treatment method including “pulse intensive” doses with same results
and decreased toxicities– Cost therapy decreased with pulse regimen
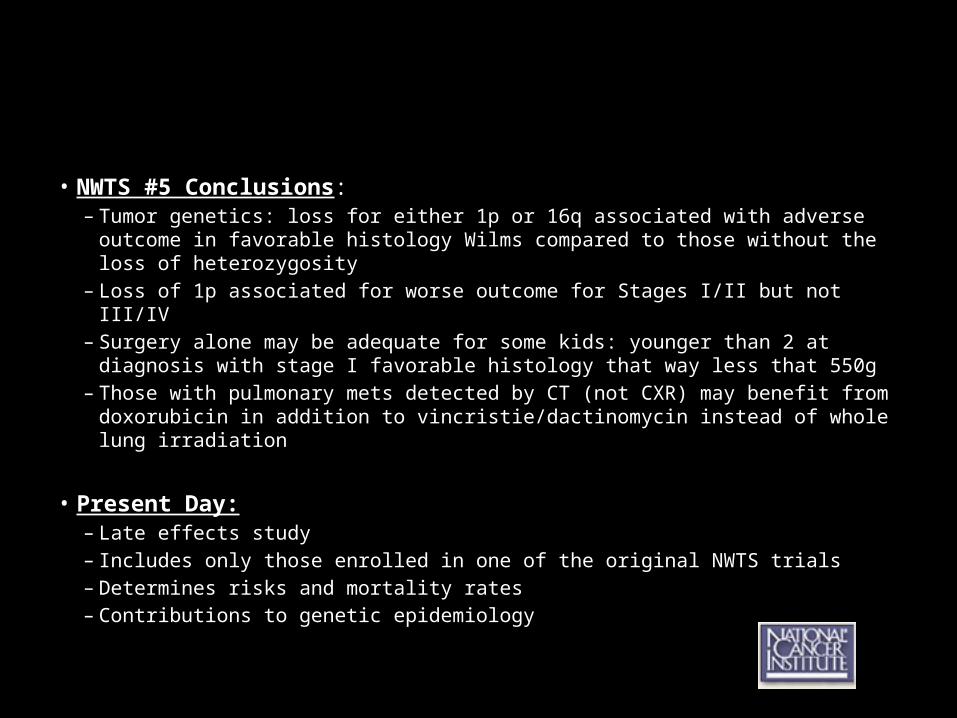
• NWTS #5 Conclusions:– Tumor genetics: loss for either 1p or 16q associated with adverse outcome in
favorable histology Wilms compared to those without the loss of heterozygosity– Loss of 1p associated for worse outcome for Stages I/II but not III/IV– Surgery alone may be adequate for some kids: younger than 2 at diagnosis with
stage I favorable histology that way less that 550g– Those with pulmonary mets detected by CT (not CXR) may benefit from
doxorubicin in addition to vincristie/dactinomycin instead of whole lung irradiation
• Present Day:– Late effects study– Includes only those enrolled in one of the original NWTS trials– Determines risks and mortality rates– Contributions to genetic epidemiology

SIOP• International Society of Pediatric Oncology• Strategy of giving preoperative therapy reduces risk of tumor rupture
during surgery reduce likelihood of local and distant recurrence• Succession of studies beginning in 1971 to determine optimal
preoperative therapy regimen
• UKCCSG completed randomized comparison of pre/post operative therapies in UKW3– Showed more favorable tumor stage distribution and signficant reduction in
overall burden of therapy and surgical complications in prenephrectomy chemotherapy
Metzger ML, Dome JS. Current therapy for Wilms’ tumor. Oncologist 2005; 10:815-26
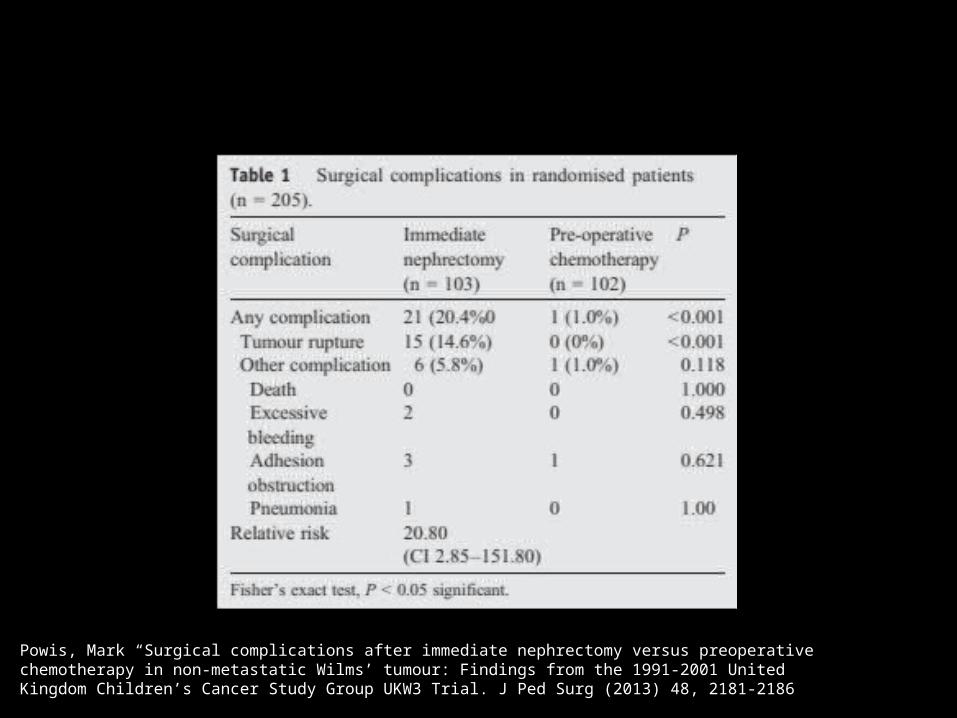
Powis, Mark “Surgical complications after immediate nephrectomy versus preoperative chemotherapy in non-metastatic Wilms’ tumour: Findings from the 1991-2001 United Kingdom Children’s Cancer Study Group UKW3 Trial. J Ped Surg (2013) 48, 2181-2186
Staging
• Based exclusively on anatomic extent of the tumor
• Staging is based on 1 of 2 systems:– NWTSG upfront surgery– SIOP upfront chemotherapy
• Both are valuable at predicting outcomes, but the difference in timing of nephrectomy limits stage-wise comparisons
• .
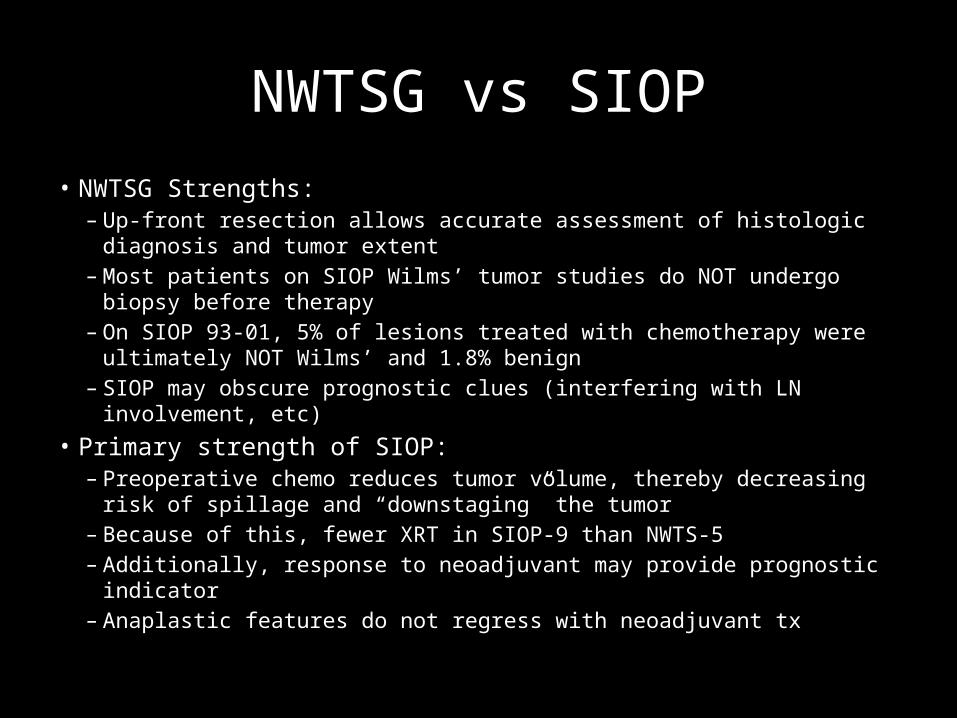
NWTSG vs SIOP• NWTSG Strengths:
– Up-front resection allows accurate assessment of histologic diagnosis and tumor extent
– Most patients on SIOP Wilms’ tumor studies do NOT undergo biopsy before therapy
– On SIOP 93-01, 5% of lesions treated with chemotherapy were ultimately NOT Wilms’ and 1.8% benign
– SIOP may obscure prognostic clues (interfering with LN involvement, etc)• Primary strength of SIOP:
– Preoperative chemo reduces tumor volume, thereby decreasing risk of spillage and “downstaging” the tumor
– Because of this, fewer XRT in SIOP-9 than NWTS-5– Additionally, response to neoadjuvant may provide prognostic indicator– Anaplastic features do not regress with neoadjuvant tx
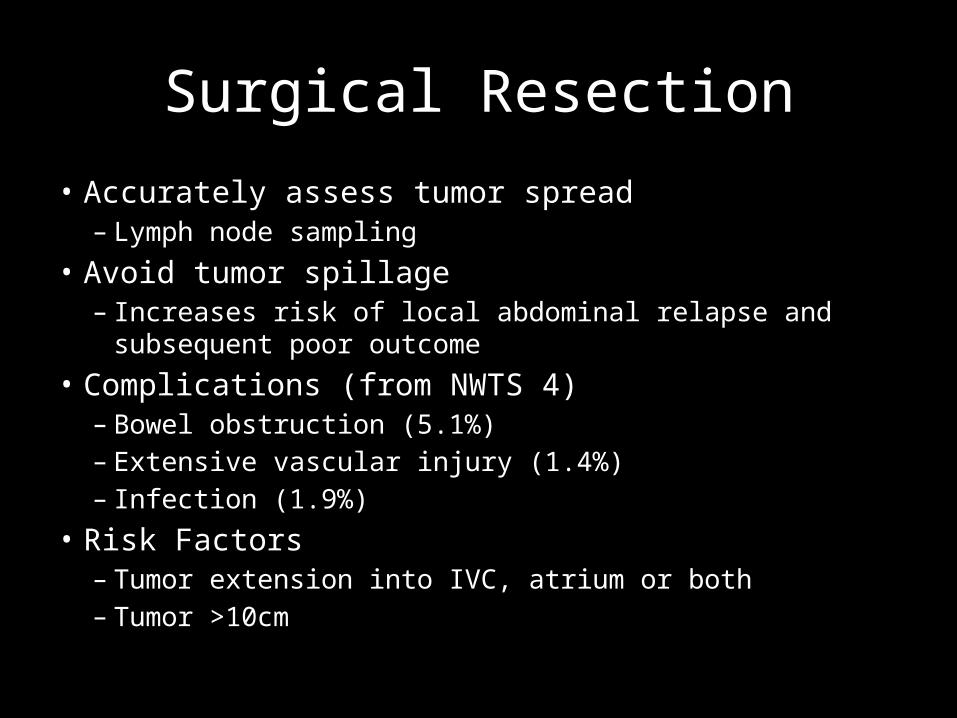
Surgical Resection
• Accurately assess tumor spread– Lymph node sampling
• Avoid tumor spillage– Increases risk of local abdominal relapse and subsequent poor
outcome• Complications (from NWTS 4)
– Bowel obstruction (5.1%)– Extensive vascular injury (1.4%)– Infection (1.9%)
• Risk Factors– Tumor extension into IVC, atrium or both– Tumor >10cm
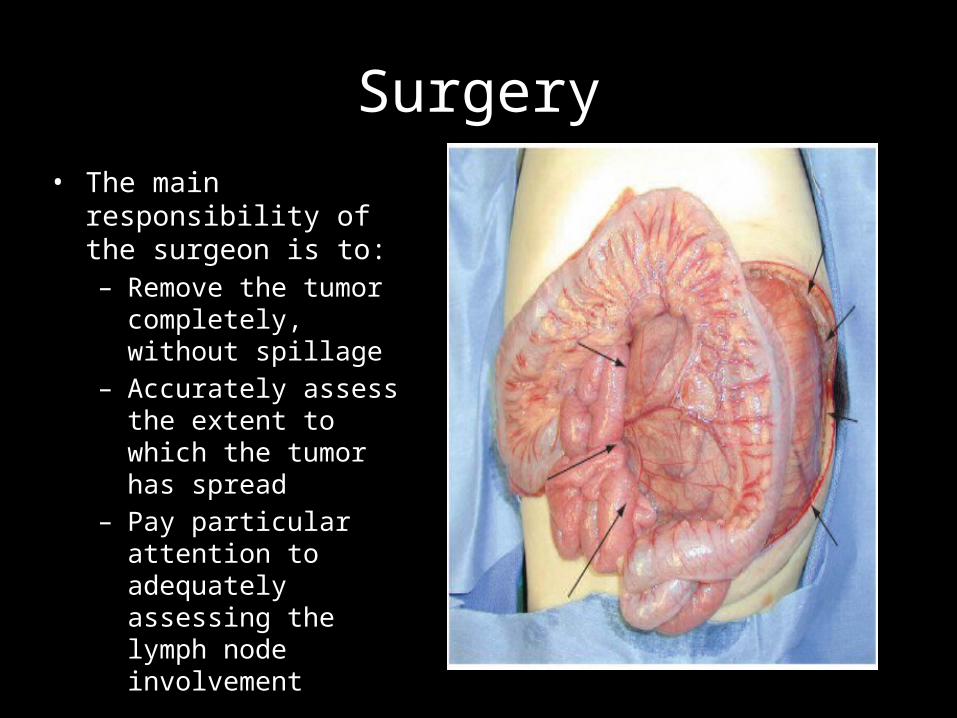
Surgery• The main responsibility of
the surgeon is to:– Remove the tumor
completely, without spillage
– Accurately assess the extent to which the tumor has spread
– Pay particular attention to adequately assessing the lymph node involvement
Who gets chemotherapy first?
• Solitary kidney• Tumor in a horseshoe kidney• Bilateral Wilms’ tumors• Tumors with IVC and intra-atrial involvement• Patients with massive tumors considered to be
unresectable by operating surgeon• Respiratory distress from extensive pulmonary
metastasis• Size of tumor alone is NOT an indication for preop
chemoradiation therapyShamberger RC. Pediatric renal tumors. Semin Surg Oncol 1999; 16:105-120
• D'angio GJ, Evans A, Breslow N, et al. The treatment of Wilms' tumor: results of the Second National Wilms' Tumor Study. Cancer. 1981;47(9):2302-11.
• Green DM, Breslow NE, Beckwith JB, et al. Effect of duration of treatment on treatment outcome and cost of treatment for Wilms' tumor: a report from the National Wilms' Tumor Study Group. J Clin Oncol. 1998;16(12):3744-51.
• Grovas A, Fremgen A, Rauck A, et al. The National Cancer Data Base report on patterns of childhood cancers in the United States. Cancer. 1997;80(12):2321-32.
• Kalapurakal JA, Dome JS, Perlman EJ, et al. Management of Wilms' tumour: current practice and future goals. Lancet Oncol. 2004;5(1):37-46.
• Perlman EJ. Pediatric renal tumors: practical updates for the pathologist. Pediatr Dev Pathol. 2005;8(3):320-38.• Zuppan CW, Beckwith JB, Luckey DW. Anaplasia in unilateral Wilms' tumor: a report from the National Wilms'
Tumor Study Pathology Center. Hum Pathol. 1988;19(10):1199-209.• Shamberger RC. Pediatric renal tumors. Semin Surg Oncol 1999; 16:105-120• Wilimas JA, Magill L, Parham DM et al. Is renal salvage feasible in unilateral Wilms’ tumor? Proposed
computed tomographic criteria and their relation to surgicopathologic functions. Am J Pediatr Hematol Oncol 1990; 12:164-167
• Ladd WE. Embyroma of the kidney (Wilms’ tumor). Ann Surg 1938; 108: 885-902• Shamberger RC, Guthrie KA, Rictchey ML et al. Surgery-related factors and local recurrence of Wilms’ tumor in
National Wilms’ Tumor Study 4. Ann Surg 1999; 220:292-297• Metzger ML, Dome JS. Current therapy for Wilms’ tumor. Oncologist 2005; 10:815-26
Resources