Embed Size (px)
Citation preview
Interdisciplinary Staff Education for COPD
Using Standardized Patient Education
Kathy Calandra, RN, BSN, CPHQ Healthcentric Advisors
Jennifer Cellar, CNP, Medical Associates of RI/St. Elizabeth Manor
Mary Biello, RN, BSN VNA of Rhode Island
This material was prepared by the New England QIN-QIO, the Medicare Quality Innovation Network-Quality Improvement Organization for New England, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. CMSRI_C3-1_052716_0576
Outline
Greater Providence Community Coalition’s Selection of A Safe Transitions Initiative
Developing Tools and Training
Measures, Data and Results
Spread
2
The Community Coalition
3

The Community Coalition
4
Greater
Providence
Community
Coalition

The Community Coalition
Greater Providence Community Coalition
• Background, state of coalition August 2014
• Kick Off 11th SOW
• Annual survey
5
The Community Coalition
Selection of First Initiative
• Discussed ways to increase attendance
• Disease focus
• Heart Failure (HF) Initiative 2013 – a
model
6
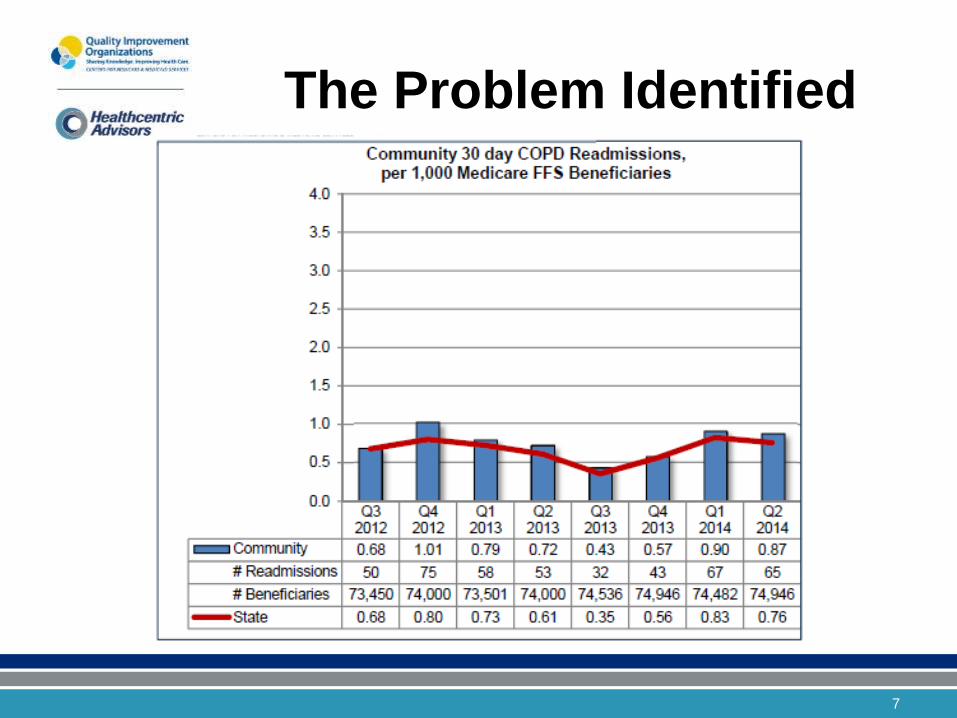
The Problem Identified
7
The Problem Identified
• Goal established by coalition chairs:
– Provide consistent, standardized messaging
to patients across care settings
• Proved to be the ticket to increased coalition engagement!
8
Available Knowledge
• IRB approved HF study 2013 showed significant reductions in readmissions
• Literature Search
– Success with proper patient self management
– Whole system approach key
– Use of Zone Tools/Action Plans
9

Developing the
Tools & Training
10

Selection of Patient
Teaching Tools • Reviewed available tools in use by multiple
providers
• Lung Talk Books and Videos
• UCONN Health
• Implementation
11
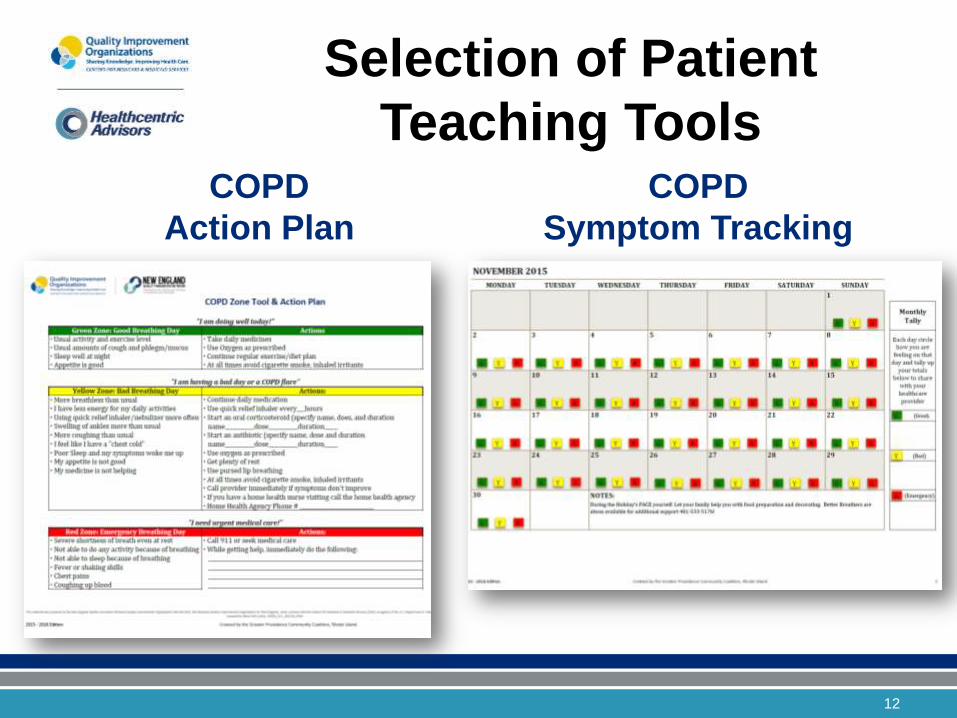
Selection of Patient
Teaching Tools COPD
Action Plan
COPD
Symptom Tracking
12
Support for Selection of
Teaching Tools
Pulmonologist Office supported the choice
American Lung Association
Better Breathers Support Group
13

Train-the-Trainer Program
Development • Survey to gauge interest and gain commitment
• Champions
– Ensure program adaptable to various settings
and staff
– Feasibility
14
Train-the-Trainer Program
Development
15
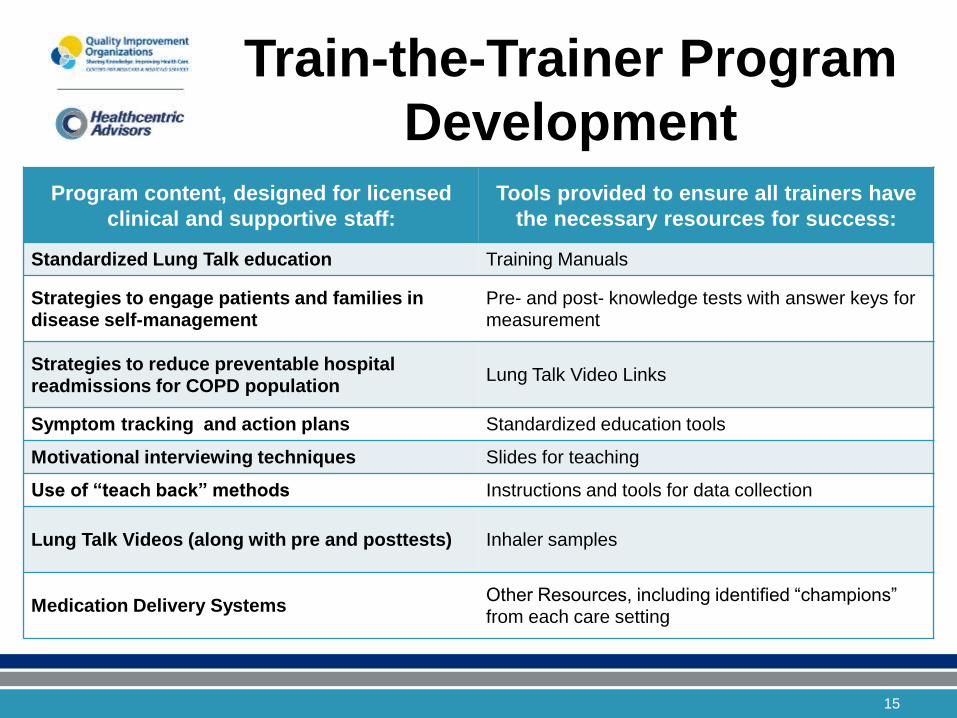
Program content, designed for licensed
clinical and supportive staff:
Tools provided to ensure all trainers have
the necessary resources for success:
Standardized Lung Talk education Training Manuals
Strategies to engage patients and families in disease self-management
Pre- and post- knowledge tests with answer keys for measurement
Strategies to reduce preventable hospital readmissions for COPD population
Lung Talk Video Links
Symptom tracking and action plans Standardized education tools
Motivational interviewing techniques Slides for teaching
Use of “teach back” methods Instructions and tools for data collection
Lung Talk Videos (along with pre and posttests) Inhaler samples
Medication Delivery Systems Other Resources, including identified “champions” from each care setting
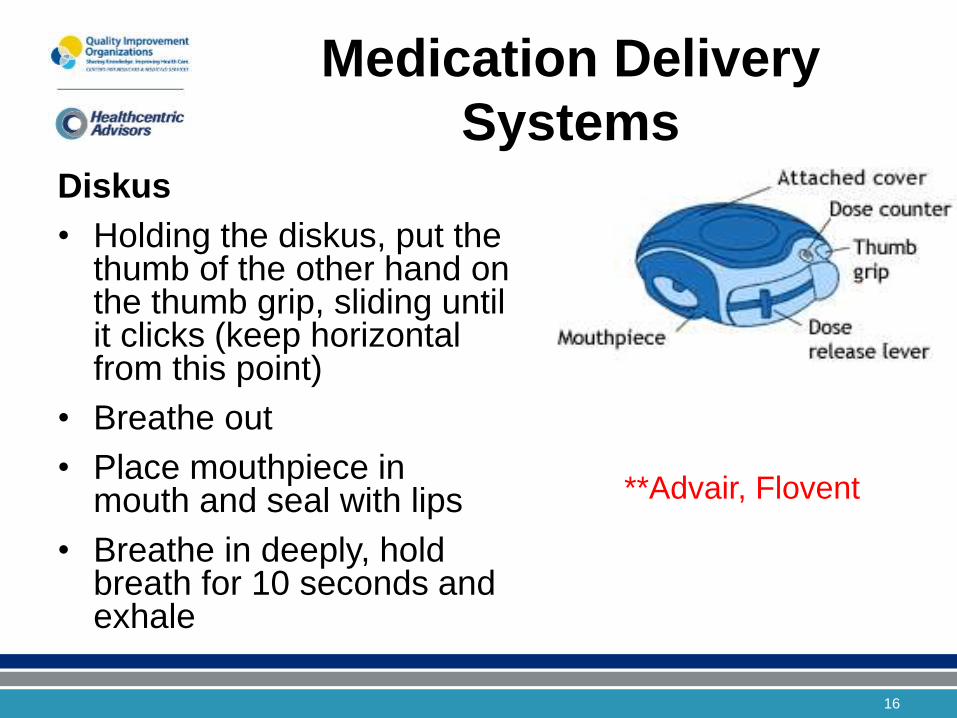
Medication Delivery
Systems Diskus
• Holding the diskus, put the thumb of the other hand on the thumb grip, sliding until it clicks (keep horizontal from this point)
• Breathe out
• Place mouthpiece in mouth and seal with lips
• Breathe in deeply, hold breath for 10 seconds and exhale
**Advair, Flovent
16
Measures, Data & Results
17
Measures and Ensuring
Data Collection
• Commitment included responsibility for data collection
• Simple tools were developed and were included in the content of the Train-the-Trainer Program
• Data collection reinforced at all coalition meetings
• Incentive to receive additional materials
18
Measures and Ensuring
Data Collection • For Staff – Proximal Outcome Measures:
– Rate of staff training towards goal
• Total # of staff trained across all participating organizations/Total # of staff identified as appropriate for training
– Outcome of training
• Rate of improvement pre and post test results
19
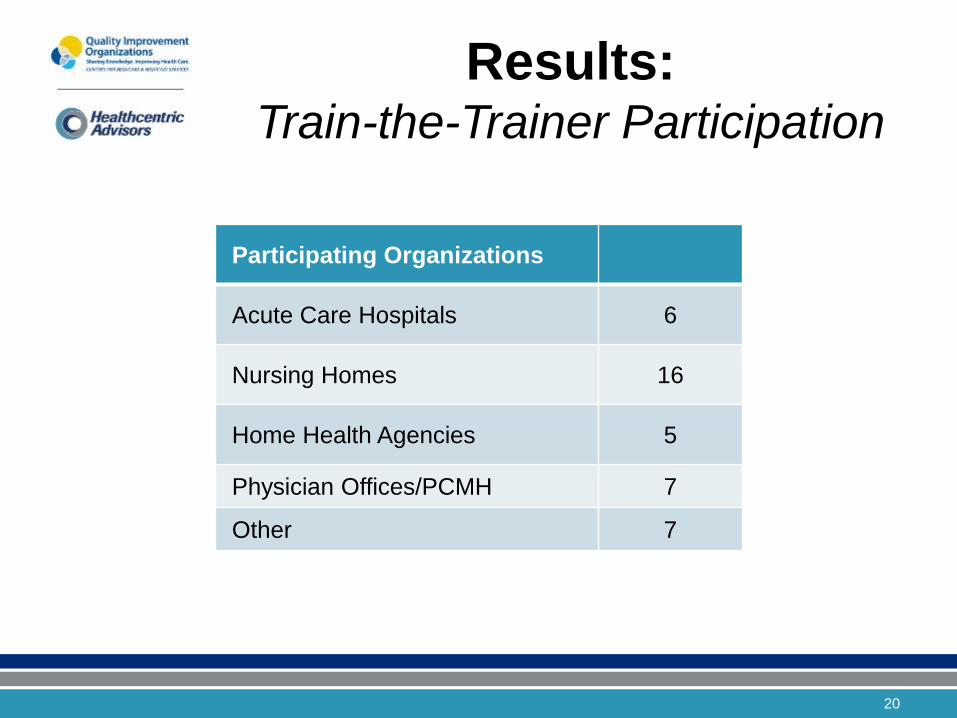
Results: Train-the-Trainer Participation
Participating Organizations
Acute Care Hospitals 6
Nursing Homes 16
Home Health Agencies 5
Physician Offices/PCMH 7
Other 7
20
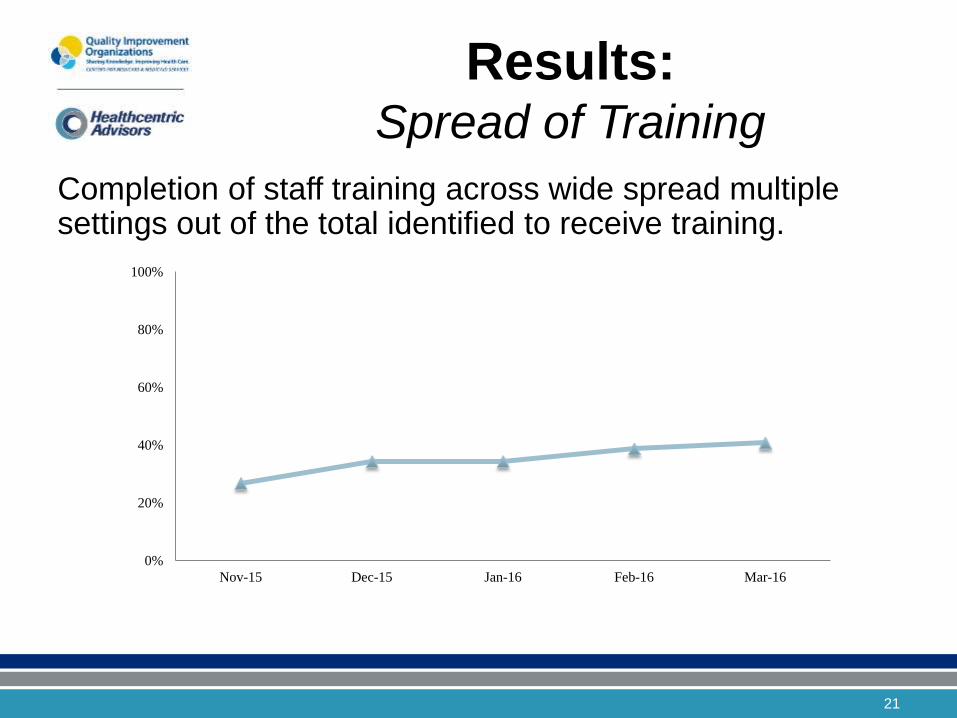
Results: Spread of Training
Completion of staff training across wide spread multiple settings out of the total identified to receive training.
0%
20%
40%
60%
80%
100%
Nov-15 Dec-15 Jan-16 Feb-16 Mar-16
21
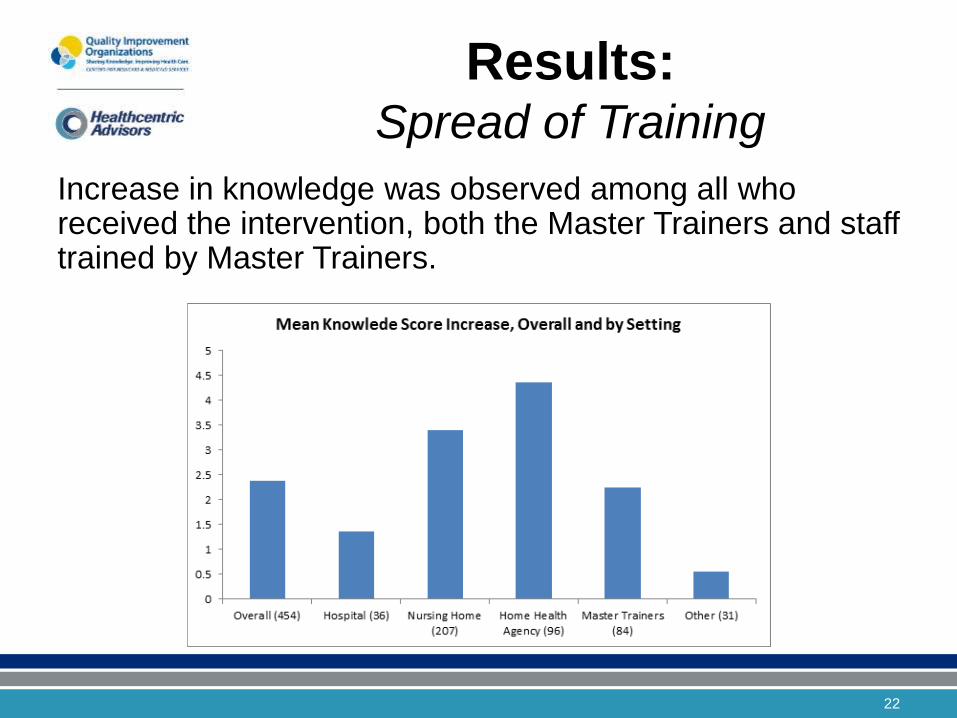
Results: Spread of Training
Increase in knowledge was observed among all who received the intervention, both the Master Trainers and staff trained by Master Trainers.
22

Results: Impact on Patients
• Limitation of Initiative
– No proximal outcome data for patient outcomes
– CMS Claims Data to calculate COPD readmissions rates is 6 months behind
• Rhode Island Hospital’s contribution
23
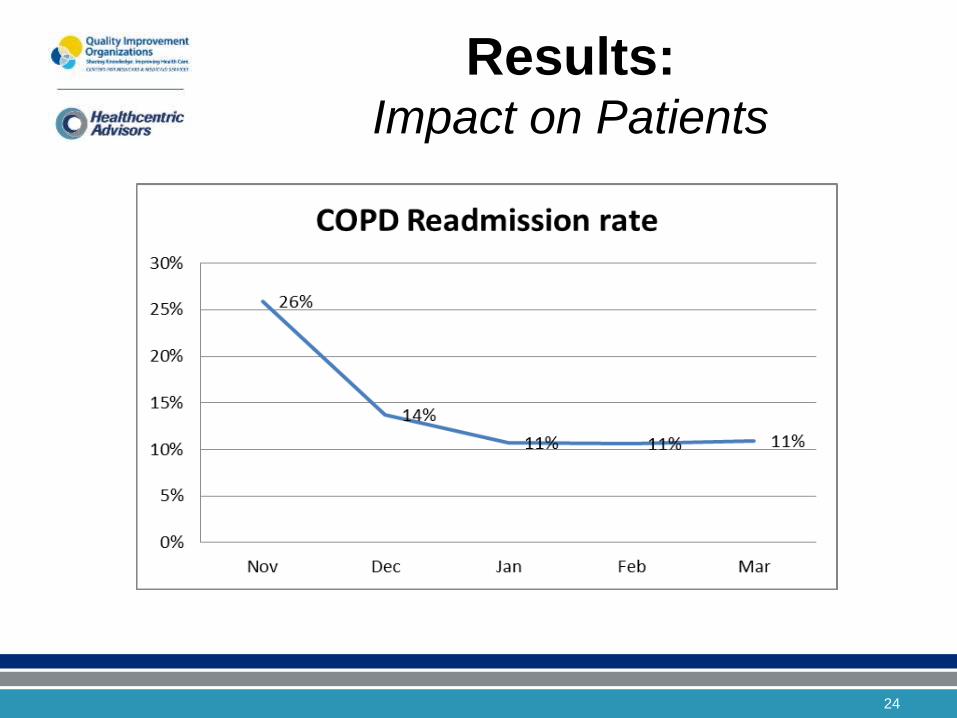
Results: Impact on Patients
24
Spreading the Program
Across Rhode Island
25
Phase II of Initiative: Plan-Do-Study-Act (PDSA)
• Survey to participants 3 months after implementation
• Meeting with small group of Master Trainers to plan improvements
– Strengths identified:
• Training manual had everything they needed for staff trainings
• Lung Talk Books and Video Links useful for teaching staff, easy to explain
• COPD Zones and Action Plan tool easy to explain
• Inhaler samples very useful
26
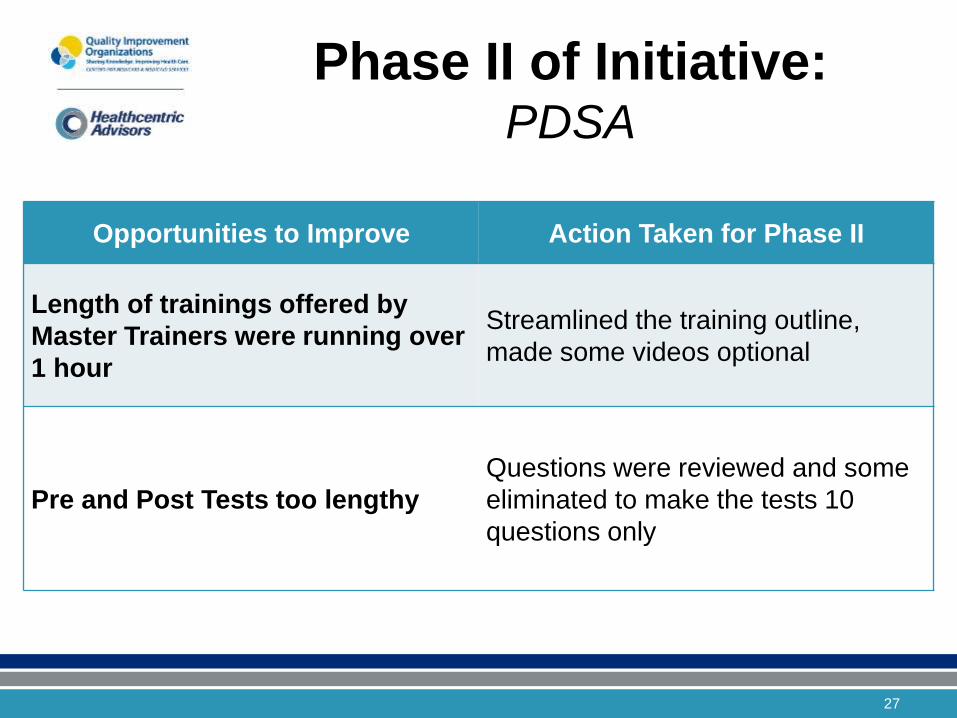
Phase II of Initiative: PDSA
27
Opportunities to Improve Action Taken for Phase II
Length of trainings offered by
Master Trainers were running over
1 hour
Streamlined the training outline,
made some videos optional
Pre and Post Tests too lengthy
Questions were reviewed and some
eliminated to make the tests 10
questions only
Phase II of Initiative: PDSA
• Reported on Progress of the Greater Providence Coalition’s COPD Initiative at all 4 coalitions’ meetings
• External presentations on progress at stakeholder meetings (Lifespan, BCBSRI)
• Checked state-wide interest in Phase II Train-the-Trainer Program with survey
• 3 Train-the-Trainer Sessions April 27th -May 3rd
28

Summary of
Spread of Initiative • 62 participants at Train-the-Trainer in April/May
• 29 organizations added
• Total “Master Trainers” around the state =137
• Total participating organizations = 70
29

Key Findings and
Strengths • Development and implementation of a
community wide, standardized COPD education for patients is a realistic means to provide COPD self-management education across settings of care.
• Train-the-Trainer participants and their trained staff increased their COPD knowledge through the program
30

Key Findings and
Strengths, continued • Community buy in and collaboration
• Materials & Resources adopted by many providers
• Commitment to Collecting Data to measure and to be a part of the outcomes
• Behavioral Health spread
31

Key Findings and
Strengths, continued
And finally – the initiative addressed the Gap:
Patients overwhelmed with various
resources in multiple settings now can
receive standardized messaging and tools.
32
Success Made Possible
by... • Train-the-Trainer developers and presenters
from Leadership of our Coalitions
• Our sponsors
• Our coalition participants committed to the triple aim
33
Questions?
34

Contact our Team
This initiative is being submitted as a SQUIRE to CMS. References available.
• For further information, contact:
Kathy Calandra - Healthcentric Advisors Safe Transitions Lead for RI
Jennifer Cellar, CNP - Medical Associates of RI/St. Elizabeth Manor
Mary Biello - Clinical Liaison VNA of Rhode Island
35
View the tools on our website:
www.healthcarefornewengland.org/event/in-person-event-all-ri-community-coalitions-copd-train-the-trainer-sessions/