Embed Size (px)
Citation preview

P
Tiplpt
PC2
Int. J. Radiation Oncology Biol. Phys., Vol. 61, No. 2, pp. 570–582, 2005Copyright © 2005 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/05/$–see front matter
doi:10.1016/j.ijrobp.2004.09.022
HYSICS CONTRIBUTION
INTERACTIVELY EXPLORING OPTIMIZED TREATMENT PLANS
ISAAC ROSEN, PH.D.,* H. HELEN LIU, PH.D.,*NATHAN CHILDRESS, PH.D.,* AND ZHONGXING LIAO, M.D.†
*Departments of Radiation Physics and †Radiation Oncology, The University of Texas M. D. Anderson Cancer Center,Houston, TX
Purpose: A new paradigm for treatment planning is proposed that embodies the concept of interactivelyexploring the space of optimized plans. In this approach, treatment planning ignores the details of individualplans and instead presents the physician with clinical summaries of sets of solutions to well-defined clinical goalsin which every solution has been optimized in advance by computer algorithms.Methods and Materials: Before interactive planning, sets of optimized plans are created for a variety of treatmentdelivery options and critical structure dose–volume constraints. Then, the dose–volume parameters of theoptimized plans are fit to linear functions. These linear functions are used to show in real time how the targetdose–volume histogram (DVH) changes as the DVHs of the critical structures are changed interactively. Abitmap of the space of optimized plans is used to restrict the feasible solutions. The physician selects the criticalstructure dose–volume constraints that give the desired dose to the planning target volume (PTV) and then thoseconstraints are used to create the corresponding optimized plan.Results: The method is demonstrated using prototype software, Treatment Plan Explorer (TPEx), and a clinicalexample of a patient with a tumor in the right lung. For this example, the delivery options included 4 open beams,12 open beams, 4 wedged beams, and 12 wedged beams. Beam directions and relative weights were optimized fora range of critical structure dose–volume constraints for the lungs and esophagus. Cord dose was restricted to45 Gy. Using the interactive interface, the physician explored how the tumor dose changed as critical structuredose–volume constraints were tightened or relaxed and selected the best compromise for each delivery option.The corresponding treatment plans were calculated and compared with the linear parameterization presented tothe physician in TPEx. The linear fits were best for the maximum PTV dose and worst for the minimum PTVdose. Based on the root-mean-square error between the fit values and their corresponding data values, the linearfit appears to be adequate, although higher order polynomials could give better results. Some of the variance infit is due to the stochastic nature of the simulated annealing optimization algorithm, which does not reproducethe exact same results in repetitions of the same calculation. Using a directed search algorithm for planoptimization should produce better parameter fits and, therefore, better predictions of plan characteristics byTPEx.Conclusions: Using TPEx, the physician can easily select the optimum plan for a patient, with no imposed arbitrarydefinition of the “best” plan. More importantly, the physician can readily see what can be achieved for the patient witha given delivery technique. There is no more uncertainty about whether or not a better plan exists. By comparing the“best” plans for different delivery options (e.g., three-dimensional conformal radiotherapy versus intensity-modulatedradiation therapy), the physician can gauge the clinical benefits of greater technical complexity. However, before theTPEx process can be clinical useful, faster computers and/or algorithms are needed and more studies are needed tobetter model the spaces of optimized solutions. © 2005 Elsevier Inc.
Radiation therapy treatment planning, Inverse planning, Treatment plan optimization.
1d
optwc
M
INTRODUCTION
he goal of treatment planning, whether forward-based ornverse-based, is to find the best plan for the individualatient. A major difficulty in accomplishing that goal is theack of universally accepted criteria for defining the “best”lan. Clearly, more dose to the tumor is better and less doseo the normal tissues is better. However, the ideal plan of
Reprint requests to: Isaac Rosen, Ph.D., Department of Radiationhysics, Unit 94, The University of Texas M. D. Anderson Cancerenter, 1515 Holcombe Blvd, Houston, TX 77030; Tel: (713) 563-
635; Fax: (713) 563-2629; E-mail: [email protected] A570
00% prescribed dose to the entire tumor volume and zeroose elsewhere is not attainable.In evaluating any given treatment plan, the radiation
ncologist is faced with a variety of issues and choices. Therimary question is whether a dose can be delivered to theumor that will achieve a high probability of local controlithout serious treatment morbidity or sequelae. If that goal
an be achieved, then the focus shifts to whether treatment
Support in part by a sponsored research agreement from Philipsedical Systems.Received Jun 8, 2004, and in revised form Sep 15, 2004.
ccepted for publication Sep 17, 2004.

mddbtteopm
mttbsfchnBmtrp
tutbemldoumitomdorqmnt
toa2wtmc
otdetap
iipbirtatmoptfiu
aplarmgboottmoacAtnl
pbdvGcdrdq
571Exploring optimized plans ● I. ROSEN et al.
orbidity can be further reduced (i.e., can normal tissueoses be lowered?). When there is a desire to escalate tumoroses because local control is not adequate, the questionecomes one of finding the best compromise between po-ential complications and potential recurrence. The answerso these questions depend on the details of treatment deliv-ry. In general, more complex treatments with more degreesf freedom in beam geometry and fluence produce betterlans with greater separation between tumor dose and nor-al tissue doses.In designing the best plan for a patient, the physicianust often compromise between the prescribed tumor dose,
he uniformity of dose in the tumor volume, and the doseso critical structures. Further compromises may be requiredetween the different adverse reactions of different criticaltructures. Unfortunately, the probabilities of complicationsor an individual patient are not binary functions and noturrently predictable. The physician must try to anticipateow the patient will respond to the planned dosage and mayeed to compromise tumor dose to manage the toxicity.ecause different physicians may choose different compro-ises based on their training and clinical experience and
heir understanding of the patient’s unique situation, theesults of treatment planning vary with physician and withatient.If it were possible to mathematically define the charac-
eristics of the best plan, then computer programs couldnerringly find it for each patient. Attempts to accomplishhis go back more than 35 years, and there is an extensiveody of literature exploring the use of algorithms such asxhaustive search, linear programming, quadratic program-ing, mixed-integer programming, gradient search, simu-
ated annealing, genetic algorithms, feasibility search,ownhill simplex, and neural networks (e.g., 1–22). In the-ry, inverse planning (or treatment plan optimization, as itsed to be called) could provide the unequivocal best treat-ent plan for a patient if the biologic responses of the
ndividual patient’s tissues could be accurately modeled andhe clinical compromises acceptable to the clinician werebjectively and unambiguously known. Although mathe-atical models of tumor and tissue response have been
eveloped, they are not yet accurate enough for predictionf individual patient responses and clinician decision crite-ia are not well simulated by computer algorithms. Conse-uently, inverse planning is still an iterative process. Aajor improvement of inverse planning over forward plan-
ing is the focus on clinical factors, such as normal tissueolerances, rather than on the details of beam geometries.
The existence of multiple competing objectives in thereatment planning problem has led to approaches that focusn the relationships between these objectives rather thanttempting to define a mathematically “best” solution (e.g.,3–28). In general, these methods compute multiple plansith different optimization criteria to find the boundary of
he space of optimized (Pareto) or feasible solutions. Theyay use sensitivity analysis to show how much tumor dose
an be increased for a given increase in normal tissue dose t
r may directly optimize the weighting factors assigned tohe different objectives. The new treatment planning para-igm presented here follows this general approach andxtends it by using the optimization criteria directly, ratherhan through surrogate preference factors, and by providingreal-time interactive interface into the space of optimizedlans.It is worthwhile to ask why treatment planning is an
terative process. The clinician presumably knows what thedeal (or acceptable) dose distribution should look like. Thehysicist or dosimetrist generates a plan that he or sheelieves is the closest approximation to what the clinician’sdeal plan is. Why should there be any iterations? Oneeason may be that the planner has not correctly anticipatedhe physician’s goals and compromise preferences. For ex-mple, the planner might have chosen to spare equal por-ions of each kidney, whereas the physician’s preferenceight be to sacrifice one kidney and completely spare the
ther. Another reason for multiple iterations may be that thehysician implicitly believes that a better plan exists andhat through more effort (and perhaps experience) it can beound. In either case, the physician is faced with a processn which the characteristics of the best achievable plan arenknown.The dilemma facing the physician can be described with
simple example. Consider a patient with a lung tumor. Thelanner generates a conventional beam arrangement usingarge anteroposterior beams for an initial dose followed byboost dose delivered with parallel-opposed oblique beams
educed in size to the primary target volume. The physicianust balance the doses to the tumor, lungs, heart, esopha-
us, and spinal cord. Changing the angles of the obliqueeams will change this balance, as will adding more beamsr fluence modulation. Presumably, the planner has alreadyptimized the directions of the oblique beams either throughrial and error or previous experience. However, based onhe single plan presented, the physician cannot know howuch improvement can be achieved by adding more beams
r adding fluence modulation. Therefore, the physician maysk for additional plans to assess the benefits of thesehanges versus the added complexity of treatment delivery.s fluence modulation or beams are added, the optimality of
he beam directions is thrown into question. The physiciano longer knows how good a plan can be achieved or whatevel of complexity is needed to achieve the clinical goals.
The information that the physician needs to make the bestossible treatment planning decision for a given patient cane encapsulated in the question, “What is the greatest tumorose that can be delivered for specified normal tissue dose–olume constraints, regardless of the beam characteristics?”iven this information in an interactive format, the physi-
ian can readily select the plan that delivers the most tumorose with acceptable normal tissue risk or the one that mosteduces the dose to selected organs while maintaining aesired tumor dose level. The answer to this question re-uires that the best possible (optimized) dose–volume his-
ogram (DVH) for the planning target volume (PTV) be
pt
tsnbpficpttsdodippa
dtmtamtsmauTpfi
fisaoTt
Frbwa9ml2wac
S
gebtosawTvuptstwbwwi
I
Fmttbuccvm
(tsrdaBad
ppnprpcb
wsptw
572 I. J. Radiation Oncology ● Biology ● Physics Volume 61, Number 2, 2005
resented to the physician for every combination of normalissue DVHs that they might want to select.
We are studying a new paradigm for treatment planninghat embodies this concept of interactively exploring thepace of optimized plans. As with some other inverse plan-ing techniques, the details of treatment delivery (such aseam weights, angles, and doses) are hidden. Instead, thehysician is presented with the relevant clinical summariesor the best possible solutions to well-defined clinical goalsn which every solution has been optimized in advance byomputer algorithms. Using an interactive interface, thehysician selects a general treatment delivery method andhen explores in real time how the maximum deliverableumor dose changes as critical structure dose–volume con-traints are tightened or relaxed. The physician can thenirectly select the compromises between doses to the vari-us organs, dose to the tumor, and complexity of treatmentelivery that he or she desires for the patient with nomposed arbitrary definition of the “best” plan. More im-ortantly, the physician can see what is achievable for theatient. There is no more uncertainty about whether or notbetter plan exists.
METHODS AND MATERIALS
A prototype system named Treatment Plan Explorer (TPEx) waseveloped using MATLAB (The MathWorks Inc., Natick, MA) toest this approach to treatment planning. It imports a set of opti-ized treatment plans, parameterizes their dose–volume charac-
eristics, and then presents the results to the physician or planner inn interactive format. Before using TPEx, multiple sets of opti-ized plans are created, each of which covers the range of poten-
ially desirable normal tissue DVH constraints. Each set corre-ponds to a different treatment delivery technique that the useray wish to explore. TPEx does not include external beam radi-
tion treatment planning (RTP) software. The optimized planssed by TPEx are created by the RTP software. The output ofPEx is a set of critical structure DVH constraints selected by thelanner, which are then used by the RTP software to create thenal optimized plan for the patient.Treatment Plan Explorer has two user interface screens. In the
rst, the planner chooses the basic plan parameters and the criticaltructures to be considered. In the second, the planner interactivelydjusts the dose–volume constraints on the critical structures andbserves the effects on the DVH of the PTV. During exploration,PEx continuously displays the values of the user parameters and
he resulting PTV parameters.The use of TPEx is demonstrated using a clinical example.
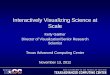
igure 1 shows three sections through a patient with a tumor in theight lung treated using three coplanar 6-MV beams. The anterioream included a 30° wedge and the posterior beam included a 45°edge. The right posterior-oblique beam included a 15° wedge
nd partial blocking. The dose distribution delivered 63 Gy to the5% isodose line. The DVH of the treatment is also shown. Theaximum dose to the spinal cord was 45.5 Gy; the volume of right
ung exceeding 20 Gy was 59%; the volume of left lung exceeding0 Gy was 19%; and the volume of esophagus exceeding 50 Gyas 21%. Because most of the PTV was superior to the heart, onlysmall volume of heart (10%) received more than 45 Gy from the
oplanar beam arrangement. c
election of plan parametersOne goal of TPEx is to avoid dealing with the details of beam
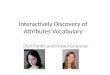
eometry. The first user screen (Fig. 2) asks for only three param-ters to define the treatment delivery—the beam energy, the num-er of beams, and the degree of fluence modulation. Based onhese selections, the program reads a set of previously computedptimized plans. It then presents the user with choices of criticaltructures to manipulate during exploration and the correspondingvailable decision doses. The decision doses are dose levels athich the physician would like to control the irradiated volume.ypically, these would be dose levels at which the irradiatedolume is predictive of complications. The choices available to theser are limited to those for which optimized sets of plans werereviously generated. Therefore, the planner should consult withhe physician before beginning the optimization phase or haveufficient experience to anticipate the physician’s general approacho treatment for the given anatomic site. The planner should knowhat decision doses the physician uses in evaluating plans, whateam energies are preferred, and how much treatment complexityill probably be needed to accomplish the clinical goals. In thatay, the planner can choose the best set of plans to be optimized
n preparation for treatment plan exploration.
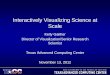
nteractive explorationThe interactive exploration of optimized solutions is shown in
ig. 3. The upper graph is a simplified DVH for the PTV showinginimum dose, 95% volume dose, and maximum dose. The bot-
om graphs are simple DVHs for the critical structures selected inhe previous input screen. Each critical structure DVH is definedy one or two control points that are individually movable by theser. The maximum dose control points can only move laterally,hanging dose but not volume. The decision dose control pointsan only move vertically, changing volume but not decision dosealue. For each point, a red bar shows the range of permissibleotion.As the planner changes the value of one of the control points
the “active” control point), two things happen in real time. First,he DVH of the PTV changes to reflect the best plan that corre-ponds to the current settings of all the control points. Second, theed bars showing the ranges of motion of the control points changeynamically, including the range for the active control point. Thective control point is not allowed to move outside of its range.ecause of the complexity of the space of optimized plans, therere strong interactions between the control points and there may beiscontinuities in the space.It is possible that the range of motion of a nonactive control
oint may change in such a way that the corresponding controloint is no longer within its range. That situation represents aonfeasible solution and should not be selected. When that controloint is activated, it is automatically relocated to a value within itsange. If a situation arises in which the maximum dose controloint is reduced to the decision dose value, then the volumeorresponding to the decision dose is automatically reduced to 0%ecause the decision dose is now also the maximum dose.The planner should explore all of the control points in various
ays and sequences to find the set of DVHs (PTV and criticaltructures) that is most desirable. Just as in conventional treatmentlanning, lower doses to the critical structures result in lower doseso the PTV. However, by observing the changes in the PTV DVHith changes in the control points, it is easy to see how much each
ritical structure limits the PTV dose and how much sparing of

easbs
samtowotttt
C
PNPw(
Fpntpm
573Exploring optimized plans ● I. ROSEN et al.
ach critical structure can be achieved for a given PTV dose. Inddition, the simultaneous changes in the magnitude of the pre-cription dose and the degree of dose homogeneity in the PTV cane observed in response to alterations in critical structure con-traint values.
After a set of control point values is chosen, those criticaltructure constraints are used as input to the RTP software to createn optimized plan with the beam characteristics (energy, number,odulation) chosen by the user at the start of the process. Because
he user is interrogating a parameterization of the original data setf optimized plans and also interpolating, the actual plan achievedill not exactly match the results of TPEx. How closely the resultsf TPEx will match the results of RTP software optimization withhe desired control point constraints depends on several factors—he density of data in the space of optimized plans, the optimiza-ion algorithm, and the quality of the function fitting. These rela-ionships have not yet been explored.
reation of optimized plan setsThe patient treatment was originally planned using
innacle3 (Philips Radiation Oncology Systems, Madison, WI).ormal tissue and tumor volume structures were extracted frominnacle3 and imported into a research planning system, Plan3D,hich uses a modified Clarkson scatter-air ratio dose calculation
Fig. 1. Transverse, sagittal, and coronal sections throughwith three coplanar 6-MV beams. The anterior beam incluwedge. The right posterior-oblique beam included a 15°Gy to the 95% isodose line.
a patient with a tumor in the right lung. The patient was treatedded a 30° wedge and the posterior beam included a 45° degree
wedge and partial blocking. The dose distribution delivered 63
29) and simulated annealing for plan optimization (14). All cal- d
ig. 2. The first Treatment Plan Explorer screen asks for only threearameters to define the treatment delivery—the beam energy, theumber of beams, and the degree of fluence modulation. Based onhese selections, the program reads a set of previously optimizedlans. It then presents the user with choices of critical structures toanipulate during exploration and the corresponding available
ecision doses.

ctwgPs
sstdbBncuwa0Hi
o
biP(csllfdcps
erawdsmu
574 I. J. Radiation Oncology ● Biology ● Physics Volume 61, Number 2, 2005
ulations included the full three-dimensional anatomy and bulkissue heterogeneity effects (Batho power-law correction). DVHsere computed using quasi-random points rather than a Cartesianrid. The number of points used per structure was 1000 for theTV, 600 for each lung, 100 for the esophagus, and 100 for thepinal cord.
Eight optimized data sets using 6-MV photons were created, ashown in Table 1. For each type of modulation, open and wedge, planets were created with 4, 6, 8, and 12 coplanar beams. In each case,he relative beam weights and their directions were optimized. Beamirection optimization was accomplished by starting with 36 eligibleeams equally spaced about the patient at 10° angular increments.eam weights were initially optimized for all 36 beams. Then theumber of eligible beams was reduced by eliminating those with lowontributions to the plan. This process was repeated up to four timesntil the desired number of beams remained. For wedge plans, theedge angles and directions were also optimized. Beam shapes were
utomatically generated to conform to the PTV projection with.5-cm margins, similar to the margins used in the clinical plan.owever, unlike the clinical plan, no partial beam blocking was
ncluded.For each delivery method (modulation and beam number), a set of
Fig. 3. The interactive exploration of all the possible odose–volume histogram (DVH) for the planning targemaximum dose. The bottom graphs are simple DVHs foEach critical structure DVH is defined by one or two cmaximum dose control points can only move laterally, chcan only move vertically, changing volume but not decipermissible motion.
ptimized plans was automatically generated using the various com- o
inations of dose–volume constraints for the critical structures shownn Table 1. The optimization objective was to maximize the minimumTV dose subject to strictly enforced dose–volume constraints“hard” constraints). For each decision dose, an optimized plan wasreated using each volume limit. For this example case, there wereeven different volume levels permitted to exceed 20 Gy for the rightung, seven different volume levels permitted to exceed 20 Gy for theeft lung, and six different volume levels permitted to exceed 50 Gyor the esophagus. The spinal cord was limited to 45 Gy maximumose, which was not varied. An optimized plan was generated for eachombination of dose–volume constraints. Therefore, there were 294lans in each set (7 � 7 � 6). No constraints were applied to the PTVo that there was always a feasible solution.
The actual volumes exceeding the decision dose values werextracted from the DVHs for all the structures in each plan andecorded. Because of the optimization method, these values werelways less than or equal to the constraint values and representedhat could theoretically be achieved by the plan. The maximumose to each critical structure was also recorded. These criticaltructure data were the control points for TPEx. For the PTV, theinimum dose, maximum dose, and prescription dose (95% vol-
me) were recorded for each plan. An example of the output from
ed solutions is shown. The upper graph is a simplifiedme showing minimum dose, 95% volume dose, andcritical structures selected in the previous input screen.points that are individually movable by the user. The
g dose but not volume. The decision dose control pointsose value. For each point, a red bar shows the range of
ptimizt volur theontrolangin
sion d
ne optimization is shown in Table 2. The constraint values used

aen
P
f
w
o
a
ts
B
opHtbTbv
dmba
wrvesoeve
OW
RLESPPP
(
575Exploring optimized plans ● I. ROSEN et al.
s input to the optimization process and the resulting beam param-ters (directions and doses) that produced the optimum plan wereot used in TPEx.
arameterization of optimized plansThe PTV characteristics of the optimized plans were fit to linear
unctions of the control points,
PTVmin � a0min � �
i�1
n
aiminVi
DD � �i�1
n
biminDi
max (1)
PTV95% � a095% � �
i�1
n
ai95%Vi
DD � �i�1
n
bi95%Di
max (2)
PTVmax � a0max � �
i�1
n
aimaxVi
DD � �i�1
n
bimaxDi
max (3)
here
PTVmin � minimum dose in PTVPTV95% � minimum dose in 95% of PTVPTVmax � maximum dose in PTVVi
DD � volume exceeding the decision dose value for criticalrgan iDi
max � maximum dose in critical organ in � number of critical organsai, bi � fit parametersThe control points (Vi
DD and Dimax) are the independent variables
nd the PTV doses are the dependent variables. For this example,
Table 1. Parameter values
ModulationNumberof beams
Criticalstructure
pen 4 Right lungedge 6 Left lung
8 Esophagus12 Spinal cord
For each decision dose, an optimized plan was created using ea
Table 2. Sample output
Critical structure
Optimization in
Decisiondose (Gy)
Volumdecisi
ight lung 20eft lung 20sophagus 50pinal cord 45TV minimum dose (100% volume)TV 95% volume doseTV maximum dose (0% volume)
Abbreviations: PTV � planning target volume; TPEx � treatmThe decision dose values, plan volumes exceeding the decision d
highlighted). The constraint volume limits for the decision doses were
he number of independent variables is twice the number of criticaltructures.
oundaries of the space of optimized plansIt is important that the user’s exploration be limited to the space
f optimized solutions. Because of the parameterization, it isossible to compute PTV values for any set of control point values.owever, not all combinations of control point values correspond
o feasible solutions. Therefore, the motions of control points muste restricted by the boundaries of the space of optimized plans.his boundary will generally be complex and nonanalytic. Theoundaries for any given independent variable (control point) willary with the specific values of the other independent variables.The space of optimized plans was quantized using a bitmap of
imension Rm, where R is the desired resolution of the bitmap andis the number of independent variables. Each dimension of the
itmap corresponds to one of the independent variables. The scalessociated with dimension i was computed by
�xi � (xmax � xmin) ⁄ (R � 1) (4)
here xmax and xmin are the maximum and minimum values,espectively, of the independent variable xi, �xi is the increment inalues along the xi axis, and R is the dimension of the bitmap alongach axis. Applying Eq. 4 to each independent variable produces aet of control point values for each point in the bitmap of the spacef optimized plans. Note that the bitmap can be very large. For thisxample with eight independent variables, a resolution of eightalues per variable was used, giving a bitmap with 16,777,216lements.
e sets of optimized plans
imum(Gy)
Decisiondose (Gy)
Volume limit for decisiondose (%)
5 20 20, 30, 40, 50, 60, 70, 805 20 10, 20, 30, 40, 50, 60, 705 50 10, 20, 30, 40, 50, 605 45 0
lume limit shown.
he optimization process
Optimization output
it fore (%)
Plan volume exceedingdecision dose (%) Maximum dose (Gy)
20.0 27.63.0 33.30.0 30.70.0 30.6
18.0 Gy19.0 Gy33.7 Gy
an explorer.ximum dose, and PTV doses were used for interactive exploration
for th
Maxdose
7774
ch vo
from t
put
e limon dos
2010
50
ent plose, ma
used for optimization but not in TPEx.

ttvvcvttf
at
I
osa
the b
576 I. J. Radiation Oncology ● Biology ● Physics Volume 61, Number 2, 2005
For each plan in the optimized set, the corresponding point inhe bitmap is set to a value of 1. Consequently, the boundary ofhe space of optimized plans is defined by the edges of theolume of 1s in the bitmap. For any set of values of m-1ariables, the range of acceptable values for the mth variablean easily be found by scanning the mth axis of the bitmap. Thealues corresponding to the limits of the bits with value of 1 arehe range for the variable. Depending on the density of data inhe space of optimized plans, there may be gaps in the bitmap
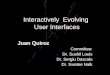
Fig. 4. A sequence of steps that leads to
rom undersampling. Therefore, the extreme limits of the 1s s
long an axis are taken as the range of the variable, even thoughhe 1s may not be continuous.
nitial solutionThe interactive exploration can start with any plan from the
ptimized set. Ideally, there should be no isolated regions in thepace of optimized plans, so that it should be possible to reachny solution from any starting point. However, a good starting
est plan selected for 12 wedged beams.
olution can be beneficial for two reasons. First, finite sampling

otSsclppmparmw
tbbvjp
sFwrwct(fPiGt
tpthdpBsplipmtbPpt
TifsDDPtTms
aaicccpiiFt
istnptcistpitteocccpfpdo
pdpm
577Exploring optimized plans ● I. ROSEN et al.
f the space might, in fact, produce isolated regions that couldrap the user and prevent reaching the most desirable one.econd, there is no reason not to expect discontinuities in thepace of optimized solutions. In suggesting that there are dis-ontinuities, we mean that every point in the space is notinearly connected to every other point. Although it should beossible to reach every point in the space from every otheroint, the sequences of moves along the multiple axes of theultidimensional space may not be commutative. Finding a
articular solution will depend on the sequence of steps as wells the starting point. Therefore, a good starting solution willeduce the amount of interactive searching needed to find theost desirable one. We chose as our initial solution the oneith the largest PTV maximum dose.
RESULTS
One of us (Z.L.) used TPEx to select the best plans forreatment configurations using 4 open beams, 12 openeams, 4 wedged beams, and 12 wedged beams. For eacheam configuration, the control point values (decision doseolumes and maximum dose values) were interactively ad-usted until a solution was found that gave the best com-romise in doses to the critical structures and PTV.Figure 4 shows a sequence of steps that led to the best plan
elected for 12 wedged beams. The initial solution is shown inig. 4a. First, the volume of left lung exceeding 20 Gy (V20)as reduced from 43.3% to 26.7% (the bottom of the available
ange) (Fig. 4b). Then, the maximum dose to the esophagusas reduced from 75 Gy to 68 Gy (Fig. 4c). This reduction
hanged the range of available values for the decision dose forhe left lung, allowing the V20 to be further reduced to 9.4%Fig. 4d). Next, reducing the maximum dose to the right lungrom 75 Gy to 71.8 Gy improved the uniformity of dose in theTV by reducing the maximum PTV dose (Fig. 4e). Finally,
ncreasing the maximum esophagus dose from 68 Gy to 70.6y further improved the PTV dose uniformity by increasing
he minimum dose (Fig. 4f).The first two steps (Figs. 4b and 4c) show that reducing
he maximum dose to the esophagus lowers the range ofossible doses to V20 of the left lung. It seems reasonablehat the lower dose levels for V20 of the left lung shouldave been available in the initial solution. We attribute thiseficiency to the coarse sampling of the space of optimizedlans and the coarse quantization of the space by the bitmap.oth of these are consequences of limited computing re-
ources. The actual sequence of steps originally used toroduce this final plan was not recorded. The results of theinear fits (Eqs. 1–3) to the control point values are shownn Fig. 5 for each of the delivery techniques. The fit value islotted against the corresponding plan value for each opti-ized plan and the root-mean-square error is shown. The
rend lines are least-squares fits to the data. The fits wereest for the maximum PTV dose and worst for the minimumTV dose. In general, the linear model seems to be appro-riate and higher order polynomials have not yet beenested.
The critical structure DVH constraint values selected in f
PEx were entered into Plan3D and used to create correspond-ng optimized plans. Figure 6 shows the results for each of theour beam configurations. The TPEx panel is shown with theelected critical structure dose limits. The dose distribution andVH from the resulting plan are also shown. On the planVH, the critical structure dose–volume limits and resultingTV values from TPEx are indicated for comparison. It is clear
hat the plan DVHs did not exactly match the TPEx values.he differences arise from the parameterization of the opti-ized plan characteristics and, as previously mentioned, the
tochastic nature of the simulated annealing algorithm.Based on the DVHs in TPEx, the plans with more beams
nd with wedges were generally better, as judged by themount of sparing of the left lung. However, the differencesn plans became progressively less as the complexity in-reased. Therefore, the physician could readily gauge thelinical benefit versus delivery complexity. These resultsould be compared with the clinical plan used to treat theatient. However, these calculations used a dose model thats less accurate than Pinnacle3, especially with heterogene-ties, and a different methodology for computing DVHs.urthermore, there was no attempt to vary beam margins or
o use partial beam blocking as was done in the clinical plan.
DISCUSSION
The treatment planning example presented is intended tollustrate the concept of interactive exploration. It istraightforward to extend this treatment-planning paradigmo include intensity-modulated radiation therapy (IMRT),oncoplanar beams, and electrons. Although the exampleresented used coplanar non-IMRT beams, this limitation isotally independent of the TPEx process or software. Be-ause the data set (the Pareto front) that underlies the TPExnterface requires computing hundreds (preferably thou-ands) of optimized treatment plans, the size of the spacehat can be explored depends on the available computingower. Including IMRT delivery will require more comput-ng capability than three-dimensional conformal radiationherapy because it adds another degree of freedom to thereatment planning problem, namely the fluence pattern forach beam. The optimization of each plan can still be basedn maximizing the tumor dose subject to dose–volumeonstraints for the critical structures. The use of only fourritical structures and one decision dose for each is also aomputer limitation and not inherent in the interactive ex-loration concept. On a positive note, it is easy and straight-orward to harness the power of parallel processing to thisroblem. After the set of optimization problems has beenefined, each problem can be run independently in paralleln a separate processor.The example presented does not explore the space of all
ossible solutions for a given delivery method and set ofecision doses. It is limited to the space defined by thearameters in Table 1. To explore the entire space of opti-ized solutions would require computing optimized plans
or the complete range of volumes (0–100%) for each

cctcdto
mvpat
amcssstwawaa
578 I. J. Radiation Oncology ● Biology ● Physics Volume 61, Number 2, 2005
ritical structure and each decision dose. We expect thatomputers and calculation algorithms will be fast enough inhe not-too-distant future to do that. Then, the finite speed ofomputation will restrict how many delivery options andecision doses can be explored, but the interactive explora-ion as shown in Fig. 3 will extend over the entire space ofptimized solutions.We hypothesize that the PTV DVH of the true opti-um solutions vary smoothly as each of the independent
ariables is changed independently. However, solutionsroduced by simulated annealing optimization have anssociated uncertainty because of the stochastic nature of
Fig. 5. The results of the linear fits (Eqs. 1–3) to the conbeams (a), 12 open beams (b), 4 wedged beams (c), ancorresponding plan value for each optimized plan andleast-squares fits to the data.
he method. Unlike directed search methods, simulated i
nnealing optimization has the potential to find a globalinimum in a space with multiple local minima and it
an easily incorporate “hard” constraints. However, itstochastic nature means that it never finds the exactolution to the problem nor does it produce the sameolution in repetitions of the same calculation. It asymp-otically approaches the true solution in a probabilisticay that depends on the length of the computation. The
nalytic fits, therefore, replace the measured “noisy” dataith smoothly varying functions that should be better
pproximations to the true optimum solutions. Thesenalytic functions also make the response of the user
int values for each of the delivery techniques—4 openwedged beams (d). The fit value is plotted against theoot-mean-square error is shown. The trend lines are
trol pod 12
the r
nterface smoother and perhaps faster. A directed search

oli
cFtshp
watw
ppsptoaptflTpDr
579Exploring optimized plans ● I. ROSEN et al.
ptimization method, such as a gradient search, wouldikely give better parameter fits and might entirely elim-nate the need for the analytic function.
The multidimensional linear function was chosen be-ause it is the simplest analytic function for the purpose.igure 5 shows that it is a good approximation. Some of
he variance in fit is due to the stochastic nature of theimulated annealing optimization algorithm. Of course,igher order functions could be applied and might im-rove the results.The dose distributions shown in Fig. 6 demonstrate the
ell-known hazard of making decisions based on DVHslone. With open beams, there are rarely hot spots outside ofhe target volume. However, such hot spots often occur with
Fig. 5.
edged beams and IMRT beams if appropriate inverse t
lanning goals/constraints are not employed. The sameroblem exists with the TPEx process. In generating thepace of optimized plans, suitable constraints must be ap-lied to normal structures to avoid such hot spots. In addi-ion, TPEx must display the DVHs for all normal structuresf concern. If important features of the treatment plan, suchs hot spots, are not controlled during the optimizationrocess or displayed during the interactive exploration, thenhe physician is attempting to make decisions based onawed or incomplete data and the process is meaningless.here is a minimum level of computer power needed toroduce a data set that is sufficiently complete so that theVHs presented during interactive exploration properly
epresent the underlying three-dimensional dose distribu-
nued).
(Contiions. The parameters for that level of computing capability

ad
maaw
ocpsri
580 I. J. Radiation Oncology ● Biology ● Physics Volume 61, Number 2, 2005
nd for the completeness of the data set have not beenetermined.As computing power increases and more efficientethods for computing optimum treatment geometries
re developed, more plans can be generated before inter-ctive exploration. In addition to faster computer hard-
Fig. 6. The critical structure dose–volume histogram ((TPEx) for each of the delivery techniques and the resbeams (b), 4 wedged beams (c), and 12 wedged beams (and resulting PTV values from TPEx are indicated for c
are, parallel processing can easily be used because each p
ptimization problem (different constraint values) can beomputed independently. In the current process of pre-aring optimized plans for TPEx, critical structure con-traint values are varied in uniform step sizes over aange of values. Other more efficient methods of search-ng the range of dose–volume constraints are certainly
constraint values selected in Treatment Plan Exploreroptimized treatment plan—4 open beams (a), 12 openthe plan DVH, the critical structure dose–volume limitsison.
DVH)ultingd). Onompar
ossible. Faster plan optimization means that a greater

ridnmmrb
pfidlter
581Exploring optimized plans ● I. ROSEN et al.
ange of treatment delivery options can be computed,ncorporating more critical structures and more decisionoses per structure. Then, at interactive treatment plan-ing, the physician or physicist could explore the treat-ent possibilities at many more levels of complexity andake a more informed decision about the greater effort
equired for more complex treatments versus the clinicalenefit to the patient.
Fig. 6.
The general goal of TPEx is the same as that of inverse t
lanning—to eliminate the details of treatment deliveryrom the planning process. However, rather than attempt-ng to define a mathematical formulation of the clinicalecision process (objectives and constraints), TPEx ana-yzes the relationships between normal tissue doses andarget volume doses under conditions of optimum deliv-ry and allows the user to interactively explore thoseelationships. The planner is effectively traveling along
nued).
(Contihe boundary of all optimal solutions. We believe that

tm
t
1
1
1
1
1
1
582 I. J. Radiation Oncology ● Biology ● Physics Volume 61, Number 2, 2005
his interactive process can make treatment planning
ore efficient and result in treatment plans that are more mREFEREN
radiotherapy. Med Phys 2001;28:1696–1702.
1
1
1
1
2
2
2
2
2
2
2
2
2
2
ailored to the needs of the patient and the clinical judg-
ent of the physician.CES
1. Bedford JL, Webb S. Elimination of importance factors forclinically accurate selection of beam orientations, beamweights and wedge angles in conformal radiation therapy.Med Phys 2003;30:1788–1804.
2. Bednarz G, Michalski D, Houser C, et al. The use of mixed-integer programming for inverse treatment planning with pre-defined field segments. Phys Med Biol 2002;47:2235–2245.
3. Cotrutz C, Xing L. Segment-based dose optimization using agenetic algorithm. Phys Med Biol 2003;48:2987–2998.
4. Deasy JO. Multiple local minima in radiotherapy optimizationproblems with dose-volume constraints. Med Phys 1997;24:1157–1161.
5. Djajaputra D, Wu Q, Wu Y, et al. Algorithm and performanceof a clinical IMRT beam-angle optimization system. PhysMed Biol 2003;48:3191–3212.
6. Gopal R, Starkschall G. Plan space: Representation of treat-ment plans in multidimensional space. Int J Radiat Oncol BiolPhys 2002;53:1328–1336.
7. Langer M, Lee EK, Deasy JO, et al. Operations researchapplied to radiotherapy, an NCI-NSF-sponsored workshopFebruary 7–9, 2002. Int J Radiat Oncol Biol Phys 2003;57:762–768.
8. Langer M, Morrill S, Brown R, et al. A comparison of mixedinteger programming and fast simulated annealing for opti-mizing beam weights in radiation therapy. Med Phys 1996;23:957–964.
9. Langer M, Brown R, Morrill S, et al. A generic geneticalgorithm for generating beam weights. Med Phys 1996;23:965–971.
0. Michalski D, Xiao Y, Censor Y, et al. The dose-volumeconstraint satisfaction problem for inverse treatment planningwith field segments. Phys Med Biol 2004;49:601–616.
1. Morrill SM, Lane RG, Jacobson G, et al. Treatment planoptimization using constrained simulated annealing. Phys MedBiol 1991;36:1341–1361.
2. Pugachev A, Xing L. Incorporating prior knowledge intobeam orientation optimization in IMRT. Int J Radiat OncolBiol Phys 2002;54:1565–1574.
3. Rosen II, Lane RG, Morrill SM, et al. Treatment plan opti-mization using linear programming. Med Phys 1991;18:141–152.
4. Rosen II, Lam KS, Lane RG, et al. Comparison of simulatedannealing algorithms for conformal therapy treatment plan-ning. Int J Radiat Oncol Biol Phys 1995;33:1091–1099.
5. Rowbottom CG, Khoo VS, Webb S. Simultaneous optimiza-tion of beam orientations and beam weights in conformal
6. Spirou SV, Chui CS. A gradient inverse planning algorithmwith dose-volume constraints. Med Phys 1998;25:321–333.
7. Starkschall G, Pollack A, Stevens CW. Treatment planningusing a dose-volume feasibility search algorithm. Int J RadiatOncol Biol Phys 2001;49:1419–1427.
8. Stein J, Mohan R, Wang XH, et al. Number and orientationsof beams in intensity-modulated radiation treatments. MedPhys 1997;24:149–160.
9. Willoughby TR, Starkschall G, Janjan NA, et al. Evaluationand scoring of radiotherapy treatment plans using an artificialneural network. Int J Radiat Oncol Biol Phys 1996;34:923–930.
0. Wu Q, Djajaputra D, Wu Y, et al. Intensity-modulated radio-therapy optimization with gEUD-guided dose-volume objec-tives. Phys Med Biol 2003;48:279–291.
1. Yu Y, Schell MC, Zhang JB. Decision theoretic steering andgenetic algorithm optimization: Application to stereotacticradiosurgery treatment planning. Med Phys 1997;24:1742–1750.
2. Zhang X, Liu H, Wang X, et al. Speed and convergenceproperties of gradient algorithms for optimization of IMRT.Med Phys 2004;31:1141–1151.
3. Cotrutz C, Lahanas M, Kappas C, et al. A multiobjectivegradient-based dose optimization algorithm for external beamconformal radiotherapy. Phys Med Biol 2001;46:2161–2175.
4. Liu H, Rosen I, Janjan N, et al. Treatment planning optimi-zation based on response-surface modeling of cost functionversus multiple constraints. CD ROM Proceedings of theWorld Congress on Medical Physics and Biomedical Engi-neering, 4 pp, July 23–28, 2000.
5. Meyer J, Phillips MH, Cho PS, et al. Application of influencediagrams to prostate intensity-modulated radiation therapyplan selection. Phys Med Biol 2004;49:1637–1653.
6. Schreibmann E, Lahanas M, Xing L, et al. Multiobjectiveevolutionary optimization of the number of beams, their ori-entations and weights for intensity-modulated radiation ther-apy. Phys Med Biol 2004;49:747–770.
7. Xing L, Li JG, Donaldson S, et al. Optimization of importancefactors in inverse planning. Phys Med Biol 1999;44:2525–2536.
8. Alber M, Birkner M, Nusslin F. Tools for the analysis of doseoptimization: II. Sensitivity analysis. Phys Med Biol 2002;47:N265–N270.
9. Rosen II, Loyd MD, Lane RG. Collimator scatter in modeling
radiation beam profiles. Med Phys 1990;17:422–428.