Embed Size (px)
Citation preview

Intensive Family Medicine Board Review. PCOM Med net
Pediatrics
Christine Black-Langenau, DO Osteopathic Residency Program Director, Byrn Mawr Hospital

Case 1. Newborn
4-day-old 39 wks. 7lbs 2oz newborn. NSVD without complications. Breastfeeding every 2 hours. Discharged from nursery day 2. (TcB=8.6 at that time) Follow up in office at 4 days of life, appears jaundiced.

Case 1. Newborn
What would be the best next step for this jaundiced 4 day old?
a) Stop breastfeeding and give formula
b) Admit to hospital for photo therapy
c) Observe bilirubin was normal at 48 hours. No further evaluation needed
d) Venous bilirubin measurement ASAP.

Case #1 Newborn with Jaundice
n Answer: d

Case 1. Newborn n Promote and support successful
breastfeeding n Measure TSB or TcB if
jaundiced in the first 24 hours n Interpret bilirubin levels
according to the infant’s age in hours
n Perform risk assessment prior to discharge
n Give parents written and oral information .
n Provide appropriate follow-up based on time of discharge and risk assessment.
n Treat newborns, when indicated, with phototherapy or exchange transfusion.

Nomo gram for designation of risk in 2840 well newborns at 36 or more weeks’ gestational age with birth weight of 2000 g or more or 35 or more weeks’ gestational age and birth weight
of 2500 g or more based on the hour-specific serum bilirubin values.
Subcommittee on Hyperbilirubinemia et al. Pediatrics 2004;114:297-316
©2004 by American Academy of Pediatrics

Risk Factors for hyperbilirubinemia
n Prematurity n Breastfeeding n Asian ethnicity n Metabolic disorder
n Hypothyroidism n Glactosemia
n Maternal Diabetes n Infection
n UTI n Sepsis
n Drugs
n Increased Bilirubin Production n Hemolytic Disease n Birth trauma n Polycythemia
n Impaired Bilirubin Conjugation n Gilbert n Milk jaundice
n Biliary Obstruction

References n American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management
of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004;114(1):297-316.
n Lauer BJ, Spector ND. Hyperbilirubinemia in the newborn.Pediatr Rev. 2011 Aug;32(8):341-9. doi: 10.1542/pir.32-8-341.
n Moerschel,S. Cianiaruso, L. A Practical Approach to Neonatal Jaundice. American Family Physician. number 9. May 2008. Vol 77,

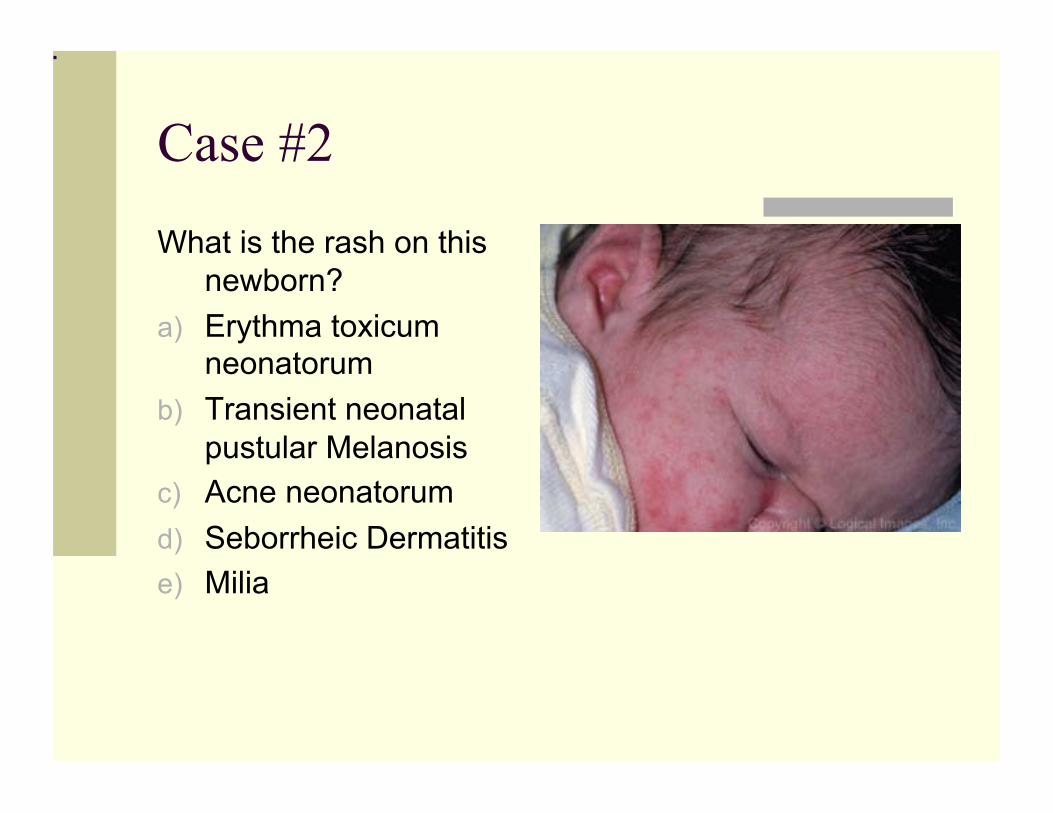
Case #2 5 day old brought by mother because concerned about
rash. States that she noticed on 3rd day of life. Looks like chicken pox on face and chest. Baby had normal pregnancy and nursery stay. Breastfeeding well and had regained birth weight. No sick contacts.
Case #2
What is the rash on this newborn?
a) Erythma toxicum neonatorum
b) Transient neonatal pustular Melanosis
c) Acne neonatorum d) Seborrheic Dermatitis e) Milia

Case #2
n Answer: a

Erythma Toxicum Most common pustular eruption (40-70%) Erythmatous macules 2-3 mm. Evolve into pustules. Lesions found on head & face, trunk and proximal extremities involved Surrounding erythma No treatment needed

Transient Neonatal Pustular Melanosis
n Vesiculopapular rash n Lack of surrounding
erythma n Pustules rupture and
leave a hyper pigmented macule lasting for 3-4 wks.

Acne Neonatorum n 20% newborns n Closed come domes on
forehead, nose and cheeks n Inflammatory papules and
pustules may develop n Acne develops from
hormonal stimulation n Resolves spontaneously in
2-4 months n Can use benzyl 2.5 % if
severe or persistent.

Seborrhea Dermatitis n Erythma and greasy scales.
On scalp, “cradle cap” n Can affect face ears, and
neck. n Erythma in folds n Occurs in first few months of
life n Not itchy n Treatment with tar shampoo n Ketoconazole or cortisone
cream both shown some benefits if persistent.

References
n O'Connor NR, McLaughlin MR, Ham P. Physician. Newborn skin: Part I Common Rashes. Am Family Physician. 2008 Jan 1;77(1):47-52.
Case # 2 b
n 5 day old brought by mother because concerned about rash. After diagnosing the rash you do a physical exam and notice a clunk when pressing upwards and abducting the left hip. What is the next step?
n a) ultrasound of hip n b) x ray of hips n c) Referral for Palvik harness n d) Observe repeat exam in 2 weeks.

Case 2-b
n Answer: d
n Hip dislocation common in the first 2 weeks of life. If found at birth should observe, and schedule repeat exam in 2 weeks.
n Reference: n Storer SK, Skaggs DL Developmental dysplasia of the hip. Am Fam Physician. 2006 Oct
15;74(8):1310-6.

Hip Dysplasia
Screened by hip exam as infant (Barlow, Ortolani)
n Risk factors: n Female, breech, family
history n What imaging
techniques are used to evaluate the condition? n 4-6 months of age:
sonogram n After 4 months: x ray
n Tests commonly used to assess hip stability. (A) Ortolani maneuver. A gentle upward force is applied while the hip is abducted.(B) Barlow maneuver. A gentle downward force is applied
while the hip is adducted.
n Figure from www.aafp.org Hip Dysplasia fromOctober 15, 2006 ◆ Volume 74, Number 8 www.aafp.org/afp American Family Physician 1311

Case #3
12 month old male for routine visit. Mother concerned about development. What expected at this visit?
n a) Lead screening and hematocrit n b) blood pressure measurement n c) developmental screening for speech
skills, asking if putting 2 words together n d)Anticipatory guidance, recommendation
for child remain in backwards facing car seat.

Case #3
n Answers: A & D


Health screening for12 month old
n Lead screening and hematocrit. n Lead screening
n Geography n Medicaid or Medicare enrolled n House older than 1950’s n Recent renovation in house older than 1978 n Sibling or friend with elevated lead level n Recent immigrant to US

Screening in 12 month old
n Low Hematocrit DDX n Iron deficiency anemia most common
n Inadequate dietary intake and chronic occult loss n Concurrent infection n Blood loss n Hgb disorders, thalassemia, sickle cell n RBC enzyme defects,G6PD or Pyruvate Kinase
deficiency n Lead poisoning n Other- Leukemia, hemylosis Drug induced, HUS

Blood pressure screening
n Screening recommended at 3 years of age n BP readings need to be looked at in regard to
age, sex or height. n Prehypertension =90-95th % or 120/80 n Stage I 95th-99th plus 5mm Hg n Stage 2 99th plus 5mm Hg
Hypertension in children- 20% from secondary causes
Renal disease or coarctation of aorta.

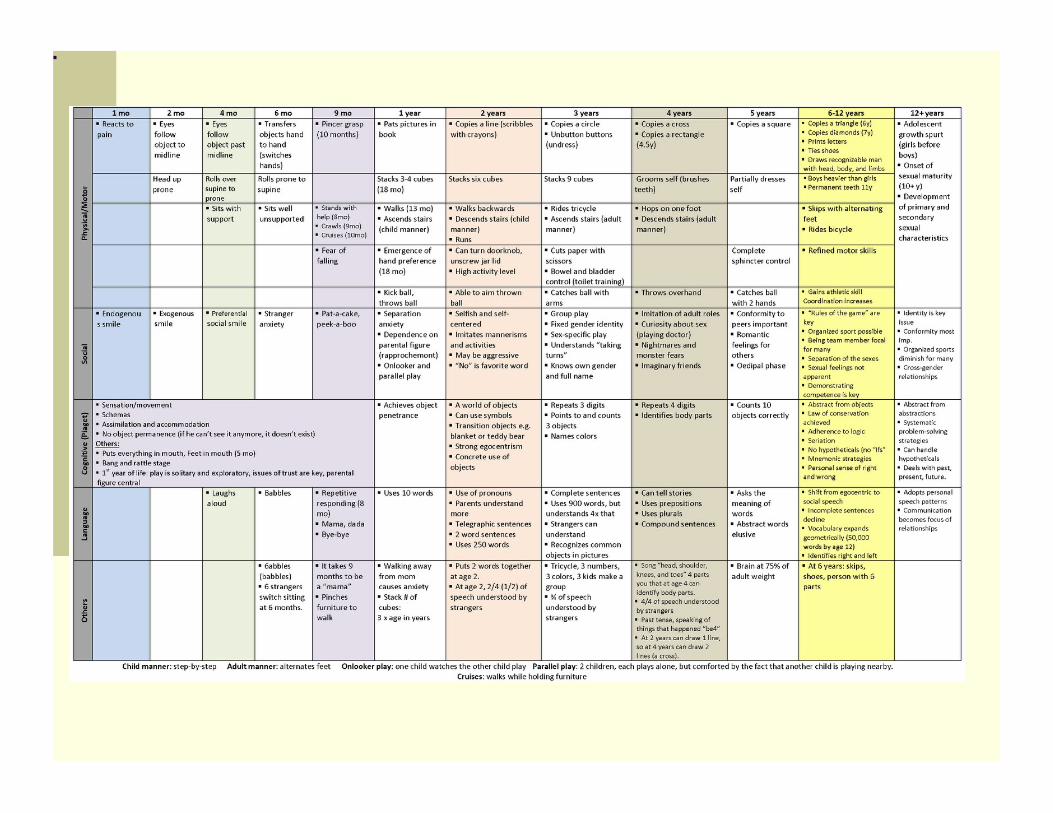
Speech development
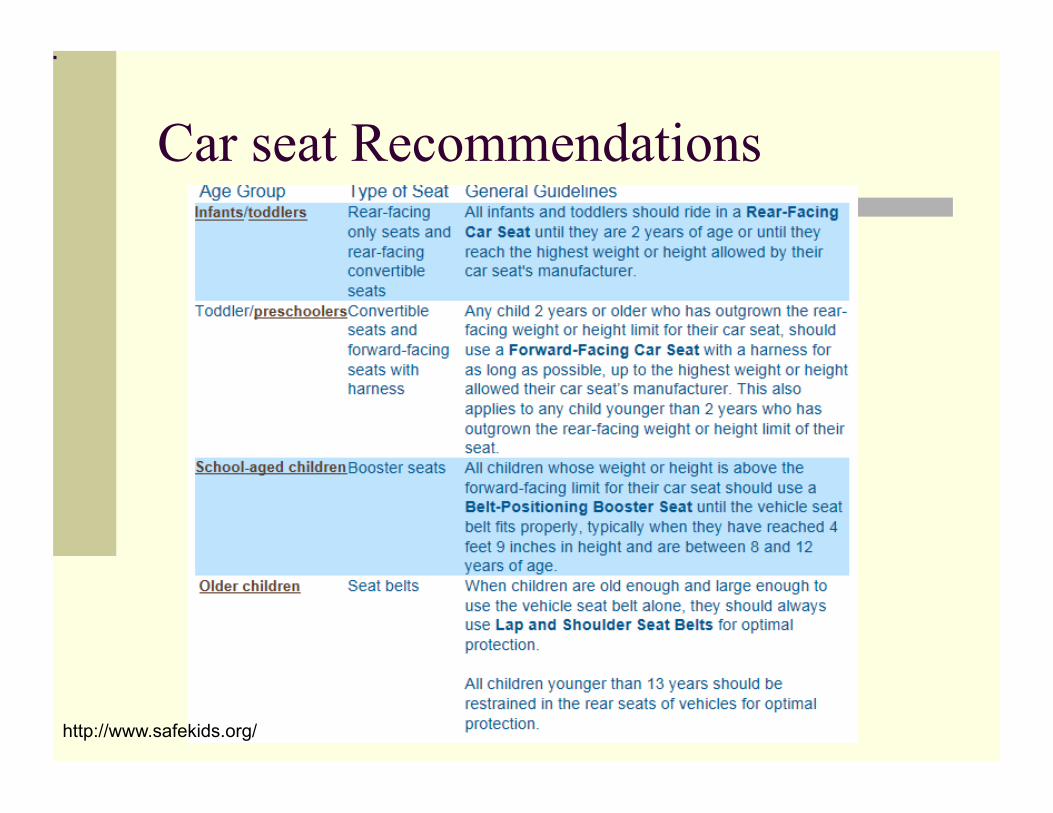
Car seat Recommendations
http://www.safekids.org/

Unintentional injury in Children
n Motor Vehicle accident is most common cause of unintentional cause of death in children.
n Motor Vehicle 58% n Drowning 10.9% n Poisoning 7.7%



Lead screening
n Risk Factors n Geographic area n Lives in house built before
1978 n Recent renovations to older
house n Medicare or Medicaid
enrolled n Sibling or playmate with
elevated lead level

Case # 4
n 4 year old female for routine visit. Patient was up to date at last visit. Mother concerned about safety of multiple vaccines at one visit.

Case #4
n What vaccines are due at this visit?
a) MMR and Varicella b) DTap and IPV c) DTap, IPV, Influenza,
MMR and Varicella d) Influenza only

Case #4
n Answer: c
n Recommended Vaccine schedule should be followed.
n No evidence that vaccines need to be split up to be more effective or safer.
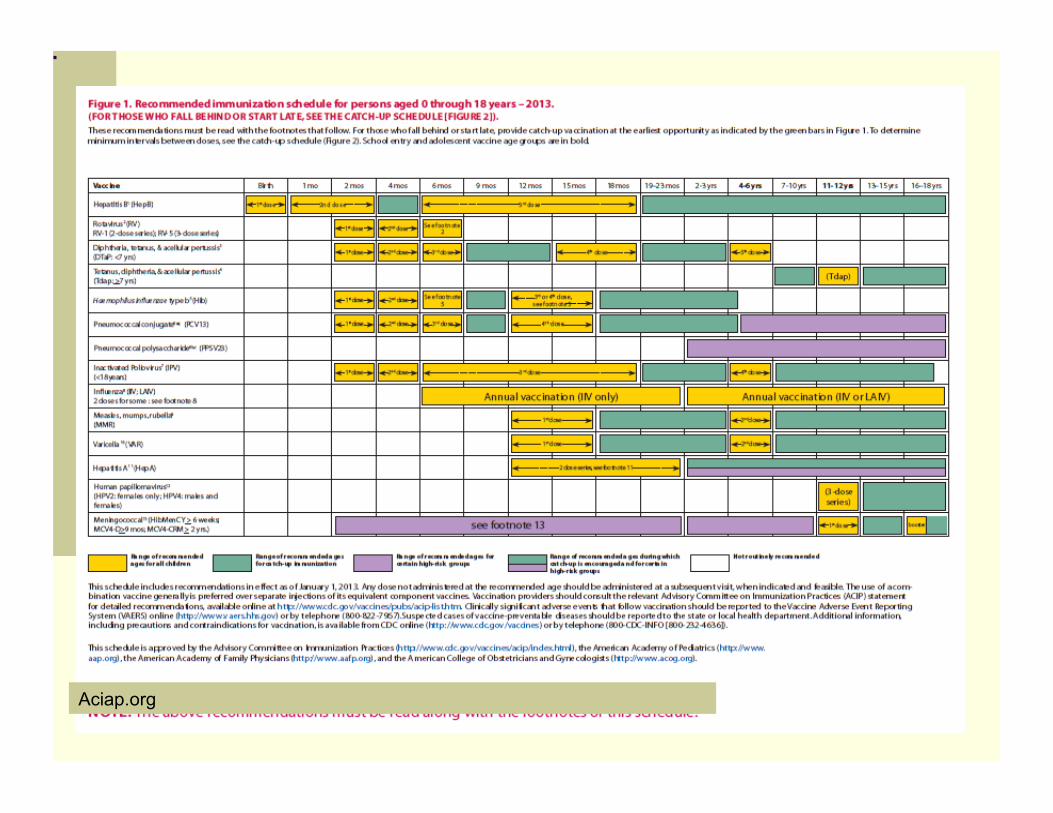
Aciap.org

Case #5
n 11 year old male for routine visit. Parents concerned with decreasing grades and lack of energy. What should be covered in this visit?
a) School and friends b) Smoking and drugs c) ADHD evaluation d) Vaccines e) All of the above
Case #5
Answer: e – all of the above

Case #5
n School and friends n Bullying is common
and should be asked about.
n Bullying most common in middle school
n Bully victims have n Higher level of health
problems n Higher academic
problems n Poorer emotional
adjustment n increased psychosocial
n Suicide n Anxiety and
depression

Depression
n 2.8% of kids younger than 13. n More likely to show irritability than sad mood.
Restlessness, separation anxiety or phobias more common.

ADHD
n 2-16% school aged children
n DSM-IV n Inattention- 6 or more symptoms of inattention
and persisted for 6 months and is maladaptive n Impulsivity-6 or more symptoms of
hyperactivity or impulsivity for 6 months and is maladaptive or inconsistent with developmental level

ADHD DSM IV
n hyperactive-impulsivity or inattention were present before 7 years of age
n Impairment are present in two or more settings
n There is clear evidence of significant impairment in social, academic, or occupational functioning
n Symptoms are not part of a psychiatric or developmental disorder
ADHD coexisting conditions
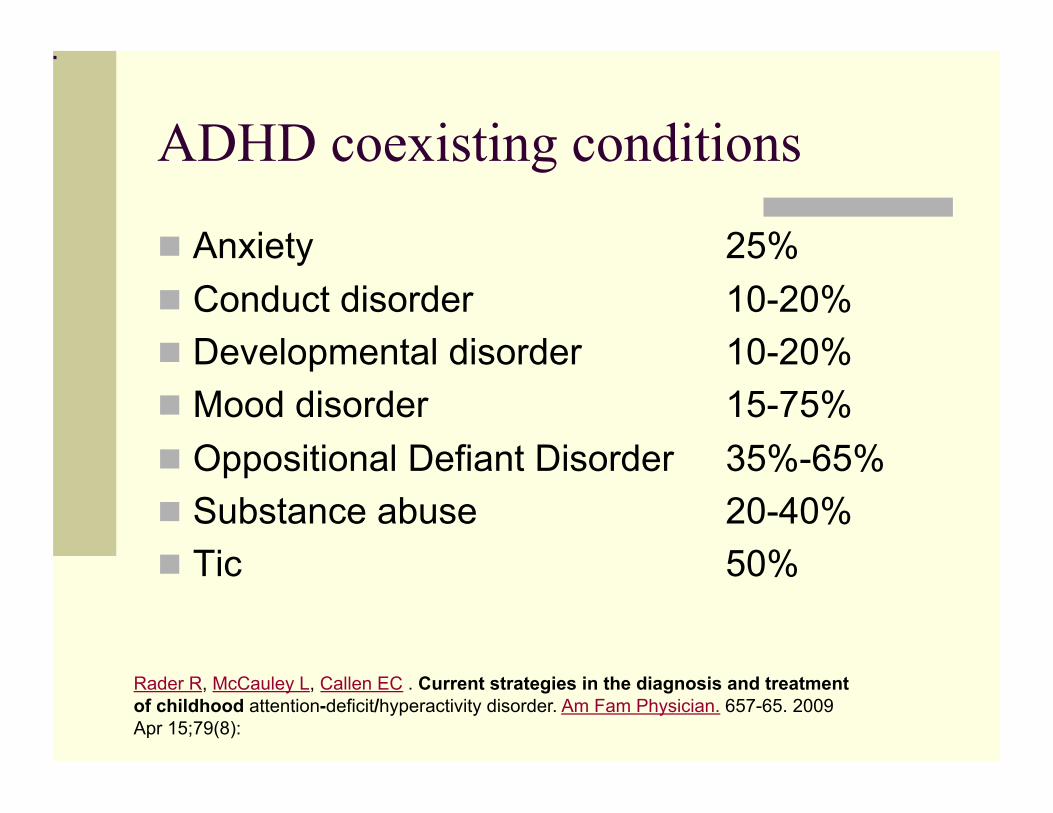
n Anxiety 25% n Conduct disorder 10-20% n Developmental disorder 10-20% n Mood disorder 15-75% n Oppositional Defiant Disorder 35%-65% n Substance abuse 20-40% n Tic 50%
Rader R, McCauley L, Callen EC . Current strategies in the diagnosis and treatment of childhood attention-deficit/hyperactivity disorder. Am Fam Physician. 657-65. 2009 Apr 15;79(8):

References n American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of
hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics. 2004;114(1):297-316.
n Lauer BJ, Spector ND. Hyperbilirubinemia in the newborn.Pediatr Rev. 2011 Aug;32(8):341-9. doi: 10.1542/pir.32-8-341.
n Moerschel,S. Cianiaruso, L. A Practical Approach to Neonatal Jaundice. American Family Physician. number 9. May 2008. Vol 77,
n Rader R, McCauley L, Callen EC . Current strategies in the diagnosis and treatment of childhood attention-deficit/hyperactivity disorder. Am Fam Physician. 657-65. 2009 Apr 15;79(8):
n Clark MS, Jansen KL, Cloy JA. Treatment of childhood and adolescent depression. Am Fam Physician. 2012 Sep 1;86(5):442-8. Review
n Storer SK, Skaggs DL. Developmental dysplasia of the hip.Am Fam Physician. 2006 Oct 15;74(8):1310-6. Review
n Riley M, Bluhm B. High blood pressure in children and adolescents. Am Fam Physician. 2012 Apr 1;85(7):693-700. Review.

References n Theurer WM, Bhavsar AK. 502-9.Prevention of unintentional childhood
injury. n Am Fam Physician. 2013 Apr 1;87(7):
n Warniment C, Tsang K, Galazka SS, Lead poisoning in children. Am Fam Physician. 2010 Mar 15;81(6):751-7.
n O'Connor NR, McLaughlin MR, Ham P. Newborn skin: Part I. Common rashes. Am Fam Physician. 2008 Jan 1;77(1):47-52.
n Riley M, Locke AB, Skye EP. Health maintenance in school-aged children: Part II. Counseling recommendations.Am Fam Physician. 2011 Mar 15;83(6):689-94
n Caudle,J. and Runyon, M.K. Bullying Among Today’s Youth:The Important Role of the Primary Care Physician. Osteopathic Family Physician 2013 Vol5, no4, July/August. 140-146





























