Embed Size (px)
Citation preview

Intensive Care Nursery House Staff Manual69Copyright © 2004 The Regents of the University of California
Intrauterine Growth RetardationCLINICAL SIGNIFICANCE: Intrauterine growth retardation (IUGR) affects 3-10% ofpregnancies; 20% of stillborn infants have IUGR. Perinatal mortality rates are 4-8 timeshigher for growth retarded infants, and morbidity is present in 50% of surviving infants.DEFINITIONS and CLASSIFICATION:-AGA, appropriate for gestational age: Birth weight is between 10th and 90th percentilefor infant’s gestational age (GA).-LGA, large for gestational age: Birth weight >90th percentile for GA.- SGA, small for gestational age: Birth weight <10th percentile for GA. Other definitionsare sometimes used for SGA, including <3rd percentile for GA or more than 2 S.D.below the mean.-IUGR vs. SGA: IUGR refers to deviation and reduction in expected fetal growthpattern. Multiple adverse conditions inhibit normal fetal growth potential. Not allIUGR infants are SGA.ASYMMETRIC vs. SYMMETRIC GROWTH RETARDATION: Most growthretarded infants have asymmetric growth restriction. First there is restriction of weightand then length, with a relative “head sparing” effect. This asymmetric growth is morecommonly due to extrinsic influences that affect the fetus later in gestation, such as preeclampsia,chronic hypertension, and uterine anomalies. Postnatal growth after IUGRdepends on cause of growth retardation, postnatal nutritional intake, and socialenvironment. Symmetric growth retardation affects all growth parameters. In the humanbrain, most neurons develop prior to the 18th week of gestation. Early gestational growthretardation would be expected to affect the fetus in a symmetric manner, and thus havepermanent neurologic consequences for the infant. Examples of etiologies for symmetricgrowth retardation include genetic or chromosomal causes, early gestational intrauterineinfections (TORCH) and maternal alcohol use.CAUSAL FACTORS:A. Maternal-Before pregnancy:• Prepregnancy weight influences fetal size• Periconceptual nutritional status can affect embryogenesis (e.g., folate deficiency).-During pregnancy: Factors that may adversely affect fetal growth include:• Low pre-pregnancy weight and small maternal size• Recent pregnancy and/or high parity• Poor weight gain during pregnancy, especially in latter half• Chronic illness - such as malabsorption, diabetes, renal disease• Inadequate or poorly balanced intake associated with alcoholism, drug abuse,poverty, adolescence, anorexia nervosa, food faddism• Maternal drug and alcohol use also influence maternal nutrition.• Decreased O2 availability to fetus (e.g., high altitude, severe maternal anemia)Intrauterine Growth Retardation70Copyright © 2004 The Regents of the University of California

B. Uterine and placental factors that can adversely affect fetal growth includeinadequate placental growth, uterine malformations, decreased utero-placental bloodflow (e.g., toxemias of pregnancy, diabetic vasculopathy) and multiple gestationsC. Fetal causes are unusual, include familial genetic and chromosomal abnormalities andintrauterine infections (i.e., TORCH), and usually have a poor long term prognosis.PATHOPHYSIOLOGY: With maternal or placental causes of IUGR, there is decreasedplacental transfer of nutrient (including oxygen) resulting in reduced fetal body stores oflipids and glycogen resulting in neonatal hypoglycemia; chronic hypoxemia stimulateserythropoietin production leading to polycythemia. These infants are also at increasedrisk for perinatal asphyxia. Other associated problems include hypocalcemia, pulmonaryhemorrhage, hypothermia and, with IUGR associated with toxemia, thrombocytopeniaand leukopenia. With fetal causes, decreased growth is constitutive (due to geneticfactors) or secondary to infection.ASSESSMENT and MANAGEMENT:-Treat asphyxia if present.-Measure weight, head circumference and length to categorize the type of IUGR.-Careful physical examination for anomalies and dysmorphic features.-Blood glucose and hematocrit to detect hypoglycemia and polycythemia. Seesections on Hypoglycemia (P. 153) and on Polycythemia (P. 112).-Serum Ca++, WBC count with differential and platelet count.-Infants with IUGR due to placental factors have ↑ O2 consumption. This ↑ insensiblewater loss to a variable degree (as much as 20-30%). Compensate for this byincreasing IV fluid intake. These infants may also need greater intake (>150 mL/kg/dand >100 kcal/kg/d) to achieve adequate growth.-Further workup and treatment depends on abnormalities identified on history andphysical examination.OUTCOME:-Perinatal mortality for IUGR infants is 5-20 times greater than for AGA, mainly dueto intrauterine death, perinatal asphyxia, and congenital anomalies.-Neurologic morbidity is 5-10 times higher than for AGA infants, especially forinfants with ↓ head circumference at birth. Intellectual and motor function (excludingthose with congenital infections, chromosomal abnormalities) depends on adverseperinatal events and on the specific cause of growth restriction. Early identificationand treatment of hypoglycemia and polycythemia improves outcome. Neurologicabnormalities are usual with genetic and infectious causes of IUGR.-Retarded growth: With placental causes of IUGR, catch-up growth occurs after birth,but these patients usually remain smaller than expected.-Fetal “programming” of cardiovascular disease: Recent studies implicate IUGRwith adult onset of hypertension, coronary heart disease, hypercholesterolemia, anddiabetes. These studies suggest that IUGR has long term affects on endocrinedevelopment and homeostasis.

Please help with the Wikimedia strategic planning process! Discuss the Strategy Task Forces' recommendations.
[Hide] [Help us with translations!]
Small for gestational ageFrom Wikipedia, the free encyclopedia
Jump to: navigation, search
Small for gestational age
Classification and external resources
ICD-10 P 05. , P 07.
ICD-9 764, 765
DiseasesDB 31952
MeSH D007230
Small for gestational age (SGA) babies are those whose birth weight lies below the 10th percentile for that gestational age.

Appropriate for gestational age (AGA) are those whose birth weight lies above the 10th percentile for that gestational age and below the 90th percentile for that gestational age.
Small for gestational age babies have usually been the subject of intrauterine growth restriction (IUGR), formerly known as intrauterine growth retardation.[1]
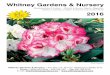
Gestational age and birth weight of infants born at 24 to 46 weeks' gestation. Infants are classified as large for gestational age (LGA), appropriate for gestational age (AGA), or small for gestational age (SGA). Another classification which takes in consideration only the weight and not the gestational age, is low body weight (LBW), VLBW and ELBW.
Low birth weight (LBW) is defined as a fetus that weighs less than 2500 g (5 lb 8 oz) regardless of gestational age. Other definitions include Very Low Birth Weight (VLBW) which is less than 1500 g, and Extremely Low Birth Weight (ELBW) which is less than 1000 g.[2] Normal Weight at term delivery is 2500 g - 4200 g.
SGA is not a synonym of LBW, VLBW or ELBW. Example: 35 week gestational age delivery, 2250g weight is appropriate for gestational age but is LBW. One third of low-birth-weight neonates-infants weighing less than 2500g - are small for gesational age.
There is a 8.1% incidence of low birth weight in developed countries, and 6–30% in developing countries. Much of this can be attributed to the health of the mother during pregnancy. One third of babies born with a low birth weight are also small for gestational age.
Contents
[hide]
1 Diagnosis

2 Predetermining factors 3 Categories of growth restriction
o 3.1 Symmetrical o 3.2 Asymmetrical
4 Treatment 5 Support 6 References
[edit] Diagnosis
The condition is generally diagnosed by measuring the mother's uterus, with the fundal height being less than it should be for that stage of the pregnancy. If it is suspected, the mother will usually be sent for an ultrasound to confirm.
[edit] Predetermining factors
The risk factor/etiology can be broadly divided into 3 categories-
Fetal Maternal Placental
The primary risk factor is that development of the placenta is insufficient to meet the demands of the fetus, resulting in malnutrition of the developing fetus. There are numerous contributing factors, of both environmental and genetic origin:
Environmental factors such as poor nutrition, tobacco smoking, drug addiction or alcoholism
Severe anaemia (although hydrops may also occur) Thrombophilia (tendency for thrombosis) Prolonged pregnancy Pre-eclampsia Chromosomal abnormalities Damaged or reduced placental tissue due to:
o Chronic renal failure o Sickle cell anemia o Phenylketonuria
Infections such as rubella, cytomegalovirus, toxoplasmosis or syphilis Twins and multiple births.
[edit] Categories of growth restriction

There are two distinct categories of growth restriction, indicating the stage at which the development was slowed. Small for gestational age babies can be classified as having symmetrical or asymmetrical [asymmetrical] growth restriction.[3][4]
[edit] Symmetrical
Symmetrical growth restriction, less commonly known as global growth restriction, indicates that the fetus has developed slowly throughout the duration of the pregnancy and was thus affected from a very early stage. The head circumference of such a newborn is in proportion to the rest of the body. Common causes include:
Early intrauterine infections, such as cytomegalovirus, rubella or toxoplasmosis Chromosomal abnormalities Chronic high blood pressure Severe malnutrition Anemia Maternal substance abuse (prenatal alcohol use can result in Fetal alcohol syndrome)
[edit] Asymmetrical
Asymmetrical growth restriction occurs when the embryo/fetus has grown normally for the first two trimesters but encounters difficulties in the third, usually pre-eclampsia. Such babies have a disparity in their length and head circumference when compared to the birth weight. A lack of subcutaneous fat leads to a thin and small body out of proportion with the head. Other symptoms include dry, peeling skin and an overly-thin umbilical cord, and the baby is at increased risk of hypoxia and hypoglycaemia.
[edit] Treatment
Possible treatments include the early induction of labour, though this is only done if the condition has been diagnosed and seen as a risk to the health of the fetus.
[edit] Support
The MAGIC Foundation for Children's Growth[1]
[edit] References
1. ̂ "eMedicine - Intrauterine Growth Retardation : Article by Vikram S Dogra, MD" . http://www.emedicine.com/radio/topic364.htm. Retrieved 2007-11-28.
2. ̂ "eMedicine - Extremely Low Birth Weight Infant : Article by KN Siva Subramanian, MD" . http://www.emedicine.com/ped/topic2784.htm. Retrieved 2007-11-28.
3. ̂ "Intrauterine Growth Restriction". http://www.obgyn.ufl.edu/ultrasound/MedinfoVersion/sec7/7_3.html. Retrieved 2007-11-28.

4. ̂ "Intrauterine Growth Restriction: Identification and Management - August 1998 - American Academy of Family Physicians". http://www.aafp.org/afp/980800ap/peleg.html. Retrieved 2007-11-28.
[hide] v • d • e
Certain conditions originating in the perinatal period / fetal disease (P, 760-779)
Maternal factors andcomplications of
pregnancy,labour and delivery
placenta: Placenta praevia · Placental insufficiency · Twin-to-twin transfusion syndrome
chorion/amnion: Chorioamnionitis
umbilical cord: Umbilical cord prolapse · Nuchal cord · Single umbilical artery
Length of gestationand fetal growth
Small for gestational age/Large for gestational age · Preterm birth/Postmature birth
Birth traumaCephalhematoma · Brachial plexus lesion (Erb's palsy, Klumpke paralysis)
By system
Respiratory
Intrauterine hypoxia · Infant respiratory distress syndrome · Transient tachypnea of the newborn · Meconium aspiration syndrome · pleural disease (Pneumothorax, Pneumomediastinum) · Wilson-Mikity syndrome · Bronchopulmonary dysplasia
CardiovascularPneumopericardium · Persistent fetal circulation
Haemorrhagic andhaematological/
hematologic disease
Vitamin K deficiency (Haemorrhagic disease of the newborn) · Hemolytic disease of the newborn (ABO HDN • Anti-Kell HDN • Rhesus c HDN • Rhesus D HDN • Rhesus E HDN) · Rh disease · Hydrops fetalis · Hyperbilirubinemia (Kernicterus, Neonatal jaundice)
Velamentous cord insertion
Digestive systemIleus · Necrotizing enterocolitis · Meconium peritonitis
Integument andtemperature regulation
Erythema toxicum

Nervous systemPeriventricular leukomalacia
Musculoskeletal system
Gray baby syndrome · muscle tone (Congenital hypertonia, Congenital hypotonia)
Other disorders
Perinatal infection (Congenital rubella syndrome, Neonatal herpes simplex) · Omphalitis · Neonatal sepsis (Group B streptococcal infection)
Stillbirth/Perinatal mortality
obstetric navs: pregnancy, conditions of mother/fetus/maternal transmission, eponymous signs, proc
Retrieved from "http://en.wikipedia.org/wiki/Small_for_gestational_age"Categories: Obstetrics | Pediatrics
Views
Article Discussion Edit this page History
Personal tools
Try Beta Log in / create account
Navigation
Main page Contents Featured content Current events Random article
Search
Interaction
About Wikipedia Community portal Recent changes Contact Wikipedia Donate to Wikipedia Help
Special:Search Go Search

Toolbox
What links here Related changes Upload file Special pages Printable version Permanent link Cite this page
Languages
Deutsch Español עברית
This page was last modified on 14 January 2010 at 12:20. Text is available under the Creative Commons Attribution-ShareAlike License;
additional terms may apply. See Terms of Use for details.Wikipedia® is a registered trademark of the Wikimedia Foundation, Inc., a non-profit organization.
Contact us Privacy policy About Wikipedia Disclaimers
AIIMS- NICU protocols 2007
Management of infants with intra-uterine growth restrictionAshok K Deorari, Ramesh Agarwal , Vinod K PaulDivision of Neonatology, Department of PediatricsAll India Institute of Medical SciencesAnsari Nagar, New Delhi –110029Address for correspondence:Dr Ashok DeorariProfessorDepartment of PediatricsAll India Institute of Medical SciencesAnsari Nagar, New Delhi 110029Email: [email protected] from www.newbornwhocc.org 1AIIMS- NICU protocols 2007

AbstractIntra-uterine growth restriction (IUGR) contributes to almost two-thirds of LBW infants born inIndia. Poor nutritional status and frequent pregnancies are common pre-disposing conditions inaddition to obstetric and medical problems during pregnancy. Growth restriction may besymmetrical or asymmetrical depending on the time of insult during pregnancy. The pathologicalinsult in an asymmetrical IUGR occurs during the later part of the pregnancy and has a brainsparingeffect. Common morbidities are more frequent in <3rd percentile group as compared to 3rd–10th percentile group. Guidelines for management of IUGR neonates in these two groups have beenprovided in the protocol.Downloaded from www.newbornwhocc.org 2AIIMS- NICU protocols 2007IntroductionNearly one third of neonates born in India are low birth weight (LBW), weighing less than 2500grams at birth. A baby’s low birth weight is either the result of preterm birth (before 37 completedweeks of gestation) or due to intrauterine growth restriction (IUGR). Later condition is akin tomalnutrition and may be present in both term and preterm infants. Neonates affected by IUGR areusually undernourished, undersized and therefore, low birth weight. Two-third LBW neonatesborn in India fall in this category1. Since IUGR neonates are more likely to suffer complicationsincluding cold stress and hypoglycemia, it is important that these infants are identified andmanaged appropriately at birth2. Even after recovering from neonatal complications, they remainmore prone to poor physical growth, poor neurodevelopmental outcome, recurrent infection andchronic diseases (hypertension, hyperlipidemia, diabetes mellitus, coronary heart disease) later inlife3.IUGR and SGA (Small-for-gestational age)Although both the terms are used inter-changeably and both denote malnutrition, there is a minordifference in the terminology. SGA a statistical definition, is used for neonates whose birth weight

is lower than (less than 10th percentile for that particular gestational age) population norms. IUGRis a clinical definition and includes neonates with clinical evidence of malnutrition. This may be inthe form of loose skin folds on the face and in the gluteal region, absence of subcutaneous fat andpeeling of skin. Although most IUGR infants would also be SGA, it is possible that a smallminority of IUGR infants may have birth weights above the 10th percentile. These morphologicalIUGR infants would behave like SGA infants and should be managed along the same lines as SGAinfants. For purposes of discussion in this paper, the term IUGR would include both the groups ofinfants .Downloaded from www.newbornwhocc.org 3AIIMS- NICU protocols 2007EtiologyPoor nutritional status of the mother and frequent pregnancies are the major cause of IUGR.Mothers with a weight of less than 40 kg and a height of less than 145 cm often give birth to SGAinfants. Insufficient nutritional intake during pregnancy also has an adverse effect on fetal weight.Maternal hypertension, pre-eclampsia, post-maturity, frequent pregnancies, multiple pregnancy,anemia, malaria and tobacco use are other causes of IUGR4-6. Chronic maternal diseases of heart,kidneys, lungs or liver may also lead to IUGR.Types of IUGRInfants with IUGR are often classified as having symmetrical (head circumference, length andweight equally affected) or asymmetrical (with relative head growth sparing) growth restriction.Infants with symmetric IUGR often have an earlier onset and are associated with causes that affecttotal fetal cell number including chromosomal, genetic, teratogenic, intra-uterine infections andsevere hypertensive etiologies. Asymmetric IUGR is often of a later onset, demonstratespreservation of blood flow to brain and is associated with poor maternal nutrition or late onsetexacerbation of maternal vascular disease (pre-eclampsia, chronic hypertension)7.Clinical features

IUGR or SGA infants are often term or near-term in gestation. Their birth weight usually fallsbelow the 10th percentile8 The neonate has an emaciated look and loose skin because of lack ofsubcutaneous tissue. These are particularly prominent over the buttocks and the thighs. They lookalert and are often plethoric. Comparison of the head circumference with chest circumference ishelpful in the identification of a SGA infant. In infants with appropriate growth, the head size isusually bigger than the chest by about 2-cm. In SGA infants, the head circumference usuallyDownloaded from www.newbornwhocc.org 4AIIMS- NICU protocols 2007exceeds the chest circumference by more than 3 cm. A preterm SGA infant would have acombination of clinical features suggestive of both, prematurity and IUGR9.Problems of SGA infantsCommon neonatal morbidities encountered in SGA infants born in our hospital are given in Table1. The common morbidities encountered in IUGR neonates include: (a) perinatal asphyxia, (b)hypothermia, (c) hypoglycemia and (d) polycythemia. These morbidities are commoner in themore severely growth restricted babies (<3rd percentile) as compared to babies in the 3rd to 10th percentile category.From August 2004 to July 2005, 144 SGA babies were born in our hospital. 24 (17%) developedhypoglycemia and 14 (10%) had polycythemia requiring partial exchange transfusion. Amongst 24babies with hypoglycemia 50% of the total episodes occurred at 2 h, 22% at 48 h, 11% each at 6and 12 h and only 4% each at 24 and 72 h of age. 12 (50%) had multiple episodes ofhypoglycemia. 3 babies were symptomatic and required intravenous fluid therapy. Rest weremanaged with supplementary oral feeds. Of 14 babies with polycythemia, only 3 weresymptomatic. Polycythemia was detected at 2 h in 50%, at 6 h in 29%, at 12 h in 14% and only 7%at 24 h of life. No cases of polycythemia were detected at 48 and 72 h of life.ManagementEarly delivery is indicated if there is arrest of fetal growth and pulmonary maturity is satisfactory.

Fetal hypoxia may necessitate emergency cesarean section and one should be prepared to receivean asphyxiated infant. If liquor is meconium stained and the neonate is depressed, endotrachealsuctioning is essential10. Infant should be screened for any congenital malformations. Based oninitial assessment, decision is taken to either keep the infant in nursery or with mother.Birth weight 3rd – 10th percentileDownloaded from www.newbornwhocc.org 5AIIMS- NICU protocols 2007In the absence of complications including perinatal asphyxia and respiratory distress, theseneonates may be managed with the mother (Table 2). Skin-to-skin care helps in maintainingtemperature and facilitates breast-feeding. Early initiation of breastfeeding and/ or assisted feedinghelps in averting hypoglycemia. Term SGA infants usually do not pose any serious difficultiesbecause they have no problems in direct breast-feeding. To avoid hypoglycemia, they should be putto breast within one hour of birth. However these infants are at risk of morbidities and should bemonitored regularly for hypoglycemia and polycythemia in the first 48-72 hours.Neonates with asymptomatic hypoglycemia should be supplemented with sugar fortified formulafeeds. This may be given with the help of a cup and spoon/ paladai. Neonates with normoglycemiaon regular feeds should be gradually weaned to exclusive breast-feeding within the next 3-4 days.Failure to maintain normoglycemia despite regular oral feeds should be treated with IV fluids.Neonates with symptomatic hypoglycemia should be shifted to a special care nursery and managedappropriately with a glucose bolus followed by a continuous glucose infusion at 6-8 mg/kg/min.Neonates with asymptomatic polycythemia and a hematocrit <75 maybe managed conservativelyby increasing fluid intake. The infant should receive regular (2-3 hourly) breast feeds with extrasupplementation. Infants with symptomatic polycythemia or hematocrit >75 should be managed bypartial exchange transfusion in the neonatal intensive care unit11.Birth weight <3rd percentile, gestation <35 weeks

Neonates with severe growth restriction (<3rd percentile) or with presence of complications shouldbe managed in the intensive care unit (Table 2). This group would include infants with perinatalasphyxia, symptomatic hypoglycemia, symptomatic polycythemia, prematurity (<35 weeks),respiratory distress and hypothermia. They should be monitored for hypoglycemia, polycythemiaand feed intolerance in the initial few days.Downloaded from www.newbornwhocc.org 6AIIMS- NICU protocols 2007Infants with gestation <30 weeks (birth weight <1200 grams) should be started on IV fluidsinitially and gradually weaned to oral feeds over the next few days. In the absence of othercomplications, oro-gastric feeds should be started for neonates >30 weeks (>1200 grams) andgradually shifted to katori-spoon/ paladai feeding. An infant on full oral feeds with spoon-feedingmay be tried on direct breast-feeding. These high-risk infants need to be observed for a minimumof 72 hours for hypoglycemia. Infants on full katori-spoon feeding and/ or breast-feeding may beshifted to the mother after 72 hours if she is confident of on going-care.Paladai/ spoon feedingFeeding with a spoon (or a similar device such as ‘paladai’) and katori (or any other receptaclesuch as cup) has been found to be safe in SGA infants8. This mode of feeding is a bridge betweengavage feeding and direct breast-feeding. It is based on the premise that neonates with a gestationof 30-32 weeks or more are in a position to swallow the feeds satisfactorily even though they maynot be good at sucking or coordinated sucking and swallowing. A medium sized katori and a small(1-2 ml size) spoon should be used. The spoon should be filled just short of the brim withexpressed milk, should be placed at the corner of mouth and milk should be allowed to flow intothe infant’s mouth slowly, avoiding any spillage. The infant would actively swallow the milk. Thisprocess should be repeated till the required amount has been fed. If the infant does not activelyaccept and swallow the feed, an attempt should be made to wake the infant with gentle stimulation.

If he is still sluggish, do not insist on this method. It is better to switch back to gavage feeds till theinfant is ready.SGA/IUGR babies with absent or reversed end-diastolic flow (AREDF) in umbilical arteryIn the IUGR fetus, hypoxaemia produces circulatory redistribution towards the brain and awayfrom the viscera and placenta, culminating in umbilical artery or aortic AREDF in the mostDownloaded from www.newbornwhocc.org 7AIIMS- NICU protocols 2007severely affected fetuses. The combination of antenatal and persisting postnatal disturbances of gutperfusion, interacting with the metabolic demands of feeding, may adversely affect intestinal tissueoxygenation, combining with stasis and immunological factors to contribute to the development ofNEC. A review by Dorling et al including 14 studies and 1178 neonates found higher risk of NECin IUGR babies with AREDF (odds ratio: 2.13; 95% CI: 1.49 to 3.03).12
Although evidence forfeeding strategy to be adopted in these babies is limited, it may be prudent to start and persist withminimal enteral nutrition for first 48-72 h of life.Long-term outcome and follow-upIUGR babies are at risk for poor growth and neuro-developmental outcome.3
We routinely followIUGR babies with birthweight below <3rd percentile and those with birthweight 3-10th percentile ifthey develop significant morbidities (e.g. hypoglycemia, polycythemia, birth asphyxia) duringhospital stay.Downloaded from www.newbornwhocc.org 8AIIMS- NICU protocols 2007References1. United Nations Childrens Fund and World Health Organization, Low Birthweight:Country,regional and global estimates. UNICEF, New York, 2004.2. Arora NK, Paul VK, Singh M. Morbidity and mortality in term infants with intrauterine growthretardation. J Trop Pediatr 1987;33: 186-9.3. Teberg AJ, Walther FJ, Pena IC. Mortality, morbidity, and outcome of the small-for-gestationalagepreterm infant. Semin Perinatol 1988;12: 84-94.4. Mavalankar DV, Gray RH, Trivedi CR, Parikh VC. Risk factors for small for gestational age

births in Ahmedabad, India. J Trop Pediatr 1994;40:285-90.5. Arora NK, Singh M, Paul VK, Bhargava VL. Etiology of fetal growth retardation in hospitalborn infants. Indian J Med Res 1987;85:395-400.6. Bhatia BD, Agarwal KN, Jain NP, Bhargava V. Growth pattern of intrauterine growth retarded(IUGR) infants in first nine months of life. Acta Pediatr Scand 1984;73:189-96.7. Singh M. Disorders of weight and gestation. In Care of the Newborn (Ed) Singh M. 5th Ed,1999, Sagar Publications, New Delhi pp 224-45.8. Singh M, Giri SK, Ramachandran K. Intrauterine growth curves of live-born infants. IndianPediatr 1974;11: 475-9.9. Paul VK. Management of LBW babies. In NNF Teaching Aids on Newborn Care. Ed DeorariAK. 2nd Ed, 1998, Noble Vision, New Delhi pp 25-3610. Niermayer S, Kattwinkel J, Van Reempts P, Nadkarni V, Phillips B, Zideman D et al.International guidelines for neonatal resuscitation. An excerpt from the guidelines 2000 forcardiopulmonary resuscitation and emergency cardiovascular care. International consensus onDownloaded from www.newbornwhocc.org 9AIIMS- NICU protocols 2007Science. Contributors and reviewers for the neonatal resuscitation guiidelines. Pediatrics2000;106:E29.11. Deorari AK, Paul VK, Shrestha L, Singh M. Symptomatic neonatal polycythemia: comparisonof partial exchange transfusion with saline versus plasma. Indian Pediatr 1995;32: 1167-7112. Dorling J, Kempley S, Leaf A. Feeding growth restricted preterm infants with abnormalantenatal Doppler results. Arch Dis Child Fetal Neonatal Ed. 2005;90:F359-63.Downloaded from www.newbornwhocc.org 10AIIMS- NICU protocols 2007Table 1: Common morbidities in SGA neonatesPeriod: Jan 1999 to Dec 00(n=156)Period: Aug 04 to Jul 05(n=144)Weight <3rd
percentile

(n=47)Weight 3rd-10th
percentile(n=109)Weight <10th
percentile(n=144)Birth asphyxiaTotalModerateSevere4 (8.5%)2210 (9.2%)8225 (17%)--HypoglycemiaTotalSymptomaticAsymptomatic12 (25.5%)6614 (12.8%)31124 (17%)321PolycythemiaTotalSymptomaticAsymptomatic14 (29.8%)31117 (15.6%)8914 (10%)

311Hypothermia 0 4 (3.7%) 19* (13.2%)*Includes 1 baby with hypothermia and 18 babies with cold stressDownloaded from www.newbornwhocc.org 11AIIMS- NICU protocols 2007Table 2: Management of SGA infantsCriteria for admission to Nursery- All SGA infants < 2 SD (3rd percentile)- Infants with gestational age < 35 wks- Infants with birth asphyxia, respiratory distress etc.Care of SGA infants with mothers (birth weight between 3rd and 10th percentile,gestation >35 wks)Early initiation of breast feeding (within 1 hour)Skin-to-skin care to maintain temperature, monitoring of cold stress by motherand health professionals.Monitor blood sugar, hematocritPrevent infectionsCare of SGA infants in Nursery (birth weight <3rd percentile or gestation <35 wks)Nurse in thermo neutral environmentIt stable, early initiation of feeds ( EBM).- Feed by orogastric tube or katori-spoon /paladai if gestation >32 wks- Initial intravenous fluids followed by orogastric or katori-spoon /paladai ifgestation <32 wksMonitor blood sugar, hematocritCare of SGA infants with absent or reversed en-diastolic blood flowAt higher risk of development of NECIf preterm (gestation <32 weeks): Nil per oral or on minimal enteral nutritionfor first 48-72 h of life followed by gradual advancement of feed volumeDownloaded from www.newbornwhocc.org 12AIIMS- NICU protocols 2007
Figure 1: Algorithm for management of SGA infants

SGA*Term (borderline) <35 wk<3rd percentile 3rd –10th percentileAdmit nursery Monitor with mother Admit nurseryBreastfeeding or katori-spoon Breastfeeding <30 wk – initial on IV30 – 34 wk orogastric or katori-spoon*Blood sugar, hematocrit, temperature monitoringDownloaded from www.newbornwhocc.org 13
PREMATURITY AND IUGRThe causes of neonatal hypoglycemia can be categorized according to associated disturbances in one or more of the processes required for normal hepatic glucose production that may lead to transient or prolonged episodes of hypoglycemia (Table 1 ). Hepatic glycogen stores are limited in both preterm infants, who have not experienced the period of rapid glycogen accumulation during late gestation, and small-for-gestational age (SGA) infants, who have not had adequate substrate supply available for glycogen synthesis, which puts these newborns at risk for hypoglycemia. IUGR due to placental
insufficiency with preservation of normal head size puts an added demand on the infant's already low glycogen stores because of the increased brain-to-bodyweight ratio. Postterm infants and infants of multiple gestations also may be at risk because of the presence of relative placental insufficiency. In addition to decreased glycogen availability, studies in preterm and IUGR infants have found altered patterns of insulin secretion, substrate metabolism, and hormonal responses to changes in blood glucose concentration compared with appropriate-for-gestational age (AGA) term infants.
University of Virginia Health SystemSkip Navigation
Health System
Calendars
Maps
A-Z Index
UVa
Home Why Choose UVa
Make an Appointment Patients & Visitors
Keyw ord or Nam HS Web Submit

Health Professionals Careers
UVa Health.com... where Answers are found
Newsletters Breast Health Diabetes Health Heart Health Men's Health Women's Health Parenting Mind & Body
Find a Doctor o Adult Congenital Heart and PregnancyDiabetes and PregnancyHigh-Risk ObstetricsReproductive
GeneticsTeen Health Maps & Directions Calendar of Events Clinical Trials Why Choose UVa
Topics
Search This Site En Español
High-Risk Pregnancy
Intrauterine Growth Restriction (IUGR)
What is intrauterine growth restriction (IUGR)?
Adolescent MedicineAllergy/Asthma/ImmunologyArthritis & RheumatologyBlood DisordersBurnsCancer
go
USSEARCH /UVAHealth/peds Go

Intrauterine growth restriction (IUGR) is a term used to describe a condition in which the fetus is smaller than expected for the number of weeks of pregnancy. Another term for IUGR is fetal growth restriction. Newborn babies with IUGR are often described as small for gestational age (SGA).
A fetus with IUGR often has an estimated fetal weight less than the 10th percentile. This means that the fetus weighs less than 90 percent of all other fetuses of the same gestational age. A fetus with IUGR also may be born at term (after 37 weeks of pregnancy) or prematurely (before 37 weeks).
Newborn babies with IUGR often appear thin, pale, and have loose, dry skin. The umbilical cord is often thin and dull-looking rather than shiny and fat. Babies with IUGR sometimes have a wide-eyed look. Some babies do not have this malnourished appearance but are small all-over.
What causes intrauterine growth restriction (IUGR)?
Intrauterine growth restriction results when a problem or abnormality prevents cells and tissues from growing or causes cells to decrease in size. This may occur when the fetus does not receive the necessary nutrients and oxygen needed for growth and development of organs and tissues, or because of infection. Although some babies are small because of genetics (their parents are small), most IUGR is due to other causes. Some factors that may contribute to IUGR include the following:
Maternal factors:
o high blood pressure o chronic kidney disease o advanced diabetes o heart or respiratory disease o malnutrition, anemia o infection o substance abuse (alcohol, drugs) o cigarette smoking
Factors involving the uterus and placenta:
o decreased blood flow in the uterus and placenta o placental abruption (placenta detaches from the uterus) o placenta previa (placenta attaches low in the uterus) o infection in the tissues around the fetus
Factors related to the developing baby (fetus):
o multiple gestation (twins, triplets, etc.) o infection o birth defects o chromosomal abnormality
Why is intrauterine growth restriction (IUGR) a concern?
IUGR can begin at any time in pregnancy. Early-onset IUGR is often due to chromosomal abnormalities, maternal disease, or severe problems with the placenta. Late-onset growth restriction (after 32 weeks) is usually related to other problems.

With IUGR, the growth of the baby's overall body and organs are limited, and tissue and organ cells may not grow as large or as numerous. When there is not enough blood flow through the placenta, the fetus may only receive low amounts of oxygen. This can cause the fetal heart rate to decrease placing the baby at great risk.
Babies with IUGR may have problems at birth including:
decreased oxygen levels
low Apgar scores (an assessment that helps identify babies with difficulty adapting after delivery)
meconium aspiration (inhalation of the first stools passed in utero), which can lead to difficulty breathing
hypoglycemia (low blood sugar)
difficulty maintaining normal body temperature
polycythemia (too many red blood cells)
Severe IUGR may result in stillbirth. It may also lead to long-term growth problems in babies and children.
How is intrauterine growth restriction (IUGR) diagnosed?
During pregnancy, fetal size can be estimated in different ways. The height of the fundus (the top of a mother's uterus) can be measured from the pubic bone. This measurement in centimeters usually corresponds with the number of weeks of pregnancy after the 20th week. If the measurement is low for the number of weeks, the baby may be smaller than expected.
Other diagnostic procedures may include the following:
ultrasoundUltrasound (a test using sound waves to create a picture of internal structures) is a more accurate method of estimating fetal size. Measurements can be taken of the fetus' head and abdomen and compared with a growth chart to estimate fetal weight. The fetal abdominal circumference is a helpful indicator of fetal nutrition.
Doppler flowAnother way to interpret and diagnose IUGR during pregnancy is Doppler flow, which use sound waves to measure blood flow. The sound of moving blood produces wave-forms that reflect the speed and amount of the blood as it moves through a blood vessel. Blood vessels in the fetal brain and the umbilical cord blood flow can be checked with Doppler flow studies.
mother's weight gainA mother's weight gain can also indicate a baby's size. Small maternal weight gains in pregnancy may correspond with a small baby.
How is intrauterine growth restriction (IUGR) managed?
Management of IUGR depends on the severity of growth restriction, and how early the problem began in the pregnancy. Generally, the earlier and more severe the growth restriction, the

greater the risks to the fetus. Careful monitoring of a fetus with IUGR and ongoing testing may be needed.
Some of the ways to watch for potential problems include the following:
fetal movement counting - keeping track of fetal kicks and movements. A change in the number or frequency may mean the fetus is under stress.
nonstress testing - a test that watches the fetal heart rate for increases with fetal movements, a sign of fetal well-being.
biophysical profile - a test that combines the nonstress test with an ultrasound to evaluate fetal well-being.
ultrasound - a diagnostic imaging technique which uses high-frequency sound waves and a computer to create images of blood vessels, tissues, and organs. Ultrasounds are used to view internal organs as they function, and to assess blood flow through various vessels. Ultrasounds are used to follow fetal growth.
Doppler flow studies - a type of ultrasound which use sound waves to measure blood flow.
Treatment for IUGR:
Although it is not possible to reverse IUGR, some treatments may help slow or minimize the effects. Specific treatments for IUGR will be determined by your physician based on:
your pregnancy, overall health, and medical history the extent of the disease your tolerance for specific medications, procedures, or therapies expectations for the course of the disease your opinion or preference
Treatments may include:
nutritionSome studies have shown that increasing maternal nutrition may increase gestational weight gain and fetal growth.
bedrestBedrest in the hospital or at home may help improve circulation to the fetus.
deliveryIf IUGR endangers the health of the fetus, then an early delivery may be necessary.
Prevention of intrauterine growth restriction:
Intrauterine growth restriction may occur, even when the mother is in good health. However, some factors may increase the risks of IUGR, such as cigarette smoking and poor maternal nutrition. Avoiding harmful lifestyles, eating a healthy diet, and getting prenatal care may help decrease the risks for IUGR. Early detection may also help with IUGR treatment and outcome.
Click here to view theOnline Resources page of this Web Site.

High-Risk Pregnancy Home
High-Risk Pregnancy Home Page Pregnancy Complications
Glossary
Online Resources
Site Index
Last modified on: February 12, 2004
Text Only Print this Page E-mail this Page
High-Risk Pregnancy PO Box 800224Charlottesville, VA 22908 434-924-3627
Maintained by Health Topics Contact© 2008 by the Rector and Visitors of the University of Virginia
Disclaimer | Privacy Policy | About this Site
Abnormal size at birthD: SGA: birth weight < 20th percentile for gestational age or < 2.5 kg.LGA: birth weight > 90th percentile for gestational age or > 4 kg.A: SGA: may be familial, constitutional, or due to IUGR.IUGR is defined as either symmetrical or asymmetrical:Asymmetrical IUGR: relative sparing of head circumference in relation toweight and length:. Due to impaired uteroplacental function 28 to maternal pre-eclampsia, DMor nutritional deficiency during the 3rd trimester.. Occurs when foetal growth rate in 3rd trimester exceeds maximal supplyfrom the placenta.. There is preferential sparing of the cerebral perfusion at times of foetaldistress.Symmetrical IUGR: head circumference, weight, and length are all proportionallyaffected to equivalent degrees:. Indicative of a prolonged period of poor intrauterine growth.. Caused by congenital intrauterine infections (TORCH) in the 1st trimester,genetic factors such as single gene deletions and chromosomal disorders,maternal smoking, drug and alcohol abuse, chronic medical conditions (e.g.CRF), malnutrition, or multiple pregnancies.LGA: macrosomia is a feature of infants of mothers with either gestational orpoorly controlled/undiagnosed DM.A/R: IUGR: previous SGA infant, low pre-pregnancy weight and poor pregnancyweight gain.E: SGA: affects by definition 20% of the population and varies with ethnic background.IUGR: 2/200 neonates; asymmetrical > symmetrical IUGR.LGA: affects by definition 20% of live births; is more common in developedcountries where there is a higher prevalence of DM.H&E:Antenatal: maternal examination and accurate dating aid diagnosis. Oligohydramniosand poor foetal movements are indications of placental insufficiency.Perinatal monitoring: foetal tachycardia, loss of variability of the baseline inthe foetal heart trace, and late decelerations may indicate foetal distress onCTG.Postnatal measurements: birth weight, length, and head circumference oncentile chart.P: See A.

I: Radiology: USS is the 18 method of diagnosing IUGR or macrosomia antenatally.Cordocentesis: percutaneous umbilical blood sampling may be used for detectionof hypoxia, lactic acidosis, hypoglycaemia, chromosomal analysis, andDNA diagnosis of congenital intrauterine infections.M: Antenatal: maternal bedrest and limitation of activity for severe IUGR.Perinatal: maternal administration of O2, continuous assessment of foetalwell-being.Delivery (IUGR): if foetus becomes hypoxic in utero, an emergencyCaesarean section is required.Macrosomia: induce at 38/40 to prevent complications in a unit with goodneonatal facilities.3
CONDITIONSAbnormal size at birth continuedC: IUGR foetus: intrauterine hypoxia, birth asphyxia, and death.IUGR infant: hypothermia (relatively large surface area), hypoglycaemia(poor fat and glycogen stores), hypocalcaemia, polycythaemia, and meconiumaspiration.LGA: birth asphyxia due to prolonged/difficult delivery, birth trauma, especiallyshoulder dystocia, hypoglycaemia in the neonatal period due to hyperinsulinism,and polycythaemia.P: Depends on the cause of abnormal size at birth. Infants with asymmetricalIUGR will rapidly put on weight in the postnatal period; symmetrical IUGRinfants are more likely to remain small permanently. Studies have shown thatIUGR infants are at "risk of developing "BP, Type II DM, and coronary heartdisease.4
CONDITIONSAcne vulgarisD: Inflammation of the pilosebaceous duct. Classified as mild, moderate, andsevere.A: Adolescent acne:. "Sebum production: androgenic stimulation of hyper-responsive pilosebaceousunits.. Impaired normal flow of sebum: obstruction of the pilosebaceous duct byhyperkeratosis.. Propioni acne bacteria: may play a role by producing cytokines and lipolyticenzymes.Infantile acne: <3 months of life; transient and usually due to maternalandrogens.A/R: Puberty, may " premenstrually, POS, excess cortisol (Cushing syndrome).E: Developed world: affects 79–95% of the adolescent population, peaking at14–18 years; tends to recede by early twenties.Developing world: acne incidence is considerably lower; likely combinationof environmental and genetic factors.H: Usually self-diagnosed, acute onset, greasy skin, may be painful.E: Open comedones: whiteheads; flesh-coloured papules.Closed comedones: blackheads; black colour is due to oxidation of the melaninpigment.Other features: pustules, nodules, cysts, scarring, and seborrhoea.Distribution: primarily affects the face, neck, chest, and back (where sebaceousglands are most numerous).P: Gross distension of the pilosebaceous follicle with neutrophil infiltration.Closed comedones may contain serous fluid. Severe acne can create fistulaebetween inflamed glands.I: Normally none required. Investigate for endocrine disorder if acne developsduring 2–10 years of age.Bloods: FSH, LH (if female, suspect POS).Urine: 24-h-urinary cortisol (if Cushing syndrome is suspected).M: Many cases may not need treatment. Indication for treatment based on classificationand degree of psychosocial impact. In severe acne, therapy should becommenced early to prevent scarring.Topical preparations:(1) Benzoyl peroxide; keratolytic agent, encourages skin peeling, and # numberof P. acnes (S/E: irritation and bleaching of clothes).(2) Vitamin A derivatives; tretinoin, may take 3–4 months to work.(3) Azelaic acid.Antibiotics:(1) Topical: clindamycin, erythromycin.(2) Systemic: tetracycline only in > 16 years. (S/E: discolours teeth and maysoften bones in children.)A gradual " in P. acne resistance to many antibiotics has been documented;growing need to use either appropriate antibiotics or change the therapeuticstrategy in favour of other regimens.

Isotretinoin (Roaccutane P.O.): vitamin A derivative, 4–6-month course onlyby specialist prescription for severe acne (S/E: teratogenic; females require OCP,hyperlipidaemia).Antiandrogens: in females only; OCP or cyproterone acetate.UVB: adjunctive therapy, but rarely used.Advice: improvement may not be seen for at least a couple of months, use nongreasycosmetics, wash face daily, moderate exposure to sunshine is beneficial.5
CONDITIONSAcne vulgaris continuedC: Physical: facial scarring (atrophic/keloid), hyperpigmentation of scars, 28 infectionand fistulae.Psychosocial: lack of self-confidence.P: Generally improves spontaneously over months/years. Persists into adulthoodin 22% of women and 3% of men.6
CONDITIONSAcquired female genital disordersD: Abnormalities of the female genital tract not present at birth.A: Labial adhesions: adherence of the labia minora in the midline; may give theappearance of absence of the vagina. A thin pale semi-translucent membranecovers the vaginal os. Trauma causes denudation of the epithelial layer of thelabia minora mucosa and leads to fibrous tissue formation; therefore sealingof the labia minora. Trauma can involve inflammatory conditions (vulvitis,vulvovaginitis), sexual abuse, or straddle injuries.Vulvovaginitis: pruritus, vulval pain, vulval erythema, vaginal discharge orbleeding. Usually associated with poor perineal hygeine, constipation, and atopicdermatitis caused by local irritants (bubble bath, soaps, shampoo) or by occlusiveclothing causing irritation. May be caused by trauma 28 to abuse; therefore thisshould be considered if other concerns are present.A/R: Vulvovaginitis is often misdiagnosed as a UTI due to its similar presentation.E: Labial adhesions: peak age: 3 months to 6 years, incidence: 1–2%.Vulvovaginitis: very common in <5-year-olds.H: Labial adhesions: usually asymptomatic and noted on routine examination.Some patients may leak urine when they stand after voiding.Vulvovaginitis: history should include toilet-training, type of nappy used,bad odour or dark discharge, scratching, history of eczema, allergic rhinitis, ordiarrhoea, tendency of child to insert objects, and any possible indication ofabuse.E: General: should be by a skilled clinician, in a well-lit room with a relaxed anddistracted child (mother reading book).Labial adhesions: the edges of the labia minora are sealed along the midline,beginning at the posterior fourchette and extending anteriorly towardsthe clitoris.Vulvovaginitis: commonly, only vulvitis will be detected, although vaginaldischarge and bleeding may also be present.P: See A.I: Exclude other vaginal disorders such as imperforate hymen or septate vaginaprior to treatment.Microbiology: vaginal swab if discharge present, MSU.Radiology: indirect cystourethrogram may show urinary retention behindthe fused labia, bladder distention þ=_ hydronephrosis in labial adhesions.M: Labial adhesions: oestrogen cream dissolves the adhesions in 90% of cases.Once adhesions have been lysed vasoline is used as prophylaxis for 1–2months.Vulvovaginitis:. Treat any underlying infection with appropriate antibiotics.. Education of adequate perineal hygiene and removal of potential irritants.C: Labial adhesions: without adequate treatment 20–40% will develop UTI.P: Labial adhesions: recurrence is common, therefore good follow-up isrequired.Vulvovaginitis: outcome good with improved perineal hygiene.7
CONDITIONS

Download our official FREE toolbarDictionary, Encyclopedia and Thesaurus - The Free Dictionary
1,867,474,407 visitors served.
T E X T forum mailing list For webmasters
TheFreeDictionary Google Bing
?
Word / Article Starts with Ends with Text
New: Language forums
Help the victims of the recent earthquake in Haiti
Dictionary/thesaurus
Medicaldictionary Legal
dictionaryFinancialdictionary
Acronyms
Idioms Encyclopedia Wikipediaencyclopedia
?
intrauterine growth retardation
Also found in: Dictionary/thesaurus, Acronyms, Encyclopedia, Wikipedia, Hutchinson
0.52 sec.
Ads by GoogleMPS VI, A Rare DisorderEarly signs of MPS VI Disorder often common symptoms. Learn more.www.mpsvi.com Truth About ScientologyLearn about beliefs, humanitarian efforts & more. Watch online videosScientology.org Meniere's SyndromeLearn about the Latest Advances for Meniere's Disease - Yours Free.www.menieres-guidebook.com
Intrauterine Growth Retardation
Definition
Intrauterine growth retardation (IUGR) occurs when the unborn baby is at or below the 10th weight percentile for his or her age (in weeks).
Description
There are standards or averages in weight for unborn babies according their age in weeks. When the baby's weight is at or below the 10th percentile for his or her age, it is called intrauterine growth retardation or fetal growth restriction. These babies are smaller than they should be for their age. How much a baby weighs at birth depends not only on how many weeks old it is, but the rate at which it has grown. This growth process is complex and delicate. There are
?Page tools
Printer friendlyCite / linkEmail
FeedbackAdd definition
Advertisement (Bad banner? Please let us
know)
Related Ads
▪ Baby Shower Games▪ Pregnancy
▪ Children Projects▪ Gas Causes▪ Con
utf-8
intrauterine grow th retardation
4 Search

three phases associated with the development of the baby. During the first phase, cells multiply in the baby's organs. This occurs from the beginning of development through the early part of the fourth month. During the second phase, cells continue to multiply and the organs grow. In the third phase (after 32 weeks of development), growth occurs quickly and the baby may gain as much as 7 ounces per week. If the delicate process of development and weight gain is disturbed or interrupted, the baby can suffer from restricted growth.IUGR is usually classified as symmetrical or asymmetrical. In symmetrical IUGR, the baby's head and body are proportionately small. In asymmetrical IUGR, the baby's brain is abnormally large when compared to the liver. In a normal infant, the brain weighs about three times more than the liver. In asymmetrical IUGR, the brain can weigh five or six times more than the liver.
Causes and symptoms
Doctors think that the two types of IUGR may be linked to the time during development that the problem occurs. Symmetrical IUGR may occur when the unborn baby experiences a problem during early development. Asymmetrical IUGR may occur when the unborn baby experiences a problem during later development. While not true for all asymmetrical cases, doctors think that sometimes the placenta may allow the brain to get more oxygen and nutrition while the liver gets less.There are many IUGR risk factors involving the mother and the baby. A mother is at risk for having a growth restricted infant if she:
Has had a previous baby who suffered from IUGR Is small in size Has poor weight gain and nutrition during pregnancy Is socially deprived Uses substances (like tobacco, narcotics, alcohol) that can cause
abnormal development or birth defects Has a vascular disease (like preeclampsia) Has chronic kidney disease Has a low total blood volume during early pregnancy Is pregnant with more than one baby Has an antibody problem that can make successful pregnancy difficult
(antiphospholipid antibody syndrome).
Additionally, an unborn baby may suffer from IUGR if it has:
Exposure to an infection, including German measles (rubella), cytomegalovirus, tuberculosis, syphilis, or toxoplasmosis
A birth defect (like a severe cardiovascular defect) A chromosome defect, especially trisomy 18 (Edwards' syndrome) A primary disorder of bone or cartilage A chronic lack of oxygen during development (hypoxia) Placenta or umbilical cord defects Developed outside of the uterus.
Website▪ Pregnancy Signs▪ Pregnancy Problem▪ Flatulence Causes
ceiving a Baby▪ Newborn Clothing▪ Infant Clothes
?My Word List
Add current page to the list
Advertisement (Bad banner? Please let us
know)
?Charity
Feed a hungry child - donate to
school feeding program
Advertisement (Bad banner? Please let us
know)

Key terms
Preeclampsia — Hypertension (high blood pressure) during pregnancy.
Diagnosis
IUGR can be difficult to diagnose and in many cases doctors are not able to make an exact diagnosis until the baby is born. A mother who has had a growth restricted baby is at risk of having another during a later pregnancy. Such mothers are closely monitored during pregnancy. The length in weeks of the pregnancy must be carefully determined so that the doctor will know if development and weight gain are appropriate. Checking the mother's weight and abdomen measurements can help diagnose cases when there are no other risk factors present. Measuring the girth of the abdomen is often used as a tool for diagnosing IUGR. During pregnancy, the healthcare provider will use a tape measure to record the height of the upper portion of the uterus (the uterine fundal height). As the pregnancy continues and the baby grows, the uterus stretches upward in the direction of the mother's head. Between 18 and 30 weeks of gestation, the uterine fundal height (in cm.) equals the weeks of gestation. If the uterine fundal height is more than 2-3 cm below normal, then IUGR is suspected. Ultrasound is used to evaluate the growth of the baby. Usually, IUGR is diagnosed after week 32 of pregnancy. This is during the phase of rapid growth when the baby should be gaining more weight. IUGR caused by genetic factors or infection may sometimes be detected earlier.
Treatment
There is no treatment that improves fetal growth, but IUGR babies who are at or near term have the best outcome if delivered promptly. If IUGR is caused by a problem with the placenta and the baby is otherwise healthy, early diagnosis and treatment of the problem may reduce the chance of a serious outcome.
Prognosis
Babies who suffer from IUGR are at an increased risk for death, low blood sugar (hypoglycemia), low body temperature (hypothermia), and abnormal development of the nervous system. These risks increase with the severity of the growth restriction. The growth that occurs after birth cannot be predicted with certainty based on the size of the baby when it is born. Infants with asymmetrical IUGR are more likely to catch up in growth after birth than are infants who suffer from prolonged symmetrical IUGR. However, as of 1998, doctors cannot reliably predict an infant's future progress. Each case is unique. Some infants who have IUGR will develop normally, while others will have complications of the nervous system or intellectual problems like learning disorders. If IUGR is related to a disease or a genetic defect, the future of the infant is related to the severity and the nature of that disorder.

Resources
BooksCunningham, F. Gary, et al. Williams Obstetrics. 20th ed. Stamford: Appleton & Lange, 1997.Gale Encyclopedia of Medicine. Copyright 2008 The Gale Group, Inc. All rights reserved.
intrauterine growth retardation
n. Abbr. IUGR Birth weight that is below the tenth percentile for gestational age. Also called intrauterine growth restriction.The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company. Published by Houghton Mifflin Company. All rights reserved.
intrauterine growth retardation, an abnormal process in which the development and maturation of the fetus are impeded or delayed more than two deviations below the mean for gestational age, sex, and ethnicity. It may be caused by genetic factors, maternal disease, or fetal malnutrition that results from placental insufficiency. See also growth retardation, small for gestational age infant. Mosby's Medical Dictionary, 8th edition. © 2009, Elsevier.
intrauterinewithin the uterus.
intrauterine contraceptive device a mechanical device inserted into the uterine cavity for the purpose of contraception. These devices, used in human gynecology, have been used in draft cattle in Asia for many years. Used occasionally also in dogs. Called also IUD.intrauterine growth retardation failure to grow properly in utero in stature, as measured by crown to rump measurement. Pituitary dwarfism in cattle and runting in piglets and puppies are typical examples.intrauterine medication medication applied to the uterus via a cervical catheter, or manually in the recently birthed mare, sow or cow.intrauterine therapy is a common practice in food animals. Infusion of fluid material or manual placement of solid materials are the usual methods employed. The method has the advantage of achieving maximum concentration of the medicament at the endometrium but only low concentrations are achieved in the deeper layers. See also infusion.Saunders Comprehensive Veterinary Dictionary, 3 ed. © 2007 Elsevier, Inc. All rights reserved
intrauterine growth retardation
Fetal growth restriction Neonatology A generic term for any delay in achieving

intrauterine developmental milestones, most commonly related to maternal drug, tobacco and alcohol abuse; IUGR affects high-risk infants with perinatal asphyxia, hypoglycemia, hypothermia, pulmonary hemorrhage, meconium aspiration, necrotizing enterocolitis, polycythemia and complications of infections, malformations and syndromes; IUGR fetuses have weight < 10th percentile for gestational age, abdominal circumference < 2.5th percentile Types Symmetric–body is proportionately small; asymmetric–head is disproportionately bigger than body, which implies undernourishment–growth of vital organs–heart, brain is at expense of liver, muscle and fat, often due to placental insufficiency; IUGR is the 2nd most common–after prematurity–cause of perinatal M&M; it affects ±5% of the general obstetric population. See Low birthweight, Small for gestational age. Intrauterine growth restriction Placental insufficiency • Unexplained elevated maternal alpha- fetoprotein level • Idiopathic • Preeclampsia • Chronic maternal disease • Cardiovascular disease • Diabetes • Hypertension Abnormal placentation • Abruptio placentae • Placenta previa • Infarction • Circumvallate placenta • Placenta accretia • Hemangioma Genetic disorders • Family history • Trisomy 13, 18 and 21 • Triploidy • Turner's syndrome (some cases) • Malformations Immunologic • Antiphospholipid syndrome Infections • Cytomegalovirus • Rubella • Herpes • Toxoplasmosis Metabolic • Phenylketonuria Other • Poor maternal nutrition • Substance abuse (smoking, alcohol, drugs) • Multiple gestation • Low socioeconomic status

McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc.
How to thank TFD for its existence? Tell a friend about us, add a link to this page, add the site to iGoogle, or visit webmaster's page for free fun content. Link to this page:
Please bookmark with social media, your votes are noticed and appreciated:
Ads by GoogleAmos Grunebaum, MD FACOGObstetrician & Gynecologist Maternal-Fetal MedicineGrunebaum.com Bilirubin Assay KitColorimetric 96-well/cuvet assays Fast, convenient and reliablewww.bioassaysys.com "Restless Leg Syndrome"A Proven Restless Leg Syndrome Cure That Always Gives "Instant Relief"www.AllCalm.com
? Mentioned in
? References in periodicals archive
Antepartum Testingexpanded rubella syndromeFGRgrowth retardationHigh-risk pregnancyIntrauterine growth restrictionIUGRlow birth weightplacental insufficiencypreeclampsia
probationpsychomotor retardationrestrictionretardationrevocationsmall for gestational ageTurner syndrometwin-to-twin transfusion syndromevaricella embryopathy
More results
Fetal transfusion syndrome, fetofetal transfusion syndrome, stuck twin syndrome Obstetrics Intrauterine growth retardation in 1 twin due to an artery-to-artery vascular shunting, which may occur in a diamnionic-dichorionic placenta
Hemodynamics and cardiology; neonatology questions and controversies by SciTech Book News
We found evidence of associations between exposure to specific HAAs and term low birth weight as well as intrauterine growth retardation and for exposure to the five regulated HAAs (HAAS) and term low birth weight.
Late pregnancy exposures to disinfection by-products and ... by Reif, John S. / Environmental
Health PerspectivesEvery 17 parts per billion increase in daily ozone levels during a woman's third trimester increases the risk of intrauterine growth retardation by 20 percent.
OZONE LEVEL POSES RISK TO WOMEN BABIES BORN UNDERWEIGHT by Daily News (Los
Angeles, CA)More results
<a href="http://medical-dictionary.thefreedictionary.com/intrauterine+grow

Medical browser ? ? Full browserintrauterine amputationintrauterine catheterintrauterine contraceptiveintrauterine deviceintrauterine fractureintrauterine growth curveIntrauterine growth restrictionintrauterine growth retardationintrauterine inseminationintrauterine pressure catheterintrauterine transfusionintravasationintravascularintravascular brachytherapyintravascular coagulation test
Intrauterine devicesIntrauterine devicesIntrauterine devicesIntrauterine devicesIntrauterine devicesintrauterine fetal deathIntrauterine fetal growth retardationIntrauterine fetal growth retardationIntrauterine fetal growth retardationintrauterine fractureintrauterine fractureintrauterine fractureintrauterine fractureintrauterine fractureintrauterine fractureintrauterine growth curve
intrauterine growth restrictionintrauterine growth restrictionintrauterine growth restrictionintrauterine growth restrictionintrauterine growth restrictionintrauterine growth restrictionintrauterine growth restrictionintrauterine growth restrictionintrauterine growth retardationIntrauterine Growth Retardation Low Birth WeightIntrauterine hypoxiaintrauterine infusionintrauterine infusionintrauterine infusionintrauterine infusionintrauterine infusionintrauterine infusion
Intrauterine inseminationIntrauterine inseminationIntrauterine inseminationIntrauterine inseminationIntrauterine inseminationintrauterine medicationintrauterine medicationintrauterine medicationIntrauterine PregnancyIntrauterine PressureIntrauterine Pressure CatheterIntrauterine Pressure CatheterIntraUterine Systemintrauterine therapyintrauterine therapyintrauterine therapy
Medical Dictionary
TheFreeDictionary Google
?
Word / Article Starts with Ends with Text
Free Tools:For surfers: Free toolbar & extensions | Word of the Day | Bookmark | Help For webmasters: Free content | Linking | Lookup box | Double-click lookup | Partner with us
Disclaimer | Privacy policy | Feedback | Copyright © 2010 Farlex, Inc. All content on this website, including dictionary, thesaurus, literature, geography, and other reference data is for informational
purposes only. This information should not be considered complete, up to date, and is not intended to be used in place of a visit, consultation, or advice of a legal,
medical, or any other professional. Terms of Use.
4 utf-8
Search

Causes and Symptoms
The two types of IUGR described previously contribute to IUGR according to the development at that stage. Symmetrical IUGR may occur when the unborn baby experiences a problem during early development. Asymmetrical IUGR may occur when the unborn baby experiences a problem during later development. In general, most physicians believe that IUGR is the consequence of a disease process within one or more of the three partitions that maintain and regulate fetal growth, i.e., the maternal compartment, the placenta, or the fetus.
In consideration of risk factors uteroplacental insufficiency contributes to 80 percent of IUGR due to the following maternal causes:
deficient supply of nutrients smoking malnutrition anemia drug abuse vascular diseases, i.e., high blood pressure chronic kidney disease severe diabetes multiple gestation
Intrauterine growth retardation (IUGR)
Conditions associated with IUGR
Maternal history Alcohol useCocaine useSmokingMalnutritionUse of prescription drugs warfarin(Coumadin, Panwarfarin) and phenytoin(Dilantin)Prior history of IUGR pregnancyResiding at altitude over 5,000 ft (1,500 m)
Medical conditions (of mother) Chronic hypertensionPreeclampia early in gestationDiabetes mellitusSystemic lupus erythematosusChronic kidney diseaseInflammatory bowel diseaseSevere lung disease
Infectious diseases SyphilisCytomegalovirusToxoplasmosisRubella

Intrauterine growth retardation (IUGR)
Conditions associated with IUGR
Hepatitis BHerpes simplex virus 1 or 2HIV-1
Congenital disorders (of fetus) Trisomy 21 (Down syndrome)Trisomy 18 (Edwards syndrome)Trisomy 13 (Patau syndrome)Turner's syndrome
antigen/antibody reactions, i.e., lupus, antiphospholipid antibody syndrome (APA) primary placental causes, i.e., extensive placental infarctions, chronic placental
separation, placenta previa
Primary fetal causes contribute to 20 percent of IUGR and include the following:
exposure to an infection, i.e., rubella (German measles), cytomegalovirus, syphilis, or toxoplasmosis
birth defects, i.e., congenital heart disease, genitourinary anomalies, central nervous system defects
chromosomal abnormalities, i.e., trisomy 13, 18, or 21 primary bone or cartilage disorder decreased intrinsic growth, symmetrical IUGR

While most fetuses with IUGR usually have no complications, there is an increased risk for intrapartum asphyxia, neonatal hypoglycemia and hypocalcemia, meconium aspiration, and neurodevelopmental delays. The following summarizes these complications:
Intrapartum AsphyxiaBecause the fetus is compromised with IUGR, its ability to tolerate the stress of labor is decreased. Therefore, when uterine contractions occur and the flow of blood to the fetus is diminished with each contraction, the fetus with IUGR may not be able to adapt. This leads to an imbalance between the ability of the placenta to supply the fetus with oxygen and nutrients and the need for these substances. When an imbalance occurs, this may lead to an accumulation of

byproducts resulting in acidosis which can be harmful. If intrapartum asphyxia is allowed to progress, irreversible brain damage can occur.Medical Literature
Neonatal Hypoglycemia and HypocalcemiaAs the result of IUGR, a newborn may be deficient in glucose (sugar) and calcium. The lack of these important substances can result in significant compromise to the newborn and result in neurological damage.Medical LiteratureMedical Literature
Meconium AspirationThis occurs when the fetus defecates in the uterus resulting in the appearance of a brown, murky substance. Since the contents from the fetal bowel contains many substances that can be harmful to the fetus if swallowed, meconium aspiration is of major concern. In severe forms, the newborn may develop lung disease resulting in respiratory and cardiovascular complications that could lead to neonatal death.Medical Literature
Neurodevelopmental DelayA number of studies have shown that fetuses with significant IUGR are at higher risk for developmental delays, cardiovascular disease, and other problems later in life. For these reasons, and those stated above, it is important to identify the fetus with IUGR and manage the pregnancy accordinglyMedical Literature

![Intensive Care - Neonatal / Special Care NurseryB-0390] Intensive Care... · The Intensive Care – Neonatal / Special Care Nursery HPU was originally developed for NSW Health and](https://img.pdfslide.us/doc/110x75/5e206e3f4ac3f2591909ccbf/intensive-care-neonatal-special-care-nursery-b-0390-intensive-care-the.jpg)