-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 1
MEDICAL AND SURGICAL NURSING
Integumentary System
Lecturer: Mark Fredderick R. Abejo RN,MAN
________________________________________________
Integument Skin
The skin is the largest organ of the body
As the external covering of the body, the skin performs the
vital function of protecting internal body structures from
harmful microorganisms and substances.
FUNCTIONS:
1. Protection Covers and protects the entire body from
microorganisms
Protects from UV rays melanin (pigment in the skin)
Keratin a protein in the outermost layer of the skin waterproofs
and toughens skin and protects from excessive water loss, resists
harmful
chemicals, and protects against physical tears
2. Regulation
Maintains normal body temperature by regulating sweat secretion
and regulating the flow of blood
close to the body surface.
Evaporation of sweat from the body surface
Radiation of heat at the body surface due to the dilation of
blood vessels close to
the skin
Excessive heat loss causes shivering (contraction of skeletal
muscle) increasing heat production and
goosebumps (contraction of arrector pili muscle)
pulling hair shaft vertical, creating an insulated air
space over the skin.
3. Absorption
Absorbs oxygen and carbon dioxide and UV rays Steroids
(hydrocortisone) and fat-soluble vitamins
(ie D) are readily absorbed
Topical medications motion sickness patch etc
4. Synthesis
Skin produces melanin, keratin, vitamin D Melanin protects the
skin from UV rays; determines
skin color
Keratin helps waterproof the skin and protects from abrasions
and bacteria
Vitamin D stimulated by UV light. Enters blood and helps develop
strong healthy bones. Vitamin D
deficiency causes Rickets
5. Sensory
Sensory nerve endings tell about environment They respond to
heat, cold, pressure, touch,
vibration, pain
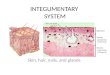
LAYERS
A. Epidermis
Avascular outermost layer Stratified squamous epithelium
Composed of keratinocytes (produce keratin
responsible for formation of hair and nails) and
melanocytes (produce melanin).
Form the appendages (hair and nails) and glands Epidermis
Stratum basale Stratum granulosum Stratum spinosum Stratum
lucidum Stratum corneum
B. Dermis
Layer beneath the epidermis composed of connective tissues.
Contains lymphatics, nerves and blood vessels. Elasticity of the
skin results from presence of
collagen, elastin and reticular fibers.
Responsible for nourishing the epidermis.
C. Subcutaneous layer
Layer beneath the dermis. Composed of loose connective tissues
and adipose
cells.
Stores fat. Important for thermoregulation.
APPENDAGES
Hair
Covers most of the body surface (except the palms, soles, lips,
nipples and parts of the external
genitalia).
Hair follicles: tube-like structures, derived from the
epidermis, from which hair grows.
Functions as protection from external elements and from
trauma.
Protects scalp from ultraviolet rays and cushions blows.
Eyelashes, hair in nostrils and in ears keep particles from
entering organ.
Hair growth controlled by hormonal influences and by blood
supply.
Scalp hair grows for 2 to 5 years. Approximately 50 hairs are
lost each day. Sustained hair loss of more than 100 hairs each
day
usually indicates that something is wrong
Nails
Dense layer of flat, dead cells, filled with keratin. Systemic
illnesses may be reflected by changes in
the nail or its bed:
Clubbing Beaus line
Glands
Eccrine sweat glands are located all over the body and produce
inorganic sweat which participate in
heat regulation.
Apocrine sweat glands are odiferous glands, found primarily in
the axillary, areolar, anal and pubic
areas; the bacterial decomposition of organic sweat
causes body odor.
Sebaceous glands are located all over the body except for the
palms and soles; produce sebum.
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 2 ASSESSMENT
Health History
Presenting problem Changes in the color and texture of the
skin,
hair and nails.
Pruritus Infections Tumors and other lesions Dermatitis
Ecchymoses Dryness
Lifestyle practices Hygienic practices Skin exposure
Nutrition / diet Intake of vitamins and essential nutrients
Water and Food allergies
Use of medications Steroids Antibiotics Vitamins Hormones
Chemotherapeutic drugs
Past medical history Renal and hepatic disease Collagen and
other connective tissue diseases Trauma or previous surgery Food,
drug or contact allergies
Family medical history Diabetes mellitus Allergic disorders
Blood dyscrasias Specific dermatologic problems Cancer
Physical Examination
Color Areas of uniform color Pigmentation Redness Jaundice
Cyanosis
Vascular changes Purpuric lesions
Ecchymoses Petechiae
Vascular lesions Angiomas Hemangiomas Venous stars
Lesions Color Type Size Distribution Location Consistency
Grouping
Annular Linear Circular Clustered
Edema (pitting or non-pitting) Moisture content Temperature
(increased or decreased;
distribution of temperature changes)
Texture Mobility / Turgor
Effects of Aging in the Skin
Skin vascularity and the number of sweat and sebaceous glands
decrease, affecting
thermoregulation.
Inflammatory response and pain perception diminish.
Thinning epidermis and prolonged wound healing make elderly more
prone to injury and skin
infections.
Skin cancer more common.
LABORATORY / DIAGNOSTIC STUDIES
Blood chemistry / electrolytes: calcium, chloride, magnesium,
potassium, sodium
Hematologic studies Biopsy
Removal of a small piece of skin for examination to determine
diagnosis
Nursing Interventions Preprocedure
- Secure consent
- clean site
Postprocedure place specimen in a clean container & send to
pathology
laboratory
- use aseptic technique for biopsy site dressing, assess site
for
bleeding & infection
- instruct px to keep dressing in place for 8hrs & clean
site daily
- instruct the patient to keep biopsied area dry until
healing
occur
Skin Culture Used for microbial study Viral culture is
immediately placed on ice Obtain prior to antibiotic
administration
Woods Light Examination Skin is viewed through a Woods glass
under UV
Nursing Interventions
Preprocedure darken room
Postprocedure assist px in adjusting to light
Skin testing Administration of allergens or antigens on
the surface of or into the dermis to
determine hypersensitivity
Types: Patch Prick Intradermal
DIAGNOSIS
Impaired skin integrity Pain Body image disturbance Risk for
infection Ineffective airway clearance Altered peripheral tissue
perfusion
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 3 PLANNING AND
IMPLEMENTATION
Goals Restoration of skin integrity. The patient will experience
relief of pain. The patient will adapt to changes in
appearance.
The patient will be free from infection. Maintenance of
effective airway
clearance.
Maintenance of adequate peripheral tissue perfusion.
Interventions: Skin Grafts Replacement of damaged skin with
healthy skin to provide protection of
underlying structures or to reconstruct
areas for cosmetic or functional purposes.
Sources: Autograft patients own skin Isograft skin from a
genetically
identical person
Homograft or allograft cadaver of same species
Heterograft or xenograft skin from another species
Nursing care: Preoperative Donor site: Cleanse with
antiseptic soap the night before
and morning of surgery as ordered.
Recipient site: Apply warm compresses and topical
antibiotics
as ordered.
Nursing care: Postoperative Donor site:
Keep area covered for 24 to 48 hours.
Use bed cradle to prevent pressure and provide greater
air circulation.
Outer dressing may be removed 24 to 72 hours post-
surgery; maintain fine mesh
gauze until it falls of
spontaneously.
Trim loose edges of gauze as it loosens with healing.
Administer analgesic as ordered (more painful than
recipient site).
Recipient site: Elevate site when possible. Protect from
pressure through
the use of a bed cradle.
Apply warm compresses as ordered.
Assess for hematoma, fluid accumulation under graft.
Monitor circulation distal to the graft.
Provide emotional support and monitor behavioral
adjustments;
refer for counseling if needed.
Provide client teaching and discharge planning concerning:
Applying lubricating lotion to maintain moisture on the
surface
of healed graft for at least 6 to 12
months.
Protecting grafted skin from direct sunlight for at least 6
months.
Protecting graft from physical injury.
Need to report changes in graft. Possible alteration in
pigmentation
and hair growth; ability to sweat
lost in most grafts.
Sensation may or may not return.
EVALUATION
Healing of burned areas; absence of drainage, edema and
pain.
Relaxed facial expression/body posture. Changes into
self-concept without negating self-
esteem
Achieves wound healing Lungs clear to auscultation Palpable
peripheral pulses of equal quality
Disorders of the Integumentary System
Primary Lesions of the Skin
Macule is a small spot that is not palpable and is less than 1
cm in diameter
Patch is a large spot that is not palpable & that is > 1
cm.
Papule is a small superficial bump that is elevated & that
is < 1 cm.
Plaque is a large superficial bump that is elevated & > 1
cm.
Nodule is a small bump with a significant deep component &
is < 1 cm.
Tumor is a large bump with a significant deep component & is
> 1 cm.
Cyst is a sac containing fluid or semisolid material, ie. cell
or cell products.
Vesicle is a small fluid-filled bubble that is usually
superficial & that is < 0.5 cm.
Bulla is a large fluid-filled bubble that is superficial or deep
& that is > 0.5 cm.
Pustule is pus containing bubble often categorized according to
whether or not they are related to hair
follicles:
follicular - generally indicative of local infection
folliculitis - superficial, generally multiple furuncle - deeper
form of folliculitis carbuncle - deeper, multiple follicles
coalescing
Secondary lesions of the Skin
Scale is the accumulation or excess shedding of the stratum
corneum.
Scale is very important in the differential diagnosis since its
presence indicates that the
epidermis is involved.
Scale is typically present where there is epidermal
inflammation, ie. psoriasis, tinea,
eczema
Crust is dried exudate (ie. blood, serum, pus) on the skin
surface.
Excoriation is a loss of skin due to scratching or picking.
Lichenification is an increase in skin lines & creases from
chronic rubbing.
Maceration is raw, wet tissue.
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 4
Fissure is a linear crack in the skin; often very painful.
Erosion is a superficial open wound with loss of epidermis or
mucosa only
Ulcer is a deep open wound with partial or complete loss of the
dermis or submucosa
Distinct Lesions of the Skin
Wheal or hive describes a short lived (< 24 hours),
edematous, well circumscribed papule or plaque
seen in urticaria.
Burrow is a small threadlike curvilinear papule that is
virtually pathognomonic of scabies.
Comedone is a small, pinpoint lesion, typically referred to as
whiteheads or blackheads.
Atrophy is a thinning of the epidermal and/or dermal tissue.
Keloid overgrows the original wound boundaries and is chronic in
nature.
Hypertrophic scar on the other hand does not overgrow the wound
boundaries.
Fibrosis or sclerosis describes dermal scarring/thickening
reactions.
Milium is a small superficial cyst containing keratin
(usually
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 5
Assessment findings: Appearance of lesions is variable and
fluctuating.
Systemic symptoms absent.
Psychologic problems such as social withdrawal, low self-esteem,
feelings of being
ugly. Pharmacologic Therapy
Benzoly Peroxide
Oral Antibiotics: Tetracycline, Doxycycline, Minocycline
Oral Retinoids: Isotretinion (Accutane) Note: commone side
effect, is cheilitis inflammation of lips
Hormone Therapy: Estrogen-progesterone preparation.
Nursing Management: Elimination of food products associated with
a
flare-up of acne such as chocolate, cola and
fried foods
Milk products should be promoted Advise the client to wash face
at least twice a
day with mild soap.
Provide positive reassurance, listening actively and being
sensitive the feelings of the patient.
Discuss over-the-counter products and their effects.
Patients are instructed to avoid manipulation of pimples or
blackheads. Squeezing merely
worsens the problem.
BACTERIAL INFECTIONS
Impetigo
Is a superficial bacterial skin infection most common among
children 2 to 6 years old.
It is primarily caused by Staphylococcus aureus, and sometimes
by Streptococcus pyogenes
Impetigo generally appears as honey-colored scabs formed from
dried serum, and is often found on the
arms, legs, or face.
The infection is spread by direct contact with lesions or with
nasal carriers.
The incubation period is 13 days. Dried streptococci in the air
are not infectious to intact
skin. Scratching may spread the lesions.
The lesions begin as small, red macules which quickly become
discrete, thin-walled vesicles that
soon ruptured and become coved with a loosely
adherent honey-yellow crust.
Medical Management: Topical or oral antibiotics are usually
prescribed:
- Benzathine penicillin
- Penicillinase-Resistant- cloxacillin
- Penicillin-Allergic- erythromycin
Treatment may involve washing with soap and water and letting
the impetigo dry in the air.
Mild cases may be treated with bactericidal ointment, such as
fusidic acid, mupirocin,
chloramphenicol or neosporin, which in some
countries may be available over-the-counter.
Nursing Management: Good hygiene practices can help prevent
impetigo from spreading. Those who are
infected should use soap and water to clean
their skin and take baths or showers regularly.
Non-infected members of the household should pay special
attention to areas of the
skin that have been injured, such as cuts,
scrapes, bug bites, areas of eczema, and
rashes. These areas should be kept clean and
covered to prevent infection.
In addition, anyone with impetigo should cover the impetigo
sores with gauze and tape.
All members of the household should wash their hands thoroughly
with soap on a regular
basis.
It is also a good idea for everyone to keep their fingernails
cut short to make hand
washing more effective.
Contact with the infected person and his or her belongings
should be avoided, and the
infected person should use separate towels for
bathing and hand washing.
If necessary, paper towels can be used in place of cloth towels
for hand drying. The
infected person's bed linens, towels, and
clothing should be separated from those of
other family members, as well.
While suffering from impetigo it is best to stay indoors for a
few days to stop any
bacteria getting into the blisters and making
the infections worse.
FOLLICULAR DISEASES
Folliculitis
Is the inflammation of one or more hair follicles. Folliculitis
starts when hair follicles are damaged by
friction from clothing, an insect bite, blockage of
the follicle, shaving or too tight braids too close to
the scalp traction folliculitis.
In most cases of folliculitis, the damaged follicles are then
infected with the bacteria Staphylococcus
Symptoms: rash (reddened skin area) pimples or pustules located
around a hair
follicle
o may crust over o typically occur on neck, axilla, or
groin area
o may be present as genital lesions itching skin spreading from
leg to arm to body through
improper treatment of antibiotics
Furuncles (Boils)
Is a skin disease caused by the infection of hair follicles,
resulting in the localize accumulation of
pus and dead tissue.
The symptoms of boils are red, pus-filled lumps that are tender,
warm, and extremely painful. A yellow
or white point at the center of the lump can be seen
when the boil is ready to drain or discharge pus.
In a severe infection, multiple boils may develop and the
patient may experience fever and swollen
lymph nodes. A recurring boil is called chronic
furunculosis.
In some people, itching may develop before the lumps begin to
form.
Boils are most often found on the back, stomach, underarms,
shoulders, face, lip, eyes, nose, thighs
and buttocks, but may also be found elsewhere.
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 6
Sometimes boils will exude an unpleasant smell, particularly
when drained or when discharge is
present, due to the presence of bacteria in the
discharge.
The cause are bacteria such as staphylococci. Bacterial
colonization begins in the hair follicles
and can lead to local cellulitis and abscess
formation.
Carbuncles
Is an abscess larger than a boil. It is usually caused by
bacterial infection, most
commonly Staphylococcus aureus.
The infection is contagious and may spread to other areas of the
body or other people.
A carbuncle is made up of several skin boils. The infected mass
is filled with fluid, pus, and dead
tissue. Fluid may drain out of the carbuncle, but
sometimes the mass is so deep that it cannot drain
on its own.
Carbuncles may develop anywhere, but they are most common on the
back and the nape of the neck.
Men get carbuncles more often than women. Things that make
carbuncle infections more likely
include friction from clothing or shaving, generally
poor hygiene and weakening of immunity.
Nursing Management Carbuncles usually must drain before they
will
heal. This most often occurs on its own in less
than 2 weeks.
Placing a warm moist cloth on the carbuncle helps it to drain,
which speeds healing.
The affected area should be soaked with a warm, moist cloth
several times each day.
The carbuncle should not be squeezed, or cut open without
medical supervision, as this can
spread and worsen the infection.
Treatment is needed if the carbuncle lasts longer than 2 weeks,
returns frequently, is
located on the spine or the middle of the face,
or occurs along with a fever or other
symptoms.
A doctor may prescribe antibacterial soaps and antibiotics
applied to the skin or taken by
mouth.
Deep or large lesions may need to be drained by a health
professional.
Proper excision under strict aseptic conditions will treat the
condition effectively.
Proper hygiene is very important to prevent the spread of
infection.
Hands should always be washed thoroughly, preferably with
antibacterial soap, after
touching a carbuncle.
Washcloths and towels should not be shared or reused. Clothing,
washcloths, towels, and
sheets or other items that contact infected areas
should be washed in very hot (preferably
boiling) water.
Bandages should be changed frequently and thrown away in a
tightly-closed bag.
If boils/carbuncles recur frequently, daily use of an
antibacterial soap or cleanser containing
triclosan, triclocarban or chlorhexidine, can
suppress staph bacteria on the skin.
VIRAL SKIN INFECTION
Herpes Zoster (Shingles)
Commonly known as shingles, is a viral disease characterized by
a painful skin rash with blisters in
a limited area on one side of the body, often in a
stripe.
The infection is caused by varicella zoster virus. Symptoms
The earliest symptoms of herpes zoster, which include headache,
fever, and
malaise.
These symptoms are commonly followed by sensations of burning
pain, itching,
hyperesthesia (oversensitivity), or
paresthesia ("pins and needles": tingling,
pricking, or numbness).
The pain may be extreme in the affected dermatome, with
sensations that are often
described as stinging, tingling, aching,
numbing or throbbing, and can be
interspersed with quick stabs of agonizing
pain.
After 12 days (but sometimes as long as 3 weeks) the initial
phase is followed by
the appearance of the characteristic skin
rash.
Later, the rash becomes vesicular, forming small blisters filled
with a serous
exudate, as the fever and general malaise
continue.
The painful vesicles eventually become cloudy or darkened as
they fill with blood,
crust over within seven to ten days, and
usually the crusts fall off and the skin
heals: but sometimes after severe
blistering, scarring and discolored skin
remain.
Medical management: Analgesics
Corticosteroids
Acetic acid compresses
Acyclovir (Zovirax) Nursing interventions:
Apply acetic acid compresses or white petrolatum to lesions
Administer medications as ordered. Analgesics for pain Systemic
corticosteroids:
monitor for side effects of
steroid therapy.
Acyclovir: antiviral agent which reduces the severity when
given
early in illness.
Herpes Simplex Virus
Assessment findings: Clusters of vesicles, may ulcerate or crust
Burning, itching, tingling Usually appears on lip or cheek.
Nursing interventions: Keep lesions dry. Apply topical
antibiotics or anesthetic as
ordered.
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 7
Condition Description Illustration
Herpes labialis
Infection
occurs when
the virus
comes into
contact with
oral mucosa
or abraded
skin.
Herpes
genitalis
When
symptomatic,
the typical
manifestation
of a primary
HSV-1 or
HSV-2
genital
infection is
clusters of
inflamed
papules and
vesicles on
the outer
surface of the
genitals
resembling
cold sores.
FUNGAL INFECTION
Types and
Location
Clinical
Manifestation
Treatment
Tinea
Capitis
( Head)
- Oval, scaling,
erythematous patches
- small papules or
pustules in scalp
- brittle hair
- Griseofulvin for 6
weeks
- Shampoo hair 2
or 3 times with
Nizoral or
Selenium sulfide
shampoo
Tinea
Corporis
(Body)
- Begins with red
macule, which spreads
to a ring of papules
- lesions found in
cluster
- very pruritic
- Mild condition:
Topical antifungal
creams
-Severe condition:
Griseofulvin or
Terbinafine
Tinea
Cruris
(Groin)
- Begins with small,
red scaling patches
which spread to form
circular elevated
plaques.
- very pruritic
- Mild condition:
Topical antifungal
creams
-Severe condition:
Griseofulvin or
Terbinafine
Tinea Pedis
athletes foot
- soles of feet have
scaling and mild
redness with
maceration in toe webs
- Soak feet in
vinegar and water
solution.
- Resistant
infection:
griseofulvin or
terbinafine
- Lamisil daily for
3 months
Tinea
Ungum
(toenails)
- Nails thicken,
crumble easily and
luck cluster
- whole nail maybe
destroyed
- Itraconazole
(sporanox)
Nursing Management
Keep feet dry as much as possible, including area between the
toes.
Wear clothing and socks should be made of cotton Anti-fungal
powder may applied twice a day to keep
feet dry.
Instruct the patient to always use a clean towel and washcloth
daily
Each person should have separate comb and hairbrush to prevent
spread of tinea capitis..
Household pets should be examined.
PEDICULOSIS
Parasitic infestation Adult lice are spread by close physical
contact such
as sharing combs, clips, caps, hats, etc.
Occurs in school-age children particularly those with long
hair.
Medical management: Special medicated shampoos (Lindane). Use of
fine-tooth comb to remove nits.
Assessment findings: White eggs (nits) firmly attached to base
of
hair shafts.
Pruritus of scalp.
Nursing interventions: Institute skin isolation precautions. Use
special shampoo and comb the hair. Provide client teaching and
discharge planning
concerning:
How to check self and other family members and how to treat
them.
Washing of clothes, bed linens, etc.; discouraging sharing of
brushes, combs and
hats.
Contact Dermatitis
Irritation of the skin from a specific substance which came in
contact with the skin.
Usually caused by irritants and allergens Contact dermatitis is
a localized rash or irritation of
the skin caused by contact with a foreign substance.
Only the superficial regions of the skin are affected in contact
dermatitis. Inflammation of the affected
tissue is present in the epidermis (the outermost
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 8
layer of skin) and the outer dermis (the layer
beneath the epidermis)
Symptoms of both forms include the following: Red rash. This is
the usual reaction. The
rash appears immediately in irritant
contact dermatitis; in allergic contact
dermatitis, the rash sometimes does not
appear until 2472 hours after exposure to the allergen.
Blisters or wheals. Blisters, wheals (welts), and urticaria
(hives) often form in
a pattern where skin was directly exposed
to the allergen or irritant.
Itchy, burning skin. Irritant contact dermatitis tends to be
more painful than
itchy, while allergic contact dermatitis
often itches.
Nursing Interventions: Apply wet dressings of Burrows
solution
for 20 minutes, 4 times a day to help clear
oozing lesions.
Provide relief from pruritus. Administer topical steroids and
antibiotics
as ordered.
Allowing crusts and scales to drop off skin naturally as healing
occurs.
Avoidance of wool, nylon, or fur fibers on sensitive skin.
Need to use gloves if handling irritant or allergenic
substances.
Provide client teaching and discharge planning concerning:
Avoidance of causative agent.
Preventing skin dryness:
Use mild soaps.
Soak in plain water for 20 to 30 minutes.
Apply prescribed steroid cream immediately after bath.
Avoid extremes of heat and cold.
Psoriasis
Is a chronic, non-contagious autoimmune disease which affects
the skin and joints.
It commonly causes red scaly patches to appear on the skin. The
scaly patches caused by psoriasis,
called psoriatic plaques, are areas of inflammation
and excessive skin production.
Skin rapidly accumulates at these sites and takes on a
silvery-white appearance.
Plaques frequently occur on the skin of the elbows and knees,
but can affect any area including the
scalp and genitals. Predisposing factors:
Stress
Trauma
Infection
Changes in climate
Excessive alcohol consumption
Smoking
Familial factors Medical management:
Topical corticosteroids Coal tar preparations Ultraviolet light
Antimetabolites (methotrexate)
Nursing Interventions: Apply occlusive wraps over prescribed
topical steroids.
Protect areas treated with coal tar preparation from direct
sunlight for 24
hours.
Administer methotrexate as ordered, assess for side effects.
Provide client teaching and discharge planning concerning:
Feelings about changes in appearance of skin (encourage client
to cover arms
and legs with clothing if sensitive about
appearance).
Importance of adhering to prescribed treatment and avoidance of
commercially advertised products.
Vitiligo
Is a chronic disorder that causes depigmentation in patches of
skin.
It occurs when the melanocytes, the cells responsible for skin
pigmentation which are derived
from the neural crest, die or are unable to function.
Unknown caused, but there is some evidence suggesting it is
caused by a combination of
autoimmune, genetic, and environmental factors.
Symptom of vitiligo is depigmentation of patches of skin that
occurs on the extremities. Although
patches are initially small, they often enlarge and
change shape.
When skin lesions occur, they are most prominent on the face,
hands and wrists.
Depigmentation is particularly noticeable around body orifices,
such as the mouth, eyes, nostrils, genitalia and umbilicus
Skin Cancer
Types of skin cancers: Basal cell epithelioma most common
type
of skin cancer; locally invasive and rarely
metastasizes; most frequently located between
the hairline and upper
lip.
Risk factors: - UV rays - May take several forms: nodular,
ulcerative, pigmented ad superficial
Hx and Assessment: - Usually asymptomatic unless
secondarily infected in advanced
disease
- Pearly-colored PAPULE - External surface - fine
telangiectasia and is translucent
Treatment: - Curettage - Surgical - Cryosurgery - Radiation -
prevention - Mohrs micrographic surgery
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 9
Squamous cell carcinoma (epidermoid) grows more rapidly than
basal cell carcinoma
and can metastasize; frequently seen on
mucous membranes, lower lip, neck and
dorsum of the hands.
Risk factors: - UV rays - Radiation - Actinic keratosis -
Immunosuppression - Industrial carcinogens
History and Assessment: - Slowly evolving - Assymptomatic -
Occassionaly bleeding and pain - Exophytic nodules w/ varying
degree of scaling or crusting
Diagnosis: - Biopsy- irregular masses of
anaplastic epidermal celss
proliferating down to the dermis
Treatment - Surgical excision - Mohrs micrographic surgery -
Radiation
Malignant melanoma least frequent of skin cancers, but most
serious; capable of invasion
and metastasis to other organs.
Risk factors: - Sun exposure - Fair skin - Positive family
history - Presence of dysplastic nevi
Hx and Assessment: - Usually asymptomatic until late - Pruritus
or mild discomfort - Recent changed in a previous skin
lesion
asymetry border irregularity color variation diameter(large)
Diagnosis: - Biopsy- melanocytes w/ marked
cellular atypia and melanocytic
invasion of the dermis
Treatment: - Surgical excision - Chemotherapy- metastasis
Precancerous lesions:
Leukoplakia white shiny patches in the mouth or on the lip.
Nevi (moles) junctional nevus may become malignant; compound and
dermal nevi
unlikely to become cancerous.
Senile keratoses brown, scale-like spots on older
individuals.
Nursing interventions: Limitation of contact with chemical
irritants. Need to report lesions that change
characteristics and/or those that do not heal.
Protection against UV rays from the sun Wear thin layer of
clothing. Use sunblock or lotion
containing PABA.
BURNS
Direct tissue injury due to:
o Thermal: scald, hot grease, sunburn, contact with flames
o Electrical o Chemical o Smoke inhalation: fumes, gasses,
smoke
I. TYPES A. Full thickness
1. First degree burns (superficial) Epidermis Common cause is
thermal burn (+) blanching upon pressure and
erythema
(+) pain 2. Second degree burns (deep burn)
Chemical (+) very painful (+) erythema or fluid filled
blisters
B. Partial thickness 1. Third to fourth degree burns
Affect all layers of skin, muscle and bones
Electrical burns Less painful than 1st and 2nd degree
burns
Dry, thick, leathery texture Eschar devitalized tissue
A description of the traditional and current
classifications of burns.
Nomenclature Traditional
nomenclature Depth
Clinical
findings
Superficial
thickness First-degree
Epidermis
involvement
Erythema,
minor pain,
lack of
blisters
Partial
thickness superficial
Second-degree
Superficial
(papillary)
dermis
Blisters,
clear fluid,
and pain
Partial
thickness deep
Second-degree
Deep
(reticular)
dermis
Whiter
appearance
Full thickness
Third- or
Fourth-
degree*
Dermis and
underlying
tissue and
possibly
fascia, bone,
or muscle
Hard,
leather-like
eschar,
purple fluid,
no sensation
(insensate)
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 10
C. STAGES 1. Emergent removal of client from source of
burn
Thermal smother burn beginning with the head.
Smoke inhalation ensure patent airway.
Chemical remove clothing that contains chemical; lavage are
with
copious amounts of water.
Electrical note victim position, identify entry and exit routes;
maintain
airway.
Wrap in dry, clean sheet or blanket to prevent further
contamination of
wound and to provide warmth.
Assess how and when burn occurred. Provide IV route if possible.
Transport immediately.
2. Shock phase (24-48 hours) shifting of fluids from
intravascular to interstitial hypovolemia
Elevated HCT Tachycardia Metabolic acidosis Low serum sodium Low
serum potassium Hypotension
3. Diuresis Phase/Fluid remobilization phase characterized by
the return of fluids from
interstitial to intravascular
Assessment findings: Elevated blood pressure, increased
urine output.
Hypokalemia, hyponatremia, metabolic acidosis
4. Convalescent/Recovery phase characterized by continuous wound
healing
Healing starts immediately after injury
Assessment findings: Elevated blood pressure, increased
urine output.
Hypokalemia, hyponatremia, metabolic acidosis
D. ASSESSMENT FINDINGS 1. Rule of 9s
Head and neck = 9 Anterior chest = 18 Posterior chest = 18 Upper
extremity = 9 x 2 Lower extremity = 18 x 2 Genital = 1
2. Severity of burns:
Major: partial thickness greater than 25%; full thickness
greater than or equal to
10%.
Moderate: partial thickness 15%-25%; full thickness less than
10%.
Minor: partial thickness less than 15%; full thickness less than
2%.
E. MEDICAL MANAGEMENT: 1. Supportive therapy: IV fluid
management,
catheterization
2. Wound care:
Hydrotherapy
Debridement (enzymatic or surgical) 3. Drug therapy:
Topical antibiotics
Systemic antibiotics
Tetanus toxoid or hyperimmune human tetanus globulin
Analgesics 4. Surgery: excision and grafting
F. NURSING MANAGEMENT
1. Administer medications as ordered Tetanus toxoid Burn surface
area is a good source of
microbial growth
CLOSTRIDIUM TETANY
Tetanospain Tatanolysin
Narcotic analgesics morphine Systemic antibiotics Cephalosporins
Penicillin Tetracyclines Topical antibiotics Silver sulfadiazide
Silver nitrate Povidone iodine
2. Provide relief/control of pain: Administer morphine sulfate
and
monitor vital signs closely.
Administer analgesics/narcotics 30 minutes before wound
care.
Position burned areas in proper alignment.
3. Monitor alterations in fluid and electrolyte balance:
Assess for fluid shifts and electrolyte alterations.
Administer IV fluids as ordered. Monitor Foley catheter output
hourly
(30 ml/hr desired).
4. Monitor alterations in fluid and electrolyte balance:
Weigh daily. Monitor circulation status regularly.
Administer/monitor
crystalloids/colloids/water solutions.
5. Formula in IVF administration:
Evans Formula: Colloids: 1 ml x wt (kg) x % BSA
burned
Electrolytes (saline): 1 ml x wt (kg) x % BSA burned
Glucose (D5W): 2000 ml for insensible loss.
Day 1: half to be given in 1st 8 hours;
remaining half over next 16 hours.
Day 2: half of previous days colloids and electrolytes; all of
insensible fluid replacement.
Maximum of 10 L over 24 hours.
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 11
Second and third-degree burns exceeding 50% BSA calculated
on
basis of 50% BSA
Brooke Army Formula: Colloids: 0.5 ml x wt (kg) x % BSA
burned
Electrolytes (lactated Ringers): 1.5 ml x wt (kg) x % BSA
burned
Glucose (D5W): 2000 ml for insensible loss
Day 1: Half to be given in first 8 hours,
remaining half over next 16 hours.
Day 2: Half of colloids, half of electrolytes, all
of insensible fluid replacement.
Second and third-degree burns exceeding 50% BSA calculated
on
basis of 50% BSA
Parkland/Baxter Formula: Lactated Ringers:
4 ml x wt (kg) x % BSA burned
Day 1: Half to be given in first 8 hours; half to
be given over next 16 hours.
Day 2: Varies; colloid is added.
Consensus Formula: Lactated Ringers:
2-4 ml x wt (kg) x % BSA burned
Half to be given in first 8 hours after burn;
remaining fluid to be given over next 16 hours.
6. Prevent wound infection. Place the patient in a controlled
sterile
environment.
Maintain strict aseptic technique Use hydrotherapy for no more
than 30
minutes to prevent electrolyte loss.
Observe wound for separation of eschar and cellulitis.
Apply mafenide (sulfamylon) as ordered: Administer analgesics 30
minutes
before application.
Monitor acid-base status and renal function studies.
Provide daily tubbing for removal of previously applied
cream.
Apply silver sulfadiazine as ordered. Administer analgesics 30
minutes
before application.
Observe and report hypersensitivity reactions.
Store drug away from heat.
Apply silver nitrate as ordered. Handle carefully: solution
leaves
gray or black stain on skin, clothing
and utensils.
Administer analgesics 30 minutes before application.
Keep dressings wet with solution; dryness increases the
concentration
and causes precipitation of silver
salts in the wound.
Apply povidone-iodone solution as ordered.
Administer analgesics before application.
Assess for metabolic acidosis/renal function studies.
Administer gentamicin as ordered: assess vestibular/auditory and
renal functions at
regularly intervals.
7. Promote maximal nutritional status:
Diet high in CHO, CHON, VIT C Monitor tube feedings/TPN if
ordered. When oral intake permitted, provide high-
calorie, high-protein, high carbohydrate
diet with vitamin and mineral
supplements.
Serve small portions. Schedule wound care and other
treatments
at least 1 hour before meals.
8. Prevent GI complications: Assess for signs and symptoms
of
paralytic ileus.
Assist with insertion of NGT to prevent/control Curlings/stress
ulcer; monitor patency/drainage.
Administer prophylactic antacids through NGT and/or IV
cimetidine or ranitidine.
Monitor bowel sounds. Test stools for occult blood.
9. If (+) to burn of the head and neck and face Assist in
intubation
10. Assist in hydrotherapy 11. Assist in surgical wound
debridement
Analgesics before debridement 12. Prevent complications
Infections Septicemia Paralytic ileus Curlings ulcers (H2
receptor
antagonists)
13. Assist in surgical procedure
14. Provide client teaching and discharge planning
concerning:
Care of healed burn wound Assess daily for changes.
Wash hands frequently during dressing change.
Wash area with prescribed solution or mild soap and rinse well
with
water; dry with clean towel.
Apply sterile dressing. Prevention of injury to burn wound.
Avoid trauma to area. Avoid use of fabric softeners or
harsh detergents (might cause
irritation).
Avoid constrictive clothing over burn wound.
Adherence to prescribed diet. Importance of reporting formation
of local
trophic changes.
Methods of coping and resocialization.
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 12
Wound Healing Process
Wound healing, or wound repair, is an intricate process in which
the skin (or some other organ)
repairs itself after injury.
In normal skin, the epidermis (outermost layer) and dermis
(inner or deeper layer) exists in a steady-
stated equilibrium, forming a protective barrier
against the external environment.
Once the protective barrier is broken, the normal (physiologic)
process of wound healing is
immediately set in motion
The classic model of wound healing is divided into three or four
sequential, yet overlapping, phases:
(1) hemostasis
(2) inflammatory,
(3) proliferative and
(4) remodeling
A. Homostasis
Within minutes post-injury, platelets (thrombocytes) aggregate
at the injury site to form a fibrin clot.
This clot acts to control active bleeding (hemostasis)
B. Inflammatory Phase
When tissue is first wounded, blood comes in contact with
collagen, triggering blood platelets to
begin secreting inflammatory factors.
Platelets, release a number of things into the blood, including
ECM proteins and cytokines, including
growth factors.Growth factors stimulate cells to
speed their rate of division.
Platelets also release other proinflammatory factors like
serotonin, bradykinin, prostaglandins,
prostacyclins, thromboxane, and histamine, which
cause blood vessels to become dilated and porous.
The main factor involved in causing vasodilation is histamine.
Histamine also causes blood vessels to:
Increased Capillary Permeability causes hyperemia that leads to
redness (rubor) and presence of heat
(calor) and
Fluid and cellular exudation that causes edemaand presence of
exudates
Within an hour of wounding, polymorphonuclear neutrophils (PMNs)
arrive at the wound site and
become the predominant cells in the wound for the
first two days after the injury occurs.They also
cleanse the wound by secreting proteases that break
down damaged tissue.
Neutrophils usually undergo apoptosis once they have completed
their tasks and are engulfed and
degraded by macrophages
The macrophage's main role is to phagocytise bacteria and
damaged tissue and it also debrides
damaged tissue by releasing proteases.
Macrophages also secrete a number of factors such as growth
factors and other cytokines, especially
during the third and fourth post-wounding days.
These factors attract cells involved in the proliferation stage
of healing to the area
C. Proliferative Phase
Fibroblasts begin to enter the wound site, marking the onset of
the proliferative phase even before the
inflammatory phase has ended.
Angiogenesis occurs concurrently with fibroblast proliferation
when endothelial cells migrate to the
area of the wound.
The tissue in which angiogenesis has occurred typically looks
red (is erythematous) due to the
presence of capillaries
Fibroblasts mainly proliferate and migrate, while later, they
are the main cells that lay down the
collagen matrix in the wound site.
Fibroblasts begin secreting appreciable collagen. Collagen
deposition is important because it
increases the strength of the wound; before it is laid
down.
Formation of granulation tissue in an open wound allows the
reepithelialization phase to take place, as
epithelial cells migrate across the new tissue to form
a barrier between the wound and the environment
D. Remodeling Phase
When the levels of collagen production and degradation equalize,
the maturation phase of tissue
repair is said to have begun.
The maturation phase can last for a year or longer, depending on
the size of the wound and whether it
was initially closed or left open.
During Maturation, type III collagen, which is prevalent during
proliferation, is gradually degraded
and the stronger type I collagen is laid down in its
place
Primary Intention:
When wound edges are directly next to one another
Little tissue loss
Minimal scarring occurs
Most surgical wounds heal by first intention healing
Wound closure is performed with sutures, staples, or adhesive at
the time of initial evaluation
Secondary Intention:
The wound is allowed to granulate
Surgeon may pack the wound with a gauze or use a drainage
system
Granulation results in a broader scar
Healing process can be slow due to presence of drainage from
infection
Wound care must be performed daily to encourage wound debris
removal to allow for granulation tissue formation
Tertiary Intention (Delayed primary closure):
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 13
The wound is initially cleaned, debrided and observed, typically
4 or 5 days before closure
Pressure Ulcer
Lesion from unrelieved pressure causing damage of underlying
tissue or a localized area of cellular
necrosis resulting from vascular insufficiency in
tissues under pressure
Occurs with limited mobility Once formed, pressure ulcers are
slow to heal Result from mechanical forces Occurs most often over
bony prominences
Pressure Points
Mechanical Forces Pressure Friction Shear
Risk Factors for Developing Pressure Ulcer
Prolong pressure on tissue Immobility, compromised mobility Loss
of protective reflexes Poor skin perfusion Edema Malnutrition
Friction Shearing forces Trauma Incontinence of urine and feces
Altered skin moisture Excessively dry skin Advance age Equipment:
cast,traction and restraints
Pressure Ulcers: Wound Assessment
Appearance changes with the depth of injury Assess for:
Location, size, color Extend of tissue involvement Condition of
surrounding tissue Presence of foreign bodies
Stages of Ulcer
Stage I
Area of erythema
Erythema does not blanch with pressure
Skin temperature elevated
Tissue are swollen
Patient complains of discomfort
Erythema progresses to dusky blue-gray
Stage II
Skin breaks
Abrasion, blister or shallow crater
Edema persists
Ulcer drains
Infection may develop
Stage III
Ulcer extends into subcutaneous tissue
Necrosis and drainage continue
Infection develops
Stage IV
Ulcer extends to underlying muscle and
bone.
Deep pockets of infection develop
Necrosis and drainage continue
Pressure Ulcers: Key Things to Remember
Pressure relieving/reducing devices do not take the place of
observation of skin color, integrity, and
temperature at intervals to determine capillary blood
flow.
In some clients pressure can occur in less than 2 hours the
actual turning/repositioning schedule should be individualized
based upon assessment
data
Pressure Ulcers: Nursing Diagnosis
Impaired skin integrity Pain Disturbed body image Ineffective
coping Imbalanced nutrition: less than body requirements Deficient
knowledge
Nursing Intevention
Prevention of Pressure: o Turned and repositioned at 1-2
hours
interval
o Encourage to shift weight actively every 15 minutes
o Pressure relief and reduction devices: Dynamic vs. Static
Frequent monitoring of ulcer progress Avoid massaging reddened
areas, because this may
increase the damage
To avoid shearing forces when repositioning the patient, the
nurse lifts and avoid dragging the
patient across a surface
Increase protein intake, iron, vitamin C Prevention of infection
and wound extension
o Be alert for classic signs of wound infection
o Prevent further pressure damage Maintaining a safe
environment
o Meticulous local wound care o Minimize cross-contamination
with
pathogens
o Standard precautions o Thorough handwashing before and
after
dressing changes
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 14
Anatomy of the Skin
Hair / Hair Growth
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 15
Nail Skin Testing Woods Light Examination
Secondary Skin Lesion
Skin Grafting
-
Medical and Surgical Nursing
Integumentary System Lecture Notes
Prepared by: Mark Fredderick R. Abejo RN,MAN 16
Burn Rule of Nine
Phases of Wound Healing