Embed Size (px)
Citation preview
Integration of Objective Metric-Based Assessment and Cognitive Performance of Surgical Trainees during Robot-Assisted Surgery
Statement of Funds
No other funds are pending or on hand through other sources.
Summary
Quality surgical mentoring and an ideal operating environment are vital to promote surgical performance, teamwork and communication while minimizing errors and surgical flow disruptions. This will ultimately promote patient safety and improve surgical outcomes for patients. Non-technical skills and cognitive input are critical in encompassing, decision making, priority setting, and leadership skills necessary to achieve competency, autonomy; translating into quality patient care.
The aim of this proposal is to assess the process of surgical teaching in the setting of robot-assisted surgery (RAS), and investigate whether robotic surgical training and skills acquisition are associated with cognitive changes in surgeons.
Assessment of surgical performance of trainees along their surgical training will be done using validated scoring systems (for both basic robotic skills and specific for anastomosis) and follow up to evaluate skills acquisition and experience, while simultaneously recording their electroencephalogram (EEG). Correlation between the process of skill acquisition, surgical performance and cognitive changes will be investigated. Moreover, the EEG pattern of trainees will be compared with that of mentors to identify possible cognitive changes associated with experience and/or technical proficiency. Validated workload subjective assessment tools will also be completed.
Exploring cognitive assessment may provide an objective measure for adequacy of robotic surgical training. Also, it may predict the potential for long term robotic skills acquisition and therefore, guide and personalize training. Our project aims at ensuring adequate robotic training especially in the era of limited time utilized for training.
Hypothesis
We hypothesize that the novel method of utilizing EEG measurements during training will help us both understand and improve the quality of surgical training and mentorship during robot-assisted surgeries (RAS). This will further help us distinguish between levels of technical proficiency that will lay the foundation for prediction of surgical mastery.
Background
Mentoring surgeons face several challenges, including limited teaching time while fully disclosing to patients the degree of trainee participation 1. This is even more challenging when it
comes to robot-assisted surgery (RAS). Best practice statements highlighted the need for validated assessment tools for robotic technical proficiency and credentialing 2. Such tools should provide objective assessment of robot-assisted skill acquisition to establish expert-guided goals and ensure adequate training that promote competency in the desired skills and deliver safe patient care. Technical skills are crucial for optimal patient outcomes. Even after controlling for surgical volume and experience, differences between surgeons can result in significant variation in quality of life and oncologic outcomes 3-5. Although surgical simulators have been developed to address this concern, none have shown sufficient predictive validity in transferring simulator skills to the to the real operative environment 6.
Developing tools to assess technical proficiency and adequacy of training is crucial. The value of cognitive assessment has been explored in many non-medical applications 7,8. Functional magnetic resonance (fMRI) imaging studies have been shown useful in studying surgical skills acquisition 9. However, brain scanning with MRI while performing or mentoring surgery is impractical owing to physical limitations, lack of real-time monitoring, and associated cost. Advents in brain-computer interfaces offers an objective and real-time alternative cognitive metrics assessment, defining the mental energy expenditure while performing a certain task 10,11. Cognitive metrics assessment allows real-time consideration of factors as teamwork and environmental interactions, which are not addressed when an expert surgeon observes a recorded performance of the trainee. Additionally, mental workload and level of engagement are the most common metrics used to evaluate the surgeon’s mental state using self-reported tools such as National Aeronautics and Space Administration Task Load index (NASA-TLX) 12. However, the concept of self-rating and the inability to administer the task as it is performed is open to both subjective and recall biases. Thorough surgical teaching is critical as surgeons have to ensure safety and achieve standard results especially when fewer training hours are available 9.
Our program has used cognitive assessment to differentiate the level of expertise and characterize the variation of utilization of different mental resources by an expert surgeon during different surgical scenarios 13,14. We also have previously investigated and published the utilization of cognitive assessment during RAS to define skills in terms of cognitive engagement, mental workload, and mental state, while objectively differentiating variation in operative experience. We found that cognitive assessment of surgeons may help in differentiating levels of expertise performing complex RAS tasks once technical competence is achieved and may be used as an adjunct to the traditional methods for skill assessment 13. Additionally, we found that different surgical scenarios were paralleled by variability in cognitive performance, from an unknown challenge where the surgeon transitions from an automated mode to effortful thought of a surgical step (e.g during lysis of adhesions), to a process involving cognitive engagement and technical skills (e.g during lymph node dissection), to a repetitive motor skill (e.g during urethrovesical anastomosis) (Figure 1) 14.
We also developed and validated an objective scoring system for assessment of robot-assisted anastomosis (urethrovesical), which can be applicable for other specialties as biliary,

vascular and gynecologic procedures 15. We recorded the EEG of an expert surgeon while observing Clinical Fellow trainee in 20 surgical procedures with simultaneous completion of NASA-TLX questionnaire by both surgeon and trainee. While comparing the brain activity of the mentor during this study to his own brain activity while actually performing the same surgical steps, we found that the mentor was mentally engaged and concerned while he was engrossed in observing the surgery. This was further supported by the finding that there was no significant difference in the mental demands and workload between observing and operating for the expert surgeon 16.
Methods
Basic robot-assisted surgical skills of trainees will be assessed using the validated scoring tool –Global Evaluative Assessment of Robotic Skills (GEARS). Whenever anastomosis is involved, the Robotic Anastomosis Competency Evaluation (RACE) developed by our own laboratory will be used. Simultaneous cognitive evaluation of the trainees will be the key objective of our study. To investigate whether surgical training and skills acquisition is associated with cognitive changes by evaluating cognitive metrics of RAS trainees at different time points (at least every 3 months for 2 years) along their surgical training “Mind Maps” project is an Institutional Review Board (IRB) approved study (I-241913) which aims at evaluating cognitive function of surgeon’s expertise and trainee’s skills 16. Simultaneous completion of National Aeronautics and Space Administration Task Load index (NASA-TLX) questionnaire is performed.
Cognitive Metrics Measurement: A 24-channel wireless electroencephalogram (EEG) recording device is used to monitor brain activity during all surgical procedures using a X 24 neuro-headset. Sensors are placed over frontal, temporal, parietal and occipital regions. EEG data from each channel is sampled at 256 samples per second. Filtering and classification techniques are used to remove signal artifacts such as muscle and eye movements 10. A pre-recording session is done to compute the surgeon’s baseline cognitive indices. Three main cognitive metrics are measured: mental state, distraction, and mental workload. The mental state is related to information gathering, visual scanning and sustained attention. It includes high-level, low-level engagement and cognitive state. Mental state is a discrete index that represents the most probable cognitive state in a given instant (1 second epoch) using numerical values (0.1=sleep onset, 0.3=distraction, 0.6=low engagement, and 0.9=high engagement) 10. Distraction measures the level of cognitive involvement of the surgeon while performing surgery. Finally, mental workload involves both executive function and loading working memory. Absolute and relative power spectral density of decontaminated data for each 1-second epoch was calculated by using Fast Fourier Transform with a 50% overlapping Kaiser Window. These data were used to extract workload, high level engagement, low level engagement, cognitive state, and distraction as EEG features.

NASA- Task Load Index Questionnaire: NASA-TLX is a validated instrument for assessment of subjective mental workload 12. It utilizes a 20-point visual analog score and provides an overall index of mental workload based on a 6-dimension scale: mental, physical, and temporal task demands; effort, frustration, and perceived performance. Mental demand estimates how much perceptual activity (e.g. thinking, deciding, calculating, remembering, looking, and searching) is required while performing the task. Physical demand estimates how much physical activity is required (e.g. for retraction and suturing). Temporal demand estimates how much time pressure subject feels due to the rate or pace during the task. Performance measures the perceived level of task accomplishment. Effort measures the extent of mental and physical hard work. Frustration measures how stressed and annoyed the subject feels, versus how content and relaxed while performing the task. NASA-TLX has been previously validated and used by the NASA Ames Research Laboratory for evaluation of individual workload during flight simulation, air traffic control and vigilance tasks 12. Perfect performance in NASA-TLX is associated with a lower numerical value on the scoring sheet.
Both the surgeon and the trainee are blinded about the outcomes until the analysis is complete to minimize any cognitive bias. Adequate signal transduction from the neuro-headset was assured by checking the impedance of the electrodes prior each procedure.
Statistical Analysis: Outcome measures will be summarized using means, and correlation between subjective metrics on NASA-TLX and EEG cognitive metrics will be computed using Spearman's rank correlation coefficient in matrix laboratory (MATLAB) environment (The Math Works Inc, USA). Two-sided p-values are computed, and values 0.05 or less are considered significant. It should be noted that only for the performance parameter in NASA-TLX, the degree of performance is inversely related to the sign of correlation.
2aCopy of Guru SAGES RoboticBudgetSheet FINAL
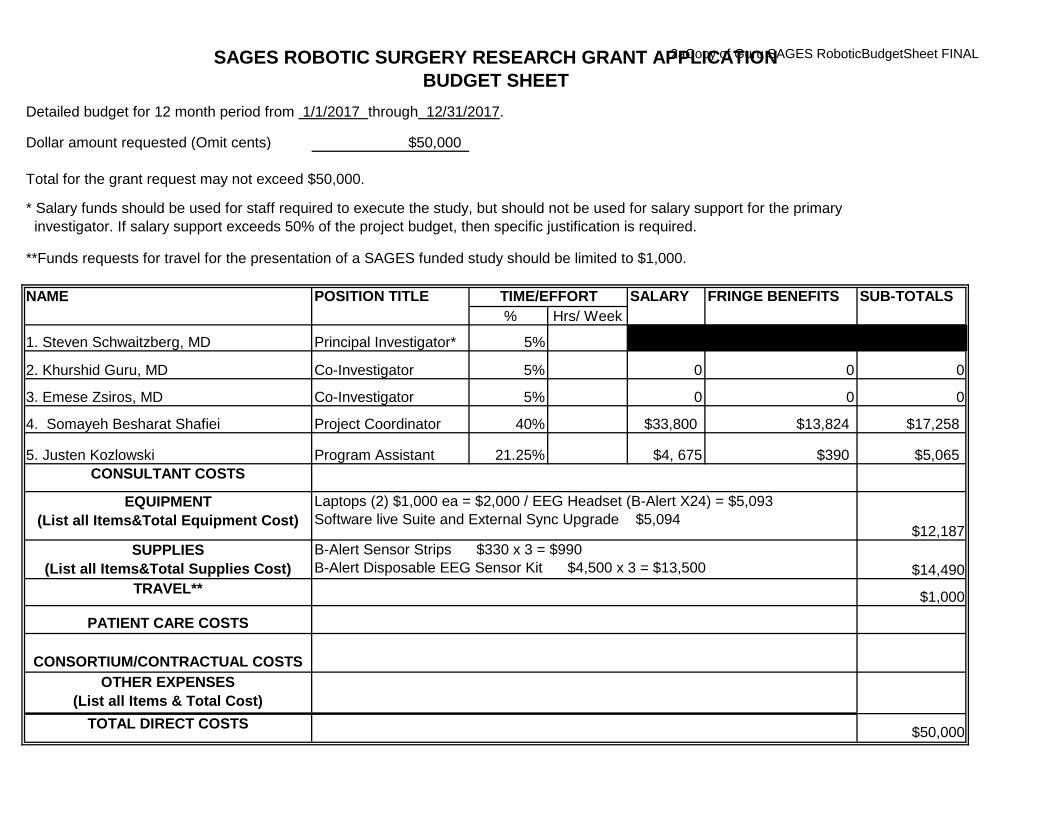
Detailed budget for 12 month period from 1/1/2017 through 12/31/2017.
Dollar amount requested (Omit cents) $50,000
Total for the grant request may not exceed $50,000.
* Salary funds should be used for staff required to execute the study, but should not be used for salary support for the primary investigator. If salary support exceeds 50% of the project budget, then specific justification is required.
**Funds requests for travel for the presentation of a SAGES funded study should be limited to $1,000.
POSITION TITLE SALARY FRINGE BENEFITS SUB-TOTALS % Hrs/ Week
1. Steven Schwaitzberg, MD Principal Investigator* 5%
2. Khurshid Guru, MD Co-Investigator 5% 0 0 0
3. Emese Zsiros, MD Co-Investigator 5% 0 0 0
4. Somayeh Besharat Shafiei Project Coordinator 40% $33,800 $13,824 $17,258
5. Justen Kozlowski Program Assistant 21.25% $4, 675 $390 $5,065CONSULTANT COSTS
EQUIPMENT (List all Items&Total Equipment Cost)
$12,187 SUPPLIES
(List all Items&Total Supplies Cost) $14,490 TRAVEL** $1,000
PATIENT CARE COSTS
CONSORTIUM/CONTRACTUAL COSTSOTHER EXPENSES
(List all Items & Total Cost)TOTAL DIRECT COSTS $50,000
SAGES ROBOTIC SURGERY RESEARCH GRANT APPLICATIONBUDGET SHEET
TIME/EFFORT
Laptops (2) $1,000 ea = $2,000 / EEG Headset (B-Alert X24) = $5,093Software live Suite and External Sync Upgrade $5,094
B-Alert Sensor Strips $330 x 3 = $990 B-Alert Disposable EEG Sensor Kit $4,500 x 3 = $13,500
NAME
PERSONNEL Dr. Steven Schwaitzberg, MD, PI, is a Professor of surgery at the University at Buffalo (UB). His research has focused on the promotion of a healthier, more productive individual and the work environment. His research aims include the promotion of surgeons training while increasing workplace productivity and reducing associated healthcare costs. No salary support will be requested for his time in this project. Dr. Schwaitzberg is a SAGES member and is formally collaborating with ATLAS at Roswell on this project. Dr. Khurshid Guru, MD, Co-Investigator, has been active in safe human machine interface, cognitive interaction, artificial intelligence and safe OR environment. As Director of the Robotic Surgery program at RPCI, Dr. Guru works to advance the learning environment for future surgeons. As Director of ATLAS, he has built a multi-disciplinary team of engineers, medical illustrators, and researchers to bridge the strengths of multiple professions into building robust new technological platforms for improved delivery of care. Currently, his research focus has been on the assessment and enhancement of training in addition to studying the cognitive function of surgeons. No salary support will be requested for his time in this project.
Dr. Emese Zsiros, MD, Co-Investigator, is Assistant Professor of Oncology in the GYN Department at Roswell Park. During her fellowship training at the University of Pennsylvania, she was actively involved in planning and conducting early phase immunotherapy clinical trials for patients with ovarian cancer. She completed a year-long training in Patient Oriented Research by the Institute of Translational Medicine at the University of Pennsylvania. Dr. Zsiros has special interest in surgeon education and development of objective assessment tools that can be used to evaluate trainees and provide structured feedback that can be used to tailor training activities. She will be evaluating the objective assessment of anastomosis. Somayeh Besharat Shaifiei, Project Coordinator, is an Engineering PhD student at the University at Buffalo. Her main focus is to study how the brains of surgeons work, and how skills acquisition with surgical training affects the cognitive function in addition to neuroplasticity. Somayeh will be doing the analysis of the captured EEG data. Justen Kozlowski, Program Assistant, has completed his Bachelor of Biomedical Sciences at the University at Buffalo (UB). He has worked as an intern throughout the development of this project and is poised to take on a more definitive role in the structured research. With a strong foundation and an established academic excellence, Justen is a valuable asset for assisting in data management and coordination for this project. Justen will be also responsible for recording the electroencephalogram (EEG) of surgeons and trainees throughout the study.
EQUIPMENT (actual costs listed - difference from SAGES award will be supported through institutional funding) EEG headset (B-Alert X24) $14,950, External sync unit upgrade and Software live Suite (autodecontamination acquisition + B-Alert Metrics) $7,000, Laptops (2 x $1,000) $2,000
SUPPLIES B-Alert® Disposables for 60 Cases: The ATLAS Program has two B-Alert® EEG and EKG devices which will be utilized throughout this project. Although the equipment has already been purchased, replacement sensor strip kits and disposable EEG & EKG sensors kits must be purchased in quantities to accommodate the 60 cases which will be utilized in this project. This equipment will provide the PI with valuable data on the physical state of the primary surgeon throughout live case recordings (IRB-approved).
TRAVEL National Conference Presentations: The results from this study will be generated into abstracts which will be submitted to national conferences. The fifteen-hundred dollar stipend should cover travel, accommodations, and a modest food remuneration for the PI to present the project results via poster and/or podium presentations at national conferences.
References
1. McAlister C. Breaking the Silence of the Switch--Increasing Transparency about Trainee Participation in Surgery. N Engl J Med. 2015;372(26):2477-2479.
2. Lee JY, Mucksavage P, Sundaram CP, McDougall EM. Best practices for robotic surgery training and credentialing. J Urol. 2011;185(4):1191-1197.
3. Begg CB, Riedel ER, Bach PB, et al. Variations in morbidity after radical prostatectomy. N Engl J Med. 2002;346(15):1138-1144.
4. Cooperberg MR, Odisho AY, Carroll PR. Outcomes for radical prostatectomy: is it the singer, the song, or both? J Clin Oncol. 2012;30(5):476-478.
5. Vickers A, Savage C, Bianco F, et al. Cancer control and functional outcomes after radical prostatectomy as markers of surgical quality: analysis of heterogeneity between surgeons at a single cancer center. Eur Urol. 2011;59(3):317-322.
6. Rashid HH, Leung YY, Rashid MJ, Oleyourryk G, Valvo JR, Eichel L. Robotic surgical education: a systematic approach to training urology residents to perform robotic-assisted laparoscopic radical prostatectomy. Urology. 2006;68(1):75-79.
7. Berka C, Behneman, A., Kintz, N. & Raphael, R. J. G. Accelerating Training Using Interactive Neuro-Educational Technologies: Applications to Archery, Golf and Rifle Marksmanship. Int. J. Sport Soc.1, 87–104 (2010).
8. Landers DM, Petruzzello SJ, Salazar W, et al. The influence of electrocortical biofeedback on performance in pre-elite archers. Medicine and science in sports and exercise. 1991;23(1):123-129.
9. Morris MC, Frodl T, D'Souza A, Fagan AJ, Ridgway PF. Assessment of competence in surgical skills using functional magnetic resonance imaging: a feasibility study. Journal of surgical education. 2015;72(2):198-204.
10. Stikic M, Johnson RR, Levendowski DJ, Popovic DP, Olmstead RE, Berka C. EEG-derived estimators of present and future cognitive performance. Frontiers in human neuroscience. 2011;5:70.
11. Corbetta M, Patel G, Shulman GL. The reorienting system of the human brain: from environment to theory of mind. Neuron. 2008;58(3):306-324.
12. Hart SGS, L. E. Development of NASA-TLX (Task Load Index): Results of Empirical and Theoretical Research. Adv. Psychol.52, 139–183 (1988).
13. Guru KA, Esfahani ET, Raza SJ, et al. Cognitive skills assessment during robot-assisted surgery: separating the wheat from the chaff. BJU international. 2015;115(1):166-174.
14. Guru KA, Shafiei SB, Khan A, Hussein AA, Sharif M, Esfahani ET. Understanding Cognitive Performance during Robot Assisted Surgery: Piercing the Hornet's Nest. Urology. 2015.
15. Raza SJ, Field E, Jay C, et al. Surgical competency for urethrovesical anastomosis during robot-assisted radical prostatectomy: development and validation of the robotic anastomosis competency evaluation. Urology. 2015;85(1):27-32.

16. Hussein AA, Shafiei SB, Sharif M, et al. Technical Mentorship during Robot-Assisted Surgery: A Cognitive Analysis? BJU Int. 2016.
I
RO \\rELL
PARK ( \ '\.( .1· R 1'-" rt J'l 'TI~
TO:
DATE:
STUDY TITLE & RPCI Number:
SUBMISSION:
IRB APPROVAL DATE: 4/4/2016
REVIEW TYPE: D AdminiStrative
Elm & Carlton Sts. Buffalo, New York 14263 Institutional Review Board Approval Notice This Institution has an approved assurance of compliance on file with HHS which covers this activity FWA 00006731 Federal Wide Assurance Identification number
Khurshld Guru, MD
~("\ '- '} I O...G \ (9
1 244113 "Observational Study to Identify Patterns in Communication and Team Interaction 1n the Operating Room"
Amendment3
APPROVAL PERIOD: 4/4/2016-3/5/2017
181Expedited D Full board
Please be advised that only the IRB approved and stamped consent form can be used to enroll subjects.
The principal investigator Is responsible for ensuring that the research complies with all applicable regulations. Any modifications In the research project are subject to approval by the Board prior to Initiation by the Investigator. The Board reserves the right to stop the research for violations of regulatory or IRB requirements.
Unanticipated Problems which occur during the course of the research study must be reported to the CRS office to be reported to the IRB in accordance with the RPCI unantiCipated problem reporting policy.
The protocol and consent forms. along with a bnef progress report must be resubmitted to the IRB at least one month pnor to the exp1rat1on date noted above for continUing rev1ew as requ1red by the federal regulations. Please consult the CRS policies and SRCIIRB calendar for the submiSSIOn date for the IRB meeting date pnor to your review date.
Please be adv1sed that your research study may be audited penodically by the IRB for compliance.
Th1s protocol has been submitted to Clln1cal Research Serv1ces (CRS) for process~ng pnor to release for protocol implementation. Please contact CRS for information regarding the protocol implementation release date.
This activity has been reviewed and approved by an IRB In accordance with the requirements of 45 CFR 46, including Its relevant Subparts. This protocol fulfills, when applicable, requi rements for certifying FDA status for each Investigational new drug or device.
Document 181 Protocol 181 Consent form 0 Recruitment Materials
D 0 HIPAA Waiver:
0 Waiver of Informed Consent/ Documentation/Elements
Institute Official or Designee:
Version/Date Document 3/3/2016 [] Delegation Form V.5 -Staff D Investigator Brochure
D Laboratory Manual
0 Pharmacy Manual
0 Other:
I I
Camille P. Wicher, Esq. R . Donald J . Handley, MSc, MBA
Version/Date
~
Rev. 03/2014
ORSP - Non-Human Subject Research Notification
TO: Dr. Guru
FROM: Office of Research Subject Protection
DATE: July 9, 2015
RE: BDR 062715: "Development and Validation of the ProstatectomyAssessment and Competency Evaluation (PACE) score"
APPROVAL PERIOD: July 7, 2015-July 6, 2018
The above referenced research activity has been reviewed and determined to be non-humansubject research (NHSR).
DHHS does not consider research involving data and specimens to involve human subjects asdefined under 45 CFR 46.102(f) if the following conditions are met:
(1) The private information or specimens were not collected specifically for the currentlyproposed research project through an interaction or intervention with livingindividuals; and
(2) The investigator(s) cannot readily ascertain the identity of the individual(s) to whomthe coded private information or specimens pertain.
In accordance with 45 CFR 46.102 of the Common Rule, your protocol does not involve humansubject research. In addition, this research activity does not involve an FDA regulated productor the collection of data to be submitted to or held for inspection by the FDA in support of amarketing application. Therefore, the research is not subject to IRB review.
All proposed changes in research activities must be promptly reported (within 10 businessdays) by the research investigator to the Office of Research Subject Protection (ORSP). If atany time identifiable private information is needed or used as part of the research, the ORSPmust be notified immediately.
In addition, this research project is approved for a period of three (3) years from the date ofnotification. If the research is to be continued beyond three years, a request for continuation isrequired. Please notify ORSP upon completion of the research.
If you have any questions, please do not hesitate to contact me at extension 7676.
K P Nof*-Huf«aii ju ject esearc iooficatioft
TO: Dr. Guru
F OM: Office of es arch Subject Protection
D TE: October 22, 2015
E: BDR 062715: 'Develo m nt and alidation of the ProstatectomyAssess ent and Competency Evaluation (PACE) score
(A endment #1)
APPRO AL PERIOD: O tober 22, 2015 - July 6, 2018
The above referenced research activity has been reviewed nd determined to be non-humansubject research (NHSR).
DHHS does not consider research involving data and specimens to involve human subjects sdefin d under 45 CFR 6.102(f) if the following conditions are met:
(1) The private info mation or specimens were not collected specifically for the currentlyproposed research project hrough an interaction or intervention wi h livingindividuals; an
(2) The investiga or(s) canno readily scertain he identity of the individual(s) to whomhe coded private information or specimens pertain.
In accordance wi h 45 CFR 46.102 of the Common Rule, your protocol does not involve humansubject research. In ddition, this research activity does not involve n FDA regulated producto the collec ion of data o be submitted to or held for inspec ion by the FDA in support of amarketing pplication. Therefore, the research is not subject to IRB review.
AH proposed changes in research activities must be promptly reported (within 10 businessd ys) by the research investigator to the Office of Research Subject Protection (ORSP). If at.any ime identifiable private information is needed or used as part of the research, the ORSPmust be notified immediately.
In ddition, this research project is approved for a period of three (3) years from the date ofnotification. If the research is to be continu d beyond three years, a r quest for continuation isequired. Please notify ORSP upon completion of the research.
If you have any questions, ple se do not: he ita e to contac me at xtension 7676.

Available Resources
Steven Schwaitzberg, MD, is the PI on the grant, a SAGES member and is formally collaborating with ATLAS at Roswell on this project. Dr. Schwaitzberg will be supervising and guiding the surgical training aspect of the project. The work will take place at Roswell Park Cancer Institute in Surgical Robotics and The Applied Technology Laboratory for Advanced Surgery (ATLAS) Program
Institution: Roswell Park Cancer Institute (RPCI), founded in 1898, is the nation’s first cancer research, treatment, and education center. It is the only NCI-designated comprehensive cancer center in upstate New York and one of 45 such centers in the United States. RPCI is a member of the prestigious National Comprehensive Cancer Network (NCCN), an alliance of the nation’s leading cancer centers, maintains affiliate sites, and is a partner in national and international collaborative programs. RPCI has 131 inpatient beds and 12 multidisciplinary specialty clinics with an outpatient volume of nearly 200,000 visits annually. Roswell Park had $90 M in grant dollars in 2014.
Surgical Robotics and The Applied Technology Laboratory for Advanced Surgery (ATLAS) Program and equipment: The ATLAS program directed by the PI, Dr. Khurshid Guru is equipped with state-of-the art laparoscopic and robot-assisted simulators, a full-fledged daVinci Surgical System ®, two conference rooms, four offices, six cubicles, and a fully functioning engineering innovation lab. The engineer lab is equipped with all components necessary to innovate medical software and hardware. The office space includes a full-fledged art studio, and stations for marketing and program outreach professionals, data managers, researchers, fellows, and collaborative PhDs to work.
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
BIOGRAPHICAL SKETCH Provide the following information for the Senior/key personnel and other significant contributors in the order listed on Form Page 2.
Follow this format for each person. DO NOT EXCEED FOUR PAGES.
NAME Schwaitzberg, Steven
POSITION TITLE Professor and Chairman Jacobs School of Medicine.
eRA COMMONS USER NAME (credential, e.g., agency login) SchwaitzbergS EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable.)
INSTITUTION AND LOCATION DEGREE
(if applicable)
MM/YY FIELD OF STUDY
The Johns Hopkins University Baylor College of Medicine Infectious Disease Research/Clinical Fellowship Baylor Affiliated Hospitals Floating Hospital for Children Harvard University
BA MD
MA (hon)
5/1977 8/1980 6/1981 6/1986 6/1986
12/2014
Biology Medicine Infectious Diseases Surgery Pediatric Trauma Surgical Sciences
A. Personal Statement More than a decade ago I began a collaboration with the department of Engineering at Tuft University in the Human Factors Section. Numerous manuscripts were produced from this collaboration. Many of the studies published from this group were in the area of MIS skills training or acquisition which often compared a variety of methods to standard FLS skills training which remains the standard assessment in the area Graduate Students were trained with NSF funding in a wide variety of surgical topics ranging from surgical residency evaluations to the effectiveness of video game training in surgery. I was then appointed Adjunct Associate Professor of Engineering at Tufts University. During this time a novel dynamic training system known as the Dynamite system was developed.) This system was conceived by Dr. Schwaitzberg and developed by one of the graduate students, Audrey Bell with patents applied for (Patent #3 WO 2008033541 A3). The success of the Human Factors- Surgery collaboration continued to grow when I moved in to the Cambridge Health Alliance where we combined interest with colleagues at Harvard Medical School and the Beth Israel Deaconess Medical Center. Human subject studies were then performed at the Carl J. Shapiro Simulation and Skills Center (SASC) in the area of skills training and acquisition. He is This collaboration has continued to grow with the development of a virtual reality computer based skills training program in collaboration with Suvranu De, DSc. Chair, Department of Mechanical, Aerospace, and Nuclear Engineering at Rensselaer Polytechnic Institute. This program currently has 3 open NIH R01 grants engaged in the development VR systems to 1) develop a VR based Fundamentals of Laparoscopic Surgery 2) VR modeling of energy based systems in surgery 3)Modeling collaborative environments in the operating room. 4 manuscripts detailing early works have been published. I have recently moved to a new position as Professor and Chairman of the Department of Surgery at the University at Buffalo School of Medicine and Biomedical Sciences -the State University of New York where we will continue these studies.
In my clinical activity in minimally invasive surgery as well as leadership in the Society of American Gastrointestinal and Endoscopic Surgeons where I have served as past president and currently chair The Fundamentals of Laparoscopic Surgery committee details both the relevant clinical and education career germane to the studies. PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
B. Positions and Honors Position and Employment 1985-1986 Instructor, Department of Surgery, Baylor College of Medicine, Houston, TX 1986-1987 Instructor, Department of Surgery, Tufts University School of Medicine, Boston, MA 1986-1987 Assistant in Surgery, New England Medical Center, Boston, MA 1987-1990 Chief of Surgery, Lemnuel Shattuck Hospital, Jamaica Plain, MA 1987-1993 Assistant Professor, Department of Surgery, Tufts University School of Medicine, Boston, MA 1987-2005 Surgeon New England Medical Center, Boston, MA 1990-1991 Chief of Surgery 365th Evacuation Hospital, US Military Medical Complex, Seeb, Oman 1994-2005 Associate Professor, Department of Surgery, Tufts University School of Medicine, Boston, MA 1994-2005 Associate Professor, Department of Otolaryngology, Head, & Neck Surgery, Tufts University
School of Medicine, Boston, MA 2004-2007 Associate Professor (Adjunct – non-voting), Department of Engineering, Tufts University School
of Medicine, Boston, MA 2005-2008 Visiting Associate Professor, Department of Surgery, Harvard Medical School, Boston, MA 2005-2015 Chief of Surgery Cambridge Health Alliance, Cambridge, MA 2009-2014 Associate Professor, Department of Surgery, Harvard Medical School, Boston, MA 2011-2014 Associate Professor (Adjunct – non-voting), Department of Engineering, Tufts University School
of Medicine, Boston, MA 2011-2015 Associate Professor (Adjunct – non-voting), Bouve College of Health Sciences, Northeastern
University, Boston, MA 2014-2015 Professor of Surgery, Harvard Medical School Boston, MA, 2015- Professor and Chairman Jacobs School of Medicine, University at Buffalo, The State University
of New York 2015- Director of Surgical Programs Great Lakes Health, Buffalo, NY Other Experience and Professional Memberships 2011 Associate Examiner
American Board of Surgery Certifying Exam Special Government Employee (Executive Branch) Consultant
Food and Drug Administration (FDA), Urology/Gastroenterology Advisory Panel (CDRH)
Selected Honors 1977 B.A. General Honors
Phi Beta Kappa The Johns Hopkins University 1985 Outstanding Emergency Physician Recognition Award
Emergency Nurse Association of Texas 1992, 1999 Teaching Award
Chief of Residents in Surgery, New England Medical Center Chief Surgical Resident Teaching Award, Tufts University School of Medicine 2003 Boston area’s Top Physicians 2003 21st Century Laureate Achievement Award – Teaching Digital Video to Surgeons
Computerworld/National Smithsonian Honors 2006-2009 Physician Commendation 2009 Leading Expert in Laparoscopy Patient’s Choice Award 2010 Health Policy Scholar, American College of Surgeons 2013 America’s Most Compassionate Doctors 2015 Top Doctors
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
C. Selected Peer-reviewed Publications 1. Schwaitzberg SD, Dorozhkin D, Sankaranarayanan G, Matthes K, Jones DB, De S. Natural orifice
translumenal endoscopic surgery (NOTES): emerging trends and specifications for a virtual simulator. Surg Endosc. 2015 Apr 4.
2. Schwaitzberg SD Financial modeling of current surgical robotic system in outpatient laparoscopic cholecystectomy: how should we think about the expense? Surg Endosc. 2015 Aug 15.
3. Robinson TN, Olasky J, Young P, Feldman LS, Fuchshuber PR, Jones SB, Madani A, Brunt M, Mikami D, Jackson GP, Mischna J, Schwaitzberg S, Jones DB. Fundamental Use of Surgical Energy (FUSE) certification: validation and predictors of success. Surg Endosc. 2015 Aug 15
4. Nurudeen SM, Kwakye G, Berry WR, Chaikof EL, Lillemoe KD, Millham F, Rubin M, Schwaitzberg S, Shamberger RC, Zinner MJ, Sato L, Lipsitz S, Gawande AA, Haynes AB Can 360-Degree Reviews Help Surgeons? Evaluation of Multisource Feedback for Surgeons in a Multi-Institutional Quality Improvement Project. J Am Coll Surg. 2015 Oct;221(4):837-44. doi: 10.1016/j.jamcollsurg.2015.06.017. Epub 2015 Jul 23
5. Awtrey C, Chellali A, Schwaitzberg S, De S, Jones D, Cao C.Validation of the VBLaST: A Virtual Peg Transfer Task in Gynecologic Surgeons. J Minim Invasive Gynecol. 2015 Jul 26. pii: S1553-4650(15)00538-5. doi: 10.1016/j.jmig.2015.07.015.
6. Mentis HM, Chellali A, Manser K, Cao CG, Schwaitzberg SD. A systematic review of the effect of distraction on surgeon performance: directions for operating room policy and surgical training. Surg Endosc. 2015 Jul 21.
7. Madani A, Watanabe Y, Vassiliou MC, Fuchshuber P, Jones DB, Schwaitzberg SD, Fried GM, Feldman LS. Long-term knowledge retention following simulation-based training for electrosurgical safety: 1-year follow-up of a randomized controlled trial. Surg Endosc. 2015 Jul 3.
8. Sankaranarayanan G, Li B, Manser K, Jones SB, Jones DB, Schwaitzberg S, Cao CG, De S. Face and construct validation of a next generation virtual reality (Gen2-VR©) surgical simulator Surg Endosc. 2015 Jun 20.
9. Sankaranarayanan G, Li B, Miller A, Wakily H, Jones SB, Schwaitzberg S, Jones DB, De S, Olasky J Face validation of the Virtual Electrosurgery Skill Trainer (VEST©). Surg Endosc. 2015 Jun 20.
10. Nemani A, Ahn W, Gee D, Intes X, Schwaitzberg S, Yucel M, De S. Objective Surgical Skill Differentiation for Physical and Virtual Surgical Trainers via Functional Near-Infrared Spectroscopy. Stud Health Technol Inform. 2016;220:256-61.
11. Ahn W, Dorozhkin D, Schwaitzberg S, Jones DB, De S. Developing Modularized Virtual Reality Simulators for Natural Orifice Translumenal Endoscopic Surgery (NOTES). Stud Health Technol Inform. 2016;220:1-4.
12. Pan JJ, Ahn W, Dargar S, Halic T, Li BC, Sankaranarayanan G, Roberts KDe S. Graphic and haptic simulation for transvaginal cholecystectomy training in NOTES. J Biomed Inform. 2016 Apr;60:410-21. . Epub 2016 Mar 12
13. Ghosh AC, Hirsh D, Schwaitzberg S, Ogur B. Bearing witness: a longitudinal integrated cancer care curriculum. Clin Teach. 2016 Feb 4. . [Epub ahead of print]
14. Boehme J, McKinley S, Michael Brunt L, Hunter TD, Jones DB, Scott DJ, Schwaitzberg SD Patient comorbidities increase postoperative resource utilization after laparoscopic and open cholecystectomy. Surg Endosc. 2015 Oct 1.
15. Schwaitzberg SD. Financial modeling of current surgical robotic system in outpatient laparoscopic cholecystectomy: how should we think about the expense? Surg Endosc. 2015 Aug 15.
16. Robinson TN, Olasky J, Young P, Feldman LS, Fuchshuber PR, Jones SB, Madani A, Brunt M, Mikami D, Jackson GP, Mischna J, Schwaitzberg S, Jones DB. Fundamental Use of Surgical Energy (FUSE) certification: validation and predictors of success. Surg Endosc. 2016 Mar;30(3):916-24. doi: 10.1007/s00464-015-4334-3. Epub 2015 Aug
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
17. Nurudeen SM, Kwakye G, Berry WR, Chaikof EL, Lillemoe KD, Millham F, Rubin M, Schwaitzberg S, Shamberger RC, Zinner MJ, Sato L, Lipsitz S, Gawande AA, Haynes AB Can 360-Degree Reviews Help Surgeons? Evaluation of Multisource Feedback for Surgeons in a Multi-Institutional Quality Improvement Project. J Am Coll Surg. 2015 Oct;221(4):837-44. doi: 10.1016/j.jamcollsurg.2015.06.017. Epub 2015 Jul 23.
D. Research Support Ongoing Research Support 2011- 2016 1R01EB009362-01A2 Developing Physics-Based Virtual Simulation Technology for Natural
Orifice Translumenal Endoscopic Surgery Development virtual simulation Natural orifice (NOTES) procedure Role: Consultant 1% effort Suvranu De, PhD PI
2011- 2016 2 R01 EB005807 Objective is to develop an Operating Room Simulator based Head mounted displays. Role: Co-Investigator 1%effort Suvranu De PhD PI
2012-2017 VEST 1R01EB014305 - 01A1 Project to develop virtual simulation of tissue energy interactions with the goal of developing surgical simulation to promote patient safety. Role: Co-Investigator 1 % effort Suvranu, PhD Pi
Completed Research Support 2010-2014 Laparoscopic Surgery Training System (LASTS) Phase I SBIR contract
Office of Naval Research (ONR), US Navy Contract #: N00014-10-M-0152 Goal – Develop Cognitive task Analysis (CTA) for laparoscopic procedures Role: Consultant 1% eff ort P Weyhrauch PI
2010-2015 Prospective Multicenter Human Clinical Trial of NOTES Versus Conventional Cholecystectomy Ethicon, Stryker, Olympus, Storz Consortium Goals: Assess effectiveness of novel surgical technique for cholecystectomy in clinical setting Role: Principal Investigator 3% effort
2010-2015 1R01EB010037-01 Developing a Virtual Basic Laparoscopic Skill Trainer (VBLaST) Development virtual simulation of standard validated laparoscopic skill trainer NIH Role: Consultant 1% effort Suvranu De, PhD PI
2011 -2014 Effects of FLS Completion on Laparoscopic Cholecystectomy Complication Rates Sponsor: Johnson and Johnson Goals: Determine if FLS certification has an independent effect on surgical complication rate. Role: Principal Investigator 2% effort
2011-2014 Laparoscopic Surgery Training System (LASTS) Phase II SBIR contract N00014-11-C-0426 Office of Naval Research Goal – Further develop Cognitive Task Analysis (CTA) for laparoscopic procedure Role: Consultant 1% effort Weyhrauch PI
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
BIOGRAPHICAL SKETCH Provide the following information for the Senior/key personnel and other significant contributors in the order listed on Form Page 2.
Follow this format for each person. DO NOT EXCEED FOUR PAGES.
NAME Guru, Khurshid A.
POSITION TITLE Attending Physician, Urology; Director, Robotic Surgery; Oncology; Professor eRA COMMONS USER NAME (credential, e.g., agency login)
KHURSHIDGURU EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable.)
INSTITUTION AND LOCATION DEGREE (if applicable) MM/YY FIELD OF STUDY
University of Mysore, JJM Medical College M.B.B.S. 1994 Medicine and Surgery
A. Personal Statement As Director of the Robotic Surgery program at Roswell Park, I invest my time and efforts to advance the learning environment for future physicians. Improving the education process for fellows and medical students reduces operating costs, recovery time and improves surgical efficiency. I have established the first structured validated curriculum, entitled the Fundamental Skills of Robotic Surgery (FSRS), as well as the first ever video-based interactive textbook on robotic surgery. As Director of the Applied Technology Laboratory for Advanced Surgery, I have built a multi-disciplinary team of engineers, medical illustrators, and researchers to bridge the strengths of multiple professions into building robust new technological platforms for improved delivery of care. I was one of the first surgeons to be trained in a robot-assisted surgical fellowship. In 2005 I was appointed Director of Robotic Surgery at Roswell Park Cancer Institute (RPCI) and performed the hospitals’ first robotic procedure. I performed one of the first robot-assisted radical cystectomy in New York and worked in the development and evolution of oncologic safety and efficacy of minimally invasive approaches to bladder cancer. Currently, my research focus has been on advancing surgeons training and acquisition of robot-assisted skills, in addition to cognitive performance during robot-assisted surgery. The current application builds logically on my prior work. In summary, I have a demonstrated record of accomplished and productive research projects in an area of advancing modes of education, and my expertise and experience have prepared me to conduct the proposed project. B. Positions and Employment 1993-1994 Rotating Internship, Medical City General Hospital, Manila, Philippines 1994-1994 House Officer, General Surgery, Institute of Medical Sciences, Srinagar, Kashmir India
University of Kashmir 09/1994-6/1996 Research Fellow, Critical Care & Pulmonary Medicine, Nassau County Medical Center,
New York, State University of New York (SUNY) at Stony brook, NY 7/1996-6/1997 Internship, Internal Medicine, Nassau County Medical Center, New York, SUNY at
Stonybrook, NY 7/1997-9/1998 Internship, General Surgery, Long Island Jewish & Beth Israel Medical Center, Albert
Einstein College of Medicine. New York 1/1999-6/2000 Fellow, Urological Surgery, Veterans Administration Medical Center, Togus, Maine 7/2000-6/2003 Resident Physician, Urological Surgery, Vattikuti Urology Institute, Henry Ford Health
Systems, Detroit, Michigan 7/2003-6/2004 Robotic Surgery Fellow, Urological Surgery, Vattikuti Urology Institute, Henry Ford
Health Systems, Detroit, Michigan
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
2/2004-4/2004 International Fellow, Urologic-Oncology, Urology & Nephrology Center, Mansoura University, Mansoura, Egypt
7/2004-7/2005 Chief Resident, Urological Surgery, Vattikuti Urology Institute, Henry Ford Health Systems, Detroit, Michigan
4/2006-2/2011 Assistant Professor of Oncology, Department of Urology, Roswell Park Cancer Institute, Buffalo, NY
9/2005-Present Director of Robotic Surgery, Roswell Park Cancer Institute, Buffalo, New York 9/2006-3/2011 Clinical Assistant Professor, Department of Urology, University at Buffalo, NY 2/2011-Present Associate Professor of Oncology, Department of Urology, Roswell Park Cancer
Institute, Buffalo, NY 3/2011-Present Clinical Associate Professor, Department of Urology, University at Buffalo, NY 2/2012-Present Robert P. Huben Professor of Urologic Oncology Other Experience and Professional Memberships American Urologic Association (AUA) Cancer Society of Kashmir Honors 2012 Editorial Board, British Journal of Urology International 2010 Editorial Board, The Canadian Journal of Urology 2009 AUAER/Pfizer Visiting Professor in Urology, Robert Wood Johnson Medical School, NJ 2004 Pfizer Scholar in Urology 2004 Third Place, Oral Presentation, Michigan Urologic Society 2003 Third Place, Oral Presentation Michigan Urologic Society 1992 First Rank, First Phase of Final Year, University of Mysore, JJM Medical College, Karnataka
India 1989 First Rank, Third Year of Medical School, University of Mysore, JJM Medical College, Karnataka
India C. Selected Peer-reviewed Publications (Selected from 124 peer-reviewed publications) Most relevant to the current application 1. Guru KA, Shafiei SB, Khan A, Hussein AA, Sharif M, Esfahani ET. Understanding Cognitive
Performance During Robot-Assisted Surgery. Urology. 2015 Oct;86(4):751-7. Epub 2015 Aug 5. PMID: 26255037.
2. Ahmad, N., Ahmed, A. A., Cavuoto L., Sharif, M., Allers, J.C., Hinata, N., Ahmad, B., Kozlowski, J., Hashmi, Z., Bisantz, A., Guru, KA. Ambulatory Movements, Team Dynamics and Surgical Flow during Robot-Assisted Surgery. BJU International. 2016 Jan 22. PMID: 26800347.
3. Hussein AA, Shafiei SB, Sharif M, Esfahani E, Ahmad B, Kozlowski JD, Hashmi Z, Guru KA. Technical Mentorship during Robot-Assisted Surgery: A Cognitive Analysis. BJU Int. 2016 Feb 11. PMID: 26864145.
4. Tiferes, J., Hussein, A., Bisantz, A., Kozlowski, J., Ahmad, B., Sharif, M., Winder, N., Ahmad, N., Allers, J., Cavuoto, L., Guru, K. The loud surgeon behind the console: Understanding team activities during robot-assisted surgery. J Surg Educ. 2016 May-Jun;73(3):504-12. PMID: 27068189.
5. Allers JC; Hussein AA, Ahmad N, Cavuoto L, Wing JF, Hayes RM, Hinata N, Bisantz AM, Guru KA. Evaluation and Impact of Workflow Interruptions during Robot-Assisted Surgery. Urology. 2016 Jun;92:33-7. PMID: 26864145.
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
Additional recent publications of importance to the field (in chronological order) 1. Lovegrove C, Novara G, Mottrie A, Guru KA, Brown M, Challacombe B, Popert R, Raza J, Van der
Poel H, Peabody J, Dasgupta P, Ahmed K. Structured and Modular Training Pathway for Robot-assisted Radical Prostatectomy (RARP): Validation of the RARP Assessment Score and Learning Curve Assessment. Eur Urol. 2016 Mar;69(3):526-35. PMID: 26585582
2. Hussein AA, Hashmi Z, Dibaj S, Altartir T, Fiorica T, Wing J, Durrani M, Binkowski J, Boateng L, Wilding G, Guru KA. Reoperations following Robot-Assisted Radical Cystectomy: A Decade of Experience. J Urol. 2015 Nov 6. pii: S0022-5347(15)05198-8. PMID: 26551296
3. Hanzly MI, Al-Tartir T, Raza SJ, Khan A, Durrani MM, Fiorica T, Ginsberg P, Mohler JL, Kuvshinoff B, Guru KA. Simulation-based training in robot-assisted surgery: current evidence of value and potential trends for the future. Curr Urol Rep. 2015 Jun;16(6):41. PMID: 26003110
4. Chan KG, Guru KA, Wiklund P, Catto J, Yuh B, Novara G, Murphy DG, Al-Tartir T, Collins JW, Zhumkhawala A, Wilson TG. Robot-assisted Radical Cystectomy and Urinary Diversion: Technical Recommendations from the Pasadena Consensus Panel. Eur Urol. 2015 Mar;67(3):423-431. PMID: 25595099
5. Wilson TG, Guru KA, Rosen RC, Wiklund P, Annerstedt M, Bochner BH, Chan KG, Montorsi F, Mottrie A, Murphy D, Novara G, Peabody JO, Palou Redorta J, Skinner EC, Thalmann G, Stenzl A, Yuh B, Catto J. Best Practices in Robot-assisted Radical Cystectomy and Urinary Reconstruction: Recommendations of the Pasadena Consensus Panel. Eur Urol. 2015 Mar;67(3):363-375.
6. Novara G, Catto JW, Wilson T, Annerstedt M, Chan K, Murphy DG, Motttrie A, Peabody JO, Skinner EC, Wiklund PN, Guru KA, Yuh B. Systematic Review and Cumulative Analysis of Perioperative Outcomes and Complications After Robot-assisted Radical Cystectomy. Eur Urol. 2015 Mar;67(3):376-401.
7. Yuh B, Wilson T, Bochner B, Chan K, Palou J, Stenzl A, Montorsi F, Thalmann G, Guru KA, Catto JW, Wiklund PN, Novara G. Systematic Review and Cumulative Analysis of Oncologic and Functional Outcomes After Robot-assisted Radical Cystectomy. Eur Urol. 2015 Mar;67(3):402-422.
8. Raza SJ, Field E, Jay C, Eun D, Fumo M, Hu JC, Lee D, Mehboob Z, Nyquist J, Peabody JO, Sarle R, Stricker H, Yang Z, Wilding G, Mohler JL, Guru KA. Surgical competency for urethrovesical anastomosis during robot-assisted radical prostatectomy: development and validation of the robotic anastomosis competency evaluation. Urology. 2015 Jan;85(1):27-32.
D. Research Support Ongoing Research Support Roswell Park Alliance Foundation Guru (PI) 02/14/11 – 03/31/17 WNY Center for Robotic Surgery The Center for Robotic Surgery will train teams that will practice robotic surgery in Western New York hospitals, thereby enhancing the quality of healthcare in this region. Role: PI Roswell Park Alliance Foundation Guru (PI) 8/21/14 – 07/31/19 Advanced Technology Laboratory for Assisted Surgery (ATLAS) The goal of this study is to assess the effectiveness of virtual reality and augmented reality procedure based training in robot assisted surgery. Role: PI Roswell Park Alliance Foundation/Vattikuti Foundation Guru (PI) 1/01/14 – 12/31/16 International Radical Cystectomy Consortium
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
The IRCC is a web-based, user-friendly database collecting quality assurance measures in a secure and HIPPA-compliant manner from an international audience of surgeons. Role: PI Completed Research Support Roswell Park Alliance Foundation/John R. Oishei Foundation Guru (PI) 7/1/09 - 6/30/14 Center for Robotic Surgery The Center for Robotic Surgery will train teams that will practice robotic surgery in Western New York hospitals, thereby enhancing the quality of healthcare in this region. The Center will also provide training for teams from outside Western New York, thereby establishing Roswell Park Cancer Institute as a pioneering institution in robotic surgery training and making Western New York a leading center for robotic surgical training in the United States Role: PI Roswell Park Alliance Foundation/John R. Oishei Foundation Guru (PI) 8/1/06 - 6/30/10 Center for Robotic Surgery The goal is to assess the effectiveness of virtual reality and augmented reality procedure-based training in robot assisted surgery. Role: PI Roswell Park Alliance Foundation (Guru) 11/1/10 - 9/30/13 Validation Study on RoSS Validation Study of the RoSS at six Beta test sites Role: PI Roswell Park Alliance Foundation Guru (PI) 2/01/09 - 8/31/10 Robotic Surgical Simulator (RoSS) Development Role: PI
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
BIOGRAPHICAL SKETCH Provide the following information for the Senior/key personnel and other significant contributors in the order listed on Form Page 2.
Follow this format for each person. DO NOT EXCEED FOUR PAGES.
NAME Zsiros, Emese
POSITION TITLE Assistant Professor of Oncology, Department of Gynecologic Oncology eRA COMMONS USER NAME (credential, e.g., agency
login) EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable.)
INSTITUTION AND LOCATION DEGREE
(if applicable)
MM/YY FIELD OF STUDY
University of Debrecen Medical and Health Science Center, Debrecen Hungary
M.D.
09/2005 Medicine
Department of Biophysics and Cell Biology, Debrecen, Hungary in conjunction with the Universidad de Complutense, Madrid, Spain
Ph.D.
05/2011
Membrane Biology, Immunology
OB/GYN resident, McGaw Medical Center, Northwestern University, Chicago, IL 06/2011 OB/GYN resident
University of Pennsylvania, Philadelphia, PA
06/2014
Gynecologic Oncology fellow
A. Personal Statement During my fellowship training at the University of Pennsylvania I was actively involved in planning and conducting early phase immunotherapy clinical trials for patients with ovarian cancer. I had also completed a year-long training in Patient Oriented Research by the Institute of Translational Medicine at the University of Pennsylvania. My research thesis focused on the chemokine microenvironment of advanced stage ovarian cancer and the homing of T cells to tumor microenvironment. Currently as a new faculty at Roswell Park Cancer Institute my protected research time focuses on the ovarian cancer tumor microenvironment as well as developing novel therapeutic targets that offer better clinical outcome and quality of life to our patients with ovarian cancer. I am specifically interested in anti-PD1 therapy combined with antiangiogenic and regulatory T cell depleting approaches and have a new clinical trial ready to enroll patients within the next few months. I am also interested in modifying the chemokine microenvironment with novel oral CXCR4 blockade in combination with check-point inhibitors and anti-VEGF treatment in preclinical models, which will lead to a phase I/II clinical trial in the next year. Moreover, I have special interest in surgeon education and development of objective assessment tools that can be used to evaluate trainees and provide structured feedback that can be used to tailor training activities.
B. Positions and Honors 2007-2011 OB/GYN resident at McGaw Medical Center, Northwestern University, Chicago, IL 2011-2014 Gynecologic oncology fellow at the University of Pennsylvania, Philadelphia, PA
PHS 398/2590 (Rev. 06/09) Biographical Sketch Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
2014-present Attending Staff Physician, Department of Gynecologic Oncology, Roswell Park Cancer Institute
Membership: Diplomate of the American Board of Obstetrics and Gynecology (ABOG) Fellow of the American Congress of Obstetricians and Gynecologists (FACOG) Candidate member of the Society of Gynecologic Oncology (SGO) Full Member of the American Association for Cancer Research (AACR) Full Member of the American Society of Clinical Oncology (ASCO) Associate Active Member of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) Honors: 2005: Outstanding Research Award, Hungarian Society of Physiologists 2005: Paul Harris Fellowship, Rotary International 2008, 2009: Teaching Award at Feinberg School of Medicine, Northwestern University 2011: Ralph Reis Research Award, Department of Obstetrics and Gynecology, Northwestern
University C. Selected Peer-reviewed Publications 1. Hajas G, Zsiros E, Laszlo T, Hajdu P, Somodi S, Rethi B, Gogolak P, Ludanyi K, Panyi G, Rajnavolgyi E: New phenotypic, functional and electrophysiological characteristics of KG-1 cells. Immunol Lett. 2004 Mar 29;92(1-2):97-106. 2. Petrohai A, Nagy G, Bosze S, Hudecz F, Zsiros E, Paragh G, Nyarady Z, Nemeth P, Berki: Detection of citrate synthase-reacting autoantbodies after heart transplantation: an epitope mapping study. Transpl Int. 2005 May;17(12):834-40 3. Kosztáczky B, Fóris G, Paragh G Jr, Seres I, Zsiros E, Koncsos P, Balogh Z, Paragh G. Leptin stimulates endogenous cholesterol synthesis in human monocytes: New role of an old player in atherosclerotic plaque formation. Int J Biochem Cell Biol 2007;39(9):1637- 45. Epub 2007 Apr 25 4. Balogh Z, Foris G, Kosztaczky B, Paragh G Jr, Seres I, Zsiros E, Konya G, Paragh G. The concentration dependent biphasic effect of leptin on endogenous cholesterol synthesis in human monocytes. Peptides. 2007 Oct;28(10);2081-3. 5. Zsiros E, Kis-Toth K, Hajdu P, Gaspar R, Bielanska J, Felipe A, Rajnavolgyi E, Panyi G. Developmental switch of the expression of ion channels in human dendritic cells, J Immunol. 2009 Oct 1;183(7):4483-92. 2009 Sep 11 6. Climent B, Zsiros E, Stankevicius E, Villa PD, Panyi G, Simonsen U, García-Sacristán A, Rivera L.: Intact rat superior mesenteric artery endothelium is an electrical syncytium and expresses strong inward rectifier K(+) conductance, Biochem Biophys Res Commun. 2011 Jun 7. 7. Barber E, Zsiros E, Rademaker A, Lurain J, Schink J, Neubauer N: The Combination of Intravenous Bevacizumab and Metronomic Oral Cyclophosphamide is an Effective Regimen for Recurrent Platinum Resistant Ovarian Cancer, J. of Gynecologic Oncology, July, 2013 8. Zsiros E, Tanyi J, Balint K, Kandalaft LE: Immunotherapy for ovarian cancer: recent advances and perspectives, Curr Opin Oncol. 2014 Sep;26(5):492-500. 9. Zsiros E, Odunsi, K: Tumor-associated macrophages: co-conspirators and orchestrators of immune suppression in endometrial adenocarcinoma. Gynecol Oncol. 2014 Nov;135(2):173-5. 10. Zsiros E, Duttagupta P, Garrabrant T, Dangaj D, Li H, Frank F, Garrabrant T, Hagemann IS, Levine B, June CH, Zhang L, Wang E, Marincola FM, Bedognetti D, Powell DJ, Tanyi J, Feldman MD, Kandalaft LE, PHS 398/2590 (Rev. 06/09) Continuation Format Page
Program Director/Principal Investigator (Last, First, Middle): Schwaitzberg, Steven
Coukos G: The Ovarian Cancer Chemokine Landscape is Conducive to Homing of Vaccine-primed and CD3/CD28 Costimulated T cells Prepared for Adoptive Therapy, Clin Cancer Res. 2015 Jun 15;21(12):2840-50 11. Zsiros E, Tsuji T, Odunsi K.: Adoptive T-cell therapy is a promising salvage approach for advanced or recurrent metastatic cervical cancer, J Clin Oncol. 2015 May 10;33(14):1521-2 12. Zsiros E, Dangaj D, June CH, Kandalaft LE, Coukos G: Ovarian Cancer Chemokines May not be a significant barrier during whole tumor antigen dendritic-cell vaccine and adoptive T-cell immunotherapy, OncoImmunology, 19 Oct 2015; 5(5).
D. Research Support Ongoing Research Support Faculty start up fund from the Center for Immunotherapy and the Department of Gynecologic Oncology at Roswell Park Cancer Institute: 09/01/2014 – 8/31/2017 Time commitment: 40% Completed Research Support None
PHS 398/2590 (Rev. 06/09) Continuation Format Page
Participation in SAGES
Committees
1998-2001 Chairman, Technology Committee 1998-2004 Fundamentals of Laparoscopy Surgery Committee 2000-2007 Chairman, Development Committee 2000 Chairman, Learning Center 2001, 2003-2008 Postgraduate Course Director 2002-2004 Board of Governors 2004-2006 Second Vice President 2005-2010 Chairman, Program Committee 2007 Program Chair for Annual Meeting 2007-2010 First Vice President 2010-2011 President-Elect 2011-2012 President 2012-2013 Immediate Past President 2012 Chairman Nominating Committee 2012 – Chairman Fundamentals of Laparoscopic Surgery Committee 2016 Distinguished Service Award
Presentation
2010 Adrenal Incidentaloma, MIS and Cancer Endocrine/Solid Organ Postgraduate Course - SAGES Annual Meeting, Washington, DC
2012 You Must be the Change You Wish to See in the World, SAGES Presidential Address - SAGES, San Diego, CA
2013 The Stretta procedure: What’s the real data? - SAGES Annual Meeting, Baltimore, MD 2013 Is it Time to Play Taps for Single Port Surgery? - SAGES’ Presidential Debate, Baltimore, MD 2014 Legal aspects and HIPAA requirements when recording surgical procedures - SAGES Annual Meeting
Salt Lake City, UT 2015 Prospective Randomized Trial of NOTES versus Laparoscopic Cholecystectomy - SAGES Scientific
Session Plenary Presentation, Nashville, TN Service to the Profession
SAGES Grant Review Committee
National and International Departmental Service
2009 Symposium Director/organizer: Society of American Gastrointestinal and Endoscopic Surgeons(SAGES)/Japanese Society of Endoscopic Surgery (JSES) – Symposium in Issues in Minimally Invasive Surgery, Tokyo, Japan
2010 Symposium Director/organizer: Society of American Gastrointestinal and Endoscopic Surgeons(SAGES)/ Association Latino Americana de Cirugia Endoscopica (ALACE) Symposium: Management of Complication in Minimally Invasive Surgery
Sponsored by ALACE/ Sociedade Brasileira de Videocirurgia (SOBRACIL), Salvador, Brazil
Courses Directed
2011 Session Co- Chair and Organizer: The Epidemic of Obesity: Surgical Implications Kelly and Carlos Pelligrini SSAT/SAGES Joint Symposium
Formally Supervised Trainees
1992-1998 Daniel M Herron, MD FACS - 1 year laboratory fellow, 5 years surgical residency.
Multiple publications while a fellow. Professor of Surgery. Chief of Minimally Invasive Surgery, Bariatric Surgery, Mount Sinai Hospital, New York, NY Second Vice-President of SAGES 2009-2011. SAGES Program Chair 2011. ASMBS Program Co- Chair 2012. Chair SAGES Program Committee. Considered a national and international expert in bariatric surgery, he has 41 publications focused on MIS and Bariatric surgery.
Clinical Reviews
1. Herron DM, Marohn M, The SAGES-MIRA Robotic Surgery Consensus Group (Advincula A Aggarwal S, Palese M, Broderick T, Broeders I, Byer A, Curet M, Earle D, Giulianotti P, Grundfest W, Hashizume M, Kelley W, Lee D, Weinstein G, McDougall E, MeehanJ, Melvin S, Menon M, Oleynikov D, Patel V, Satava R, Schwaitzberg S). A consensus document on robotic surgery. Surg Endosc 2008; 22:313 – 325.
2. Society of American Gastrointestinal and Endoscopic Surgeons, Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) statement on the relationship between professional medical associations and industry. Surg Endosc 2010;24: 742-744 **Chaired writing committee
3. Rattner DW, Hawes R, Schwaitzberg S, Kochman M, Swanstrom L. The Second SAGES/ASGE White Paper on natural orifice transluminal endoscopic surgery: 5 years of progress. Surg Endosc. 2011 Feb 27. [Epub ahead of print
4. Feldman LS, Brunt LM, Fuchshuber P, Jones DB, Jones SB, Mischna J, Munro MG, Rozner MA, Schwaitzberg SD; for the SAGES FUSE™ Committee. Rationale for the Fundamental Use of Surgical Energy™ (FUSE) curriculum assessment: focus on safety Surg Endosc. 2013 Jul 17.
5. Fuchshuber PR, Robinson TN, Feldman LS, Jones DB, Schwaitzberg SD.The SAGES FUSE program: bridging a patient safety gap. Bull Am Coll Surg. 2014 SEP;99(9):18-27. No abstract available.
Non-Peer-Reviewed Journals for a Professional Audience
EDUCATIONAL MATERIAL (COURSE SYLLABI):
1. Schwaitzberg SD. Surgeon in the Digital Age: Video Editing for Surgeons 2002, 2003. SAGES IPEG Post Graduate Course; 2005.
2. Schwaitzberg SD. Surgeon in the Digital Age: PDA for Surgeons 2004. SAGES Post Graduate Course. 3. Schwaitzberg SD. Surgeon in the Digital Age: Understanding Operating Room Video 2005; SAGES Post
Graduate Course.
Book Chapters
Schwaitzberg SD SAGES History & Commitment to Education and Safety in SAGES Manual on Quality, Outcome and Safety Springer Verlag 2011 Schwaitzberg, SD Evolultions and Revolutions in Surgical Energy In Jones, DJ, Fuchshuber,P, and Feldman L SAGES Manual The Fundamental Use of Surgical Engergy, Springer Verlag
Videos
1. Sachs B, Schwaitzberg SD. Lumbosacral Discectomy and Spinal Fusion. SAGES, Orlando, FL; March 13, 1995.
2. Schwaitzberg SD. The Utility of Articulated Manual Laparoscopic Instruments. Society of American Gastrointestinal Endoscopic Surgeons (SAGES), Dallas, TX; April 2006.
3. Lasellatta A, Fellinger E, Schwaitzberg SD. Against Occam's Razor: TAP repair of Recurrent Inguinal Hernia with Concomitant Inversion of Original Propylene Plug. Society of American Gastrointestinal Endoscopic Surgeons (SAGES), Washington, D.C. April 2010
4. Reddy S and Schwaitzberg, SD: Thoracoscopic Resection of Giant Mediastinal Parathyroid Adenoma Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) San Diego, CA 2012
5. Basu, CB and Schwaitzberg SD. Malpractice Experience with Laparoscopic Cholecystectomy in Massachusetts 1990-1998, Society Of American Gastrointestinal Endoscopic Surgeons (SAGES) San Antonio, TX; March 24-27 1999
6. Pare, G, Frieberg, M, Heilman C, Schwaitzberg SD. The Use of Ventriculoperitoneal Shunt in Laparoscopic Surgery. Society of American Gastrointestinal Endoscopic Surgeons (SAGES) San Antonio, TX March 24-27 1999
7. Park J, Quinn C, Balky h, Connolly R, Nardella P, Schwaitzberg SD. Radiofrequency Powered Linear Stapler. Society of American Gastrointestinal Endoscopic Surgeons (SAGES) San Antonio, TX: March 24-27 1999.
8. Moreau L, Graham R, Schwaitzberg SD. Cervical Scar Perception Influences the Need for Minimally Invasive Procedures, (SAGES), Atlanta, GA; March 2000.
9. Arnold WA, Schwaitzberg SD, Connolly Rogers G. Endoscopic Robotic Telemanipulator Versus Conventional Laparoscopic Instruments: Comparison Of Laparoscopic Task Performance for Surgically Naive Subjects. (SAGES) St Louis, MO; Aril 19-21, 2001.
10. Schwaitzberg, SD and Riskind D. Advances in Laparoscopic Clip Design: The Preformed Clip (SAGES) St Louis, MO; April 19-21, 2001.
11. Mixter TG, Rhim C, Arnold WA, Schwaitzberg, SD. Laparoscopic Hernia Repair in a Community Based Videoscopic Surgical Center. SAGES St Louis, MO; April 19-21, 2001
12. Ibrahim Salama and Schwaitzberg SD. Utility of Voice-Activated System in Minimally Invasive Surgery. SAGES Los Angeles, CA; March 2003.
13. Amanda Rhee and Schwaitzberg SD. Cost Containment Strategies for Laparoscopic Appendectomy SAGES Los Angeles, CA; March 2003.
14. Caroline Cao and Schwaitzberg SD. Visuomotor Constraints in Laparoscopic Surgery: A Human Factors Engineering Perspective. SAGES Los Angeles, CA; March 2003.
15. Misra, M, Schiff, J, Rendon, G, Rothschild J, Schwaitzberg, S. Laparoscopic Cholecystectomy in High Risk Cardiac Surgery Patients. (SAGES) Ft. Lauderdale, FL; April 13-16, 2005.
16. Ngyuen T, Cao, C, Schwaitzberg, SD. Force and Friction Assessment in Laparoscopic Surgery SAGES Dallas, TX; April 26-26, 2006.
17. Schwaitzberg, SD. Comparison of Trocar Insertion Force in MIS SAGES April 26-26, 2006 Dallas, TX. 18. Nemani A, Sankaranarayanan G, Roberts KE, Schwaitzberg SD, Jones, DB, De, S Time Series Analysis
for Transvaginal Notes and Laparoscopic Cholecystectomy SAGES 2013, Baltimore, MD 19. Kaplan, C, Lanigan A, Lin H, Sankaranarayanan G, Ritter ME, Schwaitzberg SD, Jones,DB, DeS
Exposure to FLS Task Outweighs Video Gaming Experience for the VBLaST PT(c) Simulator. SAGES 2013, Baltimore, MD
20. Feldman LS , Fuchshuber P , Jones DB , MD, Mischna J , Munro MG , MD, Schwaitzberg SD, Fuse Task Force. Rationale for the Fundamental Use of Surgical Energy(tm) (fuse) Educational Program SAGES 2013, Baltimore, MD
21. Dunkin BJ, , Wilcox V, Lababidi H, Al Harthi B, Al Froukh J , Al Ammar M , Okrainec A, Schwaitzberg S ,. Successful Fundamentals of Laparoscopic Surgery (FLS) Testing for Practicing Surgeons in the Middle East SAGES 2013, Baltimore, MD
22. Schwaitzberg SD, Jones DB, Scott D, McKinley SK, Hunter T, Castrillion J, Gunnarson C, Brunt LM . Duct Injury Prevention Requires a New National Training Paradigm Despite Successful Deployment of FLS SAGES 2014 Salt Lake City, UT.
23. Boehme,J, Jones DB, Scott D McKinley SK, Hunter T, Brunt LM, Schwaitzberg SD, Duct Injury Prevention Requires a New National Training Paradigm SAGES 2015 Nashville TN





























