Embed Size (px)
Citation preview

Dr. Rosanna Chau Bobath Instructor(IBITA) FHKCOP; FHKSMS; DHSc ;
MSc(HC-Physio) ; MHSc(Geron) Dip (Acup) ; PD (Physio) Department Manager,
Physiotherapy Department Kowloon Hospital
Hospital Authority Convention 2015
AH II – Technology Advancement & Innovation
19 May 2015
Integrating Transcranial Magnetic Stimulation in
Physiotherapy for Patients with Stroke
Ms. Helen Luk DHSc Candidate; MHSc(Geron)
Dip (Acup) ; PD (OSH); BSc (Physio) Senior Physiotherapist
Queen Elizabeth Hospital
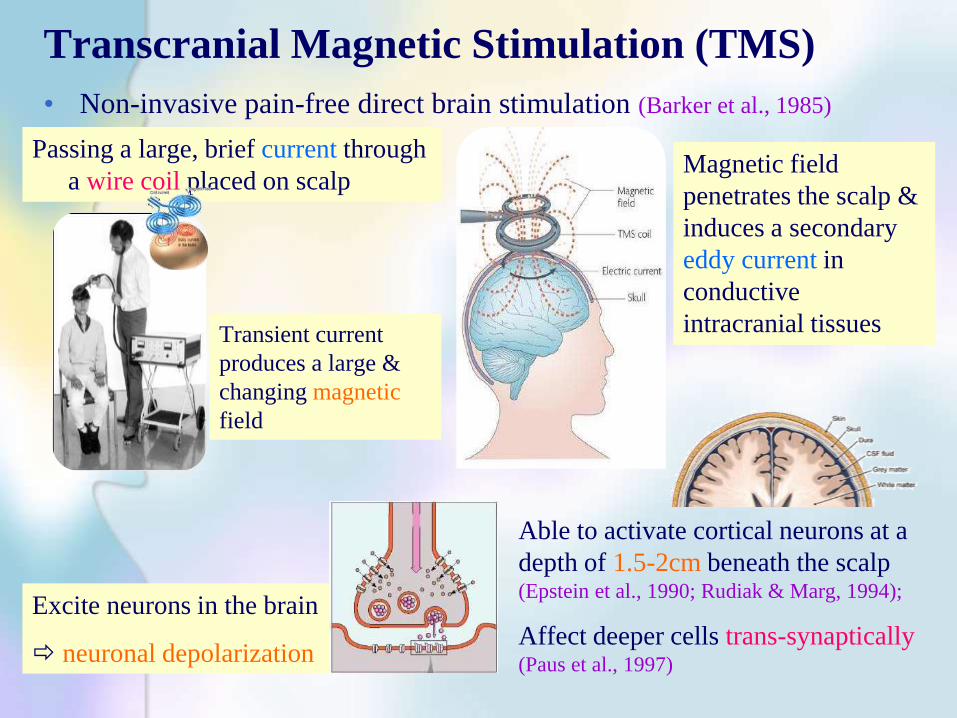
Transcranial Magnetic Stimulation (TMS)
• Non-invasive pain-free direct brain stimulation (Barker et al., 1985)
Passing a large, brief current through
a wire coil placed on scalp
Transient current
produces a large &
changing magnetic
field
Magnetic field
penetrates the scalp &
induces a secondary
eddy current in
conductive
intracranial tissues
Excite neurons in the brain
neuronal depolarization
Able to activate cortical neurons at a
depth of 1.5-2cm beneath the scalp (Epstein et al., 1990; Rudiak & Marg, 1994);
Affect deeper cells trans-synaptically (Paus et al., 1997)

Commonly Used TMS Units
Magstim
Nexstim
NeuroStar Magpro

Navigated TMS (Neuronavigator) - Frameless Stereotaxic System
• An accessory to TMS
• Assist in precise placement of TMS coils to target brain site indicated
on an MRI scan

Single Pulse
• Measure motor threshold, motor evoked potential
• Mapping motor cortical outputs
Paired Pulse
• Measure intra-cortical facilitation & inhibition
• Study cortico-cortical interactions
Repetitive Stimulation
• High frequency vs. low frequency
To the same hemisphere
To both hemisphere
Diagnostic Therapeutic
Utility of Transcranial Magnetic Stimulation
Measure connection between brain & muscle, e.g.
disorders affecting facial, cranial nerves & spinal
cord
Stimulate / inhibit brain
activities for function
enhancement
Therapeutic Application of TMS
• Depression
• Stroke
• Neglect
• Aphasia
• Epilepsy – Myoclonic, focal status
epilepticus
• Modulate cortical excitability for normalization of activity in the
targeted brain region e.g. Depression
• Suppress activity in brain region & induce paradoxical behavioral
facilitations through distant effects e.g. Neglect
• Enhance motor performance
• Facilitate adaptive brain plasticity
• Help to develop models of functional connectivity between different
brain regions
• Movement disorders
• Dystonia
• Parkinson disease
• Neuropathic pain
• Auditory hallucinations
• Tinnitus, Migraine

Repetitive Transcranial Magnetic Stimulation
in Stroke Rehabilitation

Interhemispheric Competition Model Healthy Subjects
Balanced interaction
between the 2 hemisphere
Physical Rehabilitation
Training strategy
Strategies for Promoting Motor Recovery after Stroke
To re-establish a normalized interhemispheric balance
between the lesioned & healthy hemispheres
Imbalance of interhemispheric inhibition
After stroke
stroke
Cortical excitability in affected primary motor cortex
Transcallosal inhibition from the intact to the damaged motor cortex
excitability in
affected hemisphere
excitability in the
unaffected hemisphere
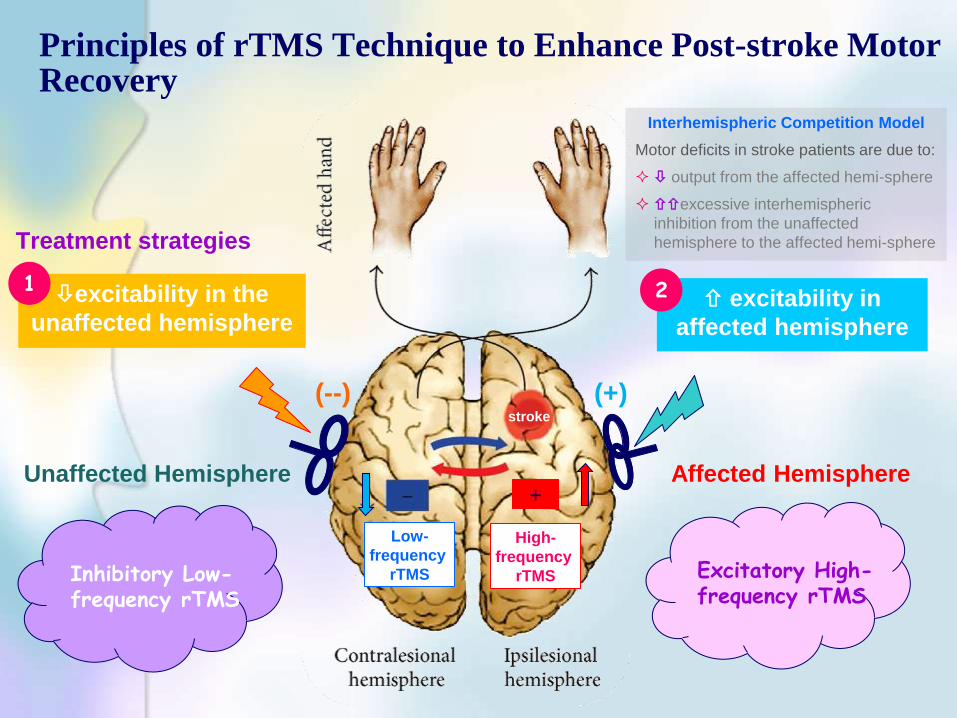
Excitatory High-frequency rTMS
Inhibitory Low-frequency rTMS
Principles of rTMS Technique to Enhance Post-stroke Motor Recovery
Interhemispheric Competition Model
Motor deficits in stroke patients are due to:
output from the affected hemi-sphere
excessive interhemispheric
inhibition from the unaffected
hemisphere to the affected hemi-sphere
Treatment strategies
High-
frequency
rTMS
Low-
frequency
rTMS
+
1 2
Affected Hemisphere Unaffected Hemisphere
(+) (--) stroke

Enhancing Motor Recovery after Stroke Using Repetitive Transcranial Magnetic Stimulation (rTMS)
• Tretriluxana et al., 2013
• Seniów et al., 2012
• Wang et al., 2012
• Conforto et al., 2012
• Takeuchi et al., 2008
• Nowak et al., 2008
• Kirton et al., 2008
• Dafatakis et al., 2008
• Liepert et al., 2007
• Fregni et al., 2006
• Boggio et al., 2006
• Fregni et al., 2006
• Mansur et al., 2005
• Takeuchi et al., 2005
• Kakuda et al., 2013b
• Kakuda et al., 2013a
• Sung et al., 2013
• Takeuchi et al., 2009
• Talelli et al., 2007
• Khedr et al., 2010
• Yozbatiran et al., 2009
• Khedr et al., 2009
• Talelli etal., 2007
• Malcom et al., 2007
• Kim et al., 2006
• Khedr et al., 2005
(+) (--)
stroke
rTMS rTMS Inhibitory Low-frequency rTMS
Excitatory High-frequency rTMS

Inhibitory rTMS over Unaffected Hemisphere (1)
Author yrs Study
design
Patient
group
Stimulation
parameter
Stimulation
area Results
Takeuchi et
al., 2005
Double-
blinded,
crossover,
sham-
controlled
Chronic
stroke
(6-60 mo)
1Hz, 90%
resting motor
threshold, 25
mins, 1500
pulses
Unaffected
hemisphere,
hand area,
1o motor
cortex
20% peak pinch acceleration
immediately after intervention, no
improvement on pinch force
Mansur et al.,
2005
Single-
blinded,
crossover,
sham-
controlled
Subacute
stroke
(12 mo)
1Hz, 100%
resting motor
threshold, 10
mins, 600
pulses, 3
sessions
Unaffected
hemisphere,
hand area,
1o motor
cortex
16 & 11% in simple & choice
reaction times; 33% in Purdue
Pegboard Test, no improvement in
index finger tapping test
Fregni et al.,
2006
Single-
blinded,
randomized,
sham-
controlled
Subacute
stroke
1Hz, 100%
resting motor
threshold, 20
mins, 1200
pulses x 5 days
Unaffected
hemisphere,
hand area,
1o motor
cortex
15 & 5% in JTHHT (post-Rx &
14 days FU); 50% in simple &
choice reaction times (both post-
Rx & 14 days FU), 60% in
Purdue Pegboard test (both post-
Rx & 14 days FU)
Boggio et al.,
2006
Single-case
study,
double-
blinded
Chronic
stroke (23
mo)
1Hz, 100% rMT,
20 mins, 1200
pulses, 2
session( 2 mo
apart btw
session)
Unaffected
hemisphere,
hand area,
1o motor
cortex
5o&15o/ 10o&20o of thumb &
finger mov’t (after 1st & 2nd rTMS
sessions resp.), no change in
Modified Ashworth scale
Low-frequency rTMS

Inhibitory rTMS over Unaffected Hemisphere (2)
Author yrs Study
design
Patient
group
Stimulation
parameter
Stimulation
area Results
Liepert et al.,
2007
Double-blinded,
crossover,
sham-
controlled
Acute
stroke
(<14 day)
1Hz, 90% of
resting motor
threshold, 25
mins
Unaffected
hemisphere,
hand area,
1o motor cortex
No improvement in peak
grip force, 10% in Nine
Hole Peg Test
Nowak et al.,
2008
Double-blinded,
crossover,
sham-
controlled
Subacute
stroke
(1-4 mo)
1Hz, 90% resting
motor threshold,
10 mins
Unaffected
hemisphere,
hand area,
1o motor cortex
25% in vel. & freq. of
index finger tapping, 30%
of vel. & timing of grasping
mov’t
Takeuchi et
al., 2008
Double-blinded,
crossover,
sham-
controlled
Chronic
stroke
(7-121
mo)
1Hz, 90% of
resting motor
threshold, 25
mins
Unaffected
hemisphere,
hand area,
1o motor cortex
30% & 20% in pinch
acceleration & peak pinch
force immediately & at 1
week post-Rx
Dafotakis et
al., 2008
Double-blinded,
crossover,
sham-
controlled
Subacute
to chronic
stroke
(1-15 mo)
1Hz, 100%
resting motor
threshold, 10
mins
Unaffected
hemisphere,
hand area,
1o motor cortex
30% in efficiency & 40%
in timing of grip force
kinetics when grasping &
lifting an object
Kirton et al.,
2008
Single-blinded,
randomized,
sham-
controlled
Chronic
stroke
(3-13 yrs)
1Hz, 100%
resting motor
threshold,
20mins x 8 days
Unaffected
hemisphere,
hand area,
1o motor cortex
9% of Medboune Ax of UE
fx, 20% grip strength
Low-frequency rTMS

Author yrs Study
design
Patient
group
Stimulation
parameters
Stimulation
area Results
Wang et al.,
2012
Double-
blinded,
randomized,
sham-
controlled
Chronic
stroke
(0.8-4.5
yr)
1Hz, 10 mins,
90% of rMT, 600
pulses + 30mins
task-orientated
training, 5/wk,2
weeks
Unaffected
hemisphere,
leg area,
1o motor
cortex
corticomotor excitability
symmetry, spatial gait symmetry,
motor control & walking ability in
rTMS gp
Conforto et
al., 2012
Double-
blinded,
randomized,
sham-
controlled
Acute
stroke
(5-45
days)
1Hz, 90% of
resting motor
threshold, 25
mins (1500
pulses)
Unaffected
hemisphere,
hand area,
1o motor
cortex
12.3% in the Jebsen-Taylor test
& pinch force (0.5 N) in the
active group
Seniów et
al., 2012
Double-
blinded,
randomized,
sham-
controlled
Subacute
stroke
(3 mo)
1Hz, 90% of
resting motor
threshold, 1800
pulses, (30 mins),
5/wk,3 weeks
Unaffected
hemisphere,
hand area,
1o motor
cortex
12.3% in the Jebsen-Taylor test
& pinch force (0.5 N) in the
active group
Tretriluxana
et al., 2013
Crossover,
sham-
controlled
Chronic
stroke
(4.8 yrs)
1Hz, 90% resting
motor threshold,
20mins (1200
pulses)
Unaffected
hemisphere,
hand area,
1o motor
cortex
total mov’t time & peak grasp
aperture, but no changes in peak
transport vel. or time of peak
transport vel or time of peak
aperture after active rTMS. Active
rTMS gp completed RTG actions
with a more coordinated pattern
Low-frequency rTMS
Inhibitory rTMS over Unaffected Hemisphere (3)
Author yrs Study
design
Patient
group Stimulation parameter
Stimulatio
n area Results
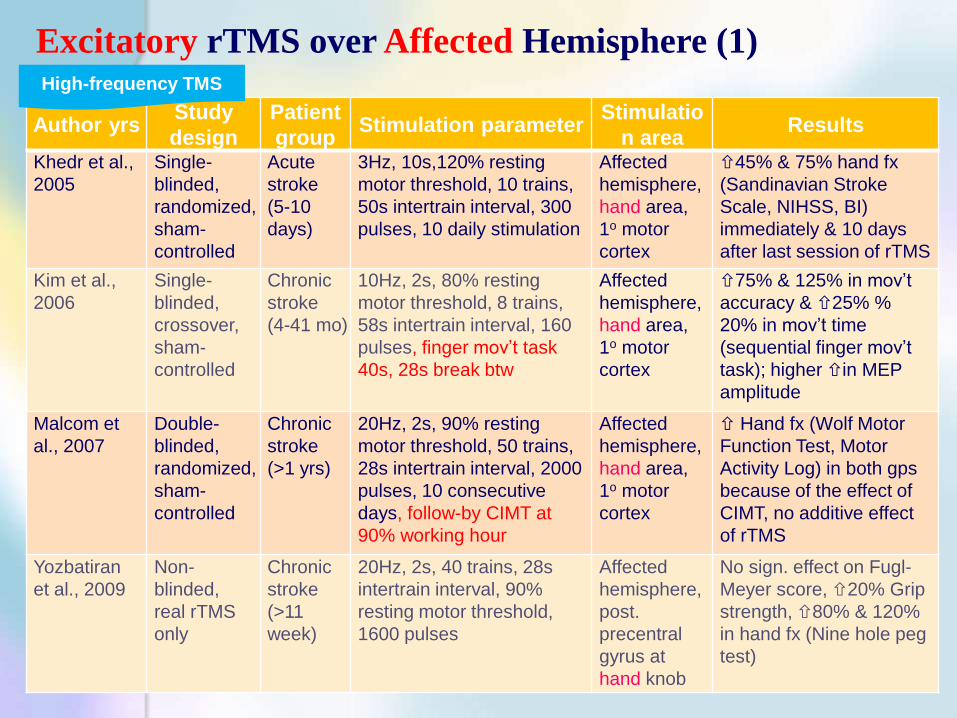
Khedr et al.,
2005
Single-
blinded,
randomized,
sham-
controlled
Acute
stroke
(5-10
days)
3Hz, 10s,120% resting
motor threshold, 10 trains,
50s intertrain interval, 300
pulses, 10 daily stimulation
Affected
hemisphere,
hand area,
1o motor
cortex
45% & 75% hand fx
(Sandinavian Stroke
Scale, NIHSS, BI)
immediately & 10 days
after last session of rTMS
Kim et al.,
2006
Single-
blinded,
crossover,
sham-
controlled
Chronic
stroke
(4-41 mo)
10Hz, 2s, 80% resting
motor threshold, 8 trains,
58s intertrain interval, 160
pulses, finger mov’t task
40s, 28s break btw
Affected
hemisphere,
hand area,
1o motor
cortex
75% & 125% in mov’t
accuracy & 25% %
20% in mov’t time
(sequential finger mov’t
task); higher in MEP
amplitude
Malcom et
al., 2007
Double-
blinded,
randomized,
sham-
controlled
Chronic
stroke
(>1 yrs)
20Hz, 2s, 90% resting
motor threshold, 50 trains,
28s intertrain interval, 2000
pulses, 10 consecutive
days, follow-by CIMT at
90% working hour
Affected
hemisphere,
hand area,
1o motor
cortex
Hand fx (Wolf Motor
Function Test, Motor
Activity Log) in both gps
because of the effect of
CIMT, no additive effect
of rTMS
Yozbatiran
et al., 2009
Non-
blinded,
real rTMS
only
Chronic
stroke
(>11
week)
20Hz, 2s, 40 trains, 28s
intertrain interval, 90%
resting motor threshold,
1600 pulses
Affected
hemisphere,
post.
precentral
gyrus at
hand knob
No sign. effect on Fugl-
Meyer score, 20% Grip
strength, 80% & 120%
in hand fx (Nine hole peg
test)
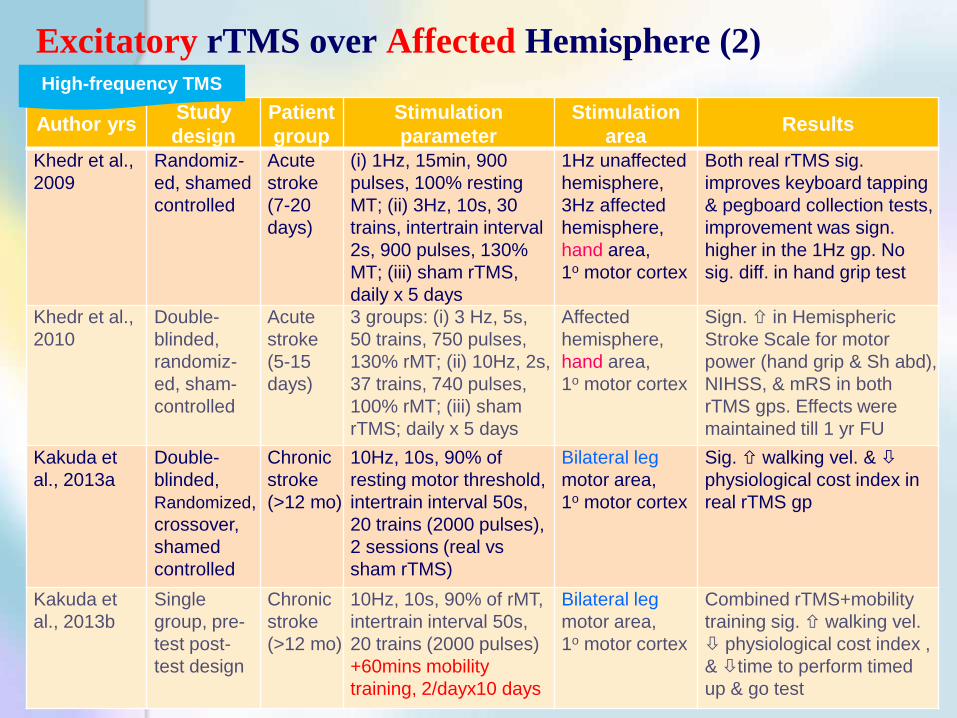
High-frequency TMS
Excitatory rTMS over Affected Hemisphere (1)
Author yrs Study
design
Patient
group
Stimulation
parameter
Stimulation
area Results
Khedr et al.,
2009
Randomiz-
ed, shamed
controlled
Acute
stroke
(7-20
days)
(i) 1Hz, 15min, 900
pulses, 100% resting
MT; (ii) 3Hz, 10s, 30
trains, intertrain interval
2s, 900 pulses, 130%
MT; (iii) sham rTMS,
daily x 5 days
1Hz unaffected
hemisphere,
3Hz affected
hemisphere,
hand area,
1o motor cortex
Both real rTMS sig.
improves keyboard tapping
& pegboard collection tests,
improvement was sign.
higher in the 1Hz gp. No
sig. diff. in hand grip test
Khedr et al.,
2010
Double-
blinded,
randomiz-
ed, sham-
controlled
Acute
stroke
(5-15
days)
3 groups: (i) 3 Hz, 5s,
50 trains, 750 pulses,
130% rMT; (ii) 10Hz, 2s,
37 trains, 740 pulses,
100% rMT; (iii) sham
rTMS; daily x 5 days
Affected
hemisphere,
hand area,
1o motor cortex
Sign. in Hemispheric
Stroke Scale for motor
power (hand grip & Sh abd),
NIHSS, & mRS in both
rTMS gps. Effects were
maintained till 1 yr FU
Kakuda et
al., 2013a
Double-
blinded,
Randomized,
crossover,
shamed
controlled
Chronic
stroke
(>12 mo)
10Hz, 10s, 90% of
resting motor threshold,
intertrain interval 50s,
20 trains (2000 pulses),
2 sessions (real vs
sham rTMS)
Bilateral leg
motor area,
1o motor cortex
Sig. walking vel. &
physiological cost index in
real rTMS gp
Kakuda et
al., 2013b
Single
group, pre-
test post-
test design
Chronic
stroke
(>12 mo)
10Hz, 10s, 90% of rMT,
intertrain interval 50s,
20 trains (2000 pulses)
+60mins mobility
training, 2/dayx10 days
Bilateral leg
motor area,
1o motor cortex
Combined rTMS+mobility
training sig. walking vel.
physiological cost index ,
& time to perform timed
up & go test
High-frequency TMS
Excitatory rTMS over Affected Hemisphere (2)

Other rTMS Protocol: TBS, Bi-hemisphere Stimulation
Author yrs Study
type
Patient
group
Stimulation
parameter
Stimulation
area Results
Talelli et al.,
2007
Single-
blinded,
randomized,
sham-
controlled
Chronic
stroke
(12-108
mo)
Each burst: 3 pulse at
50Hz given at 5Hz,
80% active motor
threshold, i) iTBS, 20
trains, 10 burst,8s inter-
train interval, 600
stimuli; (ii) cTBS, con’t
train of 100 bursts, 600
stimuli; (iii) sham TMS
iTBS on affect-
ed hemisphere;
cTBS unaffect-
ed hemisphere,
hand area,
1o motor cortex
Only iTBS sign. motor
behaviour & the
physiological measures of
the paretic hand. 90%
mov’t speed immediately &
last for 40mins, no
significant effect on peak
grip force
Takeuchi et
al., 2009
Double-
blinded,
crossover
Chronic
stroke
(>6 mo)
(i) 1Hz, 50s, 90%rMT,
20mins, 1000
pulses+sham; (ii) 10Hz,
5s, 20 trains, 1000
pulses+sham; (iii) Bil 1
& 10Hz
1Hz unaffected
hemisphere, 10
Hz affected
hemisphere,
hand area,
1o motor cortex
Bil rTMS & 1Hz rTMS
improves acceleration in the
paretic hand. 10Hz has no
effect on motor fx
Sung et al.,
2013 (consecutive
suppressive-
facilitatory
TMS protocol)
Single-
blinded,
randomized,
sham-
controlled
Chronic
stroke
(3-12
mo)
Bilateral stimulation
a) 1Hz (contra)+iTBS(ip)
b)sham(contra)+iTBS(ip)
c) 1Hz(contra)+sham(ip)
d) Bilateral sham
20 daily sessions
1Hz, 90%rMT,
10 mins (600
pulses); iTBS:
80%rMT, 3pulse
at 50Hz at 5Hz,
2s, 100 trains
(600 pulses)
Combined 1Hz+iTBS
showed greater muscle
strenght, Fugl-Meyer, Wolf
Motor Function test &
reaction time improvement
Other stimulation protocol

Benefits of rTMS in Stroke - Meta-analysis
• 18 selected articles, 392 patients
• positive effect on motor recovery (effect size of 0.55) in stroke,
• esp subcortical stroke (mean effect size, 0.73) showing neural activity in
unaffected hemisphere associated with motor recovery
• additional cortical stroke showed neural activity in the frontal & parietal
motor areas - might counteract the effect of rTMS
• good for all stages of stroke
• Post-stroke competition & imbalance could be remedied by reducing the
cortical excitability in the unaffected hemisphere using rTMS
• Low-frequency rTMS over the contra-lesional hemisphere more beneficial
than high-frequency rTMS over ipsilesional hemisphere
• No statistical evidence found for publication bias, heterogeneity

• Included 19 trials with 588 participants
• rTMS not associated with improved ADL nor sig. effect on motor function
• Current evidence is not yet sufficient to support the routine use of rTMS for the
treatment of stroke
rTMS in Stroke Management – Cochrane Review
• Sig. heterogeneity in
• time between stroke and recruitment (from 4 hours to 6 years)
• measurement time point (end of the treatment period or within one month)
• rTMS protocols (stimulation parameters of frequency, intensity, pulses)
• different motor function assessments
• Strict inclusion criteria limiting applicability
• Small sample size (10 to 123) affecting adequate power to detect a between-
groups difference
• Potential side effects e.g. seizure found to be rare or nil
Further trials with larger sample sizes are needed to determine a suitable rTMS protocol & the long-term functional outcome
Hao Z, Wang D, Zeng Y, Liu M. Repetitive transcranial magnetic stimulation for improving function after stroke.
Cochrane Database Syst Rev. 2013;5:CD008862. doi: 10.1002/14651858.CD008862

Local PT Experience in
KCC
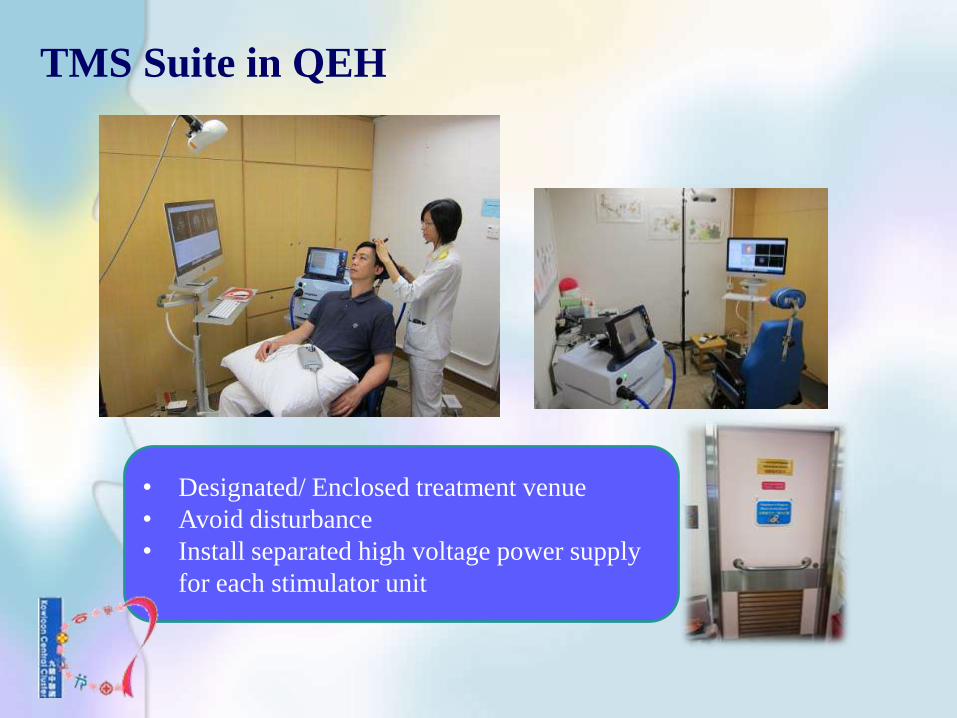
TMS Suite in QEH
• Designated/ Enclosed treatment venue
• Avoid disturbance
• Install separated high voltage power supply
for each stimulator unit

Focused Target Clientele Target Clientele
•Stroke
•Upper limb with motor control (power ≥2-)
•No history of cancer or unstable medical condition
Exclusion Criteria
• Substantial cognitive impairment with Mini Mental State Test <24
• Diagnosis of mental illness
• Pathological conditions referred to as contra-indications for rTMS in
guideline suggested by Wassermann (eg. Cardiac pacemaker, intracranial
implants, implanted medication pumps, epilepsy)
• Unstable cardio-pulmonary conditions

Repetitive Transcranial Magnetic Stimulation (rTMS)
Conventional rTMS
• Application of regularly repeated single TMS pulses
High frequency: > 1Hz (for facilitation)
Low frequency: <1Hz (for inhibition)
Patterned rTMS
• Repetitive application of short rTMS bursts at a high inner frequency
interleaved by short pauses of no stimulation e.g. Theta burst
stimulation
cTBS : for inhibition
iTBS : for facilitation

Stimulation Protocols • For excitatory rTMS over affected hemisphere
Strong intensity, numerous numbers, and long duration are most effective for motor
recovery
• For inhibitory rTMS over unaffected hemisphere
Subthreshold stimulation on unaffected hemisphere (e.g. 90% rMT)
excitability of stimulated motor cortex
facilitation effect on the contralateral motor cortex
Suprathreshold stimulation on unaffected hemisphere (e.g. 120% rMT)
excitability of stimulated motor cortex
excitability of the opposite homogenous motor cortex via activation of
interhemispheric inhibition
cancel out the facilitation effect on contralateral motor cortex
No consensus on the optimal stimulation protocol
rTMS Protocol in KCC
Inhibitory Low-frequency rTMS over contra-lesional site
1Hz x 1500 pulse at 90% rMT x 10 sessions
+ PT upper limb training program
*Safe and can be achieved same benefits with ease in locating hot spot

Safety Assurance in TMS
Hao Z, Wang D, Zeng Y, Liu M. Repetitive transcranial magnetic stimulation for improving function after stroke.
Cochrane Database Syst Rev. 2013;5:CD008862. doi: 10.1002/14651858.CD008862

Staff Credentialing Criteria in KCC
• PT with at least 5 years post-graduate
experiences in the relevant field(s)
• Successful completion of structured training
including theory & practicum of at least 40
hours by recognized training institute
• Attainment of at least a pass in formal
examination
* Audit on compliance to intervention protocol & safety measures
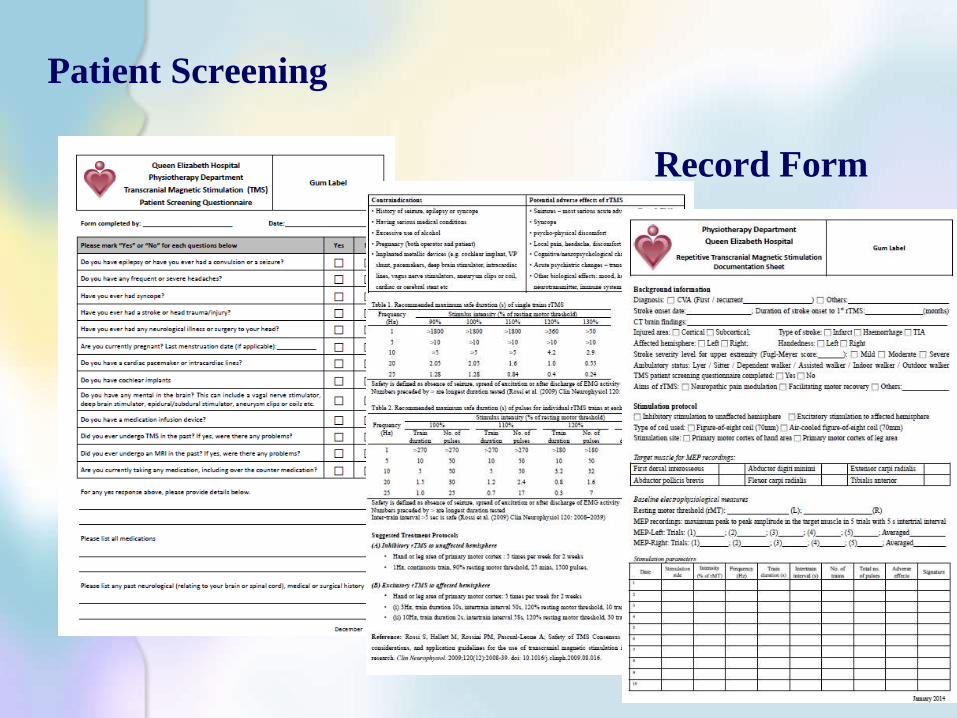
Patient Screening
Record Form

Safety Assurance
• Side effect
• Control measures
• Patient screening • Hearing
protection
Hearing
• Emergency stand-by
Seizure • Vital sign
Monitoring
Headache

PT Upper Limb Rehabilitation Program
Acupuncture
Functional Electrical
Stimulation Manual Therapy
Robotic Therapy Transcranial Magnetic Stimulation
Virtual Reality

Pilot Study
Type of stroke Ischaemic Stroke
Duration of stroke
Subacute: 2 week post-stroke onset (average 8.5 weeks)
Chronic: 8 with average of 84.66 weeks
Age 60.33
Outcome Measures Chronic
(n=8)
Subacute
(n=2)
Fugl- Meyer Score +3.3% +6.5%
Box and Block Test +22% +30.5%
Tap Test +17.5% +25%
Action Research Arm Test +10.2% +26.4 Action Research Arm Test
Box & Block Test
Overall demonstrating positive results after the rTMS+ UL rehab
No adverse effects reported
Preparation:
• Consolidate skill
• Formulate guideline/ protocol
• Establish reliability of outcome measures
10 patients completed the pilot program

Summary
rTMS is a safe intervention • Stringent staff credentialing system
• Proper patient screening
• Appropriate control measures
implementation
• Continuous evaluation/ audit
rTMS can be an effective
adjunct PT intervention in
rehabilitation
rTMS
• Positive effect on motor recovery esp. in
upper limb
• For each stage of stroke – acute, subacute and
chronic
• Subcortical stroke benefits more
• Post-stimulated effect lasting for 1- 2 hours
• Benefits are more sustainable when followed
by post-stimulation training
Effective

Thank You!





























