-
20S JADA, Vol. 141 http://jada.ada.org June 2010
Dental computer-aided design/computer-aidedmanufacturing
(CAD/CAM) technology isused in both dental laboratories and
dentaloffices for multiple restorative applications.Chairside
CAD/CAM systems for dental
offices offer dentists the opportunity to design, mill andplace
ceramic restorations in a single appointment. Asimplants become the
treatment of choice for fixed toothreplacement, dentists also are
considering using chair-side CAD/CAM systems as a restorative
solution forimplant prosthetics. A predictable CAD/CAM techniquefor
dental implantology could satisfy patients’ prefer-ence for
convenience and dentists’ desire for predictable,long-term
restorations. Clinical research provides docu-mentation of the
success of ceramic restorations createdusing the CEREC system
(Sirona Dental Systems,Charlotte, N.C.).1-4 As the technology has
evolved, it alsohas been used to restore dental implants.5,6
CAD/CAM TECHNOLOGY FOR DENTAL IMPLANTS
Initial attempts to fabricate implant restorations chair-side
with the CEREC system included the use of felds-pathic and
leucite-reinforced ceramic CAD/CAM blocks.These ceramics require
adhesive bonding to be successfulin restoring natural teeth.
Adhesive bonding to implantabutments remains unpredictable and
reduces the relia-bility of conventional all-ceramic materials.
Reports ofincreasing the occlusal thickness of the
restorationbeyond the 1.5 millimeters recommended for conven-tional
tooth preparations does not offset the fracture riskof adhesive
glass ceramic CAD/CAM blocks used onimplant abutments.6,7 The
results of the study by Wolfand colleagues6 suggest that increasing
the thickness ofthe crown to an unusual 5.5 mm in combination
withshortening the abutment does not result in greatercrown
strength. To date, there have been no publishedclinical studies in
which this type of ceramic materialwas used to restore dental
implants. Despite this lack ofpublished data, the introduction of a
lithium disilicateglass ceramic with 360 megapascals of biaxial
flexuralstrength (IPS e.max CAD, Ivoclar Vivadent, Amherst,N.Y.)
provides dentists with the option to use eithercementation or an
adhesive bonding protocol. Thismaterial has the potential to be
used for definitiveimplant restorations. The higher flexural
strength of the
Dr. Patel maintains a private practice in general dentistry,
Powell, Ohio.Address reprint requests to Dr. Patel at Infinite
Smiles, 7500 SawmillParkway, Powell, Ohio 43065, e-mail
“[email protected]”.
Integrating three-dimensional digital technologies for
comprehensiveimplant dentistryNeal Patel, DDS
Background. The increase in the popularity ofand the demand for
the use of dental implants toreplace teeth has encouraged
advancement in clin-ical technology and materials to improve
patients’acceptance and clinical outcomes. Recent advancessuch as
three-dimensional dental radiographywith cone-beam computed
tomography (CBCT),precision dental implant planning software
andclinical execution with guided surgery all play arole in the
success of implant dentistry.Methods. The author illustrates the
technique ofcomprehensive implant dentistry planning
throughintegration of computer-aided design/computer-aided
manufacturing (CAD/CAM) and CBCT data.The technique includes
clinical treatment withguided surgery, including the creation of a
final res-toration with a high-strength ceramic (IPS e.maxCAD,
Ivoclar Vivadent, Amherst, N.Y.). The authoralso introduces a
technique involving CAD/CAM forfabricating custom implant
abutments.Results. The release of software integratingCEREC
Acquisition Center with Bluecam (SironaDental Systems, Charlotte,
N.C.) chairsideCAD/CAM and Galileos CBCT imaging (SironaDental
Systems) allows dentists to plan implantplacement, perform implant
dentistry withincreased precision and provide predictable
restora-tive results by using chairside IPS e.max CAD.Conclusions.
The precision of clinical treat-ment provided by the integration of
CAD/CAM andCBCT allows dentists to plan for ideal surgicalplacement
and the appropriate thickness ofrestorative modalities before
placing implants.Key Words. CAD/CAM; cone-beam computedtomography;
implants; restorative dentistry; fixedprosthetics; guided implant
surgery.JADA 2010;141(6 suppl):20S-24S.
A B S T R A C T
Copyright © 2010 American Dental Association. All rights
reserved. Reprinted by permission.
-
JADA, Vol. 141 http://jada.ada.org June 2010 21S
material reduces the risk of fractureunder normal masticatory
load com-pared with that of conventional glassceramic CAD
blocks.7-9 The results ofthe study by Wolf and colleagues6 sug-gest
that the interaction between abut-ment material and mode of
cementa-tion plays an important role in theviability of
conventional glass ceramicCAD/CAM materials. They noted thatthe use
of adhesive resin cementincreased the overall fracture load
ofconventional CAD/CAM ceramic resto-rations compared with that of
nonad-hesive cements. With the recent avail-ability of a
high-strength ceramicmaterial, a more favorable outcome
forimplant-supported restorations mayoccur.
INTEGRATION OF CONE-BEAMCOMPUTED TOMOGRAPHY AND CAD/CAM
The primary emphasis in a surgery-focusedapproach to implant
placement is on the anatomy,bone physiology and surgical success.
The restora-tive demands of the case may be secondary
whendetermining the placement of the implant fixture.During the
restorative phase, compensation fordeviations in implant fixture
location involves theuse of complex custom prosthetics components.
Atechnique that requires custom prostheticsdesigned after surgical
placement of the endosseousdental implant does not allow for the
implant to berestored in a single visit because of the
requiredlaboratory fabrication process.
Dentists need to consider the restorative goal andsurgical
requirements to plan optimally for the sur-gical placement of
implants. This process requires aplan for the final restoration’s
optimal function,esthetics and biomechanics before making the
sur-gical plan. The traditional technique for such plan-ning begins
with using diagnostic casts, impressionsand clinical records. Using
the diagnostic casts, thedentist or laboratory technician produces
a wax-upto simulate the desired restorative outcome. A
stoneduplication of the wax-up is necessary for processingeither a
laboratory surgical guide to help with tradi-tional implant
placement or a radiographic scanningappliance for subsequent
diagnostic implant plan-ning. This work flow involves multiple
patientappointments and separate laboratory proceduresinvolving the
clinician and the laboratory technician
before the implant can be placed. Because of pro -cedural
complexity, the clinician may favor a surgi-cally focused technique
for implant placement andtreat the restorative process as
secondary.
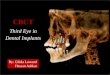
Sirona Dental Systems introduced a combinationof
three-dimensional (3-D) radiographic imagingand 3-D planning by
integrating CEREC Acquisi-tion Center (AC) design with Galileos
(SironaDental Systems) cone-beam computed tomographic(CBCT) imaging
to facilitate comprehensive implanttreatment. Galileos CEREC
integration (GCI) sim-plifies restorative-focused implant
placementsthrough the use of intraoral surface data (the
digitalimpression) and radiographic data (Figure 1). TheGCI
technique gives dentists the opportunity to planoptimum prosthetic
and surgical outcomes forimplants during the diagnostic and
planning phasesof treatment while minimizing the number of
pro-cedures and increasing work-flow efficiency.
By using GCI software, the clinician can identifythe restorative
requirements virtually, includingproper restorative material
thickness around thelong axis of the planned implant, depth of
restora-tive interface and emergence profile. Such infor-mation may
help the dentist decide whether to use
ABBREVIATION KEY. AC: Acquisition Center.CAD/CAM: Computer-aided
design/computer-aidedmanufacturing. CBCT: Cone-beam computed
tomog-raphy/tomographic. GCI: Galileos CEREC integration.3-D:
Three-dimensional.
Figure 1. Sidexis and Galileos implant software (Sirona Dental
Systems, Charlotte,N.C.) provides tools such as nerve mapping and
implant planning. Galileos CEREC(Sirona Dental Systems) integration
allows for computer-aided design/computer-aided manufacturing data
to be imported into software to create virtual prosthetics,giving
dentists the opportunity to plan comprehensive restorative
treatment in asingle visit. Image of Galileos Sidexis software
reproduced with permission of SironaDental Systems, Charlotte,
N.C.
Copyright © 2010 American Dental Association. All rights
reserved. Reprinted by permission.
-
22S JADA, Vol. 141 http://jada.ada.org June 2010
stock abutments or custom anatomic abutments.Until now, the
convenience of chairside CAD/CAMfor implant restoration was limited
by materialstrength. The ability to plan implant placementwith
restorative vision by using the GCI softwarecombined with a
restorative material whose proper-ties are an improvement over
those of conventionalglass ceramics provides the dentist with a
viablecomprehensive protocol for implant placement andchairside
CAD/CAM all-ceramic restorative success.
CLINICAL WORK FLOWS
There are a number of possible work flows thatcan be followed
when using the GCI technique.
Single-implant workflow. For a single-implant site, the clinical
work flow begins withobtaining a digital impression by using
CERECAC and Galileos CBCT during the initial consul-tation. Instead
of using conventional impressionsand diagnostic wax-ups, the
dentist can use thedigital impression to record the surface
anatomyand design an ideal restoration virtually. The dig-ital
impression is obtained by coating the toothand gingival surfaces
lightly with an opticalreflective medium to create a uniform
surface andby using the CEREC AC Bluecam to acquireimage data.
Obtaining the digital impressionincludes capturing both the
edentulous quadrantand the opposing quadrant in separate image
cat-alogs. The virtual models created from the digitalimpression
are articulated by using an additionalimage recorded when the
patient is in maximumintercuspation (buccal bite technique). The
den-tist or technician uses CEREC Biogeneric soft-ware (Version
3.80, Sirona Dental Systems) tocreate virtual wax-ups of planned
restorationsthat include parameters such as occlusal contacts,
proximal contacts, emergence profile, proximalcontours and the
desired material thickness foroptimal strength of the ceramic
restoration. Inaddition to the optical impression, a GalileosCBCT
scan of the patient is obtained by means ofa stock scanning bite
plate (SICAT, Bonn, Ger-many). The bite plate is seated clinically
by usingthe bite registration material. The bite plate isconverted
to the surgical guide at a later stage.The Galileos CBCT scans
provide a 3-D volumeimage of the hard tissue that can be evaluated
byusing software to evaluate radiographic sectionsof the anatomy
that correlate one-to-one withoutdistortion or magnification.
The CAD/CAM and CBCT systems provide com-prehensive diagnostic
data. The acquisition of sur-face anatomy and radiographic anatomy
dataallows the dentist to design and plan treatment andorder
precision surgical guides for guided implantplacement in one visit.
The process requires thedentist to combine the data sets from the
two sys-tems by using GCI integration software that
usessophisticated algorithms to match common datapoints. The
dentist need only identify common fea-tures between the two digital
images (for example,placing an identification marker on tooth no. 2
inthe CEREC AC image and on tooth no. 2 in theGalileos image) to
allow the software to correlatethe data. Once combined, the CEREC
AC data arevisible within the Galileos software, allowing
thedentist to plan the implant position as it relates toboth the
prosthetic and surgical requirements ofthe case (Figure 1). Within
the software, a library ofimplant systems from which to plan
implant posi-tioning relative to restorative and surgical goals
isavailable. Once the dentist determines the type ofimplant and
surgical positioning, he or she canorder the surgical guide. The
patient’s data set andscanning template are sent to SICAT for
fabricationof the implant surgical guide.
The dentist can order the surgical guide withmultiple options,
including a guided pilot systemfor guided pilot osteotomy,
sleeve-in-sleeve systemsfor complete guided final osteotomy or a
mastersleeve for guided implant placement. The surgicalguides are
compatible with most of the availableimplant systems. This work
flow allows for guidedsurgical implantation during the patient’s
secondvisit. Implant placement accuracy when using theSICAT
surgical guides is within 500 micrometers ofplanned implant
placement location.10 The SICATsurgical guide system’s inherent
mean deviationrates for drilled pilot osteotomies are less than
Figure 2. Clinical photo with seated custom zirconia implant
abut-ments for teeth nos. 12 through 14 and teeth nos. 18 through
20.
Copyright © 2010 American Dental Association. All rights
reserved. Reprinted by permission.
-
JADA, Vol. 141 http://jada.ada.org June 2010 23S
500 μm even at the apical end and within 1.18˚angular deviation,
and their crestal deviations aresignificantly lower than those of
apical deviations.10
Once osseointegration is complete, the restora-tive phase of
treatment can begin, and the dentistcan use the data from CEREC AC
and Galileos thatwere used during the planning phase to
understandthe restorative options in advance. The dentist canseat a
stock or standard abutment clinically andscan it intraorally with
CEREC AC to fabricate afull-contour restoration similar to a
preparation fora crown on a natural tooth (Figure 2).
Because of the nature of stock abutments, thedentist may need to
modify margin placement,reduce axial dimensions, add antirotational
facetsand produce a proper tissue emergence profile byusing
high-speed rotary instrumentation withcopious water irrigation to
reduce heat production.To reduce the risk of heat transfer and
implantdamage, modification of prosthetic componentsextraorally may
be indicated. After the dentistseats the abutment clinically, he or
she can fill thescrew access hole with a retrievable material to
pro-tect the screw for future access. Tissue retraction isnecessary
to visualize the abutment margin. Thedentist can retract the
gingivae by using conven-tional means such as a retraction cord,
retractiongels and pastes, and laser treatment. Once the den-tist
has isolated the abutment, he or she follows theconventional
chairside optical impression protocolby using CEREC AC Bluecam.
Within the CERECAC software, the dentist can evaluate and
confirmthe abutment’s restorative margin, interproximalcontacts,
occlusal contacts, emergence profile andsoft-tissue support.
Essentially, the dentist candesign a final crown by using the CEREC
AC soft-
ware and customize it to fit the restorative environ-ment
chairside (Figure 3). The dentist selects IPSe.max CAD and sends
the data to the inLab MC XL(Sirona Dental Systems) milling chamber
for chair-side computer-aided manufacturing of the crown.
After the dentist retrieves the restoration fromthe milling
chamber, he or she can evaluate the res-toration clinically and
adjust it if necessary while itis in the precrystallized state
(Figure 4). The den-tist can introduce custom staining and
glazingbefore the restoration is crystallized to final
lithiumdisilicate transformation for optimal strength andesthetics
(Figures 4 and 5). He or she can use adhesive (which requires that
zirconia abutmentsbe pretreated with 10-methacryloyloxydecyl
dihydrogen phosphate monomers) or conventionalcementation options.
The dentist should removeresidual cement carefully after
cementation anduse radiographic confirmation of abutment seatingand
cement removal.
Custom abutment and crown work flow.Another work flow relies on
the dentist’s sendingthe CEREC AC digital impression data to a
dentallaboratory by using the CEREC Connect software(Sirona Dental
Systems) via the CEREC inLab(Sirona Dental Systems) system to
fabricate acustom abutment and crown. This abutment tech-nique may
include having the dentist obtain eithera traditional fixture level
impression used to fabri-cate a master implant model or a digital
intraoralimpression of a clinically seated scan body on theimplant.
(A scan body is a plastic coping withmarkers that provide 3-D
registration of the implantlocation.) Both techniques give dentists
control overmore complex and esthetic cases when they arerestoring
multiple implants. Either intraorally or
Figure 3. CEREC Biogeneric software (Version 3.80,Sirona Dental
Systems, Charlotte, N.C.) showing thedesign process for chairside
fabrication of customimplant crowns. The image shows intraoral scan
ofseated abutments for teeth nos. 18 through 20. Thecrown design
for tooth no. 18 is completed and virtu-ally seated. The crown for
tooth no. 19 is designed forproper emergence profile, contacts and
occlusion.Image of CEREC software reproduced with permissionof
Sirona Dental Systems, Charlotte, N.C.
Figure 4. Photo showing IPS e.max CAD(Ivoclar Vivadent, Amherst,
N.Y.) block withprecrystallized chairside milled implantcrown no.
19 and the final crown after crys-tallization with custom staining
and glazing.Image of IPS e.max CAD LT reproduced withpermission of
Ivoclar Vivadent, Amherst, N.Y.
Figure 5. Clinical photo with seated IPSe.max CAD (Ivoclar
Vivadent, Amherst,N.Y.) implant crowns nos. 12 through 14and crowns
nos. 18 through 20.
Copyright © 2010 American Dental Association. All rights
reserved. Reprinted by permission.
-
24S JADA, Vol. 141 http://jada.ada.org June 2010
on a master implant model, the dentist seats theappropriate
titanium base on the implant. Then heor she introduces a scan body
that allows for digitalscanning with CEREC inLab for working
models(Figure 6) or CEREC AC for intraoral scanning. Forintraoral
scanning, the dentist can forward the scan
data to technicians who use CEREC inLab for thedesign and
milling of custom implant abutments.Using the CEREC inLab software,
the technicianhas the ability to design the ideal restoration
virtu-ally, perform a digital cutback technique or design
afull-contour abutment that mimics conventionaltooth-borne
preparations for fixed prosthodontics.Once the abutment design is
complete, the techni-cian mills the zirconia restorative component
withan inCoris ZI (Sirona Dental Systems) meso block,which is
available in multiple shades, and sinters itfor final
crystallization. The technician lutes the zir-conia meso structure
to the titanium base to formthe custom abutment. Then the CEREC
inLabsystem can mill the corresponding restoration, orthe dentist
can seat the custom abutment for chair-side CAD/CAM restoration
(Figure 6).
CONCLUSION
The integration of chairside CAD/CAM softwareand CBCT provides
dentists with a combineddata set they can use for implant planning.
Thismethod may allow dentists more flexibility fordelivering
implant prosthetics—both milledcustom abutments and milled
crowns—chairside.The digital work flow for implant dentistry
andchairside CAD/CAM offers new approaches to theway dentists can
practice implant dentistry. ■
Disclosure. Dr. Patel has served as a consultant to and
providesclinical education courses in Galileos cone-beam computed
tomographyand CEREC Acquisition Center computer-aided
design/computer-aidedmanufacturing technology for Sirona Dental
Systems, Charlotte, N.C.
1. Fasbinder DJ. Clinical performance of chairside CAD/CAM
resto-rations. JADA 2006;137(9 suppl):22S-31S.
2. Giordano R. Materials for chairside CAD/CAM-produced
restora-tions. JADA 2006;137(9 suppl):14S-21S.
3. Wittneben JG, Wright RF, Weber HP, Gallucci GO. A
systematicreview of the clinical performance of CAD/CAM
single-tooth restora-tions. Int J Prosthodont
2009;22(5):466-471.
4. Kelly JR. Machinable ceramics. In: Mörmann WH, ed. State of
theArt of CAD/CAM Restorations: 20 Years of CEREC. Hanover Park,
Ill.:Quintessence; 2006:29-38.
5. Griffin JD Jr. Quadrant rehabilitation with implants and
CAD/CAMcrowns. Dent Today 2008;27(9):122, 124, 126 passim.
6. Wolf D, Bindl A, Schmidlin PR, Lüthy H, Mörmann WH.
Strengthof CAD/CAM-generated esthetic ceramic molar implant crowns.
Int JOral Maxillofac Implants 2008;23(4):609-617.
7. Bindl A, Lüthy H, Mörmann WH. Strength and fracture pattern
ofmonolithic CAD/CAM-generated posterior crowns. Dent Mater
2006;22(1):29-36.
8. Waltimo A, Könönen M. A novel bite force recorder and
maximalisometric bite force values for healthy young adults. Scand
J Dent Res1993;101(3):171-175.
9. Waltimo A, Kemppainen P, Könönen M. Maximal contraction
forceand endurance of human jaw-closing muscles in isometric
clenching.Scand J Dent Res 1993;101(6):416-421.
10. Dreiseidler T, Neugebauer J, Ritter L, et al. Accuracy of a
newlydeveloped integrated system for dental implant planning. Clin
OralImplants Res 2009;20(11):1191-1199.
Figure 6. Laboratory process for CEREC inLab abutments
(SironaDental Systems, Charlotte, N.C.). A. A seated scan body over
a tita-nium base on a fixture level implant master model. CEREC
inLabsoftware (Sirona Dental Systems) allows for complete
customizationof an inCoris ZI (Sirona Dental Systems) meso
structure for full-contour abutment design to mimic conventional
fixed prostho-dontic tooth preparation with cutback technique in
CEREC inLabsoftware. B. Seated custom CEREC inLab implant abutment.
C. Finalcrown seated on CEREC inLab abutment.
Copyright © 2010 American Dental Association. All rights
reserved. Reprinted by permission.
Integrating three-dimensional digital technologies for
comprehensive implant dentistryCAD/CAM TECHNOLOGY FOR DENTAL
IMPLANTSINTEGRATION OF CONE-BEAM COMPUTED TOMOGRAPHY AND
CAD/CAMCLINICAL WORK FLOWSCONCLUSION