Embed Size (px)
Citation preview

Integrating Substance Use Treatment into Primary Care:
You can do it!
Aaron Fox, MD, MS, Assistant Professor of MedicineAlbert Einstein College of Medicine/Montefiore Medical Center; Attending Physician, Comprehensive Health Care Center
Beth Hribar, MPP, Program Director
Institute of Advanced Medicine of the Mount Sinai Health System
Martha A. Sparks, PhD, Associate Director Mental Health Services, Spencer Cox Center for Health, Institute of Advanced Medicine of the Mount Sinai Health System
Collaborative Family Healthcare Association 17th Annual ConferenceOctober 15-17, 2015 Portland, Oregon U.S.A.
Session # C6b, Period 6October 17, 2015

Faculty Disclosure
The presenters of this session• have NOT had any relevant financial
relationships during the past 12 months.

Learning ObjectivesAt the conclusion of this session, the participant will be able
to:
1. Identify at least one reason primary care settings provide an ideal location for implementing substance use treatment
2. Understand the regulatory and credentialing requirements for providing both medical and psychosocial interventions in substance use treatment.
3. Understand at least one common barrier to retention for individuals with substance use issues, and will identify a harm-reduction principle or intervention to support patient reengagement.
4. Identify at least one successful intervention that can be implemented in a primary care setting of a standard clinic.

Select References
Bernstein, J. et. Al. (2015). Recreational drug use among primary care patients: Implications of a positive self-report. Annals of Family Medicine, 13(3).
Buck, J. A. (2011). The looming expansion and transformation of public substance abuse treatment under the Affordable Care Act. Health Affairs, 30(8).
Institute for Clinical Systems Improvement. (2013). Patients with risky substance use in primary care settings. Retrieved from: https://www.icsi.org/_asset/s769qd/RSU-prevalent-in-PC---FINAL.pdf
United States Department of Health and Human Services. (2015). Essential health benefits. Retrieved from https://www.healthcare.gov/glossary/essential-health-benefits/
United States Department of Health and Human Services. (2014). Results from the 2013 national survey on drug use and health: Summary of national findings. Retrieved from http://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.htm#7.2

Learning Assessment
• A learning assessment is required for CE credit.
• A question and answer period will be conducted at the end of this presentation.

Outline
1. Introduction
2. Integrated care: A primary care physician’s perspective
3. Integrated care: A behavioral specialist’s perspective
4. Integrated care: Policy and regulatory issues
5. Practical recommendations

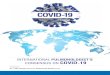
Substance use is common among primary care patients
Hypertensio
n
Hyperlipidemia
Unhealthy alco
hol use
Depression
Gastroso
phageal Reflux
Diabetes
Obesity
Asthma
Illegal d
rug use
36% 35%
20% 20%
16%13%
10%8%
6%

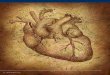
There is a large treatment gap
• Total number of individuals in need of treatment: 22.7 million
Location of substance use treatment(2.5 million unique individuals)
Prison or Jail
Emergency Room
Primary Care
Hospital Inpatient
Inpatient Rehabilitation
Outpatient MH Center
Outpatient Rehabilitation
Self-Help Group
263,000
603,000
770,000
879,000
1,042,000
1,176,000
1,753,000
2,292,000

Our perspective
• Substance use disorders are chronic relapsing conditions• Neurobiological disease with genetic, psychosocial, environmental
contributions
• Responsibility to meet patient needs
• Patient centered care
• Medications are underutilized
• Harm reduction vs. traditional model of care

Implementing substance use treatment into primary care:
The medical provider perspective

Primary care: an ideal setting for substance use treatment
• PCPs have experience in longitudinal care for chronic conditions
• Address risky/problem behavior early
• Reduce stigma
• Reduce barriers to care
• Possibly, improved outcomes (vs. specialty settings)

Treatment services delivered in primary care
• Screening and brief intervention
• Medication assisted treatment
• Relapse prevention strategies
• Harm reduction counseling

Case example: Montefiore Medical Center

Group Buprenorphine Treatment
• Team members: MD and MSW
• Patient selection: need for more intensive counseling
• Timing: 90 minutes, twice monthly
• Group Activities: self-disclosure, feedback, trauma-informed
group therapy (Seeking Safety), psycho-education, guided
relaxation, pizza
• Lessons Learned: confidentiality, voluntary, logistic support

Implementing substance use treatment into primary care:
The Behavioral Health Perspective

Benefits of behavioral health in primary care
• Coordinated care team
• Shared EMR
• Case conferences
• Reduced stigma

Treatment services provided in behavioral health in primary care
• Individual therapy
• Group therapy
• Case management
• Patient navigation
• Treatment for comorbidities
• Psychopharmacology
• EMR
• Case Conference

Case example: Morningside Clinic

Integrating substance use treatment into primary care:
Administration, regulation, and policy

Administrative and regulatory considerations
• Credentialing for treatment providers (CASAC v. Masters-level and higher clinicians)
• Buprenorphine training and panel size
• Licensing requirements from state offices of substance use services
• Clinician discomfort with and stigma surrounding patients with SUDs
• Effective screening and referral to care

The Affordable Care Act
• Substance use treatment is an “essential health benefit”
• Mental health care also an “essential health benefit”o Substance use interventions in the context of therapy can
be billed under behavioral health and not SAMHSA
• Referrals to residential treatment limited by Medicaid lawo No reimbursement for programs with more than 16 beds
• Insurance companies often limit the number of days in treatment, or require re-authorization (though not more restrictive than medical or surgical benefits)

Practical Recommendations
1. Implement routine screening using the EMR
2. Educate providers about medication assisted treatments
- identify a site champion
3. Retention in care IS an important goal
4. Mental health problems and substance use can be treated
concomitantly
5. With your training and expertise, you can do it!

Acknowledgements
• Mariel Gallego, Teresa Hurst, Hannah Wolfe, Emily Gertz, and the entire team at the Morningside Clinic
• Maritza Casillas, Angela Giovanniello, and our patients at the Comprehensive Health Care Center
• Dr. Fox is supported by K23 DA034541

PRIMECare
1. Ask – screen for alcohol use
2. Assess – relapse risk (PRECURSORS)
3. Advise – brief counseling
4. Assist – pharmacotherapy or strategy to manage high-risk
situations
5. Arrange – regular appointment
Friedmann JGIM 2006