Embed Size (px)
Citation preview

Copyrig
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
Integrating mental health care intoprimary care: the case of one ruraldistrict in Rwanda
Stephanie L. Smith,Yvonne Kayiteshonga, Claire N. Misago,Jean Damascene Iyamuremye, Jeanne d’Arc Dusabeyezu,AchourA. Mohand, Robyn A. Osrow, Manzi Anatole, Shin Daimyo,Eugenie Uwimana, Dominique Dushimiyimana&GiuseppeJ. Raviola
Key implications for practice� Describes a model to integrate men-
tal health care into primary care,embedded within an existing publicsector,healthcare strengtheningpro-gramme that emphasises generalistnurse supervision and health systemquality improvementmethods
� Highlights how mental health careandclinical supervisionwithinagov-ernmenthealthsystemwassupportedbyan international health care deliv-ery organisation, rather than devel-oping aparallel systemof care
� Provides examples of challenges andsolutionsto initial systemandhumanresource barriers to mental healthintegration into primary care inresource-limited settings
Integration ofmental health care into primary care is
a strategic priority of Rwanda’s national mental
health care programme and a central tenet of global
mental health. In 2009, the international health care
delivery organisation, Partners In Health, estab-
lished a community based mental health programme
to support national planning goals. In 2012, the
organisation collaborated with the RwandaMinis-
try of Health to implement a structured mentorship
programme enabling government employed, primary
care nurses to care for patients with severe mental
disorders at primary care health care centres in one
rural district.The implementation strategy included
decentralised training and consistent supervision
for four priority neuropsychiatric disorders. Lessons
learned were applied through the transition of super-
visory responsibilities to district hospital based
government nurses.The programme’s focus on struc-
tured mentorship for generalist nurses, systems based
improvements and use of an existing public health
care strengthening e¡orts highlight its potential as
a model for integrating mental health care into
primary care in resource limited settings.
Keywords: collaborative care, mentalhealth, nurse training, primary care integra-tion, quality improvement, Rwanda, tasksharing
IntroductionBackgroundNeuropsychiatric disorders account forabout one quarter of the global burden of dis-ability, yet rarely receive priority among
ht © War Trauma Foundation. Unautho136
the many health conditions competing forpoliticalwill andallocation of funds. Inmostlow income countries, due to the extremeshortage of mental health specialists andother factors (Kakuma et al., 2011), 90% ofpeople living with a severe mental disorderdo not have access to mental health services(Lancet Global Mental Health Group,2007).This is in spite of evidence for the e⁄-cacy of both psychosocial and pharmaco-logical interventions for treating mental
rized reproduction of this article is prohibited.

Copyrig
Smith et al.
disorders (World Health Organization(WHO), 2011a; 2011b). Innovative solutionsthat integrate mental health care intoprimary care settings, and that optimisehealth worker interventions through tasksharing, could contribute to alleviating theburden of neuropsychiatric disorders inlow income settings (Patel et al., 2007; Patelet al., 2013; Bass et al., 2012; Collins, Insel,Chockalingam, Daar, & Maddox, 2013;WHO, 2008a).Despite the potential for the integration ofmental health care into primary care toreduce the global burden of mental dis-orders, many challenges to implementa-tion of integrated mental health care in ‘realworld’, resource limited settings exist. Inthese settings, primary care is often deliv-ered by nonspecialist providers, such asnurses with little formal training in mentalhealth care, and training models acrossclinical domains often consist of short, cen-tralisedtrainingswithout follow-upsupervi-sion and support for patient care (Rowe,de Savigny, Lanata, & Victora, 2005). Inaddition, supervisory capacity for mentalhealth care provision in resource limitedsettings is challenging, asmental healthcarespecialists are frequently overburdenedclinicians with little supervisory experienceor training in public health and clinicalinterventions. In addition, budgeting andinfrastructure for building and maintain-ing regular clinical supervisory supportwithin public primary care settings isusually nonexistent.One potential solution to these challenges isto use the management and supervisoryinfrastructure of other existing, successfultask shared endeavours already embeddedwithin health systems as a starting point tointegrate mental health care into primarycare. Partners In Health (PIH), a nonpro¢torganisation working in ten countries, hasbeen working to support the public healthdelivery system in three rural districts ofRwanda since 2005. Here, the integrationof mental health care into a platform
ht © War Trauma Foundation. Unautho
developed to strengthen general primaryhealth care in one rural district in Rwandais discussed.
Setting: Rwandan contextThe Republic of Rwanda has the highestpopulation density in continental Africa,with apopulationof almost12millionpeoplecovering an area of about 26,338 squarekilometres. Beginning in the late 1950s, withthe end of colonial rule, Rwanda experi-enced decades of unrest and intermittentperiods of community level con£ict stem-ming from ethnic divisions a⁄rmed byBelgian colonialism. In April 1994, Rwandawas immersed in a brutal, state sponsored,genocide that killed over one millionpeople within a period of three months.The country’s political and socioeconomicinfrastructure, including the health caresystem, was destroyed.When post genocide reconstruction occur-red, the government began to decentralisehealth system management to the districtsin an e¡ort to provide equitable health carecloser to the communities. In short order,by 2012, every district in Rwanda had afunctioning referral hospital. Each hospitalis associated with eight to 20 primary carehealth centres. The health centre packageof activities encompasses health promotionand prevention activities, as well as curativecare and management of chronic illness(Republic of Rwanda, 2011a). CommunityHealth Workers (CHWs) associated witheach health centre (two to three per village)assist with case ¢nding, medication adher-ence, and follow-up, as well as outreachand educational activities for their commu-nities. As a result of signi¢cant investmentsin the health sector since the genocide,Rwanda has experienced signi¢cant im-provements in premature mortality, includ-ing large reductions in maternal mortality,under ¢ve mortality and deaths secondary toinfectious diseases such as HIV/AIDS, tuber-culosis andmalaria (Binagwaho et al., 2014).
rized reproduction of this article is prohibited.137

Copyrig
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
Mental health policy/systemdevelopmentAlthough data on the speci¢c burden ofmental disorders in Rwanda are limited, thelifetime prevalence ofmajormental disordersacross sub Saharan Africa is estimated to bearound 12% (Lopez et al., 2006). Over thepast half century, mental health care inRwandawas primarily provided by one cen-tral neuropsychiatric hospital, which wasestablished in the early 1970s by a Catholiccharity organisation. Traditional healerswere also called upon to provide mentalhealth care, especially in rural areas. In thewakeof thegenocide,Rwandahashadtocon-tend with signi¢cant additional mentalhealthburdens, includinghighratesofdepres-sion and posttraumatic stress related dis-orders (PTSD) (Munyandamutsa, MahoroNkubamugisha, Gex-Fabry, & Eytan, 2012).In recognition of this highburden, post geno-cide health system reconstruction e¡orts bythe government led to the creation of aDivision forMentalHealthwithintheMinis-tryofHealth (MoH) in1995.Amental healthpolicy was established, which called forthe integration of psychiatric services intogeneral district health systems (Republic ofRwanda, 2011b). Over the ensuing decade,mental health services were gradually decen-tralisedtothedistricts,with inpatientandout-patient mental health services increasinglyprovided by at least one psychiatric nurseand psychologist in each of the 42 districthospitals (Kayiteshonga et al., 2013).However, the national budget for mentalhealthcare, aswell as the ratio of publicmen-tal health workers to population withineach district, has remained low.The MentalHealth National Plan recognises that themost feasible option for improvement inaccess to mental health services is to inte-grate mental health into non specialistprimary care services (Republic of Rwanda,2011b). This integration of mental healthcare into primary care uses a task sharingapproachbydelegating the tasks and respon-sibilities of mental health care from more
ht © War Trauma Foundation. Unautho138
specialised mental health clinicians to lessspecialised primary care providers (Patel,Goel, & Desai, 2009). In 1999, the MoHinitiated basic mental health training forprimary care nurses in order to improvethe recognition and management of men-tal health conditions; however, the humanresource capacity for ongoing healthcentre level supervision following trainingsremained limited.
Partners In Health and the RwandanMinistry of Health collaborationIn 2005, PIH was invited by RwandanPresident Paul Kagame to support Rwan-dan health system development by bringingits community based model of HIV/AIDScare to several of the most rural, impover-ished districts in the country. As Rwandabuilt its national HIV/AIDS programme inthe wake of the genocide, PIH supportedthe MoH to implement additional com-munity based strategies to improve HIVtreatment adherence and retention. Thesestrategies included a CHWaccompanimentmodel that employed regular home visitsand directly observed therapy, in additionto targeted social and material supportdesigned to reduce poverty and other struc-tural barriers to treatment adherence andfollow-up (Farmer et al., 2013). These healthsystem strengthening e¡orts resulted in over92% of enrolled people living with HIV/AIDS in PIH supported districts remainingin care after two years of daily therapy (Richet al., 2012).As clinical outcomes for people living withHIV/AIDS improved, PIH expanded itshealth system strengthening e¡orts to includeother areas of clinical import. In 2009, PIHinaugurated a nascent mental health pro-gramme sta¡ed by a Rwandan national, oneof only several Rwandan psychologists withan advanced degree. This programme wasfunded in part by a gift from the Peter C.Alderman Foundation, as well as by acad-emic support from the Program in Global
rized reproduction of this article is prohibited.

Copyrig
Smith et al.
MentalHealthandSocialChangeatHarvardMedical School. The programme initiallystarted in Kayonza District, in the EasternProvince, with a focus on education andtraining of community leaders on mentaldisorders as treatable conditions. In 2010,theRwandanteamwas expanded to includea psychiatric nurse and a social worker, andstarting in 2011, additional support was pro-videdbyanexpatriateacademicpsychiatristbased in Rwanda and sponsored by PIHand Harvard Medical School (USA)(http://ghsm.hms.harvard.edu/education/fellowships#pagenel). The local Rwandanteam, alongwiththe expatriate psychiatrist,were supported and mentored remotelyand in person by a PIH cross site mentalhealth team ledbya senior psychiatrist withextensiveexperience inglobalmentalhealthdelivery, mental health care and publichealth, and PIH infrastructure with exper-tise in global health programme develop-ment, monitoring and evaluation, as well ascurriculum development and training(Raviola, Becker, & Farmer, 2011).With sev-eral years of collective experience, it wasrecognised by the local team that its activi-ties focusing on community education weredi¡use and unable to be measured ade-quately, representing a barrier in justifyingthe programme’s existence to administra-tive leadership at both PIH and the MoH.This was particularly relevant given theminimal budget for mental health relatedactivities within theMoH programme.In 2011, the collective, collaborative crossnational team developed a strategic planfocused on development of measurableactivities within a single district, Burera Dis-trict, in northern Rwanda. The district isserved by Butaro Hospital, a 150 bed publichospital built in 2011by PIH in collaborationwith the MoH. Butaro Hospital employsapproximately 35 general nurses,13 full timegeneral practitioners, four psychiatric nursesand one psychologist. The hospital includesan outpatient mental health specialty clinicwhich operates ¢ve days per week. Patients
ht © War Trauma Foundation. Unautho
in need of acute psychiatric services aretransferred from the mental health clinic ordirectly from district health centres toButaro Hospital under the care of hospitalbased mental health workers, in collabor-ation with generalist physicians. The hospi-tal is the primary referral centre for 20district health centres, and serves an over-all population of approximately 340,000people, giving a ratio of population to men-tal health sta¡ of 68,000:1.Initially in Burera District, the mentalhealth team focused its activities on support-ing MoH sta¡ to improve integration ofmental health care into medical services atButaro Hospital, particularly for peopleliving with acute psychiatric problems whopresented to the hospital. A psychiatric con-sultation liaison model was implementedwith the aim of reducing transfers by ambu-lance out of the district to the national refer-ral psychiatric hospital at Ndera (Smithet al., 2015). With the increasing transitionof patients back to the local community, thePIH mental health teambegan to work withsatellite health centres to facilitate continuityof care closer to communities and homes,and to learn about e¡ective strategies forimproved care and treatment adherencewithin this context.
Improving primary care: mentoringand enhanced supervision at healthcentresIn November 2010, the Rwandan MoH andPIHcollaboratively launchedtheMentoringand Enhanced Supervision at HealthCentres (MESH) programme for primarycare, designed to strengthen the public gen-eral health centre system and improve thequalityof careprovidedbynurses at primarycare health facilities in PIH supported dis-tricts of Rwanda (Anatole et al., 2013). Thiswas not amental health focusedprogramme.The MESH program’s initial focus was tosupport health centre nurse implementationof clinical protocols in child health, obstet-rical and neonatal care, HIVcare, and adult
rized reproduction of this article is prohibited.139

Copyrig
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
health by incorporating decentralised di-dactic training with ongoing clinical men-torship and quality improvement activitiesat health centres. The model follows closelywith WHO clinical mentoring guidelinesdeveloped for e¡ective task shifting of HIVcare (WHO, 2005).MESH mentors are experienced publicsector nurses with post secondary educationand signi¢cant training in their clinical areaof focus. Each month, the MESH mentorssupervise clinical management and buildclinical reasoning skills with nurse menteesin their area of clinical focus at assignedhealth centres, using an observation check-list to document nurses’adherence to clinicalstandards during direct patient care. MESHmentors use the checklist information to pro-vide real time feedback to nurses regardingtheir clinical performance. During theirsupervision visits, mentors also review sys-tems level performance with nurses and thehealthcentre director, andhelphealthcentresta¡ to implement data driven, qualityimprovement activities.Initial results from the MESH programmedemonstrated signi¢cant improvements ina number of quality of care indicators,including completeness of patient assessmentand improved diagnostic accuracy for cer-tain child and adult illnesses after mentoring(Anatole et al., 2013). The MESH pro-gramme is currently being brought to scalenationally for HIV care in all districts inRwanda, with preliminary plans in placefor further future scale-up in other clinicaldomains.
Integrating mental health careinto primary care: MESHmental health programmedevelopmentIt was recognised that the original HIVandprimary care focused MESH programmeo¡ered an e¡ective primary care healthdelivery strengthening platform uponwhichto implement the national policy of
ht © War Trauma Foundation. Unautho140
integrated mental health care into thepublic sector. Given the initial successes ofthe MESH programme for primary care,in August 2012, the PIH mental healthteam collaborated with Burera DistrictMoH sta¡ to implement a programmeintegrating mental health care into thepublic primary care health system usingthe MESH model.
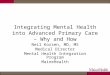
Baseline assessmentA preliminary informal situational analysisof health centres in Burera District was con-ducted in 2012. Semi structured interviewswith district health managers and healthcentre directors were completed to assessmental health service needs at healthcentres, the utility of a training and supervi-sion programme, and the motivation andcommitment of hospital services andselected health centres to participate in theprogramme. In addition, routine data fromhealth centres were informally surveyed todetermine whether mental health serviceswere being o¡ered at the health centres, aswell as any currently available interventionsand psychotropic medications. The range ofmental disorders encountered at the healthcentres was also reviewed, as well as referralpatterns for patients living with mental dis-orders and treatedwithin the BureraDistricthealth system.Three public health centres out of 20were chosen as initial MESH mental healthsites based on geography and high numbersof patients presenting with mental healthproblems (Figure 1). As nurses provide allprimary health care at health centres inRwanda, primary care nurses became thefocus for the MESH Mental Health (MH)programme. Health centre directors wereasked to choose two nurses from their healthcentre for participation in the programmebased on clinical acumen, available clinicaltime and potential aptitude to implementnewly acquired mental health knowledgeand skills. Four major neuropsychiatric
rized reproduction of this article is prohibited.

Copyrig
Health facilities in Burera District
Legend
Health centres
Health posts
New Butaro Hospital
Administrative building
Rivers
Tarmac roadDirt road A
Dirt road B
Figure 1: Map of initial MESHMH health centres.
Smith et al.
disorderswere chosen for clinical focusbasedon needs perceived by district mental healthsta¡ and health centre directors, as well asevidence of burden and treatment e¡ective-ness: schizophrenia; bipolar disorder; majordepressive disorder; and epilepsy (WHO,2011b).
Training and supervision toolsA 40-hour training was developed to teachthe practical aspects of clinical care ofpatients with mental disorders to the healthcentre primary care nurses.Training mater-ials and guidelines were developed andadapted from theWHOmental health inter-vention guide for mental, neurological andsubstance use disorders in non specialisthealth settings (mhGAP) (WHO, 2011b).Other existingMoHand PIHmental health
ht © War Trauma Foundation. Unautho
materials, and published literature for taskshifting in mental health care (Patel, 2003)were also used. The training materials weredeveloped in close collaboration with thegovernment employeddistrictmental healthsta¡, and community experts, to ensure thatall training materials were culturallyrelevant and contextually appropriate tothe local health system. The training curri-culum included: basic communication skills;triage, including recognition of delirium;diagnosis and treatment of selected majormental disorders andepilepsy; psychoeduca-tion and support to patients and families;crisis speci¢c interventions; and triage pro-tocols and referral pathways to specialistcare when appropriate.A mental health supervision checklist wasadapted from pre existing MESH clinical
rized reproduction of this article is prohibited.141

Copyrig
Table 1: MESHmental health supervision checklist elements
Intake assessment- Reason for presentation-History of present symptomatology, including disorder speci¢c follow-up questions- Psychiatric history- Safety assessment-Medical history- Family and social history- Substance use-Vital signs- Basic mental status exam- Overall interviewing skills including expression of support/empathy- Overall clinical assessment, including di¡erential diagnosis
Initial treatment planning- Basic psychoeducation for patients and family- Psychopharmacologic management, including discussion of side e¡ects- Referral to appropriate level of care- Planning for follow-up including collaborationwith community based services (CHWs)
Ongoing management- Symptom assessment- Functioning assessment including ability to get along in the community and self-care-Treatment response, including management of side e¡ects- Ongoing psychoeducation and support-Treatment follow up planning
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
programmes to assist with clinical mentor-ing and to ensure quality of care andstandardisation of activities across clinicaldomains. The checklist contained dichoto-mous scoring of key observable features of aquality psychiatric evaluation, with theintention to improve diagnostic speci¢city,accurate treatment decision making, appro-priate follow-up and referral procedures,and adequate patient and family support,including evidence based psychoeducation(Table 1). The checklist was also designed tofacilitate performance data monitoring inorder to inform the iterative adaptation ofe¡ective mental health practices at thehealth centre level through real time feed-back. In addition, a facilities checklist wasadapted from pre existing MESH clinicaltools to assist with systemsbasedquality con-trols and improvement project development.
ht © War Trauma Foundation. Unautho142
ImplementationTraining
An initialMESH training was held over ¢vedays at Butaro Hospital. This was attendedby two primary care providers from eachpublic health centre in Burera District.Two psychiatric nurses, one governmentemployed and one PIH employed, as wellas one social worker and one Rwanda basedexpatriate psychiatrist, both PIH employed,served as trainers. Training consisted ofdidactic presentations, case studies, smallgroup discussions, several role plays, andparticipatory games to foster critical think-ing and problem solving skills among theparticipants. The mental health trainingpromoted open discussion among partici-pants, and trainers and participants wereencouraged to express opinions about the
rized reproduction of this article is prohibited.

Copyrig
Smith et al.
content andthe training process, and to o¡ersuggestions for improvement. This feedbackwas providedverbally during interactive ses-sions, and by written comments at the endof the training. Three quantitative multiplechoice pre and post tests were used to evalu-ate themental health care related knowledgeof participants before and after the training.The construct validity of the tests was deter-mined by the professional judgment of localand international experts, as well ascomparison with other similar evaluationinstruments used for other MESH clinicaldomains.
Clinical mentorshipFollowing the training, a schedule of individ-ual supervision visits was arranged for thethree selected heath centres. A PIHemployed Rwandan mental health nursementor travelled to each of the three publichealth centres weekly to provide onsite, indi-vidual mentorship to the two health centrenurses trained inmental health care deliveryto run an initial pilot of the model.Themen-tor had a postsecondary degree in psy-chology, as well as training in psychiatricnursing. The health centre visits included:clinical observation, individual case review,documentation review, and brief didacticsessions. The mentor nurse used the caseobservation checklist to assess health centrenurse competency in performing keyelements of basic psychiatric evaluations,accurately diagnosing patients and o¡eringappropriate treatment and support basedon diagnosis. The checklist allowed for realtime assessment and response to trainingneeds and areas for clinical improvement.Supervisory visits initially occurred weeklywith a planned tapering down to bimonthlyvisits after six months and monthly visitsafter one year, although the frequency ofongoing supervision was also predicated onthementor’s assessment of the nurses’clinicalcapabilities and on whether satisfactoryimprovement in checklist scores wereachieved after six months and one year.
ht © War Trauma Foundation. Unautho
Mentor support and trainingThe PIH employed MESH mental healthnurse mentor, representing the role in thefuture of a government employedpsychiatricnurse, received MESH speci¢c training inconjunctionwithMESHmentors fromotherclinical areas, including an initial two-dayclinical mentoring workshop focused onteaching techniques, e¡ective communi-cation, providing feedback, adult learning,using observation checklists in clinical men-toring and quality improvement methodsincluding addressing systems issues. Inaddition, themental healthmentor attendedquarterly supervision meetings with allMESH mentors to ensure coordinationamong clinical domains as well as receivingrefresher training on clinical mentoringskills.Themental healthmentor alsoworkedclosely with the in country expatriate psy-chiatrist to review and improve clinicaltraining materials throughout the year.Thepsychiatrist periodically accompanied thementor on health centre visits to supportsupervisory activities, assess checklist imple-mentation ¢delity and solicit programmefeedback from the health centre director,nurses and patients.
Quality improvementBoth clinical and systems based qualityimprovement activities were integrated intothe MESH mental health programme fromits inception, in accordance with MESHprogramming in other clinical domains.The clinical checklist was periodicallyreviewed with health centre nurses, theexpatriatepsychiatrist, andthenursementorand was modi¢ed to include new elementsor to clarify expectations for clinical prac-tice. This process enabled health centrenurses to understand mental health serviceexpectations and to provide achievable goalsfor improvement. A three-day clinicalrefresher training was held after six months,basedon skills needing improvement as indi-cated by checklist data, as well as the nurse
rized reproduction of this article is prohibited.143

Copyrig
Table 2: Health centre quality improvement initiatives supported by theMESHmental health programme
Identi¢ed gap Action taken
1. Intermittently out of stock ofpsychotropic medications
Strengthened formulary management andcommunication between the district and healthcentre pharmacies
2. Inadequate physical facilities forpatients with mental disorders
Collaborated with health centre directors to ensurededicated clinic space for patients with mentaldisorders
3. Longitudinal documentation ofclinical visits
Health centre nurses created a separate clinic registerfor patients with mental disorders
4. Food insecurity for vulnerablepatients
Established criteria for enlisting social workers tosupport foodpackages for vulnerablepatients in thecommunity
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
mentor’s perception of areas of clinicalconfusion.During each supervision session, the nursementor also discussed systems based per-formance issues and ‘quality gaps’ with thehealth centre director and the health centrenurses, in order to improve patient care, clar-ify referral pathways, improve coordinationbetween services and promote systems levelimprovement.The nursementor alsoworkedwith the health centre sta¡ to formulatespeci¢c plans for improvements relating tothe identi¢ed gaps, using the standard‘Plan^Do^Study^Act’ quality improvementmethodology for accelerating system im-provements (Anatole et al., 2013). Table 2describes selected examples of identi¢edsystemic quality gaps and actions taken toaddress them.
Programme progressUptake by the public sector system, withoutthe creation of a parallel nongovernmentalsystemof care, was rapiddue to a high degreeof organisationandmanagement skillwithinthe Rwandan public health care sector, aclear national mental health planning tem-plate and a successful initial pilot throughthe collaboration with PIH. Preliminaryinformal reports from participating health
ht © War Trauma Foundation. Unautho144
centre nurses, patients and local authoritiesindicated that the MESH MH programmewas feasible and acceptable at the threeinitial health centres. As a result, in August2013, MESH MH mentorship was formallyincorporated into the MoH run publichealth system in Burera District.Todaymen-torship is no longer provided by a PIHemployedMESHmentor, but instead is pro-vided in full by public, governmentemployed district mental health nursesbased at Butaro Hospital.Initially following the transfer of mentorshipfrom PIH to the public sector mental healthnurses, the programme was then imple-mented at three additional health centresin the district. In 2014, the MESHMH pro-gram received a proof-of-concept seed grantfrom Grand Challenges Canada to imple-ment the programme at all 20 health centresin Burera District for full district coverage,with the principal investigators being thenational MoH director of mental healthservices and the Rwandan district clinicalmedical o⁄cer for PIH.
DiscussionFew models exist showing how evidencebased mental health care can be e¡ectivelyintegrated and delivered in real world,
rized reproduction of this article is prohibited.

Copyrig
Smith et al.
resource limited, primary care healthsettings. The MESH MH programmerepresents a systematic and innovative e¡ortto integrate mental health care into the pub-lic health centre primary care system inRwanda. The programme incorporatedmental health care within an existing healthcentre strengthening e¡ort, primarily byadapting structures of supported supervisioninitially designed to help health workersadhere to evidence based practices andguidelines in other clinical domains, initiallyfocused on community based treatment ofHIV/AIDS. There is emerging evidencethat integrated mental health service pro-vision may be most e¡ective in places whereprimary care strengthening e¡orts arestrong (Lund et al., 2012). Additionally,models of task sharing for other disorderssuch as HIV/AIDSmay o¡er other countriesa framework for beginning to integratemen-tal health care into general health settings.The programme described here has a num-ber of strengths and challenges that arediscussed below.
StrengthsPublic health system strengthening
The MESH MH program is ¢rmlygrounded in Rwanda’s National StrategicPlan for Mental Health. The MESH MHprogramme received public commitment atall health system levels both prior to andduring implementation. Initially, the pro-gramme used a nurse mentor who was anemployee of PIH, but mentorship responsi-bilities were handed over to anMoH districtmental health nurse after one year.This gov-ernment employed mental health nurse wasalready integrated into the district hospitalstructure and answers to the medical direc-tor responsible for all health care in the dis-trict. The MESH MH programme menteesare government employed health centrenurses, and all clinical and mentorshipactivities occur directly within the publichealth system. With the exception of theexpatriate psychiatrist, the programme was
ht © War Trauma Foundation. Unautho
designed from the outset to use only humanresources already working within the exist-ing district health system. This ensuredthat the MESH MH programme focusedprimarily on building public capacity toimprove mental health services at the healthcentre level. As Rwanda trains more psy-chiatrists through a new psychiatry resi-dency training programme, the clinicaland supervisory roles occupied by the expatpsychiatrist can eventually be transferredto local psychiatrists so that all roles withinthe MESH MH system will be performedwithin the public sector. In addition, pro-gramme development has been an iterativeprocess between the national MoH mentalhealth team, PIH and local district mentalhealth teams, in order to ensure that pro-gramming overall remains feasible andpossible for scale-up to other districts inthe future.
Consistent and reliable mentorship
In order to safely and e¡ectively deliver men-tal health services within primary care inresource limited settings,mental health integ-ration e¡orts must include capacity buildingfor primary care health workers to providethe actual clinical care of patients withmentaldisorders (Collins et al., 2013).Taskdelegationtofrontlineworkers forotherchronicdisordershas been most successful at improving healthoutcomes when combined with ongoing sup-portive supervision, specialist support andreliable referral networks (WHO, 2008b).The programme provided reliable, clinicallysound supervision of primary care nurses tomanage the chosen four major psychiatricdisorders with independence and to provideclear criteria for referral to district mentalhealth services for more complicated orsevere cases (WHO,2007). At the three initialhealth centres, trained and supervised pri-marycare nurses initially did not feel comfor-table or prepared to provide care on theirownwithout the direct assistance of the men-tal health mentor. After about six monthsof supervision and the additional refresher
rized reproduction of this article is prohibited.145

Copyrig
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
training speci¢cally focused on psychotic dis-orders and epilepsy, nurses reported greatercon¢dence in managing patients indepen-dently in close collaborationwith the mentor.TheMESHmentor also observed, both clini-cally and via improved checklist scores, thathealth centre nurses were managing patientsmore independently with success. A modelemergedinwhichtheprimarycarenursesper-formed the speci¢c basic tasks outlined in thesupervision checklist, including diagnosis,initial and follow-uptreatment, psychoeduca-tion and discussion of patient self-manage-ment techniques. The mentor was used forsupportandguidanceonassigneddaysofmen-torship and was available by phone through-out the week for mentorship of health centrenurses as needed.
Structured supervision checklist
The MESH MH programme adapted astructured clinical mental health supervi-sion checklist from the broader MESH pro-gramme. The checklist was designed toprovide both a baseline for quality of careprovided by health centre nurses and toestablish consistent and transparent criteriafor mentors to use for supervision. Initially,the health centre nurses were concerned thata lower score may a¡ect their work perform-ance evaluations negatively, but the clearstructure of the checklist aswell as discussionabout the purpose of the tool for provisionof quality care promoted ameaningfulwork-ing alliance between the nurses and thementor. This provided a stable and safecontext in which the interpersonal andclinical e¡ectiveness of nurse mentees couldbe improved. The emphasis on a blame freeapproach in providing feedback to cliniciansis consistent with current knowledge inter-nationally on e¡ective health system culturechange in quality improvement (Instituteof Medicine, 1999). The tool also allowedthe mentor to anticipate learning needsearly, to address them in real time, and toengage the health centre nurses in experien-tial learning of improved clinical practices.
ht © War Trauma Foundation. Unautho146
Systems based quality improvement activities
Continuous systems based quality improve-ment processes are a key component of theMESH MH programme. Although theMESHMH mentor suggested areas for sys-tems level improvement based on the facili-ties checklist, quality gaps were most oftenarticulated by the health centre director,the health centre nurses, or both. Healthcentre sta¡ took signi¢cant ownership ofthe improvement initiatives andwould oftenimplement small improvement projects ontheir own. Engaging in systems based qual-ity improvement projects also developedcon¢dence and credibility for health centredirectors andnurses, andthebelief that facil-ity needswouldbe addressed in atimely way.
ChallengesEnsuring adequate coverage of services
Participating health centre nurses wereinitially selected by health centre directors,taking into account the clinical interests ofthe nurses, as well as clinical needs of eachhealth centre. However, each nurse parti-cipating in the MESH MH programmehad numerous clinical responsibilities inaddition to the provision of mental healthcare, and balancing other clinical prioritiesat the primary care level with the provisionof mental health care proved challenging.To address this challenge, health centredirectors and nurses designated one dayper week as the mental health clinic day.One of the two selected nurses participatingin MESH was made available on this dayto receive patients seeking care for a mentaldisorder, and was not primarily responsiblefor any other clinical services on that day.This helped both to ease the clinical burdenonthe primarycare nurses providingmentalhealth care and to ensure regular provisionof services to patients.
Coordination among service levels
Prior to the MESH MH programme ini-tiation, mental health services within thedistrict had been provided almost entirelyat the district hospital mental health clinic.
rized reproduction of this article is prohibited.

Copyrig
Smith et al.
Although the MESH MH programmestrengthened basic care for four major neu-ropsychiatric disorders within the primarycare system, including referrals for compli-cated or ill patients, the process for linkinghealth centremental health care and districtmental health services was di⁄cult to organ-ise. Some patientsbegan seeking care atboththe health centre and district hospital levels,rendering a duplication of activities for ser-vice delivery. Patients whowere hospitalisedfor acute care at Butaro Hospital and thenreturned to follow-up within the primarycare system were also di⁄cult to track.More intensive psychotherapeutic and beha-vioural interventions for depression and psy-chotic disorders, treatment for alcohol andsubstance use disorders, and speci¢c treat-ment for disorders of childhood and adoles-cence also remained available only at thedistrict or central, national level mentalhealth services in the urban capital. Chal-lenges also remain in coordinating careacross sectors and engaging professionalsfrom other disciplines, such as teachers andsocial services in the care of patients withmental disorders. To overcome theseobstacles the hospital mental health clini-cians opened further communication chan-nels to the health centres participating inthe MESH MH programme in order totransmit key information and coordinatecare. A basic electronic database was alsocreated to help track patients fromacute hospitalisation to outpatient care.However, the addition of a new service deliv-ery level for mental health continues torequire further e¡orts to optimally coordi-nate care.
Management of routine and quality data
Although primary care health centres inRwanda routinely collect basic data for allpatients seen at health centres, collection ofdata on mental health services renderedafter the MESH MH programme wasimplemented was challenging. Routine ser-vice use data are recorded in paper health
ht © War Trauma Foundation. Unautho
centre registers by health centre nurses at thepoint of contact with patients. At the time ofMESH MH implementation, however, therecordingofmentalhealthdataintheregisterswas not standardised, and no resources norsta¡ time existed for routine data extractionoranalysis.Inaddition,noelectronicdatabaseexisted yet for the systematic management ofthe MESH supervision checklists in order togauge nurse progress. In response to thesechallenges, health centre nurses created aseparate register for patients with mentaldisorders for easier data extraction and theMESH mentor worked with nurses to stan-dardise the recording of health informationfor patients with mental disorders. Planshave also been made to create a database forMESH supervision checklists to gaugehealthcentre nurse progress in clinical care and tosupplement real time feedback givenbymen-tors on their weekly visit.
Next stepsIntegration of screening toolsAlthough the health centre nurse trainingincorporated both common and severemen-tal disorders, psychotic disorders and epi-lepsy received the most focus as those werethe pressing needs perceived by the healthcentre directors and nurses. As the pro-gramme progresses, valid and reliable toolswill be adapted to context as needed in orderto screen patients for common mental dis-orders, to ensure clinically and culturallysound treatment and to track patient out-comes. This will be useful to ensure reli-ability of diagnosis beyond agreement withmentors and greater diagnostic clarity forall disorders, as well as to systematicallydocument and initiate changes in thetreatment plan for patients who are notimproving.
Implementation of low intensitynonpharmacological interventionsAs the programme grows, culturally soundand evidence based behavioural interven-tions will be incorporated more fully into
rized reproduction of this article is prohibited.147

Copyrig
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
the structured supervision of the MESHMH programme. Basic psychotherapeuticapproaches to depression care, assertivecommunity treatment and psychosocialrehabilitation for patientswith psychotic dis-orders, and brief interventions for alcoholrelated disorders, will be incorporated inthe future. Ongoing needs assessment forincorporating care for the posttraumaticspectrum and acute stress reactions, andchild and adolescent disorders, will alsobe implemented.
Formal engagement with communityhealthA new national CHW curriculum forchronic care and mental disorders has been¢nalised. This curriculum includes trainingon symptom recognition, case ¢nding, refer-ral and follow-up support for patients withmental disorders who receive care at thehealth centres. The curriculum will beimplemented with CHWs associated withhealth centres in Burera District participat-ing in the MESH MH programme. CHWswill then provide the formal linkagesbetween thehealth systemandcommunities,supporting patients in ongoing engagementin care and participating in communitystigma reduction activities.
Rigorousmonitoring and evaluationAs the programme progresses, routine pro-cess data generated by the supervision toolsand checklists will be used to monitor nur-sing and health centre practices, informsupervision and guide continuous qualityimprovement endeavours. An electronicdatabase has been created for retrospectiveentry of demographic andclinical character-istics of patients across all district healthcentres, as well as the district outpatientmental health clinic and will be used forpatient tracking within the district.Indicators of programmatic success willneed to include objective measures ofimprovement in clinical outcomes. A
ht © War Trauma Foundation. Unautho148
comprehensive evaluation of the e¡ects ofMESH MH programming within the dis-trict system of care is planned for the nextphase of programme implementation inorder to document programme impact,including clinical and functioning outcomesfor patients, as well as the impact of theprogramme on individual and householdincomes.
ConclusionThe MESH MH programme to integratemental health care into primary careprovided at health centres grew from aninitial PIH^MoH collaborative e¡ort tostrengthen care provided by health centrenurses in other health domains, as well asRwanda’s strategic priorities to decentralisemental health care to the rural districthealth system.The model is based onWHOguidelines for task sharing in HIVcare thathave proven successful in rural areas ofRwanda. The programme initially used aPIHemployedmental health nurse to super-vise and mentor primary care nurses in thecare of patientswith severemental disorders,but transitioned supervision andmentorshiproles to public sector mental health nursesafter an initial pilot phase. The programmenow engages public, district hospital basedmental health sta¡ to provide ongoing men-torship and supervision of health centrenurses to improve access and quality of carefor patients living with mental disorders.The programme also provides a structuredmodel for integration of mental health careinto primary care in resource limited set-tings. Although a costing analysis is neededprior to large scale delivery of the pro-gramme, the MESH MH programme’slocationwithin the district public health sys-tem encourages its ongoing sustainabilityand creates the potential for scale-up andmore decentralisedmental health care deliv-ery nationally. PIH mental health pro-grammes in other low income countries,working in collaboration with Ministries of
rized reproduction of this article is prohibited.

Copyrig
Smith et al.
Health, have also begun to adapt theMESHMH model based on emerging ¢ndingsand experience.
ReferencesAnatole, M., Magge, H., Redditt,V., Karamaga,A., Niyonzima, S., Drobac, P., & . . . Hirschhorn,L. (2013). Nursementorship to improve the qualityof health care delivery in ruralRwanda.NursOut-look, 61(3),137-144.
Bass, J., Bornemann, T., Burkey, M., Chehil, S.,Chen, L., Copeland, J., & . . . Patel, V. (2012). AUnited Nations General Assembly special sessionfor mental, neurological and substance use dis-orders: the timehas come.PLoSMed, 9(1), e1001159.
Binagwaho, A., Farmer, P. E., Nsanzimana, S.,Karema, C., Gasana, M., de Dieu Ngirabega, J.,& . . . Drobac, P. C. (2014). Rwanda 20 years on:Investing in life.The Lancet, 384(9940), 371-375.
Collins, P., Insel,T., Chockalingam, A., Daar, A.,& Maddox,Y. (2013). Grand challenges in globalmental health: integration in research, policy,and practice. PLoSMed,10.
Farmer, P., Nutt, C.,Wagner, C., Sekabaraga, C.,Nuthulaganti, T., Weigel, J., & . . .Drobac, P.(2013). Reduced premature mortality in Rwanda:Lessons from success. BMJ, 346, f65.
Institute ofMedicine. (1999).To err is human:Build-ing a safer health system.Washington, D.C NationalAcademy Press.
Kakuma, R., Minas, H., van Ginneken, N., DalPoz, M. R., Desiraju, K., Morris, J., & . . . Schef-£er, R. M. (2011). Human resources for mentalhealth care: current situation and strategies foraction. Lancet, 378,1654-1663.
Kayiteshonga, Y., Misago, C., Iyamuremye, J.,Dusabeyezu, J., Rwagatare, P.,Wagner, C, &. . .
Binagwaho, A. Building the national mentalhealth system in Rwanda: Prioritizing equity,decentralization, and integration. In submission.
Lancet Global Mental Health Group. (2007).Scale up services for mental disorders: a call foraction. Lancet, 370(9594),1241-1252.
ht © War Trauma Foundation. Unautho
Lopez,D.,Mathers,D., Ezzati,M., Jamison,T.,&Murray, J. (2006). Global burden of disease and risk
factors. NewYork:World Bank Publications.
Lund, C., Tomlinson, M., De Silva, M., Fekadu,A., Shidhaye, R., Jordans, M., & . . . Patel, V.(2012). PRIME: a programme to reduce the treat-ment gap for mental disorders in ¢ve low- andmiddle-income countries. PLoSMedicine, 9,12.
Munyandamutsa,N.,MahoroNkubamugisha,P.,Gex-Fabry, M., & Eytan, A. (2012). Mental andphysical health in Rwanda14 years after the gen-ocide. Social psychiatry and psychiatric epidemiology,
47(11),1753-1761.
Patel,V. (2003).Where there is nopsychiatrist. London:Royal College of Psychiatrists.
Patel,V., Araya, R., Chatterjee, S., Chisholm, D.,Cohen, A., De Silva, M., & . . . van Ommeren,M.(2007).Treatmentandpreventionofmentaldis-orders in low-income and middle-incomecountries. Lancet, 370(9591), 991-1005.
Patel,V., Goel, D., & Desai, R. (2009). Scaling upservices for mental and neurological disorders inlow-resource settings. InternationalHealth,1(1),37-44.
Patel,V., Belkin, G., Chockalingam, A., Cooper,J., Saxena, S., & Unˇtzer, J. (2013). Grand Chal-lenges: Integrating Mental Health Services intoPriority Health Care Platforms. PLoSMed10(5).
Raviola, G., Becker, A., & Farmer, P. (2011). A glo-bal scope for global health^including mentalhealth. Lancet, 378(9803),1613-1615.
Republic of Rwanda,Ministry of Health. (2011a).Service Packages for Health Facilities at Di¡erent Levels
of Service Delivery. Kigali: Republic of Rwanda.
Republic of Rwanda,Ministry of Health. (2011b).National Mental Health Policy. Kigali: Republic ofRwanda.
Rich,M.L.,Miller,A.C.,Niyigena,P.,Franke,M.F., Niyonzima, J. B., Socci, A., & . . . Binagwaho,A. (2012). Excellent Clinical Outcomes and HighRetention in Care Among Adults in a Com-munity-Based HIV Treatment Program in Rural
rized reproduction of this article is prohibited.149

Copyrig
Integrating mental health care into primary care: the case of one rural district in Rwanda
Intervention 2017, Volume 15, Number 2, Page 136 - 150
Rwanda. Journal of Acquired Immune De¢ciency
Syndromes, 59(3), e35-42.
Rowe, A. K., de Savigny, D., Lanata, C. F., & Vic-tora,C.G. (2005).Howcanweachieveandmaintainhigh-quality performance of health workers inlow-resource settings? The Lancet, 366(9490), 1026-1035.
Smith, S. L., Grelotti, D. J., Fils-Aime, R., Uwi-mana, E., Ndikubwimana, J.-S.,Therosme,T., &. . . Fricchione, G. L. (2015). Catatonia inresource-limited settings: a case series and treat-ment protocol. General Hospital Psychiatry, 37(1),89-93.
World Health Organization. (2005).WHORecom-
mendations for Clinical Mentoring to Support Scale-up
of HIV Care, Antiretroviral Therapy and Prevention in
Resource-Constrained Settings. Geneva:WorldHealthOrganization.
World Health Organization. (2007).Task shiftingto tackle health worker shortages. Geneva: WorldHealth Organization.
World Health Organization. (2008a). IntegratingMental Health into Primary Care. Geneva: WorldHealth Organization.
World Health Organization. (2008b).Task shift-
ing: global recommendations and guidelines. Geneva:World Health Organization.
World Health Organization. (2011a).WHOMen-
tal Health Atlas. Geneva: World Health Organiz-ation.
World Health Organization. (2011b). mhGAP In-
tervention Guide for mental, neurological and substance
use disorders in non-specialized health settings. Geneva:World Health Organization.
Stephanie L. Smith is the Deputy Director of
MentalHealthatPartners InHealth, anAssoci-
atePsychiatristatBrighamandWomen’sHospi-
tal, and an Instructor in Psychiatry at Harvard
ht © War Trauma Foundation. Unautho150
Medical School, Boston, MA, USA. She is also
a former Pagenel Fellow in Global Mental
Health Delivery at Partners in Health in
Rwanda.
email: [email protected].
YvonneKayiteshongaistheManageroftheMen-
tal Health Division, Rwanda Biomedical
Centre, Kigali, Rwanda.
Claire N.Misago is the Director of Community
Rehabilitation, Mental Health Division,
Rwanda Biomedical Centre, Kigali, Rwanda.
Jean Damascene Iyamuremye is the Director of
the Psychiatric Unit, Mental Health Division,
Rwanda Biomedical Centre, Kigali, Rwanda.
Jeanne d’ArcDusabeyezu is the SubstanceAbuse
Specialist, Mental Health Division, Rwanda
Biomedical Centre, Kigali, Rwanda.
Achour A. Mohand is theTechnical Assistant
Psychiatrist,MentalHealthDivision,Rwanda
Biomedical Centre, Kigali, Rwanda.
Robyn A. Osrow is the Mental Health Activity
Manager, Me¤ decins Sans Frontie' res Belgium,
Kenya. She is a former Pagenel Fellow in Global
Mental Health Delivery at Partners In Health
in Rwanda.
Manzi Anatole is the Director of Global Learn-
ing andTraining at Partners In Health, Boston,
MA.
Shin Daimyo is a Senior Advisor for Mental
Health at Partners in Health and a Master of
Science in Nursing candidate at theYale School
of Nursing.
Eugenie Uwimana is the Mental Health Lead,
Butaro Hospital, Burera District, Rwanda.
Dominique Dushimiyimana is a Psychiatric
Nurse at Butaro Hospital, Burera District,
Rwanda.
GiuseppeJ. Raviola is the Director of Mental
Health at Partners in Health, Boston; and the
DirectorofthePrograminGlobalMentalHealth
and Social Change at HarvardMedical School’s
Department of GlobalHealth and SocialMedi-
cine, USA.
DOI:10.1097/WTF.0000000000000148
rized reproduction of this article is prohibited.