Embed Size (px)
Citation preview

RESEARCH ARTICLE Open Access
Integrated liaison psychiatry services inEngland: a qualitative study of the views ofliaison practitioners and acute hospitalstaffs from four distinctly different kinds ofliaison serviceKeeble Jasmin1, Andrew Walker2, Elspeth Guthrie3* , Peter Trigwell4, Alan Quirk5, Jenny Hewison3 ,Carolyn Czoski Murray3 and Allan House3
Abstract
Background: Liaison psychiatry services provide mental health care for patients in physical healthcare (usuallyacute hospital) settings including emergency departments. Liaison work involves close collaboration with acutehospital staff so that high quality care can be provided. Services however are patchy, relatively underfunded,heterogeneous and poorly integrated into acute hospital care pathways.
Methods: We carried out in-depth semi-structured interviews with 73 liaison psychiatry and acute hospital stafffrom 11 different acute hospitals in England. The 11 hospitals were purposively sample to represent hospitals inwhich four different types of liaison services operated. Staff were identified to ensure diversity according toprofessional background, sub-specialism within the team, and whether they had a clinical or managerial focus.All interviews were audio-recorded and transcribed. The data were analysed using a best-fit framework analysis.
Results: Several key themes emerged in relation to facilitators and barriers to the effective delivery of integratedservices. There were problems with continuity of care across the secondary-primary interface; a lack of mentalhealth resources in primary care to support discharge; a lack of shared information systems; a disproportionatelength of time spent recording information as opposed to face to face patient contact; and a lack of a shared visionof care. Relatively few facilitators were identified although interviewees reported a focus on patient care. Similarproblems were identified across different liaison service types.
Conclusions: The problems that we have identified need to be addressed by both liaison and acute hospitalteams, managers and funders, if high quality integrated physical and mental health care is to be provided in theacute hospital setting.
Keywords: Consultation-liaison, Liaison mental health, Liaison psychiatry, Hospital psychiatry, Qualitative, Healthservices research
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected] Institute of Health Sciences, University of Leeds, Leeds, UKFull list of author information is available at the end of the article
Jasmin et al. BMC Health Services Research (2019) 19:522 https://doi.org/10.1186/s12913-019-4356-y

Liaison psychiatry is the sub-specialty of psychiatry thatfocuses upon the interface between psychiatry and non-psychiatric clinical services [1]. Most commonly this in-volves psychiatric provision to the acute general hospitalbut can include other specialist hospitals and also pri-mary care [2]. Several different models of liaison psych-iatry exist with differing degrees of penetration into thegeneral hospital and different styles of working [3]. Themost common types of service in the UK are hospitalbased teams that provide on demand consultation andtreatment for patients in acute hospital settings, withsome also providing out-patient work or specialist in-reach to specific medical teams/specialties. The termpsychosomatic medicine has been used to refer to liaisonservices, although this term is now used more specific-ally to refer to services that provide treatment forpatients who have physical and mental co-morbidities.Liaison services provide treatment for all patients in theacute hospital with mental health problems includingthose with physical and mental co-morbidities, self-harm, dementia, alcohol and drug related problems,behavioural disturbance etc., There is growing, althoughstill somewhat limited, evidence that liaison psychiatryservices are effective [4] and may lead to cost reductionsin healthcare [5].In the United Kingdom, liaison psychiatry is a sub-spe-
cialty of general psychiatry. Psychiatric higher trainees cangain an endorsement in liaison psychiatry by undertakinga 12month training, but this is not mandatory. There areno specific training requirements in liaison psychiatry forphysicians or nurses. General practice trainees are encour-aged to spend six months in a psychiatry training postwhich can include liaison psychiatry,A recent survey of all acute general hospitals in
England reported that 168 out of the 179 acute hospitalswith an emergency department had some form of liaisonpsychiatry service [3]. Further expansion is planned, witha national target that at least 70% of all acute hospitalsin England will have liaison services staffed to keycommissioning standards by 2023/2024 [4]. This willmost probably mean an increase in staffing for manyservices, and there is an expectation that the cost offurther development will be offset by financial savings,predominantly via a reduction in either length of stay orre-admission rates.Most liaison services in England are commissioned,
managed and delivered as part of mental health servicesrather than general hospital services. The core of liaisonwork, however, involves close collaboration with generalhospital staff to ensure the best care is provided forpeople with mental and physical health problems. Therecent National Confidential Enquiry into PatientOutcome and Death (NCEPOD) into standards of carefor people with mental and physical health problems in
the general hospital highlighted various problems withcurrent provision and quality of care [5]. One of its keyrecommendations was that liaison staff should be part ofthe general hospital multidisciplinary team - fully inte-grated into the general hospital system.Integrated health systems are considered to provide
superior performance in terms of quality and safety as aresult of effective communication, and shared decision-making, although these outcomes have not been fullydemonstrated [6, 7]. Integrated care has been defined as,“a coherent set of methods and models on the funding,administrative, organisational, service delivery and clinicallevels designed to create connectivity, alignment and col-laboration within and between the cure and care sectors”[8]. There is no accepted conceptual model for health sys-tems integration but key principles affecting clinical deliv-ery include: patient focus (ensuring the patient receivesthe right care in the right place at the right time); inter-professional team working; information systems which en-hance communication capacity and information flowacross integrated pathways; and an organizational culturethat is congruent with a shared vision of care [9].To explore the degree to which current liaison
psychiatry provision in England is indeed integrated intophysical health care, we undertook the present studyinterviewing liaison mental health staff working in gen-eral hospital liaison services and acute hospital staff whohad experience of referring to liaison services. In thispaper, we focus on facilitators and barriers to providinghigh quality, multidisciplinary care in relation to each ofthe above areas, and present the themes that arose fromthis work according to the key principles of integratedcare outlined by Suter and colleagues [10]: co-ordinatedtransitions in care across the continuum of care; patientfocus; presence or absence of primary care structures tosupport discharge; inter-professional team working;communications systems; organizational goals and ob-jectives aligned across sectors; physician integrationwithin teams; and attainment of goals and objectives aresupported by funding and human resource allocation.
MethodsThis work formed part of the first phase of a programmefunded through the NIHR Health Services and DeliveryResearch scheme to evaluate the cost-effectiveness andefficiency of different configurations of liaison psychiatryservices in England (LP-MAESTRO) (http://www.nets.nihr.ac.uk/projects/hsdr/135808/#/). Ethics approval wasreceived from the North of Scotland Ethics ResearchService (REC reference: 15/NS/0025) and NHS Trust levelapprovals obtained. All participants provided writteninformed consent. We have followed the ConsolidatingCriteria for Reporting Qualitative Studies (COREQguidelines) [11].
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 2 of 14

Research team and reflexivityThe interviews were carried out by two researchers AW(male) and JK (female); one from the LP-MAESTROproject itself (AW) and one from the College Centre forQuality Improvement (JK), the Royal College of Psychia-trists, both qualified by experience and training. Neitherwere involved in the delivery of clinical services andwere not mental health professionals.
DesignA cross sectional qualitative study of liaison mentalhealth staff and acute hospital staff about their experi-ences of liaison psychiatry services.
Theoretical frameworkThe data were analysed using a best-fit frameworkanalysis [12]. The key themes that emerged weregrouped, where relevant, according to Suter andcolleagues [9]. The topic guide did not make referenceto the Suter principles, which were used after the initialframework analysis to structure the themes.
Participant selectionA sample of liaison services was identified using thefollowing procedures. All 168 hospitals in England thathad a liaison service were asked to complete an on-linesurvey about liaison psychiatry services [3]. A memberof staff from each of the 168 services (100%) completedthe survey. The survey data were analysed using a latentclass model to perform clustering of the hospitalservices, which is described in detail in a separatepublication [13]. Four clusters were identified, none ofwhich mapped onto current liaison classifications suchas CORE [14] (types of liaison services defined bycommissioning guidelines from NHS England) or RapidAssessment Interface Discharge (RAID) teams [15]. Thefour clusters basically comprised:
� small services, which in the main did not provide 24/7cover or out-patient services (Cluster 1) (n = 46)
� services that provided 24/7 acute cover but verylittle non-acute work (Cluster 2)(n = 35)
� services that covered the acute work but offerednon-acute care and ran outpatient clinics(Cluster 3) (n = 43)
� services that were not exclusively focused on theacute care pathway, provided non-acute care andhad separate adults of working age and older adultteams (Cluster 4) (n = 44)
All 168 liaison services were then contacted by emailto determine their interest in participating in the presentqualitative study. Eighty-six services (51%) did not reply,6 indicated initial interest but then provided no further
contact, 33 declined (18%), and 17 services (10%) wereexcluded as they had undergone significant change sincethe initial survey.This left 30 services (18%), staff from which were in-
vited to one of two workshops at which the aims of thepresent study were explained, in addition to those of therest of the programme. Representatives from 13 services(8%) attended the workshops and 11 of these serviceswere purposively sampled, informed by the cluster ana-lysis, to ensure that each of the 4 clusters was repre-sented by between 2 and 4 liaison services.In each of the 11 services, we sampled staff identified
to ensure they were knowledgeable about the realities ofservice provision and diverse in experience according tothe following characteristics: professional background,sub-specialism within the team, and clinical or manager-ial focus. The local Liaison Psychiatry [16] lead, receiveda list of potential interviewee roles from the projectmanager (AW). The LP lead then contacted the LP teamand asked if anyone did not want to participate. The LPlead then provided contact details by emailing potentialinterviewees with an introductory email and informationsheet and participant information sheet. The LP leadscheduled interviews and informed consent wasobtained in writing at the time of the face to faceinterview.We also interviewed acute hospital staff served by the
liaison services about their experience of the liaisonteam. We sampled staff from regular referrers to theliaison service, obtaining as wide a range of differentreferrers as possible.
Data collectionSeventy three participants were interviewed in-depth, in-dividually, using a semi-structured topic guide informedby similar approaches in for example realist evaluationfocusing on events or processes rather than norms,values or presumptive theories [17]. With permission, allinterviews were audio-recorded. The topic guide wasdeveloped specifically for this study and consisted of alist of key topic areas with open ended questions andadditional prompts. The topic guide is available anadditional file (Additional file 1). Exact wording was leftto the researchers to tailor to the individual participant.The following areas were covered:
a. Introductory questions identifying the role of theparticipant and their professional history.
b. Participant’s understanding of the structure of theliaison psychiatry service, and account of wherethey worked within it.
c. Participant’s account of types of clinical workundertaken, and outcomes aimed for.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 3 of 14

d. Nature of working relationships in the acutehospital, in the associated Mental Health Trust, andwith other professionals and agencies with whomthe participant interacted.
e. Participant’s understanding of the origins of theservice, current influences on its form andfunctions.
f. Participant’s views on desirable changes and ways toachieve them.
The interviews took place between October 2016 andJanuary 2017 at the participant’s place of work and wererecorded and transcribed verbatim. The interviews lastedbetween 30 min to 90 min.
Data analysisThe data were managed using the qualitative softwarepackage NVivo (version 11). Transcripts were systemat-ically summarised. JK and AW have a working know-ledge of mental health but are not psychiatrists and didnot have prior contact or involvement with liaisonpsychiatry services. The following researchers were in-volved in the qualitative analysis: JK, AQ, AW and AH.There is a potential bias in that one of the 73 partici-pants interviewed (EG) was a member of the researchteam, however, EG did not have access to the interviewsor transcripts and was not involved in any of the qualita-tive analyses, or any discussions about the analyses.These analyses were written up in the form of a reportby the qualitative team, with the lead author JK. EG wasnot involved in this work. There were no repeatinterviews. Transcripts were not returned to participantsfor comment or correction.
ReportingQuotations from participants are used in the resultssection to illustrate themes.
ResultsSample characteristicsSeventy three in-depth qualitative interviews wereconducted with professionals from the liaison services(n = 60) and acute trust colleagues (n = 13), who hadexperience of working with the liaison teams. Serviceswere of varied size and had diverse configurations andstaffing levels, as indicated by membership of the 4different clusters. The number of participants inter-viewed therefore varied between services -between 4 and11 interviews were conducted at case study sites.There were 2 hospitals in Cluster 1 (8 liaison mental
health staff ), 2 hospitals in cluster 2 (10 liaison mentalhealth staff and 1 acute hospital staff member), 3 hospi-tals in cluster 3 (15 liaison mental health staff and 5
acute hospital staff ) and 4 hospitals in cluster 4 (26liaison mental health staff and 8 acute hospital staff ).A greater proportion of liaison staff were interviewed
than acute hospital staff as our main focus was on theliaison teams. Fewer staff were interviewed in Cluster 1hospitals than the other hospitals as the teams weremuch smaller, and despite efforts, we were unable tointerview an acute hospital staff member in these twohospitals.
FindingsTable 1 shows the original nascent themes and how theywere grouped according to the ‘nature of the liaisonteams’ and the key principles outlined by Suter andcolleagues [16].
The nature of the liaison teamsAs is common nationally, the liaison psychiatry servicesin our sample were provided by Mental Health Trustsbut served Acute Hospital Trusts. The liaison psychiatryservices were teams of psychiatrists and liaisonpractitioners - most commonly mental health nurses,sometimes with one or more psychologist, social worker,therapist, or physician associate. They took referralsfrom physical health colleagues in acute hospitals -Emergency Departments [13], acute medical units andgeneral wards, out-patient settings and primary care.There was a broad agreement amongst the liaison teammembers interviewed of the aims and purpose of theservices. These were to help with the management ofpatients with co-morbid physical and mental healthproblems, and where relevant, facilitate the safe dis-charge of patients to appropriate settings.Seven main types of clinical scenarios emerged involv-
ing people with: self-harm; delirium and dementia, typic-ally in people with physical health problems; severemental illness co-existing with physical health problemsadmitted to hospital or seen in the ED; mental healthproblems arising as a consequence of long-term physicalillness or its medical treatment; physical illness exacer-bated or caused by mental health problems for examplethrough poor adherence to treatment regimes, or byother mechanisms; unexplained persistent physicalhealth symptoms, the severity and chronicity of whichwere disproportionate to suspected underlying diseasemechanisms; physical or psychological consequences ofalcohol or drug misuse.Our participants recognised social influences on the
referral patterns - vulnerable groups including homelesspeople and those who experienced domestic abuse wereparticularly likely to be referred, and hospitals whichserved particularly large ageing or student populationsexperienced more referrals from these groups.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 4 of 14

Several themes emerged in relation to facilitators andbarriers to the effective delivery of services. Thesethemes were considered, and discussed within theresearch group, and are presented according to keyprinciples of integrated care outlined by Suter and
colleagues (2017) [16], as nearly all were captured by thisframework. Themes that fell outside of these principlesincluded those involving internal processes within theteams for the assessment and treatment of patients,which will be covered in a separate publication.
Table 1 Original themes that emerged from the data, grouped according to the ‘nature of the liaison teams’ and the Principles ofIntegrated Care by Suter and colleagues [14]
Original themes Groupings
Role of liaison psychiatryService development and historyDiversity of workComponents of liaison services organised in different waysAims and purposes of servicesTypes of patient problems seen by liaison services
The nature of the liaison teams
Principles of Integrated Care (Suter et al., 2010) [10]
Confusion about the referral process to liaison servicesInappropriate referrals including patients with no mental health problemsOnward referral and signposting
Co-ordinated transitions in care across the continuum
Value of assessmentsResponse to non-engagementHelping patients to manage mental health issues better via informal learningopportunitiesDescription of the clinical processContinuing support and assessment of needsBrief interventions or follow-ups during admissionMedication prescribingPreventing suicidesAvoiding exacerbating long-term mental health problemsImproving quality of lifeImproving adherence to medication for physical health problemsImproving clinical outcomes for patients
Patient focused care
Gaps in service provisionInteraction with external psychiatry teams Difficulty in accessing community services
Primary care network structures in place
Relationships with referrersCollaborative workingTraining and education- Influencing team members and acute service colleagues
Inter-professional team working and team effectiveness
Notes and recording systemsTime taken to record informationDuplication of record keepingAbsence of shared record keeping
Information systems which enhance communication capacityand information flow across integrated pathways
Physical space and identityProblems with commissioning of liaison teamsVisibility
Organisational goals and objectives aligned across sectors
Hierarchies in mental health and acute trustsAlternative perspectives regarding training of acute staff
Physician integration within care teams and across sectors
Reduction in length of stayLimiting time patients spent in EDBetter communication with commissionersPromoting safe and efficient services-mismatch between staffing levels and volume ofreferralsSpecialism versus generalismInfluencing commissioners to expand systemsInfluencing mental health trust managersNational models and structuresPerceived prioritisation by commissionersPromoting safe and efficient services
Attainment of goals and objectives are supported by fundingand human resource allocation
What liaison services wanted to change- internal delivery processes and structuresChallenges in delivering trainingAddress mental health stigma amongst acute services colleaguesAlternate persectives about training
Do not map onto a specific principle
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 5 of 14

Coordinated transitions in care across the continuumProblems with coordinated transitions in care emergedin relation to referrals to the liaison teams from theacute hospital teams, and from the liaison teams tocommunity/primary care services.
i) Problems with referrals to the liaison services
Some acute trust professionals described frustrationwith a perceived lack of responsiveness from liaisonteams. This was more common in the larger liaisonservices (20+ team members) that were likely to haveseparate components leading to confusion and frustra-tion when referring a patient. There was also confusionabout the location of responsibility between hospital-based liaison teams and community mental healthservices. As a participant from an acute trust explained:
‘I have once lost my rag on the phone and said, 'I don'tbloody care. Somebody from mental health needs tocome and see this patient. You can argue betweenyourselves whether it's the inpatient team or thecommunity team. That's not my job.’ (sF_p01)
Conversely, some liaison psychiatry professionalsdescribed frustration when they received referralsfrom acute service colleagues for patients who theythought were inappropriately referred - for example, apatient who had received some distressing news orhad had a recent bereavement, and may have beenvisibly distressed but not suffering from a mental ill-ness. Liaison staff speculated that acute hospital col-leagues referred patients with these types of problembecause they lacked confidence. Liaison psychiatryprofessionals also felt that it might not be sustainableto accept referrals for what they described as morestraightforward cases which they felt acute hospitalteams should be able to manage themselves, forexample, patients with delirium. As a liaison partici-pant reported, with reference to managing deliriumon wards:
‘If we always do everything then they don’t learn to doit for themselves! …sometimes we’re inundated withreferrals so if we see everything… well actuallysometimes you can’t so sometimes they get left waitinga little bit’ [sI_p06].
While liaison staff felt it was within their remit to helpacute hospital colleagues rule out mental health/psychi-atric problems, they thought acute hospital colleaguesshould be able to manage patients who were emotionallydistressed but not mentally ill, and those with relativelystraightforward mental health problems.
Liaison staff who worked in services representative ofall the different clusters described a higher rate ofinappropriate referrals from new junior doctors whowere particularly risk averse.
ii) Difficulty in accessing community services
Several barriers emerged in being able to accesscommunity services. Liaison staff expressed concernthat patients experienced difficulties and delays inaccessing external services following liaison referral.One explanation was perceived inefficiencies in hos-pital administration systems such as delays in sendingout referral letters.Staff, however, also reported a perceived unreceptive-
ness of community services to patients who werereferred. When referrals were managed by gatekeepers,there were concerns that patients might subsequently betold they did not meet the threshold for a particular ser-vice, and no clear arrangements or plan could be estab-lished prior to discharge. Referral to some servicesinvolved long waits, resulting in what staff members feltwas an unacceptable, circular process.For example, a liaison participant described the case of
a young person who had been referred to the localImproving Access to Psychological Treatment Services(IAPT) following self-harm. The IAPT service, however,felt she was too high risk for them to manage and sug-gested placing her under the care of the CommunityMental Health Team (CMHT). Whilst this referral wasbeing expedited the young person’s state of minddeteriorated and she was re-admitted to hospitalfollowing a suicide attempt. The liaison team memberwas frustrated by this incident.
‘I mean we feel super frustrated. Incrediblyfrustrated and just really sad for this girl who justneeded … a little bit of talking therapy and sheneeded some actual practical support. She's 18 andit was all a bit horrible socially. Instead she gotpassed around which just fed into those feelings ofrejection’ [sA_p03]
There were also examples of older people, who li-aison staff suspected had dementia and were caughtup in protocols between memory clinics and commu-nity mental health teams. This presented difficultiesfor liaison psychiatry services when these patientswere repeatedly admitted to acute hospital beds, buthad not been given a diagnosis of dementia. Staffreported it was inappropriate to diagnose dementiawhen a patient was acutely unwell, so liaison staff feltfrustrated that they were unable to develop appropri-ate care plans.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 6 of 14

Patient focused careLiaison staff valued highly the role of detailed psycho-social assessments as part of their work, and assessmentswere viewed as an important step to ensuring patientsreceived the best possible care. Assessments were de-scribed as typically lasting up to an hour and involvedexploring reasons for admission, the person’s view oftheir own circumstances and risk, resulting in a detailedpicture of the patient’s current situation. Assessmentswere regarded as therapeutic in their own right,providing an opportunity for patients to feel heard andunderstood. Liaison staff reported some patients show-ing visible signs of improvement during the assessmentinterview:
‘Often we’ll get feedback from the patients saying it’sreally nice to have somebody to talk to. It’s really greatthat you really listened to me today. Because we kindof expect that we’re going to spend 40, 45 minutes withsomebody, the fact that we sit down and they get achance to talk. They don’t get that on a really busyward. Em… you know the doctors and nurses willcome in, get the information they need quite quicklyand go again. So we often get told that you’re the firstperson that’s listened to me.’ [sI_p06]
Liaison staff felt that assessments should be of ahigh quality and carried out by appropriately trainedstaff, who had the right ‘tone, volume and attitude’ tofacilitate engagement and, encourage the patient tospeak freely. Participants reflected that patientssometimes found it easier to talk to nurses, or othernon-medically trained professionals, because theyperceived them as being lower down a hierarchy ofdoctor – nurse – patient.Some staff provided continuing treatment for
patients admitted to acute hospitals over longer pe-riods. For example, at one service this involved men-tal health nurses regularly visiting older adult patientsor those on stroke wards to provide encouragementwith eating and rehabilitation; two vital componentsfor ensuring recovery. Teams that had psychologists,therapists or mental health nurses trained in specificinterventions (like cognitive behavioural therapy)offered brief interventions while the patient was in anacute hospital bed, or a follow-up appointment afterthey had been discharged.Liaison staff believed a large part of their overall work
was to teach patients how to manage their mental healthproblems better. Liaison services described this as pro-viding basic psychological education. This was true of allsettings, but particularly the focus of out-patient clinics.One service provided home-visits for COPD patients,primarily focused on education and management. This
involved a minimum of two to three sessions, which wasused to teach patients breathing and relaxation techniques.
Primary care network structures in placeLiaison staff described gaps in service provision afterdischarge. This was particularly evident for patients withmedically unexplained symptoms (MUS). Several staffexpressed concern about no suitable services for thisgroup of patients, who had persistent and disablingsymptoms, and who required more intensive treatmentthan the brief, shorter term packages available. As aparticipant explained:
‘They need long-term psychotherapy with a reliable,skilled practitioner, probably Band 8A (highly skilled) ,who will see them every week and support them inmaking small, small changes. What they get is a Band5 (moderately skilled), if you're lucky, IAPT person …and it's not therapeutic for anybody concerned.’[sB_p03]
Participants reflected that there simply was not thefunding available for this sort of treatment, which reliedon incremental change over a period of months. Somestaff reported making direct individual appeals to theirClinical Commissioning Groups to provide appropriatetreatment for certain people with severe problems. Alack of appropriate treatment facilities was a source offrustration for staff, who worried that these patientswould remain seriously unwell and could end up havingunnecessary investigations or treatments, which wouldbe detrimental to their overall health.Whilst staff who worked in liaison services with dedi-
cated out-patient clinics could provide some provisionfor these patients, they worried about their ability toprovide comprehensive care. Staff who worked in liaisonout-patient clinics did see patients with severe MUS:
They [CMHTs] would not know how to treat patientswith complex medically unexplained symptoms onhigh-dose opiates or they wouldn't know how to treatpatients with non-epileptic seizure disorder. So, I thinkwe see a different group of patients, so we provide thetherapy because the CMHTs wouldn't offer thesepatients treatment [sF_p04]
A suggestion from some liaison staff was that experi-enced liaison clinicians should be embedded either intocommunity mental health teams, or community/primarycare liaison services and should be resourced to providelong-term treatment. While liaison staff acknowledgedthis was costly, one view was that non-intervention waseven more expensive, if subsequent contacts with acuteand mental health services, were taken into account.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 7 of 14

Inter-professional team working and team effectivenessGenerally, staff described good working relationshipswith colleagues from different specialties. Close workingrelationships were described between liaison psychiatryservices and acute hospital colleagues, especially thosethat had developed over years. This sort of relationshipwas underpinned by the liaison service having credibilitythrough a detailed understanding of both medical andmental health. As an acute trust participant describedtheir relationship to their liaison service:
‘[Previous liaison psychiatrist] had a good teamaround him and provided good rapport, can relate tothe problems on the shop floor. [Current liaisonpsychiatrist], who came up through the system…youknow, there's a good knowledge of the individual andtherefore there's also a good working relationship.’[sJ_p05]
Liaison services and acute referrers who had workedin the same acute hospital over decades felt that thislength of time facilitated productive relationships andled to fewer barriers to making referrals; theyunderstood who and what the liaison team did, and howto contact them.Liaison psychiatrists felt it was part of their role to
work collaboratively with acute hospital consultants toimplement agreed plans in acute hospitals. For example,at one service (based in an acute hospital), a liaisonpsychiatrist explained how they would find the consult-ant in charge of the patient’s management plan anddiscuss the patient’s management in detail.In general, it was felt that those who worked in liaison
psychiatry services, regardless of background, needed toproject professional competence. A consultant psych-iatrist reflected:
‘If you go on the wards, you've got to get the notes,read the notes, discuss the person with the nursingstaff and the medical staff, and often they'll be justtalking about people with a consultant physician orconsultant surgeon so you have to have someconfidence in what you're saying’ [sH_p03]
Training and education was also seen as a part ofbuilding collaborative working.
‘A lot of my job is about training and understanding,and trying to have a presence there, and trying to getpeople to think about things’. [sF_p06]
Close working was also described in relation toprescribing medication. Advice and guidance about theuse of psychotropic medication in physically unwell
patients was provided by liaison services, principally byliaison psychiatrists. In many acute hospitals, liaison psy-chiatrists were not able to prescribe medication, as theywere employed by a separate organisation (e.g. a mentalhealth trust), but provided a key role in providing appro-priate advice to medical and surgical colleagues.Acute staff referred to an informal osmosis of skills in
mental health communication if inter-professionalrelationships were productive.
‘I've learned a lot from it actually. Little things like thevocabulary you use, the ways you describe some of thesymptoms that the patient is complaining of, anddescribe what's causing it…So you might say that weknow that the symptoms you have are very real, weknow that you're experiencing these symptoms and thechallenge we're facing is the way that your braininterprets those symptoms. One of the examples theyused, which I've stolen and used again, is, say, whenyou stub your toe and you're in a bad mood it feels alot worse than when you stub your toe and you'reskipping on the beach. So it's just a little explanationas to the way the mind and pain work together, so itwas a really helpful explanation which I have stolen’.[sK_p06 ]
Information systems which enhance communicationcapacity and information flow across integrated pathways
i. Time taken to record clinical contact
Liaison team members expressed concerns about theamount of time required to adequately document andrecord clinical contact with patients. This could take upto two hours in some instances and limited the respon-siveness of the team to other referrals.
ii. Absence of a shared patient record system
Both acute hospital staff and liaison team membersdescribed frustration with the absence of a sharedpatient record system.Liaison staff described having to enter similar/dupli-
cate data on mental health systems and acute hospitalsystems. If acute trusts still used paper clinical records,this would also involve writing in the clinical notes. Thisduplication added to an already lengthy process ofclinical documentation.Acute Trust staff described being unable to access
mental health records for their patients, which interferedwith providing good quality care. For example, a geriatri-cian who wanted to know if there was a pre-existing de-mentia diagnosis felt this information should be freely
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 8 of 14

available to the acute trust and did not perceive it assensitive information. Other examples involved the man-agement of patients with multiple presentations to acuteservices with medically unexplained symptoms, wheresharing of mental health information would have facili-tated improved care.Some services developed ways of circumnavigating in-
formation barriers, for example, foundation doctors(medical trainees in their earliest years of training), whowere attached to liaison services for brief training pe-riods, could access both mental health and acute trustsystems. At larger liaison services, where team memberswere more likely to attend multi-disciplinary team meet-ings in the hospital, it was easier for team members tocheck mental health records for acute services col-leagues, and report back at the next meeting, althoughthis was time consuming and cumbersome.
Organizational goals and objectives aligned acrosssectors
i) Lack of visibility
There was little evidence that acute hospitals and li-aison teams had a shared vision of integrated care. Thiswas most stark in hospitals where the liaison team re-ceived no referrals from certain parts of the acute ser-vice. Liaison staff reported a lack of visibility, forexample, not receiving any referrals from surgical wards.While liaison teams in this situation reported making ef-forts to promote their services more widely, they alsofeared this may lead to levels of service demand thatthey were insufficiently resourced to manage.
ii) Commissioning of liaison teams to only covercertain parts of the acute hospital
Another example of a lack of a shared vision, wascommissioning of liaison services to only certain parts ofthe acute hospital. This was more common in thesmaller liaison teams and was sometimes due to histor-ical reasons rather than a result of planned commission-ing. However, in some services funding had been cut,effectively de-commissioning referrals from some de-partments in the hospital. This left staff in a difficultposition, as a participant explained in relation to refer-rals from maternity services for which the team werenot commissioned to provide a service:
‘I would never turn down a maternity referral becauseof the potential risk involved…I mean you've got amother and a child, and there have been a lot of highprofile and very tragic cases of late where there's beena puerperal psychosis involved. The extra stresses on
the family with a new baby, the possible medicalproblems as well, I think it just makes it out as veryhigh-risk.’ [sB_p01]
Staff also worried, however, about the repercussions ofdoing this work, if, for example, taking a non-commis-sioned referral meant they were delayed in respondingto a patient from a commissioned department. Breach-ing the four-hour response time in emergency depart-ments was a concern because it was a key metric ofsuccess used by commissioners for some teams. Thiscaused feelings of frustration for those in those teams, asa participant reported, ‘we feel so frustrated most of thetime because we can’t do what we are trained for’.’[sA_p02].There were varied views on how liaison psychiatry ser-
vices should respond to this dilemma. One perspectivewas that liaison professionals should prioritise safety (ofpatients and staff ), regardless of formal commissioningarrangements, and take referrals they perceived as higherrisk. Clinicians linked this to their ethical obligation tohelp anyone in need. An alternative position was that li-aison services should limit themselves to what they werecommissioned to do, which was felt to avoid unneces-sary job strain. These dilemmas were not a problem forteams that were commissioned to cover the wholehospital.
iii) Lack of physical space
Several different teams reported not having enough of-fice space for supervision, meetings, and administrativework, as well as limited access to suitable rooms forassessing patients. This was practically and clinicallychallenging for liaison staff. For example, a participantdescribed having to conduct assessments in a room adja-cent to a children’s ward, with poor sound proofing, sochildren could hear loud or agitated patients in theroom. This also made it difficult to offer patientsprivacy.There was a link between the physical space made
available to liaison teams and their sense of identity.When liaison teams felt they lacked appropriate physicalspace to perform their role they sometimes felt excludedand dispirited. In contrast, when liaison teams felt ac-commodated by acute trust colleagues they reportedfeelings of integration and cohesion with acute servicescolleagues.For example, a liaison service had a dedicated team for
the assessment of people with self-harm in the emer-gency department. This team shared an office with theemergency department staff. There was a strong sugges-tion that this team felt fully integrated with their acutetrust colleagues.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 9 of 14

Physician integration within care teams and across sectorsDifferent hierarchies operated in Acute and MentalHealth Trusts. Liaison psychiatry staff typically felt thatAcute Trusts were generally more hierarchical than theirown Mental Health Trusts.
‘There is a hierarchy that exists in health andbasically the consultants over there sometimes perhapsdon't respond as well to the nurses over there as theywould respond to a consultant psychiatrist so having aconsultant psychiatrist in your team, when certainthings are going on and communication at a certainlevel is actually to an advantage of the team I think,and I think that is actually to do with the hierarchythat exists within health…Yes, I think that it exists lessin mental health but having worked in A & E for along time so a hierarchy exists … and if the consultantsays something then that is what happens.’ [sH_p04]
In Acute Hospitals, particularly EDs, liaison nursepractitioners tended to assess uncomplicated new refer-rals and develop plans independently of consultants.Practitioners only consulted a psychiatrist if they hadspecific concerns. This approach relied on liaison practi-tioners being able to act with a high degree of autonomy.It was therefore problematic for liaison nurses whentheir acute hospital colleagues were more receptive toadvice from psychiatrists.Acute Trust colleagues recognised this response to
liaison practitioners and agreed that it was, to someextent, linked to hierarchies. However, they alsohighlighted specific occasions where input from a psych-iatrist was perceived as necessary but absent, forexample, if they wanted advice on drug interactions. Inthese instances, acute referrers felt it would have savedtime if a consultant liaison psychiatrist had been able tosee and manage the case.
Attainment of goals and objectives are supported byfunding and human resource allocationMany liaison team members described rapid changes inliaison services, largely influenced by national driversand targets set out in plans to expand liaison services ona nationwide basis [4]. On the other hand, there was asense that much of this change was driven by key clin-ical specialists in particular teams, who were responsiblefor driving local expansion through direct and frequentcontact with commissioners, and aligning servicedevelopment with government targets.Liaison staff described many instances of internal
dilemmas in teams created by a need to make decisionsabout the best use of limited resources. As an example,one dilemma was between specialism and generalism.Staff expressed differing views about the extent to which
liaison practitioners should be able to specialise by ageand/or setting. Those in favour of specialisation: arguedthat different liaison professionals are more/less suitedto different types of clinical work. For example, liaisonnurses who enjoy working in the emergency departmentwere characterised as liking autonomy, positive risk-tak-ing and working at a fast pace. Those who preferredworking with older adults were characterised as liking todevelop relationships with their patients over a longerperiod of time and working at a slower pace. Those whostrongly identified with either extreme were particularlyaverse to working outside of their preferred clinical area,and expressed concern about their ability to carry outthe new role safely.
Differences in views from staff in different hospital clustersThere was little evidence of major differences in re-sponses between the different types of liaison services.More concerns about specialism were expressed inlarger services with separate components (e.g. olderadults team), in comparison to the other service types,and there also appeared to be greater confusion aboutreferral processes. However, there was remarkableconsistency across service types concerning the prob-lems or difficulties that teams described.
DiscussionThis study outlines some of the barriers to achievingintegrated physical and mental health care by liaisonmental services in the acute hospital setting. Thesebarriers are similar across the four distinctly differenttypes of liaison mental health services that are currentlyin existence in England.In general, liaison team members and hospital staff
report good personal working relationships, with a focuson patient centred care but staff report major problemswith coordinated transitions in care, referral to primary/community care services, information sharing andshared organisational goals and objectives.One of the driving purposes for the current round of
investment in England is the hope that such a move willresult in a reduction in length of stay, particularly forolder adults with physical and mental co-morbidities[4, 17–20]. This is dependent, however, upon seamlesstransitions of care between the hospital and commu-nity services, and the existence of high quality com-munity mental health services. Investment in hospitalliaison services alone, without additional investmentin crisis teams and services for the elderly withmental health problems, will risk patients being un-able to access community services because thresholdsare too high, resources are too limited, and there is afocus on gatekeeping. These factors make continuityof care challenging. Good communication with
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 10 of 14

primary care is also important as many patients seenby liaison services can be managed by their generalpractitioner (GP). Speaking directly to the GP as op-posed to written communication results in better careand patient outcomes [23].An alternative possible way to solve this problem of
bridging mental and physical healthcare is to embedmental health practitioners within physical healthcarepathways, or develop and extend liaison services to pri-mary care [2]. Such services have been tried and mayhelp some problems without fully resolving others – forexample they raise problems of scaling up, redefiningpatterns of team working, and they do not resolve thequestions related to information-sharing or the need tobalance the demands of acute rapid-response referralwork with those of slower-stream shared care in embed-ded teams.The participants we interviewed did not mention the
existence of any protocols to help clarify pathways andreferral systems, other than those used by communitypsychiatric teams which were used to set high thresholdsfor referral to these services. Acute hospital staff voicedfrustration at not knowing which service to refer to, ifthere was more than one psychiatric service within thesame hospital (e.g. an adult of working age team and anold age team). A single point of access and clearerreferral systems and protocols would help reduce someof the frustration felt by acute hospital staff.The liaison practitioners in this study reported that a
substantial amount of their time was spent in recordkeeping, limiting their ability to respond to the urgentrequirements of acute hospital staff who were used to amore rapid throughput of patients. Mental healthelectronic assessment systems have been designed in themain for patients with severe mental illness, who aremanaged by mental health staff with relatively smallcaseloads, who see their patients on a regular basis, overlong periods of time (months and years). Such systemsare inappropriate for liaison mental health teams whooperate in large volume, low contact services. It is clearlyan inefficient use of staff time if they spend twice as longrecording information about a patient as they do in face-to-face therapeutic contact with that person. Mentalhealth systems now usually involve completion of com-plex risk assessments, even though, such assessmentshave little or no predictive validity, and there is noevidence that they reduce harms associated with mentalillness [21–25].Our findings suggest that mental health recording
systems for liaison psychiatry are not fit for purpose andare severely affecting the responsiveness of teams.Liaison psychiatry electronic systems should be tailoredto meet the requirements of high volume, low intensitywork. They should not use systems that have been
designed for the assessment and long term managementof patients with severe mental illness in the communityor in-patient setting. A reduction in the time taken toelectronically record assessments is one obvious areawhere liaison services can become more efficient andeffective as it would free up staff time to have moretherapeutic time with patients, and more patients couldbe seen. As alterations to standardised information sys-tems are difficult and can potentially lead to a worseningof data transferability and efficiency, any changes shouldbe fully piloted and evaluated in a variety of centresbefore widespread introduction.There is a move in the NHS towards shared electronic
health records, and increased use of electronic devicesto record information. These initiatives are welcome butmust be accompanied by a shift away from a focus onrisk assessment to safety management, with morefocused data recording.Our findings also suggest that there needs to be a way
of sharing information across systems for liaison psych-iatry services and acute hospitals. Whilst there are genu-ine and real concerns about patient confidentiality, thismust be balanced with concerns about staff not havingaccess to important information about patients, whichmay adversely affect their welfare. Any sharing of infor-mation will need to comply with changes to the GeneralData Protection Regulation which came into force in theUK in May 2018. Separate recording systems are alsolikely to result in mistakes in medication recordingwhich again could have serious consequences. Liaisonservices which are managed by Acute Hospital Trustsmay use the acute hospital’s information system, but ifthese services are unable to access and share informationin separate mental health systems the barriers remain –just in a different place in the system.This is a complex area, but it would be helped by the
development of bespoke and standardised informationsystems for liaison psychiatry services, the developmentof which could be led by the Royal Colleges of Psych-iatry, Nursing, Medicine and Emergency Medicine. Astandardised system of recording for liaison psychiatrywould also enable easier benchmarking across servicesfor quality and performance management.There has been a national commitment by government
in England to work towards greater integration of healthand social care, with a particular focus on placing the in-dividual at the centre of change and the person aroundwhom, services should be planned [26]. The governmentdepartments of health and social care have also mergedrecently in order to pursue greater joined up care. Al-though there are many different definitions of integratedcare, most encompass the principles discussed in thispaper, including a patient focus, smooth inter and intra-professional team working and a shared vision of care.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 11 of 14

It is interesting that in the interviews with liaison andacute hospital staff, performance monitoring did notemerge as a theme, although it is considered an import-ant component of delivering effective integrated services(). It’s absence from any of the discourse during the in-terviews we carried out suggests it may require a higherprofile and greater buy-in from staff.Our findings can be summarised in diagrammatic
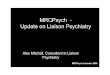
form as shown in Fig. 1. Integrated liaison servicesrequire key resources, plus an organisational structure to
deliver timely assessment and treatment, in order todeliver key outcomes (clinical or system focused).Services need to be located on site in the acute hospital,have sufficient staff and skill-mix to meet demand, andhave shared patient-focused goals within the team andwith acute hospital staff and community staff they workwith. They need to be able to record information andmonitor referral and outcome in an efficient mannerwhich is tailored to the high volume/low intensity natureof their work.
Fig. 1 Diagrammatic representation of the resources required, means to deliver outcome, and service outcomes for integrated liaison services
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 12 of 14

Strengths and limitationsThis study consisted of a relatively large sample of li-aison practitioners from services which were representa-tive of the four most common types of service inEngland at present. We deliberately sampled from thefour different service types, to ensure we obtained theviews of staff working in services of different sizes, work-ing patterns, acuity, serving different age populations,coverage of the acute hospital and acute versus lessacute care. The interviews consisted of open questionsabout services, but the themes that emerged predomin-antly concerned factors related to integration of teamswithin the hospitals in which they worked. The advan-tage of organising the themes according to the domainsdescribed by Suter and colleagues is that all thesedomains have to a greater or lesser degree tools that canbe used to measure performance [10]. Thus, many of theconcerns raised by staff in qualitative interviews can beobjectively measured in future work.Out of the 168 liaison services we initially approached,
only 13 actually sent representatives to the initiationworkshops we set up. It is possible therefore that theservices from which we sampled were different in someway to those who declined to participate or did not re-spond to our invitation. It is possible that teams whoagreed to participate in the current study are high func-tioning services who are open to scrutiny, in which caseour findings may under-estimate problems and difficul-ties in liaison services. Equally, it can be argued thatservices facing a high degree of problems and difficultieswished to participate in order to secure a platform fortheir discontent, in which case our findings may over-es-timate problems in liaison services in England.We interviewed a relatively smaller number of acute
hospital staff than liaison staff, and the hospital staff thatwere interviewed were sourced by the liaison teams. It ispossible therefore that the teams identified hospital staffwith a favourable attitude to liaison services, and againour findings may underestimate problems and difficul-ties. Despite this, the hospital staff we interviewed, wereable to raise concerns, and spoke openly and freelyabout problem areas and difficulties with the liaisonteam, with which they interacted.Another limitation of this study, is that we did not
interview any service users about their views of liaisonservices. This is something we are planning to do in aseparate phase of LP-MAESTRO.
ConclusionLiaison mental health staff working in liaison mentalhealth services in England and acute hospital staff, work-ing in hospitals served by liaison psychiatry teams, haveidentified a series of barriers to providing integratedmental and physical health care, in several key domains
including: problems with continuity of care across thesecondary-primary interface; a lack of mental healthresources in primary care to support discharge; a lack ofshared information systems and a disproportionatelength of time spent recording information as opposedto face to face patient contact; and a lack of a sharedvision of care. There was evidence of good inter-profes-sional team working, placing the patient at the heart ofthe process, and support for the development and ex-pansion of liaison services by commissioners and otherrelevant stakeholders.
Additional file
Additional file 1: Topic Guide. Topic Guide used for clinicians in the LP-Maestro study. (DOCX 58 kb)
AbbreviationsCMHT: Community Mental Health Teams; COREQ: Consolidated criteria forreporting qualitative research; CPMS: Central Portfolio Management System;ED: Emergency Department; IAPT: Improving Access to PsychologicalTreatment; LP: Liaison Psychiatry; MUS: Medically unexplained symptoms;RAID: Rapid Assessment Interface Discharge
AcknowledgmentsThis work was supported by the efforts of S Keane, M Heneghan, S Chee, JLewis, S Jayakumar at the Royal College of Psychiatrists and the NIHR ClinicalResearch Network (CRN) Yorkshire and the Humber. JK was employed by theRoyal College of Psychiatrists at the time of the study.
Authors’ contributionsAH, JH, EG, and PT conceived of the research. AW managed the project. JK andAW undertook the interviews. CCM helped in setting up the project. JK, AW, AQand AH conducted the qualitative analyses. All authors (AH, JH, EG, PT, JK, AW,CCM, AQ) contributed to the manuscript and approved the final version.
FundingThis project was funded by the National Institute for Health Research HS&DRprogramme (project reference 13/58/08). The funding body was notinvolved in any aspect of the design, data collection, analysis andinterpretation of the data, and writing of the manuscript. The views andopinions expressed are those of the author(s) and do not necessarily reflectthose of the funder NHS or the Department of Health and Social Care.
Availability of data and materialsData is not available due to the requirement to protect the confidentiality ofthe participants.
Ethics approval and consent to participateNHS Ethical permission from the North of Scotland Research Ethics Service(REC reference: 15/NS/0025). All participants gave written informed consent.We gained formal written approval from each NHS Trust. NHS Trusts do nottypically generate new reference numbers for site level participation in astudy. Rather, they refer to a Central Portfolio Management System (CPMS)reference which they use to allocate local recruitment to the same study. ForLP-MAESTRO the CPMS ID was 18727.
Consent for publicationNot applicable. No identifiable person data is presented in the manuscript.
Competing interestsAll authors have declared no support from any organization for thesubmitted work; no financial relationships with any organizations thatmight have an interest in the submitted work in the previous threeyears, no other relationships or activities that could appear to haveinfluenced the submitted work.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 13 of 14

Author details1Department of Digital, Media, Culture and Sport, London, UK. 2ClinicalResearch Network National Coordinating Centre, National Institute of HealthResearch Clinical Research Network, Leeds, UK. 3Leeds Institute of HealthSciences, University of Leeds, Leeds, UK. 4National Inpatient Centre forPsychological Medicine, Leeds and York Partnership NHS Foundation Trust,Leeds, UK. 5College Centre for Quality Improvement, Royal College ofPsychiatrists, London, UK.
Received: 4 July 2018 Accepted: 17 July 2019
References1. Aitken P, Lloyd G, Mayou R, Bass C, Sharpe M. A history of liaison psychiatry
in the UK. BJPsych Bull. 2016;40(4):199–203.2. Bestall J, Siddiqi N, Heywood-Everett S, Freeman C, Carder P, James M, et al.
New models of care: a liaison psychiatry service for medically unexplainedsymptoms and frequent attenders in primary care. BJPsych Bull.2017;41(6):340–4.
3. Barrett JAP, Lee W. Report of the 2nd annual survey of liaison psychiatry inEngland: Royal College of Psychiatrists; 2017.
4. England NHS. Five year forward view; urgent and emergency mental healthliaison in acute hospitals (adult and older adults): supportingdocumentation for transformation funding selection. London; 2016.
5. England NHS. Treat as one: bridging the gap between mental and physicalhealthcare in general hospitals: National Confidential Enquiry into PatientOutcome and Death (NCEPOD); 2017.
6. Goodwin N, Kodner D, Smith J, Manten E. Integrated care and themanagement of chronic illness: reflections on the proceedings of the 8thannual integrated care conference 2008. Int J Integr Care. 2008;8:e51.
7. Goodwin N, Smith J, Davies A, Perry C, Rose R, Dixon A, Dixon J, Ham C.Integrated care for patients and populations: improving outcomes byworking together. London: The King’s Fund; 2012.
8. Kodner DL, Spreeuwenberg C. Integrated care: meaning, logic, applications,and implications--a discussion paper. Int J Integr Care. 2002;2:e12.
9. Suter E, Oelke NDAC, Armitage GD. Ten key principles for successful healthsystems integration. Healthcare Quarterly. 2009;13:16–23.
10. Suter E, Oelke ND, da Silva Lima MAD, Stiphout M, Janke R, Witt RR, et al.Indicators and measurement tools for health systems integration: aknowledge synthesis. Int J Integr Care. 2017;17(6):4.
11. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitativeresearch (COREQ): a 32-item checklist for interviews and focus groups.Int J Qual Health Care. 2007;19(6):349–57.
12. Smith J, Firth J. Qualitative data analysis: the framework approach. NurseRes. 2011;18(2):52–62.
13. Vedsted P, Fink P, Olesen F, Munk-Jorgensen P. Psychological distress as apredictor of frequent attendance in family practice: a cohort study.Psychosomatics. 2001;42(5):416–22.
14. England NHS. Guidance for commissioning liaison psychiatry services.London; 2014.
15. Tadros G, Salama R, Kingston P, Mustafa N, Johnson E, Pannell R, Hashmi M.Impact of an integrated rapid response psychiatric liaison team on qualityimprovement and cost savings: the Birmingham RAID model. Psychiatrist.2013;37:4–10.
16. Tadros G, Naghavi M, Wang HD, Lozano R, Davis A, Liang XF, Zhou MG, etal. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysisfor the global burden of disease study 2013. Lancet. 2015;385(9963):117–71.
17. Becker L, Hardy R, Pilling S. The Raid model of liaison psychiatry: report onthe evaluation of four pilot Services in East London. London: UCL PartnersAcademic Health Science Partnership; 2016.
18. Tadros G. Intelligent outcome measures in liaison psychiatry: essential evenif not desirable: commentary on ... A multidimensional framework forroutine outcome measurement in liaison psychiatry (FROM-LP). BJPsych Bull.2016;40(4):195–8.
19. Parsonage M, Fossey M, Tutty C. Liaison psychiatry in the modern NHS.Centre for Mental Health; 2012.
20. Parsonage MFM. Tutty C. the economic evaluation of a liaison psychiatryservice. London: Centre for Mental Health; 2011.
21. Large M. MAUDSLEY DEBATE does the emphasis on risk in psychiatry servethe interests of patients or the public? No Bmj-Brit Med J. 2013;346.
22. Large M, Smith G, Sharma S, Nielssen O, Singh SP. Systematic review andmeta-analysis of the clinical factors associated with the suicide ofpsychiatric in-patients. Acta Psychiatr Scand. 2011;124(1):18–29.
23. Troquete NA, van den Brink RH, Beintema H, Mulder T, van Os TW,Schoevers RA, et al. Risk assessment and shared care planning in out-patient forensic psychiatry: cluster randomised controlled trial. Br JPsychiatry. 2013;202(5):365–71.
24. Ryan C, Nielssen O, Paton M, Large M. Clinical decisions in psychiatry shouldnot be based on risk assessment. Australas Psychiatry. 2010;18(5):398–403.
25. Steeg S, Quinlivan L, Nowland R, Carroll R, Casey D, Clements C, et al.Accuracy of risk scales for predicting repeat self-harm and suicide: amulticentre, population-level cohort study using routine clinical data. BMCPsychiatry. 2018;18(1):113.
26. NHS England. Integrated care and support: our shared commitment.London: Department of Health and Department of care and support; 2013.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Jasmin et al. BMC Health Services Research (2019) 19:522 Page 14 of 14