Embed Size (px)
Citation preview

Journal of PathologyJ Pathol 2015; 237: 363–378Published online 19 August 2015 in Wiley Online Library(wileyonlinelibrary.com) DOI: 10.1002/path.4583
ORIGINAL PAPER
Integrated genomic and transcriptomic analysis of human brainmetastases identifies alterations of potential clinical significanceJodi M Saunus,1,2#* Michael CJ Quinn,1,2,3# Ann-Marie Patch,2,3 John V Pearson,2,3 Peter J Bailey,3,4 Katia Nones,2,3Amy E McCart Reed,1,2 David Miller,3,5 Peter J Wilson,3 Fares Al-Ejeh,2 Mythily Mariasegaram,1,2 Queenie Lau,6Teresa Withers,7 Rosalind L Jeffree,8 Lynne E Reid,1,2 Leonard Da Silva,1,9 Admire Matsika,1,10 Colleen M Niland,1,2Margaret C Cummings,1,9,10 Timothy JC Bruxner,3 Angelika N Christ,3 Ivon Harliwong,3 Senel Idrisoglu,3 SuzanneManning,3 Craig Nourse,3,4 Ehsan Nourbakhsh,3 Shivangi Wani,2,3 Matthew J Anderson,3 J Lynn Fink,3 OliverHolmes,2,3 Stephen Kazakoff,2,3 Conrad Leonard,2,3 Felicity Newell,3 Darrin Taylor,3 Nick Waddell,3 Scott Wood,2,3Qinying Xu,2,3 Karin S Kassahn,3,11,12 Vairavan Narayanan,13 Nur Aishah Taib,14,15 Soo-Hwang Teo,15,16 Yock PingChow,16 kConFab,17 Parmjit S Jat,18 Sebastian Brandner,19 Adrienne M Flanagan,20,21 Kum Kum Khanna,2 GeorgiaChenevix-Trench,2 Sean M Grimmond,3,4 Peter T Simpson,1,2,9# Nicola Waddell2,3# and Sunil R Lakhani1,9,10#
1 University of Queensland, UQ Centre for Clinical Research, Herston, Queensland, Australia2 QIMR Berghofer Medical Research Institute, Herston, Queensland, Australia3 Queensland Centre for Medical Genomics, IMB, University of Queensland, St Lucia, Queensland, Australia4 Wolfson Wohl Cancer Research Centre, Institute of Cancer Sciences, University of Glasgow, UK5 Kinghorn Centre for Clinical Genomics, Garvan Institute of Medical Research, Darlinghurst, NSW, Australia6 Pathology Queensland, Gold Coast Hospital, Southport, Queensland, Australia7 Department of Neurosurgery, Gold Coast Hospital, Southport, Queensland, Australia8 Kenneth G Jamieson Department of Neurosurgery, Royal Brisbane and Women’s Hospital, Herston, Queensland, Australia9 University of Queensland School of Medicine, Herston, Queensland, Australia10 Pathology Queensland, Royal Brisbane and Women’s Hospital, Herston, Queensland, Australia11 Genetic and Molecular Pathology, SA Pathology, Women’s and Children’s Hospital, North Adelaide, South Australia, Australia12 School of Molecular and Biomedical Science, University of Adelaide, South Australia, Australia13 Division of Neurosurgery, Department of Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia14 Breast Unit, Department of Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia15 University Malaya Cancer Research Institute, University of Malaya, Kuala Lumpur, Malaysia16 Cancer Research Initiatives Foundation, Sime Darby Medical Centre, Selangor, Malaysia17 Peter MacCallum Cancer Centre, University of Melbourne, Victoria, Australia18 Department of Neurodegenerative Disease and MRC Prion Unit, UCL Institute of Neurology, London, UK19 Division of Neuropathology and Department of Neurodegenerative Disease, UCL Institute of Neurology, London, UK20 Histopathology, Royal National Orthopaedic Hospital NHS Trust, Stanmore, UK21 University College London Cancer Institute, London, UK
*Correspondence to: JM Saunus, UQ Centre for Clinical Research, B71/918, Royal Brisbane and Women’s Hospital, Herston, Queensland 4029,Australia. E-mail: [email protected]
#These authors contributed equally to this study.
AbstractTreatment options for patients with brain metastases (BMs) have limited efficacy and the mortality rate is virtually100%. Targeted therapy is critically under-utilized, and our understanding of mechanisms underpinning metastaticoutgrowth in the brain is limited. To address these deficiencies, we investigated the genomic and transcriptomiclandscapes of 36 BMs from breast, lung, melanoma and oesophageal cancers, using DNA copy-number analysisand exome- and RNA-sequencing. The key findings were as follows. (a) Identification of novel candidates withpossible roles in BM development, including the significantly mutated genes DSC2, ST7, PIK3R1 and SMC5, andthe DNA repair, ERBB–HER signalling, axon guidance and protein kinase-A signalling pathways. (b) Mutationalsignature analysis was applied to successfully identify the primary cancer type for two BMs with unknown origins.(c) Actionable genomic alterations were identified in 31/36 BMs (86%); in one case we retrospectively identifiedERBB2 amplification representing apparent HER2 status conversion, then confirmed progressive enrichment forHER2-positivity across four consecutive metastatic deposits by IHC and SISH, resulting in the deployment ofHER2-targeted therapy for the patient. (d) In the ERBB/HER pathway, ERBB2 expression correlated with ERBB3(r2 = 0.496; p < 0.0001) and HER3 and HER4 were frequently activated in an independent cohort of 167 archivalBM from seven primary cancer types: 57.6% and 52.6% of cases were phospho-HER3Y1222 or phospho-HER4Y1162
membrane-positive, respectively. The HER3 ligands NRG1/2 were barely detectable by RNAseq, with NRG1 (8p12)genomic loss in 63.6% breast cancer-BMs, suggesting a microenvironmental source of ligand. In summary, this isthe first study to characterize the genomic landscapes of BM. The data revealed novel candidates, potential clinicalapplications for genomic profiling of resectable BMs, and highlighted the possibility of therapeutically targetingHER3, which is broadly over-expressed and activated in BMs, independent of primary site and systemic therapy.Copyright © 2015 Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

364 JM Saunus et al
Keywords: brain metastasis; exome sequencing; RNA sequencing; genomic signature; targeted therapy; HER2; HER3
Received 6 May 2015; Revised 26 June 2015; Accepted 1 July 2015
No conflicts of interest were declared.
Introduction
The management of brain metastases (BMs) is a crit-ical area of unmet need [1] affecting over 100 000cancer patients annually in the USA at a cost of morethan US$ 3 billion, largely for palliative care [2,3].The incidence varies between primary cancer types(10–40% overall), being highest for lung, breast,renal cancers and melanoma [4,5]. Breast cancerpatients with triple-negative, basal-like, claudin-lowand HER2-positive (mostly ERBB2-amplified) tumoursare at highest risk of brain relapse [6–9]. Currentmanagement strategies (surgery and whole-brain orstereotactic radiotherapy) are associated with neuro-logical side-effects, are not curative and are limited topatients with one or a few small lesions [10–12]. Evenwith aggressive treatment, survival is often< 12 months[13,14]. The incidence of BMs is increasing due tomore effective treatments for systemic (extracranial)disease, sophisticated surveillance imaging modalitiesand population ageing [15].
Current data suggest that metastases originate fromclonal cell subpopulations within genetically and phe-notypically heterogeneous primary tumours [16–18].The physiological requirements can be conceptuallysummarized in a model comprising initiation (invasionand dissemination via blood/lymphatics), progres-sion (survival, extravasation) and organ colonization[19]. Colonization of the brain is a very inefficientprocess. Cells must actively cross the specializedblood-brain-barrier (BBB), and mouse models suggestthat there is huge attrition of cells that initially infil-trate this foreign microenvironment [20]. Those thatsuccessfully evade local defences adhere to the outsidesof capillaries, proliferate to form a micrometastaticsheath and may track along the vessels to facilitatespread [20,21]. Vascular co-option remains importantin larger BMs, although angiogenesis is also involvedin sustaining increasing metabolic requirements, andthe relative contributions of these mechanisms mayvary according to primary tumour type [22]. The BMmicroenvironment is complex, comprising neurons andneural progenitor cells, tumour-associated parenchymalcells (eg reactive astrocytes, endothelia, microglia),perivascular niches and heterogeneously distributedareas of oedema, hypoxia and necrosis. Several studieshave highlighted the role of this unique milieu in drivingthe speciation of cancer cells in the brain [23–26] andin therapeutic resistance [22,27].
BMs are not routinely resected and so the availabil-ity of clinical samples for research has been limited.Most research has been based on archival formalin-fixed
samples, primary tumour datasets with brain relapse dataor experimental models. These approaches have impli-cated several mechanisms in the development of BMs,eg p53, Wnt–TCF, HB–EGF, COX2, BMP-2, src, ser-pins and cathepsin-S [21,24,26,28–31]. However, theclinical relevance of many existing candidates is notfully understood. Detailed molecular analysis of humantumours could help address this deficiency and alsohighlight opportunities for drug repositioning, identifynew targets and improve our understanding of the natu-ral history.
The ERBB/HER pathway has also been implicatedin BM development, particularly the tyrosine kinasereceptors EGFR, HER2 and HER3 [7,29,32–35]. Thesereceptors engage in ligand-induced dimerization, acti-vating downstream signalling through the PI3K–AKT,PLCγ–PKC, STAT and Ras–MAPK pathways. Themost potent oncogenic unit is the HER2–HER3 het-erodimer [36]. HER2 is an orphan receptor. HER3 hasdiminished tyrosine kinase activity and is thought to beindispensable in breast tumours driven by ERBB2 ampli-fication [37]. Upon binding extracellular neuregulin lig-ands (NRG1 or NRG2), HER3 allosterically activatesother receptors, mainly HER2 and, to a lesser extent,EGFR and HER4 [36,38–40]. Recent evidence sug-gests that HER3 may be capable of homodimeric sig-nalling provided there is sufficient HER2 expression toinitiate the accumulation of signalling-competent HER3homodimers [41].
Cancer genome sequencing projects that cataloguegenomic alterations are beginning to shed light on muta-tional processes, identify genomic drivers and demon-strate the full extent of heterogeneity in cancer [42,43].These data provide a foundation for pharmacogenomicsresearch and precision medicine. Although brain relapseaccounts for the highest rates of cancer-related morbid-ity and mortality and molecular-targeted therapies arecritically under-utilized for established BMs, very fewstudies have comprehensively catalogued and analysedmetastatic brain tumour genomes.
BMs often develop in patients who have receivedprior treatment for systemic and/or primary disease(eg cytotoxic chemotherapy, molecular-targeted ther-apy). In order to survey the spectrum of genomicalterations in these highly refractory tumours, despitedifferences in their genomic and physiological evolu-tion, we performed copy-number analysis, RNA andexome sequencing on a cohort of 36 BMs from primarybreast cancer, lung cancer, melanoma and oesophagealcancer. We then analysed the data to investigate aspectsof brain metastasis biology and address issues of clin-ical relevance: (a) integrated the datasets to identify
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

Integrated genomic and transcriptomic analysis of brain metastases 365
genes and pathways that were recurrently or signifi-cantly altered across the cohort; (b) explored the diag-nostic utility of genomic profiling for BMs of unknownprimary origin; (c) investigated actionable biomarkers;and (d) interrogated the datasets and used immunohis-tochemistry to investigate the ERBB/HER pathway andthe applicability of anti-HER therapies for the treatmentof established BMs.
Methods
Brain metastases (BMs; n= 36) were collected andsnap-frozen within 2 h of collection. Blood sampleswere taken immediately before surgery. All patients pro-vided informed, written consent to use their samplesfor this study, which was approved by relevant humanresearch ethics committees.
A detailed description of sequencing, mutation call-ing, verification and subsequent analyses is included inthe supplementary material (see Supplementary mate-rials and methods). Briefly, BMs were macrodissectedon ice, then DNA and RNA were isolated simultane-ously. DNA copy-number alterations were identifiedusing SNP arrays (Illumina Human Omni 2.5 M) andthe GAP tool [44]. Exome sequencing of matchedBM and whole blood DNA and sequencing of BMRNA were performed using an Illumina HiSeq 2000instrument. Sequence data were mapped to a GRCh37assembly using BWA [45]. Substitutions were detectedusing qSNP [46] and GATK [47] and indels calledwith Pindel [48] (BAM files are available in the EGA;EGAS00001000722). Tumour cellularity was deter-mined using qpure [49]. Non-synonymous mutationswere analysed using IntOGen-mutations [50] and Mut-Sig [43] tools. Pathway analysis was conducted usingIngenuity® Pathway Assist.
For the HER/ERBB pathway, formalin-fixed,paraffin-embedded (FFPE) BMs (n= 167) were sampledin tissue microarrays, then analysed for expression ofphosphorylated HER receptors by immunohistochem-istry (IHC; see supplementary material, Supplementarymaterials and methods).
Results
Genomic landscape of human brain metastasesThirty-six fresh-frozen BMs (11 breast, 18 lung,six melanoma and one of oesophageal cancer ori-gin; Table 1) were subjected to DNA copy-numberanalysis and exome and RNA sequencing. Globally,copy-number alterations in BMs were typically ofthe respective primary tumour types (Figure 1; seealso supplementary material, Figures S1–S3, TablesS1–S5) [51–53]. For example, ER+ breast-BMs exhib-ited less complexity than HER2/ER− cases [54,55].Copy-number changes in lung-BMs were variable,
while melanoma-BM genomes were relatively silentin terms of copy-number aberrations. Using the Gis-tic tool, we identified 339 significantly amplifiedregions (including EPCAM, JAK2, HRAS, KRAS andFOXA1) and 59 significantly lost regions, includingNRG1, CDKN1B, TP53 and PTEN (see supplementarymaterial, Figure S3).
We identified 22 754 somatic single-nucleotide vari-ants (SNVs) and small insertion–deletions (indels;see supplementary material, Tables S6–S8), of which16 785 were non-synonymous mutations affecting 8305genes [46–48,56]. Somatic mutation burden variessubstantially between different cancers. Generally,haematological and childhood cancers have the lowestmutation rates, whereas those linked to chronic mutagenexposure (eg UV light and smoking) have the highest[42,43]. Consistent with this, melanoma-BMs har-boured the most coding mutations [average 1906 (range688–3283/case)], followed by lung-BMs [average491 (range 101–921)/case] and breast-BMs [aver-age 210 (range 33–822)/case] (Figure 2A; see alsosupplementary material, Table S6).
Identification of candidate genes associatedwith brain metastasisKnown mutated drivers of primary breast, melanomaand lung cancers were frequently mutated in BMs.For example, TP53 was mutated in 25/36 cases andPIK3CA was mutated or amplified in 16/36 cases[17,51,52,57,58] (Figure 2A). KRAS and BRAF weremutated in 11/18 lung-BMs and 3/6 melanoma-BMs,respectively [52,57]. CDKN2A (p16) was lost, withbarely detectable expression [mean 1.79 transcriptcounts/million (cpm)] in 6/6 melanoma-BMs (seesupplementary material, Figures S4–S6, Table S9).Twenty-six genes were significantly mutated accordingto IntOGen-mutations analysis [50], which ranks genesaccording to the predicted functional consequences ofmutations they harbour. These included TP53, KRASand DSC2 (p< 1E-09, p= 2.16E-09, p= 3.52E-09and 2.49E-07, respectively; see supplementary mate-rial, Table S10). DSC2 encodes desmocollin 2, acalcium-dependent cadherin superfamily memberinvolved in epithelial desmosome formation. Six ofthe 26 genes were significantly mutated accordingto the MutSig tool [43], which predicts significancebased on the background mutation rate of each gene:TP53, KRAS, ST7 (tumour suppressor gene [59]),PIK3R1 (PIK3CA regulatory subunit), SMC5 (DNAdouble-strand break repair [60]) and NRAS (p< 0.05).
We also investigated primary cancer type-specificmutations in breast-, lung- and melanoma-BMs, usinga variety of criteria including mutation frequency,gene size, ratio of synonymous:non-synonymous muta-tions and their predicted functional consequences (seesupplementary material, Table S11). Some genes weremutated substantially more frequently in BMs comparedto unmatched primary cancers (TCGA and COSMICdatasets), and therefore may warrant targeted analysis in
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

366 JM Saunus et al
Tabl
e1.
Basi
ccl
inic
alin
form
atio
nfo
rthe
sam
ple
coho
rtER
aH
ER2a
Age
(yea
rs)
Aliv
ePr
ogre
ssio
n(y
ears
)
Sam
ple
IDPr
imar
yty
peP
BMP
BMH
isto
logi
calt
ype
Cellu
larit
ybSe
xP
surg
BMsu
rgDe
ath
Age
(yea
rs)
Surv
ival
afte
rBM
rese
ctio
nP→
BMP→
deat
hBM
→de
ath
Q03
0Br
east
––
++
IDC
56.7
1F
50.0
051
.00
NA
NA
0.99
Q34
9Br
east
++
––
IDC
90.4
9F
49.8
750
.56
55.4
84.
920.
69Q
452
Brea
st–
–+
+ID
C49
.40
F34
.00
35.7
536
.29
1.75
2.28
0.54
Q63
5Br
east
–+
++
IDC
84.2
1F
61.3
866
.18
70.5
94.
424.
79Q
639#
Brea
stN
A–
NA
–ID
C91
.87
FN
A42
.55
45.2
52.
71N
AQ
678
Brea
st+
++
–ID
C58
.50
F38
.52
39.9
043
.99
4.09
1.38
Q75
1Br
east
++
NA
–ID
C96
.05
F49
.02
74.8
775
.14
25.8
526
.12
0.27
Q77
2Br
east
––
––
IDC
90.1
4F
51.2
853
.03
53.9
01.
752.
620.
87Q
851#
Brea
st+
+–
+ID
C84
.50
F37
.91
40.8
343
.30
3.93
2.92
Q89
6Br
east
––
++
IDC
84.1
5F
60.6
263
.57
65.8
02.
232.
95Q
898
Brea
st–
––
–ID
C91
.98
F53
.35
56.4
758
.66
2.19
3.12
Q63
0Lu
ngN
DN
DN
DN
DSC
C69
.24
M71
.54
72.8
877
.53
4.65
1.34
Q63
1Lu
ngN
DN
DN
DN
DAd
eno
56.3
1M
NA
55.2
555
.48
NA
NA
0.22
Q63
3Lu
ngN
DN
DN
DN
DLC
C*39
.55
FN
A64
.81
69.3
64.
55N
AQ
634
Lung
ND
ND
ND
ND
Aden
o*70
.56
MN
A55
.48
58.0
0N
AN
A2.
52Q
637
Lung
ND
ND
ND
ND
Aden
o*75
.18
MN
A65
.93
68.3
4N
AN
A2.
41Q
679
Lung
ND
ND
ND
ND
Aden
o*73
.47
FN
A65
.15
69.1
94.
05N
AQ
680
Lung
ND
ND
ND
ND
Aden
o*86
.80
FN
A61
.09
61.4
7N
AN
A0.
37Q
737
Lung
ND
ND
ND
ND
Aden
o-sq
uam
80.4
7M
62.5
363
.83
66.0
81.
303.
552.
25Q
739
Lung
ND
ND
ND
ND
LCC
79.8
9F
NA
59.7
260
.42
NA
NA
0.70
Q74
0Lu
ngN
DN
DN
DN
DAd
eno
70.6
3M
54.2
855
.68
59.4
63.
781.
41Q
744
Lung
ND
ND
ND
ND
SCC*
90.7
2M
NA
55.4
459
.03
3.59
NA
Q74
7Lu
ngN
DN
DN
DN
DAd
eno*
83.3
5M
42.2
641
.86
45.3
33.
470.
40Q
755
Lung
ND
ND
ND
ND
Aden
o94
.27
M67
.61
71.4
273
.52
3.82
5.91
2.09
Q75
6Lu
ngN
DN
DN
DN
DAd
eno
81.9
1M
53.2
655
.34
55.8
22.
082.
570.
48Q
757
Lung
ND
ND
ND
ND
Aden
o85
.85
F72
.52
78.5
281
.75
3.22
6.00
Q77
4Lu
ngN
DN
DN
DN
DAd
eno-
squa
m80
.93
M51
.88
51.9
153
.35
0.03
1.47
1.44
Q78
2Lu
ngN
DN
DN
DN
DAd
eno
88.4
6M
66.6
966
.70
69.7
13.
010.
01Q
822
Lung
ND
ND
ND
ND
Aden
o*87
.31
M63
.85
63.9
264
.01
0.08
0.16
0.08
Q17
8M
elan
oma
ND
ND
ND
ND
82.2
1M
57.3
459
.82
60.8
82.
483.
541.
05Q
735
Mel
anom
aN
DN
DN
DN
D78
.13
M46
.78
49.4
050
.93
2.62
4.16
1.53
Q74
1M
elan
oma
ND
ND
ND
ND
77.4
1F
NA
61.5
465
.28
3.75
NA
Q74
3M
elan
oma
ND
ND
ND
ND
95.1
1M
NA
34.5
738
.18
3.61
NA
Q74
6M
elan
oma
ND
ND
ND
ND
70.4
1M
67.3
974
.17
76.1
41.
976.
78Q
750
Mel
anom
aN
DN
DN
DN
D34
.00
MN
A66
.47
66.4
9N
AN
A0.
02Q
734
Oes
ND
ND
ND
+Ad
eno
80.2
6M
46.8
848
.51
49.5
81.
622.
701.
08Av
erag
e77
.51
54.6
257
.62
59.3
960
.78
3.56
3.17
5.01
SD15
.19
10.7
511
.21
9.52
13.1
40.
875.
147.
16
a Bio
mar
kers
tatu
sfo
rbre
asts
ampl
esw
asob
tain
edfr
omcl
inic
aldi
agno
stic
path
olog
yre
port
s:ER
stat
usw
asas
sess
edby
imm
unoh
isto
chem
istr
y(+
,≥1%
tum
ourc
ells
stai
ned)
;HER
2st
atus
dete
rmin
edby
chro
mog
enic
insi
tuhy
brid
izat
ion
(CIS
H).
b Cel
lula
rity
was
dete
rmin
edus
ing
the
qPuR
Eto
ol[4
9].
* His
tolo
gica
ltyp
ede
rived
from
the
met
asta
ticbr
ain
lesi
on(a
llot
hers
from
prim
ary
tum
oura
naly
sis)
.#Sa
mpl
esha
rbou
rpat
hoge
nic
germ
line
BRCA
1m
utat
ions
:Q63
9(B
RCA1
c.43
27C>
T(p
.Arg
1443
X))a
ndQ
851
(BRC
A1c.
5278
-del
(exo
n21_
24de
l).+
,pos
itive
;−,n
egat
ive;
BM,b
rain
met
asta
sis;
Aden
o,ad
enoc
arci
nom
a;Ad
eno-
squa
m,m
ixed
aden
o-sq
uam
ous
carc
inom
a;ER
,oes
trog
enre
cept
or;H
ER2,
hum
anep
ider
mal
grow
thfa
ctor
rece
ptor
2;ID
C,in
vasi
vedu
ctal
carc
inom
a;LC
C,la
rge
cell
carc
inom
a;N
A,no
tav
aila
ble;
ND,
not
dete
rmin
ed;P
,prim
ary;
SCC,
squa
mou
sce
llca
rcin
oma;
surg
,sur
gery
.
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

Integrated genomic and transcriptomic analysis of brain metastases 367
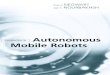
Figure 1. Copy-number landscape of brain metastases (BMs). The heat map summarizes Gistic 2.0 analysis of copy-number losses (blue),gains (red) and diploid states (white); colour intensity is proportional to peak amplitude (see supplementary material, Tables S2–5). Samplesare grouped according to primary cancer type: breast, lung, melanoma and oesophageal (E). (Lower panel) Sample codes and ER/HER2 statusfor breast-BM; black fill, positive; grey fill, negative; no fill, information not available; P, primary tumour; BM, brain metastasis; data weretaken from clinical diagnostic pathology reports for primary breast tumours. For BMs, ER status was from clinical reports and HER2 statuswas extracted from SNP-array data (GAP score≥ 6). All breast cases were invasive ductal carcinomas (IDCs); *Q639 and Q851 harbouredgermline BRCA1 mutations (Table 1)
matched BM and primary tumour samples to investigateclonal enrichment. For example, COL5A1 and MAP3K4were frequently mutated in breast-BMs (68- and 34-foldenrichment, p= 7E-05 and 2.39E-04, respectively; seesupplementary material, Table S11). The ITPR1 genewas also in this category (17-fold enrichment; 3/3assessable mutations predicted to be deleterious).Interestingly, ITPR1 expression is inversely associatedwith metastasis to the brain, but not to other sitesin breast cancer (HR> 4.0, p< 0.05; see supplemen-tary material, Figure S8) [29,61]. ITPR1 encodes theintracellular receptor for inositol 1,4,5-trisphosphate
and is involved in intracellular calcium signalling,including endoplasmic reticulum stress-induced apop-tosis. RNAseq analysis showed that mutant alleleexpression was generally undetectable or very lowfor all the aforementioned candidate BM genes (seesupplementary material, Figure S6, Table S7).
Identification of candidate pathways associatedwith brain metastasesTo identify gene networks that are recurrently alteredin BM, we performed canonical pathways analysis of
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

368 JM Saunus et al
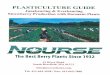
Figure 2. (A) Mutation frequencies and integrated genomic analy-sis of key genes in brain metastases. Upper panel: overall mutationfrequencies for the 36 BM (single nucleotide variants (SNVs) andsmall insertion/deletions (indels)). The matrix shows SNVs, indelsand copy-number alterations affecting key cancer genes, novelcandidate genes (see supplementary material, Tables S10, S11), coremembers of the Axon guidance and ERBB/HER signalling pathways.The histogram on the right shows the proportions of different alter-ations and the total numbers of samples harbouring alterations ineach gene. (B) Mutational signatures in human brain metastasescan be indicative of primary cancer of origin. The histograms displaySNV transition/transversion rates (upper), and relative proportionsof four mutational signatures identified in the dataset (lower). ForQ739 and Q631 (red), primary cancer types were unknown at thetime of sample collection/sequencing. They were predicted to belung cancer-derived based on smoking signature-dominated muta-tion profiles, confirmed by sourcing additional clinical information.*Germline BRCA1 mutation. Lower panels denote ER/HER2 statusfor primary breast (P) and metastatic brain (BM) tumours
mutated and integrated genomic driver genes (thosefor which copy-number alteration was correlated withabsolute expression across the cohort) (see supplemen-tary material, Tables S12, S13). Of the 46 pathwaysover-represented in this dataset, the most significantlyaltered was ‘axonal guidance signalling’, which isinvolved in actin cytoskeleton reorganization in responseto migratory guidance cues (p= 2.19E-05; Figure 2A;see also supplementary material, Figures S5–S6, TableS12). It includes Slit-Robo, Netrin, Semaphorin andEphrin signalling, which have diverse functions duringdevelopment, in normal tissues and cancer [62–64].‘Protein Kinase A signalling’ and ‘role of NFAT incardiac hypertrophy’ (including calcium–calcineurinsignalling-regulated processes) were also significantlyaltered (p= 3.24E-04 and 1.66E-03, respectively).Seventeen networks were over-represented upon inte-gration with expression data but not when mutated,and copy-number-altered genes were analysed inde-pendently (see supplementary material, Table S12),suggesting key roles for integrated genomic driversin these pathways. Interestingly, this included HER2-and GABA-receptor signalling and DNA double-strandbreak repair, which have previously been associatedwith BM development [25,65].
Clinical applications for genomic profilingBMs are not routinely biopsied in current clinical prac-tice, nor are molecular targeted therapies used as stan-dard treatment for established BMs. However, movingtowards more personalized models of cancer treatment,we will be faced with the challenge of adapting thesepractices to offer patients the most appropriate and effec-tive care [66,67]. We therefore applied the BM genomicdata to explore several clinically relevant scenarios:
• Diagnostic utility for cancers of unknown primary(CUP). According to information available at the timeof sample collection and sequencing, the primarycancer of origin was unknown for Q631 and Q739.Based on the idea that patterns of somatic mutationcan mark underlying mutagenic mechanisms in can-cer [42,43,52,68,69], we applied mutational signatureanalysis to predict the primary type for these sam-ples [42]. This revealed signatures associated withsmoking, UV exposure, APOBEC activity and ageing(Figure 2B; see also supplementary material, FigureS7); 50–90% of mutations in lung cases were con-sistent with the smoking signature, whereas >90%of melanoma-BM SNVs comprised the UV signa-ture. The smoking signature contributed the majorityof mutations harboured by Q631 and Q739 (80 and73.6%, respectively), suggesting that the primary siteof origin was lung cancer, which was later confirmedafter sourcing additional clinical information (exter-nal radiology and treatment data).
• Actionable genomic alterations. We investigatedmutation and copy-number-driven expressionfor a panel of predictive genomic markers [67],
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

Integrated genomic and transcriptomic analysis of brain metastases 369
Table 2. Potentially actionable genomic alterations in brain metastasesGene No. cases Alteration Breast-BM Lung-BM Mel-BM Oes-BM Drugs Reference
KRAS 8 Amp Q755, Q822 MEK/PI3K/mTORic
p.G12V Q631 (68.32),Q782 (79.59)
MEKia, PI3K/mTORib [110,111]
p.G12C Q757 (62.83)p.G13C Q747 (89.01)p.G13D Q756 (91.36)p.Q61H Q739 (67.15)
PIK3CA 8 Amp Q851 Q630, Q634,Q637, Q822
PI3K/AKT/mTORia [112]
p.H1047R Q678 (25.64),Q751 (64.29),Q896 (63.64)
CDKN2A 7 CN-loss Q737*, Q631 Q178*, Q741*,Q743*, Q746,Q750
CDKic [113]
ERBB2 6 Amp Q452d, Q030,Q896, Q635,Q851
Q734# ERBB2ia
NRAS 5 Amp Q734# PI3K/RAF/MEKic
p.Q61L Q740 (48.84) MEK162a [114]p.Q61R Q774 (89.31) Q750 (74.71)p.Q61K Q741 (89.36)
CDK6 2 Amp Q756 Q734# CDKic
EGFR 2 Amp Q744, Q737 EGFRia
MET 2 Amp Q680, Q756 Crizotinibb [115]PTEN 2 CN-loss Q639, Q772* PI3K/AKT/mTORib [116]AKT1 1 Amp Q756 AKT/mTORic
AKT3 1 Amp Q851 AKT/mTORic
AURKA 1 Amp Q755 CDK/AURKAic
BRCA1 1 CN-loss Q639* PARPia [117]CCND1 1 Amp Q734# CDKic
CDK4 1 Amp Q782 CDKic
HRAS 1 Amp Q678 PI3K/RAF/MEKic
KIT 1 p.L572P Q746 (99.39) KITi eg imatinibc
MEK1 1 Amp Q737 PI3K/RAF/MEKic
Analysis of these actionable genes is intended to exemplify possible opportunities for genotype-directed therapy, but is not exhaustive. A three-category system wasused to classify alterations based on the evidence linking genotypes to drug efficacy [118]:aStrong clinical evidence supporting the efficacy of a drug based on tumour genotype.bCompelling preclinical evidence for efficacy of a drug based on tumour genotype.cWhere a drug could be deployed based on a known gene-drug relationship, but where there is currently limited or inconclusive evidence supporting the efficacy ofthat drug in the context of the observed tumour genotype.For copy-number alterations, only those associated with corresponding over-/under-expression were included (expression in first/fourth quartiles for CN loss/gain,respectively, in BM of the same primary type, and/or <2 counts/million.*Homozygous loss.#For amplified genes in Q734, over-expression was defined as nCPM in the fourth quartile of expression for all other primary types.dFor Q452, RNAseq data was not available but ERBB2 amplification was retained, as this currently qualifies cancer patients for HER2-targeted therapy. Variant alleleexpression frequency is indicated in parentheses for actionable hotspot mutations.Amp, genomic amplification; CN, copy-number; mel, melanoma; oes, oesophageal.
identifying alterations with published evidence of agenotype-drug efficacy relationship in 31/36 (86%)cases, including 25 with supportive clinical evidence(Table 2). This analysis exemplifies potential thera-peutic opportunities identified by genomic profilingof resected BMs.
• Limited therapeutic options due to no/limited diag-nostic information available for the primary tumour.Two breast-BMs were in this category: for Q751,the patient was treated for primary breast cancerabroad in 1986; and for Q639, the patient presentedwith lymph node metastases and, despite thoroughdiagnostic analysis of her bilateral mastectomy tissue,the primary tumour could not be located. This patientwas a germline BRCA1 mutation carrier and thehistopathology was consistent with metastatic breast
cancer. In both cases, we identified therapeutic oppor-tunities: Q751 harboured an activating mutation inPIK3CA (p.H1047R) and Q639 harboured genomicloss/suppression of PTEN, both associated withsensitivity to PI3K/AKT/mTOR pathway inhibitors(Table 2).
• Discordance in expression of key prognostic/predictive biomarkers between primary andmetastatic disease. We identified an ERBB2-amplifiedBM (Q851); however, the matching primary breastcancer was clinically classified as HER2-negativearound 4 years earlier, based on IHC and SISH anal-ysis of a core biopsy (the only diagnostic specimenavailable as the patient was treated with chemo-and hormone-therapy in the neo-adjuvant setting).The patient had four distant relapses over 5 years
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

370 JM Saunus et al
�4 �20 �40
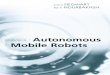
Figure 3. Case demonstrating enrichment for HER2 expression and selection of ERBB2-amplified clone(s) in brain metastases. SNP-arrayanalysis identified discordant HER2 status for sample Q851, an ERBB2-amplified BM that originated from HER2-negative breast cancer.The patient had four distant relapses over five years (one liver lesion and three BM). Retrospective immunohistochemical (IHC) andsilver in situ hybridization (SISH) analysis of all diagnostic specimens revealed progressive enrichment for HER2 expression in themetastatic deposits, with a corresponding increase in the average number of ERBB2 copies/cell over time. The figure shows the relevantclinical history, retrospective diagnostic (dx) HER2 data and representative HER2 IHC staining for the five samples. FEC, fluorouracil(5FU)+ epirubicin+ cyclophosphamide chemotherapy regimen; L, left; R, right; WBRT, whole-brain radiotherapy. Scale bar= 0.5 mm
(one liver lesion, three BMs), none of which wassubjected to diagnostic HER2 testing. Prompted bythe serendipitous SNP-array finding, retrospectiveHER2 IHC and SISH analysis were performedon all five diagnostic specimens, and showed pro-gressive enrichment for ERBB2 amplification andexpression. The patient was subsequently offeredHER2-targeted treatment, beginning with lapa-tinib/capecitabine therapy which had clinical activity
against treatment-naïve BMs in a phase II trial [70](Figure 3). The patient is currently alive and stablewith metastatic disease.
Expression and activation of the actionable HERpathway in brain metastasesThere is a growing body of literature implicating theERBB/HER pathway activation in development of BMs
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

Integrated genomic and transcriptomic analysis of brain metastases 371
Figure 4. Expression of ERBB receptors and HER3 ligands in brain metastases. (A) ERBB absolute expression (normalized counts/million,nCPM) for each sample. ERBB3 was expressed in the top 95th percentile of all genes for breast-, melanoma- and oesophageal-BM, and wasalso highly expressed in lung-BM (outliers by inter-quartile range criteria; Figure S4A). (B) Absolute levels of ERBB2 and ERBB3 transcriptswere significantly associated by both linear regression (r2 = 0.4955, p< 0.0001) and Spearman correlation analysis (r= 0.432; p= 0.014). (C)nCPM values for the HER3 ligands NRG1 and NRG2. Boxes and whiskers show the median, quartiles and the range of expression respectively
[29,32,33,35]. Therefore, taking a candidate approach,we analysed mutation, copy-number and expressionof key ERBB/HER pathway members (Figure 2A; seealso supplementary material, Figures S5, S6, S9, S10).PIK3CA was altered in 17 samples, including fivecases with amplification-associated over-expressionand three cases with the known hot-spot mutationH1047R (Table 2: see also supplementary material,Figure S9). Consistent with previous reports [71,72],we observed copy-number loss affecting PTEN in 5/11breast-BMs (associated with very low expression inthe two triple-negative cases; Table 2). Each of thefour ERBB genes was amplified in at least one case.For EGFR and ERBB2, copy-number correlated withexpression across the cohort (p< 0.0001; Figure S9).ERBB2 transcripts were abundantly expressed in lung-and breast-BMs (outliers by interquartile range criteria;Figure 4; see also supplementary material, Figure S4A),whereas expression of EGFR and ERBB4 was variableacross primary cancer types. Of the four receptors,ERBB3 was the most highly and consistently expressedacross different primary tumour types (Figure 4A)and, whilst its expression was not associated withcopy-number (see supplementary material, Figure S9),ERBB3 transcript abundance correlated with its onco-genic partner ERBB2, even in non-ERBB2-amplifiedtumours (p< 0.0001; Figure 4B).
Regarding the receptor ligands, we observed recur-rent loss at 8p12 affecting the HER3 ligand NRG1 in7/11 breast-BMs, including all five ERBB2-amplifiedcases (Figure 2A). Irrespective of copy-number, expres-sion of NRG1 and NRG2 was very low across the cohort(<1.0 cpm in 9/32 cases; Figure 4C), suggesting thatHER3-positive tumour cells are more likely to sourceligands from the neuregulin-rich brain microenviron-ment [73] than from within the tumour itself. In contrast,EGFR and HER4 ligands were variably expressed, gen-erally being highest in lung-BMs (see supplementarymaterial, Figure S10).
To investigate how these findings relate to pathwayactivation, we used immunohistochemistry (IHC) toanalyse phosphorylated HER isoforms in an indepen-dent cohort of 167 archival BMs originating from breast,melanoma, lung, colorectal, prostate, ovarian and renalcancers. Overall, the most ubiquitously activated recep-tors were HER3 and HER4, with strong complete mem-brane staining in 57.7% and 52.6% cases, respectively(Figure 5; see also supplementary material, Figures S11,S12). Since HER3 activity can be inhibited indirectlywith clinically approved HER2-targeted agents (eg lap-atinib, trastuzumab, pertuzumab), we determined theHER2 status of the archival BMs according to clinicaldiagnostic criteria (see supplementary material, FiguresS11, S12). 76.7% of HER2-positive cases showed strong
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

372 JM Saunus et al
Figure 5. Analysis of HER activation in brain metastases from different primary cancers-of-origin. Tissue microarrays containing BM samples(n= 167 in duplicate) were stained with specific antibodies targeting pEGFR (Y1068), pHER2 (Y1221/1222), pHER3 (Y1222) and pHER4 (Y1162).(A) Representative staining of the antigens indicated (primary tumour type and score in parentheses); bv, blood vessel; n, necrosis. (B)Overall phospho-HER activation frequencies. (C) Case-by-case summary of HER activation according to origin of primary cancer. Stronglymembrane-positive cases (score 3–4) are indicated with purple tiles. HER2 status was also assessed by IHC using diagnostic criteria (HER2dx)with HER2-positive cases shown in dark blue. Light blue tiles indicate cases with any phospho-HER2-positivity (>0). The number (n) of BMsanalysed is indicated for each primary cancer type; Colo, colorectal; O, ovarian; P, prostate
HER3 activation, although HER3 was also frequentlyactivated in HER2-negative cases (only 34.7% of theHER3-activated cases were HER2-positive; Figure 5C).Of HER3-activated cases, 82.1% showed some degreeof HER2 activation. Collectively these data provide sup-port to the applicability of HER2/3-targeted therapies forthe management of BMs.
Discussion
A diagnosis of metastatic brain disease marks a seri-ous physiological and psychological downturn for
cancer patients. The current mainstays of treatment arewhole-brain or stereotactic radiotherapy and/or surgicalexcision. After treatment the outcome remains poor,highlighting an urgent need for new therapeutic options.Clinical data on the efficacy of targeted therapies againstestablished BMs is limited, due to an historical lackof prospective studies in this setting, although thistrend is beginning to change, with several agents nowbeing assessed in phase I/II clinical trials [22,70,74].Therefore, notwithstanding the challenges (eg vari-ability in intratumoural perfusion and drug uptake,development of resistance [1,75,76]), preclinical and
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

Integrated genomic and transcriptomic analysis of brain metastases 373
early clinical studies with targeted agents are providingan optimistic outlook [22]. Diagnostic genomic profil-ing of resected BMs could be used to rationalize theselection of patients for clinical trials and identify newtreatment options for patients in the future.
This is the first study to apply genomic and tran-scriptomic profiling to a cohort of BMs. Globally,they were more similar than different to the respec-tive primary tumour types, consistent with previousreports [16,17,77–80]. However, differences were alsoidentified that could provide insight into BM develop-ment with further analysis. BMs are complex tumourswith diverse aetiologies, and so tumour cell-intrinsicmechanisms contributing to their growth are likelyto be highly variable. Conversely, studies demon-strating BM exploitation of neural growth pathways[23–25,76,81] raise the possibility that convergence ofdiverse metastatic entities in common soil may underpinrecurrent, targetable features [22]. We explored this byinterrogating genomic and transcriptomic data fromBM of different origins. As the cohort sizes were lim-ited, we applied multiple filters to prioritize genes andpathways of interest. Analysis of mutation significanceand frequency highlighted new candidates, includingDSC2, ST7, PIK3R1, SMC5, COL5A1, MAP3K4 andITPR1. The repertoire of alterations was enriched withfunctional gene networks, with axon guidance, proteinkinase A and calcium signalling-related processesamongst the most significant. While further investiga-tion is required to establish whether these candidatesare involved in BM development, it is encouraging thatpathways previously implicated in BMs were also iden-tified in this study (eg HER2, GABA-receptor signallingand DNA double-strand break repair [25,65]).
Targeted analysis of actionable genomic alterationsidentified potential drug targets in 31/36 cases, including25 with clinical evidence supporting a genotype–drugefficacy relationship (Table 2). This was a retrospectivestudy and it is uncertain whether the genomic data wouldhave led to deployment of alternative therapeutic agentsif known at the time of BM resection, but it is possi-ble that this information may have impacted on clini-cal management in some cases (eg clinical trial eligi-bility). For example, 10 patients in this study may havebeen eligible for a phase I trametinib (MEK-inhibitor)trial for patients with established BMs from NRAS- orKRAS-mutant cancers [74].
We had the opportunity to translate a serendipi-tous finding to therapeutic intervention for one breastcancer patient, who was still alive at completion ofthe study despite multiple recurrent BMs. This caseexemplified several challenges in the managementof metastatic brain disease that are underpinned byintratumoural heterogeneity: (a) limited tumour sam-pling for diagnostic analysis (eg core biopsy); and (b)predictive biomarker discordance between primaryand metastatic disease. In this case there was progres-sive enrichment of HER2-positivity in four distantmetastases over 5 years. We hypothesize that the bulkof the primary tumour and disseminated cells at that
stage (ER/PR-positive, HER2-negative) responded tohormone- and chemotherapy, leading to outgrowth ofER/PR-negative, HER2-positive subclone(s). Indeed,others have documented an association between HER2discordance in BM and hormone therapy for pri-mary breast cancer [82]. This finding supports theASCO/CAP recommendation to perform HER2 testingof metastatic breast cancer (particularly where theprimary was HER2-negative) if all patients who maybenefit from targeted therapy are to be offered an oppor-tunity [83,84]. We concur with some authors who havesuggested inclusion of the presence of HER2 intratu-moural heterogeneity in routine breast histopathologyreporting [85–87].
There have been a number of therapeutic develop-ments targeting the HER family; for example, erlotiniband gefitinib, which target HER1/EGFR; trastuzumab,pertuzumab and T-DM1 (HER2); patritumab andMM-121 (HER3); and multi/pan-HER inhibitors suchas lapatinib, MM-111, afatinib and dacomitinib. Theextent to which HER receptors are activated in dif-ferent types of BM has not been characterized, yetthis is a critical step if HER-targeted therapies areto be considered for clinical management. Here, weshowed that both HER3 and HER4 are extensivelyactivated in BMs. The roles of HER4 isoforms arecomplex and context-dependent [88–92]. The abun-dance of membranous phospho-HER4 in human BMswarrants more detailed analysis of HER4 isoformsin relevant experimental models. HER3 has beenimplicated in microenvironment-driven tumour growth[32,33,93], brain microvascular permeabilization [34]and therapeutic resistance [37,94–98]. Its oncogenicactivity has been characterized mainly in the contextof HER2-addicted cancers, as the pair are regardedas obligate partners. However, recent data suggestthat HER2 transactivation of HER3 is not dependenton equal surface levels of these receptors, and thatHER3 homodimers are∼ three-fold more stable thanHER2-3 heterodimers [41]. We found that only 34.7%of pHER3-positive BMs were HER2-positive by clin-ical diagnostic criteria, but> 80% expressed pHER2to some degree. Therefore, targeting HER3 directlymay be a more broadly applicable strategy than indirecttargeting via HER2 dimerization inhibitors.
It is also important to consider the IHC data in thecontext of HER2-positive breast cancer. Around 50%of these patients develop BMs over time [99,100]. Thefact that adjuvant trastuzumab treatment for primary dis-ease does not alter the overall incidence of BM hascontributed to a view that the BBB prevents uptake toefficacious levels, creating a sanctuary site for metastaticcells. However, this remains to be equivocally demon-strated in human subjects and there are several linesof evidence suggesting that inefficient delivery is notsolely responsible. First, the presence of BM is oftenan exclusion criterion in clinical trials in the primarydisease setting, as patient prognosis is deemed incom-patible with many trial endpoints. Where patients withBM are included but there is minimal or no impact
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

374 JM Saunus et al
on intracranial disease progression, it is not possible toaccurately interpret efficacy against established BMs,because dose selection is critical for achieving opti-mal tumour concentration [101] and evidence suggeststhat the BM microenvironment impacts significantly onuptake of circulating drugs [1,102,103]. Second, severalPET imaging studies have now demonstrated accumula-tion of trastuzumab in HER2-positive BMs [104–106].Finally, others have recently demonstrated uptake ofT-DM1 and bevacizumab (anti-VEGFR) to therapeu-tic levels in BMs [22]. These data highlight promis-ing opportunities with mAbs and mAb conjugates (egT-DM1, radioimmunotherapy) and that it could be timeto rethink the perceived limitation imposed by the BBBon the treatment of established BMs [22].
We postulate that the neuregulin-rich brain microen-vironment also contributes to therapeutic resistancein BMs. HER2 and HER3 are induced in BMs frombreast and lung cancers [32,33,35] and our data suggestthat this is an adaptive response to paracrine ligands(see supplementary material, Figure S13), since mostBMs lacked expression of NRG RNA. Neuregulin-1mediates resistance to cisplatin therapy in mousemodels of non-small cell lung cancer [107] and thismay also be relevant in BMs, which are essentiallytreatment-refractory manifestations of cancer arising ina neuregulin-rich microenvironment. HER3 is causallyassociated with trastuzumab escape in primary breastcancer [108] and in our cohort was activated in 55%of HER2-positive breast-BMs. The incidence of BMsin HER2-positive breast cancer patients treated withtrastuzumab and docetaxel, with or without pertuzumab(a HER2–HER3 dimerization blocker), was recentlyevaluated as part of the CLEOPATRA study [109]. Inpatients with controlled extracranial disease, where thebrain was the first site of relapse, pertuzumab signif-icantly delayed the onset of BMs and, although thecohorts were small, survival also showed an encour-aging trend. These data suggest that comprehensivemechanistic blockade of the HER2–HER3 dimer couldbe beneficial for patients with established BMs fromHER2-positive breast cancer.
To our knowledge, this is the first study to character-ize the genomic landscapes of BMs. The data revealednovel candidates and potential clinical applications forgenomic profiling of resectable BMs, and highlight thepossibility of therapeutically targeting HER3, which isbroadly over-expressed and activated in BMs, indepen-dent of primary site and systemic therapy.
Acknowledgements
This study was supported by funding from the AustralianNational Health and Medical Research Council (GrantNo. APP1030751) and the National Breast CancerFoundation, Australia (a fellowship to PTS). We wouldlike to thank D Gwynne for central coordination at theQueensland Centre for Medical Genomics and Professor
Sir Mike Stratton for his support in attracting funding forthis study. We wish to thank the Wesley-St. Andrew’sResearch Institute Tissue Bank, as well as HeatherThorne, Eveline Niedermayr and all the kConFabresearch nurses and staff, and the many families whocontribute to kConFab. We would also like to acknowl-edge the Brisbane Breast Bank for coordinating samplecollection, archiving and data management, as well asall the patients who donated tissue for this study.
Author contributions
Attracted funding for the study, JMS, PTS, LDS, KKK,GC-T, MCC, NicoW and SRL; study conception, JMS,PTS and SRL; study design, MCJQ, JMS, KKK, AMR,FA-E, GC-T, SMG, PTS, NicoW and SRL; facilitatedprovision of clinical samples and information, MM,CN, QL, TW, RLJ, VN, NAT, S-HT, YPC and kConFab;processed tissue samples and extracted/qualified DNAand RNA, JMS, LR, AMR and LDS; performed librarypreparation and sequencing, DKM, TB, AC, IH, SI, SM,CN, EN and SW; sequence data management, alignmentand mutation identification, MJA, JLF, OH, CL, FN,MCJQ, DT, NickW, SW, QX, KK, SHT, YPC, NAT,kCF, PJ and KF; data analysis, MCJQ, JMS, AMP, JVP,PJB, KN, PJW, NicoW and FA-E; constructed TMAs,PJ, SB and AMF; and IHC staining and analysis, LR,JMS, AM and PTS. JMS, MCJQ, AMR, AM, SMG,PTS, NicoW and SRL wrote the manuscript and allauthors read and approved the final version.
References1. Maher EA, Mietz J, Arteaga CL, et al. Brain metastasis: oppor-
tunities in basic and translational research. Cancer Res 2009; 69:6015–6020.
2. Benjamin L, Cotte FE, Mercier F, et al. Burden of breast cancerwith brain metastasis: a French national hospital database analysis.J Med Econ 2012; 15: 493–499.
3. Nieder C, Norum J, Stemland JG, et al. Resource utilization inpatients with brain metastases managed with best supportive care,radiotherapy and/or surgical resection: a Markov analysis. Oncology
2010; 78: 348–355.4. Gavrilovic IT, Posner JB. Brain metastases: epidemiology and
pathophysiology. J Neurooncol 2005; 75: 5–14.5. Barnholtz-Sloan JS, Sloan AE, Davis FG, et al. Incidence propor-
tions of brain metastases in patients diagnosed (1973–2001) in theMetropolitan Detroit Cancer Surveillance System. J Clin Oncol
2004; 22: 2865–2872.6. Harrell JC, Prat A, Parker JS, et al. Genomic analysis identifies
unique signatures predictive of brain, lung, and liver relapse. Breast
Cancer Res Treat 2012; 132: 523–535.7. Pestalozzi BC, Zahrieh D, Price KN, et al. Identifying breast can-
cer patients at risk for CNS metastases in trials of the Interna-tional Breast Cancer Study Group (IBCSG). Ann Oncol 2006; 17:935–944.
8. Lin NU, Vanderplas A, Hughes ME, et al. Clinicopathologic fea-tures, patterns of recurrence, and survival among women withtriple-negative breast cancer in the National Comprehensive CancerNetwork. Cancer 2012; 118: 5463–5472.
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

Integrated genomic and transcriptomic analysis of brain metastases 375
9. Fulford LG, Reis-Filho JS, Ryder K, et al. Basal-like grade IIIinvasive ductal carcinoma of the breast: patterns of metastasis andlong-term survival. Breast Cancer Res 2007; 9: R4.
10. Linskey ME, Andrews DW, Asher AL, et al. The role of stereotacticradiosurgery in the management of patients with newly diagnosedbrain metastases: a systematic review and evidence-based clinicalpractice guideline. J Neurooncol 2010; 96: 45–68.
11. Claus EB. Neurosurgical management of metastases in the centralnervous system. Nat Rev Clin Oncol 2012; 9: 79–86.
12. Soffietti R, Ruda R, Trevisan E. Brain metastases: current man-agement and new developments. Curr Opin Oncol 2008; 20:676–684.
13. Stelzer KJ. Epidemiology and prognosis of brain metastases. Surg
Neurol Int 2013; 4: S192–202.14. Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr
Oncol Rep 2012; 14: 48–54.15. Frisk G, Svensson T, Backlund LM, et al. Incidence and time trends
of brain metastases admissions among breast cancer patients inSweden. Br J Cancer 2012; 106: 1850–1853.
16. Gerlinger M, Rowan AJ, Horswell S, et al. Intratumor heterogeneityand branched evolution revealed by multiregion sequencing. N Eng
J Med 2012; 366: 883–892.17. Shah SP, Morin RD, Khattra J, et al. Mutational evolution in a lob-
ular breast tumour profiled at single nucleotide resolution. Nature
2009; 461: 809–813.18. Turajlic S, Furney SJ, Lambros MB, et al. Whole genome sequenc-
ing of matched primary and metastatic acral melanomas. Genome
Res 2012; 22: 196–207.19. Chiang AC, Massague J. Molecular basis of metastasis. N Eng J
Med 2008; 359: 2814–2823.20. Kienast Y, von Baumgarten L, Fuhrmann M, et al. Real-time imag-
ing reveals the single steps of brain metastasis formation. Nat Med
2010; 16: 116–122.21. Valiente M, Obenauf AC, Jin X, et al. Serpins promote cancer cell
survival and vascular co-option in brain metastasis. Cell 2014; 156:1002–1016.
22. Kodack David P, Askoxylakis V, Ferraro Gino B, et al. Emergingstrategies for treating brain metastases from breast cancer. Cancer
Cell 2015; 27: 163–175.23. Gril B, Palmieri D, Qian Y, et al. Pazopanib inhibits the acti-
vation of PDGFRβ-expressing astrocytes in the brain metastaticmicroenvironment of breast cancer cells. Am J Pathol 2013; 182:2368–2379.
24. Neman J, Choy C, Kowolik CM, et al. Co-evolution of breast-to-brain metastasis and neural progenitor cells. Clin Exp Metast 2013;30: 753–768.
25. Neman J, Termini J, Wilczynski S, et al. Human breast cancermetastases to the brain display GABAergic properties in the neuralniche. Proc Natl Aacad Sci USA 2014; 111: 984–989.
26. Sevenich L, Bowman RL, Mason SD, et al. Analysis of tumour- andstroma-supplied proteolytic networks reveals a brain-metastasis-promoting role for cathepsin S. Nat Cell Biol 2014; 16: 876–888.
27. Fidler IJ, Balasubramanian K, Lin Q, et al. The brain microenviron-ment and metastasis. Mol Cell 2010; 30: 93–98.
28. Nguyen DX, Chiang AC, Zhang XH, et al. WNT/TCF signalingthrough LEF1 and HOXB9 mediates lung adenocarcinoma metas-tasis. Cell 2009; 138: 51–62.
29. Bos PD, Zhang XHF, Nadal C, et al. Genes that mediate breastcancer metastasis to the brain. Nature 2009; 459: 1005–1009.
30. Zhang S, Huang WC, Zhang L, et al. SRC family kinases as noveltherapeutic targets to treat breast cancer brain metastases. Cancer
Res 2013; 73: 5764–5774.31. Lo Nigro C, Vivenza D, Monteverde M, et al. High frequency of
complex TP53 mutations in CNS metastases from breast cancer. Br
J Cancer 2012; 106: 397–404.
32. Sun M, Behrens C, Feng L, et al. HER family receptor abnormalities
in lung cancer brain metastases and corresponding primary tumors.
Clin Cancer Res 2009; 15: 4829–4837.
33. Da Silva L, Simpson PT, Smart CE, et al. HER3 and downstream
pathways are involved in colonization of brain metastases from
breast cancer. Breast Cancer Res 2010; 12: R46.
34. Momeny M, Saunus JM, Marturana F, et al. Heregulin–HER3–
HER2 signaling promotes matrix metalloproteinase-dependent
blood–brain barrier transendothelial migration of human breast
cancer cell lines. Oncotarget 2015; 6: 3932–3946.
35. Duchnowska R, Sperinde J, Chenna A, et al. Quantitative HER2
and p95HER2 levels in primary breast cancers and matched brain
metastases. Neuro Oncol 2015; PMID: 25681308 (in press).
36. Lee-Hoeflich ST, Crocker L, Yao E, et al. A central role for HER3
in HER2-amplified breast cancer: implications for targeted therapy.
Cancer Res 2008; 68: 5878–5887.
37. Amin DN, Campbell MR, Moasser MM. The role of HER3, the
unpretentious member of the HER family, in cancer biology and
cancer therapeutics. Semin Cell Dev Biol 2010; 21: 944–950.
38. Campiglio M, Ali S, Knyazev PG, et al. Characteristics of EGFR
family-mediated HRG signals in human ovarian cancer. J Cell
Biochem 1999; 73: 522–532.
39. Zhang Y, Opresko L, Shankaran H, et al. HER/ErbB receptor
interactions and signaling patterns in human mammary epithelial
cells. BMC Cell Biol 2009; 10: 78.
40. Ueno Y, Sakurai H, Tsunoda S, et al. Heregulin-induced activa-
tion of ErbB3 by EGFR tyrosine kinase activity promotes tumor
growth and metastasis in melanoma cells. Int J Cancer 2008; 123:340–347.
41. Steinkamp MP, Low-Nam ST, Yang S, et al. erbB3 is an active
tyrosine kinase capable of homo- and heterointeractions. Mol Cell
Biol 2014; 34: 965–977.
42. Alexandrov LB, Nik-Zainal S, Wedge DC, et al. Signatures of
mutational processes in human cancer. Nature 2013; 500: 415–421.
43. Lawrence MS, Stojanov P, Polak P, et al. Mutational heterogeneity
in cancer and the search for new cancer-associated genes. Nature
2013; 499: 214–218.
44. Popova T, Manie E, Stoppa-Lyonnet D, et al. Genome alteration
print (GAP): a tool to visualize and mine complex cancer genomic
profiles obtained by SNP arrays. Genome Biol 2009; 10: R128.
45. Li H, Durbin R. Fast and accurate short read alignment
with Burrows–Wheeler transform. Bioinformatics 2009; 25:1754–1760.
46. Kassahn KS, Holmes O, Nones K, et al. Somatic point mutation
calling in low cellularity tumors. PLoS One 2013; 8: e74380.
47. McKenna A, Hanna M, Banks E, et al. The Genome Analysis
Toolkit: a MapReduce framework for analyzing next-generation
DNA sequencing data. Genome Res 2010; 20: 1297–1303.
48. Ye K, Schulz MH, Long Q, et al. Pindel: a pattern growth approach
to detect break points of large deletions and medium sized insertions
from paired-end short reads. Bioinformatics 2009; 25: 2865–2871.
49. Song S, Nones K, Miller D, et al. qpure: A tool to estimate tumor
cellularity from genome-wide single-nucleotide polymorphism pro-
files. PLoS One 2012; 7: e45835.
50. Gonzalez-Perez A, Perez-Llamas C, Deu-Pons J, et al.
IntOGen-mutations identifies cancer drivers across tumor types.
Nat Methods 2013; 10: 1081–1082.
51. TCGA. Cancer Genome Atlas Network: Comprehensive molecular
portraits of human breast tumours. Nature 2012; 490: 61–70.
52. Hodis E, Watson IR, Kryukov GV, et al. A landscape of driver
mutations in melanoma. Cell 2012; 150: 251–263.
53. Imielinski M, Berger AH, Hammerman PS, et al. Mapping the hall-
marks of lung adenocarcinoma with massively parallel sequencing.
Cell 2012; 150: 1107–1120.
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

376 JM Saunus et al
54. Hicks J, Krasnitz A, Lakshmi B, et al. Novel patterns of genomerearrangement and their association with survival in breast cancer.Genome Res 2006; 16: 1465–1479.
55. Chin K, DeVries S, Fridlyand J, et al. Genomic and transcriptionalaberrations linked to breast cancer pathophysiologies. Cancer Cell
2006; 10: 529–541.56. DePristo MA, Banks E, Poplin R, et al. A framework for variation
discovery and genotyping using next-generation DNA sequencingdata. Nat Genet 2011; 43: 491–498.
57. Cancer Genome Atlas Research Network: Comprehensive genomiccharacterization of squamous cell lung cancers. Nature 2012; 489:519–525.
58. Stephens PJ, Tarpey PS, Davies H, et al. The landscape of cancergenes and mutational processes in breast cancer. Nature 2012; 486:400–404.
59. Dong SM, Sidransky D. Absence of ST7 gene alterations in humancancer. Clin Cancer Res 2002; 8: 2939–2941.
60. Jeppsson K, Kanno T, Shirahige K, et al. The maintenance of chro-mosome structure: positioning and functioning of SMC complexes.Nat Rev Mol Cell Biol 2014; 15: 601–614.
61. Wang Y, Klijn JG, Zhang Y, et al. Gene-expression profiles topredict distant metastasis of lymph-node-negative primary breastcancer. Lancet 2005; 365: 671–679.
62. Biankin AV, Waddell N, Kassahn KS, et al. Pancreatic cancergenomes reveal aberrations in axon guidance pathway genes. Nature
2012; 491: 399–405.63. Grossmann AH, Yoo JH, Clancy J, et al. The small GTPase
ARF6 stimulates β-catenin transcriptional activity duringWNT5A-mediated melanoma invasion and metastasis. Sci
Signal 2013; 6: ra14.64. Schmid BC, Rezniczek GA, Fabjani G, et al. The neuronal guidance
cue Slit2 induces targeted migration and may play a role in brainmetastasis of breast cancer cells. Breast Cancer Res Treat 2007;106: 333–342.
65. Woditschka S, Evans L, Duchnowska R, et al. DNA double-strandbreak repair genes and oxidative damage in brain metastasis ofbreast cancer. J Natl Cancer Inst 2014; 106: •••–•••.
66. Koay E, Sulman EP. Management of brain metastasis: past lessons,modern management, and future considerations. Curr Oncol Rep
2012; 14: 70–78.67. Simon R, Roychowdhury S. Implementing personalized cancer
genomics in clinical trials. Nat Rev Drug Discov 2013; 12:358–369.
68. Alexandrov LB, Nik-Zainal S, Wedge DC, et al. Deciphering signa-tures of mutational processes operative in human cancer. Cell Rep
2013; 3: 246–259.69. Nik-Zainal S, Alexandrov LB, Wedge DC, et al. Mutational pro-
cesses molding the genomes of 21 breast cancers. Cell 2012; 149:979–993.
70. Bachelot T, Romieu G, Campone M, et al. Lapatinib pluscapecitabine in patients with previously untreated brain metastasesfrom HER2-positive metastatic breast cancer (LANDSCAPE): asingle-group phase 2 study. Lancet Oncol 2013; 14: 64–71.
71. Hohensee I, Lamszus K, Riethdorf S, et al. Frequent genetic alter-ations in EGFR- and HER2-driven pathways in breast cancer brainmetastases. Am J Pathol 2013; 183: 83–95.
72. Wikman H, Lamszus K, Detels N, et al. Relevance of PTEN loss inbrain metastasis formation in breast cancer patients. Breast Cancer
Res 2012; 14: R49.73. Law AJ, Shannon Weickert C, Hyde TM, et al. Neuregulin-1
(NRG-1) mRNA and protein in the adult human brain. Neuroscience
2004; 127: 125–136.74. US National Institutes of Health: http://www.clinicaltrials.gov75. Steeg PS, Camphausen KA, Smith QR. Brain metastases as preven-
tive and therapeutic targets. Nat Rev Cancer 2011; 11: 352–363.
76. Fidler IJ, Balasubramanian K, Lin Q, et al. The brain microenviron-
ment and cancer metastasis. Mol Cell 2010; 30: 93–98.
77. Ding L, Ellis MJ, Li S, et al. Genome remodelling in a basal-like
breast cancer metastasis and xenograft. Nature 2010; 464:999–1005.
78. Yachida S, Jones S, Bozic I, et al. Distant metastasis occurs late
during the genetic evolution of pancreatic cancer. Nature 2010; 467:1114–1117.
79. Cummings MC, Simpson PT, Reid LE, et al. Metastatic progression
of breast cancer: insights from 50 years of autopsies. J Pathol 2014;
232: 23–31.
80. Brannon AR, Vakiani E, Sylvester BE, et al. Comparative sequenc-
ing analysis reveals high genomic concordance between matched
primary and metastatic colorectal cancer lesions. Genome Biol
2014; 15: 454.
81. Chuang HN, van Rossum D, Sieger D, et al. Carcinoma cells misuse
the host tissue damage response to invade the brain. Glia 2013; 61:1331–1346.
82. Duchnowska R, Dziadziuszko R, Trojanowski T, et al. Conversion
of epidermal growth factor receptor 2 and hormone receptor expres-
sion in breast cancer metastases to the brain. Breast Cancer Res
2012; 14: R119.
83. Wolff AC, Hammond ME, Schwartz JN, et al. American Society
of Clinical Oncology/College of American Pathologists guideline
recommendations for human epidermal growth factor receptor 2
testing in breast cancer. J Clin Oncol 2007; 25: 118–145.
84. Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for
human epidermal growth factor receptor 2 testing in breast can-
cer: American Society of Clinical Oncology/College of American
Pathologists clinical practice guideline update. Arch Pathol Lab Med
2014; 138: 241–256.
85. Chang MC. Letter to the editor regarding ’Seol H, Lee HJ, Choi
Y, et al. Intratumoural heterogeneity of HER2 gene amplification in
breast cancer: its clinicopathological significance’. Mod Pathol 26:609–610.
86. Lee HJ, Park SY. Reply to Intratumoral heterogeneity of HER2 gene
amplification in breast cancer: its clinicopathological significance.
Mod Pathol 2013; 26: 610–611.
87. Seol H, Lee HJ, Choi Y, et al. Intratumoral heterogeneity of HER2
gene amplification in breast cancer: its clinicopathological signifi-
cance. Mod Pathol 2012; J25: 938–948.
88. Fujiwara S, Hung M, Yamamoto-Ibusuk CM, et al. The local-
ization of HER4 intracellular domain and expression of its
alternately-spliced isoforms have prognostic significance in ER+
HER2− breast cancer. Oncotarget 2014; 5: 3919–3930.
89. Nafi S, Generali D, Kramer-Marek G, et al. Nuclear HER4 mediates
acquired resistance to trastuzumab and is associated with poor
outcome in HER2 positive breast cancer. Oncotarget 2014; 5:5934–5949.
90. Wali VB, Haskins JW, Gilmore-Hebert M, et al. Convergent and
divergent cellular responses by ErbB4 isoforms in mammary epithe-
lial cells. Mol Cancer Res 2014; 12: 1140–1155.
91. Machleidt A, Buchholz S, Diermeier-Daucher S, et al. The prognos-
tic value of Her4 receptor isoform expression in triple-negative and
Her2 positive breast cancer patients. BMC Cancer 2013; 13: 437.
92. Nielsen TO, Poulsen SS, Journe F, et al. HER4 and its cytoplasmic
isoforms are associated with progression-free survival of malignant
melanoma. Melanoma Res 2014; 24: 88–91.
93. Tiwary S, Preziosi M, Rothberg PG, et al. ERBB3 is required for
metastasis formation of melanoma cells. Oncogenesis 2014; 3:e110.
94. Huang S, Li C, Armstrong EA, et al. Dual targeting of EGFR and
HER3 with MEHD7945A overcomes acquired resistance to EGFR
inhibitors and radiation. Cancer Res 2013; 73: 824–833.
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

Integrated genomic and transcriptomic analysis of brain metastases 377
95. Carrion-Salip D, Panosa C, Menendez JA, et al. Androgen-independent prostate cancer cells circumvent EGFR inhibition byoverexpression of alternative HER receptors and ligands. Int J
Oncol 2012; 41: 1128–1138.96. Thrane S, Lykkesfeldt AE, Larsen MS, et al. Estrogen receptor-α
is the major driving factor for growth in tamoxifen-resistant breastcancer and supported by HER/ERK signaling. Breast Cancer Res
Treat 2013; 139: 71–80.97. Morrison MM, Hutchinson K, Williams MM, et al. ErbB3 downreg-
ulation enhances luminal breast tumor response to antiestrogens. J
Clin Invest 2013; 123: 4329–4343.98. Reschke M, Mihic-Probst D, van der Horst EH, et al. HER3 is a
determinant for poor prognosis in melanoma. Clin Cancer Res 2008;14: 5188–5197.
99. Lin NU, Amiri-Kordestani L, Palmieri D, et al. CNS metastases inbreast cancer: old challenge, new frontiers. Clin Cancer Res 2013;19: 6404–6418.
100. Ramakrishna N, Temin S, Chandarlapaty S, et al. Recommenda-tions on disease management for patients with advanced humanepidermal growth factor receptor 2-positive breast cancer and brainmetastases: American Society of Clinical Oncology clinical practiceguideline. J Clin Oncol 2014; 32: 2100–2108.
101. Burvenich IJ, Lee FT, Cartwright GA, et al. Molecular imagingof death receptor 5 occupancy and saturation kinetics in vivo byhumanized monoclonal antibody CS-1008. Clin Cancer Res 2013;19: 5984–5993.
102. Taskar KS, Rudraraju V, Mittapalli RK, et al. Lapatinib distributionin HER2 overexpressing experimental brain metastases of breastcancer. Pharm Res 2012; 29: 770–781.
103. Grimm SA. Treatment of brain metastases: chemotherapy. Curr
Oncol Rep 2012; 14: 85–90.104. Dijkers EC, Oude Munnink TH, Kosterink JG, et al. Biodistribution
of 89Zr-trastuzumab and PET imaging of HER2-positive lesions inpatients with metastatic breast cancer. Clin Pharmacol Ther 2010;87: 586–592.
105. Mortimer JE, Bading JR, Colcher DM, et al. Functional imagingof HER2-positive metastatic breast cancer using 64Cu–DOTA–trastuzumab PET. J Nucl Med 2014; 55: 23–29.
106. Tamura K, Kurihara H, Yonemori K, et al. 64Cu–DOTA–trastuzumab PET imaging in patients with HER2-positive breastcancer. J Nucl Med 2013; 54: 1869–1875.
107. Hegde GV, de la Cruz CC, Chiu C, et al. Blocking NRG1 andother ligand-mediated Her4 signaling enhances the magnitude and
duration of the chemotherapeutic response of non-small cell lungcancer. Sci Transl Med 2013; 5: 171ra118.
108. Swain SM, Kim SB, Cortes J, et al. Pertuzumab, trastuzumab, anddocetaxel for HER2-positive metastatic breast cancer (CLEOPA-TRA study): overall survival results from a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol 2013; 14:461–471.
109. Swain SM, Baselga J, Miles D, et al. Incidence of central nervoussystem metastases in patients with HER2-positive metastatic breastcancer treated with pertuzumab, trastuzumab, and docetaxel: resultsfrom the randomized phase III study CLEOPATRA. Ann Oncol2014; 25: 1116–1121.
110. Janne PA, Shaw AT, Pereira JR, et al. Selumetinib plus docetaxel forKRAS-mutant advanced non-small-cell lung cancer: a randomised,multicentre, placebo-controlled, phase 2 study. Lancet Oncol 2013;14: 38–47.
111. Simmons BH, Lee JH, Lalwani K, et al. Combination of aMEK inhibitor at sub-MTD with a PI3K/mTOR inhibitor sig-nificantly suppresses growth of lung adenocarcinoma tumors inKras(G12D-LSL) mice. Cancer Chemother Pharmacol 2012; 70:213–220.
112. Janku F, Wheler JJ, Naing A, et al. PIK3CA mutation H1047Ris associated with response to PI3K/AKT/mTOR signaling path-way inhibitors in early-phase clinical trials. Cancer Res 2013; 73:276–284.
113. Lee B, Sandhu S, McArthur G. Cell cycle control as a promisingtarget in melanoma. Curr Opin Oncol 2015; 27: 141–150.
114. Ascierto PA, Schadendorf D, Berking C, et al. MEK162 for patientswith advanced melanoma harbouring NRAS or Val600 BRAF muta-tions: a non-randomised, open-label phase 2 study. Lancet Oncol
2013; 14: 249–256.115. Kawakami H, Okamoto I, Okamoto W, et al. Targeting MET ampli-
fication as a new oncogenic driver. Cancers 2014; 6: 1540–1552.116. Dillon LM, Miller TW. Therapeutic targeting of cancers with loss
of PTEN function. Curr Drug Targets 2014; 15: 65–79.117. Gelmon KA, Tischkowitz M, Mackay H, et al. Olaparib in patients
with recurrent high-grade serous or poorly differentiated ovariancarcinoma or triple-negative breast cancer: a phase 2, multicen-tre, open-label, non-randomised study. Lancet Oncol 2011; 12:852–861.
118. Tothill RW, Li J, Mileshkin L, et al. Massively-parallel sequencingassists the diagnosis and guided treatment of cancers of unknownprimary. J Pathol 2013; 231: 413–423.
SUPPLEMENTARY MATERIAL ON THE INTERNETThe following supplementary material may be found in the online version of this article:
Supplementary materials and methods and clinical history relating to sample Q851
Figure S1. Copy-number summary from GAP analysis: data are organized by primary tumour type and number of affected bases/sample
Figure S2. Circos plots showing the patterns of chromosomal gains and losses in breast, lung, melanoma and oesophageal BMs
Figure S3. Significant regions of copy-number change in brain metastases by GISTIC 2.0 analysis
Figure S4. RNA-sequencing metrics
Figure S5. Heat map showing absolute expression of key cancer drivers and novel brain metastasis candidate genes
Figure S6. Expression of somatic single-nucleotide variants and corresponding wild-type alleles of key cancer genes and candidate BM genes
Figure S7. Mutational process signatures present in brain metastasis genomes
Figure S8. Expression of ITPR1 is inversely associated with development of brain metastases in breast cancer
Figure S9. Relationships between copy number and expression of key HER pathway genes
Figure S10. Expression of EGFR and HER4 ligands in brain metastases
Figure S11. Representative phospho-HER staining of human brain metastases
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com

378 JM Saunus et al
Figure S12. Phospho-HER and HER2 expression in brain metastases
Figure S13. Hypothetical model in which brain-derived neuregulin (NRG) growth factor activates HER3 and critical tumourigenic functionsdownstream of core PI3K–AKT and MAPK signalling axes
Figure SM1. Example of qVerify output (Q178) with normal and BM DNA sample BAM files and a BM RNA BAM
Figure SM2. Proportion of variants verified using the qVerify tool
Figure SM3. Case Q851: mammograph of the 6cm primary breast tumour (left upper inner quadrant)
Tables S1–S14. See: https://dl.dropboxusercontent.com/u/42452103/Saunus-Quinn_JPathol_Supp%20tables_R.xlsx
Copyright © 2015 Pathological Society of Great Britain and Ireland. J Pathol 2015; 237: 363–378Published by John Wiley & Sons, Ltd. www.pathsoc.org.uk www.thejournalofpathology.com