Embed Size (px)
Citation preview

M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | M I L I N G O S E T A L . | 2 1
INTRODUCTIONEndometriosis is a common benign gy-
necological condition that is defined asthe presence of endometrial stromal andglandular cells outside the endometrialcavity and has a prevalence of 6–10% inwomen of reproductive age (1). Thisprevalence is approximately 20% inwomen with infertility (2). Despite ex-tensive research and numerous theoriesproposed, the pathogenesis of en-
dometriosis is yet to be determined, andseveral immunological and growth fac-tors have been investigated in the estab-lishment and maintenance of endometri-otic lesions.
In addition, it has been suggested thatectopic endometrial cells undergo de-creased apoptosis compared with eutopicendometrial cells (3) and that insulinlikegrowth factor 1 (IGF-1) is one of the con-tributing factors that inhibits apoptosis
and acts mitogenically on endometrialcells in vitro (4). Furthermore, increasedlevels of IGF-1 have been found in theperitoneal fluid of women with endo -metriosis compared with controls (5) andwere associated with increased proteoly-sis of IGF-binding protein 3 (IGFBP-3)mediated by urokinase-type plasmino-gen activator (uPA) (6,7).
The igf-1 gene contains six exons that,in humans, give rise to three igf-1 genetranscripts by alternative splicing,namely IGF-1Ea, IGF-1Eb and IGF-1Ec(which has also been named mechanogrowth factor [MGF]). The resultingIGF-1 isoforms undergo posttranslationalcleavage to produce a common biologi-cally active product, namely the matureIGF-1, which is encoded by exons 3 and
Insulinlike Growth Factor-1Ec (MGF) Expression in Eutopicand Ectopic Endometrium: Characterization of the MGF E-Peptide Actions In Vitro
Dimitrios S Milingos,1 Anastassios Philippou,1 Athanassios Armakolas,1 Efstathia Papageorgiou,1
Antigone Sourla,2 Athanassios Protopapas,3 Anthi Liapi,3 Aris Antsaklis,3 Minas Mastrominas,4 and Michael Koutsilieris1
1Department of Experimental Physiology, Medical School, National and Kapodistrian University of Athens, Goudi-Athens, Greece;2Endo/OncoResearch Medical Laboratories, Ampelokipi-Athens, Greece; 3First Department of Obstetrics and Gynecology,“ALEXANDRAS” General Hospital, Medical School, National and Kapodistrian University of Athens, Ampelokipi-Athens, Greece;and 4Embryogenesis, Inc., Maroussi, Athens, Greece
The transcription of the insulinlike growth factor 1 (igf-1) gene generates three mRNA isoforms, namely IGF-1Ea, IGF-1Eb and IGF-1Ec (or MGF [mechano growth factor]). Herein, we analyzed the expression of IGF-1 isoforms in eutopic and ectopic endometrium(red lesions and endometriotic cysts) of women with endometriosis, and we characterized the actions of a synthetic MGF E-peptideon KLE cells. Our data documented that all three igf-1 gene transcripts are expressed in the stromal cells of the eutopic and ec-topic endometrium; however, endometriotic cysts contained significantly lower IGF-1 isoform expression, both at the mRNA andprotein level, as was shown using semiquantitative PCR and immunohistochemical methods. In addition, the glandular cells of theeutopic endometrium did not express any of the IGF-1 isoforms; however, the glandular cells of the ectopic endometrium (red le-sions) did express the IGF-1Ec at mRNA and protein level. Furthermore, synthetic MGF E-peptide, which comprised the last 24amino acids of the MGF, stimulated the growth of the KLE cells. Experimental silencing of the type 1 IGF receptor (IGF-1R) and in-sulin receptor expression of KLE cells (siRNA knock-out methods) did not alter the mitogenic action of the synthetic MGF E-peptide,revealing that MGF E-peptide stimulates the growth of KLE cells via an IGF-1R–independent and insulin receptor–independentmechanism. These data suggest that the IGF-1Ec transcript might generate, apart from mature IGF-1 peptide, another posttrans-lational bioactive product that may have an important role in endometriosis pathophysiology.© 2011 The Feinstein Institute for Medical Research, www.feinsteininstitute.orgOnline address: http://www.molmed.orgdoi: 10.2119/molmed.2010.00043
Address correspondence and reprint requests to Michael Koutsilieris, MD, Department of
Experimental Physiology, Medical School, University of Athens, 75 Micras Asias, Goudi,
Athens, 115 27, Greece. Phone: 0030210-7462507; Fax: 0030210-7462571; E-mail:
Submitted March 29, 2010; accepted for publication September 12, 2010; Epub
(www.molmed.org) ahead of print September 14, 2010.

2 2 | M I L I N G O S E T A L . | M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1
M G F E X P R E S S I O N I N E U T O P I C A N D E C T O P I C E N D O M E T R I U M
posttranslational bioactive E-peptide ofthe IGF-1Ec isoform may be involved inthe pathophysiology of endometriosis.
MATERIALS AND METHODS
Ethical ApprovalA written informed consent was ob-
tained by all the volunteers to participatein this study, which was approved by theEthics Committee of the National andKapodistrian University of Athens, andall experimental procedures conformedto the Declaration of Helsinki.
SubjectsThe subjects were women of reproduc-
tive age undergoing laparoscopy for en-dometriosis. Median age of the womenwas 35.7 years (range 28–49), and nonehad received any form of hormone ther-apy up to 3 months before the operation.
zation of the intracellular signaling ofMGF E-domain vis-à-vis IGF-1 signalingin endometrial-like cells (20,22).
Herein, we report that all IGF-1 iso-forms are expressed in both eutopic andectopic endometrium, which is, however,significantly lower in endometriotic cystscompared with either eutopic en-dometrium or red lesions. In addition,we report for the first time that the glan-dular cells of eutopic endometrium andendometriotic cysts are deprived of anyexpression of the IGF-1 isoforms,whereas the glandular cells of red lesionsexpress the IGF-1Ec isoform. Further-more, our data documented that a syn-thetic MGF E-peptide can stimulate theproliferation of human KLE cells, an en-dometrial carcinoma cell line with a phe-notype of endometrial-like cells, via anIGF-1R–independent and IR-independentmechanism. These data suggest that a
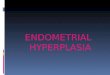
4, and it is responsible for binding withthe IGF receptors and different E-domainproducts (Figure 1), which contain differ-ent parts of exon 5 and/or exon 6 (8–11)and have been proposed to act au-tonomously (8,12).
IGF-1 mediates its actions throughbinding to specific receptors, such as thetype 1 IGF receptor (IGF-1R), the insulinreceptor (IR), and several atypical recep-tors such as the hybrid IR/IGF-1R. IGF-1R and IR are cell surface heterotetramerictyrosine kinase receptors that are coupledto intracellular signaling pathways, suchas the ras-raf-MAPK-ERKs and PI3K-AKTsignaling cascades (13).
Except for binding IGF-1, IGF-1R canalso bind insulinlike growth factor 2(IGF-2). This is a small peptide thatshares approximately 60% of amino acidswith IGF-1 and 40% with pro-insulin,and by its binding to IGF-1R, IGF-2 regu-lates cell proliferation, survival and dif-ferentiation. The affinity of IGF-2 forbinding IGF-1R is far less than IGF-1 andso it is for insulin (14,15). Although IGF-2can bind all three receptors (IGF-1R,IGF-2R and IR), its mitogenic and meta-bolic actions are mediated primarily bybinding to IGF-1R. In contrast to IGF-1R,IGF-2R is a transmembrane single-chainglycoprotein known as the cation- independent mannose-6-phosphate re-ceptor (16).
The distinctive biological roles of theIGF-1 isoforms and the mechanisms thatregulate their expression have not beenclearly documented. Several studies haveinvestigated the expression patterns ofthese IGF-1 transcripts in skeletal muscle(17–19), and there is growing interest vis-à-vis the potential role of MGF expressionin skeletal and cardiac muscle regenera-tion and hypertrophy after exercise- induced skeletal muscle damage (20) andmyocardial infarction (21,22). In addi-tion, we have previously reported pre-liminary data on the expression of IGF-1isoforms in endometriosis at mRNA level(23). However, there is little informationregarding the IGF-1Ec (MGF) expressionin stromal and glandular epithelium ofendometriotic lesions and the characteri-
Figure 1. Human IGF-1 alternative splicing and encoded propeptides. The igf-1 genegives rise to multiple mRNA transcripts by alternative splicing. The different IGF-1 mRNAtranscripts encode several precursor proteins, which differ by the length of the amino- terminal (signal) peptide and the structure of the extension peptide (E-peptide) on thecarboxy-terminal end. The mature IGF-1 peptide results from posttranslational cleavageof all precursor polypeptides, by which the signal and the E-peptide are removed. Exons5 and 6 encode distinct portions of the E-peptide (called the E-domain) with alternativecarboxy-terminal sequences of the extension peptide. The IGF-1Ec splice variant is anexon 4-5-6 variant that produces an E-peptide, termed Ec-peptide. The synthetic MGF E-peptide that comprises the last 24 C-terminal amino acids (aa) of Ec-peptide isshown.

R E S E A R C H A R T I C L E
M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | M I L I N G O S E T A L . | 2 3
embedded and processed for paraffinsections. The sections were incubatedwith the same primary antibodies usedfor the Western blot analyses (i.e., thepolyclonal anti-MGF antibody at a dilu-tion of 1:1,000 in phosphate-bufferedsaline (PBS) and the monoclonalanti–IGF-1) (1:50 dilution, MS-1508;Thermo Scientific) overnight at 4°C.After repeated PBS buffer washing, secondary biotinylated goat antirabbitIgG or goat antimouse IgG (DAB; DakoReal EnVision, Glostrup, Denmark) antibody was added for 25 min at roomtemperature, followed again by re-peated PBS buffer washes. Visualizationof the immunocomplex was obtainedby incubating the sections in a solutionof 3,3-diaminobenzidine (DAB) in PBSfor 10 min. Tissue sections were visual-ized under light microscopy, and imageswere captured on a PENTAX ASAHIdigital color camera mounted on themicroscope. A qualitative analysis ofthe tissue sections was then performedin the form of positive or negativestaining. Negative control staining pro-cedures were included in all immuno-histochemical analyses, as describedelsewhere (25).
Cell CulturesHuman KLE cells were obtained by
the American Type Culture Collection(ATCC, Bethesda, MD, USA) and main-tained as subconfluent monolayers inculture using Dulbecco’s modifiedEagle’s medium (DMEM/F-12; Cambrex,Walkersville, MD, USA) supplementedwith 10% fetal bovine serum (FBS; Invit-rogen) at 37°C in a humidified atmos-phere with 5% CO2, with culture mediabeing replaced every 2–3 d. KLE cellswere treated with 0.5 ng/mL up to30 ng/mL insulin (Novo Nordisk,Bagsværd, Denmark), with 0.5 ng/mLup to 50 ng/mL of mature IGF-1 peptide(rhIGF-1; Chemicon, Temecula, CA, USA)and with 0.5 ng/mL up to 50 ng/mL of asynthetic MGF peptide (which comprisesthe last 24 amino acids of the E-domainof human MGF, synthesized and vali-dated as previously described [25]; see
transcripts have been described else-where (23).
Protein Extraction and WesternAnalysis of IGF-1 and MGF
The extracts were analyzed for totalprotein concentration using the Bradfordprocedure (Bio-Rad Protein Assay; Bio-Rad, Hercules, CA, USA). Samples werestored in aliquots at –80°C until Westernblot analysis as previously described (25).The following primary antibodies wereused for the immunodetection of IGF-1Ec(MGF) and IGF-1: MGF, a rabbit antihu-man MGF polyclonal antibody (1:10,000dilution), which was raised against a syn-thetic peptide corresponding to the last 24amino acids of the E-domain of humanMGF (IGF-1Ec) and characterized in ourlaboratory, as has been described else-where (22); and IGF-1, a mouse mono-clonal anti–IGF-1 (1:1,000 dilution) (MS-1508; Thermo Scientific, Fremont, CA,USA; molecular weight of antigen:~7.6 kDa). After the overnight incubationof blots with the primary antibodies,membranes were incubated with a horse-radish peroxidase–conjugated secondaryantirabbit IgG (goat antirabbit, 1:2,000 di-lution; Santa Cruz Biotechnology, SantaCruz, CA, USA) or antimouse IgG goatantimouse (1:2,000 dilution; Santa CruzBiotechnology) for 1 h at room tempera-ture. Glyceraldehyde 3-phosphate dehy-drogenase (GAPDH) was used as an in-ternal control to correct for potentialvariation in the protein loading and tonormalize the protein measurements onthe same immunoblot. Blots were incu-bated with a mouse monoclonal primaryantibody for GAPDH (1:2,000 dilution;Santa Cruz Biotechnology) and with ahorseradish peroxidase–conjugated sec-ondary antimouse IgG (goat antimouse,1:2,000 dilution; Santa Cruz Biotechnol-ogy), and specific band(s) were visual-ized as described elsewhere (20).
Immunohistochemical AnalysisFormaldehyde-fixed eutopic and
ectopic endometrium (red lesions andendometriotic cysts) samples from allpatients’ biopsies were paraffin wax
Laparoscopy was performed during theproliferative phase of the menstrual cycle(fifth to tenth day after menstruation).
Tissue SamplingTissue sampling was from normal en-
dometrium (eutopic), red lesions and/orendometriotic cysts. We analyzed 15 tis-sue biopsies of endometriotic peritoneallesions (red lesions) and 20 tissue biop-sies of endometriotic cysts from 15 and20 patients, respectively. From the samewomen, normal endometrium was aspi-rated using the Cornier device (Labora-toire C.C.D., Paris, France). All patientshad stage III–IV endometriosis accordingto revised American Fertility Society(rAFS) classification. Tissue biopsies forRNA and protein extraction were snap-frozen in liquid nitrogen and then storedat –80°C until analysis, whereas biopsiesfor immunohistochemistry were trans-ferred to formaldehyde 9%. The diagno-sis of endometriosis was confirmed withhistological examination of related tissuebiopsies. The proliferative phase of themenstrual phase was determined basedon the last menstrual period and con-firmed with histological examination ofthe eutopic endometrium using theNoyes’ criteria (24).
RNA Extraction and RelativeQuantitative PCR Analysis
The expression of IGF-1 transcripts ineutopic and ectopic endometrium (redlesions and/or endometriotic cysts) andin KLE endometrial-like cells was as-sessed as previously described (23).Briefly, each endometriotic tissue samplewas homogenized and total RNA wasextracted using Trizol Reagent (Invitro-gen, Carlsbad, CA, USA) according tothe manufacturer’s recommendations.The RNA samples were used for the de-termination of the mRNA of specificIGF-1 transcripts by reverse transcription(RT) and semiquantitative RT–polymerasechain reaction (PCR) procedures. Boththese RT and PCR methods have beendescribed and extensively validated else-where (19). Primer sets and PCR condi-tions used for the assessment of IGF-1

2 4 | M I L I N G O S E T A L . | M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1
M G F E X P R E S S I O N I N E U T O P I C A N D E C T O P I C E N D O M E T R I U M
Figure 1) in a time-dependent manner(i.e., for 24 and 48 h).
Trypan Blue AssayKLE cells were plated at a cell density
of about 2.3 × 104 cell/well in 24-wellplates and grown with DMEM/F-12 con-taining 10% FBS. Twenty-four h afterplating, the media were changed toDMEM/F-12 containing 0.5% FBS, andmitogens under investigation wereadded in a dose-dependent manner (ma-ture IGF-1, MGF E-peptide and insulin).The actual living KLE cell number wasmeasured at different time intervals (24and 48 h) using the Trypan Blue exclu-sion assays, as previously described (26).
IGF-1R and IR siRNA Knock OutTo investigate if the synthetic MGF E-
peptide acts on KLE cells via the IGF-1R–or IR-mediated pathway, IGF-1R and IRexpression was silenced in KLE cellsusing the commercially available StealthsiRNA technology (Invitrogen). Threedifferent 25-mer siRNA molecules wereexamined in each case for their potentialto knock out (KO) the expression of IRand that of IGF-1R in KLE cells. It wasdetermined that the most efficient KO ofthe IR was obtained by using theACAAACUGCCCGUUGAUGACGGUGGsiRNA duplex at a concentration of40 pmol by using the reverse transfectionmethod. In the case of IGF-1R KO, themolecule of choice was the UCUUCAAGGGCAAUUUGCUCAUUAAsiRNA duplex, at a concentration of50 pmol, again by using reverse transfec-tion according to the manufacturer’s in-structions. As a negative control, weused a universal negative control stealthsiRNA (Invitrogen). In brief, KLE cellswere grown in 10% DMEM/F-12 media.The transfection mixture was obtainedby diluting the 40 pmol of the siRNA du-plex in 100 μL OptiMem serum-free medium (Invitrogen) in a well of a 24-wellplate, followed by the addition of 2 μLlipofectamine RNAiMAX (Invitrogen).After 20 min, 500 μL of the trypsinizedKLE cells was added to the mixture.Forty-eight hours after the KO, the
media switched to DMEM 0.5% FBS, andafter 24 h, the IR KO cells were exposedto either insulin or MGF E-peptide,whereas the IGF-1R KO cells were ex-posed to mature IGF-1 or MGF E-peptidefor 24 and 48 h in triplicate determina-tions. The viable cells were countedusing the Trypan Blue exclusion assay.
Expression of IGF-1R and IRThe expression level of IGF-1R and IR
transcripts, after the siRNA IGF-1R KO andIR KO in KLE cells, was assessed by quanti-tative real-time PCR (qRT-PCR). The KOmRNA levels were determined 48 h after thesiRNA KO according to the manufacturer’sinstructions. As an internal control, we usedGAPDH and β-actin. The validation of theproduct identity was obtained by the melt-ing curve. Quantitative RT-PCR to examinethe levels of expression of IGF-1R and IRwas carried out before and after the siRNAIGF-1R or IR KO in KLE cells. Briefly, RT-PCR data quantification analysis was carried
out in the forms of melting and amplifica-tion curves, cycle threshold (Ct) values andnormalized gene expression (Delta Delta Ct[ddCt]), using the Bio-Rad IQ5 optical soft-ware 2.0. The primers used in the reactionswere generated using the FastPCR programand were as follows: IGF-1R forward: ACCCGGAGTACTTCAGCGC; IGF-1R re-verse: CACAGAAGCTTCGTTGAGAA; IRforward: ACTCTCAGATCCTGA AGGAGCTGGA; IR reverse: AGTGTTGGGGAAAGCTGCCAC. The set ofprimers for IR was designed to detectboth IR isoforms in a single PCR. ThePCR conditions were the same in bothcases: 95°C for 30 s × 1 cycle, 94°C for20 s, 60°C for 30 s, 72°C for 30 s × 35 cy-cles and 72°C for 5 min.
Statistical AnalysisChanges in cell numbers were assessed
using analysis of variance (ANOVA)(SPSS v. 11 statistical package; SPSS, Chi-cago, IL, USA). Where significant F ratios
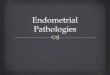
Figure 2. Expression of the different IGF-1 transcripts (IGF-1 Ea, IGF-1 Eb and IGF-1 Ec[MGF]) in eutopic endometrium (EU), peritoneal red lesion (PE) and ovarian endometrioticcyst (OvE). Representative PCR gel images demonstrate the differential mRNA expressionof the IGF-1 transcripts in PE and in OvE compared with EU (upper panel). In the lowerpanel, PCR relative quantification is presented. Values of PE and OvE were normalized toeach corresponding ribosomal 18S and expressed as percentage differences (%) from EUlevels (means ± SD, PE: n = 15, OvE: n = 20). *Significantly different from EU (P < 0.01).

R E S E A R C H A R T I C L E
M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | M I L I N G O S E T A L . | 2 5
were found (P < 0.05), the means werecompared using Tukey post hoc tests. AStudent t test was used to evaluate tran-scriptional and translational differencesin IGF-1 isoform expression between eu-topic endometrium and endometrioticcysts or red lesions. All data are pre-sented as mean ± SD. The level of signifi-cance was set at P < 0.05.
RESULTSThe expression of IGF-1 mRNA tran-
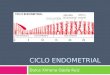
scripts was found to be significantlylower in the endometriotic cysts com-pared with that of the eutopic en-dometrium and that of the red lesions, asassessed by semiquantitative PCR meth-ods (Figure 2). Similar patterns of the IGF-1 transcripts translation were also de-tected in red lesions and endometrioticcysts compared with eutopic endo -metrium at the protein level (Figure 3A,B). The immunohistochemical analysis re-vealed that in the eutopic endo metrium(Figure 4A, E) and the endometriotic cysts(Figure 4C, G), the IGF-1 transcripts wereexpressed only in the stromal cells andnot in the glandular epithelium, whereasin the red lesions, the IGF-1 transcriptswere expressed not only in the stroma butalso in the glandular cells (Figure 4B, F).All 15 red lesion biopsies were positivefor glandular MGF/ IGF-1 expression,whereas all 15 biopsies from the eutopicendometrium (of the same women) were
negative for glandular MGF/IGF-1 ex-pression. The stroma was steady positivefor MGF/ IGF-1 expression in all eutopicand ectopic endometrial biopsies; how-ever, endometriotic cysts did express con-siderably lower MGF/IGF-1 levels, asnoted by immunohistochemical analysis.
In order to characterize the IGF-1Ecposttranslational products (mature IGF-1peptide and synthetic MGF E-peptide) invitro, we initially characterized the KLEcells. We documented that the KLE en-dometrial-like cells express all three IGF-1 mRNA transcripts, which are certainlytranslated to pro–IGF-1 and pro–IGF-1Ec(MGF) products at protein level (Fig-ure 5A, B).
Because the actions of IGF-1 can be me-diated not only via its high-affinity IGF-1Rbut also via IRs as well as hybrid IGF-1R/IR, we experimentally engineered KLEcells with silenced IGF-1R and IR expres-sion, using siRNA methods, to further
Figure 3. Representative Western blotsdemonstrating the expression of IGF-1and IGF-1Ec (MGF) in (A) peritoneal redlesion (PE) and in (B) ovarian endometri-otic cyst (OvE) samples examined in rela-tion to eutopic endometrium (EU).
Figure 4. (A–D) Cytoplasmic localization of IGF-1 in stromal cells (SC) in eutopic en-dometrium (A), endometriotic lesion (B) and endometriotic cyst (C). Note the absence ofstaining in glandular epithelium (GE) in eutopic endometrium as opposed to the positivestaining of glandular epithelium in endometriotic lesions. (D) Negative control. (E–H) Cyto-plasmic localization of MGF (IGF-1Ec) in stromal cells (SC) of tissue biopsies from eutopicendometrium (E), endometriotic lesion (F) and endometriotic cyst biopsies (G). Note theabsence of MGF staining in glandular epithelium biopsies (GE) of the eutopic en-dometrium and endometriotic cyst as opposed to the positive staining of glandular ep-ithelium in endometriotic lesion. (H) Negative control. Solid arrows represent stromal cells;hollow arrows represent glandular epithelium.
Figure 5. Expression of the different igf-1gene transcripts in KLE endometrial-likecells. (A) PCR products (that is, amplifiedtarget cDNAs) from the different primersets and PCR conditions used for the de-tection of IGF-1 transcripts at the mRNAlevel. An equal amount of each PCR prod-uct was loaded onto a 2% agarose geland separated by electrophoresis. (B)Translational products of the different IGF-1mRNA transcripts were detected by West-ern blot analysis using antibodies specificfor anti–IGF-1 and anti–IGF-1Ec (MGF).

2 6 | M I L I N G O S E T A L . | M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1
M G F E X P R E S S I O N I N E U T O P I C A N D E C T O P I C E N D O M E T R I U M
characterize MGF E-peptide actions inKLE cells. Thus, we generated transfectansof siRNA IGF-1R KO KLE cells and siRNAIR KO KLE cells. Indeed, we achieved ap-proximately 60–80% reduction of IRmRNA expression (for both IR transcripts;IR-A and IR-B) compared with the respec-tive expression levels assessed in control
KLE cells (Figure 6A, D, G). Similar resultswere obtained in the siRNA IGF-1R KLEcells (Figure 6B, E, F). Analyses of β-actin(Figure 6C) and GAPDH expression (notshown) were used as internal controls fornormalization in all cases.
Using these KLE transfectans, we wereable to show that exogenous IGF-1 and
insulin administration did not stimulatethe IGF-1R KO and IR KO KLE cells. Onthe contrary, IGF-1 and insulin stimu-lated the growth of parental KLE cells(Table 1). Interestingly, MGF E-peptidestimulated the proliferation of parentaland IGF-1R KO and IR KO KLE cells (seeTable 1).
Figure 6. Characterization of the degree of reduction of IR expression in IR KO KLE cells (A) and of IGF-1R expression in IGF-1R KO KLEcells (B) by qRT-PCR. IR KO and IGF-1R KO lines represent the melting curves of IR (IR-A and IR-B isoforms) and IGF-1R in IR KO KLE andIGF-1R KO KLE cells, respectively, compared with the lines of IR and IGF-1R in control KLE cells. The amplification curves and Cts (D, E) aswell as normalized expression (ddCt) charts (F, G) are also shown. The degree of reduction of IR and IGF-1R expression was from 60% upto 80% in this cell line. Normalization in all the cases was carried out by β-actin (C).

R E S E A R C H A R T I C L E
M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | M I L I N G O S E T A L . | 2 7
DISCUSSIONIn this study, we documented that eu-
topic and ectopic (endometriotic cysts andred lesions) endometrium obtained fromwomen with endometriosis as well ashuman KLE endometrial-like cells expressIGF-1 transcripts. We have defined thatthe IGF-1Ec transcript is expressed both atthe mRNA and protein level. This particu-lar IGF-1 transcript has been associatedwith regeneration mechanisms of skeletalmuscle and myocardial cells (20–22).
Semiquantitative analysis of the IGF-1transcript expression using PCR methodsrevealed that endometriotic cysts ex-pressed IGF-1 transcripts at a significantlylower level than eutopic endometriumand red lesions. These findings were in-line with our preliminary data previouslypublished (23). Our findings could be ex-plained by the fact that even though en-dometriotic cysts represent a feature ofadvanced disease, they are characterizedby the presence of fibrosis and low levelsof active endometriotic tissue. This resultis consistent with the natural history ofthe disease, during which active en-dometriotic tissue is substituted by fi-brotic tissue accounting for the increasedscarring and adhesion formation found inlate stages of endometriosis (23). This re-sult is also consistent with the results ofour previous studies, where we docu-mented increased expression of othercomponents of the IGF bioregulatory sys-tem, which includes IGFs/uPA/plas-min/IGFBP-3 expression (6,7,27).
In this study, we used specific antibod-ies to identify the expression of IGF-1 andMGF in endometriotic biopsies by im-munohistochemical and Western blotanalyses. Because IGF-1 peptide is a com-mon product of all three IGF-1 transcripts,anti–IGF-1 antibody can detect the expres-sion of pro–IGF-1 peptide from any IGF-1transcript. On the contrary, our anti-MGFantibody identifies the expression of theIGF-1Ec (MGF) transcript only. The im-munohistochemical analysis of IGF-1transcripts posttranslational products re-vealed that in eutopic endo metrium andendometriotic cysts, IGF-1 and IGF-1Ec(MGF) were expressed only in stromacells but not in glandular cells. In contrast,in red lesions, there was positive stainingnot only in stroma cells but also in glan-dular epithelium. Even though histologi-cal diagnosis of endo metriosis requiresthe presence of stroma and glandular cellsin tissue biopsies, the proportion ofstroma/glands in endometriotic tissue isnot constant, and it has been suggestedthat lesions related to more active formsof endo metriosis (for example, red le-sions) present a higher proportion of glan-dular cells (28). This was evident in ourbiopsies as well, as histological examina-tion showed increased proportion of glan-dular epithelium in red lesions comparedwith endometriotic cysts. This could ac-count for the increased IGF-1 transcriptsexpression (although not significant) inred lesions as it was documented by semi-quantitative PCR analysis in our study.
The expression of IGF-1 and IGF-1Ec inthe glandular epithelium of only en-dometriotic lesions and not in eutopic en-dometrium and endometriotic cysts couldfavor our hypothesis that IGF-1 and IGF-1Ec isoforms are associated with activeendometriosis, and their action in ectopicendometriotic cells could be involved inthe progression of the disease and evolu-tion of endometriotic lesions.
The IGF-1 stimulates the growth anddifferential function of endometrial cellsvia the IGF-1R, and possibly via severalatypical receptors, including the hybridIR/IGF-1R. The latter is composed of anIR hemi-receptor linked to an IGF-IRhemi-receptor and has been reported tohave an important role in cancer biology(29–31). Recently, the two IR isoforms(IR-A and IR-B) have been reported thatare overexpressed in cancer tissues (32),whereas the expression of IGF-1R hasbeen previously characterized in KLEcells in our laboratory (7). Therefore, aim-ing to the characterize the MGF E-peptideactions in KLE cells, we performed a se-ries of silencing experiments of thesemajor receptors involved in the IGF- mediated actions. Our data suggested thatsilencing of the IGF-1R and IR expressionin KLE cells did not have an important ef-fect on the proliferative activity of the ex-ogenous MGF E-peptide in vitro, thus sug-gesting that synthetic MGF E-peptideaction is apparently mediated via an IGF-1R–independent, IR- independent mecha-nism. Because the IR/IGF-1R hybrid re-
Table 1. The effects of 48 h of treatment with mature IGF-1, insulin and synthetic MGF E-peptide on KLE cell proliferation, as assessed byTrypan blue exclusion assays (cell number × 104).
IGF-1 (50 ng/mL) in MGF (50 ng/mL) in IGF-1 (50 ng/mL) in MGF (50 ng/mL) in Control siRNA-transfecteduntransfected KLE cells untransfected KLE cells IGF1R siRNA KLE cells IGF1R siRNA KLE cells KLE cells
112.5 ± 8.66 103.33 ± 5.20 76.25 ± 5.30 95.83 ± 3.81 73.75 ± 5.30a b c
Insulin (30 ng/mL) in MGF (50 ng/mL) in Insulin (30 ng/mL) in MGF (50 ng/mL) in Control siRNA-transfecteduntransfected KLE cells untransfected KLE cells IR siRNA KLE cells IR siRNA KLE cells KLE cells
32.9 ± 5.49 34.37 ± 5.15 12.5 ± 2.5 28.87 ± 4.73 11.25 ± 2.5b a b
The mitogenic activity of the IGF-1 and insulin was blocked in IGF-1R siRNA KLE cells and in the IR siRNA KLE cells, respectively, whereasMGF E-peptide mitogenic actions were not affected in IGF-1R siRNA KLE cells and in the IR siRNA KLE cells. These data suggested thatMGF actions are possibly mediated via an IGF-1R–independent, IR-independent and hybrid IGF-1R/IR–independent mechanism in KLEendometrial-like cells. Significantly different from control-siRNA transfected KLE cells: aP < 0.001; bP < 0.01; cP < 0.05.

2 8 | M I L I N G O S E T A L . | M O L M E D 1 7 ( 1 - 2 ) 2 1 - 2 8 , J A N U A R Y - F E B R U A R Y 2 0 1 1
M G F E X P R E S S I O N I N E U T O P I C A N D E C T O P I C E N D O M E T R I U M
ceptor consists of IR and IGF-1R hemi-re-ceptors, the silencing of the IR or the IGF-1R is expected to block the formation ofthe hybrid receptor. Therefore, our experi-ments suggested that mitogenic activity ofthe synthetic MGF E-peptide is mediatedvia another receptor molecule.
Further evidence for such autonomousactions of the synthetic MGF E-peptidewas provided by our recent data, whichrevealed that MGF E-peptide activatedERK1/2 phosphorylation but did not ac-tivate AKT phosphorylation in skeletalmuscle–like and myocardial-like cells(20,22). This particular phosphorylationpattern generated by the MGF E-peptideis in agreement with the trypan blue ex-clusion assays in KLE cells, thus suggest-ing that MGF E-peptide activity is via anIGFR/IR-independent mechanism andvia an as yet unidentified molecule.
In conclusion, our data suggest the pos-sible role of IGF-1Ec (MGF) expression inendometriosis. This is supported by thepreferential expression of this IGF-1 tran-script in glandular epithelial cells in ec-topic endometrium only (red lesions).Conceivably, this preferential MGF ex-pression generates posttranslational prod-ucts IGF-1 and MGF E-peptide, with thelatter being capable of stimulating theproliferation of endometrial-like cells viaan IGF-1R–independent, IR-independentand hybrid IGF-1R/IR–independentmechanism. These data suggest that theremay be a role for MGF in the pathogene-sis of endometriosis that is autonomousand independent from the IGF system.
DISCLOSUREThe authors declare that they have no
competing interests as defined by Molec-ular Medicine, or other interests thatmight be perceived to influence the re-sults and discussion reported in thispaper.
REFERENCES1. Giudice LC, Kao LC. (2004) Endometriosis. Lancet
364:1789–99.2. Gao X, Outley J, Botteman M, Spalding J, Simon
JA, Pashos CL. (2006) Economic burden of en-dometriosis. Fertil. Steril. 86:1561–72.
3. Gebel HM, Braun DP, Tambur A, Frame D, Rana N,
Dmowski WP. (1998) Spontaneous apoptosis of en-dometrial tissue is impaired in women with en-dometriosis. Fertil. Steril. 69:1042–7.
4. Koutsilieris M, Mastrogamvrakis G, Lembessis P,Sourla A, Miligos S, Michalas S. (2001) Increasedinsulin-like growth factor 1 activity can rescueKLE endometrial-like cells from apoptosis. Mol.Med. 7:20–6.
5. Kim JG, Suh CS, Kim SH, Choi YM, Moon SY, LeeJY. (2000) Insulin-like growth factors (IGFs), IGF-binding proteins (IGFBPs), and IGFBP-3 proteaseactivity in the peritoneal fluid of patients with andwithout endometriosis. Fertil. Steril. 73:996–1000.
6. Koutsilieris M, Lavergne E, Lemay A. (1997) Asso-ciation of protease activity against IGFBP-3 withperitoneal fluid mitogens: possible implications forthe ectopic growth of endometrial cells in womenwith endometriosis. Anticancer Res. 17:1239–44.
7. Lembessis P, Kalariti N, Koutsilieris M. (2004)Glucocorticoid receptor function suppresses in-sulin-like growth factor 1 activity in human KLEendometrial-like cells. In Vivo 18:43–7.
8. Siegfried JM, Kasprzyk PG, Treston AM, MulshineJL, Quinn KA, Cuttitta F. (1992) A mitogenic pep-tide amide encoded within the E peptide domainof the insulin-like growth factor IB prohormone.Proc. Natl. Acad. Sci. U. S. A. 89:8107–11.
9. Gilmour RS. (1994) The implications of insulin-like growth factor mRNA heterogeneity. J. En-docrinol. 140:1–3.
10. Chew SL, Lavender P, Clark AJ, Ross RJ. (1995)An alternatively spliced human insulin-likegrowth factor-I transcript with hepatic tissue ex-pression that diverts away from the mitogenicIBE1 peptide. Endocrinology 136:1939–44.
11. Shavlakadze T, Winn N, Rosenthal N, GroundsMD. (2005) Reconciling data from transgenicmice that overexpress IGF-I specifically in skele-tal muscle. Growth Horm. IGF Res. 15:4–18.
12. Kuo YH, Chen TT. (2002) Novel activities of pro-IGF-I E peptides: regulation of morphologicaldifferentiation and anchorage-independentgrowth in human neuroblastoma cells. Exp. CellRes. 280:75–89
13. Samani AA, Yakar S, LeRoith D, Brodt P. (2007)The role of the IGF system in cancer growth andmetastasis: overview and recent insights. Endocr.Rev. 28:20–47.
14. Jones JI, Clemmons DR. (1995) Insulin-likegrowth factors and their binding proteins: bio-logical actions. Endocr. Rev. 16:3–34.
15. LeRoith D, Werner H, Beitner-Johnson D, RobertsCT. (1995) Molecular and cellular aspects of theinsulin-like growth factor I receptor. Endocr. Rev.16:143–63.
16. Kornfeld S. (1992) Structure and function of themannose-6-phosphate/insulinlike growth factorII receptors. Annu. Rev. Biochem. 61:307–30.
17. Hameed M, Orrell RW, Cobbold M, Goldspink G,Harridge SD. (2003) Expression of IGF-I splicevariants in young and old human skeletal muscleafter high resistance exercise. J. Physiol. 547:247–54.
18. Bickel CS, Slade J, Mahoney E, Haddad F, Dudley
GA, Adams GR. (2005) Time course of molecularresponses of human skeletal muscle to acute boutsof resistance exercise. J. Appl. Physiol. 98:482–8.
19. Kim JS, Cross JM, Bamman MM. (2005) Impact ofresistance loading on myostatin expression andcell cycle regulation in young and older men andwomen. Am. J. Physiol. Endocrinol. Metab.288:E1110–9.
20. Philippou A, et al. (2009) Expression of IGF-1 iso-forms after exercise-induced muscle damage inhumans: characterization of the MGF E peptideactions in vitro. In Vivo 23:567–75.
21. Carpenter V, et al. (2008) Mechano-growth factorreduces loss of cardiac function in acute myocar-dial infarction. Heart Lung Circ. 17:33–9.
22. Stavropoulou A, Halapas A, Sourla A, PhilippouA, Papageorgiou E, Papalois A, Koutsilieris M.(2009) IGF-1 expression in infarcted myocardiumand MGF E peptide actions in rat cardiomy-ocytes in vitro. Mol. Med. 15:127–35.
23. Milingos D, et al. (2006) Insulin-like growth fac-tor-1 isoform mRNA expression in women withendometriosis: eutopic endometrium versus en-dometriotic cyst. Ann. N. Y. Acad. Sci. 1092:434–9.
24. Noyes RW, Hertig AT, Rock J. (1975) Dating the en-dometrial biopsy. Am. J. Obstet. Gynecol. 122:262–3.
25. Philippou A, Stavropoulou A, Sourla A, Pissimis-sis N, Halapas A, Maridaki M, Koutsilieris M.(2008) Characterization of a rabbit antihumanmechano growth factor (MGF) polyclonal anti-body against the last 24 amino acids of the E do-main. In Vivo 22:27–35.
26. Koutsilieris M, Rabbani SA, Goltzman D. (1987)Effects of human prostatic mitogens on rat bonecells and fibroblasts. J. Endocrinol. 115:447–54.
27. Koutsilieris M, Sourla A, Pelletier G, Doillon CJ.(1994) Three-dimensional type I collagen gel sys-tem for the study of osteoblastic metastases pro-duced by metastatic prostate cancer. J. BoneMiner. Res. 9:1823–32.
28. Donnez J, Squifflet J, Casanas-Roux F, Pirard C,Jadoul P, van Langendonckt A. (2003) Typicaland subtle atypical presentations of endometrio-sis. Obstet. Gynecol. Clin. N. Am. 30:83–93.
29. Bogdanos J, Karamanolakis D, Tenta R, TsintavisA, Milathianakis C, Mitsiades C, Koutsilieris M.(2003) Endocrine/paracrine/autocrine survivalfactor activity of bone microenvironment partici-pates in the development of androgen ablationand chemotherapy refractoriness of prostate can-cer metastasis in skeleton. Endocr. Relat. Cancer10:279–89.
30. Koutsilieris M, Mitsiades C, Sourla A. (2000) In-sulin-like growth factor I and urokinase-typeplasminogen activator bioregulation system as asurvival mechanism of prostate cancer cells inosteoblastic metastases: development of anti- survival factor therapy for hormone-refractoryprostate cancer. Mol. Med. 6:251–67.
31. Koutsilieris M. (1992) Pathophysiology of uterineleiomyomas. Biochem. Cell Biol. 70:273–8.
32. Cox ME, et al. (2009) Insulin receptor expressionby human prostate cancers. Prostate 69:33–40.