Embed Size (px)
Citation preview
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
Multiple Insulin Injection Therapy
The presentation
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
Introduction:
• Goals of multiple insulin injection.
• High light of treatment method.
• Glycemic control effect.
• Diet treatment.
Type of insulin:• Insulin preparation.
• What to mix and what not to mix.
Type of regimen:• Western regimen.
• Our regimen.
• Future regimen.
Important phenomena:• Somogyi phenomena.
• Dawn and predawn phenomena.

Goals
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
Clinical Goals:
• Elimination of ketosis.• Elimination of hyperglycemia and it’s symptoms.• Prevention of chronic complications.
Additional Goals:
• Maintaining desirable weight.• Maintaining normal growth and sexual maturation.• Maintaining psychosocial well-being.• Achieving normal fertility and pregnancy.• Sustaining normal family and sexual life.
Control Goals:
• HbA1c <7%.• Pre-meal SMBG 80-120 mg/dl (4.4-6.7 mmol/l).• Bed time SMBG 100-140 mg/dl (5.6-7.8 mmol/l).• No ketonuria.• Mean blood glucose level 120-160 mg/dl (6.7-8.9 mmol/l).
Highlights
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
Insulin:• Type 1 diabetes is dependent on insulin for survival.• Insulin is classified by source or duration of action.• Human insulin has less allergy or lipoatrophy.• More than one injection is needed and different types.• Proper action During honeymoon phase.• The commonest side effect is hypoglycemia.
Nutrition: • Enable near normal blood glucose level.• Maintain a reasonable body weight.• Protein 10-20%, Fat 15-25%, Carbohydrate 65%.• Fibers, vitamins, and minerals.• Food exchanges or carbohydrate counting.• Total daily calorie intake adjustment.
Exercise: • Should be integrated.• Weight control and improve well being.• Pre-exercise medical evaluation.
Monitoring:• Glucometer use SMBG to monitor blood glucose level.• Adjustment of insulin, diet, and exercise.• Urine testing for both glucose and ketones.• HbA1c the best index for control.
Glycemic control
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
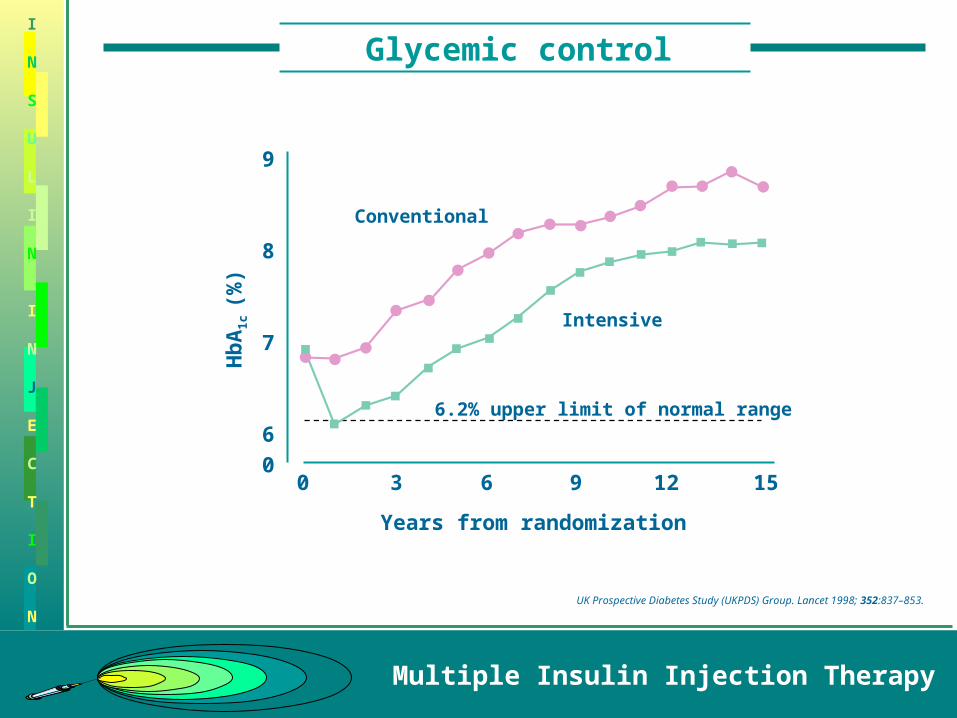
Years from randomization
Conventional
Intensive
6.2% upper limit of normal range
0 3 6 9 12 15
9
8
7
6
0
Hb
A1c
(%)
UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352:837–853.
Diet
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
30
25
20
35
30
25
40
35
30
Physical activity
Body w
eig
ht
25 years male IBW 60 kgm
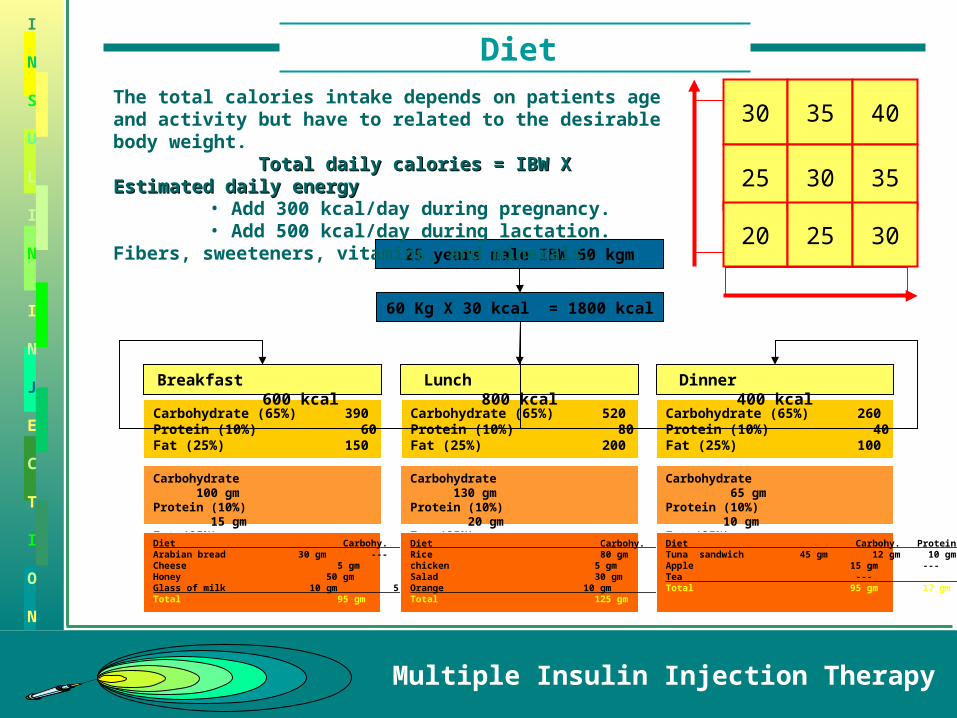
Carbohydrate (65%) 390Protein (10%) 60Fat (25%) 150
Carbohydrate 100 gmProtein (10%) 15 gmFat (25%) 17 gmDiet Carbohy. Protein Fat _Arabian bread 30 gm --- ---Cheese 5 gm 10 gm 10 gmHoney 50 gm 2 gm 3 gmGlass of milk 10 gm 5 gm 5 gm_Total 95 gm 17 gm 18 gm
Carbohydrate (65%) 520Protein (10%) 80Fat (25%) 200
Carbohydrate 130 gmProtein (10%) 20 gmFat (25%) 22 gmDiet Carbohy. Protein Fat _Rice 80 gm --- 6 gmchicken 5 gm 15 gm 12 gmSalad 30 gm 4 gm 4 gmOrange 10 gm --- ---___Total 125 gm 19 gm 22 gm
Carbohydrate (65%) 260Protein (10%) 40Fat (25%) 100
Carbohydrate 65 gmProtein (10%) 10 gmFat (25%) 11 gmDiet Carbohy. Protein Fat _Tuna sandwich 45 gm 12 gm 10 gmApple 15 gm --- ---Tea --- --- --- _Total 95 gm 17 gm 18 gm
60 Kg X 30 kcal = 1800 kcal
Breakfast 600 kcal
Lunch 800 kcal
Dinner 400 kcal
The total calories intake depends on patients age and activity but have to related to the desirable body weight. Total daily calories = IBW X Estimated daily Total daily calories = IBW X Estimated daily energyenergy
• Add 300 kcal/day during pregnancy.• Add 500 kcal/day during lactation.
Fibers, sweeteners, vitamins, and minerals.
Glucose sensor
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
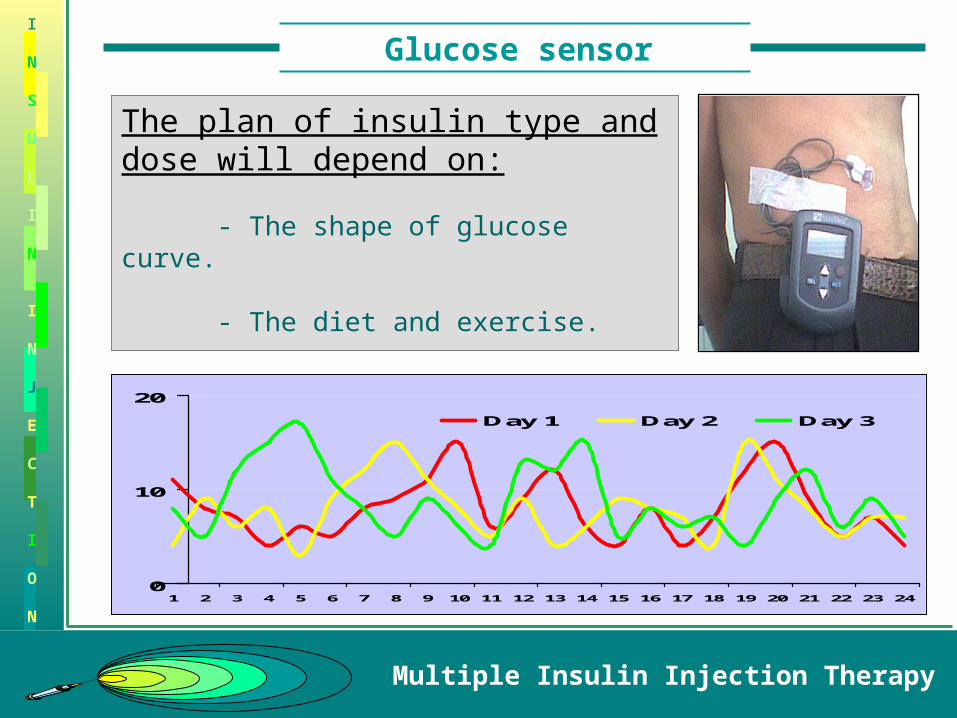
The plan of insulin type and dose will depend on:
- The shape of glucose curve.
- The diet and exercise.
0
10
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Day 1 Day 2 Day 3
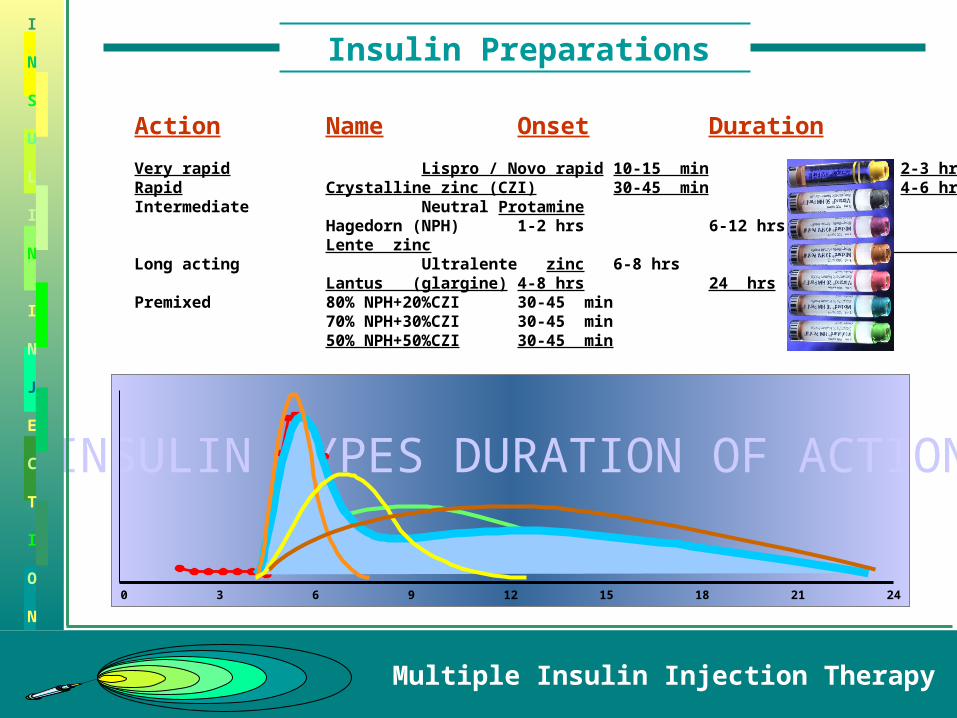
INSULIN TYPES DURATION OF ACTION
0 3 6 9 12 15 18 21 24
Insulin Preparations
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
Action Name Onset Duration
Very rapid Lispro / Novo rapid 10-15 min 2-3 hrsRapid Crystalline zinc (CZI) 30-45 min 4-6 hrsIntermediate Neutral Protamine
Hagedorn (NPH) 1-2 hrs 6-12 hrsLente zinc
Long acting Ultralente zinc 6-8 hrs 18 hrsLantus (glargine) 4-8 hrs 24 hrs
Premixed 80% NPH+20%CZI 30-45 min 6-12 hrs70% NPH+30%CZI 30-45 min 6-12 hrs50% NPH+50%CZI 30-45 min 6-12 hrs
Insulin Mixing
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
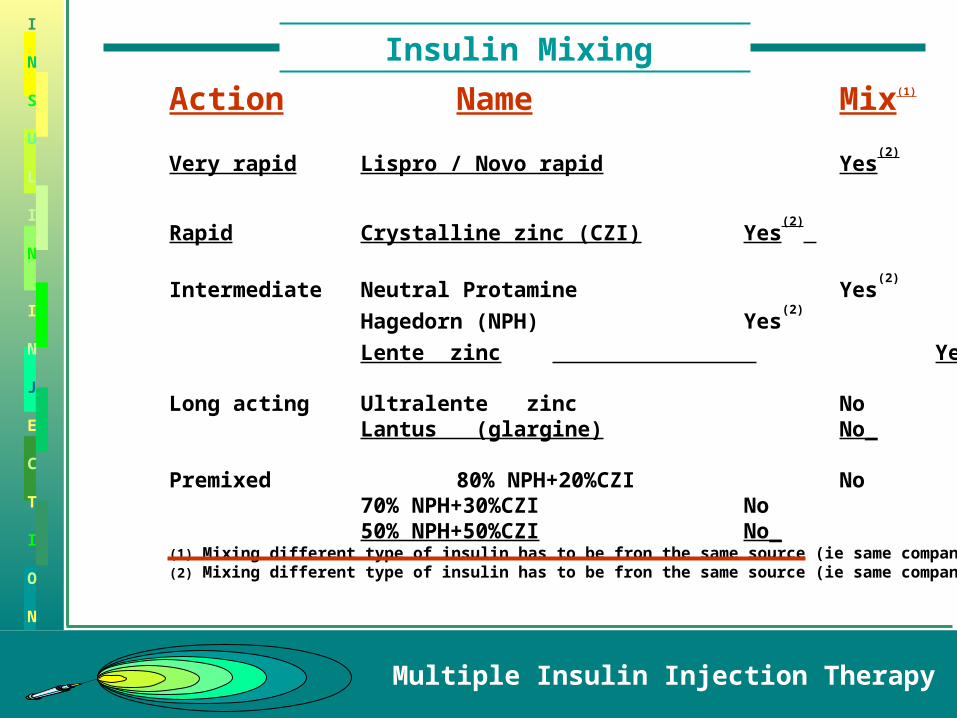
Action Name Mix(1)
Very rapid Lispro / Novo rapid Yes(2)
Rapid Crystalline zinc (CZI) Yes(2)
Intermediate Neutral Protamine Yes(2)
Hagedorn (NPH) Yes(2)
Lente zinc Yes(2)
Long acting Ultralente zinc NoLantus (glargine) No_
Premixed 80% NPH+20%CZI No70% NPH+30%CZI No50% NPH+50%CZI No_
(1) Mixing different type of insulin has to be fron the same source (ie same company) (2) Mixing different type of insulin has to be fron the same source (ie same company)
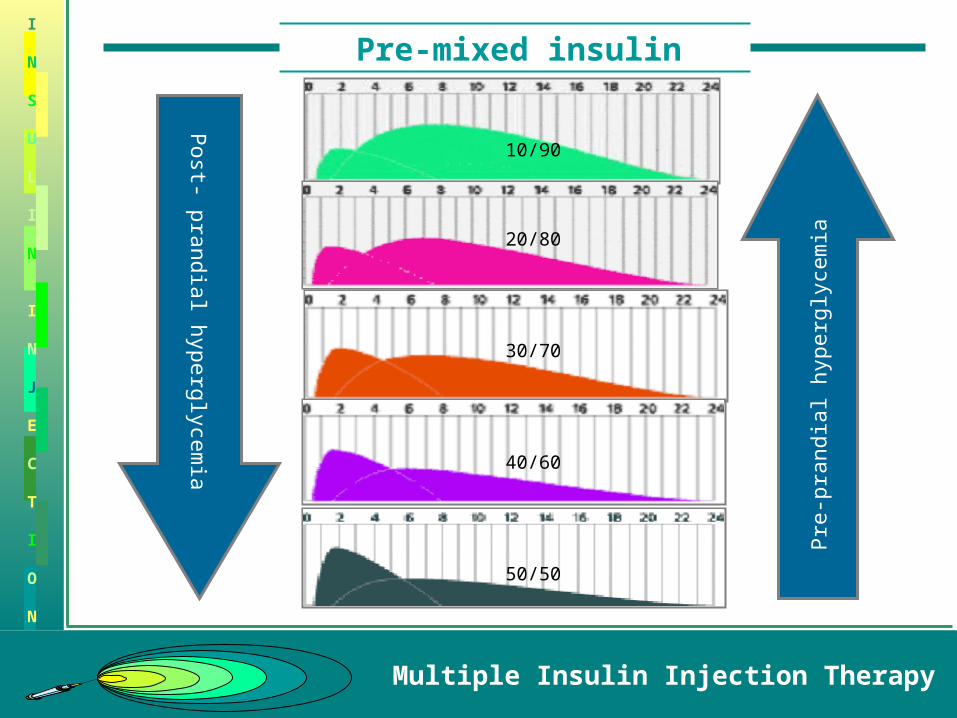
Pre-mixed insulin
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
10/90
20/80
30/70
40/60
50/50
Post- p
randia
l hyperg
lyce
mia
Pre
-pra
ndia
l hyperg
lyce
mia
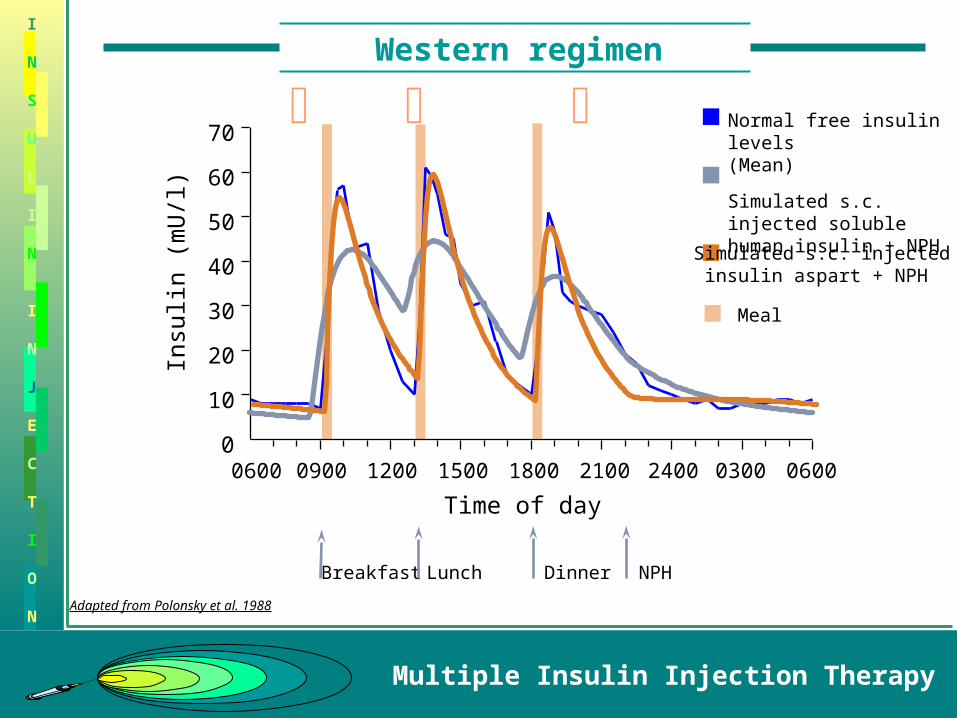
Western regimen
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
Time of day
0
10
20
30
40
50
60
70
0600 0900 1200 1500 1800 2100 2400 0300 0600
Insu
lin (
mU
/l)
Normal free insulin levels (Mean)
Simulated s.c. injected soluble human insulin + NPH
Adapted from Polonsky et al. 1988
Dinner NPHBreakfast Lunch
Simulated s.c. injected insulin aspart + NPH
Meal
Western regimen
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
50
150
6 9 12 3 6 9 12 3
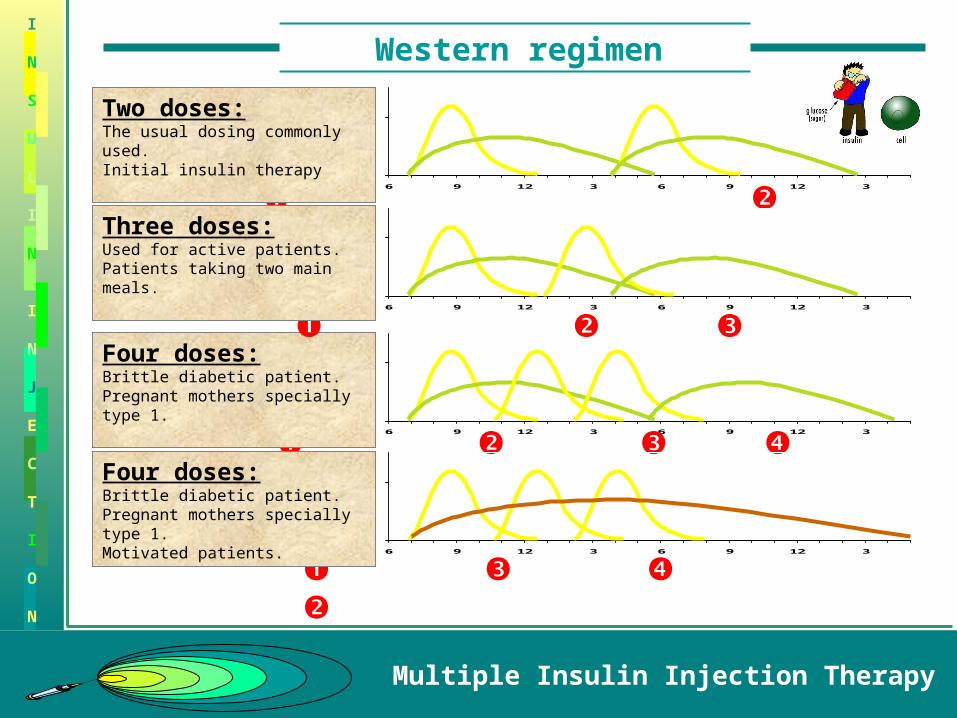
Two doses:The usual dosing commonly used.Initial insulin therapy
50
150
6 9 12 3 6 9 12 3
Four doses:Brittle diabetic patient.Pregnant mothers specially type 1.
50
150
6 9 12 3 6 9 12 3
Four doses:Brittle diabetic patient.Pregnant mothers specially type 1.Motivated patients.
50
150
6 9 12 3 6 9 12 3
Three doses:Used for active patients.Patients taking two main meals.
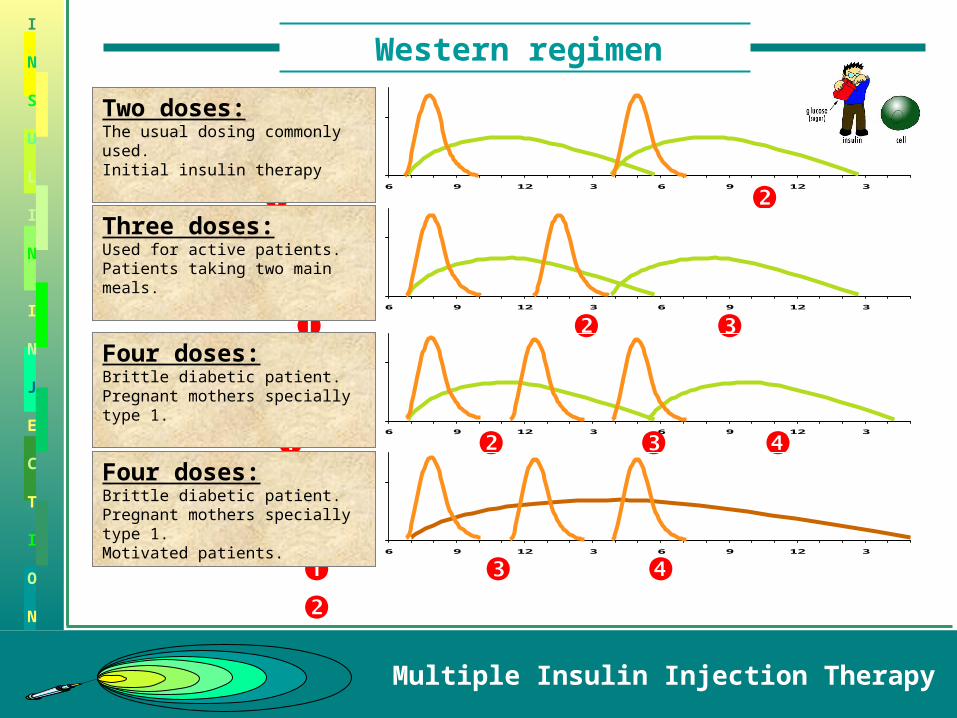
Western regimen
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
50
150
6 9 12 3 6 9 12 3
Two doses:The usual dosing commonly used.Initial insulin therapy
50
150
6 9 12 3 6 9 12 3
Three doses:Used for active patients.Patients taking two main meals.
50
150
6 9 12 3 6 9 12 3
Four doses:Brittle diabetic patient.Pregnant mothers specially type 1.
50
150
6 9 12 3 6 9 12 3
Four doses:Brittle diabetic patient.Pregnant mothers specially type 1.Motivated patients.
Blood Glucose Curve
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
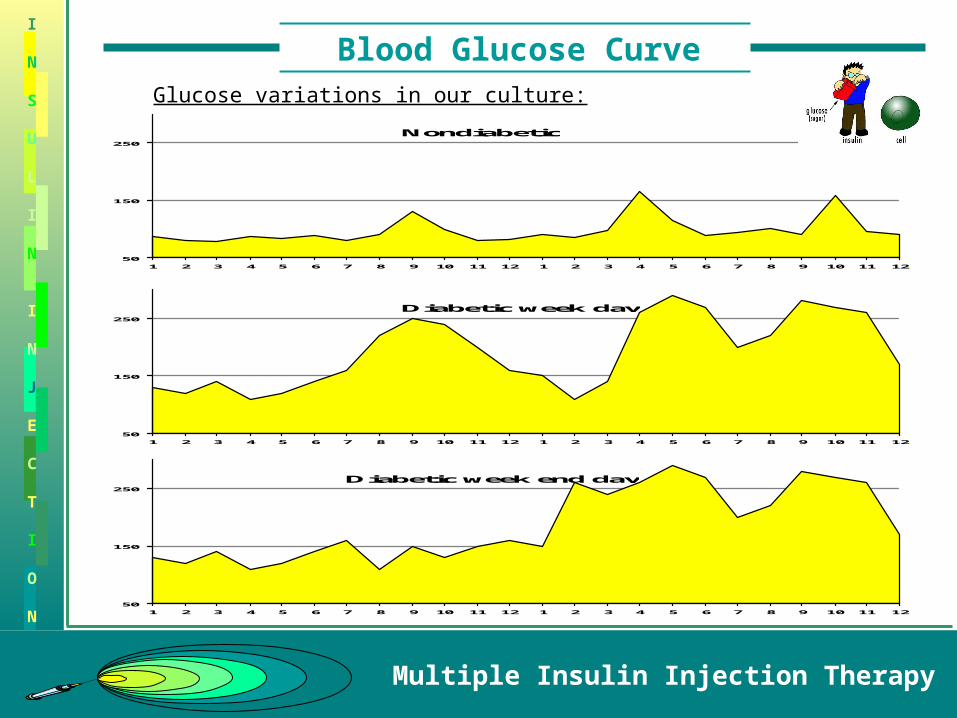
50
150
250
1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12
Nondiabetic
50
150
250
1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12
Diabetic week day
50
150
250
1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12
Diabetic week end day
Glucose variations in our culture:

Insulin Use
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
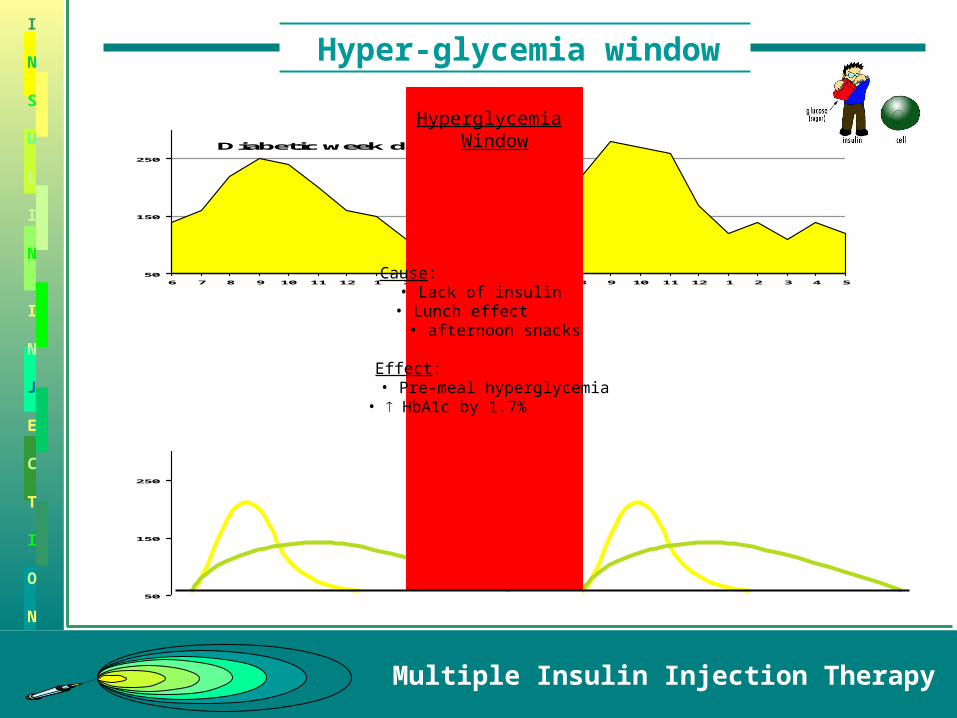
• Regular and NPH use twice daily the commonest regimen used.• Premixed with different concentration (30/70, 40/60, 50/50).• Lunch is the biggest meal usually but no insulin dosing.
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Diabetic week day
Hyper-glycemia window
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Diabetic week day
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Hyperglycemia Window
Cause: • Lack of insulin • Lunch effect • afternoon snacks
Effect: • Pre-meal hyperglycemia• HbA1c by 1.7%
Hyper-glycemia window
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
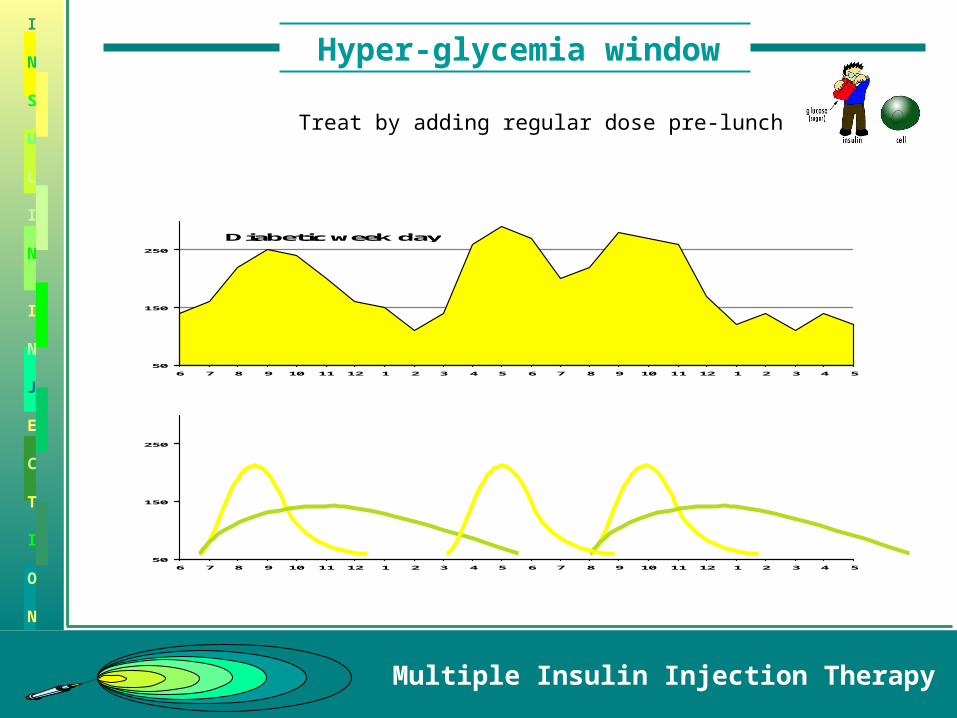
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Diabetic week day
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Treat by adding regular dose pre-lunch
Hyper-glycemia window
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
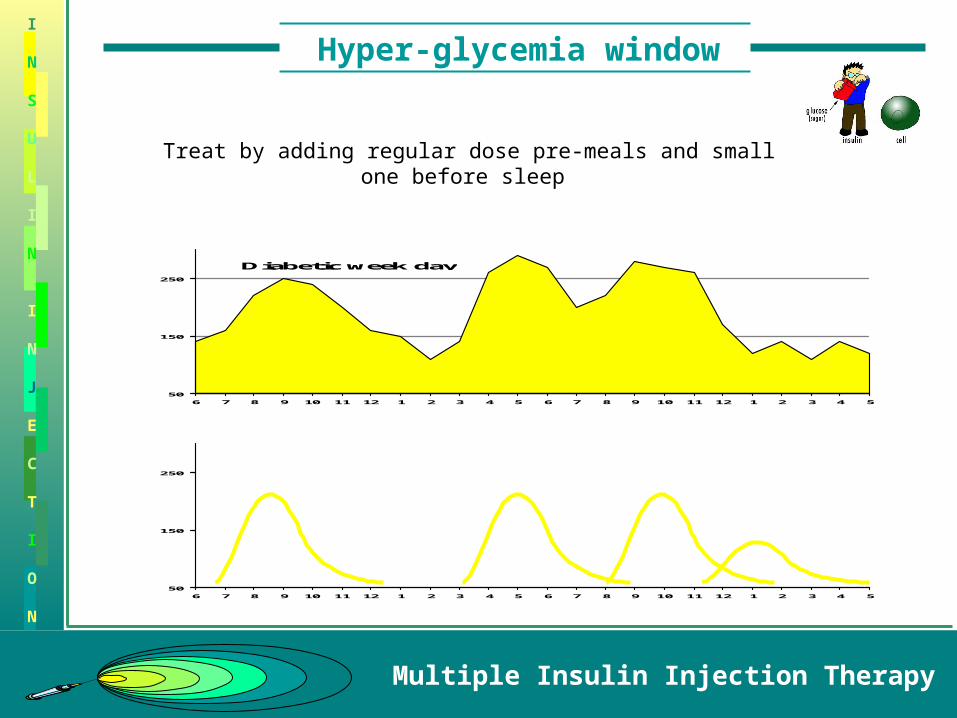
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Diabetic week day
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Treat by adding regular dose pre-meals and small one before sleep
Hypo-glycemia window
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
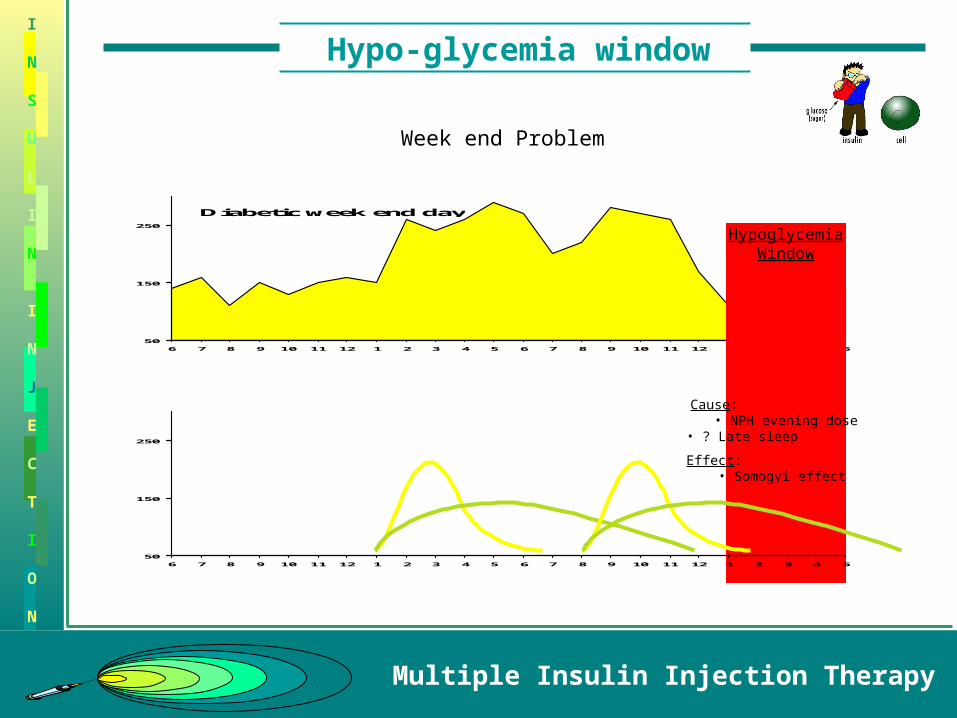
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Diabetic week end day
HypoglycemiaWindow
Cause: • NPH evening dose• ? Late sleep
Effect: • Somogyi effect
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Week end Problem
Hypo-glycemia window
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
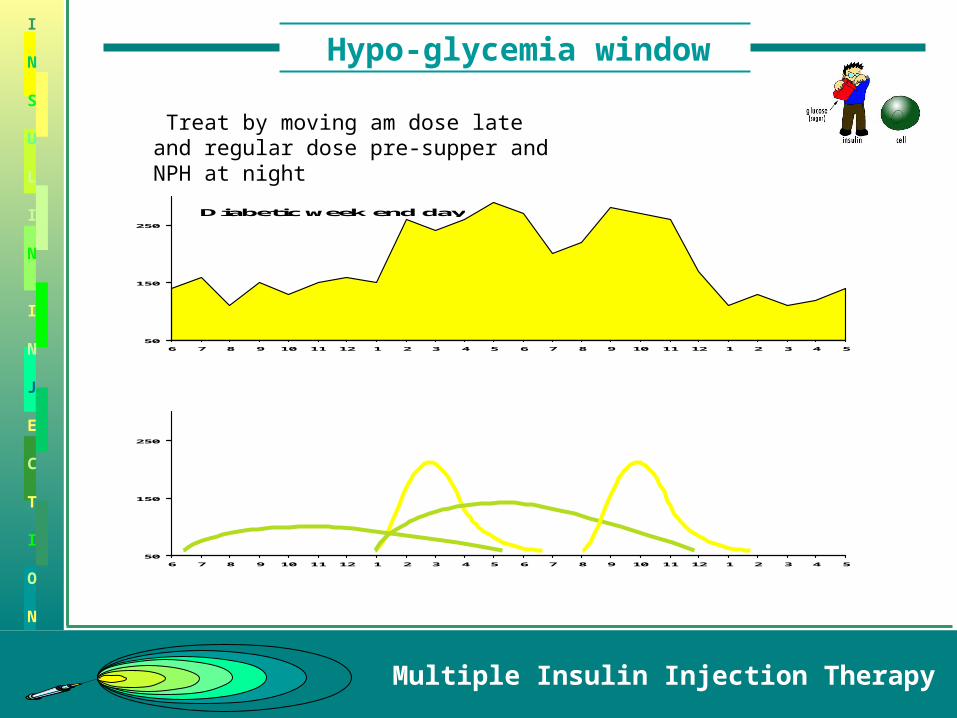
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Diabetic week end day
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Treat by moving am dose late and regular dose pre-supper and NPH at night
Hypo-glycemia window
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
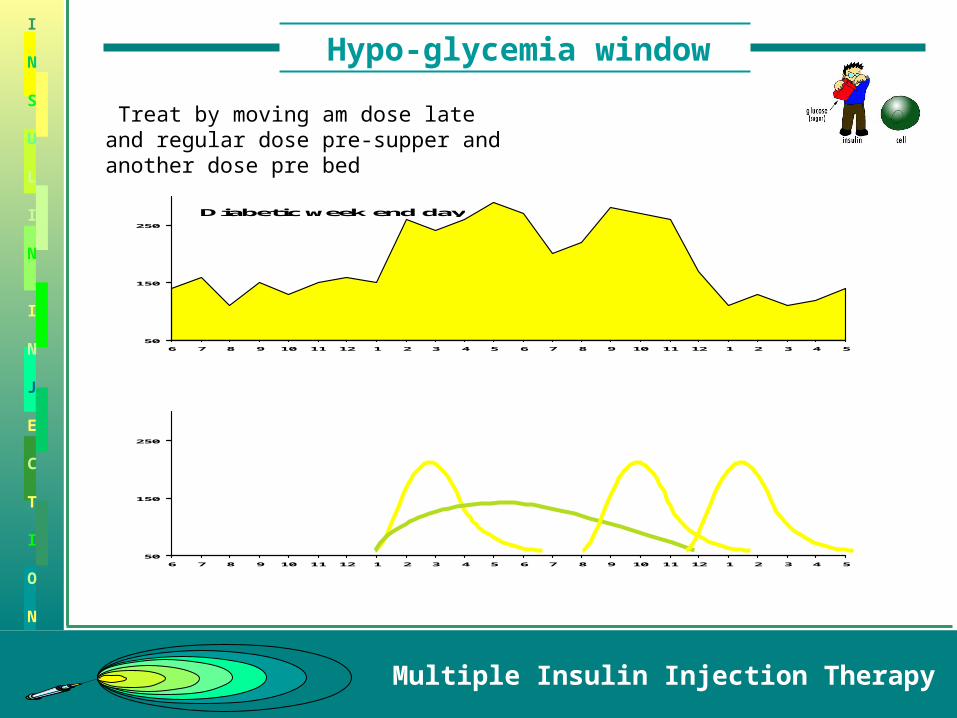
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Diabetic week end day
50
150
250
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5
Treat by moving am dose late and regular dose pre-supper and another dose pre bed
Somogyi Phenomenon
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
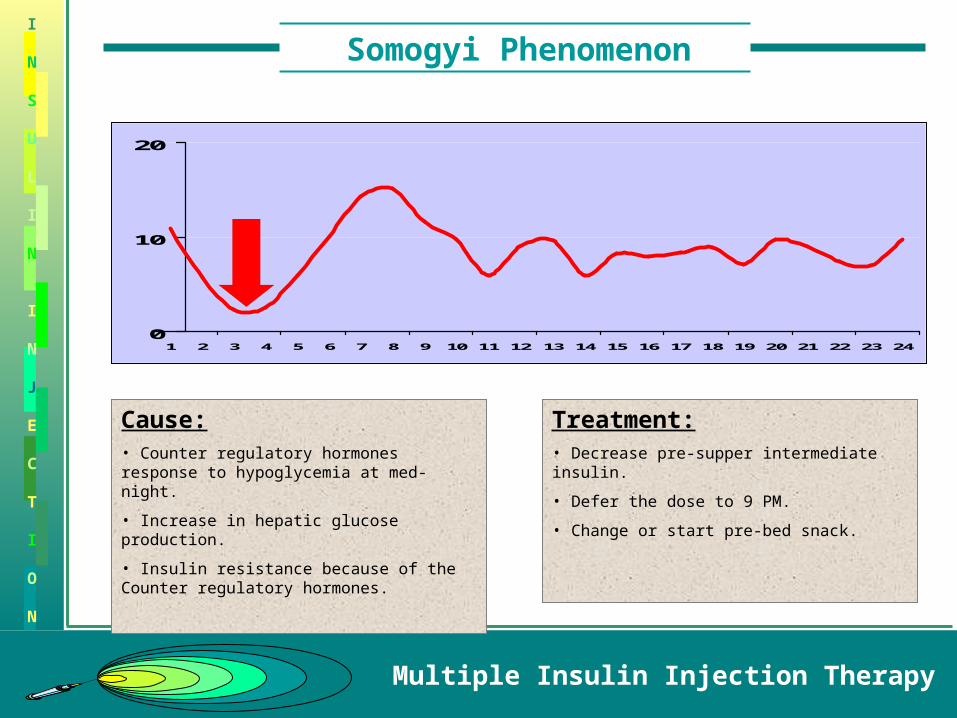
0
10
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Cause:• Counter regulatory hormones response to hypoglycemia at med-night.
• Increase in hepatic glucose production.
• Insulin resistance because of the Counter regulatory hormones.
Treatment:• Decrease pre-supper intermediate insulin.
• Defer the dose to 9 PM.
• Change or start pre-bed snack.
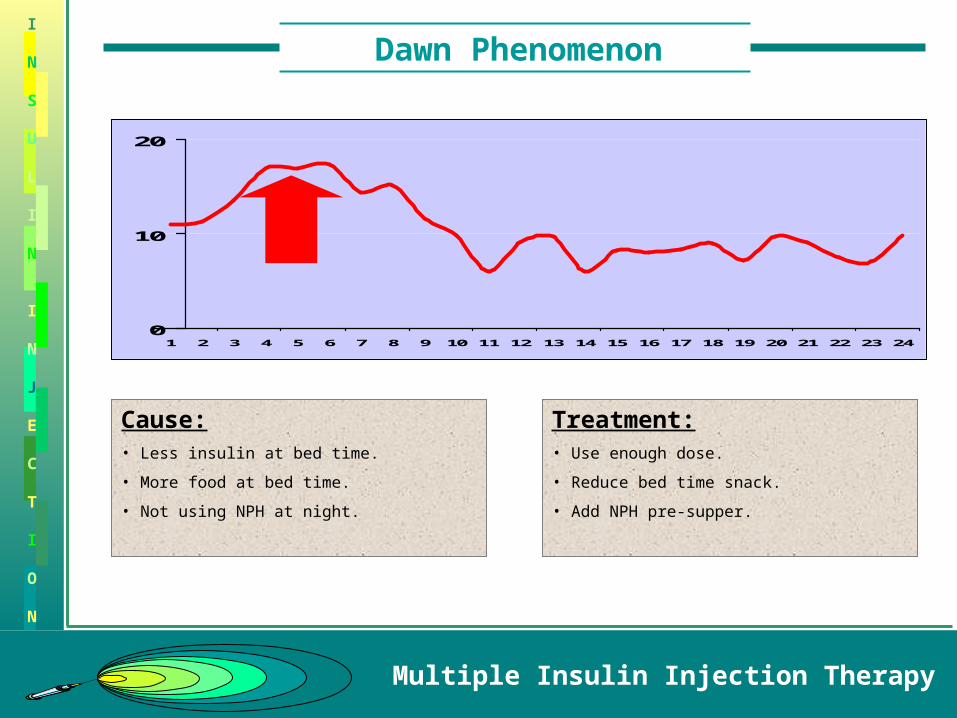
Dawn Phenomenon
Multiple Insulin Injection Therapy
I
N
S
U
L
I
N
I
N
J
E
C
T
I
O
N
0
10
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Cause:• Less insulin at bed time.
• More food at bed time.
• Not using NPH at night.
Treatment:• Use enough dose.
• Reduce bed time snack.
• Add NPH pre-supper.






![Lantus (insulin glargine [rDNA origin] Injection, 100 … · ®insulin glargine [rDNA origin] injection) is a sterile solution of insulin glargine for use as an injection. Insulin](https://img.pdfslide.us/doc/110x75/5b5e31c57f8b9a310a8bf7bc/lantus-insulin-glargine-rdna-origin-injection-100-insulin-glargine-rdna.jpg)






















