Embed Size (px)
Citation preview

www.elsevier.com/locate/jhep
Journal of Hepatology 47 (2007) 142–156
Review
Insulin resistance in hepatocytes and sinusoidal liver cells:Mechanisms and consequences
Isabelle A. Leclercq1,*, Alain Da Silva Morais1, Ben Schroyen2,Noemi Van Hul1, Albert Geerts2
1Laboratory of Gastroenterology, Faculty of Medicine, Universite catholique de Louvain (UCL),
GAEN 53/79, Avenue Mounier, 53, B-1200 Brussels, Belgium2Department of Cell Biology, Vrije Universiteit Brussel (VUB), Brussels, Belgium
Hepatic insulin resistance is an important underlying cause of the metabolic syndrome that manifests itself in diseasessuch as diabetes type II, atherosclerosis or non-alcoholic fatty liver disease (NAFLD). In this paper, we summarize com-
prehensively the current state of knowledge pertaining to the molecular mechanisms that lead to insulin resistance in hepa-
tocytes and sinusoidal liver cells.
In hepatocytes, the insulin resistant state is brought about by at least one, but more likely by a combination, of the fol-
lowing pathological alterations: hyperglycaemia and hyperinsulinaemia, formation of advanced glycation end-products,
increased free fatty acids and their metabolites, oxidative stress and altered profiles of adipocytokines. Insulin resistance
in hepatocytes distorts directly glucose metabolism, especially the control over glucose output into the circulation and
interferes with cell survival and proliferation, while hepatic fatty acid synthesis remains stimulated by compensatory hyper-insulinaemia, resulting in steatosis.
Very few studies have addressed insulin resistance in sinusoidal liver cells. These cells are not simply bystanders and
passive witnesses of the changes affecting the hepatocytes. They are target cells that will respond to the pathological alter-
ations occurring in the insulin resistant state. They are also effector cells that may exacerbate insulin resistance in hepa-
tocytes by increasing oxidative stress and by secreting cytokines such as TNF and IL-6. Moreover, activation of sinusoidal
endothelial cells, Kupffer cells and stellate cells will lead to chemo-attraction of inflammatory cells. Finally, activation of
stellate cells will set in motion a fibrogenic response that paves the way to cirrhosis.
� 2007 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
0168-8278/$32.00 � 2007 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
doi:10.1016/j.jhep.2007.04.002
* Corresponding author. Tel.: +32 2 764 52 73.E-mail address: [email protected] (I.A. Leclercq).Abbreviations: AGE, advanced glycation end-products; AMPK, AMP-dependent kinase; ChREBP, carbohydrate regulatory element-binding
protein; ECM, extracellular matrix; ERK, extracellular regulated kinase; FAS, fatty acid synthase; FFA, free fatty acids; GLUT4, glucose trans-porter-4; GSK-3, glycogen synthase kinase-3; HSC, hepatic stellate cells; IKKb, Inhibitory kappa B kinase beta; IL, interleukin; IR, insulin receptor;IRS, insulin receptor substrate; JNK, c-Jun-N-terminal kinase; KC, Kupffer cells; LPC, liver progenitor cells; MAPK, mitogen-activated proteinkinase; MCD, methionine and choline-deficient; NAFLD/NASH, non-alcoholic fatty liver disease/non-alcoholic steatohepatitis; NF-jB, nuclearfactor-kappa B; PEPCK, phosphoenol-pyruvate carboxy-kinase; PI3K, phosphatidylinositol-3-kinase; PIP3, Phosphatidylinositol (3,4,5) triphos-phate; PKB, protein kinase B; PKC, protein kinase C; PKD1, phosphoinositide-dependent protein kinase; PPAR, peroxisome proliferator-activatedreceptor; RAGE, receptor of advanced glycation end-products; ROS, reactive oxygen species; SEC, sinusoidal endothelial cells; SOCS, suppressor ofcytokine signaling; SREBP-1c, sterol regulatory element-binding protein-1c; TNF, tumor necrosis factor a; VLDL, very low density lipoprotein.

I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156 143
1. Introduction
The metabolic syndrome (visceral adiposity, dyslip-idaemia, hyperglycaemia and hypertension) is a clusterof metabolically related abnormalities predicting anincreased risk for cardio-vascular diseases [1], type IIdiabetes mellitus, non-alcoholic steatohepatitis and cer-tain cancers (Table 1). While the pathogenesis of themetabolic syndrome is not well understood, centralobesity and insulin resistance are acknowledged asimportant causative factors [2,3]. Hypotheses relatingcentral obesity to the metabolic syndrome focus on theconcept that the adipose tissue, and in particular visceraladipose tissue, is a source of factors such as free fattyacids, reactive oxygen species, TNF and other adipocy-tokines, that impair insulin action in muscles and liver.
Insulin is the principal regulator of whole body glu-cose homeostasis, regulating glucose supply accordingto the needs. It promotes glucose disposal in adipose tis-sue and muscles, and prevents the liver from producingmore glucose by inhibition of glycogenolysis and gluco-neogenesis. Insulin also controls other important pro-cesses such as synthesis and storage of fat, proteinsynthesis, cell growth, cell proliferation, survival anddifferentiation. Therefore, assessment of alterations ofglucose homeostasis evaluates only one aspect of insulinresistance. Importantly, organs, cell types and intracel-lular pathways do not present resistance to insulinaction at the same time or to the same extent. Severalcomplications or negative consequences of the insulinresistant state result from adverse impact of compensa-tory hyperinsulinaemia on cell types or intracellularpathways that remain, normally or partially, insulin sen-
Table 1
Metabolic syndrome definition: International Diabetes Federation [1]
Central obesity Waist circumference >94 cmfor men; >80 cm for women a
(adjustment for ethnicity)
Or, BMI > 30 kg/m2
Plus any two
Raised triglycerides > Or = 150 mg/dLOr, treatment for this lipidabnormality
Reduced HDL cholesterol <40 mg/dL in men; <50 mg/dLin womenOr, treatment for this lipidabnormality
Raised blood pressure > Or = 130/85 mm HgOr, treatment of previouslydiagnosed hypertension
Raised fasting plasma glucose > Or =100 mg/dLOr, previously diagnosed type 2diabetes
a Cutoff waist circumferences for white people of European origin.Refer to [1] for cutoff values for other ethnicities.
sitive. This is well exemplified by the polycystic ovariansyndrome or by persistent hepatic de novo lipogenesis.
The liver is an insulin sensitive organ that plays a keyrole in the regulation of the whole body energy homeo-stasis. Insulin resistance in metabolically very activehepatocytes is thus expected to have important systemicconsequences. Besides this, insulin resistance, nowrecognised as a pathological factor in the developmentof non-alcoholic fatty liver disease [4], is also a determi-nant of disease progression in chronic viral hepatitis Cand alcohol-induced liver disease [5]. These clinicalobservations provide further evidence that factors linkedto insulin resistance exert important pathobiologicaleffects on the liver.
The aim of this review is to summarize the alterationsof insulin signaling in individual cell types constitutingthe liver, and to evaluate their functional consequences,at the level of the cell, the organ or the whole body, inthe context of the insulin resistance syndrome.
2. Definitions and assessment of insulin resistance
Systemic insulin resistance is defined as the increasedrequirement for insulin to maintain glucose homeostasis(Fig. 1). Peripheral insulin resistance refers to dimin-ished insulin-mediated uptake of glucose principally byskeletal muscle. It depends primarily on the control ofGLUT4 glucose transporter expression and transloca-tion to the plasma membrane. Hepatic insulin resistancedescribes impaired suppression of hepatic glucose pro-duction, which largely accounts for hyperglycaemiaand glucose intolerance.
The hyperinsulinaemic-euglycaemic clamp method isthe gold standard to assess insulin sensitivity in vivo
[6,7]. In this technique insulin is infused continuously.The amount of glucose to be infused to maintain con-stant blood glucose levels is proportional to the amountof glucose taken up and metabolised by the muscle, andthus to the peripheral insulin sensitivity. Glucose tracers(radioactive or stable isotopes) are used to measure thehepatic glucose output. During the clamp, the suppres-sion of hepatic glucose output by low doses of insulinis a measure of hepatic insulin sensitivity.
Cellular insulin resistance is defined as the alterationof the intracellular propagation of the signals evokedupon activation of the insulin receptor [8]. It is evaluatedby measuring phosphorylation of intermediate proteins,changes in activity of intermediate kinases and/or mod-ulation of target gene expression or target cellular func-tions in response to insulin stimulus.
3. Insulin signaling
Studies from numerous laboratories have elucidatedthe principal features of insulin action at the molecular

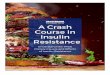
Fig. 1. (a) Insulin regulates glucose homeostasis and maintains normoglycaemia. Insulin favours glucose uptake by adipocytes and skeletal muscles and,
by controlling glucose synthesis and storage, inhibits hepatic glucose output. In addition, insulin inhibits the activity of hormone-sensitive lipoprotein
lipase, and thereby stimulates lipid storage in the adipose tissue. (b) In the insulin resistant state, decreased insulin sensitivity results in decreased glucose
uptake by the peripheral tissues and decreased inhibition of hepatic glucose output. This concurs to hyperglycaemia and compensatory hyperinsulinaemia.
The inhibition of lipoprotein lipase is reduced, leading to increased lipid storage in non-adipose tissues such as the liver and the muscles. This has
significant consequences on insulin signaling in those tissues. In addition, the balance of adipocytokines is altered in fat-laden and insulin resistant adipose
tissue impinging on insulin sensitivity.
144 I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156
level (reviewed in [8–12]). They are schematically repre-sented in Fig. 2. Insulin signaling is triggered by bindingof insulin to its receptor located in the plasma mem-brane of target cells [13]. The insulin receptor (IR) is a
Fig. 2. Schematic representation of intracellular insulin signaling. Upon insulin
(IR) trans-phosphorylates several tyrosine residues, acting as docking sites fo
(including insulin receptor substrates (IRS) 1–6, Shc, Cbl, p62dok, or Gab-1
phosphatidylinositol-3-kinase (PI3K) pathway is mainly involved in the contro
transcription of GLUT4, protein synthesis (via mTOR) and control of cell sur
mediates the mitogenic, growth and cell differentiation effects, and (3) signa
membrane translocation of glucose transporter GLUT4, in GLUT4-expressing
receptor tyrosine kinase that uses docking proteins, suchas insulin receptor substrates (IRS) 1–6, Shc, Cbl,p62dok, and Gab-1, to mediate his signaling [11,14].Tyrosine phosphorylation of IRS by insulin is a crucial
binding, the cytoplasmic kinase domain of the activated insulin receptor
r downstream interacting proteins. Insulin receptor interacting proteins
) are in turn phosphorylated, activating three main pathways: (1) the
l of metabolic actions by insulin (glucose, lipid and protein metabolism),
vival, (2) the mitogen-activated protein kinase (MAPK) pathway which
l transduction through the CAP/Cbl/Tc10 pathway which controls the
cells.

I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156 145
event in mediating insulin action, defective in most casesof insulin resistance, both in experimental models and inhumans [15].
There are three major pathways emanating from theactivated IRS (Fig. 2): (i) the PI3K–Akt pathway whichis mainly involved in the control of metabolic actions byinsulin (glucose, lipid and protein metabolism), (ii) theMAPK pathway which mediates the mitogenic, growthand cell differentiation effects, and (iii) signal transduc-tion through the CAP/Cbl/Tc10 pathway which con-trols the membrane translocation of GLUT4. Inadipocytes and muscle cells, insulin uses the latter path-way to regulate glucose intake. In hepatocytes, glucosetransport is mediated through GLUT2. This transporterresponds to the gradient of glucose concentration acrossthe membrane. Its expression is not regulated by insulin.The physiological control of the rate and direction ofglucose fluxes across the plasma membrane of the hepa-tocyte depends on intracellular glucose phosphoryla-tion/dephosphorylation balance. Insulin promotesindirectly hepatic glucose influx by stimulating glucoki-nase and thus the use of glucose for energy consump-tion, glycogen and lipid synthesis.
3.1. Control of hepatic glucose production
Upon binding of insulin to its receptor, tyrosinephosphorylation of IRS1 and 2 results in the recruit-ment of phosphatidylinositol-3-kinase (PI3K), which
Fig. 3. Regulation of SREBP-1c. The transcription factor sterol regulatory el
lipogenesis. The precursor is retained into the endoplasmic reticulum and can b
Golgi where it is cleaved by specific proteases: the released N-terminal fragment
lipogenesis [19]. In addition, its level of phosphorylation modulates SREBP-1c a
the maturation and activity of SREBP-1c. Insulin regulates the maturation, the
participates in the retention of SREBP-1c in the endoplasmic reticulum.
phosphorylates phosphatidylinositol [4,5] biphosphateinto phosphatidylinositol [3–5] triphosphate (PIP3)[16,17]. PIP3 recruits to the membrane and activatesthe serine/threonine kinases PKD1 and PKB/Akt.The activation of this pathway mediates glycogen syn-thesis, via PKB/Akt inhibitory phosphorylation of gly-cogen synthase kinase 3 (GSK3), a kinase thatnegatively regulates glycogen synthase. It inhibits, viaPKB/Akt-activation of FOXO-1, the transcription ofkey enzymes for gluconeogenesis: phosphoenolpyr-uvate carboxy-kinase (PEPCK) and glucose-6-phos-phatase. Thus through activation of PI3K and PKB/Akt, and subsequent inactivation of GSK3 and activa-tion of FOXO-1, insulin promotes storage of glucoseas glycogen and inhibits glucose synthesis and glucoseoutput.
3.2. Transcriptional control of hepatic lipogenesis
The transcription factor sterol regulatory element-binding protein (SREBP-1c) mediates most of insulin’seffects on lipogenesis, by regulating the entire programof mono-unsaturated fatty acids synthesis [18]. SREBP-1c is subjected to complex regulations [19] (Fig. 3).Several lines of evidence suggest that insulin regulatestranscription, maturation and activity of SREBP-1c[20]. Classically, those pathways remain insulin sensi-tive. Moreover, phosphorylation of SREBP-1c byGSK3 or ERK, an intermediate of the MAPK pathway,
ement-binding protein (SREBP-1c) mediates most of insulin’s effects on
e freed in times of sterol depletion. Free SREBP-1c translocates to the
migrates to the nucleus and activates transcription of genes implicated in
ctivity. Sterol depletion and TNF regulate, in an insulin-independent way,
activity as well as the transcription of SREBP-1c and Insig2a. The latter

146 I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156
modulates its activity. In addition, TNF, the expressionof which is increased in insulin resistant states, stimu-lates the maturation and the activity of SREBP-1c.Thereby, TNF participates in increased intrahepaticlipid synthesis [21] (Fig. 3).
3.3. Cell growth, proliferation and survival
Downstream of IR phosphorylation, IRS, Gab-1 andShc activate the mitogen-activated protein kinase(MAPK) cascade via activation of the G protein Ras(Fig. 2). The MAPK pathway is associated with themitogenic and proliferative effect of insulin via the con-trol of the cell cycle, but it does not appear to have amajor role in mediating insulin effects on hepatic glucoseproduction or on anabolic effects of insulin [10].
The PKB/Akt pathway also participates in mediat-ing the effect of insulin on cell growth and survival.Phosphorylated Akt promotes anti-apoptotic effectsand protein synthesis. The initiation stage of proteintranslation is controlled by eIF2B, a guanine nucleo-tide exchange factor inhibited upon phosphorylationby GSK3, and protein biosynthesis is stimulatedby PKB/Akt-dependent phosphorylation of mTOR[10].
4. Molecular mechanisms for insulin resistance
4.1. Underlying mechanisms
Several mechanisms, acting individually or in syn-ergy, inhibit insulin signaling [8–12]. First, signal propa-gation may be altered by decreased expression (orincreased degradation) of any one of the componentsof the insulin cascade. Increased protein expression oractivation may also act as negative feedback signals.Second, proteins of the pathway may undergo post-translational modifications changing their activity. Inparticular, inhibitory serin phosphorylation of IRS1/2,by various kinases, alters the capacity of this proteinto engage in insulin-receptor signaling [22]. Among theIRS-modifying enzymes, mounting evidence indicatesthat activation of stress-activated protein kinaseJNK1, inhibitory kappa B kinase beta (IKKb) and pro-tein kinase C (PKC) is central to mediating insulin resis-tance in response to various stress factors such asexposure to lipid metabolites and mediators, to pro-inflammatory cytokines, to oxidative stress and to stressof the endoplasmic reticulum (ER stress) (reviewed in[23]). The third level of regulation is the interaction withinhibitory proteins. SOCS proteins are a family of sup-pressors of cytokine signaling induced by inflammatorycytokines, including low-grade inflammation associatedto obesity. SOCS-3 seems to reduce insulin signalingby inhibition of the insulin receptor and by ubiquitin-
mediated degradation of IRS1 and 2 [11,24]. Finally,increased activity of phosphatases will dephosphorylateintermediate proteins and reverse insulin action. Therole of tyrosine phosphatases and PIP3 phosphatasessuch as Pten and SHIP in putting a break on insulin sig-naling is increasingly recognised [25].
4.2. Insulin resistance-inducing factors
Insulin resistance is classically associated with obesity[2]. Although epidemiological correlations are estab-lished, the cellular and molecular mechanisms are onlypartially unravelled. Increased visceral adiposity is asso-ciated with lipid accumulation in the liver. The lattercorrelates with the severity of insulin resistance [26].Growing evidence links a chronic, low-grade inflamma-tory state as well as chronic oxidative stress to the co-existing conditions of obesity, insulin resistance andmetabolic syndrome [27,28]. The production of adipocy-tokines is altered in fat-laden adipocytes. Many adipo-cytokines modulate insulin sensitivity and theinflammatory reaction.
4.2.1. Hyperinsulinaemia and hyperglycaemia
The most obvious clinical parameters modified in theinsulin resistant state are increased glycaemia and thesubsequent compensatory hyperinsulinaemia. Bothhyperinsulinaemia and hyperglycaemia per se are factorsthat exacerbate the insulin resistant state. Hyperinsuli-naemia induces downregulation of the IR at the proteinlevel by ligand internalisation and degradation, andresistance downstream of the receptor by increased deg-radation of IRS1/2 and other insulin signaling molecules[23,29]. In addition, hyperinsulinaemia can damage thepancreatic b-cell and participate in reduced insulinsecretion and type II diabetes (reviewed in [30]). Exper-iments in diabetic Zucker rats and in streptozotocin-induced type I diabetic rats at a stage of hyperglycaemiaand hypoinsulinaemia suggest that hyperglycaemiareduces the efficiency of the activation step from PI3Kto PKB/Akt, but does not affect the proximal part ofthe insulin-receptor mediated pathway [31,32].
Importantly, hyperglycaemia and hyperinsulinaemiaboth concur to stimulate de novo hepatic lipogenesisby activation of the transcription factors carbohydrateregulatory element-binding protein (ChREBP) andSREBP-1c, respectively [20].
4.2.2. Fatty acids
By analogy to the mechanisms of insulin resistanceunravelled in muscle [8,33], the role of fatty acids orfatty acid metabolites in inducing hepatic insulin resis-tance has been explored. There is an inverse correlationbetween hepatic triglyceride stores and insulin sensitivity[26,34,35]. Recent experiments have proposed mechanis-tic links between intrahepatic lipids and insulin

I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156 147
resistance. Kim et al. generated mice in which liver-lipo-protein lipase (LPL) was over-expressed primarily in theliver. As a result of enhanced hydrolysis of triglyceridesfrom chylomicrons and VLDL, these mice accumulatedtriglycerides in the liver only. Severe alterations in hepa-tic insulin signaling were observed, in particular theabsence of tyrosine phosphorylation of IRS2 and down-stream activation of PKB/Akt [36]. Samuel et al. usedrats subjected to a 3-day high fat diet to stimulate hepa-tic fat accumulation [37]. Such a regimen did not alterperipheral insulin sensitivity, fasting plasma glucoseconcentrations or basal rate of hepatic glucose produc-tion. However, insulin infusion during the clamp studyfailed to inhibit hepatic glucose output, demonstratinghepatic insulin resistance. At the molecular level, insu-lin-stimulated phosphorylation of IRS1 and 2 wasblunted. The proposed mechanism is the stimulationof PKC and JNK by increased intracellular fatty acidmetabolites [37]. Thus, fat accumulation alone appearssufficient to induce hepatic insulin resistance. However,this resistance is not sufficient to alter basal hepatic glu-cose production, nor to induce glucose intolerance orperipheral insulin resistance.
4.2.3. Oxidative stress
As mentioned, hepatic steatosis and insulin resistanceare intimately linked. A feature of hepatic steatosis is itsassociation with oxidative stress leading to the inductionof a stress response via JNK and NF-jB [38]. The originof this oxidative stress is under debate. Increased activ-ity of CYP2E1 or CYP4As may contribute to the pro-duction of reactive oxygen species [39]. Interestingly,over-expression of CYP2E1 in hepatic cell lines inducesinsulin resistance by decreasing tyrosine phosphoryla-tion and increasing serine phosphorylation of IRS1/2in response to insulin. This effect partially results fromthe activation of JNK and NF-jB [40]. Other authorssuggest that the increased rate of b-oxidation, associatedwith lipid overload, generates peroxidation products,culminating in NF-jB activation [41]. This propositionis not supported by experimental evidence in animalmodels of steatohepatitis [42]. However, in humans,the generation of peroxidation products by enhancedb-oxidation may have pathologic significance given thechronicity of the steatotic disorder, the association withaltered mitochondrial function and reduced anti-oxidantdefences [43].
4.2.4. Stress of the endoplasmic reticulum
The endoplasmic reticulum (ER) is proposed as a sitefor sensing the metabolic stress and for its translationinto inflammatory signals [23]. All the secretory andmembrane proteins are folded into their secondary andtertiary structures in the ER. Stress of the ER is createdfrom accumulation of unfolded proteins, energy andnutrient fluctuation, hypoxia, toxins and increased
demand on synthetic machinery. Recent studies con-firmed that in genetic and dietary models of obesityER stress is increased in the adipose tissue and in theliver [44]. Notably, the two principal inflammatory path-ways that disrupt insulin action, namely JNK andIKKb, are linked to the unfolded protein response acti-vated during ER stress. Subsequently, a close linkbetween ER stress and insulin sensitivity has been dem-onstrated in vitro and in vivo [45].
4.2.5. Glycated proteins and advanced glycation end-
products
Glucose reacts slowly (non-enzymatically) with freeamino groups of proteins to form glycation products.The level of glycated haemoglobin is a widely used indi-cator to assess occurrence of hyperglycaemia. Insulinitself has been shown to be glycated, resulting inimpaired biological activity [46]. Glycation productsare further degraded to advanced glycation end-prod-ucts (AGEs), a process accelerated by oxidative stress[47]. Increased AGEs and interaction with cellularreceptor RAGE have been implicated in the pathogene-sis of diabetic complications. During chronic hyper-glycaemia, the soluble form of RAGE (sRAGE),acting as a scavenger receptor, is downregulated. Thisenhances the noxious consequences of AGEs [48]. Inanimal models, there is a positive correlation betweendietary AGE/glycoxidation products and insulin sensi-tivity [49,50]. Methylglyoxal, the most important precur-sor to yield irreversible AGE, impairs insulin signaling:methylglyoxal appears to form a complex with IRS thatinduces conformational changes affecting the tyrosinephosphorylation and the docking function of these pro-teins [51].
4.2.6. Adipocytokines
The adipose tissue serves as a key site for the interac-tion of adipocytes with effector cells of the inflammatoryand immune system and for the production of adipocy-tokines. These peptides have important properties asmodulators of insulin sensitivity, lipid metabolism,inflammatory and immune reactions, inside the adiposetissue and more importantly on distant organs such asthe liver (reviewed in [52–54]). Alterations in secretionof adipocytokines are specifically relevant in obesity,insulin resistance and the metabolic syndrome. Table 2summarizes the main adipocytokines and their effectson liver cells.
Adiponectin is the most abundant adipocytokine inplasma. Its production decreases with adiposity andinsulin resistance. It circulates in the bloodstream asmultimere of full-length proteins or as cleaved proteinscontaining the globular domain only [55]. Adiponectinhas anti-inflammatory properties, increases the sensitiv-ity of hepatocytes to insulin-mediated inhibition of glu-coneogenesis and hepatic glucose output, and regulates

Table 2
Adipocytokines and their effects on hepatic cells
Subtype Adipocytokine Effect on hepatocytes[52–54]
Effect on stellate cells[121,122]
Effect on Kupffer cells Effect on sinusoidalendothelial cells
Cytokines TNF Induces insulin resitance Anti-fibrogenic, orpro-fibrogenic
Activation Unknown
IL-6 Causes insulin resistance(SOCS-3-dependent)
Pro-fibrogenic Activation Protection againstnecroapoptosis
Chemokines MCP-1 Unknown Activation of PI3K Recruitment UnknownStimulation of migration [73]
Growth factors VEGF Unknown PI3K/Akt & ERK/MAPKphosphorylation
Unknown Stimulation ofproliferation &increased permeability
Hormones Leptin Ameliorates insulinresistance
Pro-fibrogenic [108,109] Up-regulates TGF-b1[109,115]
Up-regulates TGF-b1 ?[109]
Adiponectin Increases insulinsensitivity
Anti-fibrogenic [119,120] Anti-inflammatory[117,118]
Unknown
Resistin Causes insulin resistance Unknown Unknown UnknownASP Unknown Unknown Unknown UnknownVisfatin Ameliorates insulin
resistanceUnknown Unknown Unknown
Adipsin Unknown Unknown Unknown Unknown
Vaso-activepeptides
Angiotensinogen Unknown Pro-fibrogenic (whenconverted to angiotensin II)
Pro-inflammatory(when convertedto angiotensin II)
Unknown
Inhibitor offibrinolysis
PAI-1 Unknown Pro-fibrogenic Unknown Unknown
TNF, tumor necrosis factor; IL-6, interleukin 6; MCP-1, monocyte chemoattractant protein 1; VEGF, vascular endothelial growth factor; ASP,acylation stimulating protein; PAI-1, plasminogen activator inhibitor-1.
148 I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156
hepatic FFA metabolism via suppression of lipogenesisand activation of fatty acid oxidation [54,55]. Adiponec-tin exerts its effects by binding to its receptors. Hepato-cytes express mainly adipoR2, which binds with equalaffinity the full-length and the cleaved globular formof adiponectin. Upon adiponectin binding, the receptorelicits activation of the transcription factor peroxisomeproliferator-activated receptor (PPAR) a and stimulatesthe activity of AMP-dependent kinase (AMPK) [56].Activation of PPARa enhances transcription of theenzymes of the fatty acid b-oxidation machinery [57]and has anti-inflammatory consequences, probablythrough transrepression of NF-jB [58]. The activationof AMPK, via regulation of acyl CoA-carboxylaseactivity and intracellular malonyl-CoA concentrations,inhibits de novo lipogenesis and favours fatty acid b-oxi-dation [56]. Thus, adiponectin combats intrahepaticlipid accumulation. This mechanism is largely impli-cated in the insulin sensitising effect of adiponectin. InNAFLD patients, serum adiponectin is negatively corre-lated to hepatic insulin resistance and to the amount offat in the liver [59].
Tumor necrosis factor a (TNF) is an important pro-inflammatory cytokine that plays a central role in insu-lin resistance. Several, possibly cumulative, mechanismsby which TNF may impair insulin signaling have beenproposed.
First, TNF represses genes involved in uptake andstorage of non-esterified fatty acids in the adipose tis-sue [60]. Those fatty acids are thus readily availablefor the liver, and increase the pool of intrahepaticFFA. Second, TNF activates JNK and IKKb. Thisresults in serin phosphorylation of IRS and inhibitionof insulin signaling [11,23]. Additionally, JNK activa-tion induces TNF, therefore representing an auto-crine/paracrine loop potentiating insulin resistance.Several lines of evidence support the role of TNF/NF-jB-mediated activation of IKKb as a mechanismfor insulin resistance. Mice lacking TNF or TNF-receptors have improved insulin sensitivity in bothdietary and genetic models of obesity [61]. High dosesalicylate inhibits IKKb activity [62] and reversesinsulin resistance, hyperglycaemia and hyperinsulina-emia in obese and diabetic rodents [63], while hetero-zygous depletion of IKKb protects against thedevelopment of insulin resistance during high fatfeeding [64]. Conversely, mice with chronic hepatocel-lular activation of NF-jB, resulting in continuousactivation of IKKb, have insulin resistance and a dia-betic phenotype [65]. Third, TNF is a potent pro-inflammatory cytokine, which favours IL-6 andrelated SOCS-3 production [66–68]. The latter blocksthe activity of the insulin receptor. Finally, adiponec-tin and TNF suppress each other’s production and

I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156 149
activity [54,55]. In conditions of obesity, high TNFand low adiponectin cooperate to the developmentof insulin resistance.
Interleukin-6: In non-inflammatory conditions, one-third of circulating IL-6 originates from adipose tissue.Circulating IL-6 is strongly associated with obesityand is a predictor of development of type II diabetes.IL-6 is an inhibitor of insulin signaling in isolated hepa-tocytes and in the liver of experimental animals [67,69].In models of genetic or diet-induced obesity, injectionsof IL-6 neutralizing antibodies allow normalisation ofIR phosphorylation in response to insulin and increaseinsulin-mediated suppression of hepatic glucose output[70]. This improvement of insulin signaling is restrictedto the liver. Glucose uptake and insulin resistance inmuscle and adipose tissue are not affected. It remainsto be confirmed whether IL-6-dependent transcriptionalactivation of SOCS-3 is responsible for the inhibition ofthe IR.
Leptin, produced by adipose tissue, may be seen as ananti-steatotic hormone protecting non-adipose tissuefrom fat accumulation and lipotoxicity [71]. Interest-ingly, in obesity and states of insulin resistance, the pro-tective effects of hyperleptinaemia seem to be limited dueto leptin resistance [72].
5. Insulin resistance in hepatocytes
5.1. Pivotal role of hepatic insulin resistance forhyperglycaemia, glucose intolerance and the metabolic
syndrome
Hepatic insulin resistance refers to impaired suppres-sion by insulin of glucose production by hepatocytes[9]. Failure of insulin to inhibit hepatic gluconeogenesisand glycogenolysis is to a large extent responsible forthe development of fasting hyperglycaemia and persis-tent stimulation of insulin production by pancreaticb-cells. Animals with tissue specific deletion of the IRhave been invaluable to dissect single components ofinsulin signaling and to demonstrate the importanceof the liver for insulin resistance (reviewed in [10,73]).Mice lacking IR in hepatocytes exhibit dramatic insulinresistance, severe glucose intolerance and failure ofinsulin to regulate hepatic gene expression and to sup-press hepatic glucose output [74]. In contrast, normalglucose and insulin levels are found in mice with a dele-tion of IR in skeletal muscle [75,76]. Deletion of IR inthe adipose tissue is associated with low insulin levelssuggesting improved insulin sensitivity [77]. When IRis simultaneously knocked down in fat and muscle,there is no change in glucose or insulin levels. Thus,hepatic insulin resistance, but not peripheral insulinresistance, is necessary to develop hyperglycaemia andglucose intolerance.
5.2. De novo lipogenesis remains stimulated by
hyperinsulinaemia in the insulin resistant hepatocyte
In obesity, increased adipocyte mass and insulinresistance, especially in visceral adipose tissue, contrib-utes to elevated plasma levels of FFAs through lipoly-sis. As the rate of hepatic FFA uptake is directlyproportional to plasma FFA concentrations, increasedlipolysis appears as the major contributor to intrahe-patic lipid accumulation. In addition, de novo lipogene-sis is activated by glucose and hyperinsulinaemiathrough activation of ChREBP, SREBP-1c [20], andby low-grade inflammation and increased TNF(Fig. 3). Increased de novo lipogenesis in hepatocytesis indeed observed in NAFLD patients with hepaticinsulin resistance. While in normal subjects, the contri-bution of hepatic de novo lipogenesis to the pool ofhepatic fatty acids is less than 5%, it increases up to25% in NAFLD patients [4]. Thus, fat accumulationin the hepatocytes is a direct consequence of insulinresistance in the adipose tissue and of hyperinsulina-emia. Hepatic insulin resistance contributes indirectlyto hepatic steatosis by increasing glucose levels andworsening hyperinsulinaemia.
5.3. Consequences of insulin resistance for the control of
survival and proliferation of hepatocytes
Insulin is a co-mitogen for numerous cell types. TheMAPK pathway is associated with the proliferativeeffects of insulin (Fig. 2). Pharmacological inhibitorsand dominant negative mutants of intermediate proteinsof this cascade reduce insulin-mediated cell growth buthave little impact on metabolic effects [10]. Activationby insulin of the PI3K/Akt/p70S6K/mTor pathwaycontrols protein synthesis which is of paramount impor-tance during cell proliferation [78].
As demonstrated experimentally, insulin signaling inhepatocytes is required to maintain hepatic functionand to allow liver regeneration [74,79]. Insulin may benecessary to meet metabolic demands imposed by thisenergy consuming process. Additionally, competenthepatic insulin signaling may be pivotal for normalfunction/activation of pathways controlling cell cycleand cell differentiation. In hypoinsulinaemic streptozo-tocin treated rats, normal liver regeneration is observedat the expense of an adaptative increase of insulinsensitivity of hepatocytes [80]. Conversely, constitutivehepatic insulin hypersensitivity in mice with a hepato-cyte-specific Pten deficiency is associated with enhancedproliferation of hepatocytes and hepatocellular carci-noma. Pten is a phosphatase with a main substratePIP3. When Pten is deficient, the half-life of PIP3 isincreased and PKB/Akt and MAPK are thereby consti-tutively activated [81].

150 I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156
Several groups have explored the consequences offatty liver on hepatic cell proliferation. The restorationof liver mass after partial hepatectomy is near to normalin models of hepatic steatosis due to impaired VLDLexport, decreased b-oxidation or in MCD diet-inducedsteatohepatitis (reviewed in [82]). By contrast, liverregeneration is impaired in rodents with disrupted leptinsignaling [83], or in rodents fed a high fat diet [84]; bothbeing associated with insulin resistance.
Although insulin clearly participates in the control ofcell cycle and cell survival pathways in hepatocytes, theeffects of intrahepatic insulin resistance on proliferationand apoptosis, and during the wound healing processremain to be explored. This has clinical relevance sinceincreased susceptibility to apoptosis coupled to impairedregeneration with failure to replace damaged hepato-cytes could participate in the liver pathology associatedwith the metabolic syndrome.
6. Consequences of insulin resistance for liver progenitor
cells
Liver progenitor cells (LPCs) are bipotent cellslocated in terminal branches of the bile ductules andthe canals of Hering. LPCs give rise to hepatocytesand to bile duct epithelial cells. In adult wild typemice, LPCs are scarce. By contrast, in the liver ofobese and insulin resistant ob/ob mice, Yang et al.demonstrated the expansion of progenitor cells [85].This phenomenon has also been described in the liverof patients with NASH [86]. The significance of prolif-eration of progenitor cells is still debated but mightrepresent an adaptative response of the organ in theface of chronic cell loss and replicative senescence ofmature hepatocytes [85,86]. Further studies are neededto analyse whether insulin itself, intracellular insulinresistance or the changes in cellular environment asso-ciated with the insulin resistant state influence thebehaviour of LPCs.
7. Insulin resistance in sinusoidal cells
Besides parenchymal cells, the liver also containssinusoidal cells (around 35% of total liver cells). Thosecells exert important functions in liver morphology,function, defence and wound healing. Kupffer cells(KC) are liver-resident macrophages, with key functionin innate immunity and in parenchymal inflammation[87]. Sinusoidal endothelial cells (SEC) form the fenes-trated endothelium in the liver parenchyma. These scav-enger cells are able to secrete a large array of cytokinesor modulators of matrix homeostasis with paracrine orsystemic effects [88]. Hepatic stellate cells (HSC) are sit-uated in the space of Disse, lining SEC. They exertimportant functions such as the storage and homeostasis
of retinoids, the synthesis and remodelling of extracellu-lar matrix, the regulation of vascular tone of the sinu-soids and the propagation of neural signals [89]. Uponliver injury of different origin, HSC are activated andchange to proliferative, fibrogenic and contractile myo-fibroblast-like cells [90]. Those are the main effector cellsof hepatic fibrosis.
7.1. Insulin responsiveness and insulin resistance in
sinusoidal cells
The literature provides scarce information regardinginsulin sensitivity of sinusoidal cells and as to whetherhepatic sinusoidal cells develop insulin resistance.
The expression of the insulin receptor on KC is stillcontroversial. SEC carry the insulin receptor. They bindand take up insulin with a high binding affinity, and par-ticipate in the hepatic clearance of insulin [91]. Theabsence of alteration of glucose homeostasis in mice car-rying a specific deletion of the insulin receptor in vascu-lar endothelial cells (including SEC) suggests that thiscell type participates marginally in the control of wholebody glucose balance. This deletion however protectsagainst neo-vascularization under conditions of relativehypoxia and may also have effects on vascular haemody-namics [10,73]. The importance of competent insulin sig-naling in SEC for liver function and wound healingduring pathological insults has not been explored.
The effect of insulin on HSC is unclear. In someexperimental conditions, insulin has been shown to stim-ulate the MAPK and PI3K signal transduction path-ways and cell proliferation [92,93]. In our hands, highinsulin concentrations have no direct effect on prolifera-tion, activation or collagen mRNA synthesis of humanactivated HSC (Durnez et al. submitted). Recently, Tsu-kamoto’s group has demonstrated that exposure of qui-escent rat primary HSC to insulin induced thephosphorylation of IR, IRS1 and Akt, and stimulatedglucose uptake. In activated stellate cells, IR and IRSwere hyperphosphorylated. Exposure to insulin failedto further activate the IRS/Akt pathway or to induceglucose uptake [94]. These data suggest that the degreeof insulin sensitivity is dependent on the state of activa-tion of HSC.
7.2. Reactions of sinusoidal cells to insulin resistance-inducing factors
The second question of importance is how the hepaticsinusoidal cells react to the many consequences of insu-lin resistance.
All the sequelae of systemic insulin resistance (hyper-glycaemia, hyperinsulinaemia, increased fatty acids,altered adipocytokine profile, intra- and extracellularAGE, etc.) contribute to arterial endothelial dysfunction[95]. Under the influence of these pathological factors,

I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156 151
endothelial cells undergo dramatic functional alterations[96]. Whether similar changes occur in venous, capillaryor sinusoidal endothelial cells of the liver remains to beinvestigated.
7.2.1. Effects of increased glucose concentrationsA role for hyperglycaemia in the activation of HSC
and in the pathogenesis of fibrogenesis has beenproposed. Experimental evidence suggests that connec-tive tissue growth factor (CTGF), a known fibrogenicfactor, could be involved: high glucose (5–30 mM) orhigh insulin (20 UI/mL) concentrations stimulatedCTGF mRNA and protein synthesis in rat HSC [97]at levels able to enhance significantly collagen expres-sion, proliferation and migration of HSC [98].
7.2.2. AGEs, oxidative stress and hepatic sinusoidal cells
Up to 60% of total liver AGEs, generated during con-ditions of hyperglycaemia, are taken up by SEC and20% by KC [99]. This uptake is dependent on scavengerreceptors CD36, SR1 and SR2. Several reports showthat AGEs have an important impact on cytokinerelease and oxidative stress leading to vascular compli-cations and inflammatory reaction [100]. The influenceof AGEs on liver sinusoidal endothelial cells and resi-dent macrophages has not been explored yet.
HSC are the only liver cell type to express the specificAGE receptor RAGE. Its expression is increased in acti-vated HSC, and is modulated by TGFb1 [101]. Ligandactivation of RAGE leads to formation of reactive oxy-gen species and induction of MAPK and NF-jB signal-ing pathways. The correlation between RAGEactivation, HSC trans-differentiation and fibrogenesisremains to be clarified.
Oxidative stress stimulates the deposition of excessECM in the liver through activation of HSC [102]. Manyanti-oxidants have proven hepato-protective and anti-fibrotic effects [103]. Activation of HSC occurs by directinteraction with oxygen radicals or via endogenous/exog-enous interaction with lipid peroxidation products mal-ondialdehyde or 4-hydroxynonenal [102–104].
Besides being exposed to oxidative stress, HSC, KCand inflammatory cells recruited to the liver also pro-duce ROS mainly through increased activity of NADPHoxidase [105,106]. Whether and to which extent this oxi-dative stress generated by these cells participates inhepatic insulin resistance has not been studied.
7.2.3. Adipocytokines and sinusoidal cells
Many adipocyte-derived proteins modulate immu-nity, inflammation and fibrogenesis in the liver.
Leptin has pro-inflammatory effects in the liver [107]and has been linked to fibrogenesis [108,109]. The liter-ature provides contradictory data on the mechanismsimplicated. Leptin may interact with the long form ofthe leptin receptor (ObRb) expressed on HSC to stimu-
late the transcription of pro-fibrotic genes [110,111], andto increase mitogenesis and cell survival through activa-tion of the MAPK and Akt pathways [112,113]. Otherstudies using rodent primary HSC did not confirmObRb expression, or leptin-dependent activation ofJAK/STAT signaling pathway [109,114,115]. In thosestudies, leptin-dependent stimulation of TGFb1 expres-sion and release by KC or SEC [109,115,116] is pro-posed as indirect mechanism by which leptin influencesfibrogenesis. In the metabolic syndrome, circulating lev-els of leptin are generally elevated, but it appears moreand more that the effects of hyperleptinaemia are largelyprevented by the development of a state of leptin resis-tance. Whether resistance to leptin action occurs inhepatic sinusoidal cells is unknown.
Adiponectin has anti-inflammatory properties, bydirect signaling and by opposing the synthesis, therelease and the effects of TNF from macrophages withinthe adipose tissue and from KC. In KC, adiponectinreduces LPS-stimulated ROS production, TNF expres-sion and enhances the release of anti-inflammatoryIL-10 [117,118]. Conversely, LPS and inflammatorycytokines induce adiponectin expression in spleen andperitoneal macrophages. Whether adiponectin produc-tion by activated KC may represent a mechanism tocontrol the intensity of hepatic inflammatory reactionand hepatic insulin sensitivity remains to be addressed.
Mice lacking adiponectin are exquisitely sensitive tohepatic fibrosis while supra-physiological levels ofadiponectin prevent CCl4-induced fibrosis in wild typemice [119]. Ding et al. have found expression of adipo-nectin receptors AdipoR1 and R2 on cell membranesof primary rat HSC, both at the quiescent and activatedstate [120]. Adiponectin prevents activation, prolifera-tion and migration of quiescent HSC [119,120]. Whenapplied on activated cells, adiponectin induces apoptosis[120] suggesting that adiponectin may counteract fibro-sis by eliminating fibrogenic effector cells. Hypoadipo-nectinaemia such as associated to the metabolicsyndrome may therefore enhance fibrogenesis. However,adiponectin activity strongly depends upon metabolicmilieu, inflammatory pattern and receptor expression.Adiponectin concentrations in the plasma and liver donot always run parallel.
In obese and/or diabetic subjects increased serum lev-els of TNF and IL-6 originate largely from the adiposetissue. However, KC are capable of releasing, amongother factors, large quantities of TNF and IL-6 directlyin contact with liver cells. Those influence hepatic inflam-mation and fibrogenesis [121,122]. They may also act onhepatocytes to worsen insulin resistance and fatty liver.
7.3. Sinusoidal cells as actors of insulin resistance?
The last important question concerns the role of hepa-tic sinusoidal cells in the induction of intrahepatic and

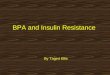
Fig. 4. Intrahepatic insulin resistance: possible interactions between sinusoidal cells and hepatocytes. Hyperglycaemia, hyperinsulinaemia, increased free
fatty acids (FFA) and increased intracellular fatty acids, reactive oxygen species (ROS) and advanced glycation end-products (AGEs), altered balance of
adipocytokines and the low-grade inflammation, all concur and participate in intrahepatic insulin resistance. Those factors are able to alter the biology of
sinusoidal cells, in ways that are only partially understood. Whether those factors also induce insulin resistance in sinusoidal cells, and in the affirmative,
whether signaling modifications alter the biology of those cells have been poorly explored. Sinusoidal cells produce reactive oxygen species (ROS) and a
large array of bioactive peptides. Whether those are implicated, via paracrine stimulations, in hepatic insulin resistance remains to be investigated. KC,
Kupffer cells; HSC, hepatic stellate cells; SEC, sinusoidal endothelial cells.
152 I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156
systemic insulin resistance (Fig. 4). The adipose tissuehas attracted a lot of attention as a pathogenic site ofobesity-induced insulin resistance, because of the meta-bolic alterations, the change in adipocytokine produc-tion and the inflammatory state of this organ. Asunderlined by Shoelson et al. [123], the fatty liver, asso-ciated with obesity and insulin resistance, resembles theadipose tissue. As in adipose tissue, fat-laden metaboliccells (the hepatocytes) are in close proximity to macro-phages (the Kupffer cells) and are surrounded by a vastnetwork of vascular structures (the hepatic sinusoids).NASH is the hepatic complication of the metabolic syn-drome. Hepatic inflammation and fibrosis may resultfrom the exposure of the (fatty) liver to metabolic andpro-inflammatory mediators, produced by visceral fatand drained by the portal circulation. It is however alsoplausible that steatosis may induce a low-grade inflam-matory response, similar to the adipose tissue inflamma-tion that follows adipocyte lipid accumulation. The liveris densely (and permanently) populated by professionalcytokine producing Kupffer cells, and other immunecells. Inflammatory cells may influence systemic andintrahepatic insulin sensitivity as demonstrated in micewith genetic modulation of the IKKb system in myeloidcells [27]. Moreover, adoptive transfer of NKT cells,which are functionally and numerically deficient in theliver of obese, diabetic and severely steatotic ob/ob mice,improves fatty liver and glucose tolerance [124]. Thisreinforces the concept that hepatic non-parenchymalcells may be effectors of insulin resistance and metabolicsyndrome.
Thus, hyperglycaemia, AGEs, oxidative stress, andaltered adipocytokine balance are all risk factors forintrahepatic inflammation and fibrosis. Those factorsactivate cells of the sinusoids to produce large quantitiesof cytokines. Whether those cytokines released in theclose vicinity of hepatocytes participate, via paracrine
stimulation, in hepatic insulin resistance and in the met-abolic syndrome remains to be investigated.
8. Unresolved questions and perspectives for further
research
At the molecular level, insulin resistance can beacquired through multiple mechanisms, and may affectvarious steps in the insulin signaling cascade. This maylead to various forms of insulin resistance. As far asinsulin resistance in hepatocytes is concerned, not allinsulin signaling pathways are affected in the sameway. The PKB/Akt pathway that controls ultimatelygluconeogenesis and glycogenolysis is severely affectedwhich leads to loss of control over glucose output, thecause of hyperglycaemia and compensatory hyperinsuli-naemia. On the contrary, hepatic fatty acid synthesiswhich is largely controlled by the transcription factorSREBP-1c does not seem to be affected in the insulinresistant state. Because of the compensatory hyperinsu-linaemia, it may even be stimulated.
The hepatocyte plays undoubtedly a prominent rolein the development of hepatic and systemic insulin resis-tance, but the liver is more than hepatocytes alone. Insu-lin resistance in sinusoidal liver cells is largely terra
incognita. How do these cells react to the pathologicalchanges associated with insulin resistance? Are they sim-ply bystanders that are not affected by what happens inthe hepatocytes? Are these cells target cells that developtheir own form of insulin resistance? Do they respond totheir changing environment by secreting soluble factorsthat influence hepatocytes and/or recruit inflammatorycells? To what extent do these cells participate in theload of adipocytokines in the liver? Are they able toinduce or modulate insulin signaling in hepatocytes?These questions require more in-depth analysis beforewe can give definitive answers.

I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156 153
Many issues regarding the pathogenesis of insulinresistance in liver cells remain unresolved. Further stud-ies in animal models, in particular in transgenic mice,will be needed. Then, animal data must be verified incohorts of well-characterized patients. Insight into thepathogenesis of insulin resistance related diseases willpave the way to new therapeutic modalities for non-alcoholic fatty liver disease.
Acknowledgements
This work has been supported by grants from the Bel-gian ‘‘Fonds National de la Recherche Scientifique’’(FNRS conventions Nos.: 3.4507.04 and 3.4578.07;IL), from ‘‘Fonds voor Wetenschappelijk Onderzoek –Vlaanderen’’ (FWO-V G.0512.04; AG), la Direction dela Recherche Scientifique de la Communaute Francaisede Belgique (Action de Recherche Concertee, Grant05/10-328; IL), from Onderzoeksraad Vrije UniversiteitBrussel (project OZR 1149BOF; AG), and from theEuropean Union (Sixth Framework program, HEPA-DIP, contract LSHM-CT-2005-018734; AG). IL isResearch Associate for the FNRS.
References
[1] Alberti KG, Zimmet P, Shaw J. The metabolic syndrome – a newworldwide definition. Lancet 2005;366:1059–1062.
[2] Despres JP, Lemieux I. Abdominal obesity and metabolicsyndrome. Nature 2006;444:881–887.
[3] Anderson PJ, Critchley JA, Chan JC, Cockram CS, Lee ZS,Thomas GN, et al. Factor analysis of the metabolic syndrome:obesity vs insulin resistance as the central abnormality. Int JObes Relat Metab Disord 2001;25:1782–1788.
[4] Bugianesi E, McCullough AJ, Marchesini G. Insulin resistance: ametabolic pathway to chronic liver disease. Hepatology2005;42:987–1000.
[5] Hickman IJ, Clouston AD, Macdonald GA, Purdie DM, PrinsJB, Ash S, et al. Effect of weight reduction on liver histology andbiochemistry in patients with chronic hepatitis C. Gut2002;51:89–94.
[6] Defronzo RA, Tobin JD, Andres R. Glucose clamp technique: amethod for quantifying insulin secretion and resistance. Am JPhysiol 1979;237:E214–E223.
[7] Samuel VT, Shulman GI. Insulin resistance in NAFLD:potential mechanisms and therapies. In: Farrell GC, George J,Hall P, McCullough AJ, editors. Fatty Liver Disease – NASHand related disorders. Oxford Publishing Ltd.: Blackwell; 2004.p. 38–54.
[8] Shulman GI. Cellular mechanisms of insulin resistance. J ClinInvest 2000;106:171–176.
[9] Reaven GM. Pathophysiology of insulin resistance in humandisease. Physiol Rev 1995;75:473–486.
[10] Biddinger SB, Kahn CR. FROM MICE TO MEN: insights intothe insulin resistance syndromes. Annu Rev Physiol2006;68:123–158.
[11] Taniguchi CM, Emanuelli B, Kahn CR. Critical nodes insignalling pathways: insights into insulin action. Nat Rev MolCell Biol 2006;7:85–96.
[12] White MF. IRS proteins and the common path to diabetes. Am JPhysiol Endocrinol Metab 2002;283:E413–E422.
[13] De Meyts P, Whittaker J. Structural biology of insulin and IGF1receptors: implications for drug design. Nat Rev Drug Discov2002;1:769–783.
[14] Cai D, Dhe-Paganon S, Melendez PA, Lee J, Shoelson SE. Twonew substrates in insulin signaling, IRS5/DOK4 and IRS6/DOK5. J Biol Chem 2003;278:25323–25330.
[15] Wellen KE, Hotamisligil GS. Inflammation, stress, and diabetes.J Clin Invest 2005;115:1111–1119.
[16] Previs SF, Withers DJ, Ren JM, White MF, Shulman GI.Contrasting effects of IRS-1 versus IRS-2 gene disruption oncarbohydrate and lipid metabolism in vivo. J Biol Chem2000;275:38990–38994.
[17] Taniguchi CM, Ueki K, Kahn R. Complementary roles of IRS-1and IRS-2 in the hepatic regulation of metabolism. J Clin Invest2005;115:718–727.
[18] Horton JD, Shah NA, Warrington JA, Anderson NN, Park SW,Brown MS, et al. Combined analysis of oligonucleotide micro-array data from transgenic and knockout mice identifies directSREBP target genes. Proc Natl Acad Sci USA2003;100:12027–12032.
[19] Horton JD, Goldstein JL, Brown MS. SREBPs: activators of thecomplete program of cholesterol and fatty acid synthesis in theliver. J Clin Invest 2002;109:1125–1131.
[20] Foufelle F, Ferre P. New perspectives in the regulation of hepaticglycolytic and lipogenic genes by insulin and glucose: a role forthe transcription factor sterol regulatory element binding pro-tein-1c. Biochem J 2002;366:377–391.
[21] Lawler Jr JF, Yin M, Diehl AM, Roberts E, Chatterjee S. Tumornecrosis factor-alpha stimulates the maturation of sterol regula-tory element binding protein-1 in human hepatocytes throughthe action of neutral sphingomyelinase. J Biol Chem1998;273:5053–5059.
[22] Gual P, Marchand-Brustel Y, Tanti JF. Positive and negativeregulation of insulin signaling through IRS-1 phosphorylation.Biochimie 2005;87:99–109.
[23] Hotamisligil GS. Inflammation and metabolic disorders. Nature2006;444:860–867.
[24] Rui L, Yuan M, Frantz D, Shoelson S, White MF. SOCS-1 andSOCS-3 block insulin signaling by ubiquitin-mediated degrada-tion of IRS1 and IRS2. J Biol Chem 2002;277:42394–42398.
[25] Vinciguerra M, Foti M. PTEN and SHIP2 phosphoinositidephosphatases as negative regulators of insulin signalling. ArchPhysiol Biochem 2006;112:89–104.
[26] Yki-Jarvinen H. Fat in the liver and insulin resistance. Ann Med2005;37:347–356.
[27] Arkan MC, Hevener AL, Greten FR, Maeda S, Li ZW, LongJM, et al. IKK-beta links inflammation to obesity-inducedinsulin resistance. Nat Med 2005;11:191–198.
[28] Houstis N, Rosen ED, Lander ES. Reactive oxygen species havea causal role in multiple forms of insulin resistance. Nature2006;440:944–948.
[29] Rui L, Aguirre V, Kim JK, Shulman GI, Lee A, Corbould A,et al. Insulin/IGF-1 and TNF-alpha stimulate phosphorylationof IRS-1 at inhibitory Ser307 via distinct pathways. J Clin Invest2001;107:181–189.
[30] Prentki M, Nolan CJ. Islet beta cell failure in type 2 diabetes. JClin Invest 2006;116:1802–1812.
[31] Nawano M, Ueta K, Oku A, Arakawa K, Saito A, Funaki M,et al. Hyperglycemia impairs the insulin signaling step betweenPI 3-kinase and Akt/PKB activations in ZDF rat liver. BiochemBiophys Res Commun 1999;266:252–256.
[32] Oku A, Nawano M, Ueta K, Fujita T, Umebayashi I, ArakawaK, et al. Inhibitory effect of hyperglycemia on insulin-inducedAkt/protein kinase B activation in skeletal muscle. Am J PhysiolEndocrinol Metab 2001;280:E816–E824.
[33] Yu C, Chen Y, Cline GW, Zhang D, Zong H, Wang Y, et al.Mechanism by which fatty acids inhibit insulin activation of

154 I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156
insulin receptor substrate-1 (IRS-1)-associated phosphatidylino-sitol 3-kinase activity in muscle. J Biol Chem 2002;277:50230–50236.
[34] Goudriaan JR, Dahlmans VE, Teusink B, Ouwens DM,Febbraio M, Maassen JA, et al. CD36 deficiency increasesinsulin sensitivity in muscle, but induces insulin resistance in theliver in mice. J Lipid Res 2003;44:2270–2277.
[35] Voshol PJ, Haemmerle G, Ouwens DM, Zimmermann R, ZechnerR, Teusink B, et al. Increased hepatic insulin sensitivity togetherwith decreased hepatic triglyceride stores in hormone-sensitivelipase-deficient mice. Endocrinology 2003;144: 3456–3462.
[36] Kim JK, Fillmore JJ, Chen Y, Yu C, Moore IK, Pypaert M,et al. Tissue-specific overexpression of lipoprotein lipase causestissue-specific insulin resistance. Proc Natl Acad Sci USA2001;98:7522–7527.
[37] Samuel VT, Liu ZX, Qu X, Elder BD, Bilz S, Befroy D, et al.Mechanism of hepatic insulin resistance in non-alcoholic fattyliver disease. J Biol Chem 2004;279:32345–32353.
[38] Schattenberg JM, Singh R, Wang Y, Lefkowitch JH, Rigoli RM,Scherer PE, et al. JNK1 but not JNK2 promotes the develop-ment of steatohepatitis in mice. Hepatology 2006;43:163–172.
[39] Leclercq IA, Farrell GC, Field J, Bell DR, Gonzalez FJ,Robertson GR. CYP2E1 and CYP4A as microsomal catalystsof lipid peroxides in murine nonalcoholic steatohepatitis. J ClinInvest 2000;105:1067–1075.
[40] Schattenberg JM, Wang Y, Singh R, Rigoli RM, Czaja MJ.Hepatocyte CYP2E1 overexpression and steatohepatitis lead toimpaired hepatic insulin signaling. J Biol Chem2005;280:9887–9894.
[41] Reddy JK, Rao MS. Lipid metabolism and liver inflammation.II. Fatty liver disease and fatty acid oxidation. Am J PhysiolGastrointest Liver Physiol 2006;290:G852–G858.
[42] Ip E, Farrell G, Hall P, Robertson G, Leclercq I. Administrationof the potent PPARalpha agonist, Wy-14,643, reverses nutri-tional fibrosis and steatohepatitis in mice. Hepatology2004;39:1286–1296.
[43] Sanyal AJ, Campbell-Sargent C, Mirshahi F, Rizzo WB, ContosMJ, Sterling RK, et al. Nonalcoholic steatohepatitis: associationof insulin resistance and mitochondrial abnormalities. Gastro-enterology 2001;120:1183–1192.
[44] Ozcan U, Cao Q, Yilmaz E, Lee AH, Iwakoshi NN, Ozdelen E,et al. Endoplasmic reticulum stress links obesity, insulin action,and type 2 diabetes. Science 2004;306:457–461.
[45] Ozawa K, Miyazaki M, Matsuhisa M, Takano K, Nakatani Y,Hatazaki M, et al. The endoplasmic reticulum chaperoneimproves insulin resistance in type 2 diabetes. Diabetes2005;54:657–663.
[46] Abdel-Wahab YH, O’Harte FP, Ratcliff H, McClenaghan NH,Barnett CR, Flatt PR. Glycation of insulin in the islets ofLangerhans of normal and diabetic animals. Diabetes1996;45:1489–1496.
[47] Baynes JW. Role of oxidative stress in development of compli-cations in diabetes. Diabetes 1991;40:405–412.
[48] Basta G, Sironi AM, Lazzerini G, Del Turco S, Buzzigoli E,Casolaro A, et al. Circulating soluble receptor for advancedglycation end-products (sRAGE) is inversely associated withglycemic control and S100A12 protein. J Clin Endocrinol Metab2006;91:4628–4634.
[49] Hofmann SM, Dong HJ, Li Z, Cai W, Altomonte J, Thung SN,et al. Improved insulin sensitivity is associated with restrictedintake of dietary glycoxidation products in the db/db mouse.Diabetes 2002;51:2082–2089.
[50] Sandu O, Song K, Cai W, Zheng F, Uribarri J, Vlassara H.Insulin resistance and type 2 diabetes in high-fat-fed mice arelinked to high glycotoxin intake. Diabetes 2005;54:2314–2319.
[51] Riboulet-Chavey A, Pierron A, Durand I, Murdaca J, GiudicelliJ, Van Obberghen E. Methylglyoxal impairs the insulin signaling
pathways independently of the formation of intracellular reactiveoxygen species. Diabetes 2006;55:1289–1299.
[52] Kim S, Moustaid-Moussa N. Secretory, endocrine and auto-crine/paracrine function of the adipocyte. J Nutr2000;130:3110S–3115S.
[53] Guerre-Millo M. Adipose tissue and adipokines: for better orworse. Diabetes Metab 2004;30:13–19.
[54] Kershaw EE, Flier JS. Adipose tissue as an endocrine organ. JClin Endocrinol Metab 2004;89:2548–2556.
[55] Kadowaki T, Yamauchi T, Kubota N, Hara K, Ueki K, Tobe K.Adiponectin and adiponectin receptors in insulin resistance,diabetes, and the metabolic syndrome. J Clin Invest2006;116:1784–1792.
[56] Yamauchi T, Kamon J, Minokoshi Y, Ito Y, Waki H, Uchida S,et al. Adiponectin stimulates glucose utilization and fatty-acidoxidation by activating AMP-activated protein kinase. Nat Med2002;8:1288–1295.
[57] Kersten S, Seydoux J, Peters JM, Gonzalez FJ, Desvergne B,Wahli W. Peroxisome proliferator-activated receptor alphamediates the adaptive response to fasting. J Clin Invest1999;103:1489–1498.
[58] Delerive P, Gervois P, Fruchart JC, Staels B. Induction ofIkappaBalpha expression as a mechanism contributing to theanti-inflammatory activities of peroxisome proliferator-activatedreceptor-alpha activators. J Biol Chem 2000;275:36703–36707.
[59] Bugianesi E, Pagotto U, Manini R, Vanni E, Gastaldelli A, deIasio R, et al. Plasma adiponectin in nonalcoholic fatty liver isrelated to hepatic insulin resistance and hepatic fat content, notto liver disease severity. J Clin Endocrinol Metab2005;90:3498–3504.
[60] Ruan H, Miles PD, Ladd CM, Ross K, Golub TR, Olefsky JM,et al. Profiling gene transcription in vivo reveals adipose tissue asan immediate target of tumor necrosis factor-alpha: implicationsfor insulin resistance. Diabetes 2002;51:3176–3188.
[61] Uysal KT, Wiesbrock SM, Marino MW, Hotamisligil GS.Protection from obesity-induced insulin resistance in micelacking TNF-alpha function. Nature 1997;389:610–614.
[62] Yin MJ, Yamamoto Y, Gaynor RB. The anti-inflammatoryagents aspirin and salicylate inhibit the activity of I(kappa)Bkinase-beta. Nature 1998;396:77–80.
[63] Yuan M, Konstantopoulos N, Lee J, Hansen L, Li ZW, KarinM, et al. Reversal of obesity- and diet-induced insulin resistancewith salicylates or targeted disruption of Ikkbeta. Science2001;293:1673–1677.
[64] Kim JK, Kim YJ, Fillmore JJ, Chen Y, Moore I, Lee J, et al.Prevention of fat-induced insulin resistance by salicylate. J ClinInvest 2001;108:437–446.
[65] Cai D, Yuan M, Frantz DF, Melendez PA, Hansen L, Lee J,et al. Local and systemic insulin resistance resulting from hepaticactivation of IKK-beta and NF-kappaB. Nat Med2005;11:183–190.
[66] Emanuelli B, Peraldi P, Filloux C, Chavey C, Freidinger K,Hilton DJ, et al. SOCS-3 inhibits insulin signaling and is up-regulated in response to tumor necrosis factor-alpha in theadipose tissue of obese mice. J Biol Chem2001;276:47944–47949.
[67] Senn JJ, Klover PJ, Nowak IA, Zimmers TA, Koniaris LG,Furlanetto RW, et al. Suppressor of cytokine signaling-3(SOCS-3), a potential mediator of interleukin-6-dependent insu-lin resistance in hepatocytes. J Biol Chem 2003;278:13740–13746.
[68] Ueki K, Kondo T, Tseng YH, Kahn CR. Central role ofsuppressors of cytokine signaling proteins in hepatic steatosis,insulin resistance, and the metabolic syndrome in the mouse.Proc Natl Acad Sci USA 2004;101:10422–10427.
[69] Klover PJ, Zimmers TA, Koniaris LG, Mooney RA. Chronicexposure to interleukin-6 causes hepatic insulin resistance inmice. Diabetes 2003;52:2784–2789.

I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156 155
[70] Klover PJ, Clementi AH, Mooney RA. Interleukin-6 depletionselectively improves hepatic insulin action in obesity. Endocri-nology 2005;146:3417–3427.
[71] Lee Y, Wang MY, Kakuma T, Wang ZW, Babcock E, McCorkleK, et al. Liporegulation in diet-induced obesity. The antistea-totic role of hyperleptinemia. J Biol Chem 2001;276:5629–5635.
[72] Flier JS. Obesity wars: molecular progress confronts an expand-ing epidemic. Cell 2004;116:337–350.
[73] Nandi A, Kitamura Y, Kahn CR, Accili D. Mouse models ofinsulin resistance. Physiol Rev 2004;84:623–647.
[74] Michael MD, Kulkarni RN, Postic C, Previs SF, Shulman GI,Magnuson MA, et al. Loss of insulin signaling in hepatocytesleads to severe insulin resistance and progressive hepaticdysfunction. Mol Cell 2000;6:87–97.
[75] Bruning JC, Michael MD, Winnay JN, Hayashi T, Horsch D,Accili D, et al. A muscle-specific insulin receptor knockoutexhibits features of the metabolic syndrome of NIDDM withoutaltering glucose tolerance. Mol Cell 1998;2:559–569.
[76] Kim JK, Michael MD, Previs SF, Peroni OD, Mauvais-Jarvis F,Neschen S, et al. Redistribution of substrates to adipose tissuepromotes obesity in mice with selective insulin resistance inmuscle. J Clin Invest 2000;105:1791–1797.
[77] Bluher M, Michael MD, Peroni OD, Ueki K, Carter N, KahnBB, et al. Adipose tissue selective insulin receptor knockoutprotects against obesity and obesity-related glucose intolerance.Dev Cell 2002;3:25–38.
[78] Martin KA, Blenis J. Coordinate regulation of translation by thePI 3-kinase and mTOR pathways. Adv Cancer Res 2002;86:1–39.
[79] Starzl TE, Porter KA, Putnam CW. Insulin, glucagon, and thecontrol of hepatic structure, function, and capacity for regener-ation. Metabolism 1976;25:1429–1434.
[80] Carrillo MC, Favre C, Monti JA, Alvarez ML, Carnovale CE.Insulin hyperresponsiveness in partially hepatectomized diabeticrats. Life Sci 2001;68:1417–1426.
[81] Horie Y, Suzuki A, Kataoka E, Sasaki T, Hamada K, Sasaki J,et al. Hepatocyte-specific Pten deficiency results in steatohepatitisand hepatocellular carcinomas. J Clin Invest 2004;113:1774–1783.
[82] Leclercq IA, Horsmans Y. Cell biology of NASH: fibrosis andcell proliferation. In: Farrell GC, George J, Hall P, McCulloughAJ, editors. Fatty Liver Disease: NASH and Related Disor-ders. Oxford: Blackwell Publishing Ltd; 2005. p. 143–158.
[83] Leclercq IA, Vansteenberghe M, Lebrun VB, Vanhul NK,Abarca-Quinones J, Sempoux CL, et al. Defective hepaticregeneration after partial hepatectomy in leptin-deficient miceis not rescued by exogenous leptin. Lab Invest 2006;86:1161–1171.
[84] DeAngelis RA, Markiewski MM, Taub R, Lambris JD. A high-fat diet impairs liver regeneration in C57BL/6 mice throughoverexpression of the NF-kappaB inhibitor, IkappaBalpha.Hepatology 2005;42:1148–1157.
[85] Yang S, Koteish A, Lin H, Huang J, Roskams T, Dawson V,et al. Oval cells compensate for damage and replicative senes-cence of mature hepatocytes in mice with fatty liver disease.Hepatology 2004;39:403–411.
[86] Roskams T, Yang SQ, Koteish A, Durnez A, DeVos R, HuangX, et al. Oxidative stress and oval cell accumulation in mice andhumans with alcoholic and nonalcoholic fatty liver disease. Am JPathol 2003;163:1301–1311.
[87] Naito M, Hasegawa G, Ebe Y, Yamamoto T. Differentiationand function of Kupffer cells. Med Electron Microsc2004;37:16–28.
[88] Wisse E. An electron microscopic study of the fenestratedendothelial lining of rat liver sinusoids. J Ultrastruct Res1970;31:125–150.
[89] Geerts A. History, heterogeneity, developmental biology, andfunctions of quiescent hepatic stellate cells. Semin Liver Dis2001;21:311–335.
[90] Friedman SL. Liver fibrosis – from bench to bedside. J Hepatol2003;38:S38–S53.
[91] Soda R, Tavassoli M. Distribution of insulin receptors in livercell suspensions using a minibead probe. Highest density is onendothelial cell. Exp Cell Res 1983;145:389–395.
[92] Svegliati-Baroni G, Ridolfi F, Di Sario A, Casini A, Marucci L,Gaggiotti G, et al. Insulin and insulin-like growth factor-1stimulate proliferation and type I collagen accumulation byhuman hepatic stellate cells: differential effects on signal trans-duction pathways. Hepatology 1999;29:1743–1751.
[93] Gentilini A, Marra F, Gentilini P, Pinzani M. Phosphatidylino-sitol-3 kinase and extracellular signal-regulated kinase mediate thechemotactic and mitogenic effects of insulin-like growth factor-I inhuman hepatic stellate cells. J Hepatol 2000;32:227–234.
[94] She H, Wang J, Tsukamoto H. Activated hepatic stellate cells areinsulin resistant and have ER stress. Hepatology 2006;44:A1322.
[95] Rask-Madsen C, King G. Mechanisms of Disease: endothelialdysfunction in insulin resistance and diabetes. Nat Clin PractEndocrinol Metab 2007;3:46–56.
[96] Schalkwijk CG, Stehouwer CD. Vascular complications indiabetes mellitus: the role of endothelial dysfunction. Clin Sci(Lond) 2005;109:143–159.
[97] Paradis V, Perlemuter G, Bonvoust F, Dargere D, Parfait B,Vidaud M, et al. High glucose and hyperinsulinemia stimulateconnective tissue growth factor expression: a potential mecha-nism involved in progression to fibrosis in nonalcoholic steato-hepatitis. Hepatology 2001;34:738–744.
[98] Paradis V, Dargere D, Bonvoust F, Vidaud M, Segarini P,Bedossa P. Effects and regulation of connective tissue growthfactor on hepatic stellate cells. Lab Invest 2002;82:767–774.
[99] Smedsrod B, Melkko J, Araki N, Sano H, Horiuchi S. Advancedglycation end products are eliminated by scavenger-receptor-mediated endocytosis in hepatic sinusoidal Kupffer and endo-thelial cells. Biochem J 1997;322:567–573.
[100] Ramasamy R, Vannucci SJ, Yan SS, Herold K, Yan SF, SchmidtAM. Advanced glycation end products and RAGE: a commonthread in aging, diabetes, neurodegeneration, and inflammation.Glycobiology 2005;15:16R–28R.
[101] Fehrenbach H, Weiskirchen R, Kasper M, Gressner AM. Up-regulated expression of the receptor for advanced glycation endproducts in cultured rat hepatic stellate cells during transdiffer-entiation to myofibroblasts. Hepatology 2001;34:943–952.
[102] Parola M, Robino G. Oxidative stress-related molecules and liverfibrosis. J Hepatol 2001;35:297–306.
[103] Poli G, Parola M, Leonarduzzi G, Pinzani M. Modulation ofhepatic fibrogenesis by antioxidants. Mol Aspects Med1993;14:259–264.
[104] Svegliati BG, D’Ambrosio L, Ferretti G, Casini A, Di Sario A,Salzano R, et al. Fibrogenic effect of oxidative stress on rathepatic stellate cells. Hepatology 1998;27:720–726.
[105] Choi SS, Sicklick JK, Ma Q, Yang L, Huang J, Qi Y, et al.Sustained activation of Rac1 in hepatic stellate cells promotesliver injury and fibrosis in mice. Hepatology 2006;44:1267–1277.
[106] Teufelhofer O, Parzefall W, Kainzbauer E, Ferk F, Freiler C,Knasmuller S, et al. Superoxide generation from Kupffer cellscontributes to hepatocarcinogenesis: studies on NADPH oxidaseknockout mice. Carcinogenesis 2005;26:319–329.
[107] Shen J, Sakaida I, Uchida K, Terai S, Okita K. Leptin enhancesTNF-alpha production via p38 and JNK MAPK in LPS-stimulated Kupffer cells. Life Sci 2005;77:1502–1515.
[108] Leclercq IA, Farrell GC, Schriemer R, Robertson GR. Leptin isessential for the hepatic fibrogenic response to chronic liverinjury. J Hepatol 2002;37:206–213.
[109] Ikejima K, Takei Y, Honda H, Hirose M, Yoshikawa M, ZhangYJ, et al. Leptin receptor-mediated signaling regulates hepaticfibrogenesis and remodeling of extracellular matrix in the rat.Gastroenterology 2002;122:1399–1410.

156 I.A. Leclercq et al. / Journal of Hepatology 47 (2007) 142–156
[110] Cao Q, Mak KM, Ren C, Lieber CS. Leptin stimulates tissueinhibitor of metalloproteinase-1 in human hepatic stellate cells:respective roles of the JAK/STAT and JAK-mediated H2O2-dependant MAPK pathways. J Biol Chem 2004;279:4292–4304.
[111] Saxena NK, Ikeda K, Rockey DC, Friedman SL, Anania FA.Leptin in hepatic fibrosis: evidence for increased collagenproduction in stellate cells and lean littermates of ob/ob mice.Hepatology 2002;35:762–771.
[112] Aleffi S, Petrai I, Bertolani C, Parola M, Colombatto S, Novo E,et al. Upregulation of proinflammatory and proangiogeniccytokines by leptin in human hepatic stellate cells. Hepatology2005;42:1339–1348.
[113] Saxena NK, Titus MA, Ding X, Floyd J, Srinivasan S,Sitaraman SV, et al. Leptin as a novel profibrogenic cytokinein hepatic stellate cells: mitogenesis and inhibition of apoptosismediated by extracellular regulated kinase (Erk) and Aktphosphorylation. FASEB J 2004;18:1612–1614.
[114] Ikejima K, Honda H, Yoshikawa M, Hirose M, Kitamura T,Takei Y, et al. Leptin augments inflammatory and profibrogenicresponses in the murine liver induced by hepatotoxic chemicals.Hepatology 2001;34:288–297.
[115] George J, Wang J, Ramezani M, London R, Brymora J, LeclercqI. Kupffer cells: the main player in leptin-induced liver fibrosis. JGastroenterol Hepatol 2006;21:A315.
[116] Leclercq IA, Field J, Farrell GC. Leptin-specific mechanisms forimpaired liver regeneration in ob/ob mice after toxic injury.Gastroenterology 2003;124:1451–1464.
[117] Park PH, Thakur V, Pritchard MT, McMullen MR, Nagy LE.Regulation of Kupffer cell activity during chronic ethanolexposure: Role of adiponectin. J Gastroenterol Hepatol2006;21:S30–S33.
[118] Thakur V, Pritchard MT, McMullen MR, Nagy LE. Adiponec-tin normalizes LPS-stimulated TNF-alpha production by ratKupffer cells after chronic ethanol feeding. Am J PhysiolGastrointest Liver Physiol 2006;290:G998–G1007.
[119] Kamada Y, Tamura S, Kiso S, Matsumoto H, Saji Y, YoshidaY, et al. Enhanced carbon tetrachloride-induced liver fibrosisin mice lacking adiponectin. Gastroenterology 2003;125:1796–1807.
[120] Ding X, Saxena NK, Lin S, Xu A, Srinivasan S, Anania FA. Theroles of leptin and adiponectin: a novel paradigm in adipocyto-kine regulation of liver fibrosis and stellate cell biology. Am JPathol 2005;166:1655–1669.
[121] Maher JJ. Interactions between hepatic stellate cells and theimmune system. Semin Liver Dis 2001;21:417–426.
[122] Bataller R, Brenner DA. Liver fibrosis. J Clin Invest2005;115:209–218.
[123] Shoelson SE, Lee J, Goldfine AB. Inflammation and insulinresistance. J Clin Invest 2006;116:1793–1801.
[124] Elinav E, Pappo O, Sklair-Levy M, Margalit M, Shibolet O,Gomori M, et al. Adoptive transfer of regulatory NKT lym-phocytes ameliorates non-alcoholic steatohepatitis and glucoseintolerance in ob/ob mice and is associated with intrahepaticCD8 trapping. J Pathol 2006;209:121–128.