Embed Size (px)
Citation preview
Instruments for investigation and correction of the human eye
disordersDepartment of medical physics of diagnostic and treatment
equipment
I. Ya. Horbachevsky Ternopil State Medical University
By Oksana Bagrij-Zayats and Oleksandr Tokarskyy

Posterior Pole of fundus

Diagram of Fundus Layers

Rods and Cones• Because of their different functions, rods and cones are
present in varying densities in the retina. The blind spot is due to the connection of the optic nerve
Light Sensitivity• Remember we talked about rods and cones• Cones:
– Sensitive to bright light, photopic conditions– Densely packed in the fovea– Only a few cones per nerve fiber
• Rods:– Sensitive to low light, scotopic conditions– Widely distributed across the retina– Up to 1000s of rods per nerve fiber (think of this as
many many drops falling into the same pipe, one drop can’t be detected, but many drops generate some water flow that can be measured)

Dark Adaptation
Object must be very bright to be seen
Dim objects can be seen
Near and Far Points
• The eye lens has two extreme points, fully relaxed and fully “bulged”, called fully accommodated.
When the lens is fully accommodated, which object is in focus on the retina?
A. A distant starB. A tree outside in your yardC. Your cell phone screen when texting

Far Points
• When the lens is fully relaxed, a normal eye cornea and lens will focus distant objects (at infinity) on the retina
• This is known as the “far point” of the eye

Near Points
• When the lens is fully accommodated (bulged), the eye will focus an object at about 25 cm (10 inches) away onto the retina
• This is known as the “near point” of the eye
25 cm (10 inches)

Basic Physical ExamBasic Physical Exam
• General physical examination should include :General physical examination should include :– Visual acuityVisual acuity– Pupillary reactionPupillary reaction– Extraocular movementExtraocular movement– Direct ophthalmoscope Direct ophthalmoscope – Dilated exam (in case of visual loss or retinal pathology)Dilated exam (in case of visual loss or retinal pathology)

Visual Acuity Visual Acuity
• Distance or NearDistance or Near• Distance visual acuity at age 3Distance visual acuity at age 3
– early detection of amblyopia early detection of amblyopia
• TerminologyTerminology– VA - Visual acuity VA - Visual acuity – OD - ocular dexterOD - ocular dexter– OS - ocular sinisterOS - ocular sinister– OU - oculus uterqueOU - oculus uterque

Imperfect Vision
• Let’s consider light coming into the eye from a distant object, approximated as parallel rays. In a normal eye, these rays focus on the retina when the eyelens is fully relaxed
• If the cornea is not properly shaped, these rays will not focus on the retina
parallel rays focus past the retina parallel rays focus in front of the retina

Myopia (Nearsightedness)

Myopia• Myopia occurs when the cornea is too powerful.
• When the eyelens is fully relaxed, the far point is not at infinity, but closer
• This results in distant objects appearing blurry
far point is less than infinity

Hyperopia (Farsightedness)• Hyperopia is the opposite problem, when the
cornea is not powerful enough, and parallel rays are not focused by the time they reach the retina.
• The eyelens can partially accommodate to increase the power of the cornea-lens system, and focus these rays on the retina
eyelens partially accommodated to increase lens power

Hyperopia• Because the eyelens has to partially accommodate to
focus rays from distant objects, its range will not be sufficient to focus near objects on the retina
25 cm
more than 25 cm
This results in a near point that is more distant than the standard 25 cm
Power of a Lens• It’s going to be easier to think about corrective lenses
using lens power rather than focal length, so let’s review what this means
• Remember:
• The more a lens bulges, the shorter its focal length, and the larger its ray-bending power

Power of a Lens
When the eyelens is fully relaxed, the power of the cornea plus the eyelens is 60 diopters in a normal eye.
If the eyelens then fully accommodates, does the power of the cornea plus eyelensA.increaseB.stay the sameC.decrease

Power of a Lens• When fully accommodated, the power of the
cornea plus eyelens increases by about 4 diopters.
• Your eyeglass or contact lens prescription is given in diopters, the power of the lens needed to correct the imperfect curvature of your cornea
• Converging lenses have a positive power (positive focal length) and diverging lenses have a negative power (negative focal length)

Corrective Lenses
• Myopic (nearsighted) eyes have a cornea plus lens that is too powerful – They will require a negative (diverging) lens to
compensate
• Hyperopic (farsighted) eyes have a cornea plus lens that is not powerful enough– They will require a positive (converging) lens to
compensate

Lens Power
A myopic eye is too powerful, say it has a power of 63 diopters. What power of lens should we put next to it to get a combined power of 60 diopters (normal eye)
A. -2 dioptersB. -3 dioptersC. 2 dioptersD. 3 diopters

Lens Power
If we have a hyperopic eye of power 58 diopters wearing corrective lenses of power 2 diopters, what is the focal length of the combined set of lenses?
A. 1.5 cm (0.015 m)B. 1.7 cm (0.017 m)C. 2 cm (0.02 m)

Myopia - DefinitionMyopia - Definition
• When parallel rays of light enter the eye (When parallel rays of light enter the eye (with with accommodation relaxedaccommodation relaxed) and come to a single ) and come to a single point focus point focus in front ofin front of the retina the retina

EtiologyEtiology
• Axial lengthAxial length– The axial length of the eye is The axial length of the eye is longerlonger than normal due than normal due
to imperfect emmetropizationto imperfect emmetropization– The most common cause of myopia for The most common cause of myopia for high myopeshigh myopes

EtiologyEtiology
• Refractive powerRefractive power– The refractive power of the eye is The refractive power of the eye is too strongtoo strong
• Curvature myopiaCurvature myopia– Cornea or lens has a steep curvature (e.g., keratoconus)Cornea or lens has a steep curvature (e.g., keratoconus)
• Increased index of refraction (e.g., cornea, lens)Increased index of refraction (e.g., cornea, lens)• Anterior movement of the lens (e.g., nuclear sclerosis)Anterior movement of the lens (e.g., nuclear sclerosis)

Corrective Lenses: Myopia
To correct myopia (nearsightedness), a diverging lens creates an intermediate image of a distant star at your far point so that your eye can see it even though the star is beyond your far point.

Corrective Lenses: Myopia
To correct myopia (nearsightedness), a diverging lens creates an intermediate image of a distant star at your far point so that your eye can see it even though the star is beyond your far point.
far point
image of distant object
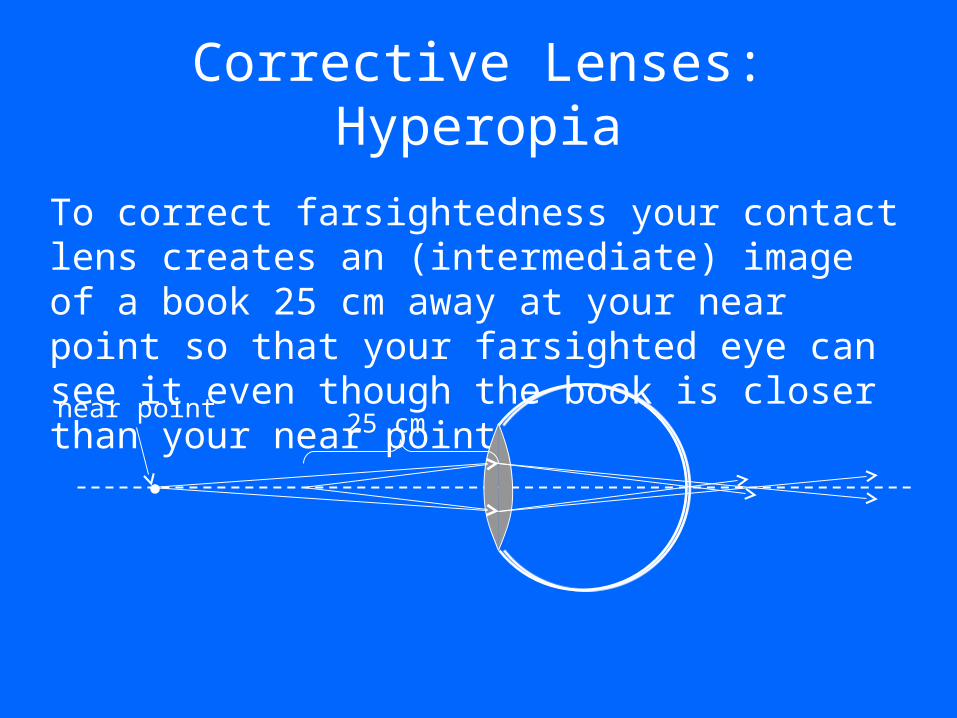
Corrective Lenses: Hyperopia
To correct farsightedness your contact lens creates an (intermediate) image of a book 25 cm away at your near point so that your farsighted eye can see it even though the book is closer than your near point
25 cmnear point

Corrective Lenses: Hyperopia
To correct farsightedness your contact lens creates an (intermediate) image of a book 25 cm away at your near point so that your farsighted eye can see it even though the book is closer than your near point
near point 25 cm
focal point of corrective lens

Determining Prescription

Determining Prescription

Determining Prescription
You are near sighted and your far point is 1 meter away. What is your prescription?
A. +1 diopterB. -1 diopterC. +2 dioptersD. -2 dioptersE. +3 diopters
Determining Prescription
You are far sighted and your near point is 1 meter away instead of 25 cm. What is your prescription?
A. +1 diopterB. -1 diopterC. +2 dioptersD. -2 dioptersE. +3 diopters

Presbyopia: Bifocals
• It is possible to have both a near point that is more distant than 25 cm and a far point that is closer than infinity.
• In this case, you need bifocals, which have two lenses in them, one to correct each imperfection
The top part of the lens (the picture shows a pair of bifocals upside down) corrects the far pointThe bottom part of the lens corrects the near point

Contact Lenses
Contact lenses are just a thinner and smaller version of glasses that rest directly on the cornea, with a thin layer of fluid in between.

Image Size on the Retina
• The size of an object on your retina is related to the angle between the axis and the ray passing through the center of the lens
• A large angle means a large image on the retina.
• Here we see an example that you all know intuitively: that objects look smaller when they are farther away
this angle is large so the object is large
this angle is small so the object is small
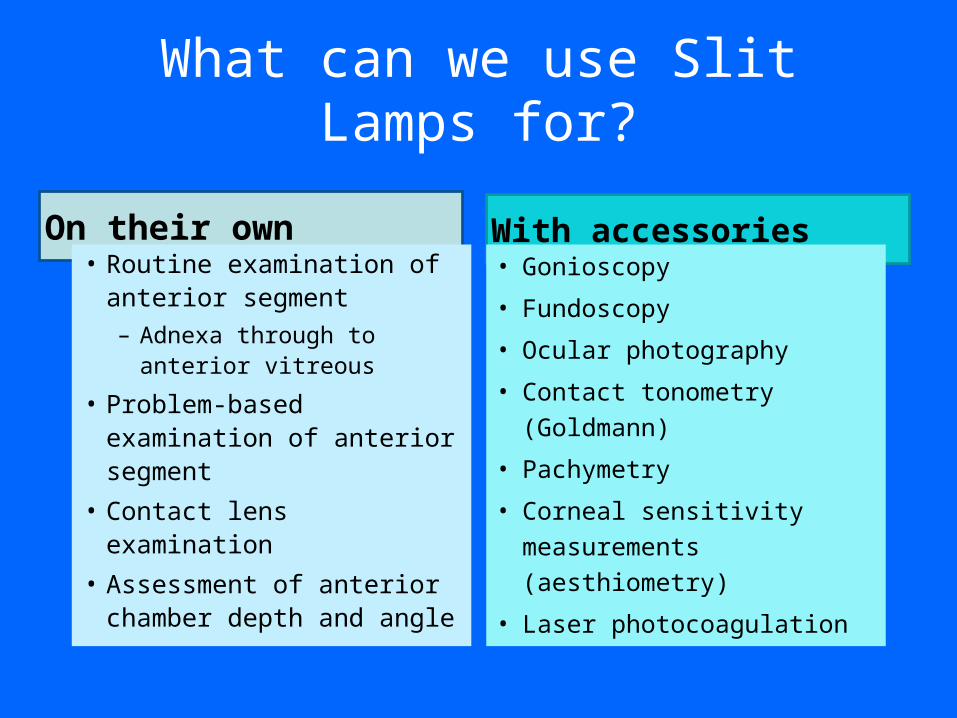
What can we use Slit Lamps for?
On their own With accessories• Routine examination of
anterior segment– Adnexa through to anterior
vitreous
• Problem-based examination of anterior segment
• Contact lens examination• Assessment of anterior
chamber depth and angle
• Gonioscopy
• Fundoscopy
• Ocular photography
• Contact tonometry (Goldmann)
• Pachymetry
• Corneal sensitivity measurements (aesthiometry)
• Laser photocoagulation

Basic Design of a Slit Lamp• Viewing arm
– Biomicroscope– Adjustable focus eyepieces– Magnification dial
• Illumination arm– The “slit lamp”– Slit size, shape and filter controls– Variable size, shape, colour and brightness
• Biomicroscope and illumination are mechanically coupled around central pivot point (copivotal)
– Both focus at the same point (parfocal)– Both arms can swing independently 180º along horizontal –
there is a scale in degrees– Both always central regardless of angle (isocentric)
• Moveable base plate and joystick control
Slit Lamp Magnification• Slit lamps provide variable magnification• Lower magnifications are used for general
assessment and orientation• Higher magnifications are used for detailed
inspections of areas of interest• There are several ways to do this
– Common methods: Littmann-Galilean telescope and zoom systems
– Less common methods: Change the eyepieces and/or change the objective lens

Littmann-Galilean telescope method
• A separate optical system is placed in between the eyepiece and the objective
• It consists of a rotating drum that house 2 Galilean telescopes plus a pair of empty slots– Optics refresher: Galilean telescopes consist of a positive and
negative lens that provide magnification based on the lens powers and their separation
• It is easy to identify whether the slit lamp you are using has this inside– The magnification dial will click into place as you turn it, and
there will be numbers on the dial that correspond to the magnification in each position

Two telescopes produce two magnificationsMag highest when the
convex lens is near objective
Reversal of these two telescopes produces two further minifications
No telescope provides 5th option

Change eyepieces or objective
Eyepieces Objective• Often two sets provided with
slit lamp– Typical values 10x, 12.5x, 15x or 20x
• Inconvenient so rarely used• Generally unnecessary on
modern slit lamps
• Flip arrangement for rapid change
• Usually only two options due to space confinements
• Typical values are 1x and 2x
Lever
Slit width• Continuously variable (0 to
12-14mm)• May be graduated to allow
measurement• Narrow slits are used to
“slice” through the cornea to determine depth or thickness
• Wide slits are used to inspect surfaces

Definition: Gonioscopy is a clinical technique used to
examine structures in the anterior chamber angle.
Trantas, using limbal indentation in an eye with keratoglobus in 1907, first visualized the anterior chamber angle in a living eye and coined the term gonioscopy.

The normal angle of the eye is not visible to us due to total internal reflection of light emanating from the angle.

DIRECT Gonioscopy:The anterior curve of the goniolens is such that the critical angle is not reached, and light rays are refracted at the contact lens- air interface
EG: Koeppe, Shaffer, Layden, Barkan, Thorpe, Swan Jacob
. INDIRECT Gonioscopy:The light rays are reflected by a mirror/ prism in the contact lens and leave the lens at nearly a right angle to the contact lens- air interface.Eg: Goldmann single, and three mirror lenses, Ziess four mirror lenses, posner and susmann four mirror lenses, Thorpe four mirror, Ritch trabeculoplasty lens

Various Diagnostic Gonio Lenses and Specifications
Direct Goniolenses:
-Koeppe- Prototype
-Shaffer. – small Koeppe lens(infants)
-Barkan- prototype surgical goniolens
-Thorpe- surgical and diagnostic lens.
-Swan Jacob- surgical goniolens for children

Indirect goniolenses:
Goldmann single mirror- mirror inclined at 62 degree for gonioscopy.
Central well- dia of 12 mm, post radius of curvature of 7.38 mm
Goldmann three mirror- 59 degrees
Zeiss four mirror- all four mirrors inclined at 64 degree.
Ritch trabeculoplasty lens.

CORNEAL WEDGE
Identification of Schwalbe’s line

How to do Gonioscopy?
• Anesthetize the cornea.
•Insert the lens with or without coupling device.
• Short beam of light, avoid illuminating the pupil
• To manipulate - ask patient to look in the direction of the mirror
•Indent the cornea with a four mirror lens ( appearance of Descemet’s folds)

Direct Ophthalmoscopy Direct Ophthalmoscopy
• Tropicamide or phenylephrine for dilationTropicamide or phenylephrine for dilation– unless shallow anterior chamberunless shallow anterior chamber– unless under neurological evaluationunless under neurological evaluation
• Use own OD to examine ODUse own OD to examine OD– Same for OSSame for OS

Direct Ophthalmoscope

Examiner right eye, hand, right patient eye

Structures of the retinaStructures of the retina
nasal temporal

• Have patient sit in a comfortable positionHave patient sit in a comfortable position• Tell them to look at something straight ahead and level Tell them to look at something straight ahead and level
over your shoulderover your shoulder• Dim light in the room, so patients pupils dilate a little. You Dim light in the room, so patients pupils dilate a little. You
can also use mydriatic eyedrops to dilate the pupilcan also use mydriatic eyedrops to dilate the pupil• Hold ophthalmoscope in same hand as eye you are Hold ophthalmoscope in same hand as eye you are
looking at, and looking through (e.g. left hand for looking at, and looking through (e.g. left hand for examining patients left eye, using your left eye)examining patients left eye, using your left eye)
• Hold head steady with thumb above eyebrow, or hold Hold head steady with thumb above eyebrow, or hold shouldershoulder

• At about 30cm distance with light on eye, locate red reflex (seen as At about 30cm distance with light on eye, locate red reflex (seen as an orange glow in the pupil)an orange glow in the pupil)
• Follow red reflex into the eye as 15 degrees lateral to the patients line Follow red reflex into the eye as 15 degrees lateral to the patients line of vision, this will get you directly into the optic discof vision, this will get you directly into the optic disc
• If you cannot find the disc, trace any blood vessels back to itIf you cannot find the disc, trace any blood vessels back to it• Examine vessels in all 4 quadrants of eye (upper and lower nasal and Examine vessels in all 4 quadrants of eye (upper and lower nasal and
temporal quadrants)temporal quadrants)• Identify macula – slightly darker pigmented area, 2 optic disc widths Identify macula – slightly darker pigmented area, 2 optic disc widths
lateral away from the optic disclateral away from the optic disc• You can tell the patient to look at the light – this will put the macula You can tell the patient to look at the light – this will put the macula
in your focus, however don’t look at it too long as it can be irritatingin your focus, however don’t look at it too long as it can be irritating

• 1 The size, shape and borders of the optic disc1 The size, shape and borders of the optic disc• 2 The disc to cup ratio2 The disc to cup ratio• 3 The relative size of the arteries and veins3 The relative size of the arteries and veins• 4 The texture of the retina4 The texture of the retina• 5 The color of the retina5 The color of the retina• 6 Trace the vascular structure to the equator of 6 Trace the vascular structure to the equator of
the retina.the retina.• 7 Find the macula and note its color and size7 Find the macula and note its color and size

GlaucomaGlaucoma
• Identify disc-to-cup ratioIdentify disc-to-cup ratio• The pink rim of disc The pink rim of disc
contains nerve fibers. The contains nerve fibers. The white cup is a pit with no white cup is a pit with no nerve fibers. As glaucoma nerve fibers. As glaucoma advances, the cup advances, the cup enlarges until it occupies enlarges until it occupies most of the disc area. most of the disc area.

OpthalmoscopyOpthalmoscopy
• Turning the dial to positive (or green) numbers increases Turning the dial to positive (or green) numbers increases the refractive index – short focal length lenses – for the refractive index – short focal length lenses – for examining cornea, iris, or opacities in vitreous or lens. e.g. examining cornea, iris, or opacities in vitreous or lens. e.g. start at +20 and use the slit lightstart at +20 and use the slit light
• Turning the dial to negative (or red) numbers decreases – Turning the dial to negative (or red) numbers decreases – infinite focal length lens that fits your refractive power infinite focal length lens that fits your refractive power (individual) – for examining retina, start at +10 as you (individual) – for examining retina, start at +10 as you move in and dim the scope light about halfwaymove in and dim the scope light about halfway
• Rule of thumb: You will focus on the retina with same Rule of thumb: You will focus on the retina with same number as your refractive error, then correct for your number as your refractive error, then correct for your patients refractive errorpatients refractive error

GlaucomaGlaucomaA disease of progressive optic neuropathy with loss of retinal A disease of progressive optic neuropathy with loss of retinal
neurons and their axons (nerve fiber layer) resulting in neurons and their axons (nerve fiber layer) resulting in blindness if left untreated.blindness if left untreated.
““High IOP (intraocular pressure) is the strongest known risk High IOP (intraocular pressure) is the strongest known risk factor for glaucoma but it is neither necessary nor sufficient factor for glaucoma but it is neither necessary nor sufficient to induce the neuropathy.”to induce the neuropathy.”
• Classification:Classification:– Open-angle glaucoma Open-angle glaucoma – vs. angle-closure glaucomavs. angle-closure glaucoma– Primary vs. SecondaryPrimary vs. Secondary

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA Types of glaucomaTypes of glaucoma
I. Primary: A. Congenital B. Hereditary C. Adult (common types) 1. Narrow angle 2. Open angle (Normal tension glaucoma) II. Secondary A. Inflammatory B. Traumatic C. Rubeotic D. Phacolytic etc.

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA
How do we diagnose it?How do we diagnose it?
IOP is not helpful diagnostically until it reaches IOP is not helpful diagnostically until it reaches approximately 40 mm Hg at which level the approximately 40 mm Hg at which level the likelihood of damage is significant.likelihood of damage is significant. Visual fields are also not helpful in the early stagesVisual fields are also not helpful in the early stages of diagnosis because a considerable number of neurons must be lost before VF of diagnosis because a considerable number of neurons must be lost before VF
changes can be changes can be detected.detected. Optic nerve damage in the early stages is difficultOptic nerve damage in the early stages is difficult or impossible to recognize.or impossible to recognize. 50% of people with glaucoma do not know it!50% of people with glaucoma do not know it!

Glaucoma EvaluationGlaucoma Evaluation
• Complete historyComplete history• Complete examinationComplete examination
– IOPIOP– GonioscopyGonioscopy– Optic discOptic disc– Visual FieldsVisual Fields

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA
How do we measure IOP?How do we measure IOP?
ApplanationApplanation
TonopenTonopen
SchiotzSchiotz
AirAir
Non-contactNon-contact
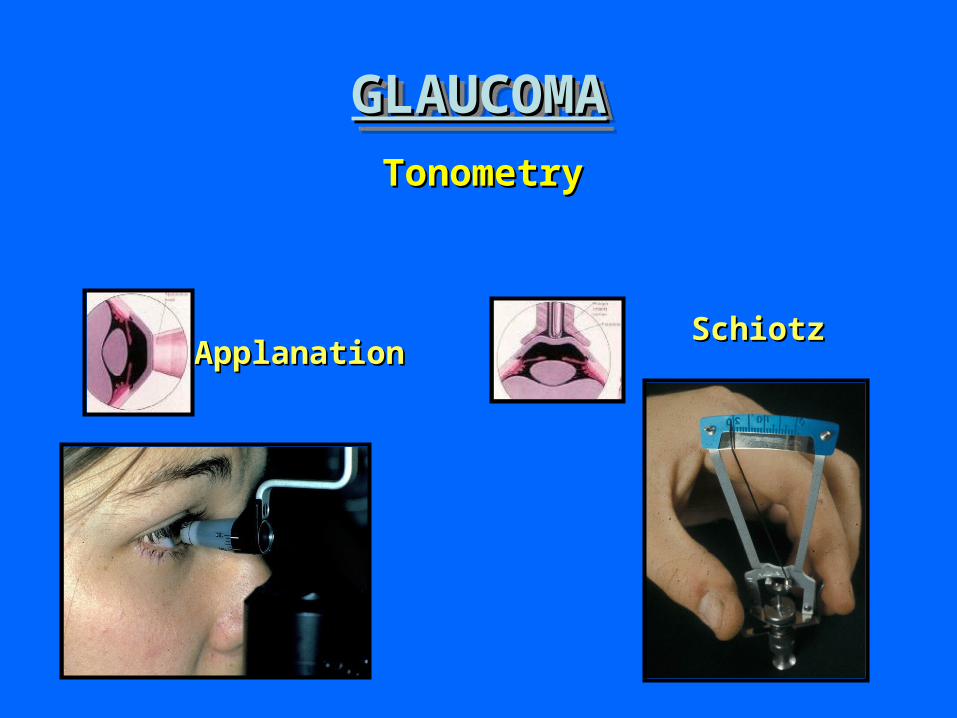
GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMATonometryTonometry
ApplanationApplanationSchiotzSchiotz

Intraocular Pressure Measurement Intraocular Pressure Measurement
• Range: 10 - 22Range: 10 - 22

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA
Goldmann applanation Goldmann applanation tonometertonometer

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA
TonopenTonopen
GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA
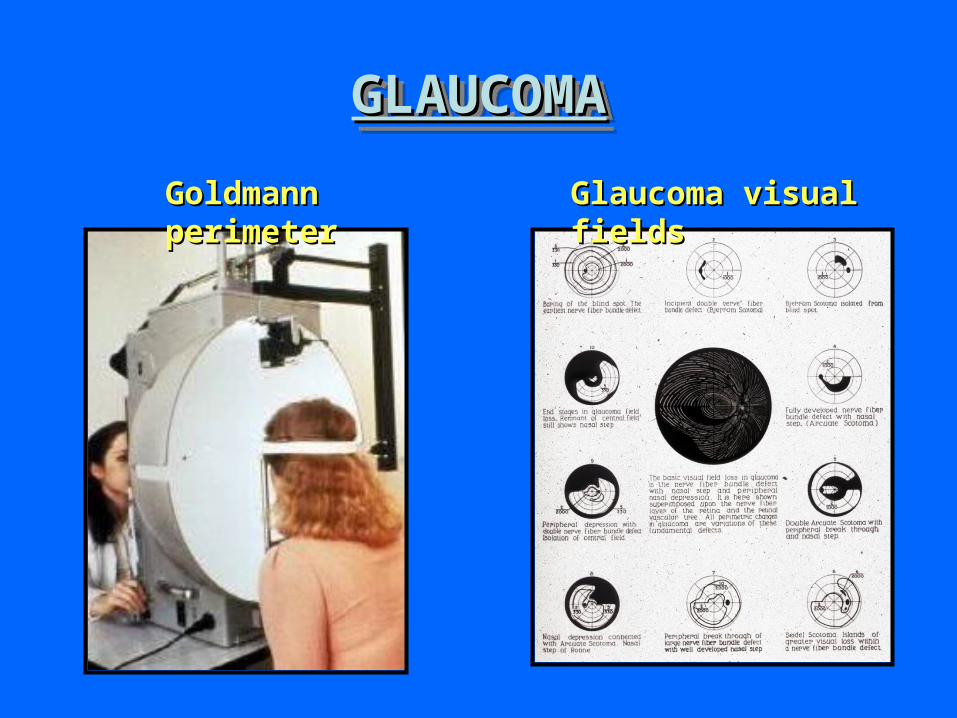
Goldmann perimeterGoldmann perimeter Glaucoma visual fieldsGlaucoma visual fields

THE VISUAL FIELDTHE VISUAL FIELDHumphrey automated perimetry

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA
Cup-to-disk ratioCup-to-disk ratio

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMA
NormalNormal
DISK CUPPINGDISK CUPPING
GlaucomaGlaucoma

GLAUCOMAGLAUCOMAGLAUCOMAGLAUCOMASurgical treatment of glaucomaSurgical treatment of glaucoma
Argon laserArgon lasertrabeculoplastytrabeculoplasty
FiltrationFiltrationproceduresprocedures

CataractCataract
• Opacification of the lensOpacification of the lens• Congenital vs. acquiredCongenital vs. acquired• Often age-relatedOften age-related• Different formsDifferent forms
– Nuclear, cortical, PSCCNuclear, cortical, PSCC• Very successful surgeryVery successful surgery

Keratometry: Main Points so Far• Keratometry uses the anterior cornea as a mirror• Distant object: h rAC • Keratometer Equation: • Virtual corneal image (h) inaccessible, small and unstable (eye
movements), so:– Use objective lens to focus reflected rays as a real image– magnify the real image with an eyepiece lens (~ 5 mag)– split the real image inside the keratometer into two using a half-field prism;
adjust prism to “double” images
h
hbrAC
2

OBJECTIVE
h
½ hC
MIRE
F
CORNEA
½ h
h
< h
PRISM (P)IMAGE PLANE
P
Fig 13.17, Page 13.18
Moving prism toward image plane decreases image displacement (x)
Previously doubled images are no longer doubled (now overlap)
What new corneal radius would this prism position “suit”?
What happens if we move the prism?
x
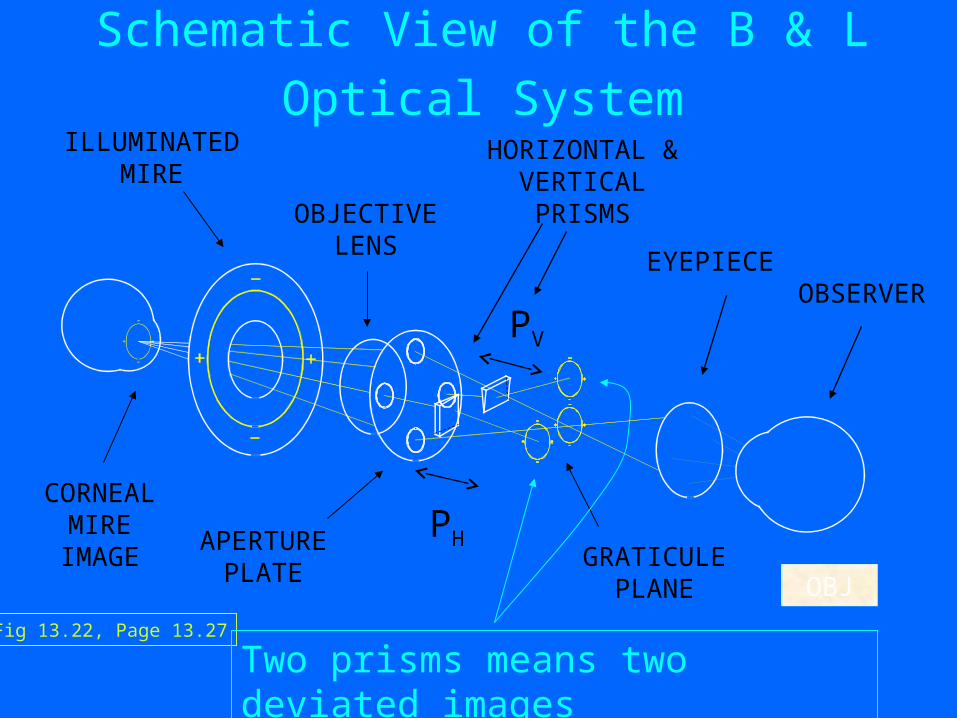
Fig 13.22, Page 13.27
ILLUMINATED MIRE
HORIZONTAL & VERTICAL PRISMS
EYEPIECEOBSERVER
GRATICULE PLANE
APERTURE PLATE
CORNEAL MIRE
IMAGEPH
PV
OBJECTIVE LENS
Schematic View of the B & L Optical System
Two prisms means two deviated images
OBJ

Topcon Keratometer
What the Clinician Sees
V 90 / H 180

h'90
Corneal vertex
B & L: Oriented to Measure r90 and r180
h'180
Question: If most corneas are aspheric, what is one drawback with a keratometer?
Answer: only measuring radius at one location (annulus) on cornea; and it is NOT central radius
OBJ

h'60
Corneal vertex
B & L: Oriented to Measure r60 and r150
h'150
60
150 30
90
180 (0)
15
45
75105120
135
165
180

Q2: What does this appearance indicate?
Spheric
al corn
eal surfa
ce
Irregular A
stigmatism
Obliq
ue Astigmatism
With
-the-R
ule Astigm
atism
Against-th
e-Rule Asti
g...
20% 20% 20%20%20%
1. Spherical corneal surface2. Irregular Astigmatism3. Oblique Astigmatism4. With-the-Rule Astigmatism5. Against-the-Rule Astigmatism

Basis of Corneal Power Estimate - Exact Eye
r1 = +7.7 mm
naqueous
1.336
ncornea
1.376
nair
1.000
r2 = +6.8 mmFe (cornea) +43.05 D
F1 = +48.83 D
F2 = 5.88 D
Page 13.23

Electrooculography - DEFINITION
• The clinical electro-oculogram is an electrophysiological test of function of the outer retina and retinal pigment epithelium in which the change in the electrical potential between the cornea and the fundus is recorded during successive periods of dark and light adaptation.

• The eye has a standing electrical potential between front and back, sometimes called the corneo-fundal potential. The potential is mainly derived from the retinal pigment epithelium (RPE), and it changes in response to retinal illumination
• The potential decreases for 8–10 min in darkness. Subsequent retinal illumination causes an initial fall in the standing potential over 60–75 s (the fast oscillation (FO)), followed by a slow rise for 7–14 min (the light response). These phenomena arise from ion permeability changes across the basal RPE membrane.
Measurement of the clinical EOG
• The calibration of the signal may be achieved by having the patient look consecutively at two different fixation points located a known angle apart and recording the concomitant EOGs .
• By attaching skin electrodes on both sides of an eye the potential can be measured by having the subject move his or her eyes horizontally a set distance .
• Typical signal magnitudes range from 5-20 µV/°.



• A ground electrode is attached usually to either the forehead or earlobe.
• Either inside a Ganzfeld, or on a screen in front of the patient, small red fixation lights are place 30 degrees apart .
• The distance the lights are separated is not critical for routine testing.


The standard method
• Typically the voltage becomes a little smaller in the dark reaching its lowest potential after about 8-12 minutes, the so-called “dark trough”.
• When the lights are turned on the potential rises, the light rise, reaching its peak in about 10 minutes.
• When the size of the "light peak" is compared to the "dark trough" the relative size should be about 2:1 or greater .
• A light/dark ratio of less than about 1.7 is considered abnormal.

Electroretinogram: An electrical diagnostic test of retinal function in situ
• Electro -part– Currents, wires, voltage, resistance
• Retino - part– Cell types, membrane potential, radial currents.
• Gramo - part– Diagnostic test of patient retinal health– Research test retinal circuitry, cell function, disease
states, drug efficacy

The Eye generates a lot of electrical signal, some fast . . some slow. . .

Methods
• Dark adapt 20-45 min• Anesthetize subjects cornea (paracaine)• Dilate iris (tropicamide; phenylephrine)• Attach electrodes: Burian-Alled, Or
– Forehead (neg)– Corneal (pos) (DTL microfiber)– Behind Ear (reference)

Burian-Allen Electrode for Human Use

Electroretinogram (ERG)
600
400
200
0
-200
r (µ
V)
0.30.20.10.0
time (s)
B wave
A wave

Basic Clinical ERG tests
• Dark adapted, dim (blue) flash response– Isolated rod-driven response
• Dark adapted, bright (white) flash response – Generates Max a-wave, b-wave, also generates OPs :
• Light adapted, bright flash– Isolated cone-driven response
• 30 Hz Flicker– Another method of isolating cone responses.

Different conditions yield different responses
Rod Rod & Cone Cone