Instructions and Reporting Requirements Module 8 Electronic Reporting For Facilities March 2013...
30
Instructions and Reporting Requirements Module 8 Electronic Reporting For Facilities March 2013 North Carolina Central Cancer Registry State Center for Health Statistics Division of Public Health Department of Health and Human Services 1908 Mail Service Center Raleigh, NC 27699-1908 http://www.schs.state.nc.us/units/ccr/ North Carolina Central Cancer Registry
Instructions and Reporting Requirements Module 8 Electronic Reporting For Facilities March 2013 North Carolina Central Cancer Registry State Center for
Instructions and Reporting Requirements Module 8 Electronic
Reporting For Facilities March 2013 North Carolina Central Cancer
Registry State Center for Health Statistics Division of Public
Health Department of Health and Human Services 1908 Mail Service
Center Raleigh, NC 27699-1908
http://www.schs.state.nc.us/units/ccr/
http://www.schs.state.nc.us/units/ccr/ North Carolina Central
Cancer Registry
Slide 3
Part VIII Entering Information Into the New Case Abstract
Form
Slide 4
Part VIII: Entering Information Into the New Case Abstract Form
Before beginning a new report, read the following VERY IMPORTANT
information A separate report must be completed and submitted for
each independent primary tumor. o Example: If a patient is
diagnosed with bladder cancer and a separate kidney cancer, a
separate report must be submitted for each diagnosis. o Please
complete the New Case Abstract form as ACCURATELY and COMPLETELY as
possible. o Once the report is free of errors and is successfully
submitted, it is considered as having been reported to the
NCCCR.
Slide 5
Part VIII: Entering Information Into the New Case Abstract Form
Before opening a new form and beginning data entry: o Make sure all
information necessary for entering the case is available and on
hand o Review the chart in its entirety o Make notes on a note pad
or scrap paper if necessary to facilitate data entry o Confirm any
information that is confusing or unclear with the physician.
Session times out after 30 minutes if no activity takes place. o
All information entered for the case (and not submitted) will be
lost. o All information necessary for completing the case should be
on hand prior to beginning data entry for that case.
Slide 6
Part VIII: Entering Information Into the New Case Abstract Form
There is a Save function o Cases should be saved on a frequent
basis. o Once the case is completely entered and all error messages
are cleared, hospital staff must select Finish and Complete.. o If
it is known that more information is needed or will be forthcoming,
hold the case for a later time. Do not start data entry. o Cases
started, but not completed, can be accessed at a later time. o Any
information not saved will be lost and must be re- entered.
Slide 7
Part VIII: Entering Information Into the New Case Abstract Form
Treatment information is very important: o Wait to enter report
AFTER treatment plan is established Make sure START DATES for each
treatment modality are known o It is not required for all treatment
to be completed Treatment may continue for months or years o For
patients who refuse treatment, do not receive treatment for any
reason or when there is a decision not to treat (watchful waiting
or active surveillance) Specifically record that decision of why
there was not treatment in the treatment text area.
Slide 8
Part VIII: Entering Information Into the New Case Abstract Form
Text is CRITICAL! o Over 100 additional data items will be coded by
the NCCCR staff after the report is submitted. o This coding is
highly dependent on the text you provide. o Provide as much
information and detail as possible to describe the case. o It is
critical to the accuracy and completeness of the final coding for
the reported case.
Slide 9
Part VIII: Entering Information Into the New Case Abstract Form
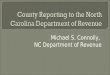
Screen Shots o A screen shot for each tab is provided in the
following slides Each screen shot shows an example of what a
completed screen would look like using a hypothetical prostate case
o A table per screen shot is included with information on Each data
field on the tab Any additional coding instructions for each tab o
Pay particular attention to the format and content of the text
areas used to describe the case In the screen shots, a red box [ ]
indicates a required field Text boxes allow a limited number of
characters
Slide 10
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.1: Entering Patient Personal Data on the Demographic
Tab
Slide 11
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.1: Entering Patient Personal Data on the Demographic
Tab - continued Data Field NameSpecial Coding Instructions Last
Name* Special characters (,. / : ~ @ # & *) are not allowed in
name fields. Enter the name without special characters. For
example, enter OHARA for OHara. First Name* Middle SuffixLetters,
numbers and periods only are allowed. SSN*The SSN can be entered
with or without hyphens. Unknown should be avoided. 999-99-9999 is
only allowed if the patient refused to provide his or her SSN.
Sex/Gender*Unknown should be avoided. Birth Date*Date of birth may
not be blank or unknown. Place of BirthCode 999 (unknown) if not
specifically stated. Do not assume patient was born in the United
States Race*Unknown should be avoided if at all possible. Race is
very important in demographic studies. Request that this be
dictated by the physician if not requested from the patient on the
pre-visit paperwork. If patient is multiracial and one race is
white, code the other race. Persons of Spanish or Hispanic origin
may be of any race. Spanish OriginIf the patient is of Spanish or
Hispanic origin, select the code that describes the specific
origin. Use Code 0 (Non-Spanish) if there is no indication that
patient is of Spanish/Hispanic Origin. Use Code 6 (Spanish/Hispanic
NOS) if there is evidence (other than surname or maiden name) that
the person is Hispanic, but cannot be assigned to the category in
codes 15. Use Code 7 (Spanish Surname) when it is unknown if the
patient is of Spanish/Hispanic Origin but the patient has a
Spanish/Hispanic Surname. Industry and Occupation Record the
occupation and industry where the patient worked for the majority
of his or her lifetime. Example: Industry: Education, Occupation:
Teacher If the usual occupation is not clear, enter the current
occupation. If no information is known about the patients
occupation, leave blank. Do not record Unknown. If the patient is a
minor, or a student, or has never held an occupation (such as a
homemaker), record Minor, Student or Never Worked.
Slide 12
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.2: Entering Diagnostic Data on the Dx/Staging Tab -
continued Special Coding Instructions Record the primary residence
for the patient at the time of diagnosis. The address should be
fully spelled out with standardized use of abbreviations and
punctuation per U.S. Postal Service postal addressing standards.
This is not necessarily the same as the patients current address.
If it is known that the patient was living at a different address
at the time of diagnosis, enter as much as is known and record
UNKNOWN in the remaining address fields. For example, if all that
is known is the city, then enter the city, state and zip and enter
UNKNOWN in the street address. If no information regarding the
address at diagnosis is known, then enter the current address. This
is preferred over recording the address as entirely unknown.
Patient Address at Diagnosis Should be the street address. PO Box
is allowed but should only be used if the physical address is not
known. City* State* Zip* If the last four digits of the zip code
are known, enter them preceded by a hyphen. County* Use the drop
down menu to make a selection. Type the county name to begin the
search. Special Codes: 998 Residence not in North Carolina. The
address at diagnosis was a state other than North Carolina. 999 -
County is unknown. This is only allowed if the city is
unknown.
Slide 13
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.2: Entering Diagnostic Data on the Dx/Staging Tab
Cannot be unknown. Estimate as closely as possible. Pathology
information is very important. Be very detailed. Use any available
text field to provide additional pertinent information. Each
procedure must include: Date, Procedure, Place, Findings. Text
describing the primary site and histology (including behavior and
grade) MUST be included here to validate the codes selected.
Slide 14
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.2: Entering Diagnostic Data on the Dx/Staging Tab -
continued Data Field NameSpecial Coding Instructions Date of
Dx*Enter the first date it was stated the patient had this cancer.
This may be a physicians statement of diagnosis or it may be based
on the results of a diagnostic test or procedure. Date of Diagnosis
cannot be blank or unknown and must be the earliest of all dates
except for Birth Date. Estimate as closely as possible if an exact
date is unknown. At least a valid year must be recorded. If there
is absolutely no information to even estimate the year, record the
same year as the patients first visit to your facility. Refer to
Section VII.2: General Instructions for Using the Data Entry
Screens for more information on how to complete the Date and Date
Flag fields. Place of DxEnter the facility, treatment center, or
physicians office that performed the first test or made the first
statement that confirmed this diagnosis. If this was at your
facility, then enter your facility name. If this is unknown, then
record UNKNOWN.
Slide 15
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.2: Entering Diagnostic Data on the Dx/Staging Tab -
continued Data Field NameSpecial Coding Instructions Use free text
in the following designated text areas to describe the
results/findings of any diagnostic workup, staging workup,
biopsies, and surgical procedures performed. For each procedure,
record the date of the procedure, the procedure name, the place
where the procedure took place, and the pertinent results/findings
of the procedure. This should include pertinent negative findings
in addition to positive findings. Example: 10/19/2011, CT
ABD/PELVIS, UROL ASSOC. ENLARGED PROSTATE. NO ADENOPATHY. NO MET DZ
SEEN Physical Exam Include age, rage and sex of patient Include
pertinent information from the H&P including the evaluation of
the location and extent of the tumor and other symptoms that may
suggest further disease spread. X-rays/Scans Include the results of
any imaging or ultrasound tests performed to evaluate the tumor
Scopes This includes endoscopies, etc. Lab Values In addition to
the lab test and result, state whether the test was considered to
be elevated, abnormal or within normal limits Only lab tests that
are diagnostic or prognostic for that primary site need to be
summarized. Examples include CA-125, CEA, PSA, etc. Routine blood
tests such as CBC do not need to be included
Slide 16
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.2: Entering Diagnostic Data on the Dx/Staging Tab -
continued Data Field NameSpecial Coding Instructions Use free text
in the following designated text areas to describe the
results/findings of any diagnostic workup, staging workup,
biopsies, and surgical procedures performed. For each procedure,
record the date of the procedure, the procedure name, the place
where the procedure took place, and the pertinent results/findings
of the procedure. This should include pertinent negative findings
in addition to positive findings. Example: 10/19/2011, CT
ABD/PELVIS, UROL ASSOC. ENLARGED PROSTATE. NO ADENOPATHY. NO MET DZ
SEEN Path/Autopsy* This section is very important. Include the
findings from all cytologic (FNA, brushings, etc.) and histologic
(biopsy, surgical resection, etc.) examinations performed. Clearly
separate each procedure and findings with separate statements. In
addition to the basic text elements such as date, procedure, place
and findings, include the status of the following: Final diagnosis
as written on the report Location of the tumor (primary site and
laterality) Histology (EXACTLY as stated on the report) Behavior
(invasive or in situ) Grade including site specific grade such as
Gleason Tumor Size Tumor extension into other surrounding tissues
Surgical Margins # Lymph Nodes removed and positive Examination of
metastatic tissues Ancillary studies such as tumor markers Relevant
findings from the gross examination including aids in identifying
the primary site and extent of disease
Slide 17
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Tumor Data on the Dx/Staging Tab -
continued Data Field NameSpecial Coding Instructions Site* Select
the organ/tissue in which the primary tumor arose/originated. If
the exact site cannot be identified, but it is known to have
originated in the breast, select code C50.9 breast, NOS If the
exact site cannot be identified, but it is known to have originated
in the skin, select code C44.9 Skin, NOS Codes ending in.9 are used
when there was a single tumor that overlapped the boundaries of two
or more sub-sites and the point of origin could not be determined
(Bladder, NOS C67.9) or there is not a choice of sub-sites
(Prostate C61.9) Dx Confirmation Select the code that describes the
best diagnostic method used to confirm the cancer being reported.
The coded are listed in priority order. Code 1 has the highest
priority. If the presence of cancer is confirmed with multiple
diagnostic methods, select the code with the lower numeric value.
Code 1 (positive histology) includes: Tissue specimens from biopsy,
frozen section, surgery, autopsy or D&C, aspiration or biopsy
of bone marrow. Code 2 (positive cytology) includes: Cytologic
examination of cells such as sputum smears, bronchial brushings,
bronchial washings, prostatic secretions, breast secretions,
gastric fluid, spinal fluid, peritoneal fluid, pleural fluid,
urinary sediment, cervical smears and vaginal smears, or from
paraffin block specimens from concentrated spinal, pleural, or
peritoneal fluid.
Slide 18
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Tumor Data on the Dx/Staging Tab -
continued Data Field NameSpecial Coding Instructions Laterality* If
the primary site is a bilateral organ, the side in which the tumor
originated (laterality) must be specific. We have provided a few of
The following are the paired organ sites below. C34.1 C34.9 Lung
C44.1 Skin of eyelid C44.2 Skin of external ear C50.0 c50.9 Breast
C62.0 C62.9 Testis C63.0 Epididymis C63.1 Spermatic cord C64.9
Kidney, NOS Use code 0 for all other non-paired organs Use code 4
if the following conditions are met (e.g. bilateral Wilms tumors):
There was a bilateral involvement at time of diagnosis, It
contained the same histology, And it is considered a single
primary.
Slide 19
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Tumor Data on the Dx/Staging Tab -
continued Data Field NameSpecial Coding Instructions Use text in
the following designated text areas to describe the facts about the
stage (extent of disease) of the cancer at the time of diagnosis.
The Staging text areas may not be left blank. This information will
be used by the NCCCR staff to code 42 data items related to the
stage of the tumor. Be as specific as possible, even if it means
repeating information from the previous tab. Include descriptive
words such as consistent with, probably, suggests, with features
of, abutting, extending to, etc. Enter NONE to indicate there was
not information available from the workup to evaluate that
particular extent of disease (extension, lymph nodes, or mets).
Summarize the extent of the disease using all of the workup
performed (clinical and pathologic). This includes the findings
from the physical exam, imaging, scopes, lab work, biopsies,
surgeries, etc. For these three text areas, the date or place of
the procedure does not need to be repeated unless it is needed to
clarify the information. Extension* From all of the workup
performed, summarize the extent of the primary tumor. Summarize the
following: Tumor size Involvement with the primary organ Extension
into surrounding tissues. Mets at Dx* From all of the workup
performed, summarize any evidence of metastatic disease present at
the time of diagnosis. It is very important to differentiate
metastatic disease present at the time of diagnosis and metastatic
disease discovered after initial diagnosis and treatment. Lymph
Node involvement* From all of the workup performed, summarize any
evidence of regional lymph node involvement present at the time of
diagnosis. Summarize the following: Name of the lymph node chain
involved Number of lymph nodes involved Number of lymph nodes
examined Any documentation that the lymph nodes were evaluated and
were negative.
Slide 20
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Tumor Data on the New Case Abstract Form -
continued Data Field NameSpecial Coding Instructions
RemarksDocument ALL known previous primaries including site,
laterality, histology & diagnosis date if available. Family
History. Smoking History. Information that explains unusual
circumstances, use of estimated dates, referral information,
etc.
Slide 21
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.3: Entering Facility Data on the Hospital Tab Include
the NPI number for each facility. Include the NPI number for each
physician. First date the patient was seen at your facility with
cancer. Type of facility Name and type of Insurance
Slide 22
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.3: Entering Facility Data on the Hospital Tab -
continued Data Field NameSpecial Coding Instructions Facility
information must be entered by the user each time the user logs on
to the Eureka system, Facility information only needs to be entered
for first case entered. Facility #* Select the Facility
Identification Number assigned to the facility in which you are
reporting cases. This was the number assigned to your facility when
you requested a Eureka account. If the patient was seen at another
hospital, treatment center or physicians office for the management
of this tumor, select the appropriate code for Referred From or
Referred To from the drop down menu. If the facility or physicians
office for the Referred From of Referred To fields was not an
available option in the associated selection boxes, leave the
default o 0000000000 and record the name of the facility in the
Remarks text section. There are several special codes for when the
exact facility name is not known or the patient was referred out of
state. Search the menu options carefully before making a final
selection. Referred From Patient seen elsewhere for management of
this tumor before visit at your office. If the patient was not
referred, leave the default of 0000000000. Referred To Patient seen
elsewhere for the management of this tumor after visit at your
office. If the patient was not referred, leave the default of
0000000000. Attending MD Enter the name of the physician at your
office caring for the patient. Surgeon Enter the name of the
physician who performed the cancer-directed surgery for the
treatment of this tumor.
Slide 23
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.3: Entering Facility Data on the Hospital Tab -
continued Data Field NameSpecial Coding Instructions NPI Numbers
For each facility and physician recorded above, enter their NPI
number assigned by CMS. This must be entered as a 10-digit number.
To obtain NPI numbers for your facility and other local providers
start with the billing department. It may be helpful to create a
list of numbers for physicians and hospitals commonly participating
in the care of your patients to have on hand when entering cases.
For NPI numbers not available by the billing department, use the
Centers for Medicare and Medicaid Services (CMS) website. The Data
Dissemination page provides further links to access a searchable
database where you can search for individual providers. NPI
Registry (searchable data base):
www.cms.hhs.gov/National/ProvidentStand/www.cms.hhs.gov/National/ProvidentStand/
Click on Data Dissemination
Slide 24
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.2: Entering Facility Data on the Hospital Tab -
continued Data Field NameSpecial Coding Instructions Medical Rec
#Letters, numbers and hyphens only are allowed. Insurance (Pay
Source &Text) Admission Date (Date 1st seen with Cancer) This
is the first date the patient was seen at your facility with a
diagnosis of cancer. If the patient is diagnosed as a result of
testing performed during the visit, the date will be the date of
this visit. This should not be blank or unknown. Type of
AdmissionSelect the type of admission (inpatient, outpatient,
etc.)
Slide 25
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Treatment Data on the New Case Abstract
Form Each procedure must include: Date, Procedure Name and Place
(where the procedure was done). Findings, if summarized on the
previous tab, do not need to be repeated here. If the patient did
not receive that particular type of treatment, select the flag code
of 11.
Slide 26
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Treatment Data on the New Case Abstract
Form - continued Data Field NameSpecial Coding Instructions Surgery
Date, Flag, Text Record the first date caner-directed surgery was
performed as part of the first course of therapy. If multiple
surgical procedures were performed, record the date of the first
surgical procedure. Do not include biopsy dates unless the biopsy
removed the entire tumor. In the text area, describe as much as is
known about the following: Procedure date Place/facility performed
It is important to delineate the specific details for each
procedure performed. While biopsies are not included in the Surgery
Date, a summary of any biopsies should be included in the Surgery
Text. Chemo Date, Flag, Text For each of these treatment types,
record the first start date for that treatment delivered to the
patient as part of the first course of therapy. If multiple drugs
were given, record the date the first drug was taken. For each of
the treatment types, describe as much as is known about the
following: Start and end dates Place/facility given Name of each
drug/treatment given Note: Other Treatment includes any treatment
that does not qualify as Radiation, Surgery, Chemo, Hormones, or
Immunotherapy. Other treatment also includes experimental and
non-traditional treatment. Hormone Date, Flag, Text Immunotherapy
Date, Flag, Text Other Treatment Date, Flag, Text
Slide 27
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Treatment Data on the New Case Abstract
Form - continued Data Field NameSpecial Coding Instructions Use the
following date fields to record the start date for each type of
treatment received for this tumor. If that particular treatment was
not given, leave the date blank and select code 11 as the
corresponding date flag. Refer to Section VII.2: General
Instruction for Using the Date Entry Screens for more information
on how to complete the Date and Date Flag fields. Use free text in
the corresponding text area to describe that particular first
course of treatment. See the definition of first course treatment
below. These text areas may be left blank if that particular
treatment was not given. No therapy is a treatment option that
occurs if the patient refuses treatment, the family or guardian
refuses treatment, the patient dies before treatment starts, or the
physician recommends no treatment to be given (patient is too sick,
watchful waiting, etc.). If no treatment is given, record the
reason for no treatment in any one of the following text areas.
Radiation Date, Flag, Text Record the start date for the radiation
therapy delivered to the patient as part of the first course of
therapy. In the text area, describe as much as is known about the
following: Start and end dates Place/facility given Area of body
treated Modality (type, energy) Dose (amount of radiation)
Slide 28
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.4: Entering Treatment Data on the Tumor Data Tab
continued Definition of First Course of Treatment First course of
treatment includes all methods of treatment recorded in the
treatment plan and administered to the patient at the time of the
initial diagnosis and before disease progression or recurrence. A
treatment plan describes the type(s) of therapies intended to
modify or control the malignancy. The documentation confirming a
treatment plan may be found in several different sources; for
example, medical or clinic records, consultation reports, and
outpatient records. All therapies specified in the physician(s)
treatment plan are a part of the first course of treatment if they
are actually administered to the patient. An established protocol
or accepted management guidelines for the disease can be considered
a treatment plan in the absence of other written documentation. If
there is no treatment plan, established protocol, or management
guidelines, and consultation with a physician advisor is not
possible, only record treatment that began within four months of
the date of initial diagnosis.
Slide 29
Part VIII: Entering Information Into the New Case Abstract Form
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.5: Entering Information on the Follow-up Tab continued
Enter the last date the patient was seen or the date of death.
Select the option which indicates the condition of the cancer at
the time of the visit.
Slide 30
Part VIII: Entering Information Into the New Case Abstract Form
Part VIII: Entering Information Into the New Case Abstract Form
Section VIII.5: Entering Information on the Follow-up Tab continued
Data Field NameSpecial Coding Instructions Vital Status The Vital
Status should remain Alive unless there is documentation of the
patients death prior to reporting the case. Follow-up Date (Date of
Last Appt.) This is the last date the patient was seen at your
facility, regardless of the reason for the visit or the disease
status. This should not be blank or unknown. *If Date of Death is
entered, it must be the latest date entered in the record. State
and Place - Country of Death Enter the state and country where the
patient died. Tumor StatusAt the time of the last visit to your
facility, indicate whether the patient had evidence of this disease
or was considered disease free.
Slide 31
Part VIII Entering Information Into the New Case Abstract Form
Completed