Embed Size (px)
Citation preview

Institutional Protocols for Decisions AboutLife-Sustaining Treatments
July 1988
NTIS order #PB89-138895

Recommended Citation:U.S. Congress, Office of Technology Assessment, Institution) Protocols for Decisions AboutLife-Sustaining Treatments —Special Report OTA-BA-389 (Washington, DC: U.S. Govern-ment Printing Office, July 1988).
Library of Congress Catalog Card Number 88-600547
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402-9325
[order form can be found in the back of this report)

Foreword
This special report extends the analysis provided in OTA0’s 1987 assessment of Life-Sustaining Technologies and the Elderly. That report documented the numerous, seri-ous uncertainties that complicate inherently difficult decisions about the use of medicaltechnologies that are potentially life-sustaining. OTA described uncertainties regard-ing: 1) outcomes of treatment—whether the patient will survive and, if so, with whatquality of life; 2) circumstances in which nontreatment may be ethical and legal; and3) decisionmaking procedures—whose judgment to seek, for what, and when, and howto resolve conflicts and ensure that a decision, once reached, is carried out.
To help reduce these various sources of uncertainty and their serious consequences,OTA suggested a variety of actions Congress might take. One of these was to focuson the policies and guidelines by which health care institutions circumscribe and articu-late the procedures they will follow in making decisions whether to initiate, withhold,or withdraw life-sustaining treatments.
This option struck a responsive chord in Senator John Heinz and RepresentativeEdward Roybal, requesters of the 1987 OTA report. Representing, respectively, the SenateSpecial Committee on Aging and the House Select Committee on Aging, they requestedthis study of the development and implementation of institutional policies and guide-lines for decisionmaking with respect to life-sustaining treatments.
This report was prepared by OTA based on a contract report by Steven H. Miles,M. D., and his colleagues at the University of Chicago’s Center for Clinical Medical Ethics.Other important contributors were the individuals who participated in the OTA work-shop on “Institutional Protocols for Decisions About Life-Sustaining Treatments” heldOctober 15, 1987. The workshop was a forum for discussion of key issues and reviewof the contractor’s draft. Participants were selected for their expertise in legal, ethical,and clinical problems related to the use of life-sustaining treatments and in some casesalso for their representation of major associations of health care institutions and profes-sionals. In subsequent months, workshop participants and additional outside reviewers(see app. C) commented on the revised draft. This final report incorporates many valu-able suggestions from all these individuals.
The authors and the members of the workshop represented a diversity of experi-ence and interests regarding the use of life-sustaining technologies. However, they agreedunanimously that institutional policies and guidelines such as those discussed here canbe a good approach for encouraging patients’ rights, institutional accountability, andethical treatment decisions, These individuals did not endorse any particular policy orset of guidelines, nor did they say that institutional policies and guidelines alone wouldsolve the problems in clinical decisionmaking. Project participants’ different views aboutwhat role, if any, Congress should take reflect an incomplete but noteworthy consensuson these difficult questions.

— .
Workshop Participants: Institutional Protocols for DecisionsAbout Life-Sustaining Treatments, Oct. 15, 1987
Marshall B. Kapp, ChairmanProfessor, Wright State University School of Medicine
Robert Wood Johnson Faculty Fellow in Health Care Finance, 1987-88
C. Ross AnthonyAssociate Administrator for Program
DevelopmentHealth Care Financing Administration
Mila A. AroskarAssociate ProfessorSchool of Public HealthUniversity of Minnesota
David AxelrodCommissionerNew York State Department of Health
Sr. Diana BaderSenior Associate for Clinical EthicsCatholic Health Association of the
United States
John H. BurkhartChairmanCouncil on Ethical and Judicial AffairsAmerican Medical Association
Nancy M. ColemanStaff DirectorCommission on Legal Problems of the ElderlyAmerican Bar Association
Msgr. Charles J. FaheyDirectorThird Age CenterFordham University
Susan HarrisGeneral CounselAmerican Health Care Association
Elma L. HolderExecutive DirectorNational Citizens Coalition on
Nursing Home Reform
Jane HoytChairpersonNursing Home Action GroupSt. Paul, MN
Alan MeiselProfessor of Law and PsychiatryCo-DirectorCenter for Medical EthicsUniversity of Pittsburgh
Nicholas RangoExecutive DirectorVillage Nursing HomeNew York, NY
Dorothy Rasinski-GregoryAssociate Chief of Staff/EducationVeterans Administration Medical CenterLong Beach, CA
William A. ReadPresidentHospital Research and Educational TrustAmerican Hospital Association
Paul M. SchyveDirectorDepartment of StandardsJoint Commission on the Accreditation of
Healthcare Organizations
Alan J. WeisbardExecutive DirectorNew Jersey Commission on Legal and Ethical
Problems in the Delivery of Health Care
Susan M. WolfAssociate for LawThe Hastings Center
Stuart J. YoungnerAssociate Professor of Psychiatry and MedicineCase Western Reserve University
School of Medicine
NOTE: OTA is grateful for the valuable assistance and thoughtful critiques provided by the workshop participants. The work-shop participants do not, however, necessarily approve or endorse this report. OTA assumes full responsibility for ‘the report and the accuracy of its contents.
iv

OTA Project Staff—Institutional Protocols for Decisions AboutLife-Sustaining Treatments
Roger C. Herdman, Assistant Director, OTAHealth and Life Sciences Division
Gretchen S. Kolsrud, Manager, Biological Applications Program
Claire W. Maklan, Study Director
Katie Maslow, Analyst
Sharon Kay Oatman, Administrative AssistantLinda Rayford, Secretary/Word Processor Specialist
Linda Starke, Contract Editor
Based on Report Prepared Under Contract,at The University of Chicago, by:
Steven H. MilesAssistant Professor of Medicine
Associate Director of the Center for Clinical Medical Ethics
Christine K. CasselAssociate Professor of Medicine
Chair, Section of General Internal Medicine
Mark SieglerProfessor of Medicine
Director of the Center for Clinical Medical Ethics
Carlos F. GomezPew Scholar in Medicine and Public Policy Studies
Bryan J. MarshPritzker School of Medicine

—
Contents
PageChapter 1: Rationale for Institutional Decisionmaking Protocols . . . . . . . . 3Social and Historical Context of Decisionmaking Protocols . . . . . . . . . . . . . . . . . . . . . . 4Objectives of Decisionmaking Protocols ., . . . . . . . . . . . . . . . . . . ... , . . . . . . . . . . . . . . 6
Objectives Related to Clinical Decisions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Objectives Related to Institutional Responsibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Chapter Z : Prevalence of Institutional Protocols: Current Status andFuture Prospects.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Current Situation .., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13In Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13In Nursing Homes and Other Health Care Institutions . . . . . . . . . . . . . . . . . . . . . . . . 14In Emergency Medical Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Incentives for Protocol Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Accreditation Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Other Incentives in the Private Sector, . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Incentives and Obligations in the public sector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Legal Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Barriers to Protocol Development and Implementation . . . . . . . . . . . . . . . . . . . . . . . . . 20Barriers Within Health Care Institutions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Public Policy Barriers. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Barriers Within Patient-Provider Encounters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Essential Steps in Protocol Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Recognition of Need.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Formation of a Drafting Committee . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Protocol Drafting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Staff Education and Commitment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Congressional Options. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Appendix A: Content and Format of Decisionmaking Protocols . . . . . . . . . 33General Comments. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Paradigms of Decisionmaking Protocols . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Specific Provisions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Appendix B: Sample Decisionmaking Protocols . . . . . . . . . . . . . . . . . . . . . . . . . 45Appendix C: List of Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75Appendix D: Glossary of Acronyms and Terms . . . . . . . . . . . . . . . . . . . . . . . . . 76Appendix E: References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
BoxBox PageA. Profiles of Individuals Facing Decisions About Life-Sustaining Treatments . . . . . . . 7
FiguresFigure Pagel. Public Interests and Institutional Responsibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82. Adoption of Decisionmaking Protocols in Minnesota Hospitals . . . . . . . . . . . . . . . . . . 14
vi

Chapter 1
Rationale for InstitutionalDecisionmaking Protocols
This report focuses on the formal policies andguidelines’ through which health care institu-tions articulate decisionmaking procedures andidentify permissible options regarding the use oflife-sustaining treatments for adult patients in theircare. Like the ethical dilemmas they seek to ad-dress, these policies and guidelines (referred tocollectively throughout this report as “institutionalprotocols” or “decisionmaking protocols”) are re-cent developments and still controversial. Theyare promoted by some—and decried by others—as facilitators of the complex and momentous de-cisions made daily in health care institutionsthroughout this country.
Protocols for making decisions about life-sus-taining treatments are used to reach decisions toprovide and decisions not to provide particulartreatments. Thus, they proceed from the beliefthat withholding or withdrawing life-sustainingtreatment is sometimes the right decision. Somepeople reject this basic position and, with it, theycategorically reject the idea of decisionmaking pro-tocols. Others reject the idea of decisionmakingprotocols because of their potential for misuse.It is certainly true that, if poorly designed orwrongly applied, decisionmaking protocols canlegitimize bad decisions, diffuse responsibility, orbe too rigid.
This report proposes that well-designed deci-sionmaking protocols at the institutional level of-fer positive benefits. Institutional protocols arenot held out as a panacea, nor as a way to maketreatment decisions easy. Moreover, no single pro-tocol will suit all institutions. However, thought-fully designed and accurately implemented pro-tocols are one promising and feasible method tofoster clinical decisions that are responsive simul-
‘See app. D for definitions. The protocols that are the subject ofthis report apply to health care decisions for adults of all ages. Pro-tocols for decisions about the care of newborns or minors, for whomdifferent considerations may be indicated, are not addressed.
taneously to the needs of patients and the obliga-tions of health care institutions and professionals.
The need to improve clinical decisionmaking aswell as the belief that institutional protocols willhelp to do so find strong support in OTA’s 1987report Life-Sustaining Technologies and the El-derly (156). For each of five life-sustaining medi-cal technologies (cardiopulmonary resuscitation(CPR), mechanical ventilation, renal dialysis, nu-tritional support (tube and intravenous feeding),and antibiotic therapy for life-threatening infec-tions), OTA reported on how clinical decisions aremade for elderly persons with life-threatening con-ditions, including who is involved and how deci-sionmaking varies from case to case and institu-tion to institution.
Despite general acknowledgment of patients’rights, OTA found that, in practice, treatment de-cisions are sometimes made unilaterally by phy-sicians or other caregivers without knowing, orwithout following, the wishes of individual pa-tients. Further, the serious clinical, legal, and ethi-cal uncertainties that prevail result in decisionsthat are inconsistent and, too often, wrong. Inaddition to the exigencies of each case, the typeof institution in which the patient receives care,the State in which it is located, and the particulartreatment being considered are among the varia-bles that affect how and by whom treatment de-cisions are made. Frequently, neither patients norhealth care professionals know ahead of time whatan institution’s response to particular treatmentrequests will be. OTA found both intense inter-est in means to reduce decisionmaking problemsand mistakes and widespread optimism about thepotential value of institutional protocols.
The suggestion that there might be a role forCongress in this matter derives from the fact thatmany hospitals and most nursing homes in thiscountry currently have no formal procedures re-garding decisionmaking about life-sustaining treat-ments. Moreover, the vast majority of existing in-
3

4
stitutional protocols are narrow in scope and leaveimportant questions unanswered. There is evi-dence of considerable interest in decisionmakingprotocols among health care institutions, as wellas forceful incentives in the form of new accredi-tation standards (see ch. 2). However, serious ques-tions remain about whether voluntary incentivesgo far enough and whether they are sufficientto overcome serious inter- and intra-institutionalbarriers to the development and implementationof effective decisionmaking protocols. Thus, thecentral congressional issue can be identified atthe outset: What steps, if any, should Congresstake with respect to institutional protocols fordecisions about lift+ sustaining treatments foradults?
In this era of concern about health care costs,skeptics warn that interest in institutional pro-tocols, including the Government’s interest inthem, might be motivated by efforts to reducehealth care costs—by reducing care. Certainly, re-cent changes in public and private reimbursementprograms (e.g., Medicare’s prospective payment
system and capitated payment agreements) pro-vide strong incentives for health care institutionsto restrain the use of expensive technologies (33).Institutions’ financial survival is now linked di-rectly to their ability to control costs generatedby individual patient care decisions, Thus, pro-tocols that make it easier to limit care might beadopted as a way to control costs. This potentialfor abuse necessitates careful articulation of thepublic interests to which health care institutionsare accountable—in addition to cost containmentand institutional survival.
Cost containment, especially in the form of lim-ited health insurance benefits, also affects patientdecisionmaking, forcing some patients to forgobeneficial treatments they otherwise would wishto receive. Institutional protocols that make it eas-ier for patients to refuse treatment must not atthe same time make it harder for those who wantrecommended treatment to get it. Questions abouthow financial considerations affect treatment de-cisions are be.vend the scope of this paper. Never-theless, they warrant careful study.
SOCIAL AND HISTORICAL CONTEXT OFDECISIONMAKING PROTOCOLS
The impetus for development of decisionmak-ing protocols can be traced to broad social trendsand to specific events within health care institu-tions. Traditionally, hospitals and other health careinstitutions were seen as places in which patientswould be provided whatever treatments—andonly those--deemed useful and appropriate basedon medical criteria (85). Challenges by patientsto a paternalistic model of health care were rare,health professionals seldom challenged their col-leagues, and administrators entrusted clinical deci-sionmaking to the clinicians.
Scientific, technological, social, and economicdevelopments over the past three decades havebrought major changes throughout the health caresystem. An impressive array of “life-sustaining”technologies, including new drugs, devices, andprocedures, emerged, and these technologies rap-idly became available in hospitals and other treat-ment settings throughout the country. Thesepowerful medical technologies have brought pa-
tients, health professionals, and families newhope—and new, often difficult, choices.
Difficult choices about medical care have beenaccompanied by new attitudes and behaviors thatare characterized, at least in part, by greater in-sistence on accountability. For example, interestin human rights and consumer advocacy of allkinds has led to the articulation of and demandfor patients’ rights. A general diminution of re-spect for and trust in traditional authority, includ-ing medical authority, has contributed to increasedmalpractice claims, peer review of physicians, andincreased regulation of health care facilities. Mul-tiple caregivers, the patient, and sometimes thepatient’s family members now expect to participatein treatment decisions. New treatment options,patient autonomy, the protection of vulnerablepatients, consideration of costs, and institutions’need to manage all sorts of “risks” have beenadded to the decisionmaking equation. In this envi-ronment, the complex relationships between phy-

5
sicians and patients, physicians and nurses, staffand administrators, and institutions and the pub-lic have been increasingly tested.
The special requirements of one particular life-sustaining technology stimulated thinking aboutand development of decisionmaking protocols. Ef-fective techniques for cardiopulmonary resusci-tation were introduced in the late 1950s.2 Thistechnology is distinguished by the need to applyit, if at all, immediately. Once a cardiac arrest oc-curs, taking time to deliberate or to consult wouldrender efforts at CPR uniformly useless. This factresulted in a general presumption in favor of pro-viding CPR, a presumption that came to be em-bodied in a “standing order.”
Although it was acknowledged that CPR is un-warranted if it is known in advance that a patientcannot be saved, the standing order could not beignored. In response to this dilemma, an Ad HocCommittee of the American Heart Association andthe National Academy of Sciences described the“do not resuscitate” (DNR) order, a physician’s or-der to countermand the standing order for CPR(118). The first hospital DNR policies were devel-oped in the late 1960s.
It was another 10 years before institutional pro-tocols regarding other life-sustaining treatmentsreceived explicit attention. Following the 1976 de-cision in the landmark case of Karen Ann Quin-lan (75), an editorial published in the New Eng-land Joural of Medicine proclaimed that “limitingmedical treatment” was “out of the closet” (55).The same issue included the policies of two hos-pitals regarding how decisions about life-sustain-ing technologies were to be made in these institu-tions (99, 132). These were not the first suchinstitutional protocols, but their assertive pre-sentation marked a new phase.
Institutional resuscitation policies and guidelinesreceived an important boost a few years later
2(:PR refers to a range of technologies that restore heartbeat andmaintain blood flow and breathing following cardiac or respiratoryarrest, Procedures range from “basic life support ,“ which uses man-ual, external rardiac massage and mouth-to-mouth ventilation, to“adlanced life support ,“ which may include prescription drugs andsophisticated dmices such as an electrical defibrillator, temporar}’card iac parrmaker and me(hanica] ventilator ( 156).
when they were advocated by the President’sCommission for the Study of Ethical Problems inMedicine and Biomedical and Behavioral Research(130). Presently, DNR policies remain the mostcommon form of institutional protocol regardinglife-sustaining treatment.
In some institutions, early DNR policies havenow been revised to reflect changes in thinkingand changes in needs. One significant change isexplicit concern with the patient wishes regard-ing resuscitation, not just medical judgments aboutits appropriateness or likely outcome. Also, someinstitutions have developed decisionmaking pro-tocols that go beyond considerations of resusci-tation to address other life-sustaining treatments.But many institutions are still struggling to getresuscitation protocols in place, and others havenot yet reached even that point. Among thosewithout a protocol in place, the reasons rangefrom ignorance, to opposition, to practical difficul-ties (57, 80) (see ch. 2).
Decisionmaking protocols within health careinstitutions need to be understood as just one ofseveral complementary mechanisms for improv-ing clinical decisionmaking for persons with life-threatening conditions. Legal tools for appointinga surrogate (or proxy) decisionmaker (especiallydurable power of attorney statutes) or for speci-fying advance directives (living will statutes) nowexist in many States. New Jersey has establisheda Commission on Legal and Ethical Problems inthe Delivery of Health Care, and New York Statehas a Task Force on Life and the Law, to advisetheir respective legislatures. Another approachis professional education and research by publicand private agencies, professional associations,and individuals. Complementing this, some educa-tional and advocacy groups (e.g., American Asso-ciation of Retired Persons, Nursing Home ActionGroup, Concern for Dying, Oregon Health Deci-sions, Vermont’s “Taking Steps, ” Society for theRight to Die, and Americans Against Human Suf-fering) direct their activities toward the generalpublic. Institutional ethics committees, now com-monplace in hospitals and beginning to appearin nursing homes, also fill a combination of rele-vant educational, advisory, and patient advocacyroles.

6
OBJECTIVES OF DECISIONMAKING PROTOCOLS
Decisionmaking protocols mediate the variousparties and interests to which health care institu-tions are accountable. If well-crafted and if im-plemented, they offer patients and their familiesprotection from poorly considered or imposedtreatment decisions; offer health care profes-sionals and institutions much needed guidanceabout ethical and legal dilemmas and a degree ofprotection from censure or liability by directingthem toward acceptable practices; and permit cus-tomization to the needs of individual institutions,
It is essential to recognize that the individualsfor whom institutions’ decisionmaking protocolsbecome important are an extraordinarily hetero-geneous population (156). A person dependent ona mechanical ventilator might be lying in a comaor, as was so dramatically shown by Senator JacobJavits, flying around the country giving speeches,contributing to public life and savoring his own.
To help illustrate the objectives of decisionmak-ing protocols (and, in app. A, the implications ofspecific design features), it is useful to describesome of the people who face decisions about life-sustaining treatments, The four hypothetical casespresented in box A (and referred to throughoutthe report) differ in diagnosis, prognosis, wishesregarding life-sustaining treatments, and capac-ity to participate in a treatment decision; they arein different kinds of settings and in very differ-ent social and economic circumstances. A hypo-thetical physician is also described to give somefeel for the ethical dilemmas that confront healthcare professionals.
Objectives Related to Clinical Decisions
Although ethical, legal, and professional codesalways presume in favor of sustaining life, thereis wide consensus that this presumption must beratified for each patient (62, 129, 130, 156). Life-sustaining treatment may be forgone when an in-formed patient declines it or when treatmentwould be futile. Similarly, withdrawal of treatmentis not permitted without the patient’s (or sur-rogate’s) consent. Thus, treatment decisions mustbe individualized, in light of each patient’s clini-cal situation, treatment objectives, and the bene-
fits and burdens of the particular treatment be-ing considered.
Encouraging appropriate, individualizedclinical decisionmaking is a major purpose ofprotocols for decisions about life-sustainingtreatments. This involves creating treatmentplans that accommodate Robert Swanson’s cate-gorical rejection of CPR as well as his wish to re-ceive other indicated life-sustaining treatments insome circumstances. It involves creating institu-tional means to allow Mary Hinkel to reject ag-gressive life-sustaining treatments while assuringshe will receive care to maintain her comfort anddignity. It involves creating procedures to ensurethat Thomas Johnson’s appointed surrogate willbe allowed to serve in that capacity. And it involvesprocedures that protect Mae Carver from deci-sions based on the judgment of other personsabout the quality of her life.
In addition to the overriding theme of individu-alizing clinical decisions, decisionmaking proto-cols purport to improve clinical decisions throughaiming to: clarify the rights, interests, and obliga-tions of all involved, i.e., patient, family members,and health care professionals; communicate prac-tice standards; establish mechanisms for imple-mentation of treatment plans, for staff accounta-bility, and for resolution of disputes; provideevidence of an institution’s effort to educate itsstaff as to standards of clinical practice; and fa-cilitate review to confirm either that proper carehas been given or that some changes are in order.
More specifically, proponents believe institu-tional protocols can improve clinical decisionmak-ing
●
●
if they:
decrease staff uncertainties about what prac-tices are permitted, particularly in such un-clear areas as termination of life-sustainingtreatments, decisionmaking for incompetentpatients, and decisionmaking when familymembers disagree;reduce stress and conflict among health careprofessionals, patients, and families concern-ing controversial, difficult, or complex treat-ment plans, by focusing discussion and offer-ing ethical guidance;

7
Box A.— Profiles of Individuals Facing Decisions About Life-Sustaining Treatments
Robert Swanson is an 84-year-old resident of the intermediate care section of a private nursing home.He is without family but active in the affairs of the home. He has stated clearly and consistently that hedoes not want any attempt at resuscitation in the event of a cardiac arrest, and he does not want anyform of life-sustaining treatment if he has lost the ability to interact with other persons. However, he hasstated with equal force that, as long as he remains able to interact socially, he does wish to receive aggres-sive life-sustaining treatment and emergency treatment to relieve symptoms of potentially fatal conditions.
Mae Carver is 64 and aphasic (unable to comprehend or express language), paralyzed on one side,and incontinent of urine since a massive stroke 2 years ago. She has resided for 8 years in the skilled nursingsection of a private nursing home, at public expense. She appears to enjoy food, television, and the compan-ionship of the nurse’s aides. She is not capable of clearly expressing any preferences regarding her healthcare, and she has no family.
Mary Hinkel is a 47-year-old woman whose advanced cancer has progressed despite surgery, chemo-therapy, and radiation. She has just been readmitted to the community hospital where she was previouslyin the care of an oncologist. Now she is back in the care of her family physician, who had not seen herfor 2 years. Hospital nurses know this patient from her many previous admissions. They have discussedwith her many times her wish to receive only palliative care and to forgo any treatments that would prolongher life. Mrs. Hinkel is confined to bed and near death.
Thomas Johnson is a 35-year-old with acquired immunodeficiency syndrome who is currently livingat home. He is well aware that, as his disease progresses, he may suffer serious cognitive losses and eventu-ally become incapable of participating in treatment decisions. For now, despite his physician’s reservations,he says that he wants all life-sustaining measures including CPR. But he strongly opposes life-sustainingtreatment in the event of permanent loss of cognitive function. Mr. Johnson is estranged from his family.His male companion has offered to serve as his surrogate if one is needed. Mr. Johnson wants to be assuredthat his wishes regarding life-sustaining treatments will be honored, whether he is still at home or in ahealth care institution, and that, if he cannot do so himself, this friend will be allowed to speak on his behalf.
Dr. Ruth Levin is medical director of Torah Home, a nursing home created and supported by a largeOrthodox Jewish congregation. Torah Home mainly serves elderly members of the congregation but isopen to noncongregants as well. Dr. Levin regularly encourages her staff to reflect on the ethical aspectsof their work. She, the rabbi, and the staff of the home are aware of recent court cases regarding discon-tinuation of nutritional support. While this is not an immediate clinical issue in their facility, they do notwant ever to be compelled, against their moral beliefs, to withhold or withdraw this particular life-sustainingtreatment from any resident.
● reduce ad hoc decisionmaking proceduresand arbitrary decisions;
● increase patient or family involvement intreatment decisions, by explicitly affirmingthe principles of patient autonomy and shareddecisionmaking, and by empowering patients;
● improve the accuracy with which decisionsabout life-sustaining treatments are imple-mented, by clarifying terminology and pro-cedures for implementing treatment plans;
● decrease confusion and conflict regarding theimplementation of plans or orders to limittreatment, by clarifying professional duties,and by suggesting processes and procedures
for making and implementing treatment de-cisions;
● improve accountability for decisions, by speci-fying duties and requiring signed documen-tation;
● reduce unwarranted fear of litigation, bysanctioning deliberative consideration and byrequiring documentation;
● reduce bad clinical practices such as deliber-ately ineffective resuscitation efforts, called“slow codes, ” either by prohibiting them orby offering morally and administrativelyacceptable alternatives;
. increase caregivers' empathy toward dying

8
patients, by creating processes that articulatepositive health care goals other than sustain-ing life, when this is no longer possible orwanted; and
● improve the ability to audit the quality of care,by establishing written accountability for sig-nificant treatment decisions.
Objectives Related to InstitutionalResponsibilities
The second major focus of decisionmaking pro-tocols is on institutional responsibilities to a vari-ety of public and private interests that are broaderthan those of any individual patient (see figure1). These responsibilities are the substance of “in-stitutional conscience, ” a conscience that is partlymoral (as in the case of Dr. Levin’s Torah Home),partly practical (as in the need to be Medicare-certified), and partly legal (as in the need to com-ply with State guardianship regulations). Thesediverse interests are embodied in law, accredita-tion requirements, a facility’s elected mission, orprofessional codes. The responsibilities, and per-ceptions of them, constitute the governance agendaof the institution, and they powerfully shape theactions that are permitted or encouraged, and thatare openly or covertly practiced.
protocols for decisions about life-sustainingtreatments provide formal mechanisms to address
Figure 1.- Public Interests and InstitutionalResponsibilities
Protection ofvulnerable patients Patient autonomy
I Institution
institutional responsibilities. Specifically, these in-stitutional policies and guidelines address the fol-lowing objectives:
1. Promote the institution’s responsibility tosafeguard the patient’s right to exercise auton-omy in personal health care decisions.
The principle of patient autonomy (as distinctfrom the autonomy of a particular patient) iswidely supported in statutory, constitutional, andcase law and by a consensus of bioethicists (62,75, 85, 130, 156). Further, the patient’s right toaccept or refuse life-sustaining treatments is thefoundation for institutional practices and proce-dures to formulate and implement treatment plans(6, 62, 130, 156).
In practice, however, patient autonomy is oftenlost or denied. Many patients are unable to com-municate their preferences and did not do so inadvance; health professionals sometimes fail tofully inform patients about options regarding life-sustaining treatments or they proceed to providetreatment without a patient’s (or surrogate’s) con-sent (156). Institutional protocols aim to supportthe treatment preferences of all patients—those,like Robert Swanson and Thomas Johnson, whoare decisionally capable and have expressed clearand firmly held treatment preferences, as wellas patients like Mary Hinkel, who previously ex-pressed her treatment preferences but can nolonger do so,
Patient autonomy is not, however, absolute.Thus, when forgoing life-sustaining treatmentwould result in direct harm to a patient’s minorchildren, autonomy may be restricted (18). Con-versely, patient autonomy does not mean thereis an unrestricted right to all health care a personmay want. Decisionmaking protocols intend to en-sure that patients receive desired treatments thatoffer them a chance of survival or improvedhealth, but they do not protect a claim on cos-metic surgery or other treatments that are notmedically indicated.
2. (Above and beyond #l): Promote protectionof vulnerable persons from decisions that arecounter to their preferences or interests.
Health care institutions are legally (77) andmorally accountable to the public interest to pro-

9
tect vulnerable patients.3 Protocols seek to ad-vance the welfare of vulnerable persons by ensur-ing proper oversight and deliberation of treatmentdecisions. Surgeon General C. Everett Koop andothers have asserted that nursing home residentsare especially vulnerable to having medical treat-ment improperly withheld because of prejudicedevaluations of the quality of their lives (67, 68,69, 73, 74, 87). This suggests that the protectionof vulnerable persons may be a particularly im-portant objective for nursing home protocols.
3. Promote the institution’s particular medi-cal or moral mission.
Many health care institutions are committed toa particular medical or moral mission (125, 150)that determines what treatment options will beavailable. This mission may reflect interests of thecommunity that formed and supports the facilityor it may be a strategy to attract patients witha certain viewpoint. For example, Dr. Levin’s To-rah Home is accountable to a moral view that pur-ports to enrich patient care by serving the needsof a particular community. By formulating pro-tocols that address their mission, institutions as-sert and seek to protect their individuality. Thus,a Catholic hospital might use an institutional pro-tocol to state its policy of not performing abor-tions (124). Hospices can describe their view ofappropriate care for persons with advanced can-cer; tertiary cancer treatment and research centerscan do likewise.
Clear, timely, public statements of an institutionalmission may also help avoid conflict over treat-ment plans. To a certain extent, patients and healthprofessionals can choose institutions whose mis-sion is compatible with their personal interests,or at least avoid institutions with incompatible mis-sions. It is unlikely that an institution’s mission(whether expressed in standards for minimal careor commitment to some religious doctrine) wouldhave legal precedence over the contradictory
3A]] patients with life-threatening conditions are vulnerable. Inthis report, the term “vulnerable patients” refers specifically to per-sons who are so ill or disabled that they are unable to leave a facilityor challenge its practices; lack decisionmaking capacity or the abil-ity to protect their own interests; lack family or friends to advocatetheir interests should they be unable to speak on their own behalf;or belong to classes of persons, like the elderly, whose interests maybe threatened by prejudire or stereotyping.
wishes of patients or their surrogates. However,if a patient claims a right to treatment that is in-compatible with the institution’s mission, it mightbe necessary to transfer the person to a differentinstitution, with a different mission.
4. promote the public interest in protecting thecivil liberties of individual staff, so as not tocompel them to perform duties to which theyhave a moral objection.
Health care facilities employ individuals whooften have their own deeply held views about theuse of life-sustaining treatments. The value thissociety places on moral pluralism and voluntarismweighs against compelling health care staff tocarry out treatment decisions to which they ob-ject (96). As long as it does not restrict a patient’sright to refuse treatment, individual staff may bepermitted to excuse themselves from patient care(39).
Institutional protocols can anticipate possiblestaff conflict by making provisions both for ex-cusing staff who have conscientious objections andfor transferring their patients to other providers,when necessary. For example, by permitting a phy-sician to withdraw from a case, a protocol couldenable Robert Swanson’s physician to stand byhis or her belief that it would be unconscionableto withhold cardiopulmonary resuscitation froma previously healthy 84-year-old.
S. Promote clinical practices that conform topublic policies, including statutes, regulations,and common law, as well as to voluntarystandards.
Health care institutions are accountable to therules and norms of society, and practices withinsuch institutions must be consistent with these.Thus, certain clinical practices are precluded, andno protocol will change this. The intentional ad-ministration of a lethal drug, for example, is pro-hibited, even if a patient like Thomas Johnson orRobert Swanson should request it. Similarly, in-stituting mechanical ventilation in a patient likeMary Hinkel, who has a clear, contrary directive,might constitute battery.
Protocols that encourage conformity to volun-tary standards also serve practical goals. For ex-ample, regulations of the Health Care Financing

10
Administration requiring physicians to be respon-sible for treatment orders must be met for eligi-bility for financial reimbursement, and standardsof the Joint Commission on the Accreditation ofHealthcare Organizations must be met for accred-itation. 4 Health care facilities that violate acceptedstandards face possible criminal, regulatory, orcivil sanctions—including fines, ineligibility forreimbursement, loss of required or desired ac-creditations, loss of licensure, placement in pub-lic receivership, suspension of admissions, or lossof teaching programs or prestigious affiliations(58, 68, 77, 79).
‘In 1987, the Joint Commission on the Accreditation of Hospitalswas renamed Joint Commission on the Accreditation of HealthcareOr&iIIkiMiOnS. Hereinafter, it k referred to as JCAHO or as the JointCommission.
6. Protect the institution from public notoriety.
Protocols that promote decisions that are con-sistent, ethical, and humane offer health careproviders a degree of protection from publicnotoriety. In addition, it appears that well-designeddecisionmaking protocols can reduce the risk oflegal action, and thereby also remove some of theunwarranted fear of litigation that at times con-strains ethical practice. Neither Robert Swanson’snursing home, nor Mary Hinkel’s hospital, norThomas Johnson’s physician has any legitimatefear that should cause them to fail to record andhonor the preferences of these individuals forlimited life-sustaining treatment. On the contrary,faithful implementation of decisionmaking pro-tocols that honor the treatment preferences ofindividual patients will help keep health care pro-viders out of the public eye.
CONCLUSION
Society has charged health care institutions toconserve a diverse set of public interests and,simultaneously, to protect the interests of indi-vidual patients. In general, since public interestsare grounded in a vision of good health care, theyconverge with the interests of patients. For ex-ample, patients are generally served by principlesembodied in accreditation standards, as well asby an institution’s cautious self-interest in not cut-ting corners in health care. As members of sec-tarian communities, patients are served by theavailability of health care facilities that strive toprovide care that respects the patient’s own moralviews. Disabled and vulnerable persons are servedby a special public interest in their welfare.
At times, however, necessary clinical choices pitpublic against private interests, or one public (or
private) interest against another. Containment ofMedicare costs versus assuring access to care isone example. Striving to provide optimal healthcare while respecting a patient’s right to refusetreatment is another. The high stakes in everydecision about initiating, withholding, or with-drawing treatment that is potentially life-sustain-ing escalate the seriousness and urgency of theseconflicts.
Institutional decisionmaking protocols that es-tablish procedures and identify the range of ac-ceptable choices offer a measure of guidance andauthority to assist the individuals who ultimatelymust make treatment decisions. Implementationof these protocols helps assure that similar caseswill be managed consistently and in accordancewith shared values.

Chapter 2
Prevalence of Institutional Protocols:Current Status and Future Prospects
This chapter examines the extent to which deci-sionmaking protocols already exist in hospitals,nursing homes, and other health care institutions,and considers current activities within the pub-lic and private sectors that may encourage or im -
CURRENT
Several surveys have tried to determine theprevalence of decisionmaking policies and guide-lines in hospitals and nursing homes, but avail-able data are incomplete and inconclusive. Thedata do reveal substantial growth in the preva-lence of protocols over the last decade, but theyalso suggest serious remaining deficits. In addi-tion, differences in focus, methods, and timingof completed surveys leave some important ques-tions unanswered. Some studies focus exclusivelyon do-not-resuscitate (DNR) policies; others reporton broader guidelines to limit treatment. Unspeci-fied definitions leave unclear what it means to havean “informal” protocol, to be “considering” devel-oping a protocol, or to “accept” orders fromanother institution.
National estimates of the prevalence of decision-making protocols come from a survey conductedin 1986 for the Joint Commission on the Accredi-tation of Healthcare Organizations (JCAHO) (93).Data were obtained from a stratified, random sam-ple of four kinds of health care institutions: acutecare hospitals, long-term care facilities, psychiatrichospitals, and hospice organizations. The reportprovided national estimates of the prevalence ofDNR policies as well as limited information aboutthe prevalence of policies for “withholding and/orwithdrawal of [other] treatment.”
In Hospitals
Of the four types of institutions surveyed, theJoint Commission found that acute care hospitalswere the most likely to have a policy regardingresuscitation. Fifty-seven percent of acute care
pede future development. Taking these existingincentives and barriers into account, the final sec-tion identifies and discusses five congressional op-tions for promoting wider adoption and use ofdecisionmaking protocols.
SITUATION
hospitals reported that they had a “formal” DNRpolicy in place in 1986; another 28 percent saidthey had an “informal” policy. The national sur-vey found (and this is consistent with findings fromsmaller surveys) that DNR policies were most com-mon in large, urban hospitals, especially those withacademic or religious affiliations. Most of the hos-pitals with no resuscitation policy were small andlocated in rural areas. Only 20 percent of all re-sponding hospitals reported that they addressedissues of withholding and withdrawing treatmentsother than resuscitation (93).
Published examples of hospital protocols includethose by: F.P. Arena et al. (15); Beth Israel Hospi-tal (26); City of Boston, (36); F. Davila et al. (46);R.S. Duff (50); M. Halligan and R.P. Hamel (60);Los Angeles County (94); M. Mahowald et al. (97);Massachusetts General Hospital (99); A. McPhailet al. (100); A. Meisel et al. (104); S.H. Miles et al.(107); Northwestern Memorial Hospital (123); Pres-byterian University Hospital (128); T.E. Quill etal. (131); Somerville Hospital (140); St. Joseph’sHospital, St. Paul, MN (143); St. Joseph’s Hospital,Orange, CA (144); University of Wisconsin Hospi-tal (155); J. Van Eys et al. (159); L. Volicer (162);and Yale New Haven Hospital (169).
National data obscure possible State-to-State andregional variations. Information on the prevalenceof decisionmaking protocols in different parts ofthe country comes from a handful of surveys con-ducted within single States and one multi-Statesurvey. A survey in five Midwestern States (Illinois,Indiana, Iowa, Michigan, and Wisconsin) foundthat 35 percent of the responding hospitals had
13

14
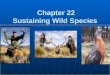
a formal DNR policy in 1982, and an additional24 percent were in the process of developing one(117). The next year, a survey of Minnesota hos-pitals found that 44 percent of acute care hospi-tals had adopted DNR protocols and another 8 per-cent had protocols for “supportive care only” (seefigure 2 and app. A) (110). A 1986 survey by NewYork State’s Task Force on Life and the Law (122)found that only 29 percent of the responding hos-pitals had written guidelines for determining apatient’s capacity to participate in a treatment de-cision.
The fact that large numbers of hospitals haveno decisionmaking protocol or have one that dealsonly with resuscitation increases the probabilitythat the treatment preferences of the hypotheti-cal patients described in chapter 1 would be car-ried out, if at all, only partially, and largely bychance. The majority of acute care hospitals appar-ently do have a protocol that provides a meansto implement a DNR order. If Mary Hinkel is ad-
Figure 2.-Adoption of Decionmaking ProtocolsIn Minnesota Hospitals
0
mitted to one of those hospitals, her advance direc-tive rejecting cardiopulmonary resuscitation (CPR)is likely to be implemented, But how many pa-tients know, upon admission, whether the hospi-tal has a protocol or what it says? Further, evenwhile honoring her DNR request, on-call person-nel might also provide Mary Hinkel with unwanteddiagnostic tests or unwanted, potentially life-sustaining treatments such as intravenous antibi-otics. For patients like Thomas Johnson, evenwhere there is a protocol permitting the treatmenthe wishes, problems can still arise if the protocoldoes not specify who may serve as decisionmak-ing surrogate.
In Nursing Homes and Other HealthCare Institutions
The first nursing home protocols regarding de-cisions about life-sustaining treatments were de-veloped several years after hospital ones, and theirprevalence remains much lower. In 1986, only 20percent of nursing homes reported having a writ-ten DNR policy and another 29 percent said theyhad an “informal” policy (93). Published examplesof nursing home protocols include those by: KingCounty Medical Society (86); S.A. Levenson et al.(88); J.D. Hoyt and J.M. Davies (67, 68); Task Forceon Supportive Care (149); and R.F. Uhlmann etal. (152).
A 1984 sample survey of nursing homes in Min-nesota found that only 10 percent of the respond-ing institutions had a DNR protocol and 16 per-cent had institutional protocols for “limitedtreatment .“ At the same time, the majority of theseinstitutions said that they “accept DNR orders”(73 percent) or ‘(accept orders for limited treat-ment” (66 percent) (112). A 1984 survey of alllicensed nursing homes in the Portland, OR, met-ropolitan area reported that 41 percent of the re-sponding institutions had a policy regarding resus-citation (89). New York State’s Task Force alsosurveyed nursing homes, but did not ascertainthe prevalence of resuscitation protocols. It wasdetermined that only 13 percent of New York’snursing homes, in 1986, had written guidelinesfor determining residents’ capacity to participatein treatment decisions, despite the fact that staffestimated nearly half their residents had no ca-

15
pacity and a fourth had only partial capacity tomake decisions (122).
This low level of formal protocols in nursinghomes means that for a patient like Robert Swan-son, refusal of CPR will be difficult to implement.Moreover, his ability to prevail in rejecting life-sustaining treatments other than CPR would belimited by the particular provisions of the nurs-ing home’s protocol and by his ability to clearlyexpress his qualified request. For a patient likeMae Carver, who cannot speak for herself, theabsence of a protocol that makes the decisionprocess explicit and opens it to public question-ing can invite inattention to her wishes or bestinterests.
In 1986, 15 percent of nursing homes reportedthat they had protocols addressing withholdingand withdrawing life-sustaining treatments otherthan resuscitation (93). Examples described in theliterature consider decisions about nutritional sup-port, antibiotic therapy, and transfer to hospitals(25, 30, 59, 64, 88, 112).
The Joint Commission’s national survey also ob-tained data for representative samples of hospiceprograms and psychiatric hospitals across thecountry (93). In 1986, 43 percent of hospice pro-grams reported that they had a formal DNR pol-icy in place. Among psychiatric hospitals, only 11percent had such a policy. About 12 percent ofthe hospices and fewer than 2 percent of the psy-chiatric hospitals said they had protocols on with-holding or withdrawing other life-sustainingtreatments.
In Emergency Medical Services
Decisionmaking protocols also have a place inemergency medical services (EMS). Paramedics
and technicians employed by most emergencymedical services are required to provide aggres-sive life-sustaining treatment, without asking ques-tions. This practice can conflict with an order ina patient’s record or with a patient’s advance direc-tive, especially in a health care system that tendsto automatically transfer people to a hospital whena cardiac or respiratory arrest occurs (63).
To date, very few emergency medical serviceshave developed protocols that allow paramedicsto honor a DNR order received from a nursinghome or hospice home care program (98, 108,116). Thus, nursing home and home care patientslike Robert Swanson or Thomas Johnson mighthave their rejection of life-sustaining treatmentshonored so long as they remain in the nursinghome or at home, but they might face unwantedtreatment if transferred. In some places, the onlyapparent way to avoid an EMS standing order forCPR is to not call the service if a patient who hasdeclined CPR has a cardiac or respiratory arrest(25, 64, 88). This practice would protect patientslike Robert Swanson and Thomas Johnson fromunwanted CPR, but it could also deprive them ofdesired treatment for reversible conditions or forthe prompt relief of severe distress.
Ideally, a single, coordinated set of protocolswould be in place for the emergency medical serv-ice and the health care institutions that might callit, but this exists in very few places. In Minneapolis,the EMS developed a model protocol for nursinghomes and for home care programs to go alongwith its own (108, 116). Detailed discussion of in-terfacility protocols and the portability of pro-tocols is beyond the scope of this report. (For fur-ther information on this subject see, e.g., the articleby S.H. Miles (106) or the forthcoming book byS.H, Miles and C. Gomez (109).)
INCENTIVES FOR PROTOCOL DEVELOPMENT
Within both the public and the private sector, Accreditation Standardsa variety of incentives and requirements pushhealth care facilities to develop decisionmaking JCAHO accredits more than 5,000 of the 6,000protocols. To date, the action likely to have the general hospitals in this country and over 3,000most far-reaching impact is adoption by JCAHO other health care facilities. Thus any Joint Com -of an accreditation requirement regarding resub- mission position on decisionmaking protocols car-citation protocols. ries great weight. In spring 1987, the Joint Com-

—
16
mission approved a new standard that requiresall accredited hospitals to adopt a policy on “with-holding of resuscitative services” (78). Hospitalswere required to have a resuscitation policy inplace by January 1, 1988; nursing homes mustdo so by July 1988; and psychiatric facilities musthave one by January 1989. Similar standards forhospice programs accredited by the Joint Com-mission preceded these by a few years.
For hospitals and nursing homes, the Joint Com-mission’s new standards are essentially the same.They direct the chief executive officer to providefor development and implementation of a resus-citation policy that is developed in consultationwith medical staff, nursing staff, and “other appro-priate bodies.” The Joint Commission requiresthat:
●
●
●
●
●
the resuscitation policy be designed “to as-sure that patients’ rights are respected,”procedures be described for reaching deci-sions about withholding resuscitation and forresolving conflicts,orders regarding resuscitation be written bythe physician primarily responsible for thepatient,orders be documented in the patient’s medi-cal record, andthe medical staff of the hospital (or physicianmembers of the nursing home’s professionalstaff) and governing body of the institutiongive formal approval before the resuscitationpolicy takes effect.
This action by the Joint Commission will un-doubtedly lead to development of a DNR policyin many institutions that currently do not haveone. Even institutions that are not applicants foraccreditation by the Joint Commission may bemotivated to develop DNR protocols becausestandards of that influential body can serve asquasi-legal standards of practice to which any in-stitution may be held accountable (see section onlegal considerations), For hospitals, moreover, ac-creditation by JCAHO confers ‘(deemed status” forpurposes of Medicare certification. Still, the in-fluence of any voluntary incentive clearly is notunlimited. In addition, JCAHO’s requirements areconservative, in that they say nothing about life-sustaining treatments other than resuscitation.
Other Incentives in the Private Sector
Incentives for developing decisionmaking pro-tocols also come from the professional associa-tions to which institutions or their staff belong.Numerous associations of health care institutionshave developed position papers or educational ma-terials promoting development of decisionmak-ing protocols, though most have stopped shortof specifying procedures to follow (156). The “Pa-tient’s Bill of Rights” of the American Hospital Asso-ciation (AHA) endorses the patient’s right to re-ceive information about his or her diagnosis,treatment, and prognosis, and to refuse treatment“to the extent permitted by law” (7). A 1983 posi-tion paper of the AHA (134) encouraged develop-ment of institutional protocols regarding resus-citation decisions.
The American Health Care Association, repre-senting about 9,000 (out of approximately 17,000)nursing homes (158), circulated a report on “HealthCare Decisionmaking in Long-Term Care Facilities”(6). This report encouraged development of in-stitutional protocols for “life-and-death” decisionsand identified topics that should be addressed.The Catholic Health Association of the UnitedStates (CHA) provides educational programming,consultation, and publications to encourage estab-lishment of institutional ethics committees, institu-tional protocols, and use of advance directives.Upon request, CHA distributes samples of deci-sionmaking protocols to member hospitals andnursing homes, currently numbering over 900(17).
Associations of health care professionals alsosupport various means of improving and stand-ardizing decisionmaking procedures. The bien-nial Current Opinions of the Council on Ethicaland Judicial Affairs of the American Medical Asso-ciation (AMA) spells out standards of conduct forphysicians in relation to withholding or withdraw-ing a variety of life-sustaining treatments. In 1986the AMA took the controversial position that “life-prolonging medical treatment includes medicationand artificially or technologically supplied respi-ration, nutrition or hydration” (10). In December1987, the AMA Council on Ethical and Judicial Af-fairs recommended to the AMA House of Delegates .that “hospital medical staffs, with the approval

of governing boards, adopt statements of policyregarding do not resuscitate (DNR) orders. ” Thereport stated that “DNR policies should be basedon medical, ethical, legal, and community stand-ards and should be consistent with any religiousprinciples adhered to by the hospital,” and it in-cluded some specific suggestions individual hos-pitals might consider in draftingaDNRpolicy(11).
State medical societies also influence the activi-ties of their members and the hospitals and nurs-ing homes in which these professionals work. Min-nesota’s was the first State medical association toadopt DNR guidelines, in 1981. This provided amodel for physicians belonging to that associa-tion and for the medical associations of some otherStates. By 1985, 40 percent of all State medicalassociations had adopted a model policy or modelguidelines for DNR decisions (105). One physicianspecialist association that has addressed the sub-ject of institutional protocols directly is the Amer-ican College of Emergency Physicians. The asso-ciation has resolved to develop a model protocolon how emergency medical services should ad-dress DNR orders (I, 2) and has taken the posi-tion that decisions to forgo resuscitation in thefield must be in accord with written protocols (3).
The American Nurses’ Association (ANA) andsome State nurses’ associations encourage theirmembers to consider the appropriate role ofnurses in decisionmaking about withholding orwithdrawing life-sustaining treatments and to cre-ate formal documents on these topics. Examplesinclude the ANA’s Guidelines for Nurse Participa -tion and Leadership in Institutional Ethical ReviewProcesses (12), the California Nurses’ Association“Statement on the Nurse’s Role in Withholding andWithdrawing Life-Sustaining Treatment” (32), andthe Florida Nurses Association resolution on“Clients Rights Regarding Administration of Arti-ficial Sustenance” (52).
Decisionmaking protocols have also been de-vised and encouraged by individual researchersand by research organizations. A notable exam-ple is a 1987 publication by the Hastings Center,Guidelines on the Termination of Life-SustainingTreatment and the Care of the Dying (62). In addi-tion, citizens’ groups (149, 152) and State and lo-cal health departments (36, 94, 145) have pro-moted decisionmaking protocols.
Incentives and Obligations in thePublic Sector
The Veterans Administration (VA) exemplifiesa large, public network of health care institutionsin which central management now requires deci-sionmaking protocols for life-sustaining treat-ments. Throughout the VA system, the norm hasbeen to provide CPR to every patient who sus-tains a cardiopulmonary arrest “except where themedical record contains a DNR order or resusci-tation would be futile or useless. ” A new chapterin the VA Manual makes explicit the autonomyof terminally ill patients (VA Manual, M-Z, Pt. 1,ch. 30, change 81, Aug. 18, 1987), requiring thatall VA Medical Centers develop a protocol “for deal-ing with issues involved when terminally ill pa-tients request no CPR. ” At the discretion of in-dividual VA hospitals, ‘(terminally ill” can bebroadened to include persons who are chronicallyill with no hope of recovery (133).
Another new chapter of the VA Manual will ad-dress life-sustaining treatments other than resus-citation and the withholding and withdrawing ofthese treatments in situations other than cardio-pulmonary arrest. ’ The DNR protocols of indi-vidual VA Medical Centers may vary, but all mustaddress the provisions and principles outlined bythe Central Office. Following the VA model, deci-sionmaking protocols could be imposed by cen-tral management in other public health care sys-tems and in jointly owned or managed privatehospital and nursing home chains.
The approach taken in New York State illustratesanother way public action can lead to decision-making protocols in health care institutions. InJuly 1987, New York enacted legislation that clar-ified the rights and obligations of patients, familymembers, and health care professionals in mak-ing decisions about resuscitation (N.Y. Pub. HealthLaw §§ 2960-78). The legislation, effective April1, 1988, requires all hospitals, nursing homes, andmental health facilities in the State to develop DNRprotocols consistent with the provisions of the leg-islation. The law was enacted in response to twowidespread problems: the entry of DNR orders
‘Chapter 31 of the L’A Manual (M-Z, Pt. 1) is currently undergo-ing final rek’iek~ (133).

18
without the consent of patients or family mem-bers, and the provision of resuscitation when itwas medically futile because of fear of liabilityfor entering a DNR order explicitly.
Legal Considerations
The central legal problem related to institutionalprotocols is whether or not they have the forceof law (103). These protocols may be character-ized as a form of private, interstitial lawmaking(35, 103)–private lawmaking in that they are cre-ated by nongovernmental entities yet may turnout to have legal force; interstitial lawmaking inthat they make rules on topics that are not gov-erned (or not governed clearly) by existing judi-cial, statutory, or regulatory law.
Like judicial, statutory, and regulatory law (i.e.,public law), institutional protocols establish sub-stantive standards for conduct and set forth rulesof procedure for determining the applicability ofthose standards to particular cases. Unlike pub-lic law, however, it is uncertain whether institu-tional protocols will be found by the ultimate ar-biters of law—the courts-to have the force of law.The result is serious uncertainty about the roleof protocols in potential litigation concerning life-sustaining treatments.
The potential role of institutional protocols inlitigation is a key concern of litigation-conscioushealth care institutions and health professionals.To date, the subject has received little explicit con-sideration, and it remains an “open question” (35).The possible effects of protocols range from pre-venting litigation to inviting it. And if litigation doesensue, protocols may constitute evidence thatranges from irrelevant to conclusive. In this un-certain environment, counsel for different healthcare institutions will continue to offer differentadvice about the pros and cons of protocols andabout their particular provisions. However, someof the factors likely to determine the role of pro-tocols in litigation can be identified and controlled,thus increasing the probability that protocols areto the institution’s, as well as the patient’s, ad-vantage.
Whether protocols forestall or invite criminalor civil litigation depends mainly on three factors:consistency with existing Federal and State law,
consistency with accepted standards of practice,and faithful implementation (113). Protocols thatmeet these conditions can be expected to providea degree of legal protection to institutions and topersons who are responsible for their adoptionor implementation. Thus implementation of a hos-pital protocol to withdraw mechanical ventilationfrom a brain-dead patient is legally low-risk if theprotocol’s provisions for determining brain deathmeet accepted professional standards and if Statelaw recognizes brain death, On the other hand,when a protocol conflicts with the law or fails tomeet professional standards, litigation—with a de-cision against the institution—is a realistic con-cern. A New York grand jury, for example, con-cluded that a hospital’s use of colored dots on anonpermanent record (rather than use of a writ-ten DNR order) “eliminated professional account-ability, invited clerical error, and discouraged phy-sicians from obtaining informed consent” (47, 58,170).
The first factor in determining the effect of in-stitutional protocols is consistency with existinglaw. The effect of a protocol is safest, from theperspective of institutional liability, and most cer-tain when the protocol accurately embodies Statelaw. While such protocols (or particular provisionsof them) may perform important educational func-tions within health care institutions, they have noindependent legal effect because health care pro-viders who rely on them are in reality relying onexisting law.
Protocols that go beyond the law–in that theystake out institutional positions on issues that havenot been addressed (or have not been thoroughlyor clearly addressed) in legislation, regulation, orjudicial decision—are more helpful to health careprofessionals, but their legal effect is less certain.For instance, an institutional protocol may rec-ognize and give effect to living wills, even in Statesthat have no living will law. (As of January 1987,38 States and the District of Columbia had enactedliving will laws (156),) The legality of withholdingor withdrawing life-sustaining treatments in reli-ance on such a protocol is uncertain.
Institutional protocols that clearly and directlyconflict with existing State law are an invitationto litigation, the result of which may be adverseto the health care institution, its employees, and

19
staff acting in reliance on the protocol. For exam-ple, the living will statutes of at least eight Statesspecifically proscribe the withholding or with-drawing of nutritional support (156). At the sametime, many institutional protocols regard artifi-cial nutrition and hydration as medical treatmentsthat may, like other life-sustaining treatments, bewithheld from terminally ill patients who refusethem. It would appear that to follow such a pro-tocol raises serious legal risk. In fact, however,courts have repeatedly concluded that the livingwill statute is only one way to exercise the rightto refuse treatment and that the right to rejectartificial feeding exists independently (40, 42, 70,71, 76).
Some institutional protocols conflict with thespirit, but not the letter, of existing law. An exam-ple would be a protocol that permits withholdingor withdrawing of artificial nutrition and hydra-tion at the request of a patient who is able to makeand express a contemporaneous, informed deci-sion, in a State where the living will statute pre-cludes withholding of artificial nutrition andhydration. Natural death acts apply specificallyto the advance directives of patients who are cur-rently unable to participate in decisions about theircare. It can be inferred that the legislative intentis to prohibit the withholding of artificial nutri-tion and hydration. On the other hand, in the ab-sence of clear legislative history, it is also reason-able to conclude that the legislature merely meantto prohibit the withholding of artificial nutritionand hydration from patients who lacked the ca-pacity to make a contemporaneous decision aboutso significant an issue, rather than to override theclear preferences of a decisionally capable patient(103).
An institutional policy is more likely to becreditable to a court, and thus more likely to pro-vide a defense in litigation, if it is embodied inwriting and formally adopted by the institution.The New Jersey Supreme Court would not sup-port a nursing home’s wish to discharge a patientwhose treatment preference (discontinuation ofnutritional support) was morally objectionable tothe facility (73). Instead, the Court ordered thenursing home to discontinue tube feeding forNancy Jobes, who was in a persistent vegetativestate for 7 years (72). In doing so, the court noted
that the nursing home’s ‘(policy” against discon-tinuing nutritional support was unwritten and thatthe patient’s family had not been informed of thispolicy before requesting that treatment be dis-continued. The opinion left open the question ofwhether the institution’s obligation might havebeen interpreted differently had the patient’s fam-ily been prospectively informed of the informalpolicy. (Ultimately, Mrs. Jobes was transferred toMorristown Memorial Hospital, where nutritionalsupport was discontinued and she died.)
Protocols that go beyond existing law (but donot clearly conflict with it) are more likely to berecognized by courts as valid (and therefore toprovide protection from liability) if they are con-sistent with prevailing professional standards ofpractice. In legal procedures, a protocol could bevariously interpreted as evidence of a standardof care, as a safety code, as defendant’s own rules,as a Iearned treatise, or as inadmissible evidence(35). Since the 1965 Darling decision 45), policiesof health care institutions pertinent to their dutyto patients have been consistently admissible asevidence of a standard of care and, as such, con-sidered along with other relevant evidence.
The standard of care, established by commonlaw or statute, is the criterion by which healthcare professionals can be found liable if their con-duct results in injury to a patient, or by whichhealth care institutions can be found liable fornegligence if conduct of their employees resultsin injury to a patient. Traditionally, the standardof care is established by the common law stand-ard of “reasonable care. ” That is, in order not tobe held liable, an individual must act as a reason-ably prudent person would under like circum-stances. Where the person sought to be held lia-ble is a professional, the “usual and customary”standard of practice of the profession is strongevidence of what constitutes reasonably prudentcare.
In the Darling decision, standards of JCAHOwere for the first time accepted as evidence ofa standard of practice (24, 127). Based on failureto meet the Joint Commission’s standards of prac-tice regarding appropriate care of a patient’s bro-ken leg, as well as violation of its own internalpolicies, the hospital was held directly liable for

20
injuries to the patient. Since Darling, standardsof JCAHO have been used routinely by the courtsto determine negligence by health care institu-tions. Although such institutions may not be ex-plicitly required to conform to standards proposedby professional associations or accrediting bod-ies, nonconformity—if causally connected to a pa-tient injury--can be used as evidence of negligentinstitutional administration. This lends added im-port to the Joint Commission’s new standard call-ing for resuscitation policies.
differently in different places. However, there isno evidence that institutional protocols that areconsistent with the law and with standards ofpractice increase legal risk, and there is some evi-dence they reduce risk, especially compared withresort to ad hoc or halfway procedures, such as“slow codes” and undocumented DNR orders (82).Accumulating case law, statutes like New York’s,and new accreditation standards make a strongcase for the legal benefits of protocols.
In summary, the legal effects of protocols havenot been tested directly, and thus will be viewed
BARRIERS TO PROTOCOL DEVELOPMENT AND IMPLEMENTATIoN
As noted in chapter 1, substantial consensus al-ready exists among the public, the health profes-sions, and the law regarding fundamental prin-ciples for shared decisionmaking and patientautonomy. However, considerable work remainsto be done to realize this consensus in practice,and theoretical and practical problems impede ef-forts to develop and implement protocols that havethis goal, Moreover, consensus appears a long wayoff on some issues, especially appropriate use ofnutritional support and appropriate care of un-communicating, dying persons who did not pre-viously express treatment preferences.
Barriers to development and implementation ofprotocols for decisions about life-sustaining treat-ments extend all the way from private fears ofdeath to political and practical problems in effect-ing institutional and public policy change. The in-tensity and complexity of these private anxietiesand public interests suggest there is no simplemeans to overcome them. In addition, these bar-riers are interconnected, each reinforcing theothers. For example, Mary Hinkel’s difficulty inraising her wishes with her physician accommo-dates the physician’s reluctance to yield a pater-nalistic claim on medical decisionmaking, RobertSwanson’s complex and conditional care plan goesbeyond the simplified assumptions of many nurs-ing homes’ supportive care policies (see app. A).Health care facilities that are sensitive to the needsof vulnerable persons like Mae Carver have noframework for balancing the benefits of treat-
ment, the burdens of overtreatment, and theirown financial interests.
Thus, the first hurdle for those trying to developa decisionmaking protocol may be to revise thegoal of accomplishing what is ultimately hopedfor or what seems intellectually complete in fa-vor of goals that are attainable in the short termand that at least improve the status quo, Develop-ment of decisionmaking protocols is best seen asan incremental process, building over time on anexisting, evolving consensus. In addition, becausethe barriers are interrelated, efforts to resolvethem will involve cooperation among health careinstitutions, practitioners, educators, patients, asso-ciations, foundations, and government agencies.
Barriers to development and deployment of in-stitutional protocols, as well as some potential so-lutions, are discussed here under three generalrubrics: barriers within health care institutions,in the domain of public policy, and in interper-sonal encounters between patients and health careprofessionals. As will be indicated, problems arisein each stage of protocol development.
Barriers Within Health CareInstitutions
Different kinds of health care institutions facedifferent problems in attempting to develop andthen implement decisionmaking protocols, Vari-ations in institutional mission, patient population

21
served, staff size and composition, available treat-ments, regulatory requirements, and organiza-tional complexity are among the major variablesthat distinguish health care institutions from eachother and that may facilitate or impede protocoldevelopment. Other distinctions-including whethernonprofit or proprietary, with academic or with-out academic affiliation, sectarian or nonsectar-ian, urban or rural, and government or private—are also important. The following barriers can oc-cur in any kind of institution.
Inadequate MultidisciplinaryStaff Forums
Health care institutions are staffed by diversegroups of professionals with different perspec-tives, knowledge, roles, and interests. Physicians,nurses, social workers, allied health workers, law-yers, and administrators have different relation-ships with patients and with each other, (And thepatterns are different in different types of insti-tutions.) As a result, their views on the use of life-sustaining treatments and on what constitutesappropriate decisionmaking often conflict (54, 156,168). Forums for communication and exchangeamong those who are responsible for makingtreatment decisions and those who must carrythem out provide a base for developing protocolsthat effectively integrate treatment planning,caregiving, and legal responsibility.
Several existing types of multidisciplinary fo-rums could be instrumental in protocol develop-ment and, later, can play a key role in implement-ing the protocols by educating staff about theirrationale, interpretation, and use. Ethics commit-tees have already assumed an active role in pro-tocol development. However, one-fourth to one-half of all hospitals (especially small and rural ones)still have no ethics committee (156). In nursinghomes, well over 90 percent may have no ethicscommittee. (A national survey found “a minimumof 2 percent” of nursing homes do have an ethicscommittee (56).) (For a review of the purposes,uses, and forms of institutional ethics committees,see, e.g., the book by R. E. Cranford and A. E.Doudera (44), the report of the president’s Com-mission (130)) or the article by F. Rosner (135).)
Patient care conferences are another forumfrom which protocols could emerge, provided time
is reserved from talking about day-today detailsfor more generalized discussion of ways to im-prove patient care. In some institutions, ad hocprotocol committees, study groups, or investiga-tive task forces have been convened. Another pos-sible forum for consideration of protocols is utili-zation review committees; however, because theprimary agenda of these committees is cost con-tainment, some people warn against this (105).
For a variety of reasons, health care institutionshave limited ability to establish and sustain themultidisciplinary interaction necessary to createand implement decisionmaking protocols. In somefacilities, especially small nursing homes and ru-ral hospitals, limited staff size (both in absolutenumbers and relative to the workload) is a majorobstacle. Many clinicians resist committee work;crowded schedules, competing demands, and lackof interest incline them against it. In most nurs-ing homes, physicians’ limited presence makes col-laboration with other staff difficult. This worksagainst the resolution of role-related tensions andagreement on treatment plans or policy issues.
Inadequate Expertise
Another substantial barrier to protocol devel-opment is inadequate expertise among staff in ei-ther clinical ethics or health care law. Health carestaff are often not fully informed of current opin-ion in clinical ethics, especially in complex, con-stantly evolving areas such as surrogate decision-making. professional ethicists are increasinglyseen in hospitals, but institutions with a staff ethi -cist are still very exceptional. Approximately 300professional ethicists are employed by hospitalsin this country (80).
Many health professionals also have mistakenviews of their legal and professional duties (83).Moreover, misconceptions among health profes-sionals are sometimes amplified by lawyers forthe institution or by insurance companies that is-sue malpractice policies (23). Also, attorneys whoare unfamiliar with recent developments in med-ical ethics or with the constraints of clinical prac-tice (as well as those inclined to rely on the judi-cial process for dispute resolution) may giveinaccurate or unrealistic advice regarding over-sight, surrogate designation, or dispute review.For example, lawyers for health care institutions

22
may conclude that lack of absolute protectionsoffered by explicit governance of clinical decision-making does not warrant the effort required todevelop a protocol. Indeed, as noted earlier, somelawyers believe that a decisionmaking protocolcould increase the institution’s risk of liability orpublic notoriety.
Obtaining or building the necessary expertisewill require personal and institutional commit-ments of time, money, and support for ethics andlegal education to develop a core of staff to serveas resources in every health care facility. oncestaff are trained and protocols are developed, on-going programs of staff education will be requiredto encourage implementation of improved deci-sionmaking practices.
Inadequate Leadership
Some health care institutions, especially nurs-ing homes, lack leaders who can identify the needfor decisionmaking protocols and can initiate andsustain the multidisciplinary effort needed to de-velop and implement them. Inadequate leadershipmay take the form of resistance to protocols. De-spite publicity and pressure on health care insti-tutions about the value of decisionmaking policiesand guidelines, observers report that many peo-ple still believe such protocols are not needed (80)or that they will have no effect on health care(159), will abridge physicians’ prerogatives (100),will increase patients’ anguish (21, 91, 141, 160),or will be used to discriminate against personswith severe disabilities (41). Others charge thatdecisionmaking protocols are an attempt to engi-neer rather than to inculcate values into practice(84).
Inadequate leadership is often associated withinadequate resources for ethics activities, espe-cially shortages of financial support, staff time,and clerical assistance. Lack of leadership to cre-ate and sustain multidisciplinary staff forums isa common problem, as noted earlier. Unpublisheddata suggest that many nursing homes have notdeveloped protocols because no one in the insti-tution has identified their function or need (33).
Leadership might be strengthened througheducational programs within health care facilities,focused on the fundamental issues of good clini-cal decisionmaking practices. Such programswould be appropriate for all staff and adminis-trative groups. One element of this educationmight be the dissemination of prestigiously en-dorsed model protocols that could be adapted toindividual facilities. External pressures,JCAHO standards, might also effectivelyage leadership within institutions.
Public Policy Barriers
Inadequate Theory ofInstitutional Governance
such asencour-
The individual goals and responsibilities of in-stitutional governance with regard to decisionsabout life-sustaining treatments have not been ade-quately defined or interrelated. Public attentionhas so far focused on distinct clinical decisionmak-ing principles, such as patient autonomy, not onhow to integrate treatment decisions into a com-prehensive understanding of a health care facil-ity’s total governance duties. The uncertainty thatresults when diverse responsibilities conflict (seeapp. A) is a disincentive to creating institutionalprotocols. Another problem is that public policy(in the form of statutes, case law, and institutionalprotocols) can leave unclear the interpretation ofsuch key concepts as “decisionmaking capacity”and medical “futility.” In addition, as discussed,basic questions about the legal status of institu-tional decisionmaking protocols remain unan-swered. All these problems impede both devel-opment and implementation of protocols.
For nursing homes, an additional public policyproblem is related to the highly regulated envi-ronment in which they operate. Federal and Stateregulations, and especially what some people per-ceive as their inconsistent interpretation, createwhat may be a unique and serious barrier to de-velopment of protocols in nursing homes. A nurs-ing home surveyor may judge a decisionmakingprotocol either as an asset or as an outrage. Un-. .

23
able to predict which, some nursing home adminis-trators believe that a protocol with which a nurs-ing home surveyor might find fault is worse thanno protocol at all (61). This kind of uncertaintyargues for examining the regulations and mak-ing sure they are understood by those who en-force them.
Questions involving the interrelationships of thevarious responsibilities that health care institu-tions must balance warrant careful study. Betterunderstanding of these interrelationships wouldhelp guide both public policy and clinical policiestoward the goal of improving decisions and ad-vancing public interests.
Inadequate Financial Supportfor Ethics Programs
The costs to health care institutions of employ-ing professional ethicists, establishing and main-taining an ethics committee, and training healthcare staff in clinical ethics are high. Health careinstitutions that undertake these initiatives cur-rently do so without public support, often by ab-sorbing the expense into their net costs. Ethicsconsultations, education, and related activities(especially ethics education of those who teachcore staff in all health care disciplines) are essen-tial to improving health care decisionmaking. Re-quiring certain minimum standards of ethics pro-gramming would help ensure that health carefacilities allocate funds, staff, and other support.
Financial support might come from Federal,State, or private sources. Grants would be espe-cially appropriate for support of academic or re-search initiatives, such as evaluative research onprotocol design and pilot programs for staff andpatient education and counseling, as discussedearlier. The day-to-day operation of ethics pro-grams within health care facilities will probablyneed to be supported as a general administrativecost. Some commentators have proposed that phy-sician time to educate and inform patients aboutoptions regarding life-sustaining treatments bedirectly reimbursed by health insurance (53).
Present data and auditing procedures do notallow good estimates of the costs of protocol de-sign, staff education, the operation of ethics com-mittees, or related activities. To a certain extent,the reduction of misdirected or unwanted medi-cal treatment and litigation would offset the costsof this programming.
Barriers Within Patient-ProviderEncounters
Patients’ Inadequate Knowledgeor Motivation
Implementation of a decisionmaking protocolrequires a degree of support and cooperation onthe part of patients or their surrogates. That is,while protocols specify procedures to follow whenthe patient cannot participate in a treatment de-cision and when no surrogate has been designated,they assume that when the patient is able to par-ticipate and when a surrogate is designated, heor she will in fact do so—either by taking partin discussions at the time the treatment is beingconsidered or by making a clear directive or ap-pointing a surrogate in advance.
However, some patients who are decisionallycapable and the surrogates for some patients whoare not decisionally capable have great difficultydiscussing such personal and serious problemsfrankly, or they are unable to grasp the medicaland legal information presented to them. Somepatients choose to defer decisionmaking respon-sibility to their physician or to a family member(156). Others resist giving an advance directive,fearing its mere existence might preclude discus-sion even while they remain able to participatein a decision (66). After 15 years of spirited pub-lic debate, only a small percentage of patients havediscussed treatment preferences with their fam-ilies or physicians or have written an advancedirective such as a living wiill.2
Whe only known data on this subject ~ome from a 1986 surle~’
of Oregon households. Researchers found that adults in 82 percent
of sampled Oregon households had heard about li\ing t~ills, Hot\ -e~’er, respondents in only 16 percent of households said the} hada Ii\’ing will. In households tiith one or more person(s) oi’er age65, 23 percent reporting haling a ]il ing Jvill (20)

24
One way to reduce this problem is public edu-cation regarding patients’ rights and principles forresponsible decisionmaking. A major objectivewould be to foster dialog within families as wellas between patients and health professionals. Suchpublic education would primarily aim to protectpatient autonomy through encouraging advanceplanning for health care decisions. For efficiency,the educational effort could be directed to indi-viduals whose progression toward death or in-competence is foreseen.
Health Professionals’ InadequateKnowledge or Motivation
Like patients, staff of health care institutionsoften have a poor understanding of decisionmak-ing principles or, more likely, lack the fortitudeto apply them in difficult clinical cases. In caringfor patients who are critically or terminally ill,health professionals’ personal fear of death and
fear of failure as a healer may make them delayraising the subject of life-sustaining technologiesor may make them unable to discuss treatmentoptions with sensitivity and openness. Timely andskillful communication with patients and theirloved ones are basic to the implementation of deci-sionmaking protocols.
One solution is to translate the principles forgood communication and shared decisionmakinginto practical terms so that health professionalsare motivated and capable of applying them con-sistently and in timely fashion. Professional train-ing of those who care for persons with potentiallylife-threatening conditions must also inculcate real-istic attitudes toward death and dying and towardthe role of health care professionals, to promotebeneficial communication. Part of this educationwould focus on clinical ethics and, in particular,respect for persons who are elderly, disabled, orotherwise vulnerable.
ESSENTIAL STEPS IN PROTOCOL DEVELOPMENT
Development and adoption of decisionmakingprotocols appear to have four distinct stages. Theresources and routines of health care institutionsmay be challenged at each stage, and the incen-tives and barriers just described can influence de-velopments throughout the process.
Recognition of Need
The first step in developing a decisionmakingprotocol is to recognize that decisionmaking prob-lems exist, to embrace the idea that a formal pro-tocol will reduce these problems, and to put pro-tocol development on the institutional agenda.Anecdotal accounts (100, 159) suggest that the spe-cific events and individuals within a facility thatpropel protocol development are quite varied: anew kind of case may raise legal and ethical un-certainties; difficult treatment decisions for a fa-vorite patient may cause staff conflict; a lawsuitagainst the facility (actual or threatened) or a pub-licized legal case elsewhere may heighten legalfear; awareness that a neighboring facility has aprotocol may stimulate competition; concerned
staff may believe that a decisionmaking protocolwill improve responsiveness to patients’ needs;or consumer groups such as nursing home resi-dents’ councils may push for clarification of deci-sionmaking practices.
The events and perspectives that sometimesstimulate development of protocols exist in allkinds of health care institutions. These may rein-force and help prepare the way for any legal oraccreditation requirements that, in effect, forceinstitutions to recognize their need for a decision-making protocol. Because the events and theirinterpretation vary, they may lead to differentkinds of protocols. For example, if a CPR case trig-gers discussion, CPR maybe all the resulting pro-tocol addresses. Conversely, if the precipitatingproblem concerns other treatments, the protocolthat is developed may be more inclusive.
Formation of a Drafting Committee
Another prerequisite to protocol developmentis committed leadership. This may come from the

25
administration, ethics committee, chaplaincy of-fice, or clinical staff. Protocol drafting maybe as-signed to an existing group, often an ethics com-mittee, or to a special task force (e.g., of a medicalpractice review board). Self-selected, ad hoc draft-ing committees are seldom empowered by thehighest governing boards, though they may re-ceive encouragement from senior administrators.Rather, their strength stems from their internalleadership and the commitment of a core groupof respected staff associated with their effort. Offi-cial empowerment may come later, when thegroup’s purpose and track record are clearer.
For reasons discussed in the preceding section,successful protocol development is greatly facili-tated by a multidisciplinary staff team. Typically,this includes physicians, nurses, social workers,clergy, ethicists, and administrators. The actualcomposition depends in part on the size and na-ture of the facility’s staff: physicians tend to bemore prominent in hospital committees; nursesand social workers, in nursing home committees.Other staff members will round out the group.Some people believe that involvement of the in-stitution’s legal counsel throughout the processof protocol drafting is especially valuable. Thishelps ensure that counsel has an understandingof clinical and ethical issues, without which heor she may be unable to provide either construc-tive evaluation of the finished protocol or realis-tic advice during the drafting process.
Protocol Drafting
The drafting process commonly begins with sev-eral meetings to allow members to express theirconcerns and set an agenda for member educa-tion. To start, drafting committees need familiar-ity with and understanding of current policies andpractices within their institution regarding deci-sions about life-sustaining treatments. The headof one drafting committee reported that an in-formal survey of staff helped identify sources ofconfusion, conflict, and consensus, and therebyhelped focus the work of the committee (80).
Although decisionmaking protocols are meantto fit the specific interests and circumstances ofindividual institutions, this does not mean thateach drafting group must “recreate the wheel. ”
Published protocols provide a range of startingpoints and ideas. Some drafting committees startwith a published policy or set of guidelines or usea protocol of a neighboring facility as the basicstructure. Other committees rely on “model” pro-tocols to guide their work. These are advisory doc-uments, developed by institutions or individualsclaiming special expertise or authority, for the ex-press purpose of assisting health care facilities indeveloping their own policies or guidelines. (Ex-amples of model protocols include those by: Amer-ican Hospital Association (9); Bar Association ofSan Francisco (19); Hastings Center (62); J.D. Hoytand J.M. Davies (67, 68); Joint Commission (78);Medical Association of Alabama (101); Medical So-ciety of NY (102); Minnesota Medical Association(115); Task Force on Supportive Care (149); R.F.Uhlmann et al. (152); Veterans’ Administration(161); and S.H. Wanzer et al. (165).)
Amendments to a good model should be vigor-ously debated, but they may be necessary when,to cite one consideration, external agencies im-pose requirements on a facility that are not ade-quately addressed in the model. For example, ex-isting models for DNR protocols will have to beamended if they fail to meet specifications of theJoint Commission’s new standard. Models alsomight be amended to conform to local usage ofkey terms, in order to decrease confusion amongpractitioners working at several different insti-tutions, or to improve communication in interfa-cility transfers (106).
Adaptations may be made to conform to spe-cial moral (150) or medical (159) missions, or toidentify specific officers or bodies responsible forimplementing and revising the protocols (114). Anursing home chain operating within a single Stateshould be able to design a model that can be usedby all its facilities with a minimum of modifica-tion. However, models proposed by nationalgroups may need to be substantially changed ifthey are to work in diverse facilities in differentStates. In anticipating the diverse needs of theinstitutions starting from a single model, somemodels provide a “menu” of optional provisions,applicable or acceptable to certain institutions andcertain purposes. After dissemination of a model,followup research could look at the adaptationsmade by different institutions and evaluate whether

26
these suggest needed changes in the model itself(111).
Drafting an original protocol or adapting anavailable model does more than produce a pro-tocol for a particular facility. The process is a cru-cial one, through which health care staff can learnthe intent and operation of the protocol and cometo “own” its provisions. This is another reason itis important to have wide representation in thedrafting and review process. Restricting discus-sion to the administrative or trustee level, as hassometimes been done, is bound to create prob-lems later.
Health care institutions usually crosscheck theproposed protocol at several levels. Most protocolsgo through numerous drafts within the commit-tee, where terms and concepts are vigorously de-bated. Early drafts might be circulated among clin-ical supervisors and other key personnel, and laterdrafts among the entire staff for comment andrevision. In addition to permanent medical staff,it is important to include housestaff and nurses—the individuals who often must implement the pro-tocols. This process is crucial if a facility like To-rah Home is to claim that the protocol representsthe moral position of staff or of the institution.Institutions may enlist outside ethics consultantsor lawyers before finalizing a decisionmaking pro-tocol. Some people take the position that repre-sentatives of all groups that will be affected bythe protocol should have a say in its development.This suggests that patients and family represent-atives should also be involved in the drafting orreview (23, 80).
Protocol drafting is a difficult process that cantake a longtime. Moreover, the importance of the
protocol and the educational value of the processitself argue against rushing (171). Personal ac-counts of experience in several large universityhospitals suggest that, from start to finish, pro-tocol drafting and adoption often takes a full year,and sometimes 2 years (16, 80, 104, 171).
Staff Education and Commitment
It can never be assumed that creation and adop-tion of a decisionmaking protocol ensures its ac-curate and reliable implementation. Ideally, theprocess of protocol development has created amultidisciplinary core of staff who understandthe rationale for the policy or guideline and itsapplication to their work, and who will help toeducate their trainees and coworkers. Provisionfor ongoing staff education to promote familiar-ity with, understanding of, and commitment tothe protocol is an important component of thetotal effort to develop a decisionmaking protocol.Moreover, the agenda for staff education isbroader than the procedures outlined in the pro-tocol. It includes education in the ethical and le-gal principles that underlie good decisionmakingand their application to clinical care.
Protocol implementation also requires sustainedand coordinated leadership and commitment bythe institution’s administration. This must extendbeyond the leadership of the individuals or com-mittees that initiated development of the protocol.Only institutional leadership can establish mech-anisms for the periodic review of adopted pro-tocols and for allocation of funds and staff timefor ethics committees and in-service training.
CONGRESSIONAL OPTIONS
The central issue for congressional considera-tion was identified at the outset of this report.3
3Many of the congressional policy options presented in chapter1 of OTA’S report Life-Sustaining Technolo&”es and the Elderly (156)pertain to improved decisionmaking. In particular, OTA identifiedstrategies that address access to health care, patients’ rights, andsupport for research to improve clinical decisionmaking. The op-tions presented here expand on that discussion.
What steps, if any should Congress take withrespect to institutional protocols for decisionsabout life-sustaining treatments for adults?The potential range of congressional responsesis as follows:
● Option 1: Take no action.● Option 2: Seek more information.● Option 3: Encourage and facilitate, within

27
●
●
the private sector and the States, voluntaryapproaches to addressing problems in clini-cal decisionmaking.Option 4: Encourage States and voluntaryagencies to adopt consistent and enforceablestandards for decisionmaking.Option 5: Instruct the Health Care Financ-ing Administration (HCFA), the Public HealthService, other agencies of the Department ofHealth and Human Services (DHHS), the VA,and the Department of Defense to adopt reg-ulations to require health care facilities un-der their authority to do one of the following:5a: Adopt a resuscitation protocol compara-
ble to that required by JCAHO;5b: Adopt a decisionmaking protocol that
contains, as a minimum, elements speci-fied directly or indirectly by Congress; or
5C. Adopt a protocol prescribed by Federallaw.
Any congressional action to encourage and im-prove institutional protocols for decisions aboutlife-sustaining treatments will proceed in the con-text of ongoing private-sector and State and localinitiatives. It could be argued that the activitiesof non-Federal legislatures, courts, and regulatorybodies, as well as private voluntary organizations,collectively provide sufficient incentives and assis-tance to promote better decisionmaking regard-ing life-sustaining treatments. If this is the case,congressional initiatives in this area would be un-necessary or redundant, and no congressional ac-tion is warranted (Option 1).
Among the members of OTA’s workshop panelfor this project, representing many of the majorassociations of health care institutions and profes-sionals, the option of no congressional action re-ceived only one strong vote of support. The chair-man of AMA’s Council on Ethical and JudicialAffairs indicated that he “and probably most doc-tors” would find congressional action in this areaunwarranted and unnecessary.
Many people, including the vast majority ofOTA’s workshop panelists, argue that Congresscould play a helpful role by actively seeking moreinformation on how treatment decisions currentlyare made, on the effects of decisionmaking pro-tocols, and on the adequacy of voluntary meas-ures to promote them (Option 2). This could be
accomplished by holding hearings or by appropri-ating support for research through DHHS. Advo-cates of such research include the American BarAssociation, whose February 1988 conference onBirth, Death and Law recommended that researchon treatment decisions precede any effort to en-courage new legislation, since existing law maybe adequate (92).
Various aspects of the research agenda for sup-porting optimal decisionmaking protocols havebeen discussed in the preceding sections. Theseinclude study of how best to meet the objectivesof protocols and how to overcome barriers to theiradoption and implementation, specifically:
●
●
●
●
If
research that tests the basic assumptions ofinstitutional protocols—i.e., that they improveclinical decisionmaking and reduce legal riskto health care institutions;trials of various model protocols and of meth-ods to train health care professionals in theiruse, especially addressing protocols in nurs-ing homes, emergency medical services, andhome care, where experience is most limited,to determine what specific design featureswork best;research to refine definitions of critical con-cepts used in decisionmaking protocols andhealth law, e.g., “decisional capacity,” “termi-nal illness, ” and “treatment futility”; andresearch on model legislation for advancedirectives and interfacility communication ofthem.
such research substantiates the presumedbenefits of institutional protocols, its dissemina-tion might help to encourage their wider adop-tion. Also, specification of the impact of variousprotocol designs could assist Congress, as well asthe States and individual health care institutions,to formulate effective solutions to meet particu-lar needs.
Option 3 is for Congress to encourage and pro-mote, within the States and the voluntary sector,activities that are related broadly to reducing prob-lems in clinical decisionmaking. Activities alreadyoccurring at the State level that may warrant con-gressional acknowledgment and support includepassage of living will legislation; development ofcommissions to advise State legislatures on mat-

28
ters of health care ethics (New Jersey and NewYork); and development of grassroots organiza-tions concerned with ethical dilemmas in healthcare (California, Oregon, Vermont, and elsewhere).The contributions of professional associations, in-dividual health care institutions, and private orga-nizations include education, advocacy, and re-search. Emphasizing State-level and voluntaryactivities would maximize flexibility and creativity,and take advantage of existing initiatives. A seri-ous reservation, however, is that many States donot have the committed leadership or resourcesto take up matters of health care decisionmakingin an effective or timely way. The Federal Gov-ernment could facilitate dissemination of infor-mation among the States.
Another approach is for Congress to encourageStates and non-Federal health care systems tovoluntarily develop and adopt enforceable stand-ards that support consistent and ethical decisionsabout life-sustaining treatments (Option 4). Amongthe diverse examples are the decisionmakingguidelines developed for nursing homes in Cali-fornia by that State’s department of health, NewYork’s legislation on resuscitation, and JCAHO’sstandard requiring resuscitation protocols in theinstitutions it accredits. Development of suchstandards might be encouraged by Federal grantsto support State and local legislation, research,education, and institutional initiatives. Financialsupport would facilitate and stimulate a varietyof local solutions, from which much could belearned. It would also signal the seriousness andurgency with which Congress views this matter.
Option 5 would provide more definitive congres-sional leadership by imposing Federal regulationon decisionmaking practices within health careinstitutions. This could be accomplished by man-dating the adoption of decisionmaking protocolsin all Federal health care institutions and by add-ing decisionmaking protocols to the requirementsfor certification for Medicare and Medicaid. Thevast majority of hospitals and nursing homes inthe country would thus be affected.
In mandating decisionmaking protocols, Con-gress could leave a great deal, or nothing at all,to the discretion of individual institutions. Onepossibility (Option 5a) is to require that institu-
tions adopt the resuscitation standard of JCAHO.This standard indicates general topics that mustbe addressed in any resuscitation protocol with-out specifying what the protocol will or will notallow. Alternatively, Congress could require allFederal health care institutions as well as non-Federal institutions that receive Medicare or Med-icaid reimbursement to adopt decisionmaking pro-tocols that go beyond decisions about resuscita-tion and that include certain specific features(Option 5b). Finally, Congress could prescribe com-plete decisionmaking protocols and insist on theiradoption without modification (Option 5C).
The idea of congressionally mandated protocols(whatever the degree of specificity) assumes thatprivate-sector and local initiatives are and will re-main inadequate. Such a mandate was stronglyadvocated by only one OTA workshop participant,the director of a nursing home. He argued thatprotocols are far less likely to be developed if leftto voluntary efforts and that, in many places, forCongress to “not mandate” is equivalent to “allownot to be done. ” The majority of workshop par-ticipants believed that the intense pursuit of thesequestions by the health care sector, State legisla-tures, legal groups, patient advocacy groups, andacademic centers suggests no lack of will. Still,some would argue, Congress could assume leader-ship in this area.
If Congress were to mandate adoption of deci-sionmaking protocols, this could be in accord withone or more long-range goals. For example, thegoal might be for all health care institutions tohave a protocol in place by some specified futuredate, say 1990 or 1992. Alternatively, Congresscould set target dates by which hospitals, thennursing homes, and then other kinds of healthcare institutions would have a protocol in place.This type of long-range plan would encourage ex-perimentation and permit time for research andaccumulating experience to be put to good use.
With Option 5a, resuscitation protocols wouldbe adopted throughout the health care system,based on the most current and most widely ac-cepted of private-sector standards, namely thoseof JCAHO. Determination of specific provisionsof protocols would be left to the individual insti-tutions, as would be the work of protocol devel-

29
opment, but the standards of JCAHO would pro-vide guidance. Current HCFA regulations forMedicare and Medicaid certification have no ana-log to the recent JCAHO requirement for a resus-citation protocol.
Option 5a is really a conservative step in thatthe new decisionmaking protocols it requireswould not necessarily address life-sustainingtreatments other than resuscitation, despite agrowing consensus that this is important. Further,the majority of non-Federal hospitals are alreadyobliged to meet the Joint Commission’s resuscita-tion standard, and many Federal institutions (nota-bly VA facilities) are already required to have aresuscitation protocol. The main effect of Option5a would thus be to increase the adoption of resus-citation protocols in private institutions that arecurrently not accredited by the Joint Commission.The effect in nursing homes would be more sig-nificant than in hospitals since the majority ofnursing homes are not accredited by JCAHO.
Option 5b is for Congress to mandate that allFederal hospitals and nursing homes and all non-Federal institutions that receive Medicare or Med-icaid funds adopt a decisionmaking protocol thatmeets certain specified, minimal requirements.Regulations associated with Option 5b could, forexample, specify that protocols must address de-cisions about life-sustaining treatments in addi-tion to resuscitation. Minimal, essential elementsof protocols could be identified without impos-ing rigid solutions and without attempting to becomprehensive. For example, Congress could in-sist that protocols indicate how the patient’s ca-pacity to participate in a decision will be assessed,
without imposing a method for this assessment,Further, Congress could insist that all protocolsaddress assessment of capacity and documenta-tion of decisions without suggesting that these es-sential elements make a complete protocol.
Support for mandatory decisionmaking pro-tocols that are partially or totally prescribed byCongress assumes that Congress or the agencyto which protocol design would be assigned is well-qualified for this task. Among participants at OTAworkshop, some strongly opposed the idea of Con-
gress mandating protocols with content even par-tially specified. Some people reject, in principle,legislative involvement in the details of clinicalpractice. Others appreciate the laudatory intent,but fear that the actual regulations would quicklyexceed the few ideas on which there is a soundand stable consensus.
The most active congressional role would be todictate specific conditions and procedures for de-cisions about the use of life-sustaining treatments(Option 5c). This approach would eliminate thevariability that now exists from institution to in-stitution and State to State. However, objectionsto Option 5b apply and are multiplied. I.ack ofempirical research on the strengths and weak-nesses of particular features of protocols suggestsit would be premature for Congress (or for anyother group) to attempt to write an acceptable“national” protocol. Congressional action to directclinical decisionmaking in advance of a consensusfrom leadership within the health care industrywould be immensely controversial, would be un-likely to succeed, and might preempt construc-tive public discussion,

Appendix A
Content and Format ofDecisionmaking Protocols
General Comments
Decisionmaking protocols currently in use differ inscope, content, format, and style. In this section, threegeneral protocol designs and some significant differ-ences of style and content are described.
While considering the differences among protocols,it is useful to remember that all have the same prin-cipal goal: to help a physician and patient (or surrogate)choose the most appropriate care for an individual pa-tient. Each approach to protocol design has advantagesas well as disadvantages, and each has features thatfit particular circumstances better or worse. It is prob-ably premature to conclude that any single approachis best or that any approach should be avoided.
Some advocates of institutional protocols believe thatthe essential test is whether a protocol indeed works,i.e., whether it successfully encourages dialog abouttreatment questions and subsequent development andimplementation of appropriate treatment plans (16).Delineating the effects of different types of protocolsand of specific features will require careful empiricalstudies. Such evaluative studies could accompany theongoing process of protocol design and updating.
There has so far been very little investigation of theeffects of institutional protocols on decisionmakingpractices. Thus, numerous studies have reported thatphysicians often do not involve patients in decisionsabout resuscitation (21, 22, 51, 138, 153, 156, 166, 172,173) but very few studies relate this finding to the pres-ence or absence of a do-not-resuscitate (DNR) protocol.Two hospital studies reported that the use of DNRorders increased after a DNR protocol was introducedand that understanding of DNR orders improved (22,131). Another study reported that hospital staff readthe DNR protocol and said it helped their practice be-cause it clarified the processes of making and imple-menting decisions to withhold life-sustaining treatmentand encouraged more open dialog (100). More detailed
studies of protocols and of specific design featurescould lead to more effective protocol design.
Voice: Prescriptive v. Advisory
One key distinction among decisionmaking protocolsis the “voice” with which the processes of making andimplementing decisions are addressed. These processesmay be addressed either by a prescriptive voice (char-acteristic of policies) or an advisory voice (character-istic of guidelines). The difference should be kept inmind in order to avoid using prescriptive language forprinciples that are intended to be advisory, or viceversa.
Hallmarks of the prescriptive voice are precise as-signment of responsibility for decisions and detailingof procedures to be followed in implementation. “Thenurse acknowledges the order by co-signing the ‘levelsof treatment order sheet ’,” for example, is a policy state-ment (154). This is quite unlike the advisory statement“It is wise for the primary physician to ensure throughfurther discussion that the patient family has full un-derstanding of the decision” (37). The prescriptive voiceis especially appropriate for stating fundamental in-stitutional precepts, directing that essential proceduresbe accomplished, and coordinating interactions amonghealth care professionals. Prescriptive language is lesswell suited to directing the subtle encounters of phy-sicians, patients, and family (84), especially in areaswhere practice standards are incompletely defined.(Published policies include those by: Beth Israel Hos-pital (26); City of Boston (36); Los Angeles County (94);Massachusetts General Hospital (99); A. McPhail et al.(100); Northwestern Memorial Hospital (123); PresbyterianUniversity Hospital (128); Somerville Hospital (140); E.V.Spudis et al. (142); University of Wisconsin Hospital(155); L. Volicer et al. (163); and Yale New Haven Hos-pital (169).)
The advisory or teaching voice of guidelines seemsbetter suited for assisting health care professionals.
33

34
Guidelines suggest approaches to morally and legallydifficult decisions about life-sustaining treatment whileallowing interpretive latitude to accommodate the am-biguity of clinical situations. Guidelines can elaborateon fundamental principles (e.g., patient autonomy), ex-plain the rationale for policy provisions (e.g., the roleof an ethics committee), or suggest approaches for dif-ficult clinical situations (e.g., assessment of decision-making capacity or initiation of discussion about lim-iting treatment). (Examples of published guidelinesinclude those by: M. Halligan and R.P. Hamel (60); Hast-ings Center (62); S.A. Levenson et al. (88); J. Van Eyset al. (159); St. Joseph’s Hospital, St. Paul, MN (143);St. Joseph’s Hospital, Orange, CA (144); and S.H, Wan-zer et al. (165).)
The flexibility of guidelines can accommodate thenuanced and idiosyncratic physician-patient-family en-counter (129, 139). This flexibility also allows for aninitial, provisional articulation of an emerging con-sensus within an institution regarding how to addressdecisions about life-sustaining treatments, Some peo-ple believe that the flexibility of guidelines should beretained in the final protocol; others maintain thatguidelines are an agreement on principles for decision-making about life-sustaining treatments, from whichmore detailed procedural duties might later be derived(159).
Prescriptive and advisory language are often com-bined in a single protocol (e.g., 26, 104, 107). Ideally,the prescriptive language sets minimal standards forprocedural accountability and implementation, and theadvisory language elaborates on subjects or ideals thatare too elusive to be captured in prescriptive language.Protocols that employ prescriptive language to stateadvisory principles lead to confusion. Examples includeprotocols that restrict the right to refuse life-sustainingtreatment to persons who are “terminally ill. ” Omis-sion of any reference to persons who have not beendiagnosed as terminally ill implies that they do not havethe same right (100, 161).
Other Elements of Style
Several general principles can be recommendedbased on experience to date with protocols in healthcare facilities across the country.
Protocols are intended to influence medical, nurs-ing, and social work practice and should be writtenfor the practitioners who use them. This suggests that:
s protocols should not employ arcane or legalisticlanguage,
● protocols should be formatted to facilitate locat-ing desired information, and
c protocols should be as brief as possible so thathealth care staff can grasp the totality of their in-tent and implementation (though a longer, com-panion protocol could include rationale and fullerexplanations).
With model protocols, designed to address the di-verse needs of numerous health care facilities, lengthis less important, The expectation is that models willbe shortened in creating individual protocols. Becauseit is assumed that model protocols will be interpretedand adapted by a facility’s “ethics experts,” models mayalso be relatively complex. Still, designers of a modelshould recognize that expertise in medical ethics orlaw may be scarce among those charged with adapt-ing it.
Paradigms of DecisionmakingProtocols
There are three basic types of decisionmaking pro-tocols, distinguished by whether they provide for do-not-resuscitate orders only, care categories based oneither “treatment levels” or “treatment goals,” ordetailed treatment plans. (Examples of each appear inapp. B.)
Do-Not-Resuscitate Protocols
Protocols providing for implementation of do-not-resuscitate orders were the first, and remain the mostprevalent, form of decisionmaking protocol (65, 110,117). Numerous samples have been published. (Exam-ples of DNR protocols include those by: Beth Israel Is-rael Hospital (26); City of Boston (36); Cleveland Clinic(38); Los Angeles County (94); M. Mahowald et al. (97);A. McPhail et al. (100); S.H. Miles et al. (107); NationalInstitutes of Health (120); Northwestern Memorial Hos-pital (123); Somerville Hospital (140); St. Joseph’s Hos-pital, St. Paul, MN (143); St. Joseph’s Hospital, Orange,CA (144); and University of Wisconsin Hospital (155).)
DNR orders provide an exception to a unique stand-ing order to provide cardiopulmonary resuscitation(CPR). The order is directed to on-call staff who, be-cause of the urgency of cardiac arrest, are unable toconsult with the patient or primary physician aboutthe desired course of therapy (170), DNR orders arecommonly written on general medical wards and inintensive care units (ICUs) (51, 90, 153, 166, 172). TheDNR protocol (usually called a “policy”) typically indi-cates the conditions under which DNR orders maybewritten; the roles of the patient, physicians, and otherparties; and how the order is to be documented andcarried out.

35
Protocols concerning CPR, more than any other life-sustaining treatment, became an urgent institutionalneed. The practice of universal standing orders forCPR could not be abandoned in favor of individual CPRorders upon admission because the latter approachwould seriously endanger patients for whom a CPRorder might inadvertently be omitted, either becauseof oversight or failure to anticipate a cardiac arrest.
Experts agree that DNR orders should apply exclu-sively to CPR and should not restrict other life-sustain-ing treatments or lessen measures to prevent cardiacarrest (9, 48, 107, 119, 130, 134, 156, 161). Some clini-cal studies document this intended effect (34, 131, 172);however, other studies show that DNR protocols canlead to limitation of a cluster of life-sustaining treat-ments (22, 51, 90, 104, 138, 151). A DNR protocol in-vites this mistake if it fails to include clear definitionsof the specific procedures that constitute resuscitationand the intent of the order (170).
Experience with DNR protocols has helped to focusdiscussions of protocol design and to identify crucialcontent areas (such as documentation and decision-making principles, for persons with and without deci-sionmaking capacity) that may be applicable to othertypes of decisionmaking protocols as well. In addition,the uniquely auditable written DNR order has per-mitted research about CPR decisions that maybe help-ful in understanding decisionmaking about other life-sustaining treatments (21, 51, 90, 151, 153, 156, 166,172).
DNR protocols address a decision of limited scope,a single element in a treatment plan. As such, DNRprotocols do not fully address the needs of any of thehypothetical patients described in chapter 1: not RobertSwanson, whose DNR request is made in concert withconditional decisions that address other treatments;not Thomas Johnson, who wants CPR now but wantsit withheld if he becomes irreversibly incompetent; andnot Mary Hinkel, who wishes to reject all forms of life-sustaining treatment.
Care-Category Protocols: TreatmentLevels and Treatment Goals
The narrow scope of DNR protocols has engenderedinterest in approaches that address a broader rangeof treatment issues. Care-category protocols are oneresult. This type of protocol is based on the assump-tion that patients can be classified into one of severalcategories that signify a particular treatment plan. Twomajor types of care-category protocols have been pro-posed, one based on categories of treatment levels andthe other on categories of treatment goals.
Treatment-level protocols define clusters of treat-ments, order them hierarchically, and assign each pa-tient to a single category. (Examples have been pub-lished by: F.P. Arena et al. (15); F. Davilla et al. (46);S.A. Levenson et al. (86); Massachusetts General Hos-pital (99); A. Meisel et al. (104); Presbyterian Univer-sity Hospital (128); T.E. Quill et al. (131); L. Volicer (162);and Yale New Haven Hospital (169).) Patients in a givencategory are considered eligible for all treatments inthat category and any lower categories, but ineligiblefor treatments in higher categories. The protocol ofPittsburgh-Presbyterian Hospital (104, see app. B) setsup the following levels of “acceptable orders” to facili-tate communication when detailed orders are notavailable:
1. All But Cardiac Resuscitation (i.e., vigorous treat-ment, including measures to prevent cardiac ar-rest, but no CPR except in special, defined circum-stances);
2. Limited Therapy (i.e., no new therapy except forhygiene and comfort; new drug therapy includedin special circumstances); and
3. Comfort Measures Only (i.e., discontinue all treat-ments not related to comfort and hygiene).
Other protocols differentiate treatment levels by thedecisions on whether to provide CPR, whether to hos-pitalize, or whether to admit to an intensive care unit.
Treatment-goal protocols define categories of treat-ment in terms of goals such as to “palliate withoutprolonging life” or to “preserve comfort, hygiene anddignity, but not to prolong life” (28, 60, 110, 149). Thesecare categories are typically referred to as “Suppor-tive Care,” “Comfort Care,” or “Routine Terminal Care.”Implementation of this type of protocol, most com-monly found in nursing homes, presumes that prolon-gation of life is no longer a treatment goal (112).
Conceptual and operational difficulties attend bothtypes of care-category protocols. First, specification ofthe care categories is very problematic. Althoughhealth professionals might place all antibiotic therapyin a single treatment level, patients might place intra-venous antibiotics in one category and oral antibioticsin another. This problem becomes acute in determin-ing “comparable” treatments that constitute a category.Some protocols would place Robert Swanson, basedon his refusal of CPR, in a care category that precludesother treatments he might elect. In this way, predeter-mined treatment categories may abridge the patient’sability to autonomously define his or her overall treat-ment plan (95, 151).
Similar problems occur with categories of treatmentgoals. Patients like Robert Swanson may reject CPR

36
in order to avoid the burden of that particular treat-ment, not because they reject the goal of prolongedlife (164). In contrast, Mary Hinkel has rejected all treat-ments that might sustain her life. These individualsdo not have the same goal; there maybe no single carecategory that meets both their needs. In addition,treatment-goal categories are too broad to addresssome patient goals, such as to stay at home as longas possible, to see a sister one last time, or to protectlife savings,
Conceptual difficulties with care categories becomepractical concerns when they must be interpreted bystaff who are unfamiliar with particular patients andmust make momentous decisions about their care. Carecategories aggregate urgent, discrete interventionslike CPR with less urgent or more complex interven-tions like the use of antibiotics or transfer from a nurs-ing home to a hospital.
Care categories that limit transfers from chronic toacute care settings or from a general hospital unit toan ICU seem especially arbitrary. Patients maybe moreclosely monitored in an ICU, and treatment moreclosely supervised. Intensity of care is not a clear prin-ciple by which to distinguish acceptable from unac-ceptable therapies. Even patients who have rejectedall life-sustaining treatments, Mary Hinkel for exam-ple, might opt for transfer to an ICU if severe paincould not be controlled elsewhere (95).
Likewise, a “supportive care plan” would be a dan-gerous way for Robert Swanson to avoid CPR and me-chanical ventilation. If he were to develop dysuria andfever during the night, on-call staff implementing thisplan could legitimately withhold antibiotics, a step thatcould lead to Mr. Swanson’s premature death.
Care-category protocols may help patients, families,nurses, and physicians who are grappling with complexquestions about the nature and purpose of medicalcare, by clarifying their thinking or communicationabout medical treatment. They may have a continu-ing role in patient education and counseling. For in-stance, the concept of treatment-goal categories mayhelp Robert Swanson understand whether he meansto reject medical care altogether, or only to avoid theburdens associated with particular treatments. As thepatient comes to understand the options implicit inchoosing among categories, he or she can be offeredthe opportunity to individualize the treatment plan,and the individualized plan can be entered in the med-ical record.
Still, use of care categories for counseling is not asubstitute for individualized treatment planning. Theuse of such categories as orders or as designations in
the medical record or nursing plans could fosterstereotyping and undermine the nuances of autono-mous decisionmaking. This, in turn, could endangerpatients by inviting on-call personnel to implementsweeping life-or-death decisions without consulting theprimary physician,
Treatment-Plan Protocols
Treatment-plan protocols allow for fully individual-ized treatment plans in a manner analogous to tradi-tional medical orders. They attempt to be more compre-hensive than DNR protocols and to avoid the problemsof care categories. Some, like the new policy called“Limiting Life-Sustaining Treatment” from UniversityHospitals of Cleveland (154) (see app. B), offer specificnontreatment choices. The first consideration is DNR,which is specifically defined as a decision to withholdresuscitation (defined to include mechanical ventila-tion, endotracheal incubation, chest compression, andthe administration of emergency medication or fluids)in the event of an arrest.
Once the DNR order is written, nontreatment of life-threatening conditions short of an arrest (but likelyto lead to one) maybe considered. The potential treat-ment limitation and the clinical situation in which itapplies, e.g., “no incubation” in the event of dyspneaor “no defibrillation” for ventricular fibrillation, areclearly spelled out, to avoid the possibility of misin-terpretation. A patient designated DNR but not desig-nated “no defibrillation” would thus be defibrillatein the event of a severe arrhythmia, but would notbe resuscitated in the event of an arrest (171).
Another example of a treatment-plan protocol is themodel developed by the Minnesota Hospital Associa-tion (114). In this, the available treatments are notlisted, but critical terms that must be understood, in-cluding “life-sustaining treatment, ” “DNR,” and “DNI”(do-not-intubate), are clearly defined (see app. B).
Treatment-plan protocols are a quite recent devel-opment; longer experience with them is required be-fore they can be evaluated. These protocols probablypoint to the eventual development of a new sectionin the medical chart, for recording treatment objec-tives, treatment decisions, conditions in which the pa-tient’s wishes change, and designated proxies. Fore-runners of this type of chart section are seen in someunpublished nursing home protocols (although manyof these bear the name of a care-category protocol,i.e., “Supportive Care Plan”),
Treatment plans address the individuality of MaryHinkel’s, Robert Swanson’s, or Thomas Johnson’swishes, but sacrifice the simplicity of DNR or care-

37
category protocols. Critics of treatment-plan protocolssuggest that it is impractical to prospectively considerevery potential life-sustaining treatment. Supportersof these protocols argue that the relative complexityof treatment-plan protocols could be managed withmore intensive staff education—which is required inany event to prevent misinterpretation of DNR or care-category protocols, as has been discussed.
Specific Provisions
A protocol for decisionmaking about life-sustainingtreatments must be designed with full understandingof what the instrument is to accomplish, with respectto both clinical care and other institutional responsi-bilities, and with a realization of the various constraintsthat need to be overcome in order for it to be effective.
Provisions for Meeting InstitutionalResponsibilit ies
Health care institutions are responsible to a diverseset of public interests that pertain to decisions aboutlife-sustaining treatment (see ch. 1). This section ex-amines ways that decisionmaking protocols may ar-ticulate and help in fulfilling these responsibilities.
Assurance of Patient Autonomy.—Protocols oftenexplicitly state the institution’s commitment to the prin-ciple of patient autonomy (60, 68, 104, 114, 132, 152).This commitment requires that protocols provide adecisionmaking process that identifies and honors thecurrent or previously expressed wishes of patients.
An explicit affirmation of the principle of patient au-tonomy can serve several useful purposes. It helps fo-cus the development of the rest of the protocol’s pro-cedures. It may be appealed to as a way to resolvedilemmas not anticipated by other provisions of theprotocol. For example, though a hospital or nursinghome may not have anticipated a request like ThomasJohnson’s for a nonfamily proxy, a formal expressionof commitment to patient autonomy would go a longway toward clarifying duties in this specific case. Anexplicit affirmation of autonomy can also help educatestaff to view treatment decisions as involving morethan clinical indications and professional judgment. Fi-nally, patients, when informed of the institution’s com-mitment to patient autonomy, may feel reassured abouttheir future and may be empowered to speak to staffforthrightly about their treatment preferences.
Surgery raises special considerations that can be ad-dressed in decisionmaking protocols. Typically, sur-gery is performed by someone other than the patient’sprimary physician; it sometimes entails use of inva-
sive life-sustaining technologies, either during or im-mediately after the operation. Some protocols suspendall orders to withhold life-sustaining treatment dur-ing and immediately following surgery. Honoring pa-tient autonomy requires that patients are informed ofthis practice prior to consenting to elective surgery,for example, for a hernia repair (114).
Protection of vulnerable Patients.—Decisionmak -ing protocols can promote this interest with languageaffirming the equal value of the lives of elderly, disa-bled, or indigent persons, and a commitment to non-discrimination against them in the provision of treat-ment (68, 114). An institutional commitment to protectpatients who are vulnerable due to decisional incapac-ity or other causes can also be advanced by proceduralprovisions (5, 43, 46, 87, 124) that include:
1.
2.
3.
4.
5.
6.
7.
requiring or encouraging the use of an ethics com-mittee or prognosis committee, particularly for pa-tients who are decisionally impaired or when theinstitution has a financial or other interest in theoutcome of a treatment decision (44);having surrogates to advocate on behalf of all pa-tients who lack decisionmaking capacity (43, 152);ensuring that staff are aware of State or local lawsregarding decisions for vulnerable persons whohave neither a surrogate nor an advance direc-tive (73);ensuring that staff, families, and patients areaware of decisionmaking principles, procedures,and advocacy resources (68, 146);ensuring that staff and other caregivers are awareof procedures and duties to report any abuse ofvulnerable patients (68);facilitating formation of independent patients’rights committees and/or quality assurance mech-anisms to audit protocols and individual decisionsto limit treatment (68); andproviding for accountability of health care profes-sionals in all aspects of treatment planning andimplementation (discussed later in this app.).
Some commentators have suggested that protocolsthat facilitate the patient’s choice to refuse life-sus-taining treatment by privatizing decisionmaking withinthe health care staff, patient, and family encounter mayendanger vulnerable patients (13, 49, 68, 87). A pri-vate decision based on “substituted judgment” or “bestinterests” by even well intentioned professional care-givers regarding life-sustaining treatment for an in-continent, aphasic, isolated, financially dependent pa-tient like Mae Carver raises troubling issues aboutsocial prejudices, caregiver fatigue or frustration, andpublic resources. (If Mae Carver is under public guard-ianship, the facility may be obliged to follow very spe -

38
cific procedures; if there is no guardian, she may stillbe protected by regulatory or professional standards,such as vulnerable adult protection acts. )
The duty to ensure that vulnerable persons arerespectfully and equitably treated is a serious and dif-ficult challenge. Fundamentally, this responsibility restswith individual staff who are sensitive to the needs,values, and perspectives of vulnerable patients, andwho are aware of the special dangers that arise fromsocial stigmatization and patients’ inability to protecttheir own interests. Such sensitivity will need to beinculcated and cannot be fully protected by proceduralmechanisms.
Promotion of Institutional Mission.–All healthcare institutions are members of a professional tradi-tion that strives to promote beneficence, especiallyhealth, life, restoration of function, and alleviation ofsuffering. Many protocols explicitly state their com-mitment to this moral mission (68, 104, 114). A com-mitment to beneficence underlies the “fail-safe” pro-visions of decisionmaking protocols, like the universalstanding order for CPR. It also guides treatment deci-sions in cases of attempted suicide and in emergen-cies when a patient’s prognosis and preferences areunknown.
Some authorities have proposed that the principleof beneficence be formulated in standards for mini-mal care, consisting of specific treatments (usuallynourishment) that may never be withheld (87, 112).A few nursing home protocols have done so.
Some health care institutions have specific medicalmissions that determine the treatment options that willbe available to patients and that staff will be expectedto carry out. Hospices are one example. In addition,some institutions are associated with sectarian com-munities or organizations that have religiously basedpositions regarding the provision or discontinuationof life-sustaining treatments. A decisionmaking pro-tocol is one mechanism by which to state this mission,for the benefit of both patients and staff.
Accommodation of Staff Objections.—Some pro-tocols affirm respect for the personal moral sentimentsof staff and exempt designated staff from participat-ing in treatment plans to which they object (60, 62,104, 152). For example, the guidelines of Pittsburgh-presbyterian Hospital permit physicians, but not nurses,to excuse themselves from participation in treatmentsto which they have a moral objection (104). This typeof provision goes beyond the section of the Health Pro-grams Extension Act of 1973 (Public Law 93-45) thatprohibits hospitals receiving certain Federal fundsfrom requiring staff with moral objections to par-
ticipate in abortions and sterilizations (42 U.S.C.300a- 7(b,d)).
Such provisions can foster moral deliberation by staffand help maintain staff morale. These provisions neednot be based on an interest in the general “moral in-tegrity of the medical profession, ” an interest that hasnot been found to outweigh a particular patient’spreferences. They might, however, be supported byan affirmation of a mutually voluntary treatment rela-tionship between patients and health care staff (129).Thus, Torah Home may choose to inform residents thatit supports Dr. Levin’s personal right to refuse, onmoral grounds, to participate in certain treatmentplans, even if those plans are not inconsistent withstandards of the institution. Torah Home might prom-ise, in such cases, to try to find another physician whois willing to provide the full range of treatment op-tions implicitly or explicitly promised.
Reconciliation of Conflicting Responsibilities.—The diversity of institutional responsibilities brings thepotential for tension or conflict. This is manifested intwo particularly troublesome ways, both of which bearon protocol design. First, a tension exists between theunencumbered exercise of patient autonomy and theprocedural oversight needed to protect the interestsof vulnerable persons. Procedures to advance the pub-lic interest in the protection of vulnerable persons suchas Mae Carver should not be so complex or costly asto effectively destroy Robert Swanson’s ability to di-rect his care. Thus, it is unreasonable to propose a le-gal requirement that all life-sustaining treatments begiven unless prior court approval to do otherwise hasbeen obtained. However, procedures to permit patientsto decline life-sustaining treatments cannot be so per-functory as to compromise protection for patients whomight be improperly induced to refuse treatment ormisconstrued as having refused life-sustaining treat-ment (87, 95). For example, a nursing home policy thatleaves all orders regarding life-sustaining treatmentsin the hands of the physician would make it easier toact in accordance with Robert Swanson’s clearly statedtreatment preferences. But the same policy may notprovide adequate oversight to protect Mae Carver, whocannot express her treatment preferences.
Second, there is sometimes tension between patientautonomy and institutional mission. A patient beliefscan and often do diverge from customary sectarianpositions or from an institution’s expressed view ofits mission. It is important to note that the diversityof missions reflects the diversity of moral communi-ties in this society. Thus, differences between a patientpreference and Torah Home’s mission do not consti-tute a gratuitous threat to patient autonomy, but rather

39
the meeting of moral differences between a patientand persons who have joined together to providehealth care in a manner consonant with their moralviews. If moral communities are to be able to operateinstitutions that reflect their values, an accommoda-tion on this issue is needed.
Public policy could preemptively solve the difficul-ties raised by contending public and patient interestseither by dispensing with some of them or by arrang-ing them in a rigid hierarchy. One way would be tocompel health care institutions to obey any patient orproxy wish. However, this would undermine the insti-tution’s accountability to other public interests. Thecomplexities and tensions that emerge from institu-tions’ diverse responsibilities indicate the importanceof the competing claims and values to which institu-tions are accountable. In the last analysis, this debatecannot be preempted.
Provisions for Good Decisionmaking
Protocols can include provisions to facilitate a gooddecisionmaking process without proposing rigid al-gorithms that would dictate a particular treatment plan(156). This prudent approach reflects the complexityof decisions about life-sustaining treatments and re-spect for moral pluralism and patient autonomy.
Some protocols contain principles for making deci-sions about life-sustaining treatments but do not sug-gest any procedures for implementation (28, 60, 159,165). Others mandate detailed procedures for imple-menting decisions. While some discussions of gooddecisionmaking allude to professional virtues, such ascompassion, respect for life, and beneficence (159),others emphasize patients’ rights (7, 68, 146).
Assessment of Decisional Capacity. -Decisional ca-pacity is a watershed assessment: Adult patients whoare decisionally capable have the legally protected rightto accept or refuse any medical treatment, whereaspatients who are deemed decisionally incapable or ad-judicated incompetent can participate in treatment de-cisions only through a proxy or an advance directive.A large proportion of patients for whom life-sustainingtreatment is considered are in the latter categories dueto permanent or temporary loss of consciousness, pro-found confusion, or depression (156). Victims of cardiacor respiratory arrest, for example, are typically un-consciousness or in a severely compromised mentalstate. A survey in New York nursing homes found thatalmost half of all elderly residents are disoriented orhave impaired memory (157). (Disorientation or mem-ory impairment was defined in this survey as inabilityto remember dates or time, to identify familiar loca-
tions or people, to recall important aspects of recentevents, or to make straightforward judgments.)
Decisionmaking protocols area vehicle for address-ing the essential concept of decisional capacity, to helpensure that it is clearly understood and accuratelyassessed. The two major definitions are: “competence, ”a global assessment that can be determined only ina legal proceeding, and “decisionmaking capacity, ” atask-specific assessment that is determined without le-gal involvement (13, 130, 156).
Protocols handle this topic in a variety of ways. Somediscuss definitions of decisional capacity (62, 114, 169).Others note the procedural significance of this assess-ment without proposing definitions (100, 115).
Some protocols include precautionary provisions forassessment of decisional capacity. One such safeguardis to state a presumption in favor of the direct partici-pation of all patients in treatment decisions unless abasis for the conclusion of decisional incapacity hasbeen recorded in the medical record. For example, theprotocol of University Hospitals of Cleveland states,“competent patients must be consulted and have a rightto refuse treatment” (154). Some protocols point outthat a patient preference that contradicts medical ad-vice (e.g., Thomas Johnson’s request for CPR shouldit be needed, despite his physician’s contrary view)should never, by itself, be taken as proof of decisionalincapacity.
Few protocols address the issue of who should as-sess decisional capacity; most that do so leave it to theattending physician (60, 104, 130) or a consulting psy-chiatrist.
Patients Who Are Decisionally Capable.—In sup-port of patient autonomy, institutional protocols oftenstate that decisionally capable patients, like RobertSwanson or Thomas Johnson, should be fully informedof treatment options and given an opportunity to ex-press their treatment preferences. Many protocols alsostate that the institution will honor an advance direc-tive of a patient who later loses decisionmaking ca-pacity.
To further patient participation, institutions oftentry to foster communication between their staff andpatients. protocols may advise patient counseling, stat-ing that health care staff are responsible for initiatingdialog about life-sustaining treatments or for creatinga climate in which Robert Swanson or Thomas John-son’s friend would feel comfortable raising treatmentissues (62, 137). Hospital protocols often assign to thephysician the responsibility for initiating this conver-sation (60, 104, 107). Nursing homes are more likely

40
to give more responsibility to nurses or social work-ers in initiating these discussions (112), reflecting theirrole in creating treatment plans for nursing home resi-dents and the more limited presence of physicians (25,130). Some protocols, while presuming that physiciansplay a central role in the treatment decision, encouragenurses to record patients’ preferences in the chart,to inform physicians of these preferences, and thento record that the physician has been so informed (110,134).
Recognizing that many acute life-threatening eventscan be expected to leave their victims, at least tem-porarily, incapable of expressing treatment prefer-ences, newer protocols commonly encourage prospec-tive decisionmaking through advance directives likeliving wills or proxy designations (62, 94, 100, 107, 130,152). Some facilities distribute forms for advance direc-tives upon admission. In some nursing homes and hos-pitals, admitting social workers or nurses are respon-sible for informing persons like Robert Swanson orthe families of patients like Mary Hinkel of the possi-bility of writing an advance directive. This practicehas been criticized by people who believe that initiat-ing discussion of life-sustaining treatments before staff-patient relationships are established may increase pa-tient or family fear and distrust. Fears that the hospi-tal or nursing home is a place to die, that the facilitywould try to save money by limiting treatment, or thatthe patient will be abandoned might lead some patientsor families to initially express treatment preferencesthey later disavow. Advocates of advance directivesview these forms as a way to prevent the unnecessarycircumvention of patient preferences in medical emer-gencies.
Patients Who Are Not Decisionally Capable.–Pub-lished reviews emphasize that medical decisionmak-ing for patients who are not decisionally capable shouldstill respect their autonomy and should honor theirpreviously expressed treatment preferences and values,by seeking a surrogate who has intimate, loving knowl-edge of the patient, and by being mindful of socialprejudices (14, 62, 129, 130, 156). In addition, becausemany patients have medical histories that portend lossof decisional capacity, health professionals and insti-tutions share responsibility for ascertaining treatmentpreferences while this is still possible.
Institutional protocols have addressed the special fea-tures of decisionmaking for decisionally incapable pa-tients in several ways. As with decisions for capablepatients, the decisionmaking process can begin in ad-vance of medical crises, sometimes in advance of in-stitutionalization, so that appropriate parties and prox-ies can be fully empowered and so that important
clinical decisions can be fully considered. To this end,some protocols, especially in nursing homes or in hos-pital units working with persons with dementia, re-quire prospective family conferences with physicians,nurses, and social workers (100, 162). Such conferencescan help ensure that interdisciplinary communicationoccurs. In such meetings, for example, Mary Hinkel’snurses would be able to communicate to her new phy-sician her wish to have only palliative care.
Increasingly, protocols recognize that decisionally im-paired patients may need a proxy decisionmaker (5,62). For patients with caring and involved family mem-bers, many protocols simply accept family membersinto treatment planning. Family members can be in-valuable sources of information about a patient’spreferences, and family acceptance of a treatment planas being in the patient’s best interest or consonant withthe patient wishes is an important safeguard for vul-nerable persons. Family involvement is also evidenceof a prudential approach to decisionmaking. Despitethe value of family in these roles, health care facilitiesshould be mindful of State laws that pertain to familyproxies; family members are not legally empoweredto act as surrogate decisionmakers in all States (14, 136).
In several situations, selection of proxies is of spe-cial concern. Some protocols propose or require le-gally appointed proxies for decisions to forgo certainlife-sustaining treatments, especially when family mem-bers are not available or are in disagreement, or whena treatment decision is not adequately supported bysubstituted judgment (5, 104). Thus, even though itseems clear that Robert Swanson desires to have nolife-sustaining treatments when he loses his ability tointeract, to ensure his preference is interpreted as hewould wish, he should be encouraged to appoint aproxy as a part of creating his treatment plan. ThomasJohnson, like many patients with acquired immuno-deficiency syndrome (147), wishes to designate a non-family proxy even though family members are avail-able. When prospective planning is possible, suchpatients might use a durable power of attorney to ap-point a proxy of their choice and to avoid any defer-ence to family. Even without formal assignment, how-ever, nonfamily proxies may be given great weight ifthey have demonstrated significant, caring knowledgeand regard for the patient’s preferences and interests.For patients like Mae Carver who are without familyor proxies to represent their interests, protocols mightprovide for referral to appropriate Government officeswhen reporting is legally mandated or when the treat-ment decisions are of great consequence (5).
Medical Criteria for Limiting Treatment.—Someprotocols establish medical criteria that must be met

41
before certain treatment decisions are allowed. Forexample, some require that patients be diagnosed as“terminally ill” before withholding of life-sustainingtreatment will be permitted (100, 110, 112, 126, 161).Some suggest conditions, like “serious disability, ” wheretreatment might be limited (112, 149).
The use of medical criteria in protocols for decisionsabout life-sustaining treatments is controversial, in partbecause of conceptual difficulties. ‘(Terminal illness”is not clearly distinguished from chronic, progressivedisease. Treatment “futility” can be defined as eitherthe inability to prolong life or the inability to reversedisability. Moreover, reliable clinical measures of theseconcepts are not available (156).
There are also fears that negative and sometimessubjective assessments like ‘(terminally ill, ” “braindamaged, ” or ‘(severely disabled” may lead health carestaff to withhold life-sustaining treatment unjustlyfrom people described by these terms (67, 68). Fur-thermore, some people believe that using criteria liketerminal illness as a prerequisite for decisions to forgolife-sustaining treatments wrongly restrains patient au-tonomy (126) by discouraging or preventing a personwho is not terminally ill from articulating or effectivelycommunicating treatment preferences.
Despite objections to including medical criteria indecisionmaking protocols, many people argue that de-cisions about life-sustaining treatments are not an is-sue when the treatment in question cannot preventan imminent death (27). Thus, even some protocols thatstrenuously protect the rights of vulnerable patientshave attempted to differentiate patients who are “im-minently dying” from those who are not (68). For apatient like Mary Hinkel, this type of provision maypermit health care staff to suspend customary aggres-sive care in the event of cardiac arrest.
The Role of Ethics Committees.--Ethics committeeshave a role in the creation of protocols, in their imple-mentation through staff education, and in prospectivetreatment conferences. Ethics committees can also as-sist health staff by providing information pertinent tocontroversial procedural questions (such as ThomasJohnson’s nonfamily proxy) or by advising on difficultclinical decisions. Ethics committees provide a forumfor collection and communication of information amongmultiple caregivers and perspectives.
Few institutional protocols require that ethics com-mittees be routinely involved in treatment decisions(11 O). Some protocols propose or require use of suchgroups to address controversial or disputed decisionsor as a safeguard for vulnerable patients (44, 62, 100,104, 121, 132, 169). Some require ethics committees
to review decisions to limit life-sustaining treatmentfor decisionally incapable patients (5, 29).
It is not clear whether health care institutions canlessen their risk of adverse legal action by imposingprocedural consultation requirements, and such re-quirements sometimes create obstacles to decisionallycapable patients who would decline life-sustainingtreatment. Courts have been variously disposed towardthe necessity or authority of ethics committees in de-cisions about life-sustaining treatments (167).
The Role of the Courts.—There is wide agreement,especially among health care providers and lawyers,that the courts should be drawn into decisions aboutlife-sustaining treatments only in exceptional cases (62,121, 156). Court hearings are used routinely to namelegal guardians or surrogate decisionmakers for per-sons who lack decisional capacity, Courts may also becalled upon when there is an irreconcilable contro-versy about proxy selection, about a decision madeby a proxy, or when no proxy is available and life-or-death decisions are being made (5). Some protocolsstate that, as a general principle, judicial interventionor guidance is unnecessary except where all othermeans of dispute resolution have failed (104). Othersspecify the situations in which resort to the courts isappropriate.
Provisions for Implementing Decisions
A major purpose of institutional decisionmaking pro-tocols is to provide for proper implementation of treat-ment decisions once they have been made (62, 81, 130,156). Health care facilities are complex institutions;many persons are involved in creating and carryingout treatment plans. There are many opportunities formiscommunication, disagreement, and errors. often,the staff who carry out a treatment plan are unfamiliarwith the patient or have not been involved in treat-ment decisions. In this environment, the role of pro-tocols in trying to facilitate the proper implementa-tion of treatment decisions is as important as theirfacilitation of good decisionmaking itself.
Protocols can address treatment plan implementa-tion through provisions for:
●
●
●
●
accurate communication of treatment intentions;treatment plans that are “fail-safe)” to preventunintended withholding of life-sustainingtreatment;accountability of individual staff for the implemen-tation of decisions to limit treatment;assistance to health care staff, families, and pa-tients in complex, controversial decisions;

42
● ensuring compliance with the requirements ofagencies external to the health care institution; and
. implementation of the protocol itself.
Accurate Communication.—To facilitate accurateimplementation of decisions about life-sustaining treat-ments, protocols need to provide for unambiguouscommunication of the treatment plan from decision-makers to on-call staff. It maybe inadequate to simplyassert that the physician should convey informationabout the treatment plan to health care staff involvedin the patient’s care (26, 115, 132, 169), especially inlong-term care settings, where physicians frequentlyare not available.
Protocols usually state that treatment intentions,such as Robert Swanson’s DNR request, are to be im-plemented by explicit, permanently recorded medicalorders signed by the physician (62, 78, 130). In addi-tion to orders, many protocols say that the medicalrecord should contain a note by the physician discuss-ing the genesis and intent of the treatment plan (19,26, 104, 114, 132). This note should record the diagno-sis, prognosis, patient or proxy wishes, recommenda-tions of the treatment team, treatment objectives, anda discussion of key treatment decisions. In the caseof decisionally incapable patients, the note should doc-ument the finding of incapacity, record the basis ofthat assessment, the identity of the proxy decision-makers, the rationale for selecting them as proxies,and the proxy’s directive. This more completedocumentation can convey the complexity of RobertSwanson’s or Thomas Johnson’s treatment plan andalso Johnson’s wish to have a nonfamily proxy,
Protocols that apply to patients who are terminallyill, imminently dying, or permanently unconscious re-quire definitions of these terms and documentationthat the criteria are fulfilled (67, 100). Some nursinghome protocols establish separate areas of the medi-cal record for documentation of the assumptions thatare to govern decisions about life-sustaining treat-ments, For outpatients, like Thomas Johnson, the treat-ment plan will be maintained in the physician’s officerecord. Patients and their proxies should be aware ofthe location of this material, to help bring it to the at-tention of hospital staff in a medical emergency. Somehospitals give patients DNR wristbands so that off-wardstaff can be instantly aware of each person’s treatmentintentions (114).
To promote accurate communication, protocols oftendefine important and commonly used terms, like DNR,do-not-intubate, or care categories (19, 108, 115, 130,154). Misinterpretation of terms, as has been discussed,may also be anticipated and addressed.
Accurate and reliable communication of treatmentplans for patients transferred between health care fa-cilities poses especially difficult problems. So that in-terfacility transfers can proceed smoothly, protocolsshould conform to the procedural format used by am-bulance services (108). Most importantly, the possibil-ity of an interfacility transfer should be anticipatedso that patient preferences with regard to such trans-fers or to the treatment provided at the receiving fa-cility can be elicited and incorporated into treatmentplanning (62).
Interfacility protocols need to provide for commonusage of terms, to ensure accurate communication oftreatment intentions (62, 108). This type of protocolalso helps to assure the receiving institution that treat-ment directives have been properly made, since pa-tients often will be unable and proxies unavailable toreconstruct the decisionmaking process. For MaeCarver and Robert Swanson, interfacility communi-cation can occur in the context of an agreement be-tween the emergency medical service and communitynursing homes and hospitals, For outpatients likeThomas Johnson, good communication is needed be-tween individual physicians and community hospitals.The latter is much more difficult and, to date, dependson the initiative of individual physicians, institutions,and patients or their proxies,
Fail-Safe Provisions. -Many decisionmaking pro-tocols contain provisions that intend to ensure that,in the absence of unambiguous and properly formu-lated directives, treatment assumptions will “fail safe”in favor of sustaining life. Standing orders for emer-gency life-sustaining treatment, especially CPR, are acommon fail-safe provision (19, 46, 114). In nursinghomes, another normal provision is a standing orderto call an ambulance service in every medical emer-gency. The rationale for such provisions is that someindividuals who desire a potentially beneficial treat-ment (especially CPR) would otherwise not get it.
Some emergency medical systems that accept DNRorders do not accept vague directives to limit life-sus-taining treatments, e.g., orders for “supportive care.”For patients like Robert Swanson, whose wishes aretied to his ability to interact with others, an order for“no heroic measures” is confusing. If an unclear orderis presented, customary standing orders for CPR areto be followed (108, 140),
Some health care institutions provide for the revo-cation of an order to limit treatment when there isreason to believe it no longer reflects the patient’swishes or interests. This type of provision recognizes

43
the possibility that a patient’s condition or his or heracceptance of it may change.
Many protocols state that a decision about life-sus-taining treatment may be changed at any time. Oneunpublished nursing home protocol allows patients torevoke a DNR order by notifying a nurse, who is em-powered to revoke the DNR order in the name of themedical director. The patient’s attending physician isnotified of this revocation so that further discussionsbetween the patient and physician can occur. Compara-ble provisions in some hospital protocols authorizefamily members to revoke a DNR order with the sameease (100). A Minneapolis area emergency medicalservice policy covering CPR specifies that for homecare patients, like Thomas Johnson, a patient’s destruc-tion of the home care form restores the standing or-der for aggressive treatment.
As a further fail-safe measure, some protocols re-vert to a presumption in favor of treatment unless thetreatment decision is reaffirmed. Thus, some protocolsprovide for automatic expiration of orders to limittreatment after a certain time in order to ensure thatorders undergo continual review by the patient andhis or her physician (26, 46, 114, 140). In nursinghomes, the period of time is usually from 1 to 3 months;in hospitals, it is typically from 1 to 7 days (110, 112).
Some facilities prohibit discharge documents fromcarrying orders to limit medical treatment beyond thetime required to transfer the patient to another healthcare facility (114). The intent is to ensure that a physi-cian is continually responsible for treatment orders.Other protocols provide for continuity by recommend-ing that transferring physicians inform receiving phy-sicians of any decisions about life-sustaining treatments(62). Information about the patient’s history is espe-cially important when the patient has become deci-sionally incapable. New York State’s 1987 legislationallows the receiving physician to accept a DNR desig-nation from a transferring facility, to enter it in thepatient’s record, and to accept responsibility for it (121).
Provisions for Accountability
Accountability to Coworkers.—Professional ac-countability for decisions about life-sustaining treat-ments is addressed by two principal provisions: assign-ment of staff responsibilities for the formulation andimplementation of decisions about life-sustaining treat-ments, and requirements for signed staff documenta-tion during this process.
Protocols define a variety of physician responsibili-ties. The consensus is that physicians should sign all
treatment orders in the medical record (78, 130). Inaddition, many protocols require a signed descriptionof the intent of limited treatment plans. Most teachinghospitals require attending staff physicians to coun-tersign any orders to limit treatment that are writtenby interns or residents. This ensures that senior phy-sicians are aware of and accountable for all such de-cisions.
Some protocols require nurses to record critical pro-cedures for implementing decisions about life-sustain-ing treatments (110, 112). These include any discus-sions between nurses and patients about treatmentdecisions, notification of physicians about such discus-sions, the implications of treatment decisions for nurs-ing care, and the communication to emergency medicalservice personnel of directives to withhold life-sustain-ing treatment. Specification of these duties can be aneffective way to ensure that critical information, likethe conversations between Mary Hinkel and her nurses,are entered into the medical record. Some policies di-rect nurses to challenge resuscitation orders if the pa-tient has not been involved in decisionmaking (110,134).
Some protocols address orders that physicians oc-casionally give to nurses by telephone to withhold life-sustaining treatment. A telephone order may repre-sent an ad hoc decision, rather than a carefully thoughtout plan based on discussion with the patient. Otherprotocols prohibit telephone directives (104). Thosethat do permit telephone orders might require thatnurses record all such telephone conversations, or theymight provide for the automatic expiration of any tele-phone order that the physician does not countersignwithin 24 to 72 hours (111, 112, 123).
Accountability to Patients—The effect of protocolsin promoting optimal communication and understand-ing between health care staff and patients or theirproxies is a matter of considerable dispute. Certainly,the protocol framework emphasizing good decision-making principles, articulating institutional mission,detailing staff responsibilities, establishing reliableinterstaff communication, and providing ongoing staffeducation contributes to a good decisionmaking envi-ronment. Some protocols go farther and promote spe-cific decisionmaking encounters (62).
Some institutions, mainly nursing homes, give allnewly admitted residents or their family members anopportunity for initial discussion of the purposes oflife-sustaining treatments and the possibility of request-ing that their use be limited. New York State’s law re-garding resuscitation requires that physicians discussresuscitation with all decisionally capable patients and

44
enter a DNR order only with the patient’s prior con-sent, unless such discussion would cause “severe andimmediate harm to the patient” (121). Similarly, somehospitals require that, for all patients admitted to anICU, physicians note the objectives of and possiblelimits on the use of life-sustaining treatments.
The use of admission conferences to determine thepatient’s wishes regarding life-sustaining treatmentshas some limitations. First, this could be the first meet-ing of patient and health care staff, and trust may belacking. Second, crucial prognostic information maynot yet be available. Third, it is difficult within the com-pressed time of an admission to inform patients andtheir families fully about the range of choices avail-able. Fourth, patients newly admitted to a health carefacility are usually ill and under considerable stress;their ability to participate in treatment decisions maybe severely compromised.
Despite these reservations, admission or soon there-after can be a good time to raise questions about life-sustaining treatments and to make patients awarethere will be future opportunities to discuss any con-cerns and preferences. Some institutions distribute in-formation packets that include forms for designatingtreatment preferences or surrogate decisionmakers(148), or that introduce care categories as a way toinform patients of the range of treatment options. Someadmission procedures include asking patients to des-ignate a surrogate decisionmaker in the event one willbe needed. The opportunity for knowledgeable coun-seling should be offered whenever such informationis distributed and when such questions are asked. Insome institutions, nurses or social workers coordinateinitial discussions with patients, to prepare them formore detailed discussions with their physicians (112).
Some institutions require all patients for whom life-sustaining treatments are to be limited to sign a livingwill. This provision may be difficult to implement inthat many people are not psychologically able to com-mit themselves in writing to a course of action theyotherwise might affirm. A less rigid variation on thistype of provision is Pittsburgh-Presbyterian Hospital’srequirement that when a signed advance directive isavailable, it must be included in the patient’s chart(104). Another is Yale New Haven Hospital’s policy ask-ing the patient (or surrogate) to sign an authorizationfor a DNR order if there is reason to believe that theorder will be disputed (169).
Compliance With External Agencies—Protocolsmust be consistent with legal requirements regardingliving wills, durable powers of attorney, and other rele-vant matters (e.g., organ donation, brain death) (152).
Many local or State governments have requirementsas to the handling of DNR orders for incompetent pa-tients who are under State guardianship or withoutclose family. Some protocols identify the classes of per-sons to whom such laws apply and refer decisions tothe institution’s lawyer or to the identified governmentbody. Generally, protocols do not list the special re-quirements or restrictions that pertain to orders tolimit treatment for such persons, in order to avoid giv-ing the impression that such restrictions apply to allpersons.
Provisions for Implementingthe Protocol
Implementation of protocols occurs within the muchbroader context of administrative responsibilities formonitoring health care practice and assuring qualitycare. Some protocols include a provision identifyingthe individual office or official with specific responsi-bility for ensuring that the protocol is used routinelyand as intended. For example, the Joint Commissionon the Accreditation of Healthcare Organizations as-signs responsibility for implementation (as well as de-velopment) of DNR policies to the hospital’s chief ex-ecutive officer. The model protocol by the MinnesotaHospital Association provides for similar specificationin stating “Implementation of this policy is the respon-sibility of [officer]” (114).
Beyond this, the protocol may indicate what meanswill be used to ensure implementation by staff. TheMinnesota Hospital Association model indicates thatthe “[named officer] shall establish procedures to fa-miliarize medical staff in its provision and provide forits implementation,” It further specifies that this offi-cer is responsible for “regular review and updatingof the policy,” to ensure it meets current legal, clini-cal, ethical, and procedural needs.
Staff involvement in the process of developing theprotocol helps establish initial familiarity with the pro-tocol as well as commitment to it, but this is not enough.Changes in staff as well as revisions in the protocolnecessitate ongoing efforts to educate staff regardingthe rationale for and specific provisions of the pro-tocol. Without continuing staff education, breakdownsin the implementation of protocols are likely to occur.
In addition, implementation of a decisionmaking pro-tocol assumes that administrators will supply any doc-uments or agents referred to in the protocol. This in-cludes, for example, establishing and supporting ethicscommittees, retaining legal counsel, and making liv-ing will documents available.

Appendix B
Sample Decisionmaking Protocols
Do-Not-Resuscitate Protocol (see pp. 46-50)‘(Guidelines for Orders Not to Resuscitate, ”Beth Israel Hospital, Boston, MA
Care-Category Protocols:Treatment Levels (see pp. 51-62)
‘(Guidelines on Foregoing Life-Sustaining Treatment, ”Presbyterian-University Hospital, Pittsburgh, PA
Treatment Goals (see pp. 63-67)“The Supportive Care Plan—Its Meaning and Application:Recommendations and Guidelines, ” Task Force on Supportive Care, St. Paul, MN
Treatment-Plan Protocol (see pp. 68-72)“Limiting Life-Sustaining Treatment, ”University Hospitals of Cleveland, Cleveland, OH
Model Guidelines (see pp. 73-74)“Medical Management Decisions in Nursing Home Patients,Principles and Policy Recommendations, ”King County Medical Society, WA
45

46

47

48

49

50

51
PRESBYTERIAN-UNIVERSITY HOSPITALGUIDELINES ON FOREGOING LIFE-SUSTAINING TREATMENT
Prepared by: Ethics and Human Rights CommitteeApproved: Executive Committee, May 30, 1985
I . INTRODUCTION

52
l i f e - s u s t a i n i n g t r e a t m e n t . T h u s , t h e G u i d e l i n e s a r ea d o p t e d a n d p r o m u l g a t e d t o d e a l s p e c i f i c a l l y w i t hd e c i s i o n s t o f o r e g o f u t i l e l i f e - s u s t a i n i n g t r e a t m e n t .
3 .
4 .
5 .
6 .
7 .
8 .

53
(c)
(d)

54
(b)
(c)
(d)
(e)

— —
55

58
legal status of any aspect, i n c l u d i n g a l a c k o f c l a r i t y a st o w h o s h o u l d a c t a s t h e p a t i e n t ’ s s u r r o g a t e . The goal ofsuch a consul ta t ion may inc lude: c o r r e c t i n g m i s u n d e r -s t a n d i n g s , h e l p i n g i n t h e a c q u i s i t i o n o f n e e d e di n f o r m a t i o n , a l l o w i n g v e n t i l a t i o n o f e m o t i o n s a n do t h e r w i s e a i d i n g i n t h e r e s o l u t i o n o f d i s p u t e s . In orderf o r p a t i e n t s a n d s u r r o g a t e s e f f e c t i v e l y t o e x e r c i s e t h i sprerogat ive , they must be made aware of the exis tence andpurpose of the Ethics and Human Rights Committee.
1.
2.
(b)
(c)
(d)
(e)
(f)

57

58
v.
1.
2,
3.

59
2.

60
3 .
a.b.c*
d.
e .
(a)
(b)
(c)

—
SUMMARY OF GUIDELINES ON FOREGOING LIFE-SUSTAINING TREATMENT

62

63
THE SUPPORTIVE CARE PLAN—ITS MEANING AND APPLICATION:RECOMMENDATIONS AND GUIDELINES
I. What Is Supportive Care?
A decision to provide supportive careto an individual means a decision toprovide care and treatment to pre-serve comfort, hygiene and dignity,but not to prolong life. Supportivecare is not considered to be part ofthe concept of euthanasia or causingdeath, but rather should be viewed asnot extending life in hopeless situa-tions. See Section II, For Whom Sup-portive Care Might Be Considered.
Once it has been determined thatsupportive care is appropriate, afterutilizing the decision-making proce-dures outlined below, written ordersfor the individual plan of care mustbe established. The primary aims of asupportive care plan should be to pro-mote the dignity of the individual andto minimize pain or discomfort.There should also be active supportfor the psychological, social, emo-tional and spiritual needs of the indi-vidual and family.
An individual supportive care planfor a resident in a long term care fa-cility should include consideration ofthe following guidelines:
A. A specific disease or life-threaten-ing condition which could end lifebut which does not cause pain or dis-comfort normally would not betreated. For example, pneumonia notcausing dyspnea or pleuritic painwould not be treated.
B. Specific medical conditions whichcompromise comfort, hygiene, anddignity would be treated. For exam-ple, oxygen would be provided to al-leviate dyspnea; pneumonia causingpleuritic pain would be treated; aclear airway would be maintained asby suctioning; localized infectionsand fractures would be treated,
C. Specific nursing care for comfort,hygiene, bowel care, skin care, pas-
By The Task Force on Supportive
sive range of motion (PROM) and po-sitioning, and catheter care would begiven.
D. Hospitalization or more extensivemedical intervention would not ordi-narily be indicated. There may be ex-ceptions to this (see above).
E. In most cases, a resident with asupportive care plan would have a donot resuscitate (DNR) order in themedical record. 1
F. Life sustaining nutrition and hydra-[ion needs would ordinarily be met.There is no consensus within the taskforce on the controversial issue ofwhen and under what circumstancesfood and fluids may be withheld. Wedo agree, however, that the existenceof a supportive care plan does not initself predetermine whether artificialmeans of providing fluids and nutri-tion will be continued or discontin-ued. Each individual case must begiven careful and sensitive considera-tion.
G. The resident and family shall haveas much control as possible over thecare and activity level of the resident,
II. For Whom Supportive CareMight be Considered
Residents in long term care facilitieswho fall within the following majorcategories of medical conditions maybe considered potential candidatesfor supportive care plans, when thereexists clear documentation of themedical condition, and a high degreeof certainty of the diagnosis and prog-nosis. Our intent in setting forth thesecategories is to limit rather than ex-pand the numbers of long term careresidents who may be considered forsupportive care plans.
A. Terminally Ill and ImminentlyDying, for example, from cancer orcardiac disease.
B. Severe and Irreversible MentalDisability, where the resident demon-strates a significant inability to com-municate, or to interact meaningfullywith the environment, and an una-wareness of self and/or the environ-ment; for example, those with pre-se-nile and senile dementia (Alz-heimer’s disease) and cerebral vascu-lar disease (strokes).2
C. Severe and !rreversible PhysicalDisability, where there may exist nor-mal mental functioning but, becauseof pain and suffering, or severe motorimpairment, the resident demon-strates a significant inability to inter-act physically in a meaningful waywith the environment; for example,spinal cord injury, head trauma, em-physema, and amyotrophic lateralsclerosis. 3
111. Procedures for Initiation of aSupportive Care Plan
A. When a Supportive Care PlanShould Be Considered. There is noneed for any haste in evaluating a res-ident for initiation of a supportivecare plan. Time should be allowed tocarefully and thoroughly consider allaspects of the resident’s condition.
1) A supportive care plan is gener-ally inadvisable as part of the initialadmission care plan. Before the ap-propriateness of supportive care canbe fully determined, a complete med-ical record, including a full analysis ofrehabilitative potential, should be cre-ated within the long term care settingitself. However, in some cases a sup-portive care plan on admission maybe appropriate depending on the resi-dent’s condition, previous course ofcare, completeness of previous rec-ord, and so forth. The physician andthe facility should be open to full dis-cussion of the issue if it is raised atadmission.
Care, Law, Medicine and Health Care, 97-102, June 1984. Reprinted with permission.

64
2) We recommend that the facilitynot affirmatively suggest the initiationof a supportive care plan. Such a planis a very personal medical, religiousand ethical matter for the resident,family and attending physician. How-ever, we do recommend that the facil-ity staff be open and receptive to dis-cussions of death and the dying pro-cess. The facility staff may serve as avaluable resource to residents andfamilies, but should also act as achampion for any rehabilitative poten-tial that may exist.
3) If a resident is admitted to a fa-cility with physician orders for a sup-portive care plan, we recommend thatthe order not be followed withoutgoing through the decision-makingprocess outlined below, or, at thevery least, without thoroughly assur-ing, and carefully documenting, that adecision-making process raising allrelevant issues had previously beenundertaken. In all cases, the facilityshould clarify the orders received sothat no ambiguity exists about the in-tentions of the physician and the resi-dent.
B. Participants in a Supportive CareDecision.
1 ) Resident: The resident must al-ways be involved to the fullest extentpossible, even if the resident is un-derguardianship. The procedures rec-ommended here are intended to in-volve all interested persons to thefullest extent possible in the final de-cision so that all viewpoints are repre-sented and thoroughly aired, and sothat legal risks are minimized if theresident is unable to make the finaldecision,
Since supportive care may beviewed by some as placing a residentin a life-threatening situation, anysuch plan for an incompetent or ques-tionably competent resident involvesconsiderable exposure to serious le-gal risks. Such a plan may, however,be in the best interests of the residentif all viewpoints, including medical,religious, ethical and personal, as
well as legal, are weighed against oneanother.
There is some question underguardianship law as to whether aguardian of a person has the legal au-thority to consent to a supportive careplan. Therefore, while these guide-lines recommend having a guardianappointed if at all possible, a guardi-an’s consent is not an absolute guar-antee of proper authority to undertakea supportive care plan.
a) Competent Resident: Whenthe resident is clearly competent, theresident has the full authority to makethe decision on a supportive careplan, one way or the other.
b) Questionably Competent Resi-dent: When there are questions aboutthe resident’s competence, but theresident is not under guardianshipand is still able to express his or herwishes, the following principlesshould govern:
(i) If the resident does notwant a supportive care plan, no planshould be initiated.
(ii) If the resident seems towant a supportive care plan, the initia-tion of a guardianship for the residentshould be encouraged so that some-one is legally designated to speak forthe resident.
(iii) If the resident seems towant a supportive care plan and ifguardianship is not a viable alterna-tive, a supportive care plan may prop-erly be initiated after thorough family,physician, staff and Bio-medical Eth-ics Committee involvement, as out-lined below.
c) Incompetent Resident Not Un-der Guardianship: If the resident isclearly incompetent but not underguardianship, and the resident is una-ble to express himself or herself, thefollowing principles should govern:
(i) Without a guardian, no oneis legally authorized to speak for theresident. This situation involves seri-ous risks for the physician, the facilityand the family. However, we all agreethat an incompetent resident shouldnot be deprived of the right to a sup-
portive care plan merely because ofincompetence. Therefore, we recom-mend the initiation of a guardianshipfor the resident, so that someone islegally authorized to speak for theresident.
(ii) If guardianship is not a via-ble alternative, but a supportive careplan seems highly appropriate underall the circumstances, a supportivecare plan can be initiated after thecareful involvement of family, inter-ested parties, staff, physician and Bio-medical Ethics Committee. Be aware,however, that such a situation doespose great risks to all Involved.
(iii) If there is no guardian andno family to involve in the decision-making process, but a supportive careplan seems highly appropriate, a phy-sician and a facility should carefullyconsider whether to initiate a suppor-tive care plan without receiving courtapproval. In this case, the involve-ment of the Bio-medical Ethics Com-mittee is particularly important andstrongly recommended. Facilities andphysicians are cautioned, however,that deciding against a supportivecare plan in highly appropriate cir-cumstances because of potential legalrisks for themselves may in itself vio-late the rights of the resident, bothlegally and ethically’.
d) Incompetent Resident UnderGuardianship:
(i) The consent of both theguardian and the resident should beobtained, if the resident can in anyway express his or her wishes. Thefamily should be involved as outlinedbelow.
(ii) A guardian may wish toseek probate court approval of a sup-portive care plan; however, at thispoint, it is not at all clear how thecourt would view such a request.
2) Family and Interested Persons:a) Whenever possible, unless the
resident is clearly competent and for-bids it, the family should be fully in-volved in t-he decision-making pro-cess. All family members who are in-

65
volved with the resident’s care and ac-tivitles should be included, and allfamily members as close or closer indegree of relationship to the residentas the involved persons should be no-tified of the discussion. Any otherfamily members who may reasonablewish to be included in the decision-making process should also be noti-fied.
b) Other persons or groups in-volved in the resident’s care and/oractivities, or in support of the familyshould also be involved.
c) We recommend that the resi-dent’s attending physician take pri-mary responsibility for the notifica-tion and involvement of family andothers. Each physician and facilitycould, however, develop cooperativeprocedures in this respect.
3) Resident's Attending Physician:a) A supportive care plan should
be initiated by orders of the resident’sattending physician only, never by thefacility medical director unless themedical director is the attending phy-sician.
b) If the resident and family arestrongly in favor of supportive careand the physician is not, they havethe right to consult another physicianwhose philosophy is more akin totheir own. However, the resident andfamily should be strongly encouragedto consider why the physician is op-posed and we encourage the involve-ment of the Biomedical Ethics Com-mittee.
c) If the physician questions afamily's motivation for initiation ofsupportive care plan, or if there is ir-resolvable conflict among familymembers, the matter should be re-ferred to the facility Bio-medical Eth-ics Committee for additional guid-ance.
4) Long Term Care Facility In-volvement :
a) Administrative and Profes-sional Staff:
(i) The Director of Nursing
Services, the Resident Services Direc-tor and the Social Services Director,or their delegates, should be involvedin the discussion. Minimally, the Ad-ministrator should be informed of theexistence of the discussion.
(ii) General supportive carepolicies should be developed, alongwith a basic evaluation sheet, to en-sure that all relevant information isgathered and assessed.
b) Direct Care Givers: Inputshould be solicited from those di-rectly involved in care of the residentas they may notice small details orpatterns of significance in the condi-tion of the resident. Careful noteshould be given to the observationsand opinions of the direct care givers.particularly when they conflict withthe recommendation of the residentor the physician that a supportive careplan is appropriate.
c) Medical Director: The medicaldirector of a long term care facilityshould not direct a supportive careplan unless he or she is also the resi-dent’s attending physician.
We recommend involvement of themedical director in each supportivecare decision-making process, but donot see this as an absolute require-ment. He or she should at least beinformed of the existence and prog-ress of the consideration, and shouldbe available for counsel or conflictresolution, if necessary.
The medical director should partici-pate in the development of, and ulti-mately approve, all general supportivecare policies developed by the facil-it}’.
d) Biomedical Ethics Commit-tee: We encourage consideration ofeach potential supportive care plan byan inter-disciplinary Bio-medical Eth-ics Committee. In most facilities, thebeginnings of such a committee mayalready exist (e.g., Utilization Re-view),
Even when it is quite certain that acompetent resident may authorize asupportive care plan for himself orherself, we nevertheless would en-
courage committee review. In casesof questionably competent or incom-petent residents, we feel it very im-portant to have the committee’s moreobjective involvement.
While the use of a facility’s Utiliza-tion Review Committee as a Bio-med-ical Ethics Committee may be reason-able for the present, we would rec-ommend future development of anexpanded committee to include lay,religious, medical, legal and otherprofessional representation.
C. Supportive Care Decision MakingProcess
1 ) The decision. making processshould be designed to encourage fulldiscussion of all relevant facts and op-tions so that the meaning and signifi-cance of supportive care is fullyunderstood by all participants, and toensure that all views are expressedand weighed, and so that full docu-mentation of the plan will be possi-ble. The following steps are recom-mended:
a) The issue is raised by the resi-dent, family or physician.
b) The attending physician andfacility should obtain complete medi-cal and psycho-social informationfrom the resident’s records, at boththe hospital and the long-term carefacility. Observations and other com-ments which may not be completelyreflected in the medical recordsshould be solicited from direct caregivers.
c) The physician and/or facilitystaff should privately discuss the po-tential supportive care plan and thesignificance with the resident, if at allpossible, so that an assessment can bemade in the absence of any pressureby family members.
d) The physician should partici-pate in a full discussion with familymembers and/or other interested andinvolved persons, with the consent ofthe resident if competent. Other fam-ily members should be notified of thediscussions by the physician.

66
e) The resident’s physician andfacility staff should discuss the issuethoroughly among themselves. Thefacility should assure itself that fulldiscussion between the physician andthe resident and family has takenplace.
f) All issues should be raised anddiscussed with facility staff in a careconference format.
g) The proposed plan should beconsidered by the Bio-medical EthicsCommittee, particularly if the plan isfor an incompetent or questionablycompetent resident.
2) GeneralAdmonitions:a) Document all conferences
carefully and thoroughly.b) Do not force a final decision
too soon after ail discussions havetaken place. Let all involved haverime to mull matters over.
3) Conflict Resolution Principles:a) If the resident can express
himself or herself and does not wanta supportive care plan, it should notbe initiated, or, if initiated by the phy-sician, it should not be carried out bythe facility.
b) If the resident and family wanta supportive care plan and the resi-dent’s physician will not initiate one,the resident and family have the rightto consult another physician. In suchcases, however, the facility should en-sure that the initial physician’s con-cerns and viewpoints are fully consid-ered.
c) If the resident is unable to ex-press himself or herself and familyseems to be pressing for a plan, thephysician and facility should carefullyweigh all factors before initiating andcarrying out the plan to ensure its ap-propriateness. The physician and fa-cility should carefully consider thefamily’s intentions and motivationsand should refer the case to the Bio-medical Ethics Committee before ini-tiating the plan.
d) If there is an intra-family dis-pute over the appropriateness of a
plan, we recommend careful consid-eration by the physician and facility asthis poses a great risk of legal chal-lenge. We also recommend utilizationof the Bio-medical Ethics Committeeor other facility or community re-sources to resolve the conflict prior toinitiating the plan.
e) If the facility staff, medical di-rector or Bio-medical Ethics Commit-tee do not concur with the resident,family or physician on the appropri-ateness of a plan (for example, if thefacility feels significant rehabilitationpotential exists), the facility shouldforcefully express such opinion to theresident, family and physician to en-sure that its objections are heard andunderstood. The facility may chooseto refuse to implement the plan andrecommend discharge, or may evenconsider resort to the courts.
D. Documentation of a SupportiveCare Plan.
1) Physician authorization for a sup-portive care plan should be a specific,individualized set of orders, statingexplicitly what will and will not bedone for the resident. It must be partof the medical record. An order say-ing just “Supportive Care” (unlike“DNR”) is not sufficient.
2) Written authorization for theplan should be obtained from the res-ident whenever possible, even if un-der guardianship. The guardianshould also authorize the plan.
3) Written acknowledgment of theplan should be obtained from thoseinterested persons who have been in-volved in the decision-making pro-cess whenever possible.
4) The specific plan and the facilitypolicies on supportive care should begiven to the resident and family sothat no ambiguity exists.
5) The decision, the nature of theplan, and other relevant mattersshould be thoroughly discussed withall staff involved with the resident.
E. Re-Evacuation of a SupportiveCare Plan.
1 ) The plan must be t-e-evaluatedwhenever the facts or conditionswhich led to the initial plan change,or whenever the resident, family orother involved person requests it. Thesame persons should be involved inre-evaluation as were included in theinitial decision.
2) The supportive care plan shouldbe reviewed periodically, when thegeneral plan of care is reviewed. Werecommend review on a 30-day basis,in any event.
3) We recommend that criteria andan input sheet be developed for re-evaluation, to ensure that direct caregivers are given guidance on whatchanges in conditions to look for.
IV. Conclusion
The task force does not view theserecommendations and guidelines asthe definitive resolution of the dilem-mas raised by the supportive careconcept, but rather as part of an ongo-ing dialogue on supportive care is-sues and practices. Comments arewelcome and may be directed to indi-vidual members of the task force.
The recommendations and guide-lines set forth in this report representthe views of the signatories as individ-uals. They do not necessarily reflectthe policy of any institution, profes-sional organization or governmentalagency with which the signatory is af-filiated.
References1. See Minnesota Medical Association,
DNR Guidelines (adopted by the Board ofTrustees of the Minnesota Medical Associa-tion) (January 1981).
2. The life of a physically or mentallydisabled person is just as valuable as thatof a person described as normal orhealthy. It is not appropriate to consider asupportive care plan on the basis of aphysical or mental disability alone.
3. Id.

67
Task Force on Supportive Care
Barbara J. Blumer, J.D. Iris C. Freeman Pamela J. ParkerBroeker, Hartfeldt, Hedges & Director Former Long Term Care Ombuds-
Grant Nursing Home Residents’ Advo- manBloomington, Minnesota cates Minnesota Board on Aging
Minneapolis, Minnesota St. Paul, MinnesotaM. Chervenak, J.D.Legal Aid Sociecy of Minneapolis Paul Goldstein Arnold RosenthalMinneapolis, Minnesota Assistant Director of Social Serv- Director, Office of Health Facility
ices ComplaintsRonald E. Cranford, M.D. Hennepin County Medical Center Minnesota Department of HealthAssociate Physician in Neurology Minneapolis, Minnesota St. Paul, MinnesotaHennepin County Medical CenterMinneapolis, Minnesota F. Allen Hester, J.D. Lisa Laffoley Schmidt, J.D.
Adjunct Professor of Law Minnesota Legal Services CoalitionJulie L. Ditzler, R. N., B.S.N. William Mitchell College of Law Minneapolis, MinnesotaResident Services Director St. Paul, MinnesotaCedar Pines Health Care Facility Jim VarpnessMinneapolis, Minnesota Grace Nelson Long Term Care Ombudsman
Long Term Care Committee Minnesota Board on AgingJenean Erickson, R. N., FACNHA Minnesota Senior Federation St. Paul, Minnesota
Administrator Minneapolis, MinnesotaYorkshire,ManorMinneapolis, Minnesota
Affiliations are provided only to aid in the identification of the signatories. Theviews expressed are not necessarily chose of the organizations.

..
68
ADMINISTRATIVE POLICYand
PROCEDURE MANUAL II
LIMITING LIFE-SUSTAININGTREATMENT
Policy:
A. Statement of Purpose
It is the policy of University Hospitals of Cleveland to providehigh qual i ty medica l care to i t ’ s pa t ients wi th the objec t ive ofsaving and sus ta in ing l i fe . However, this commitment involvesrecognition that initiation or continuation of t reatment may notconstitute optimum care when the burdens of such treatmentoutweigh its benefits to the patient. At these times, theobjective is to allow as peaceful a death as possible.
B. Guidel ines and Pr inc ip les
When such treatment limitation is considered, the followingguidelines and principles should apply:
1.
2.
3.
4.
5.
6.
7.
8.
9.
Competent patients must be consulted and have a right torefuse treatment.
The wishes of incompetent adults and legal minors should begiven consideration.
Plans to limit treatment must be discussed with the familyunless the patient requests otherwise.
Consultation with other health professionals involved withthe care of the patient is strongly recommended.
Members of the health care team, particularly physicians andnurses, have the responsibility to provide an appropriatelevel of assistance to patients in reaching decisions abouttheir care. Such efforts should be carefully coordinated.
Maintaining the dignity and comfort of the patient willreceive the highest priority.
Limitation of life-sustaining treatment in no way impliesabandonment.
There is no morally relevant distinction between withholdingand withdrawing a life-sustaining treatment when its burdensoutweigh its benefits to the patient.
If treatment limitation is not documented in the patient’s

—
69

—
70
1.
2.
3.
4.
5.

71
1.
2.
3.
4.

72
I I

73
MEDICAL MANAGEMENT DECISIONS IN NURSING HOME PATIENTSPRINCIPLES AND POLICY RECOMMENDATIONS
A Model Developed by the King County Medical Society
Principle Practice
Patients have “autonomy,” the right tochoose health care options, includingthose at the end of life.
Patients should be provided with adequateinformation to make informed choices re-garding health care options.
Unpleasant information should not be with-held from patients simply because it isunpleasant.
Although the patient’s desires are primary,the physician is not required to followthem if they violate professional ethicsor judgment, or if they violate the physi-cian’s moral or religious beliefs.
When patients and physicians irrevocablydisagree on treatment options, patientsmay obtain another physician and physi-cians may withdraw from the patient’scare.
The preeminence of the patient’s choicedoes not preclude physicians from shar-ing with the patient a personal judgmentabout treatment options.
Advance care directives in the form of “in-struction” (living wills) or “proxy” (dura-ble power of attorney) carry moral author-ity and are helpful guides to caregiversshould patients become unable to com-municate their treatment preferences.
Patients lacking full decisionmaking capac-ity should be consulted to the degreefeasible.
When the patient is not capable of choos-ing a course of action and does not havean advance directive, the physician shouldseek to discover the patient’s preferences.
When a patient’s desires cannot be discov-ered, a substituted judgment or determi-nation of best interest should be made.
Physicians have the responsibility to elicit patient preferences abouttreatment decisions, including life-sustaining treatment.
Comprehensible information pertaining to rationale, benefits, risks,and alternatives should be provided to allow patient to make in-formed choices.
The provision of information, even if unpleasant, allows the patientto make informed choices. Information regarding poor prognosismay also allow the patient to attend to personal matters at theend of life. Such information can be communicated in a humaneand compassionate manner.
As examples, assisting patients with suicide or treating them withunapproved drugs violates the physician’s ethic. Some treatmentsin terminally ill patients maybe medically futile. Limitation of life-sustaining treatment, such as cardiopulmonary resuscitation, mayviolate the physician’s moral or religious beliefs.
Either the patient or the physician may terminate the patient-physician relationship. The physician is responsible for the patient’scare until another physician has assumed the patient’s care,
The physician may share his judgment with the patient, but alterna-tives should also be made apparent. Statements such as “You haveno choice” and “You must . . .“ are inappropriate.
Physicians and other caregivers should make advance directives avail-able to nursing home patients early in their institutionalizationwhen they are maximally competent to make choices. Advancedirectives are legal, under specific circumstances, in most states.Although living wills refer only to “terminal” conditions they maybe legally enforceable for other conditions.
Although a patient’s memory may be impaired, he or she may un-derstand the ramifications of certain decisions. In these situations,patients’ preferences deserve preeminence.
Often patients have previously declared to family, friends or care-givers how they would choose to care for themselves at the endof their lives. If the patient is no longer competent, his or her pre-vious desires should be respected if they can be discovered.
Some patients who are incapable of decisionmaking have never beencapable (such as the congenitally mentally retarded) or were capa-ble at one time but never made their wishes known. For thesepersons family (especially spouses) or, if available, existing legalguardians are preferred surrogates. They should provide substi-
Reproduced, with permission, from R.F Uhlmann, H. Clark, R.A. Pearlman, et al.,“Medical Management Decisions in Nursing Home Patients:Principles and Policy Recommendations,” Annals of Internal Medicine, 106: 879-885, 1987.

74
Principle Practice
In the absence of these preferred decision-making surrogates, a surrogate must,nevertheless, be sought to represent thepatient.
When decisions to limit treatment arebaeed on substituted judgments or deter-minations of best interest, consensusamong involved parties is preferable.
When in doubt about the appropriatecourse of action, the physician shouldpresume in favor of life.
The physician’s desire to sustain the pa-tient’s life can conflict with two venera-ble values in medicine, the relief of suffer-ing and the avoidance of harm.
For patients who are in a chronic vegeta-tive state, it is morally justifiable to limitlife-sustaining treatment, allowing the pa-tient to die.
No-code status never means withdrawingpersonal attention from the patient orlimiting attention to the relief of suf-fering.
Resuscitation status of nursing home pa-tients should be determined prospectively,defined in terms of specific interventions,and communicated to caregivers.
As the patient’s advocate it is inappropri-ate for the physician to deny treatmenton the basis of cost or social allocationpriorities.
tuted judgment, that is, seek to choose as the patient would havechosen. If the surrogate is uncertain as to what the patient’s prefer-ence would have been, they should act according to their inter-pretation of what would have been in the patient’s best interest.
Several options for alternative surrogate decisionmaking exist. Theseoptions include but are not limited to legal guardians, ethics com-mittees, and physicians. Although physicians may have a long-standing relationship with the patient, they may also be heavilyinvested in the patient’s medical outcome. From this perspective,guardians and ethics committees may provide a more balancedperspective for the patient and are preferable surrogates. The phy-sician, however, may function as surrogate if designated by thepatient,
Irrevocable differences may be resolved by third parties, such asinstitutional ethics committees or the courts.
If patients’ desires are not known or their prognosis is unclear, thephysician should act to support life.
When further intervention has only the prospect of prolonging thedying process, it may be preferable to limit life-sustaining treat-ment if this enhances patient comfort.
Nutrition and hydration provided by vein or gastric tube and treat-ment for life-threatening intercurrent illness may be withheld fromsuch patients.
Continuation of care and support must be explicitly expressed tothe patient and other caregivers and documented in the medicalrecord. Orders may direct action for the relief of pain, thirst, dysp-nea, anxiety, and other discomforts and may take priority overcorrecting physiologic conditions in the dying patient. In addition,vigorous treatment of potentially reversible superimposed condi-tions may be appropriate.
patients’ resuscitation preferences can usually be determined on ad-mission and made readily identifiable in the medical record. Deci-sionmaking at the time of cardiac arrest is a suboptimal standardof care.
Withholding costly or scarce medical resources should be based onexplicit normative standards such as laws, regulations, or institu-tional policies and not on physicians’ personal values.

. —
Appendix C
List of Reviewers
OTA acknowledges and wishes to thank the following individuals for their comments on drafts of this report.
Faye AbdullahDeputy Surgeon GeneralU.S. Public Health ServiceWashington, DC
Robert A. ArnoldDivision of General Internal MedicineUniversity of PittsburghPittsburgh, PA
Elena CohenSociety for the Right to DieNew York, NY
Timothy M. CookPublic Interest Law Center of PhiladelphiaPhiladelphia, PA
Edward R. GrantHinshaw, Coulbertson, Moelmann, Hoban & FullerChicago, IL
Brian HinesExecutive DirectorOregon Health DecisionsPortland, OR
George A. KanotiDirectorDept. of BioethicsThe Cleveland Clinic FoundationCleveland, OH
Shelah LeaderPublic Policy InstituteAmerican Association of Retired PersonsWashington, DC
John LombardMorgan, Lewis, and BockiusPhiladelphia, PA
Joanne LynnAssociate ProfessorGeorge Washington UniversityWashington, DC
Tracy E. MillerExecutive DirectorNew York State Task Force on Life and the LawNew York, NY
Michael NevinsRiver Vale, NJ
Susan NobelSociety for the Right to DieNew York, NY

Appendix D
Glossary of Acronyms and Terms
AHAAMAANACHA
CPRDHHSDNRDODEMsHCFA
Acronyms
—American Hospital Association—American Medical Association—American Nurses’ AssociationCatholic Health Association of
States-cardiopulmonary resuscitation
the United
—Department of Health and Human Services-do-not-resuscitate (order)—Department of Defense-emergency medical service—Health Care Financing Organization
JCAHO—Joint Commission on-the-Accreditation ofHealthcare Organizations (formerly the JointCommission on the Accreditation of Hospitals)
OTA Officeof Technology Assessment (U.S. Congress)PHS —Public Health ServiceVA —Veterans’ Administration
Terms
Health Care Institution (or Facility): Health care in-stitution refers to any hospital, nursing home, emer-gency medical service, hospice, or home care pro-gram that is engaged in direct patient care.
Life-Sustaining Treatment: Life-sustaining treatmentsare drugs, medical devices, or procedures that cankeep alive a patient who would otherwise die within
a foreseeable, though usually uncertain, time. Exam-ples include cardiopulmonary resuscitation, mechan-ical ventilation, renal dialysis, nutritional support(i.e., tube or intravenous feeding), and antibioticsto fight life-threatening infections.
Protocol: Protocol refers collectively to decisionmak-ing guidelines, policies, and models, defined asfollows:Guidelnes: Guidelines are advisory documents. This
report considers guidelines that are intended toassist health care providers by suggesting morallyand legally acceptable approaches to the diffi-cult questions related to the provision, withhold-ing, or withdrawing of life-sustaining treatment.
Policy: A policy is an instrument of health care fa-cility governance that is designed to ensure thatessential administrative objectives are met. Pol-icies can state fundamental principles for con-duct, provide for orderly, accountable interac-tions between practitioners within an institution,and ensure that social expectations or legal require-ments for health care are met. The hallmarksof policies are their prescriptive language, theirprecise assignment of responsibility for decisions,and their detailing of procedures to be followedin implementing decisions.
Model: A model protocol is an advisory documentintended to assist health care institutions in de-veloping their own policies or guidelines.
78

Appendix E
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
American College of Emergency Physicians, “Med-ical, Moral, Legal, and Ethical Aspects of Resusci-tation for the Patient Who Will Have Minimal Abil-ity to Function or Ultimately Survive, ” Annals ofEmergency Medicine 14:919-926, 1985.American College of Emergency Physicians, Boardof Directors, “Directors Consider Council Reso-lutions,” ACEP News, Oct. 4, 1986.American College of Emergency Physicians, Boardof Directors, ‘(Policy Statements)” ACEP News, Jan.2, 1987.American Health Care Association, “AHCA PolicyPaper: Patients’ Rights,” American Health CareAssociation Journal 7(5):55-60, 1981,American Health Care Association, “QuestionablyCompetent Long-Term Care Residents: Problemsand Possible Solutions)” Washington, DC, 1982.American Health Care Association, “Views of theAmerican Health Care Association: Health CareDecisionmaking in Long-Term Care Facilities)”Washington, DC, 1982.American Hospital Association, “Statement on aPatient’s Bill of Right)” Hospitals 47(4):41, 1973.American Hospital Association, Policy and State-ment: The Patient Choice of Treatment Options,Catalogue No. 157628 (Chicago, IL: 1984).American Hospital Association, Values in Conflict:Resolving Ethical Issues in Hospital Care (Chicago,IL: 1985).American Medical Association, Council on Ethi-cal and Judicial Affairs, Current Opinions of theCouncil on Ethical and Judicial Affairs of theAmerican Medical Association-1986 (Chicago, IL:1986).American Medical Association, Council on Ethi-cal and Judicial Affairs, “Report on Do Not Resus-citate Orders, ” presented by John H. Burkhart,chairman, to the AMA House of Delegates, De-cember 1987.American Nurses’ Association, Committee onEthics, “Guidelines for Nurse Participation andLeadership in Institutional Ethical Review Proc-esses,” Kansas City, MO, 1984.
13. Annas, G.J., and Glantz, L. H., “The Right of ElderlyPatients to Refuse Life-Sustaining Treatment, ’’Mil-bank Quarterly 64(Suppl. 2):95-162, 1986.
14. Areen, J., “The Legal Status of Consent ObtainedFrom Families of Adult Patients to Withhold orWithdraw Treatment, ” Journal of the AmericanMedical Association 258:229-235, 1987.
15. Arena, F. P., Perlin, M., and Turnbull, A. D., “Ini-
16.
17
18.
19.
20.
21.
22.
23.
24.
25.
26.
27
28
tial Experience with a ‘Code-No Code’ Resuscita-tion System in Cancer Patients, ” Critical CareMedicine 8:733-735, 1980.Arnold, R. M., School of Medicine, University ofPennsylvania, Philadelphia, PA, personal commu-nication, Oct. 22, 1987.Bader, D., Senior Associate for Clinical Ethics,Catholic Health Association of the United States,St. Louis, MO, personal communication, Jan. 6,1988.Ball, J. R., “Withholding Treatment: A Legal Per-spective)” Journal of the American Geriatrics So-ciety 32:528-530, 1984.Bar Association of San Francisco and the San Fran-cisco Medical Society, “Policy Statement on OrdersAgainst Resuscitation)” Deciding to Forego Life-Sustaining Treatment, President’s Commission forthe Study of Ethical Problems in Medicine and Bio-medical and Behavioral Research (Washington,DC: U.S. Government Printing Office, 1983).Bardsley & Haslacher, Inc., “Awareness and Inci-dence of Having a ‘Living Will’ in Oregon, ” un-published report prepared for Oregon Health De-cisions, September 1986.Bedell, S. E., and Delbanco, T. L., Choices AboutCardiopulmonary Resuscitation in the Hospital,”New England Journal of Medicine 31O:1089-1093,1984.Bedell, S. E., Pelle, D., Maher, P.l., et al., “Do-Not-Resuscitate Orders for Critically III Patients in theHospital: How Are They Used and What Is TheirImpact?” Journal of the American Medical Asso-ciation 256:233-237, 1986.Berger, S., Consultant, National Citizens' Coalitionfor Nursing Home Reform, Washington) D.C. per-sonal communication, Mar. 15, 1988.Bertolet, M. M., and Goldsmith, L.S. (eds.), Hospi-tal Liability: Law and Tactics, 4th ed. (New York,NY: Practicing Law Institute, 1980).Besdine, R. W., “Decisions to Withhold Treatrnentfrom Nursing Home Residents, ” Journal of theAmerican Geriatrics Society 31:602-606, 1983.Beth Israel Hospital (Boston, MA), “Guidelines:orders Not to Resuscitate,” Life-Sustaining Tech-nologies and the Elderly, U.S. Congress, Office ofTechnology Assessment, OTA-BA-306 (Washing-ton, DC: U.S. Government Printing Office, July1987).Blackhall, L. J., “Must We Always Use CPR?” NewEngland Journal of Medicine 317:1281-1285, 1987.Braithwaite, S., and Thomasma, DC., “New (;uide-
77

78
lines on Forgoing Life-Sustaining Treatment in In-competent Patients: An Anti-Cruelty Policy,” An-nals of Internal Medicine 104:711-715, 1986.
29. Brown, B. A., Miles, S. H., and Aroskar, M.A., “ThePrevalence and Design of Ethics Committees inNursing Homes,” Journal of the American Geri-atrics Society 35:1028-1033, 1987.
30. Brown, N. K., and Thompson, D.J., “Non-Treat-ment of Fever in ExtendedCare Facilities,” IVewEngland Journal of Mech”cine 300:1246-1250, 1979.
31. California Hospital Association, “DNR Studies inCalifornia,” California Hospital Association Inter-nal Document, 1987.
32. California Nurses’ Association, Ethics Committee,“Statement on the Nurse’s Role in Withholding andWithdrawing Life-Sustaining Treatment,” adoptedMay 17, 1987.
33. Cassel, C. K., Chair, Section of General InternalMedicine, University of Chicago, Chicago, IL, per-sonal communication, Oct. 15, 1987.
34. Charlson, M.E., Sax, F.L., MacKenzie, C. R., et al.,“Resuscitation: How Do We Decide? A Prospec-tive Study of Physicians’ Preferences and the Clin-ical Course of Hospitalized Patients,” Journal ofthe American Medical Association 255:1316-1322,1986.
35. Chernus, S., ‘(Institutional Protocols on Decisionsto Forgo Life-Sustaining Treatment: An Evidence/Negligence Perspective,” unpublished paper, Uni-versity of Pittsburgh Law School, March 1, 1988.
36. City of Boston Department of Health and Hospi-tals, “Guidelines: Do Not Resuscitate Orders,”Deciding to Forego Life-Sustaim”ng Treatment,President’s Commission for the Study of EthicalProblems in Medicine and Biomedical and Be-havioral Research (Washington, DC: U.S. Govern-ment Printing Office, 1983).
37. Cleveland Clinic Foundation, “A Statement of Pol-icy on Care of the Hopelessly Ill,” Cleveland, OH,Jan. 1, 1988.
38. Cleveland Clinic Foundation, “A Statement of Pol-icy on Do Not Resuscitate,” Cleveland, OH, Jan.1, 1988.
39, Cohen, E., Staff Attorney, Society for the Rightto Die, New York, NY, personal communication,Apr. 19, 1988.
40. Conservatorsh”p of Drabick, No. HO02349 (Cal. Ct.App. 6th Dist. Apr. 13, 1988).
41. Cook, T. M., Public Interest Law Center of Phila-delphia, Philadelphia, PA, personal communica-tion, Feb. 26, 1988.
42. Corbett v. D’Alessandro, 487 So. 2d 368 (Fla. Dist.Ct. App.), review dem”ed, 492 So. 2d 1331 (Fla.1986).
43. Cournos, F., ‘(orders Not to Resuscitate and thePsychiatric Hospital)” Psychiatry Quarterly 58(l):24-31, 1986.
44. Cranford, R. E., and Doudera, A.E. (eds.), Institu-tional Ethics Committees and Health Care Deci-sionmaking (Ann Arbor, MI: AUPHA Press, 1984),
45. Darling v. Charleston Community Memorial Hos-pital, 33 Ill. 2d 326, 211 N.E. 2d 253 (1965), cert.denied, 386 U.S. 946 (1966).
46. Davila, F., Boisaubin, E. V., and Sears, D. A., “Pa-tient Care Categories: An Approach to Do-Not-Resuscitate Decisions in a Public Teaching Hospi-tal)” Critical Care Medicine 14:1066-1067, 1986.
47. Deputy Attorney General for Medicaid Fraud Con-trol, Supreme Court of the State of New York,Queens County, Criminal Term, Grand Jury Re-port, Report of the special January third additional1983 Grand Jury Concerning “Do-Not-Resuscitate”Procedures at a Certain Hospital in Queens County,1983.
48. Donnelly, W .J., “DNR: The Case for Early Retire-ment,” Archives of Internal Medicine 147:37-38,1987.
49. Dornette, W.H.C., “The Legal Impact on Volun-tary Standards in Civil Actions Against the HealthCare Provider,” New York Law School, Law Re-view 22:925, 1977.
50. Duff, R. S., “Guidelines for Deciding the Care ofCritically Ill or Dying Patients,’’Pedjatrics 64(1):17-23, 1979.
51. Evans, A. L., and Brody, B. A., “The Do-Not-Resus-citate Order in Teaching Hospitals,” .lourna] of theAmerican Medical Association 253:2236-2239,1985.
52. Florida Nurses Association, “Clients’ Rights Re-garding Administration of Artificial Sustenance,”adopted by House of Delegates, November 1987.
53. Fogel, B., Forrow, L., and Arnold, R. M., “The De-cision to Limit Life Support—A Medical Proce-dure,” in press.
54. Frampton, M.W., and Mayewski, R.J., “Physicians’and Nurses’ Attitudes Toward Withholding Treat-ment in a Community Hospital,” Journal of Gen-era] Internal Medicine 2:394-399, 1987.
55. Fried, C., “Terminating Life Support: Out of theCloset,” New England Journal of Medicine 295:390-391, 1976.
56. Glasser, G., Zweibel, N. R., and Cassel, C. K., “TheEthics Committee in the Nursing Home; Resultsof a National Survey, ” Journal of the AmericanGeriatrics Society 36:150-156, 1988.
57. Gordon, M., “Problems and Challenges in For-mulating and Implementing Do Not ResuscitatePolicies for an Institutionalized Elderly Popula-

79
58
59
tion,” presentation at Annual Meeting of theGerontological Society of America, Washington,DC, NOV. 20, 1987.Grand Jury of the Supreme Court of the State ofNew York, Queens County, ‘(DNR Procedures: Pur-ple Dots Revisited,” Connecticut Medicine 49:367-376, 1985.Greenlaw, J., “Orders Not To Resuscitate: Dilemmafor Acute Care As Well As Long-Term Care Facil-ities,”La w, Medicine and Health Care 10:29-31,45,1982.
60. Halligan, M., and Hamel, R. P., “Ethics CommitteeDevelops Supportive Care Guidelines,” HealthProgress 66(10):26-30,60, 1985.
61. Harris, S., General Counsel, American Health CareAssociation, Washington, DC, personal commu-nication, Oct. 15, 1987.
62. Hastings Center, Guidelines on the Terminationof Life-Sustaining Trea tment and the Care of theDying (Briarcliff Manor, NY: 1987).
63. Haynes, B. E., and Niemann, J. T., ‘(Letting Go: DNRorders in Pre-Hospital Care, ’’Journal of the Amer-ican MedicaJ Association 254:532-533, 1985.
64. Hilfiker, D., “Allowing the Debilitated to Die: Fac-ing Our Ethical Choices, ” IVew England Journalof Medicine 308:716-719, 1983.
65,
66.
67,
68.
69.
70.
71.72.
73.74.75.
76,
Hospital Council of Southern California, “Life-Support Survey)” Filing Code GI-171, June 26,1984.Hoyt, J., Chairperson, Nursing Home Action Group,Minneapolis, MN, personal communication, Feb.22, 1988.Hoyt, J. D., and Davies, J. M., “A Response to theTask Force on Supportive Care, ” Law, Medicineand Health Care 12:103-105, 1984.Hoyt, J. D., and Davies, J. M., ‘(Meeting the Needfor Clear Guidelines: Protecting Vulnerable Adultsfrom Improper Limitation of Medical Treatmentin Institutions, ” La w and Inequality: A Journal ofTheory and Practice 4:355-378, 1986.In re Conroy, 98 N.J. 321, 486 A.2d 1209 (N.J.1985).In re Estate of Prange, No. 86-3398 (Ill. Ct. App.4th Div. Feb. 11, 1988) (Jiganti, J.).In re Gardner, 534 A.2d 947 (Me. 1987).In re Jobes, 210 N.J. Super. 543,510 A.2d 133 (su-per. Ct. Ch. Div.), review denied (N.J. Mar. 10,1986).In re Jobes, 108 N.J. 394, 529 A.2d 434 (1987).In re Peter, 108 N.J. 365, 529 A.2d 419 (1987).Zn re Quinlan, 70 N.3. 10, 355 A.2d 64?, cert. de-nied, 429 U.S. 922 (1976).h re Rodas, No. 86 PR139 (Colo. Dist. Ct. MesaCountv Jan. 22, 1987) (Buss, J.)
77.
78
79
80
81
82.
83.
84
85
86.
87.
88.
89
90
914
92.
Johnson, S,, “State Regulation of Long-Term Care:A Decade of Experience with Intermediate Sanc-tions,’’Law, Med”cine and Health Care 13:173-188,1985.Joint Commission on Accreditation of Hospitals,“New and Revised Standards Approved: Withhold-ing Resuscitative Services,” JCAH Perspectives7(5/6):5, 1987.Jest, T. S., “Enforcement of Quality Nursing HomeCare in the Legal System,” Law, Medicine andHealth Care 13:160-172, 1985.Kanoti, G., Director, Bioethics Department, Cleve-land Clinic Foundation, Cleveland, OH, personalcommunications, Oct. 16, 1987, and Feb. 17, 1988.Kapp, M., Preventing Malpractice in Long-TermCare: Strategies forllisk Management (New York,NY: Springer Publishing Co., 1987).Kapp, M. B., Professor, Wright State UniversitySchool of Medicine, Dayton, OH, personal com-munication, January 1988.Kapp, M. B., and Lo, B., “Legal Perceptions andMedical Decision Making,” Mi~bank Quarterly64(Su@. 2):163-202, 1986.Kass, L. R., Toward a More Natural Science: Biol-o~ and Human Affairs (New York, NY: The FreePress, 1985).Katz, J., The Silent World of Doctor and Patient(New York, NY: The Free Press, 1984).King County Medical Society, Ad Hoc Committeeon Nursing Home Care, “Principles for Determin-ing Code Status of Patients in Nursing Homes, ”King County Medical Society Bulletin 64:13-16,1985.Koop, C.E., and Grant, E. R., “The Small Beginningsof Euthanasia: Examining the Erosion in Legal Pro-hibition Against Mercy Killing,” Notre Dame Jour-nal of Law, Ethics, Public Policy 2:585-634, 1986.Levenson, S.A., List, N. D., and Zaw-Win, B., ‘(Ethi-cal Considerations in Critical and Terminal Illnessin the Elderly,” Journal of the American Geriat-rics Society 19:563-567, 1981,Levinson, W., Shepard, M. A., Dunn, P. M., et al.,“Cardiopulmonary Resuscitation in Long-termCare Facilities: A Survey of Do-Not-ResuscitateOrders in Nursing Homes,” Journal of the Amer-ican Geriatrics Society 35:1059-1062, 1987.Lipton, H. L., “Do-Not-Resuscitate Decisions in aCommunity Hospital: Incidence, Implications, Out-comes, ” Journal of the American Medical Asso-ciation 256:1164-1169, 1986.Lo, B., and Steinbrook, R. L., “Deciding Whetherto Resuscitate,” Archives of Internal Medicine143:1561-1563, 1983.Lombard, J.J., Jr., Morgan, Lewis& Bockius, Phil-.

80——
adelphia, PA, personal communication, February1988.
93. Longo, D. R., Warren, M., Roberts, J. S., et al., “Ex-tent of ‘Do Not Resuscitate’ Policies Varies AcrossHealthcare Settings, ” Health Progress 69:66-73,June 1988.
94. Los Angeles County Department of Health Serv-ices’ Hospitals, “Guidelines for ‘No-Code’ Orders, ”Deciding to Jqorego Life-Sustaining Treatment,President’s Commission for the Study of EthicalProblems in Medicine and Biomedical and Be-havioral Research (Washington, DC: U.S. Govern-ment Printing Office, 1983).
95. Lynn, J., “Dying and Dementia, ” JOurna] of theAmerican Medical Association 256:2244-2245,1986.
96. Lynn, J., “Much Accomplished But Much To BeDone,” New Jersey Law .lournal 120:24, July 16,1987.
97. Mahowald, M., Schubert, D., and Gordon, I. B.,“How One Hospital Resolved the DNR Question.Cardiopulmonary Resuscitation Guidelines atCleveland Metropolitan General and HighlandView Hospitals,” Ohio State Medical Journal 82:382-385, 1986,
98. Marshall, L., “Resuscitating the Terminally Ill,”Journal of Enlergency Medical Services 10:24-28,1985.
99. Massachusetts General Hospital, Critical CareCommittee, “Optimum Care for Hopelessly Ill Pa-tients)” New England Journal of Mech”cine 295:362-364, 1976.
100. McPhail, A., Moore, S., O’Connor, J., et al., “One
101
Hospital’s Experience with a ‘Do-Not-Resuscitate’Policy,” Canada Medical Association Journal 125:835-837, 1981.Medical Association of the State of Alabama, “DoNot Resuscitate (DNR) Guidelines,” Deciding toForego Life-Sustaining Treatment, President’sCommission for the Study of Ethical Problems inMedicine and Biomedical and Behavioral Reseaich(Washington, DC: IJ.S. Government Printing Of-fice, 1983).
102. Medical Society of the State of New York, “Guide-lines for Hospitals and Physicians on ‘Do-Not-Re-suscitate’,” Deciding to Forego Life-Sustaim”ngTreatment, President’s Commission for the Studyof Ethical Problems in Medicine and Biomedicaland Behavioral Research (Washington, DC: U.S.Government Printing Office, 1983).
103. Meisel, A., Professor of Law and Psychiatry, Uni-versity of Pittsburgil, Pittsburgh, PA, personalcommunications, Oct. 15, 1987, January 1988, andMarch 1988.
104. Meisel, A., Grenvik, A., Pinkus, R. L., et al., “Hos-pital Guidelines for Deciding About Life-SustainingTreatment: Dealing with Health ‘Limbo’,” CriticalCare Medicine 14:239-246, 1986.
105. Miles, S. H., Assistant Professor of Medicine,University of Chicago, Chicago, IL, personal com-munication, December 1987.
106. Miles, S. H., “Advance Directives to Limit Treat-ment: The Need for Portability)” Journal of theAmerican Geriatrics Society 35:74-76, 1987.
107. Miles, S. H., Cranford, R., and Schultz, A. L., “TheDo-Not-Resuscitate Order in a Teaching Hospital:Considerations and a Suggested Policy,” Anna/sof Internal Medicine 96:660-664, 1982.
108. Miles, S. H., and Crimmins, T.J., “Orders to LimitEmergency Treatment for an Ambulance Serv-ice in a Large Metropolitan Area,” Journal of theAmerican Medical Association 254:525-527, 1985.
109. Miles, S. H., and Gomez, C,, Health Faci]ity PoZiciesfor Elti”ve Use of Life4Wstaini”ng Treatment mewYork, NY: Springer, in press).
110. Miles, S. H., and Moldow, D.G., “Hospital Policies
111
on Limiting Medical Treatment, ” Archives of In-ternal Medicine 144:1841-1843, 1984.Miles, S. H., and Moldow, D.G., ‘(Commentary onthe Minnesota Medical Association’s Do-Not-Re-suscitate Guidelines, ’’iMinnesota Medicine 68:603-605, 1985.
112. Miles, S. H., and Ryden, M. B., “Limited-TreatmentPolicies in Long-Term Care Facilities,” Journal ofthe American Geriatrics Society 33:707-711, 1985.
113. Miller, T.E., Executive Director, New York StateTask Force on Life and the Law, New York, NY,personal communication, Feb. 24, 1988.
114. Minnesota Hospital Association and Biomedical
115
Ethics Commit~ee of Fairview Riverside Hospital,“Limited Treatment Policies and Guidelines: AModel for Hospitals and Nursing Homes,” Min-neapolis, MN, 1986.Minnesota Medical Association, “Do-Not-Resus-citate (DNR) Guidelines, ’’Deciding to Forego Life-Sustaining Treatment, President’s Commission forthe Study of Ethical Problems in Medicine and Bio-medical and Behavioral Research (Washington,DC: U.S. Government Printing Office, 1983).
116. Minnesota Medical Association Trustees, “Controlof Pre-Hospital Care at the Scene of Emergencies)”Minnesota Medicine 69:86-88, 1986.
117. Mozdzierz, G.J., and Schlesinger, S. E., “Do-Not-Resuscitate Policies in Midwestern Hospitals: AFive-State Survey,” Health Services Research 20:949-960, 1986.
118. National Academy of Sciences-National ResearchCouncil, Ad Hoc Committee on Cardiopulmonary

81
Resuscitation of the Division of Medical Sciences,“Cardiopulmonary Resuscitation,” Journal of theAmerican Medical Association 198:372-379, 1966.
119. National Conference on Cardiopulmonary Resus-citation and Emergency Cardiac Care, “Standardsand Guidelines for Cardiopulmonary Resuscita-tion (CPR) and Emergency Cardiac Care (ECC),”Journal of the American Medical Association 255:2905-2989, 1986.
120. National Institutes of Health, The Clinical Center,“Medical Administrative Policy No. 82-4, Subject:orders Not to Attempt Cardiac Resuscitation Pol-icy and Communications Bulletin, Medical Admin-istrative Series (July 12, 1982), ’’Deciding to ForegoLife-Sustaining Treatment, President’s Commis-sion for the Study of Ethical Problems in Medi-cine and Biomedical and Behavioral Research(Washington, DC: U.S. Government Printing Of-fice, 1983).
121. New York State Task Force on Life and the Law,Do Not Resuscitate Orders: The Proposed Legis-lation and Report of the New York State TaskForce on Life and the Law (Albany, NY: 1986).
122. New York State Task Force on Life and the Law,Life -Sustaim”ng Treatment: Making Decisions andAppointing a Health Care Agent (Albany, NY:1987).
123. Northwestern Memorial Hospital, “Guidelines ForDo-Not-Resuscitate Orders,” Legal and EthicalAspects of Treating Critically and Terrninah’y 111Patients, A.E. Doudera and J.D. Peters (eds.) (AnnArbor, MI: AUPHA Press, 1982).
124. Paris, J.J., “Personal Autonomy Over InstitutionalConsiderations,” New Jersey Law Journal 120:23-24, 1987.
125. Pellegrino, E.D., and Thomasma, D.C., A Philo-sophical Basis of Medical Practice (New York, NY:oxford University Press, 1981).
126. Perkins, H. S., “Ethics at the End of Life,” Journalof General Internal Medicine 1:170-176, 1986.
127. Peters, J., and Peraino, J., “Malpractice in Hospi-tals: Ten Theories for Direct Liability,” Law, Medi-cine and Health Care 12:254-259, 1984.
128. Presbyterian University Hospital, Executive Com-mittee, “Guidelines for the Care of Hopeless/Mori-bund Patients,” Medical Ethics and Legal Liabili-ty, Cyril Wecht (chairman), Litigation CourseHandbook Series No. 85 (New York, NY: Practic-ing Law Institute, 1976).
129. President’s Commission for the Study of EthicalProblems in Medicine and Biomedical and Be-havioral Research, Making Health Care Decisions(Washington, DC: U.S. Government Printing Of-fice, 1982).
130. President’s Commission for the Study of EthicalProblems in Medicine and Biomedical and Be-havioral Research, Deciding to Forego Life-Sus-taim”ng Treatment (Washington, DC: U.S. Govern-ment Printing Office, 1983).
131. Quill, T.E., Stankaitis, J.A., and Krause, C.R., ‘TheEffect of a Community Hospital Resuscitation Pol-icy on Elderly Patients,” New York State Journa/of Medicine 86:622-625, 1986.
132. Rabkin, M.T., Gillerman, G., and Rice, N. R., “OrdersNot To Resuscitate,” New England Journal ofMedicine 295:364-366, 1976.
133. Rasinski-Gregory, D., Associate Chief~f-Staff forEducation, Veterans’ Administration Medical Cen-ter, Long Beach, CA, personal communications,October 1987 and February 1988.
134. Read, W .A., “Hospital’s Role in Resuscitation De-cisions,” Hospital Research and Education Trust,Chicago, IL, 1983.
135. Rosner, F., “Hospital Medical Ethics Committees:A Review of Their Development,” Journal of theAmerican Medical Association 253:2693-2697,1985.
136. Rouse, F., and Cohen, E., Letter to the Editor, Jour-nai of the American M&”cal Association 258:2696-2697, 1987.
137. Schneiderman, L.J., and Arras, J.D., “CounselingPatients to Counsel Physicians on Future Care inthe Event of Patient Incompetence,” Annals of In-ternaf Medicine 102:693-698, 1985.
138. Schwartz, D. A., and Reilly, P., “The Choice NotTo Be Resuscitated, ’’Journal of the American Ger-iatrics Society 34:807-811, 1986.
139. Siegler, M., “Searching for Moral Certainty inMedicine: A Proposal for a New Model of theDoctor-Patient Encounter,” Bulletin of the NewYork Academy of Medicine 57: 56-59, 1982.
140, Somerville Hospital, Somerville, MA, “Guidelines:Orders Not-to-Resuscitate,” Deciding to ForegoLife-Sustaining Treatment, President’s Commis=sion for the Study of Ethical Problems in Medi-cine and Biomedical and Behavioral Research(Washington, DC: U.S. Government Printing Of-fice, 1983).
141. Spencer, S.S., “ ‘Code’ or ‘No Code’: A NonlegalOpinion,” New England Journal of Medicine 300:138-140, 1979.
142. Spudis, E.V., Lambeth, W.A., and Simmons, P.,“Determination of ‘Code Status’ in North Carolina:Still a Delicate Process,” North Carolina MedicalJournal 44:785-788, 1983.
143. St. Joseph’s Hospital, St. Paul, MN, “Guidelines forDo-Not-Resuscitate Orders,” Legal and EthicalAspects of Treating Critically and Terminally Ill

82
Patients, A.E. Doudera and J.D. Peters (eds.) (AnnArbor, MI: AUPHA Press, 1982).
144. St. Joseph’s Hospital, Orange, CA, “Principles andGuidelines for the Treatment of a Patient forWhom a No-Code Order Has Been Written,” Le-galand Ethical Aspects of Treating Critically andTermindy W Patients, A.E. Doudera and J.D.peters (eds.) (Ann Arbor, MI: AUpHA presst 1982).
145. State of California, Health and Welfare Agency,Department of Health Services, “Guidelines Re-garding Withdrawal or Withholding of Life-Sus-taining Procedure(s) in Long-Term Care Facilities,”Sacramento, CA, Aug. 7, 1987.
146. State of Minnesota, “Patients’ and Residents’ Billof Rights,” 1986.
147. Steinbrook, R., Lo, B., Moulton, J., et al., “Prefer-ences of Homosexual Men with AIDS for Life-Sus-taining Treatment,” New England Journal of Medi-cine 314:457-460, 1986.
148. Stephens, R.L., “ ‘Do Not Resuscitate’ Orders: En-suring the Patient’s Participation,” Journa/ of theAmerican MedicalAssociation 255:240-241, 1986.
149. Task Force on Supportive Care, “The SupportiveCare Plan—Its Meaning and Application: Recom-mendations and Guidelines,” Law, Medicine andHealth Care 12:97-102, 1984.
150. Thomasma, D.C., “Hospital Ethics Committees andHospital Pohq,’’@~’tyRetiew B~efi (July):204-209, 1985.
151. Uhlmann, R.F., Cassel, C. K., and McDonald, W .J.,“Some Treatment-Withholding Implications of No-Code Orders in an Academic Hospital,” CriticalCare Medicine 12:879-881, 1984.
152. Uhlmann, R.F., Clark, H., Pearlman, R.A., et al.,“Medical Management Decisions in Nursing HomePatients: Principles and Policy Recommendations,”Annals of Interna] Medicine 106:879-885, 1987.
153. Uhlmann, R.F., McDonald, W.J., and Inui, T. S.,“Epidemiology of NoGde Orders in an AcademicHospital,” Western Journal of Medicine 140:114-116, 1984.
154. University Hospitals of Cleveland, “Limiting Life-Sustaining Treatment,” Cleveland, OH, 1987.
155. University of Wisconsin Hospital and Clinics,“Guidelines Regarding Decisions to Give, Withholdor Terminate Care,” Deciding to Forego Life-Sus -- l%afment, President’s Commission for theStudy of Ethical Problems in Medicine and Bio-medical and Behavioral Research (Washington,DC: U.S. Government Printing Office, 1983).
156. U.S. Congress, Office of Technology Assessment,~“fe-Sustaim”ng Technologies and the Elderly,OTA-BA-306 (Washington, DC: U.S. GovernmentPrinting Office, 1987).
157. U.S. Department of Health and Human Services,.
158,
159<
160.
National Center for Health Statistics, Division ofHealth Care Statistics, “Use of Nursing Homes bythe Elderly: Preliminary Data from the 1985 Na-tional Nursing Home Survey,” Advancedata No.135, by Esther Hing, May 14, 1987.U.S. Department of Health and Human Services,National Center for Health Statistics, Division ofHealth Care Statistics, “Nursing and Related CareHomes as Reported from the 1986 Inventory ofLong-Term Care Places,” Advancedata No. 147,by Al Sirrocco, Jan. 22, 1988.Van Eys, J., Bowen, J. M., Alt, J., et al. (M.D. An-derson Hospital and Tumor Institute), “Creatinga Code of Ethics: Report of the University of TexasSystem Cancer Center,” Cancer 36:115-119, 1986.V“an Scoy-Mosher, M., “An Oncologist’s Case forNo-Code Orders,” Legal and Ethical Aspects ofTreating Critically and Terminally Lll Patients, A.E.Doudera and J.D. Peters (eds.) (Ann Arbor, MI:AUPHA Press, 1982).
161. Veterans’ Administration, “Guidelines for Do-Not-Resuscitate Protocols Within the VA,” Circular 10-83-140, Aug. 25, 1983.
162. Volicer, L., “Need for Hospice Approach to Treat-ment of Patients with Advanced Progressive De-mentia, ” Journal of the American Geriatrics Soci-ety 34:655-658, 1986.
163. Volicer, L., Rheaume, Y., Brown, J., et al., “HospiceApproach to the Treatment of Patients with Ad-vanced Dementia of the Alzheimer Type,” Jour-nal of the American Medica!Association 256:2210-2213, 1986.
164. Wagner, A., “Care?.#monary Resuscitation inthe Aged: A Prospective Study,” New EnglandJournal of Medicine 310:1129-1130, 1984.
165. Wanzer, S.H., Adelstein, S.J., Cranford, R. E., etal., “The Physician’s Responsibility to HopelesslyIll Patients,” New England Journal of Medicine310:955-959, 1984.
166. Witte, K. L., ‘(Variables Present in Patients WhoAre Either Resuscitated or Not Resuscitated in aMedical Intensive Care Unit,” Heart and Lung13(2):159-163, 1984.
167. Wolf, S.M., “Ethics Committees in the Courts,”Hastings Center Report 16(3):12-15, 1986.
168. Wolff, M. L., Smo]en, S., and Ferrara, L., “Treat-ment Decisions in a Skilled Nursing Facility: Dis-cordance with Nurses Preferences, ’’Journal of theAmerican Geriatrics Society 33:440-444, 1985.
169. Yale New Haven Hospital, Committee on Policyfor DNR Decisions, “Report on Do-Not-ResuscitateDecisions,” Connecticut Medicine 47:477-483,1983.

——
170. Youngner, S.J., “Do-Not-Resuscitate Orders: NoLonger Secret, But Still a Problem,” Hastings Cen-ter Report 17(1):24-33, 1987.
171. Youngner, S.J., Department of Psychiatry andMedicine, University Hospitals, Cleveland, OH,persona] communication, March 1988.
172. Youngner, S.J., Lewandowski, W., McClish, D. K.,et al., “Do-Not-Resuscitate Orders: Incidence and
Implications in a Medical Intensive Care Unit,”Journal of the American Medical Association253:54-57, 1985.
173. Zimmerman, J.E., Knaus, W.A., Sharpe, SM., etal., ‘The Use and Implications of Do Not Resusci-tate Orders in Intensive Care Units,” Journal ofthe American Medical Association 255:351-356,1986.

.— .
List of Related OTA Reports
● Life-Sustaining Technologies and the Elderly.This assessment focuses on five life-sustaining technologies: cardiopulmonary resuscitation, mechanical venti-lation, renal dialysis, nutritional support, and life-sustaining antibiotic therapy. It describes the use of thesetechnologies for life-threatened elderly patients, presents data on use and cost in different settings, and dis-cusses aspects of treatment and outcomes that distinguish elderly patients from younger ones. Ethical andlegal questions, particularly those related to patients’ rights and surrogate decisionmaking are reviewed. Alsoaddressed are manpower and training issues and likely future developments in life-sustaining technologies.472 p.OTA-BA-306, July 1987, GPO stock #052-003-01074-7. NTIS order #PB 87-222 527/AS.
(Contractor Docments/Working Papers, available from NTIS)
● Summary: Life-Sustaining Technologies and the Elderly.OTA-BA-307, July 1987, GPO stock #052-003-01078-0.
NOTE: Reports are available through the U.S. Government Printing Office, Superintendent of Documents, Washington, DC 20401-9325, (202)783-3238; and the National Technical Information Service, 5285 Port Royal Road, Springfield, VA 22161-0001, (703) 487-4650.
4