Embed Size (px)
Citation preview
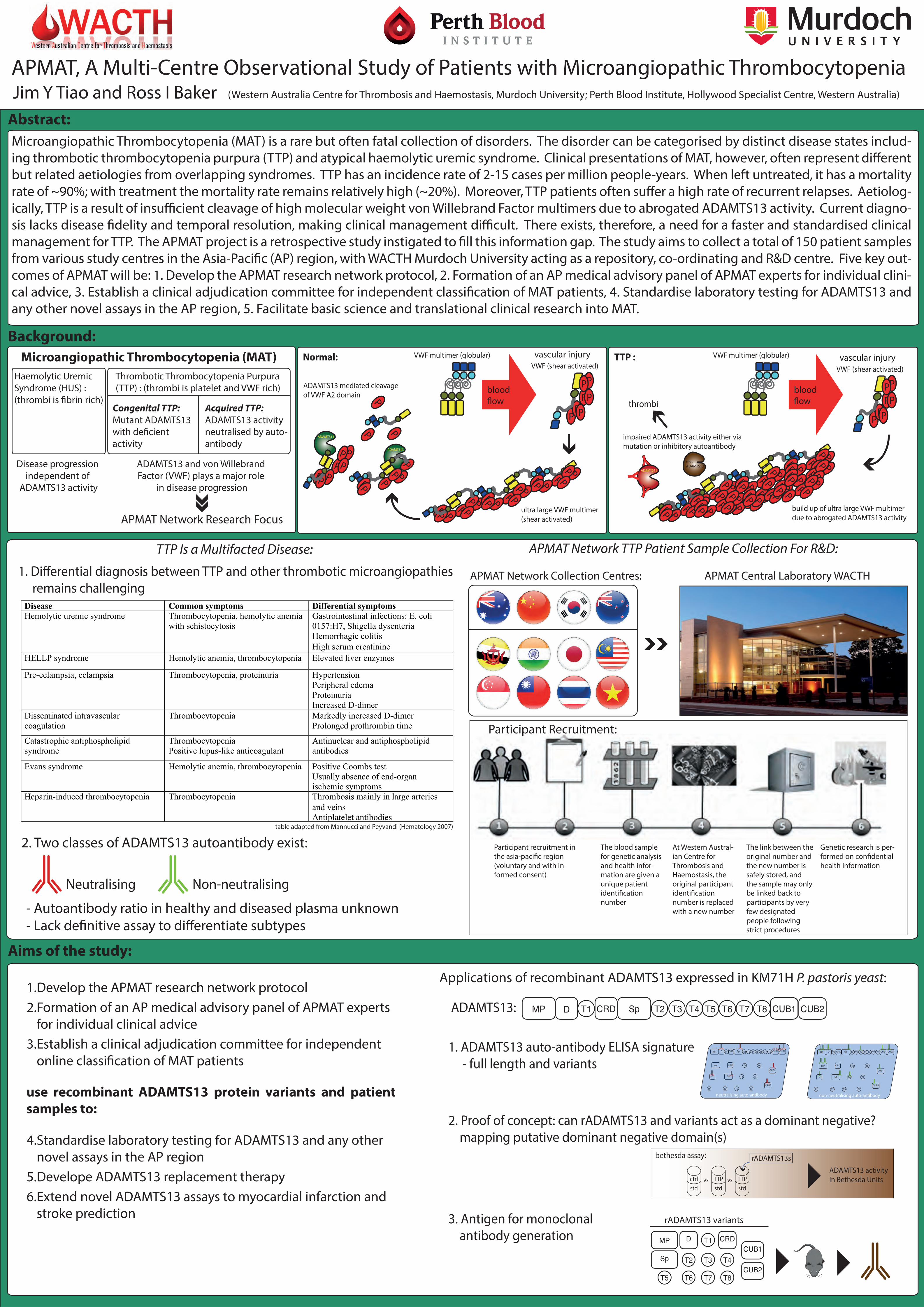
Microangiopathic Thrombocytopenia (MAT) is a rare but often fatal collection of disorders. The disorder can be categorised by distinct disease states includ-ing thrombotic thrombocytopenia purpura (TTP) and atypical haemolytic uremic syndrome. Clinical presentations of MAT, however, often represent di�erent but related aetiologies from overlapping syndromes. TTP has an incidence rate of 2-15 cases per million people-years. When left untreated, it has a mortality rate of ~90%; with treatment the mortality rate remains relatively high (~20%). Moreover, TTP patients often su�er a high rate of recurrent relapses. Aetiolog-ically, TTP is a result of insu�cient cleavage of high molecular weight von Willebrand Factor multimers due to abrogated ADAMTS13 activity. Current diagno-sis lacks disease �delity and temporal resolution, making clinical management di�cult. There exists, therefore, a need for a faster and standardised clinical management for TTP. The APMAT project is a retrospective study instigated to �ll this information gap. The study aims to collect a total of 150 patient samples from various study centres in the Asia-Paci�c (AP) region, with WACTH Murdoch University acting as a repository, co-ordinating and R&D centre. Five key out-comes of APMAT will be: 1. Develop the APMAT research network protocol, 2. Formation of an AP medical advisory panel of APMAT experts for individual clini-cal advice, 3. Establish a clinical adjudication committee for independent classi�cation of MAT patients, 4. Standardise laboratory testing for ADAMTS13 and any other novel assays in the AP region, 5. Facilitate basic science and translational clinical research into MAT.
APMAT, A Multi-Centre Observational Study of Patients with Microangiopathic ThrombocytopeniaJim Y Tiao and Ross I Baker
Background: Microangiopathic Thrombocytopenia (MAT)
Disease progression independent of
ADAMTS13 activity
Haemolytic Uremic Syndrome (HUS) : (thrombi is �brin rich)
APMAT Network Research Focus
ADAMTS13 and von Willebrand Factor (VWF) plays a major role
in disease progression
Acquired TTP:ADAMTS13 activity neutralised by auto-antibody
Congenital TTP: Mutant ADAMTS13 with de�cient activity
Thrombotic Thrombocytopenia Purpura (TTP) : (thrombi is platelet and VWF rich)
VWF multimer (globular)
VWF (shear activated)
PP
P
PPP
P
build up of ultra large VWF multimerdue to abrogated ADAMTS13 activity
mutADAMTS13
impaired ADAMTS13 activity either via mutation or inhibitory autoantibody
TTP :
Y
ADAMTS13Y
Y
P P
PPPPP
P P
PPPPP
P P
PPPPP
P P
PPPPP
P P
PPPPP
P P
PPPPP
P P
PPPPP
P P
PPPPP
P P
PPPP
thrombi
blood�ow
vascular injury
Participant recruitment in the asia-paci�c region (voluntary and with in-formed consent)
The blood sample for genetic analysis and health infor-mation are given a unique patient identi�cation number
At Western Austral-ian Centre for Thrombosis and Haemostasis, the original participant identi�cation number is replaced with a new number
The link between the original number and the new number is safely stored, and the sample may only be linked back to participants by very few designated people following strict procedures
Genetic research is per-formed on con�dential health information
Participant Recruitment:
APMAT Network Collection Centres: APMAT Central Laboratory WACTH
APMAT Network TTP Patient Sample Collection For R&D:
T6 CUB2CUB1T8T7T5T4T3T2SpCRDT1DMP
Applications of recombinant ADAMTS13 expressed in KM71H P. pastoris yeast:
ADAMTS13:
1. ADAMTS13 auto-antibody ELISA signature - full length and variants T6
CUB2
CUB1
T8
T7
T5
T4
T3
T2
Sp
CRD
T1
D
MP
T6 CUB2CUB1T8T7T5T4T3T2SpCRDT1DMP
non-neutralising auto-antibody
T6
CUB2
CUB1
T8
T7
T5
T4
T3
T2
Sp
CRD
T1
D
MP
T6 CUB2CUB1T8T7T5T4T3T2SpCRDT1DMP
neutralising auto-antibody
2. Proof of concept: can rADAMTS13 and variants act as a dominant negative? mapping putative dominant negative domain(s)
ADAMTS13 activityin Bethesda Units
bethesda assay:
vsvsstdTTP
stdctrl
rADAMTS13s
stdTTP
3. Antigen for monoclonal antibody generation
T6CUB2
CUB1
T8T7T5
T4T3T2Sp
CRDT1DMP
rADAMTS13 variants
Abstract:
Aims of the study:
TTP Is a Multifacted Disease:
1. Di�erential diagnosis between TTP and other thrombotic microangiopathies remains challenging
Non-neutralising
2. Two classes of ADAMTS13 autoantibody exist:
Neutralising
- Autoantibody ratio in healthy and diseased plasma unknown- Lack de�nitive assay to di�erentiate subtypes
table adapted from Mannucci and Peyvandi (Hematology 2007)
1.Develop the APMAT research network protocol2.Formation of an AP medical advisory panel of APMAT experts
for individual clinical advice3.Establish a clinical adjudication committee for independent
online classi�cation of MAT patients
4.Standardise laboratory testing for ADAMTS13 and any other novel assays in the AP region
5.Develope ADAMTS13 replacement therapy6.Extend novel ADAMTS13 assays to myocardial infarction and
stroke prediction
use recombinant ADAMTS13 protein variants and patient samples to:
PP
P
PPP
P
Normal: VWF multimer (globular)
P P
PPPPP
P P
PPPPP
P P
PPPPP
ultra large VWF multimer(shear activated)
ADAMTS13
PP
PPP
PP
P P
P
ADAMTS13
P
P P
PP
P
ADAMTS13 mediated cleavageof VWF A2 domain blood
�ow
VWF (shear activated)vascular injury
Disease Common symptoms Differential symptomsHemolytic uremic syndrome Thrombocytopenia, hemolytic anemia
with schistocytosisGastrointestinal infections: E. coli 0157:H7, Shigella dysenteria Hemorrhagic colitis High serum creatinine
HELLP syndrome Hemolytic anemia, thrombocytopenia Elevated liver enzymes
Pre-eclampsia, eclampsia Thrombocytopenia, proteinuria Hypertension Peripheral edema Proteinuria Increased D-dimer
Disseminated intravascular coagulation
Thrombocytopenia Markedly increased D-dimer Prolonged prothrombin time
Catastrophic antiphospholipid syndrome
Thrombocytopenia Positive lupus-like anticoagulant
Antinuclear and antiphospholipid antibodies
Evans syndrome Hemolytic anemia, thrombocytopenia Positive Coombs test Usually absence of end-organ ischemic symptoms
Heparin-induced thrombocytopenia Thrombocytopenia Thrombosis mainly in large arteries and veins Antiplatelet antibodies
(Western Australia Centre for Thrombosis and Haemostasis, Murdoch University; Perth Blood Institute, Hollywood Specialist Centre, Western Australia)