Embed Size (px)
Citation preview
Insomnia
St. Joseph’s Annual Family Practice Refresher March 1, 2018 Robert J. Ostrander, M.D
If in bed I say, “When shall I arise?” then the night drags on; I am filled with restlessness until the dawn. Job 7:4
Disclosures: None Goals: Understand basic information about the physiology of sleep and the neurotransmitters involved Improved familiarity with nonpharmacologic interventions to treat insomnia Understand the rationale for choosing pharmacologic agents to treat insomnia.
Sleep disorders ●Insomnia ●Sleep-related breathing disorders ●Central disorders of hypersomnolence ●Circadian rhythm sleep-wake disorders ●Parasomnias ●Sleep-related movement disorders ●Other sleep disorders
Definition of Insomnia: Subjective report of difficulty initiating or maintaining sleep, at least 3 times a week to the extent that it disrupts daytime functioning. Prevalence: 30% of adults (intermittent or chronic) 50% of those over 65
Why is this so common? Thomas Edison and clocks. The primary regulator of normal sleep is an internal circadian clock which is entrained and “set” by similar light and dark cycles day after day, detected by the retina and relayed to the pineal gland, whose cyclic release of melatonin drives internal rhythms. Secondary contributors to this regulation include stimulation through other senses and activity. It is obvious, then, how living in modern society in the developed world undermines healthy sleep biology.
Evaluation: HPI-we all know how to do this—details are key Medications and substance history Evaluate for depression or other mood disorder And all the rest…..
Insomnia
Secondary Causes of Poor Nighttime Sleep: Stress Anxiety Depression (and its treatment) Obstructive Sleep Apnea Restless Leg Syndrome Nocturnal Myoclonus Nocturnal Leg Cramps GERD Pain Shift Work Bed Partner Nocturia Etc.,etc.,etc......... (Bear in mind when we discuss Cognitive Behavioral Therapy---CBT-I)
Insomnia
“Primary” altered sleep physiology. Sleep is ½ intrinsic biology and ½ learned
behavior.
Insomnia
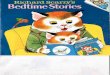
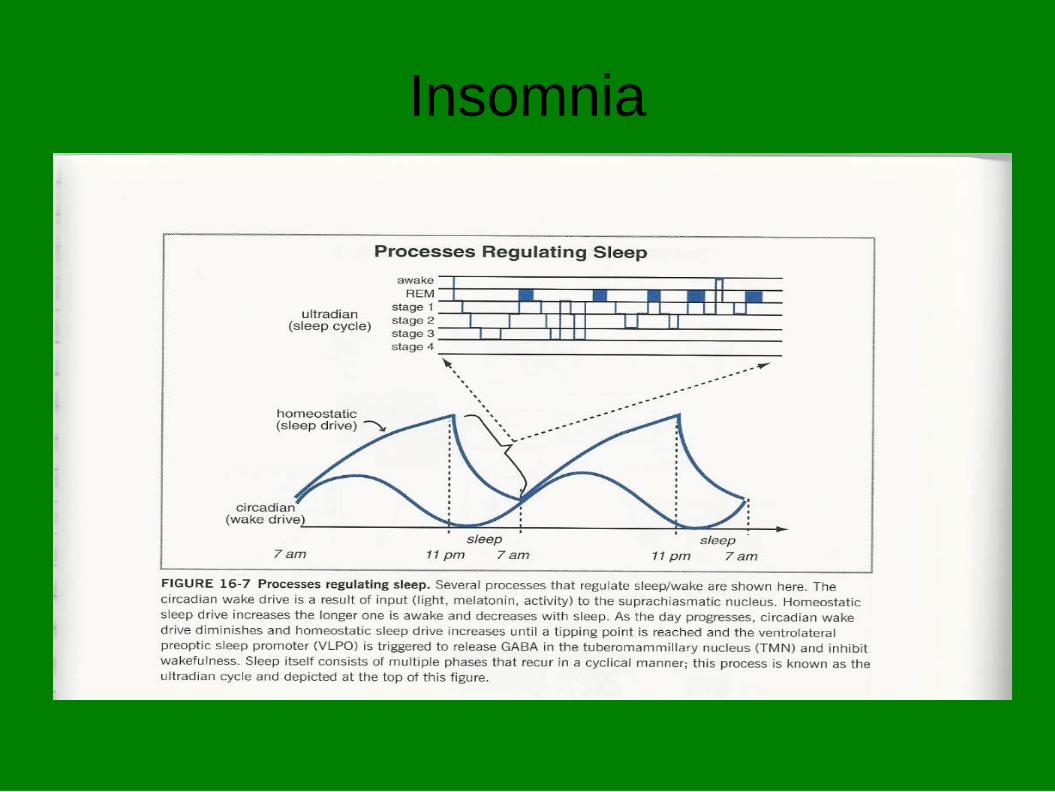
Two Process Model: 1) Sleep deprivation drives sleepiness and inhibits
wakefulness. “Inhibitory” pathways. (GABA) 2) Circadian “excitatory” pathways drive wakefulness and
inhibit sleepiness. (Absence of melatonin allows Histamine release.)
Insomnia
Sleep deprivation peaks at bedtime and dissipates overnight.
Circadian arousal peaks in the early evening or
late afternoon,wanes at bedtime, reaches nadir in the early am hours and waxes as time for waking approaches.
Insomnia
Insomnia
Circadian arousal “clock” set by: Light-dark Entering a deep sleep Stress and demands for alertness Age– (an exaggeration) Youth are awake 20 hours, then sleep 10. Elders are awake 14 hours and sleep 7.
Insomnia
Treatment: Meds—like with anxiety a double edged sword Cognitive Behavioral Therapy for Insomnia (CBT-I)/ Sleep Hygiene/Training
Insomnia
CBT-I, Sleep Hygiene Recognize contributors + and - No bedtime ritual—relaxation before bed EtOH, caffeine, decongestants.... Too little exercise early, too much late Food—The Goldilocks Principle ?Sex
Insomnia
CBT-I, Sleep Hygiene (Cont'd) Stimulus Control—all mammals have a sleeping place Don't work, watch TV etc. in bed or even bedroom Control light and sound—not just for sleeping Sleep Restriction—later bedtime, no naps. Relaxation Techniques-trying to sleep is the enemy of sleep Relapse Prevention
Insomnia
Specific Patterns: Advanced Sleep Phase Asleep and up too early Treat with bright evenings, dark mornings Sleep restriction at hs (+/- afternoon power nap) More common in depression and the elderly Delayed Circadian Cannot fall asleep, and then cannot wake up, OR Sleeps 2-4h, wake 2-3h, sleep 3-4 h Treat with light mornings, dark and quiet evenings Common in adolescents
Insomnia
Medications: “Use the medication nightly for one to two weeks to re-
entrain a normal sleep pattern, then on nights when there has been poor sleep the night or two before; or when the next day is likely to be stressful or demanding. Avoid using it nightly. Avoid going more than 2 nights in a row with poor sleep.”
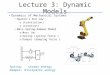
Insomnia Neurotransmitters: GABA-released by sleep deprivation, promotes sleepiness inhibits wakefulness. Histamine (H1 receptor) release driven by intrinsic circadian rhythm, promoting wakefulness. Serotonin (5HT). Many receptor types. Activation at 2A receptor tends to fragment sleep and decrease REM Orexin-helps maintain wakefulness, diminished in those with narcolepsy. Melatonin release promotes sleepiness through various neural pathways including inhibiting histamine release. Others-NE,Ach,Adenosine,glutamate
Insomnia Medications GABA receptor drugs—benzos, zolpidem, etc. zolpidem
more selective for receptors in the sleep center. Anti-H1 (usually anticholinergic with all that baggage) E.g. Diphenhydramine and Doxylamine. Tolerance develops. Low-dose doxepin not as anticholinergic. 2-6mg,
FDA approved, only available branded at that dose. Melatonin and agonists (e.g Rozerem-ramelteon) Aid in sleep initiation, not maintenance. Not habit forming. Trazodone—5HT-2A Receptor Blockade and H1 antagonist
Insomnia
Medications Mirtazapine. Central alpha-2, H1 and 5HT-2
antagonist. Stimulates appetite. T ½ 20-40h. Consider if insomnia is part of a symptom complex.
Number of good studies varies for these medications,
especially if not FDA approved for insomnia/approval not sought. Few head to head studies. Patients not sorted by characteristics.
Insomnia
Let’s talk about why I like trazodone… SARI-serotonin antagonist and reuptake inhibitor. It is a different drug in low dose them in the usual
antidepressant dose. In low doses (25-50 mg) it primarily blocks 5 HT/2A and H1 receptors. Very little serotonin reuptake inhibition or blocking of other serotonin receptors.
Short half-life Works great with SSRIs
Insomnia Suvorexant (Belsomra) FDA approved in 2014. Blocks orexin T ½=12 hours Class IV $12 per pill Side effects can include all of those things seen with other sedatives, as well as narcolepsy-type symptoms. I remain skeptical until it has been available longer-using cautiously only in patients resistant to other measures and still having significant problems with daytime functioning.
References Electrical Activity of the Brain, Sleep–Wake States, & Circadian Rhythms. In: Barrett KE, Barman SM, Boitano S, Brooks HL. eds. Ganong’s Review of Medical Physiology, 25e New York, NY: McGraw-Hill; . http://accessmedicine.mhmedical.com.libproxy1.upstate.edu/content.aspx?bookid=1587§ionid=97163575. Accessed February 18, 2018. McGinty DT. Serotonin and Sleep: Molecular, Functional, and Clinical Aspects.Sleep. 2009;32(5):699-700. Institute of Medicine (US) Committee on Sleep Medicine and Research; Colten HR, Altevogt BM, editors. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem, Chapter 2, Sleep Physiology. Washington (DC): National Academies Press (US); 2006. Mihic S, Harris R. Chapter 17. Hypnotics and Sedatives. In: Brunton LL, Chabner BA, Knollmann BC, eds. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill; 2011. http://www.accessmedicine.com/content.aspx?aID=16663643. Accessed January 1, 2013.
References
Smith, Howard S MD1*; Barkin, Robert L MBA, Pharm D, FCP2,3; Barkin, Stacy J MED, MA, PSYD, LISAC, LPC4. American Journal of Therapeutics, Issue: Volume 18(3), May 2011, pp 227-240. Copyright: © 2011 Lippincott Williams & Wilkins, Inc. Kierlin, Lara MD. Sleeping Without a Pill: Nonpharmacologic Treatments for Insomnia, Journal of Psychiatric Practice. Issue: Volume 14(6), November 2008, pp 403-407. Copyright: © 2008 Lippincott Williams & Wilkins, Inc. Buysse, Daniel J. M.D., Chronic Insomnia, The American Journal of Psychiatry, Issue: Volume 165(6), June 2008, p 678–686 Stahl, Steven M., Stahl’s Essential Psychopharmacology-Neuroscientific Basis and Practical Applications, 4th Edition, Cambridge University Press, 2013.
Insomnia
THANK YOU!