Embed Size (px)
Citation preview

REVIEW
Insights into keratoconus from a genetic perspective
Clin Exp Optom 2013; 96: 146–154 DOI:10.1111/cxo.12024
Kathryn P Burdon* PhD BSc(Hons)Andrea L Vincent† MBChB FRANZCO* Department of Ophthalmology, Flinders University,Adelaide, South Australia, Australia† Department of Ophthalmology, New ZealandNational Eye Centre, Faculty of Medical and HealthSciences, University of Auckland, Auckland,New ZealandE-mail: [email protected]
Keratoconus is a progressive and non-inflammatory thinning of the cornea, which mayresult in severe visual impairment due to irregular curvature and scarring. It can occur inisolation but is often seen in association with other systemic or ocular disorders. There is awell-recognised genetic component to keratoconus, as evidenced by family and twin studies;however, the aetiology of the disease is complex with both genetic and environmental factorsplaying a role. Over the last decade significant progress has been made in identifying geneticrisk factors for keratoconus. Multiple approaches have been taken including candidate genestudies and genome-wide studies. VSX1 remains as the best characterised keratoconus genebut only accounts for rare cases. Other candidate genes with a role to play include SOD1,other corneal dystrophy genes such as ZEB1 and TGFBI and collagen genes. Family-basedstudies have recently led to the identification of the MIR184 gene for keratoconus withcataract and to the DOCK9 gene in a family with isolated keratoconus. Numerous otherlinkages have been reported and new sequencing technologies are set to rapidly expand thenumber of identified keratoconus genes in these regions. Similarly, recent genome-wideassociation studies in case-controlled cohorts have identified common variations in andaround HGF, RAB3GAP1 and LOX as candidate risk factors for keratoconus. These geneidentifications are beginning to reveal the molecular aetiology of keratoconus but despitethis recent progress, there remain numerous genetic risk factors to be identified for thisrelatively common yet complex disease.
Submitted: 30 July 2012Revised: 18 October 2012Accepted for publication: 30 October 2012
Key words: cornea, genetics, keratoconus
Keratoconus most likely represents a multi-genic disease with a complex mode ofinheritance and environmental factors con-tributing to the disease manifestation. Therelative contribution of each is subject todebate and likely varies between individuals.It appears that at one end of the spectrum,disease in some individuals is probably dueentirely to environmental influences, as seenfollowing trauma,1 yet at the other endmay be solely under the control of geneticmechanisms, as evidenced by strong auto-somal dominant inheritance in certain fami-lies.2,3 The majority of cases will most likelybe the result of a genetic predispositionwith precipitating environmental stressorsor modifiers. This review article summarisesthe historical and current level of knowledgeof the genetic risk factors for keratoconus.
PHENOTYPIC SPECTRUM
Early descriptions of keratoconus werefocused on advanced disease, that is, severe
corneal disease causing marked visualimpairment or other clinical symptoms.The advent of more sophisticated cornealimaging modalities, such as computerisedcorneal topography and in vivo confocalmicroscopy has led to a greater understand-ing of the vast variation in expressivity ofcorneal diseases. This allows objective meas-urement of earlier and/or milder changes inthe disease process. In particular, cornealtopography of ‘unaffected’ family membersin keratoconus demonstrated abnormalitiesof corneal shape that were not within the‘normal’ range, yet did not meet the existingclinical criteria for keratoconus.4 Cliniciansnow refer to this entity as ‘forme fruste’keratoconus, with a re-definition of therefractive and topographic criteria. Simi-larly, imaging with the in vivo confocalmicroscope now allows micro-structuralanalysis, demonstrating alterations in veryearly or mild corneal disease, rather thanonly at the end-stage.5 Large variations inintra- and inter-familial ‘disease’ are antici-
pated when careful, expert phenotyping isundertaken as recently demonstrated in aNew Zealand cohort and in twins.6,7
HEREDITY OF KERATOCONUS
The role of heredity in keratoconus is welldocumented,4,8–10 with concordance in twinsand a positive family history reported insix to 23 per cent of patients with kerato-conus.11,12 Using more sophisticated cornealimaging modalities, such as computerisedcorneal topography, prevalence in first-degree relatives is 15 to 67 times higher thanthe general population.10
The mode of inheritance is reportedas sporadic, autosomal recessive10 andautosomal dominant.13 Other studies14 haveestablished linkage by using a model ofinheritance that lies somewhere betweenthese two.
Twin studies have emerged as a powerfultool to determine the effect of heredity ondisease manifestation. Comparing cohorts
C L I N I C A L A N D E X P E R I M E N T A L
OPTOMETRY
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
146 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

of monozygotic (MZ) twins, with a cohortof dizygotic (DZ) twins, an assessment can bemade of the relative contributions of thegenotype and environment to the pheno-type. A recent small study demonstratedhigher concordance of keratoconus inmonozygotic than in dizygotic twins, witha greater similarity of phenotype in themonozygotic twins, consistent with a stronggenetic component to this disorder.7
EPIDEMIOLOGY
The incidence of keratoconus is estimated tobe between 29 and 229 per 100,000 depend-ing on the population examined7 and therates among different ethnic groups aredocumented to vary.11,15–18 A study of inci-dence and severity of keratoconus at theLeicester Royal Infirmary in the UnitedKingdom identified a four-fold greater inci-dence of keratoconus among Asians (pre-dominantly Indian) living in the catchmentarea than among Caucasians.18 The severityof the disease, defined as age of onset andtime from presentation to graft was alsofound to be greater among the Asian group.Although race was assigned on the basis ofthe patient’s name rather than collecteddirectly from the patient, the comparisonsbetween races in this study are strong, as allpatients were resident in the same area anda single definition of disease was used. Itis widely believed that keratoconus is moreprevalent and aggressive in New Zealand,especially in the Maori and Polynesian po-pulations, although exact figures are notavailable.19 Keratoconus is the leading indi-cation for corneal transplantation in bothadults and children in New Zealand andAustralia.20–22 Of the affected Maori andPacific peoples, 31 per cent have a positivefamily history.6 Many multi-generationalfamilies are identified that show manymembers affected in many generations. Thestrong familial aggregation of keratoconusobserved within this population is likely to bedue to a major gene effect.
ASSOCIATION WITHOTHER DISORDERS
The occurrence of keratoconus in associa-tion with a wide range of other diseasesmay also provide clues as to the underlyinggenetic mechanisms. Connective tissue dis-orders are over-represented among patientswith keratoconus, suggesting an underlying
structural abnormality and include EhlersDanlos syndrome23 osteogenesis imperfecta,mitral valve prolapse12 and craniosynostoses,such as Crouzon.24 Keratoconus is frequentlyreported as a manifestation of Marfansyndrome,25 although the cornea in Marfansyndrome is clearly characterised as beingflatter in curvature and generally thin-ner.26–28 This may suggest that given theright environmental stressor, the inherentcorneal structure reaches a tipping point tobecome keratoconic.
Keratoconus frequently occurs in isola-tion, but is often associated with a wide rangeof ocular disorders, including cataract,29
atopy,30 Leber congenital amaurosis,31
other corneal dystrophies and retinal dys-trophies.32 Other associations include X-linked hyphidrotic ectodermal dysplasia,with changes in the EDA gene33 andWilliams–Beuren syndrome.34 The observa-tion of keratoconus occurring in associationwith an unusual syndrome or disorder, doesnot in itself mean the underlying geneticcause may be common to both concurrentdiseases but it may suggest that a manifesta-tion of the syndrome is an environmentalagonist for keratoconus. As keratoconus isnot uncommon, it feasibly may occur inde-pendently of the coexistent disorder.
Many genetically determined cornealdystrophies can also occur in associationwith keratoconus including posterior poly-morphous corneal dystrophy (PPCD),35
lattice dystrophy,36 granular dystrophy37 andFuchs’ endothelial dystrophy.38 The asso-ciation of keratoconus with so many cor-neal dystrophies and ocular abnormalitiesimplies either a similarity in the underlyinggenetic defect or a tightly linked network ofinteracting proteins, with a final commondevelopmental pathway. Keratoconus alsooccurs with a range of chromosomal abnor-malities, most commonly in Down syndromedue to trisomy 2139 and also in Turner syn-drome,40 chromosome 13 ring anomaly41
and translocation 7;11.42
CANDIDATE GENE ANALYSIS
Depending on knowledge of the underlyingbiology of the trait, it may be possible topredict genes involved in particular diseases.In keratoconus, potential candidates arethose associated with other corneal dystro-phies, connective tissue disorders or locatedon chromosomes where chromosomal aneu-ploidy or breakpoints are associated withthe disease, for example, chromosome 21
in Down syndrome. Bioinformatic databasesare used to determine if putative genes makebiological sense and are expressed in therelevant tissue (cornea). Genes are usuallyprioritised according to their likelihood asdisease-causing genes in keratoconus onthe basis of their expression patterns andany known functions or mutations, whichare relevant to the eye. If the ocular expres-sion of any of the most promising genesis not clear, expression studies using reversetranscription-polymerase chain reaction(RT-PCR) and/or Western blotting of cor-neal tissue may be performed to assist inevaluating the significance of any variantsfound in genes that are expressed in thecornea.
Mutations in a number of candidate geneshave been determined in a small percentageof patients with keratoconus. These43–48 arelisted in Table 1 and their genomic locationindicated in Figure 1.
VISUAL SYSTEM HOMEOBOX 1 GENE
The visual system homeobox 1 gene (VSX1)is a member of the ‘paired-like’ homeodo-main transcription factors. This family playsa role in craniofacial and ocular develop-ment. Human VSX1 has been mapped to20p11.2. It was initially reported to consistof five exons and be approximately 6.2 kbin size.49 An additional two exons were latercharacterised,50,51 which encode alternativeisoforms of the VSX1 transcript. The expres-sion of VSX1 has been detected in embryoniccraniofacial tissues, adult retina and adultcorneas.49,52 Mutations in VSX1 were report-edly associated with craniofacial abnormali-ties, empty sella tunica and abnormal retinalcells53 but more frequently and controver-sially to a number of corneal dystrophies andectasias, specifically keratoconus and PPCD.
Gene Locus Reference
VSX1 20p11.2 43ZEB1 10p11.22 44SOD1 21q22.11 45TGFBI 5q31.1 46COL4A3/COL4A4 2q36.3 47FLG 1q21 48
Table 1. Candidate genes with mutationsidentified in patients with keratoconus
Genetics of keratoconus Burdon and Vincent
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 147
The relationship between kerato-conus and VSX1 was first reported in thestudy by Héon and colleagues.43 Severalmutations linked to keratoconus have sincebeen identified.50,54–57 The role of VSX1 inthe pathogenesis of keratoconus has beencontroversial, as a number of other studieshave failed to identify an association be-tween VSX1 variants/polymorphisms andkeratoconus.58–62 These contradictory resultsmay be attributed partly to the low frequencyof changes, ethnic variation, and the mount-ing evidence that keratoconus is likely to bea multifactorial and polygenic disease.62
VSX1 expression in keratocytes has beencharacterised both in vitro and in vivousing RT-PCR, immunohistochemistry andin situ hybridisation. Although not observedin resting or quiescent human keratocytes,in wounded corneas, or when culturedin serum to mimic wounded conditions,the keratocytes express VSX1 and this isalso associated with fibroblastic transforma-tion.52 These observations add strength
to the hypothesis that VSX1 is involved inthe wound healing response and thus maycontribute to the underlying pathology incorneal disease.
The largest published series on thissubject looked at an Italian cohort of 302individuals with keratoconus and foundchanges in VSX1 in 3.2 per cent of theaffected population.63 A study of Iranianfamilies with keratoconus also showedHis244Arg segregating with disease in atwo generation pedigree. Four affectedindividuals were heterozygous, whereas fiveunaffected were not, and the mutation wasnot present in extensively phenotyped con-trols.64 Analysis of the pedigrees has demon-strated a 58 per cent reduced penetrancein general amongst the Iranian familieswith keratoconus, which could explainthe finding of Tang and colleagues,61 whoreported the presence of this same variantin unaffected family members. Other recentstudies also highlight segregation of otherVSX1 changes.63,65
ASSOCIATION WITH PPCD AND THEZEB1 GENE
The association of PPCD with keratoconusis also well documented with many cases ofthese two conditions occurring in the samecornea.8,66–71 PPCD and keratoconus share apotential common mode of involvement ofthe posterior surface of the cornea, specifi-cally Desçemet’s membrane and/or anunderlying commonality in the pathophysi-ology of corneal dystrophies. A recent papercharacterised the cornea in patients withPPCD showing the topographic parametersare significantly steeper but with no clinicalor topographical evidence of keratoconus.72
This group of patients was not geneticallycharacterised but another study demon-strated that in six patients with ZEB1 (zincfinger E-box binding homeobox 1) genemutations, three had steep corneas but noevidence of keratoconus.73 Another groupreported changes in the ZEB1 gene inpatients with keratoconus44 indicating theremay be genetic overlap between these cor-neal diseases.
OXIDATIVE STRESS GENES
Another explanatory hypothesis is that oxi-dative stress plays a role in the aetiology ofkeratoconus. A superoxide dismutase isoen-zyme SOD1 was considered a candidatebecause of its location on chromosome 21,given the association of trisomy 21 with kera-toconus, and a differential level of expres-sion in healthy corneas compared withkeratoconic corneas. An intronic sequencedeletion was found to segregate with diseasein two families with keratoconus45 butit remains unclear whether this is a trulypathogenic association, as it has only beendetected in a further two patients of a total of430 (0.9 per cent).60,63,64
To explore the putative role of oxidativestress, another group undertook mito-chondrial complex 1 gene analysis (ND1–6,encoded by the mitochondrial genome) in agroup of 20 patients with keratoconus nega-tive for VSX1 mutations.74 Complex 1 varia-tions may result in an increase in reactiveoxygen species (ROS). An extraordinarilylarge number of changes (n = 84) werefound in the ND group of genes, with themajority occurring in ND5 and included twonovel frameshift mutations.74 Some of thechanges detected are reported as also occur-ring in other mitochondrial related disor-ders. With such diverse variation and the
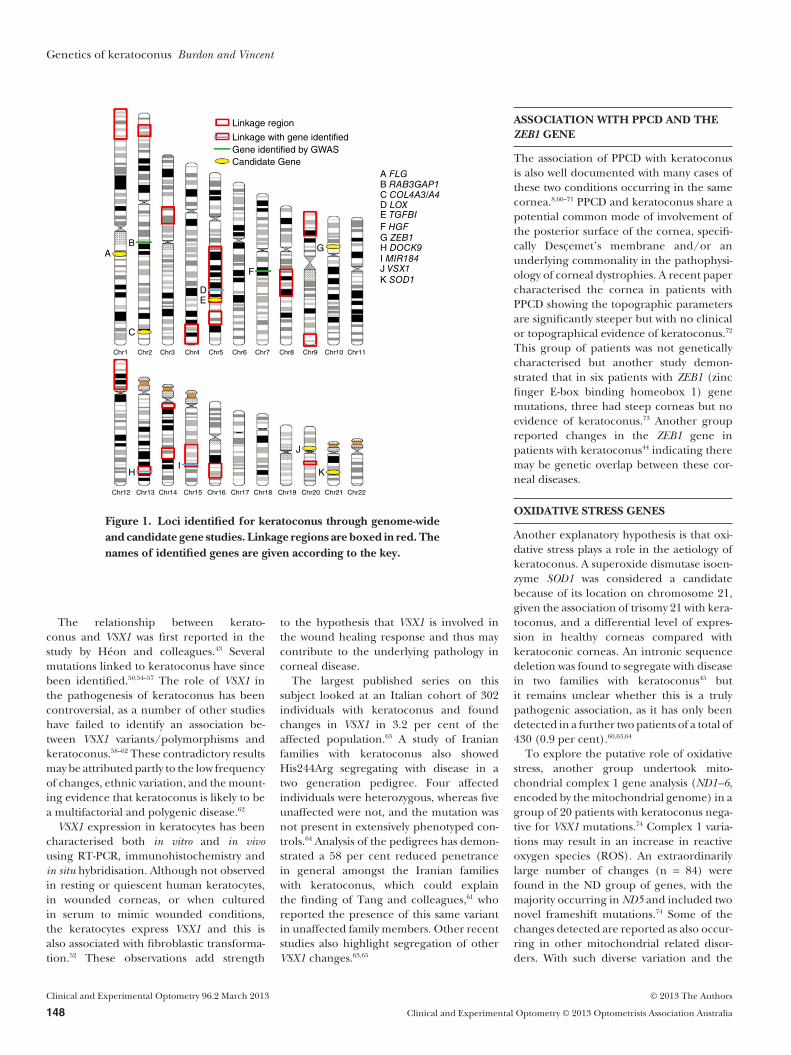
A FLGB RAB3GAP1C COL4A3/A4D LOXE TGFBIF HGFG ZEB1H DOCK9I MIR184J VSX1K SOD1
Linkage region
Linkage with gene identifiedGene identified by GWASCandidate Gene
AB
C
DE
F
G
HI
J
K
Chr1 Chr2 Chr3 Chr4 Chr5 Chr6 Chr7 Chr8 Chr9 Chr10 Chr11
Chr12 Chr13 Chr14 Chr15 Chr16 Chr17 Chr18 Chr19 Chr20 Chr21 Chr22
Figure 1. Loci identified for keratoconus through genome-wideand candidate gene studies. Linkage regions are boxed in red. Thenames of identified genes are given according to the key.
Genetics of keratoconus Burdon and Vincent
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
148 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

complexities associated with mitochondrialdisease, the true impact of these changes willrequire larger studies to verify the interest-ing findings.
EXTRACELLULAR MATRIX GENES
The tissue inhibitors of metalloproteinases(TIMPs) are naturally occurring inhibitorsof the matrix metalloproteinases and thebalance between the two regulates extracel-lular matrix remodelling. As TIMP3 showeddifferential expression in the keratoconiccornea, it has also been screened for muta-tions with none detected.63
A recent study looked at the role of thetransforming growth factor beta-induced(TGFBI) gene which is an extracellularmatrix gene responsible for many dominantcorneal dystrophies.75 The gene was inves-tigated in a Chinese cohort of 30 patientswith keratoconus and a novel nonsensemutation, G535X, was observed in oneindividual.46 The relevance of this geneto keratoconus more broadly is yet to bedetermined.
COLLAGENS
Another theory of disease pathogenesis isan underlying alteration in the corneal col-lagen structure, function and/or develop-ment during embryology. Thus, a number ofcollagen genes have been investigated, aswell as genes thought to be involved in thecollagen pathways. Sequencing COL4A3 andCOL4A4 failed to detect any pathologicalvariants in 107 patients with keratoconus butsignificant allele frequency differences atthe D326Y variant in COL4A3 and M1237Vand F1644F in COL4A4 were distinctive ofpatients with keratoconus.47
Another study analysed COL4A1 andCOL4A2 in 15 Ecuadorian families withkeratoconus and although a number of mis-sense variants were detected in both genes,none segregated with disease in the families,suggesting some other genetic cause fortheir disease.76 COL8A1 and COL8A2 werealso investigated in 50 patients but yetagain no pathogenic sequence variants weredetected.77
APOPTOSIS RELATED PATHWAYS
The occurrence of atopic/allergic eyedisease in association with keratoconus iswell documented in up to 50 per cent of
individuals.48 One postulated mechanismis the mechanical stimulation from eyerubbing causes epithelial damage resultingin keratocyte apoptosis, via the Fas-ligand orInterleukin 1 pathway,62 although it cannotbe excluded that the genetic cause for thetwo conditions is more tightly linked. Filag-grin (FLG) mutations are a strong geneticrisk factor for atopic dermatitis, with theprotein expressed in the corneal epithelium,rendering this gene a good candidate.Two prevalent loss-of-function FLG alleles(R501X and 2282del4) were screened forin a keratoconic population, and five of 89demonstrated at least one FLG mutation.48
This was lower than expected with the muta-tion frequency in a population with atopicdermatitis around 12 to 15 per cent.
GENOME-WIDE STUDIES
Genome-wide studies aim to take an unbi-ased approach towards gene mapping andthe identification of candidate genes fordisease. They have the advantage of notrelying on prior knowledge of the functionof a gene, as illustrated above with candidategene studies but have the disadvantage ofa more stringent level of statistical signifi-cance to prevent the reporting of false posi-tive findings due to chance and multiplehypothesis testing. Both linkage and associa-tion studies2,3,13,14,78–87 have been used at thegenome-wide level in keratoconus (Table 2,Figure 1). Increasing evidence suggests copynumber variation (CNV) is a significantgenetic mechanism in Mendelian disorders.Such variants can be detected on a genome-wide level using array CGH; however, in arecent study of 20 keratoconic patients fromSaudi Arabia, no changes were detected thatwould account for keratoconus.88
LINKAGE STUDIES INEXTENDED FAMILIES
Linkage analysis has been used extensivelyto map susceptibility loci for keratoconus.The approach of using large extended pedi-grees has proven the most successful withtwo potential genes identified though thisapproach.
MIR184 IN A NORTHERNIRISH FAMILY
In 2003, Hughes and colleagues reported asingle extended pedigree from Northern
Ireland with keratoconus and cataractco-segregating in an autosomal dominantinheritance pattern. Using microsatellitemarkers, the authors demonstrated linkageof the phenotype to chromosome 15q22–q24,29 which was further refined by subse-quent fine mapping to a critical region of5.5 Mb.89 Recently introduced high through-put (‘next generation’) DNA sequencingtechnology was then used to sequence theentire region. This resulted in the identi-fication of three novel variants (in genesDNAJA4, IREB2 and MIR184) that segre-gated with the phenotype in this family.78
The r.57 c > u mutation in the microRNAgene MIR184, was considered to be the mostlikely cause, as the IREB2 mutation was in the3’UTR and DNAJA4 was not known to playa role in the eye. MIR184 is abundantlyexpressed in the cornea and lens epitheliaand the mutation was located in the seedregion and thus, highly likely to affectthe function of the microRNA. The studytook over a decade to identify the causativevariant and was eventually achieved onlythrough the use of cutting edge technologyand relying on the well-annotated humangenome reference sequence. A subsequentreport has identified the same mutationin a family with EDICT syndrome (cornealendothelial dystrophy, iris hypoplasia, con-genital cataract and corneal stromal thin-ning),90 expanding and further defining thephenotype associated with this mutation.The primary known role of microRNA inthe cell is the regulation of gene expression,through inhibition of translation by bindingto complementary sequences in the 3’UTRof target mRNA. Only a few direct diseaseassociations have been reported in micro-RNA genes; however, as the catalogue ofknown microRNA grows and these genesare more routinely assayed in gene dis-covery projects, their relative contribution todisease is likely to grow. This finding repre-sented the first successful outcome froma linkage/positional cloning study for kera-toconus, although it is not yet known ifMIR184 is relevant in isolated keratoconus.
DOCK9 in an Ecuadorian familyIn 2009, Gajecka and colleagues3 reported astudy of 18 Ecuadorian families with auto-somal dominant keratoconus. They identi-fied linkage in one of these families toa 5.59 Mb region of chromosome 13q32using a whole-genome single-nucleotidepolymorphism (SNP) array with 250,000SNPs. Eight candidate genes of the 25
Genetics of keratoconus Burdon and Vincent
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 149
located in the linkage region were sub-sequently sequenced in the family.79
They identified a novel variant, c.2262A(Gln745His) in the DOCK9 (dedicator ofcytokinesis 9) gene that segregated in thefamily and was absent from ethnicallymatched controls. This mutation is pre-dicted to be ‘possibly damaging’ to proteinfunction by the PolyPhen algorithm91 andis possibly the cause of keratoconus inthis family. DOCK9 specifically activates theG-protein, CDC42. It is expressed in bothkeratoconic and normal corneas by RT-PCR.The reported mutation is located in theDHR1 domain, which binds phospholipidsand is likely involved in the recruitment ofthe protein to the cell membrane.79 It is notclear how mutations in this gene might causekeratoconus specifically and there havebeen no further reports of mutations in thisgene in patients with keratoconus.
Other loci identified inextended familiesFour other chromosomal loci have beenidentified using extended pedigrees. In2004, Brancati and colleagues2 reporteda three-generation Italian family with 11affected members showing linkage to a53 Mb region of chromosome 3, flankingthe centromere. Tang and colleagues80
described a four-generation pedigree fromthe United States of America with multipleaffected founders and demonstrated linkagein one branch of the pedigree to chromo-some 5q14–q21. A further two loci werereported by Burdon and colleagues81 in asingle three generation Australian pedigreeshowing potential digenic inheritance,with affected individuals displaying segrega-tion of haplotypes on chromosomes 1p36and 8q13–q21. Although all these studiesscreened likely candidate genes within thelinkage regions, causative mutations are yetto be identified. Modern sequencing tech-nology opens the way for gene identificationin these families in the near future.
IDENTITY-BY-DESCENT APPROACH TOGENE MAPPING
A novel approach to keratoconus genemapping was taken by Fullerton and col-leagues,14 who reported a locus on chromo-some 20q12. This study was based onmeasuring identity-by-descent in apparentlyunrelated individuals from a single clinic,in a small regional city in the island stateof Tasmania, Australia. This approachassumed that patients with keratoconusin the area were distantly related due to afounder effect. This study identified a region
on 20q12 that was shared between sevenaffected individuals and also showed associa-tion in a larger cohort, with the allele fre-quency differing significantly from thenormal Tasmanian population.
LINKAGE STUDIES IN SMALL FAMILIES
Several linkage studies for keratoconus havebeen conducted using cohorts of multiplesmall families. These studies have identifiedmultiple risk loci through the use of bothparametric and non-parametric linkageanalysis.
In 2002, Tyynismaa and colleagues13
reported a linkage study in 20 families fromnorthern Finland. Linkage was detected onchromosome 16q22–q23 over a region of6.0 cM. Hutchings and colleagues82 con-ducted a genome-wide linkage study initiallyusing a small cohort of seven families ofCaucasian and Arab origin. Putative linkageto chromosome 2p24 was identified but didnot meet the required Logarithm of theodds (LOD) score of 3.3 for statistical signifi-cance. To improve the power, they investi-gated this region in a further 21 familiesfrom the same ethnic groups. Multipointparametric linkage analysis gave a LODscore of 5.13, when 52 per cent of the fami-lies were included in the analysis (maximum
Locus Method Cohort type Marker type Ethnicity Comments Ref
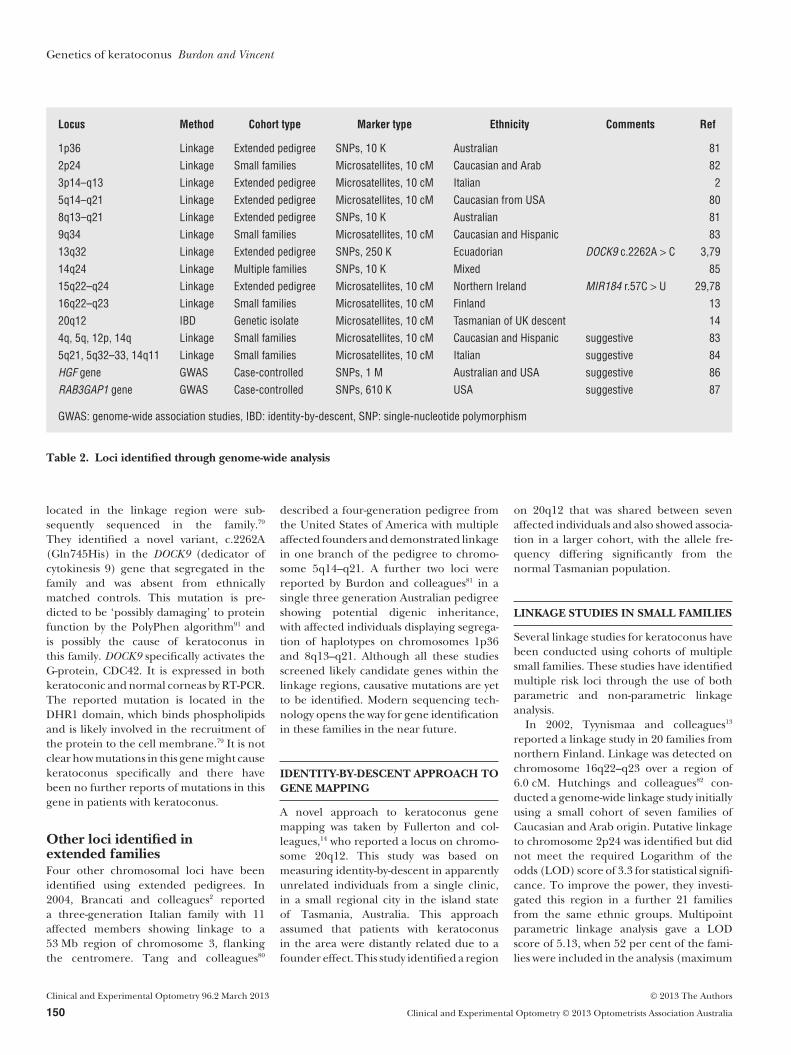
1p36 Linkage Extended pedigree SNPs, 10 K Australian 812p24 Linkage Small families Microsatellites, 10 cM Caucasian and Arab 823p14–q13 Linkage Extended pedigree Microsatellites, 10 cM Italian 25q14–q21 Linkage Extended pedigree Microsatellites, 10 cM Caucasian from USA 808q13–q21 Linkage Extended pedigree SNPs, 10 K Australian 819q34 Linkage Small families Microsatellites, 10 cM Caucasian and Hispanic 8313q32 Linkage Extended pedigree SNPs, 250 K Ecuadorian DOCK9 c.2262A > C 3,7914q24 Linkage Multiple families SNPs, 10 K Mixed 8515q22–q24 Linkage Extended pedigree Microsatellites, 10 cM Northern Ireland MIR184 r.57C > U 29,7816q22–q23 Linkage Small families Microsatellites, 10 cM Finland 1320q12 IBD Genetic isolate Microsatellites, 10 cM Tasmanian of UK descent 144q, 5q, 12p, 14q Linkage Small families Microsatellites, 10 cM Caucasian and Hispanic suggestive 835q21, 5q32–33, 14q11 Linkage Small families Microsatellites, 10 cM Italian suggestive 84HGF gene GWAS Case-controlled SNPs, 1 M Australian and USA suggestive 86RAB3GAP1 gene GWAS Case-controlled SNPs, 610 K USA suggestive 87
GWAS: genome-wide association studies, IBD: identity-by-descent, SNP: single-nucleotide polymorphism
Table 2. Loci identified through genome-wide analysis
Genetics of keratoconus Burdon and Vincent
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
150 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

hierarchical LOD or max HLOD). Nospecific mutations have been reported ineither cohort.
A larger study of 67 families of both Euro-pean (Caucasian) and Hispanic origin con-taining 110 sib-pairs was reported in 2006 byLi and colleagues.83 The most significantassociation identified was on chromosome9q34 in the Caucasian families alone but wasstrengthened by the inclusion of the His-panic cohort. Other suggestive loci includedregions on 4q, 5q, 12p and 14q. The 5q locusis in close proximity to the previouslyreported linkage in the large family by Tangand colleagues,80 although the peaks did notoverlap. Further support for linkage to chro-mosome 5 was gained from the study byBisceglia and colleagues,84 which reported astudy of 25 families from Southern Italy.They showed replication of linkage at 5q21overlapping with the significant findingof Tang and colleagues.80 In addition, theyreported suggestive linkage at 5q32–q33 and14q11, in both cases overlapping with thesuggestive linkage reported by Li and col-leagues.83 Although neither of the latterpeaks reached formal statistical significancein either study, the similar findings in twoindependent studies provides further confi-dence that these regions do harbour kerato-conus susceptibility loci. As with most otherloci reported, the causative genes are yet tobe identified.
The most recent reported linkage studyfor keratoconus was published in 2010 byLiskova and colleagues.85 The study con-sisted of six moderately sized families frommixed ethnic backgrounds recruited atMoorfields Eye Hospital in London. Thestudy identified significant linkage to chro-mosome 14q24. The authors investigatedone candidate gene from the region, VSX2,which is known to cause other ocular pheno-types and is related to VSX1, which has beenpreviously implicated in keratoconus. Nocoding mutations were identified in thisgene.
LIMITATIONS OF FINDINGS BYLINKAGE ANALYSIS
It is of note, that although some of the lociidentified by linkage analysis of keratoconusin collections of small families have beenidentified in multiple studies (5q21, 5q32and 14q11), few if any causative mutationshave been reported from these familialcohorts. This may be due to a lack ofresources to screen the large numbers of
genes under each peak but could also indi-cate the limitations of using multiple fami-lies to map complex disease traits by linkage,particularly in small numbers. The heteroge-neity of the disease can mask linkage signalsin such cohorts, particularly where indi-vidual families within the study do not havesufficient power to detect significant linkagein their own right. In contrast, the studies ofextended pedigrees have led to the identifi-cation of mutations in MIR184 and DOCK9 ;however, further work on these genesin other cohorts is required to determinethe mutation frequency of these genes inkeratoconus in general and determine theoverall contribution of these genes to thedisease.
ASSOCIATION STUDIES
Genome-wide association studies (GWAS)in case-controlled cohorts have been a valu-able addition to the techniques availableto interrogate the genetics of complexdisease. These studies aim to identify single-nucleotide polymorphisms, at which theallele frequency differs significantly be-tween cases and controls. The finding ofsuch a single-nucleotide polymorphism thenimplies that a causative variant is located inlinkage disequilibrium with that SNP (thatis, usually inherited with the SNP dueto physical proximity and disinclinationtowards recombination). Two such studieshave been reported for keratoconus,although neither has identified loci reach-ing strict statistical significance of p < 5¥10-8
to account for multiple testing. The firstreport by Burdon and colleagues86 usedcohorts from Australia, Northern Irelandand the USA in parallel and identified asso-ciation between keratoconus and SNPsin the promoter region of the hepatocytegrowth factor (HGF) gene. The finding wasconsistent across three cohorts, with thefourth replication cohort trending in thesame direction. On meta-analysis of all fourcohorts, a p-value of 9.9¥10-7 was obtained,falling slightly short of genome-wide signifi-cance. The study also showed a relationshipbetween genotype at the associated SNP(rs3735520) and serum hepatocyte growthfactor levels in normal individuals. In addi-tion, this gene has been associated withrefractive error and specifically with myopiain multiple studies,16,92,93 making it an attrac-tive candidate for keratoconus.
The second GWAS study for keratoconuswas reported by Li and colleagues87 and
described the findings from the USA cohortsthat also contributed to the HGF-associationresults. This study of 222 Caucasian casescompared to 3,324 controls identified mul-tiple putative loci that were then followedin a further 304 cases and 518 controls, aswell as a panel of 307 patients from 70 fami-lies. After typing of 4,905 SNPs of high pri-ority in the follow-up panels, SNP rs4954218located near RAB3GAP1 was the most con-sistently and significantly associated. Thisgene has been reported previously in asso-ciation with corneal malformation and thus,is an excellent candidate for a keratoconussusceptibility locus.
COMBINING GWAS ANDLINKAGE STUDIES
The amount of data generated through aGWAS is a valuable resource, which can bemined well beyond the top few significantassociations. The USA GWAS of Li and col-leagues87 has recently shed light on a genethat may have led to the linkage signalobserved in a large family at chromosome5q by the same group.83 All the genes underthe previously described linkage peaks werereviewed for their likely role in keratoconus,based on their expression pattern anddescribed roles in the literature and biologi-cal databases. One gene in particular, LOX,located under the 5q peak stood out asa particularly relevant candidate. LOX isinvolved in cross-linking collagen and elastinfibres in the corneal stroma. Artificial colla-gen fibre cross-linking using riboflavin andUV light is a procedure currently beingexplored for the treatment of keratoconuswith some success.94 The GWAS data wasexamined for evidence of association in theLOX gene and SNPs with nominally signifi-cant p-values were identified.95 These SNPsand others nearby were then genotyped in aconfirmation cohort and also in the family-based cohort. Evidence of association atsimilar significance was also seen in thesecohorts, suggesting that the LOX locus isassociated with keratoconus and may havecontributed to the linkage signal seen in thisregion. Other genes and rare variants underthe linkage peak have not yet been assessedin the family cohort and may also be contrib-uting to the signal.
SUMMARY
Although it is clear that keratoconus has amajor genetic component, identification of
Genetics of keratoconus Burdon and Vincent
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 151

the specific causative genes has been slow.Studies of individual large pedigrees haveprovided the clearest results but these find-ings are yet to be expanded to keratoconusin the general population. Further findingsin such families are expected in the nearfuture through the use of the advancedtechnology, high throughput sequencing, toscreen large numbers of genes in parallel.Candidate gene studies have also identifiedsome associations but again, they tend to berare variants with limited applicability to thebroader population. Genome-wide associa-tion studies also hold promise but requirelarger cohorts than those analysed to gainsufficient power to detect the small effectsexpected at individual loci. An alternativeapproach is to take information fromgenome-wide association studies of relevantquantitative traits to help select candidategenes for analysis. In particular, assessmentof genes known to be involved in the deter-mination of normal central corneal thick-ness or corneal curvature could be relevantin keratoconus. Much progress has beenmade recently in the understanding of thegenetics of central corneal thickness96–98
in particular and this opens the way fordetailed analysis of such genes in kerato-conus cohorts. In the era of genomicsand international co-operation betweenresearch groups, the stage is set for a rapidexpansion of knowledge in the area of genet-ics keratoconus.
GRANTS AND FINANCIAL ASSISTANCEKPB is supported by a Career DevelopmentAward from the National Health andMedical Research Council of Australia.
REFERENCES1. Bareja U,Vajpayee RB. Posterior keratoconus due
to iron nail injury-a case report. Indian J Ophthalmol1991; 39: 30.
2. Brancati F, Valente EM, Sarkozy A, Feher J, CastoriM, Del Duca P, Mingarelli R et al. A locus forautosomal dominant keratoconus maps to humanchromosome 3p14–q13. J Med Genet 2004; 41: 188–192.
3. Gajecka M, Radhakrishna U, Winters D, Nath SK,Rydzanicz M, Ratnamala U, Ewing K et al. Locali-zation of a gene for keratoconus to a 5.6-Mb inter-val on 13q32. Invest Ophthalmol Vis Sci 2009; 50:1531–1539.
4. Rabinowitz YS, Garbus J, McDonnell PJ. Computer-assisted corneal topography in family members ofpatients with keratoconus. Arch Ophthalmol 1990;108: 365–371.
5. Grupcheva CN, Malik TY, Craig JP, Sherwin T,McGhee CN. Microstructural assessment of rarecorneal dystrophies using real time in vivo confocalmicroscopy. Clin Experiment Ophthalmol 2001; 29:281–285.
6. Jordan CA, Zamri A, Wheeldon C, Patel DV,Johnson R, McGhee CN. Computerized cornealtomography and associated features in a large NewZealand keratoconic population. J Cataract RefractSurg 2011; 37: 1493–1501.
7. Tuft SJ, Hassan H, George S, Frazer DG,Willoughby CE, Liskova P. Keratoconus in 18 pairsof twins. Acta Ophthalmol 2012; 90: e482–486.
8. Bechara SJ, Waring GO, 3rd, Insler MS. Kerato-conus in two pairs of identical twins. Cornea 1996;15: 90–93.
9. Redmond KB. The role of heredity in keratoconus.Trans Ophthalmol Soc Aust 1968; 27: 52–54.
10. Wang Y, Rabinowitz YS, Rotter JI, Yang H. Geneticepidemiological study of keratoconus: evidence formajor gene determination. Am J Med Genet 2000; 93:403–409.
11. Kennedy RH, Bourne WM, Dyer JA. A 48-year clini-cal and epidemiologic study of keratoconus. AmJ Ophthalmol 1986; 101: 267–273.
12. Rabinowitz YS. Keratoconus. Surv Ophthalmol 1998;42: 297–319.
13. Tyynismaa H, Sistonen P, Tuupanen S, Tervo T,Dammert A, Latvala T, Alitalo T. A locus for auto-somal dominant keratoconus: linkage to 16q22.3–q23.1 in Finnish families. Invest Ophthalmol Vis Sci2002; 43: 3160–3164.
14. Fullerton J, Paprocki P, Foote S, Mackey DA, Wil-liamson R, Forrest S. Identity-by-descent approachto gene localisation in eight individuals affected bykeratoconus from north-west Tasmania, Australia.Hum Genet 2002; 110: 462–470.
15. Ihalainen A. Clinical and epidemiological featuresof keratoconus genetic and external factors in thepathogenesis of the disease. Acta Ophthalmol 1986;Suppl 178: 1–64.
16. Kok YO, Tan GF, Loon SC. Review: keratoconus inAsia. Cornea 2012; 31: 581–593.
17. Nielsen K, Hjortdal J, Aagaard Nohr E, Ehlers N.Incidence and prevalence of keratoconus inDenmark. Acta ophthalmol Scand 2007; 85: 890–892.
18. Pearson AR, Soneji B, Sarvananthan N, Sandford-Smith JH. Does ethnic origin influence the inci-dence or severity of keratoconus? Eye (Lond) 2000;14: 625–628.
19. Owens H, Gamble GD, Bjornholdt MC, Boyce NK,Keung L. Topographic indications of emergingkeratoconus in teenage New Zealanders. Cornea2007; 26: 312–318.
20. Edwards M, McGhee CN, Dean S. The genetics ofkeratoconus. Clin Experiment Ophthalmol 2001; 29:345–351.
21. Patel HY, Ormonde S, Brookes NH, Moffatt LS,McGhee CN. The indications and outcome of pae-diatric corneal transplantation in New Zealand:1991–2003. Br J Ophthalmol 2005; 89: 404–408.
22. Williams KA, Lowe MT, Keane MC, Jones VJ, LohRS, Coster DJ. The Australian Corneal Graft Regis-try 2012 Report. Adelaide: Flinders Universtiy,2012.
23. Cameron JA. Corneal abnormalities in Ehlers-Danlos syndrome type VI. Cornea 1993; 12: 54–9.
24. Perlman JM, Zaidman GW. Bilateral kerato-conus in Crouzon’s syndrome. Cornea 1994; 13:80–81.
25. Bass HN, Sparkes RS, Crandall BF, Marcy SM. Con-genital contractural arachnodactyly, keratoconus,and probable Marfan syndrome in the same pedi-gree. J Pediatr 1981; 98: 591–593.
26. Heur M, Costin B, Crowe S, Grimm RA, Moran R,Svensson LG, Traboulsi EI. The value of keratom-etry and central corneal thickness measurements
in the clinical diagnosis of Marfan syndrome. Am JOphthalmol 2008; 145: 997–1001.
27. Maumenee IH. The eye in the Marfan syndrome.Trans Am Ophthalmol Soc 1981; 79: 684–733.
28. Sultan G, Baudouin C, Auzerie O, De Saint Jean M,Goldschild M, Pisella PJ. Cornea in Marfan disease:Orbscan and in vivo confocal microscopy analysis.Invest Ophthalmol Vis Sci 2002; 43: 1757–1764.
29. Hughes AE, Dash DP, Jackson AJ, Frazer DG, Sil-vestri G. Familial keratoconus with cataract: linkageto the long arm of chromosome 15 and exclusion ofcandidate genes. Invest Ophthalmol Vis Sci 2003; 44:5063–5066.
30. Harrison RJ, Klouda PT, Easty DL, Manku M,Charles J, Stewart CM. Association between kerato-conus and atopy. Br J Ophthalmol 1989; 73: 816–822.
31. Godel V, Blumenthal M, Iaina A. Congenital Leberamaurosis, keratoconus, and mental retardation infamilial juvenile nephronophtisis. J Pediatr Ophthal-mol Strabismus 1978; 15: 89–91.
32. Wilhelmus KR. Keratoconus and progressive conedystrophy. Ophthalmologica 1995; 209: 278–279.
33. Piccione M, Serra G, Sanfilippo C, Andreucci E,Sani I, Corsello G. A new mutation in EDA gene inX-linked hypohidrotic ectodermal dysplasia associ-ated with keratoconus. Minerva Pediatr 2012; 64:59–64.
34. Pinsard L, Touboul D, Vu Y, Lacombe D, Leger F,Colin J. Keratoconus associated with Williams-Beuren syndrome: first case reports. OphthalmicGenet 2010; 31: 252–256.
35. Gasset AR, Zimmerman TJ. Posterior polymor-phous dystrophy associated with keratoconus. Am JOphthalmol 1974; 78: 535–537.
36. Sassani JW, Smith SG, Rabinowitz YS. Keratoconusand bilateral lattice-granular corneal dystrophies.Cornea 1992; 11: 343–350.
37. Wollensak G, Green WR, Temprano J. Keratoconusassociated with corneal granular dystrophy ina patient of Italian origin. Cornea 2002; 21: 121–122.
38. Lipman RM, Rubenstein JB, Torczynski E. Kerato-conus and Fuchs’ corneal endothelial dystrophy ina patient and her family. Arch Ophthalmol 1990; 108:993–994.
39. Shapiro MB, France TD. The ocular features ofDown’s syndrome. Am J Ophthalmol 1985; 99: 659–663.
40. Macsai M, Maguen E, Nucci P. Keratoconus andTurner’s syndrome. Cornea 1997; 16: 534–536.
41. Heaven CJ, Lalloo F, McHale E. Keratoconus asso-ciated with chromosome 13 ring abnormality. Br JOphthalmol 2000; 84: 1079.
42. Morrison DA, Rosser EM, Claoue C. Keratoconusassociated with a chromosome 7,11 translocation.Eye (Lond) 2001; 15: 556–557.
43. Heon E, Greenberg A, Kopp KK, Rootman D,Vincent AL, Billingsley G, Priston M et al. VSX1:a gene for posterior polymorphous dystrophyand keratoconus. Hum Mol Genet 2002; 11: 1029–1036.
44. Muszynska D, Lechner J, Dash D, Heon E, HughesA, Willoughby C. Identification and characterisa-tion of a novel missense homeodomain mutation inZEB1 resulting in keratoconus. Invest OphthalmolVis Sci 2011; 52: 1077; abstract #149.
45. Udar N, Atilano SR, Brown DJ, Holguin B, Small K,Nesburn AB, Kenney MC. SOD1: a candidate genefor keratoconus. Invest Ophthalmol Vis Sci 2006; 47:3345–3351.
46. Guan T, Liu C, Ma Z, Ding S. The point mutationand polymorphism in keratoconus candidate gene
Genetics of keratoconus Burdon and Vincent
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
152 Clinical and Experimental Optometry © 2013 Optometrists Association Australia

TGFBI in Chinese population. Gene 2012; 503: 137–139.
47. Stabuc-Silih M, Ravnik-Glavac M, Glavac D,Hawlina M, Strazisar M. Polymorphisms inCOL4A3 and COL4A4 genes associated with kera-toconus. Mol Vis 2009; 15: 2848–2860.
48. Droitcourt C, Touboul D, Ged C, Ezzedine K,Cario-Andre M, de Verneuil H, Colin J et al. Aprospective study of filaggrin null mutations inkeratoconus patients with or without atopic disor-ders. Dermatology 2012; 222: 336–341.
49. Semina EV, Mintz-Hittner HA, Murray JC. Isolationand characterization of a novel human paired-likehomeodomain-containing transcription factorgene, VSX1, expressed in ocular tissues. Genomics2000; 63: 289–293.
50. Dash DP, George S, O’Prey D, Burns D, Nabili S,Donnelly U, Hughes AE et al. Mutational screeningof VSX1 in keratoconus patients from the Euro-pean population. Eye (Lond) 2010; 24: 1085–1092.
51. Hosseini SM, Herd S, Vincent AL, Heon E. Geneticanalysis of chromosome 20-related posterior poly-morphous corneal dystrophy: genetic heterogene-ity and exclusion of three candidate genes. Mol Vis2008; 14: 71–80.
52. Barbaro V, Di Iorio E, Ferrari S, Bisceglia L,Ruzza A, De Luca M, Pellegrini G. Expression ofVSX1 in human corneal keratocytes during differ-entiation into myofibroblasts in response to woundhealing. Invest Ophthalmol Vis Sci 2006; 47: 5243–5250.
53. Mintz-Hittner HA, Semina EV, Frishman LJ, PragerTC, Murray JC. VSX1 (RINX) mutation withcraniofacial anomalies, empty sella, cornealendothelial changes, and abnormal retinal andauditory bipolar cells. Ophthalmology 2004; 111:828–836.
54. Bisceglia L, Ciaschetti M, De Bonis P, Campo PA,Pizzicoli C, Scala C, Grifa M et al. VSX1 mutationalanalysis in a series of Italian patients affected bykeratoconus: detection of a novel mutation. InvestOphthalmol Vis Sci 2005; 46: 39–45.
55. Eran P, Almogit A, David Z, Wolf HR, Hana G, YanivB, Elon P et al. The D144E substitution in the VSX1gene: a non-pathogenic variant or a disease causingmutation? Ophthalmic Genet 2008; 29: 53–59.
56. Mok JW, Baek SJ, Joo CK. VSX1 gene variants areassociated with keratoconus in unrelated Koreanpatients. J Hum Genet 2008; 53: 842–849.
57. Paliwal P, Singh A, Tandon R, Titiyal JS, Sharma A.A novel VSX1 mutation identified in an individualwith keratoconus in India. Mol Vis 2009; 15: 2475–2479.
58. Aldave AJ, Yellore VS, Salem AK, Yoo GL, RaynerSA, Yang H, Tang GY et al. No VSX1 gene muta-tions associated with keratoconus. Invest OphthalmolVis Sci 2006; 47: 2820–2822.
59. Liskova P, Ebenezer ND, Hysi PG, Gwilliam R,El-Ashry MF, Moodaley LC, Hau S et al. Molecularanalysis of the VSX1 gene in familial keratoconus.Mol Vis 2007; 13: 1887–1891.
60. Stabuc-Silih M, Strazisar M, Hawlina M, Glavac D.Absence of pathogenic mutations in VSX1 andSOD1 genes in patients with keratoconus. Cornea2010; 29: 172–176.
61. Tang YG, Picornell Y, Su X, Li X, Yang H, Rabinow-itz YS. Three VSX1 gene mutations, L159M,R166W, and H244R, are not associated with kera-toconus. Cornea 2008; 27: 189–192.
62. McGhee CN. 2008 Sir Norman McAlister GreggLecture: 150 years of practical observations on the
conical cornea–what have we learned? Clin Experi-ment Ophthalmol 2009; 37: 160–176.
63. De Bonis P, Laborante A, Pizzicoli C, Stallone R,Barbano R, Longo C, Mazzilli E et al. Mutationalscreening of VSX1, SPARC, SOD1, LOX, andTIMP3 in keratoconus. Mol Vis 2011; 17: 2482–2894.
64. Saee-Rad S, Hashemi H, Miraftab M, Noori-DaloiiMR, Chaleshtori MH, Raoofian R, Jafari F et al.Mutation analysis of VSX1 and SOD1 in Iranianpatients with keratoconus. Mol Vis 2011; 17: 3128–3136.
65. Paliwal P, Tandon R, Dube D, Kaur P, Sharma A.Familial segregation of a VSX1 mutation adds anew dimension to its role in the causation of kera-toconus. Mol Vis 2011; 17: 481–485.
66. Blair SD, Seabrooks D, Shields WJ, Pillai S,Cavanagh HD. Bilateral progressive essential irisatrophy and keratoconus with coincident featuresof posterior polymorphous dystrophy: a case reportand proposed pathogenesis. Cornea 1992; 11: 255–261.
67. Cremona FA, Ghosheh FR, Rapuano CJ, Eagle RCJr., Hammersmith KM, Laibson PR, Ayres BD et al.Keratoconus associated with other corneal dystro-phies. Cornea 2009; 28: 127–135.
68. Lam HY, Wiggs JL, Jurkunas UV. Unusual presen-tation of presumed posterior polymorphous dys-trophy associated with iris heterochromia, bandkeratopathy and keratoconus. Cornea 2010; 29:1180–1185.
69. Mazzotta C, Baiocchi S, Caporossi O, Buccoliero D,Casprini F, Caporossi A, Balestrazzi A. Confocalmicroscopy identification of keratoconus associ-ated with posterior polymorphous corneal dystro-phy. J Cataract Refract Surg 2008; 34: 318–321.
70. Weissman BA, Ehrlich M, Levenson JE, Pettit TH.Four cases of keratoconus and posterior polymor-phous corneal dystrophy. Optom Vis Sci 1989; 66:243–246.
71. Bechara SJ, Grossniklaus HE, Waring GO, 3rd,Wells JA, 3rd. Keratoconus associated with poste-rior polymorphous dystrophy. Am J Ophthalmol1991; 112: 729–731.
72. Raber IM, Fintelmann R, Chhabra S, RibeiroMP, Eagle RC Jr, Orlin SE. Posterior polymorphousdystrophy associated with nonkeratoconic steepcorneal curvatures. Cornea 2011; 30: 1120–1124.
73. Liskova P, Filipec M, Merjava S, Jirsova K, Tuft SJ.Variable ocular phenotypes of posterior polymor-phous corneal dystrophy caused by mutationsin the ZEB1 gene. Ophthalmic Genet 2010; 31: 230–234.
74. Pathak D, Nayak B, Singh M, Sharma N, Tandon R,Sinha R, Titiyal JS et al. Mitochondrial complex 1gene analysis in keratoconus. Mol Vis 2011; 17:1514–1525.
75. Munier FL, Frueh BE, Othenin-Girard P, Uffer S,Cousin P, Wang MX, Heon E et al. BIGH3 muta-tion spectrum in corneal dystrophies. Invest Oph-thalmol Vis Sci 2002; 43: 949–954.
76. Karolak JA, Kulinska K, Nowak DM, Pitarque JA,Molinari A, Rydzanicz M, Bejjani BA et al.Sequence variants in COL4A1 and COL4A2 genesin Ecuadorian families with keratoconus. Mol Vis2011; 17: 827–843.
77. Aldave AJ, Bourla N, Yellore VS, Rayner SA, KhanMA, Salem AK, Sonmez B. Keratoconus is not asso-ciated with mutations in COL8A1 and COL8A2.Cornea 2007; 26: 963–965.
78. Hughes AE, Bradley DT, Campbell M, Lechner J,Dash DP, Simpson DA, Willoughby CE. Mutation
altering the miR-184 seed region causes familialkeratoconus with cataract. Am J Hum Genet 2011; 89:628–633.
79. Czugala M, Karolak JA, Nowak DM, Polakowski P,Pitarque J, Molinari A, Rydzanicz M et al. Novelmutation and three other sequence variants segre-gating with phenotype at keratoconus 13q32 sus-ceptibility locus. Eur J Hum Genet 2012; 20: 389–397.
80. Tang YG, Rabinowitz YS, Taylor KD, Li X, Hu M,Picornell Y, Yang H. Genomewide linkage scan in amultigeneration Caucasian pedigree identifies anovel locus for keratoconus on chromosome5q14.3–q21.1. Genet Med 2005; 7: 397–405.
81. Burdon KP, Coster DJ, Charlesworth JC, Mills RA,Laurie KJ, Giunta C, Hewitt AW et al. Apparentautosomal dominant keratoconus in a large Aus-tralian pedigree accounted for by digenic inherit-ance of two novel loci. Hum Genet 2008; 124: 379–386.
82. Hutchings H, Ginisty H, Le Gallo M, Levy D,Stoesser F, Rouland JF, Arne JL et al. Identificationof a new locus for isolated familial keratoconus at2p24. J Med Genet 2005; 42: 88–94.
83. Li X, Rabinowitz YS, Tang YG, Picornell Y, TaylorKD, Hu M, Yang H. Two-stage genome-wide linkagescan in keratoconus sib pair families. Invest Ophthal-mol Vis Sci 2006; 47: 3791–3795.
84. Bisceglia L, De Bonis P, Pizzicoli C, Fischetti L,Laborante A, Di Perna M, Giuliani F et al. Linkageanalysis in keratoconus: replication of locus 5q21.2and identification of other suggestive Loci. InvestOphthalmol Vis Sci 2009; 50: 1081–1086.
85. Liskova P, Hysi PG, Waseem N, Ebenezer ND, Bhat-tacharya SS, Tuft SJ. Evidence for keratoconus sus-ceptibility locus on chromosome 14: a genome-wide linkage screen using single-nucleotidepolymorphism markers. Arch Ophthalmol 2010; 128:1191–1195.
86. Burdon KP, Macgregor S, Bykhovskaya Y, JavadiyanS, Li X, Laurie KJ, Muszynska D et al. Association ofpolymorphisms in the hepatocyte growth factorgene promoter with keratoconus. Invest OphthalmolVis Sci 2011; 52: 8514–8519.
87. Li X, Bykhovskaya Y, Haritunians T, Siscovick D,Aldave A, Szczotka-Flynn L, Iyengar SK et al. Agenome-wide association study identifies a poten-tial novel gene locus for keratoconus, one of thecommonest causes for corneal transplantation indeveloped countries. Hum Mol Genet 2012; 21: 421–429.
88. Abu-Amero KK, Hellani AM, Al Mansouri SM,Kalantan H, Al-Muammar AM. High-resolutionanalysis of DNA copy number alterations inpatients with isolated sporadic keratoconus. Mol Vis2011; 17: 822–826.
89. Dash DP, Silvestri G, Hughes AE. Fine mapping ofthe keratoconus with cataract locus on chromo-some 15q and candidate gene analysis. Mol Vis2006; 12: 499–505.
90. Iliff BW, Riazuddin SA, Gottsch JD. A single-basesubstitution in the seed region of miR-184 causesEDICT syndrome. Invest Ophthalmol Vis Sci 2012; 53:348–353.
91. Adzhubei IA, Schmidt S, Peshkin L, RamenskyVE, Gerasimova A, Bork P, Kondrashov AS et al.A method and server for predicting damagingmissense mutations. Nat Methods 2010; 7: 248–249.
92. Veerappan S, Pertile KK, Islam AF, Schache M,Chen CY, Mitchell P, Dirani M et al. Role of thehepatocyte growth factor gene in refractive error.Ophthalmology 2010; 117: 239–245.
Genetics of keratoconus Burdon and Vincent
© 2013 The Authors Clinical and Experimental Optometry 96.2 March 2013
Clinical and Experimental Optometry © 2013 Optometrists Association Australia 153

93. Yanovitch T, Li YJ, Metlapally R, Abbott D, Viet KN,Young TL. Hepatocyte growth factor and myopia:genetic association analyses in a Caucasian popula-tion. Mol Vis 2009; 15: 1028–1035.
94. Suri K, Hammersmith KM, Nagra PK. Corneal col-lagen cross-linking: ectasia and beyond. Curr OpinOphthalmol 2012; 23: 280–287.
95. Bykhovskaya Y, Li X, Epifantseva I, Haritunians T,Siscovick D, Aldave A, Szczotka-Flynn L et al. Vari-ation in the lysyl oxidase (LOX) gene is associatedwith keratoconus in family-based and case-controlstudies. Invest Ophthalmol Vis Sci 2012; 53: 4152–4157.
96. Lu Y, Dimasi DP, Hysi PG, Hewitt AW, BurdonKP, Toh T, Ruddle JB et al. Common genetic vari-ants near the Brittle Cornea syndrome locusZNF469 influence the blinding disease risk factorcentral corneal thickness. PLoS Genet 2010; 6:e1000947.
97. Vitart V, Bencic G, Hayward C, Skunca Herman J,Huffman J, Campbell S, Bucan K et al. New lociassociated with central cornea thickness includeCOL5A1, AKAP13 and AVGR8. Hum Mol Genet2010; 19: 4304–4311.
98. Vithana EN, Aung T, Khor CC, Cornes BK, Tay WT,Sim X, Lavanya R et al. Collagen-related genesinfluence the glaucoma risk factor, central cornealthickness. Hum Mo Genet 2011; 20: 649–658.
Genetics of keratoconus Burdon and Vincent
Clinical and Experimental Optometry 96.2 March 2013 © 2013 The Authors
154 Clinical and Experimental Optometry © 2013 Optometrists Association Australia