Embed Size (px)
Citation preview
A Publication of Correct Rx Pharmacy Services, Inc. Volume 2 • Issue 2 • 2008
DOSEC
over
art
by M
att C
hapm
an INSIDEremote physician order entry
alcohol withdrawal syndrome
Correct Rx 3
8 Drugs and the Elderly
12 Alcohol Withdrawal Syndrome
17 Treatment of Tardive Dyskinesia
6 Safe Medication Practices
Contents
Tardive dyskinesia (TD) is a neurological syndromethat is not well understood. TD is severely debilitat-ing and often warrants the discontinuation of neu-roleptic treatment that have provided control of psy-chotic symptoms. Management of TD is especiallychallenging in schizophrenic patients who have founda neuroleptic that offers control for their psychoticsymptoms after a potentially long process of trial anderror with very few alternatives remaining.
The presentation of TD symptoms is highly stigmatizing and hassocial implications for patients treated with antipsychotic medica-tion. The classic description of TD is the Buccal-Lingual-Masticatory Syndrome, or oral-facial movements. The firstdetectable signs may be a slight back and forward movement of thetongue, then progression to a more pronounced thrusting or rollingof the tongue with or without chewing or lateral jaw movements.
TreatmentDyskinesia
by Hui W. Seo,Pharm.D.
800.636.0501 . 803-A Barkwood Court . Linthicum, MD 21090 . www.correctrxpharmacy.com . [email protected]: Helena H. Kim, Pharm.D.Cover Illustrator: Matt Chapman
Dose is published by Innovative Publishing Ink. For more information on how your company can have its own publication, contact Aran Jackson at 502.423.7272.
Innovative Publishing Ink • 10629 Henning Way, Suite 8 • Louisville, KY 40241 • 502.423.7272 • www.ipipublishing.com
Correct Rx Pharmacy Services, Inc. is neither accountable for the content of paid advertisements nor does it endorse same. No outside parties influenced the text or participated in the editing of this publication. Professional standards of carewere taken to ensure accuracy; however, the authors and editors do not attest that the information contained herein is free of errors or omissions. Sound clinical judgment is the responsibility of every professional in addition to full consultationof all prescribing information prior to medication administration.
Other Features
15 Greetings from the President
10 Medical Waste
21 Bridging the Gap:Opioid TreatmentProgram in Corrections
4 Correct Rx
Greetings from the President
Each edition of Dose begins with the “Greetings from the President.”This is a great avenue for me to update our friends, associates andclients on the most recent Correct Rx news. It also provides a forumfor me, as the president, to share my ideas and opinions on topicsthat are of particular importance to Correct Rx. It is often an insight intomy vision for the future of pharmacy, as it affects the patients we serve.
In this edition, I need enough space for two letters, as there is suffi-cient news to fill up an entire letter just on the happenings at CorrectRx, yet I feel compelled to also address the topic depicted by our coverart and heading, Collaboration the “Correct Way.” Therefore, I willtry to do both, starting with Correct Rx updates and closing with acommentary on Pharmacist-Directed Patient Care.
The News at Correct Rx Is Very ExcitingWeddings, New Babies and EngagementsThere is something about a wedding that puts everyonein a good mood, so we should be giddy with happiness aswe announce the weddings of several of our key staffmembers. John Nattans, our Director of ProgramServices and Quality Assurance, will be getting marriedon November 15, and Dr. Akilah Streets had a destina-tion wedding September 25. And lastly, I am getting mar-ried. Yes, you read correctly — Ellen Yankellow is gettingmarried, too! If I have seemed a little distracted or busierthan usual, this should provide a little insight into my world these days.In addition, Martin Yankellow and his wife, Irene, are expecting BabyYankellow in November, while Dr. Sankung Sise had a little boy in July.Lastly, Dr. Helena Kim returned from the Olympics engaged.
We have a lot of wonderful events to celebrate, and I know you willjoin me in congratulating our team as you speak to them during thenext few months.
Board Appointments and HonorsI have recently been asked to chair the University of MarylandSchool of Pharmacy’s Board of Visitors. This is a tremendous honorand will allow Correct Rx to work closely with Dean Eddington asshe forges her vision for the School of Pharmacy. In addition, I wasselected to join the boards of the Baltimore City Foundation, theGirl Scouts of Central Maryland, JJ Haines and the CharlestownRetirement Community. These are all wonderful organizations, andI am looking forward to a great year!!
Chimes, an international multiservice agency delivering a wide rangeof programs, services and support to people with disabilities, hasselected me as its 2008 Hall of Fame honoree. I will be sharing theevening with none other than Bernadette Peters!
Fax Server, Software Upgrades, Electronic Medical Record Interface andExpanded Network CapabilitiesCorrect Rx has been very busy and continues to invest in upgradesto our systems and technology capabilities. We are installing a state-of-the-art fax server that will automatically verify orders and providean electronic image of all transmissions. Also, we have installed thenewest version of our senior care and correctional software. We havesuccessfully provided an interface with our largest skilled nursingfacility and are about to implement an electronic order entry systemat one of our jail sites. More to come, as we seem to have new devel-opments on a daily basis!
Now that I have shared the news at Correct Rx, Iwould like to focus the remaining portion of my let-ter addressing the subject of Pharmacist-DirectedPatient Care with an emphasis on collaboration.This initiative, I strongly believe, significantly dif-ferentiates Correct Rx!
First, there is no question that multiple studies andclinical initiatives, including our own, have proven thatpatient-centered pharmacy provides real value to thepatient, the client and the greater public; but how doyou go about measuring and quantifying that value?
The traditional singular focus on drug acquisition costignores the potentially important issues of quality of
outcome and the even greater cost savings to overall health carebudgets. We must accurately measure such outcomes and attach rel-ative values to them so that decision-makers may fully understandthe costs and consequences of allocation decisions. Institutionalpharmacy provides an excellent environment for medical and men-tal health providers to work collaboratively with clinical pharma-cists. Correct Rx has found that practitioners, who are open todeveloping working relationships, have respect and appreciationfor the pharmacist’s contribution, responsibility and knowledge.Correct Rx is proud of our role in improving patient health carethrough the implementation of patient-centered pharmacy, utiliz-ing a collaborative model where pharmacy, medical and mentalhealth practitioners all work together for the greater good of thepatient. This is wonderful news for Pharmacist-Directed PatientCare and the patients we serve. We call it Collaboration the“Correct Way!”
Ellen H. Yankellow, Pharm.D.President and CEO
Ellen H. Yankellow , Pharm.D.
Correct Rx 5
News, Notes and Collaboration
6 Correct Rx
While there have been heated discussions inthe medical community pertaining to the useof remote physician order entry systems(RPOES) for many years now, its adoption bycommunity practitioners and small medicalunits has been slow. This is due in large part tothe fact that current systems, albeit dated,allow for the processing of pharmacy orders.The downside of the current systems availableis the increased probability of transcriptionerrors and misinterpretation of illegible orders.
With only a few options to transmit orders to the pharmacy, addition-al avenues are always welcome. Today, new prescription orders must befaxed to the pharmacy. While this is a proven system, it has severaldrawbacks. Fax-machine malfunction, presenting in many ways, is acommon source of frustration. Missing or illegible pages require addi-tional time at both the facility and the pharmacy to verify the receiptof faxes. Similarly, refills face the same type of limitations, althoughrefill orders can also be sent using our advanced barcode reorder sys-tem. Ordering refills using the barcode system eliminates the problemsabove, but it does not address the issue on initial ordering.
The main goal of RPOES is to reduce medication errors, therebydecreasing the numbers of adverse events related to these errors. Whilethese systems, if implemented properly, have many benefits, there needsto be careful design and deployment to obtain the desired outputs.
The successful deployment of RPOES positively affects the followingchanges within the medication procurement process:• Medication orders are entered electronically• Medication information is available online in one location in the
electronic chart
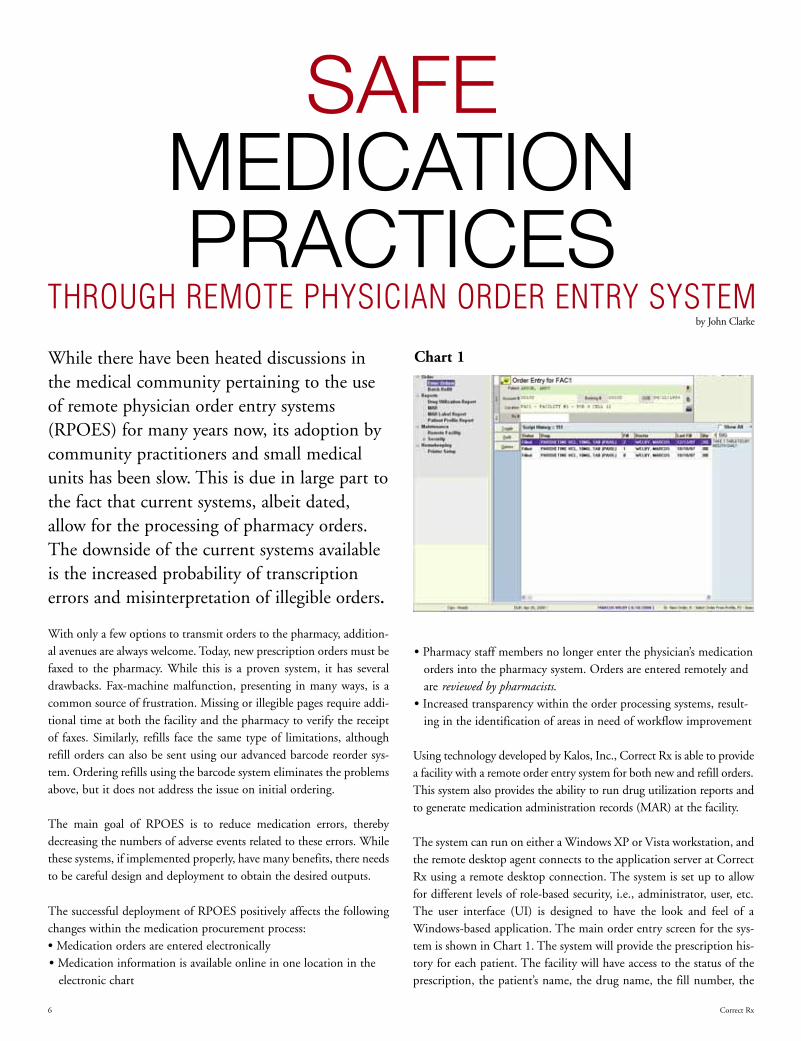
Chart 1
• Pharmacy staff members no longer enter the physician’s medicationorders into the pharmacy system. Orders are entered remotely andare reviewed by pharmacists.
• Increased transparency within the order processing systems, result-ing in the identification of areas in need of workflow improvement
Using technology developed by Kalos, Inc., Correct Rx is able to providea facility with a remote order entry system for both new and refill orders.This system also provides the ability to run drug utilization reports andto generate medication administration records (MAR) at the facility.
The system can run on either a Windows XP or Vista workstation, andthe remote desktop agent connects to the application server at CorrectRx using a remote desktop connection. The system is set up to allowfor different levels of role-based security, i.e., administrator, user, etc.The user interface (UI) is designed to have the look and feel of aWindows-based application. The main order entry screen for the sys-tem is shown in Chart 1. The system will provide the prescription his-tory for each patient. The facility will have access to the status of theprescription, the patient’s name, the drug name, the fill number, the
SAFEMEDICATIONPRACTICES
THROUGH REMOTE PHYSICIAN ORDER ENTRY SYSTEMby John Clarke
doctor, the last fill, quantity, directions, start and stop dates, the facil-ity of patient at the time of fill and the prescription number.
The system displays information in a tree format and is divided intofour main function categories: Orders, Reports, Maintenance andHousekeeping. The physician is connected directly to the patient pro-file. As the physician enters orders, the system will check the patientprofile for known drug allergies and drug interactions. The system alsohas the ability to check the order against the formulary — if one isentered. The physician also has the option to enter patient notes; thesenotes automatically display whenever the patient is selected.
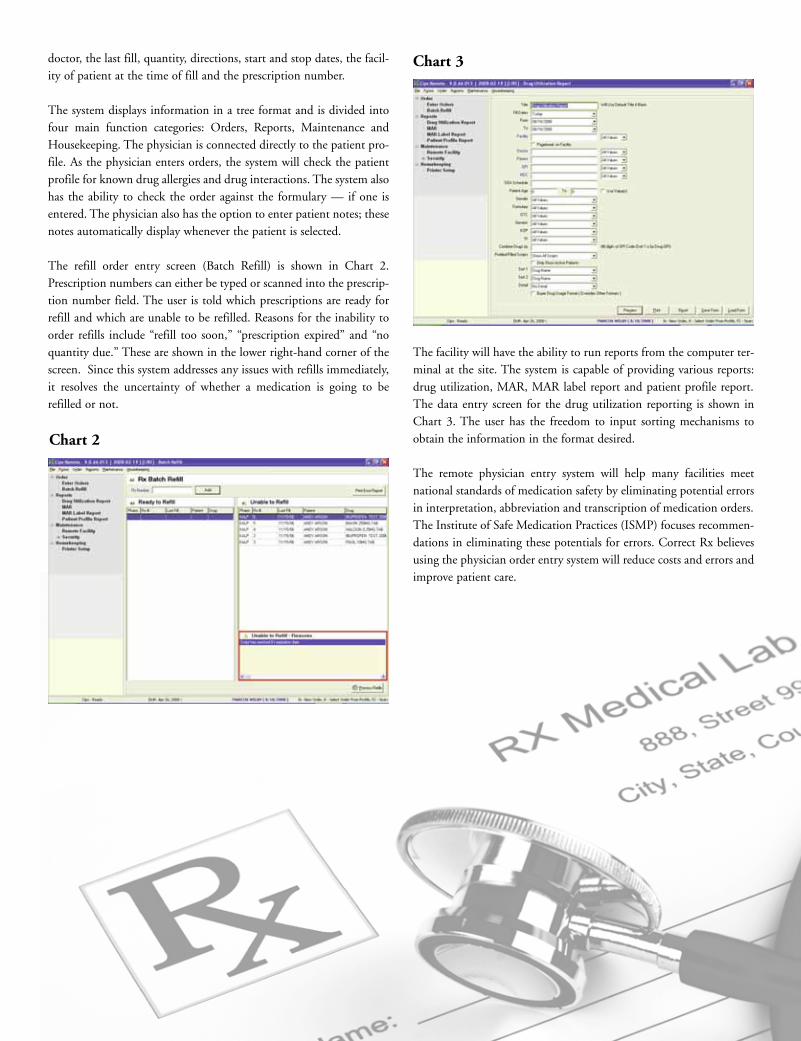
The refill order entry screen (Batch Refill) is shown in Chart 2.Prescription numbers can either be typed or scanned into the prescrip-tion number field. The user is told which prescriptions are ready forrefill and which are unable to be refilled. Reasons for the inability toorder refills include “refill too soon,” “prescription expired” and “noquantity due.” These are shown in the lower right-hand corner of thescreen. Since this system addresses any issues with refills immediately,it resolves the uncertainty of whether a medication is going to berefilled or not.
The facility will have the ability to run reports from the computer ter-minal at the site. The system is capable of providing various reports:drug utilization, MAR, MAR label report and patient profile report.The data entry screen for the drug utilization reporting is shown inChart 3. The user has the freedom to input sorting mechanisms toobtain the information in the format desired.
The remote physician entry system will help many facilities meetnational standards of medication safety by eliminating potential errorsin interpretation, abbreviation and transcription of medication orders.The Institute of Safe Medication Practices (ISMP) focuses recommen-dations in eliminating these potentials for errors. Correct Rx believesusing the physician order entry system will reduce costs and errors andimprove patient care.
Chart 2
Chart 3
8 Correct Rx
Falls can be markers of poor health and
declining function. Those who fall experi-
ence greater functional declines in activi-
ties of daily living (ADLs) and in physical
and social activities compared to those
who do not fall. Major injuries, including
head trauma, soft tissue injuries, fractures
and dislocations, occur in 5 to 15 percent
of falls. Fractures account for 75 percent
of serious injuries, with hip fractures
occurring in 1 to 2 percent of falls. More
than 90 percent of hip fractures occur as a
result of falls, with most of these fractures
occurring in persons over 70 years of age.
Hospital stays are almost twice as long for
elderly patients who are hospitalized for a
fall than for elderly patients who are
admitted for other reasons.
In older patients, a fall may be a nonspe-
cific presenting sign of acute illnesses,
such as pneumonia, urinary tract infection
or myocardial infarction. It may also be a
sign of acute exacerbation of a chronic dis-
ease. Table 1 lists risk factors associated
with falls in the elderly.
While the use of a particular drug or drug
class can be an independent risk factor for
falls, other parameters relating to drug use
can increase the risk even further. Both
dose and time since initiating a medica-
tion have been reported to impact the risk
Drugs and the Elderly
by Akilah Streets,Pharm.D.

Correct Rx 9
Table 3: Physical Examination Findings
Inflammation of joints
Hypotension (orthostatic blood pressure changes)
Auditory and visual changes
Tremor (Parkinson’s disease)
Equilibrium disturbances
Foot problems
Arrhythmias
Generalized weakness
Nutrition deficiencies
Gait disturbances
Table 1: Risk Factors Associated with Falls in the Elderly
Demographic FactorsOlder age (especially �75 years), white race, housebound,
living alone
Associated History Use of cane or walker, previous falls, acute illness
Physical BarriersCognitive impairment, reduced vision, foot problems,
hearing impairment
Other Environmental hazards, polypharmacy
Table 2: Common Causes of Falls in the Elderly
Cause Medication(s)
Cognitive impairment, confusionBenzodiazepines, narcotics, neuroleptics, drugs with
anticholinergic effect
Dizziness; orthostatic hypotension Anticonvulsants, antidepressants, antihypertensives
Gait abnormalities Antidepressants, metoclopramide
Increased ambulation Diuretics
Postural disturbances Anticonvulsants, neuroleptics, benzodiazepines
Sedation/drowsiness Anticonvulsants, narcotics, antidepressants, neuroleptics
Syncope Beta-blockers, nitrates, vasodilators
Visual disturbances Neuroleptics
of falls. Taking a greater number of prescrip-
tion medications, regardless of pharmacologic
classification, has also been associated with
increased risk for falls. Table 2 lists common
causes of falls associated with medications.
EvaluationWhen evaluating a patient who has fallen, it is
important to take a focused history with an
emphasis on medications. A directed physical
examination and simple tests of postural con-
trol and overall physical function are also nec-
essary. An evaluation for treatable causes
should be done if an elderly patient falls more
than twice in a six-month period. A thorough
history is essential to determine the mechanism
of falling, specific risk factors for falls, impair-
ments that contribute to falls and the appropri-
ate diagnostic workup. Table 3 lists key
physical findings that health care
providers should pay particular close
attention to.
Prevention/ManagementAccording to the CDC falls prevention
program, patients are encouraged to
follow four key components. (1)
Exercise: maintaining strength and
flexibility is the best way to mini-
mize the risk of falls. Exercise will
improve balance and coordination.
( 2 ) Safeguard your home: reduce clut-
ter and keep pathways open. Use only
throw rugs with rubber or non-skid
backing. (3) Have your vision checked:
See an eye doctor on an annual basis.
Vision loss is often gradual and can go
unnoticed. (4) Have a health care
provider review your medication.
Tips for PharmacistsPharmacists should periodically review
medication regimens of fall patients or
patients at a significant risk of falling.
Red flags are polypharmacy (four or
more prescription medications), the
initiation of a new drug therapy in the
previous two weeks or the use of any
drugs listed in Table 2. If possible, such
medications should be avoided where
not clinically essential. When therapy
with an agent that may increase risk for
falls is required, starting with “geriatric
doses” (typically from one-fourth to
one-half the normal adult dose) and
titrating slowly with close monitoring
can help minimize risk.
Approximately 5,000 tons of pharmaceuti-cals and related personal products are dis-carded annually. The general public tendsto discard prescription drugs that are nolonger being used more than 50 percent ofthe time in the trash; about 30 percent ofthe public will flush their medications inthe toilet. Trace amounts of medicationsdisposed through the sewer system mayadversely impact our environment and ourdrinking water supply.
Keeping medications in the home beyondthe time that they are needed by the personfor whom they were prescribed is an unsafemedication practice. It creates a potentialfor medication misuse and abuse. Patientswho require multiple medications forhealth maintenance oftentimes have theirmedication regimens changed. Patients maybecome confused about which medicationsthey should take. Removing these medica-tions in a timely fashion would help todeter adverse medication events. In addi-tion, prescription medication abuse hasincreased during the past decade, and it isthe most commonly abused substanceamong adolescents. They also present anadditional hazard for even younger chil-dren. Children under 12 years of age havemade prescription drugs the third leadingcause of poisoning, following cosmetics andhousehold cleaners.
The federal government does not provide aclear guideline for the disposal of unused or
unwanted medications. In contrast, medicalwaste is heavily regulated and the disposalmethods are very costly. The Medical WasteTracking Act of 1988 defines medical wasteas “any solid waste that is generated in thediagnosis, treatment, or immunization ofhuman beings or animals, in research per-taining thereto, or in the production ortesting of biologicals.” This definitionincludes but is not limited to the following:• Blood-soaked bandages• Culture dishes and other glassware• Discarded surgical gloves• Discarded surgical instruments• Discarded needles and other
medical sharps• Swabs used to inoculate cultures• Removed body organs• Discarded lancets
Medical waste from health care and medicalfacilities falls into four general categories:infectious, hazardous, radioactive and gen-eral waste. The U.S. EnvironmentalProtection Agency (EPA) estimates that 10to 15 percent of medical waste could beclassified as infectious. The remaining 85 to90 percent is very similar to wastes generat-ed in households and offices.
Investigations by the Associated Press haverevealed that there is a vast array of pharma-ceuticals, including antibiotics, anticonvul-sants, mood stablilizers and sex hormonesthat have been found in the drinking watersupplies of at least 41 million Americans. It
was discovered that drugs have been detect-ed in the drinking water supplies of 24major metropolitan areas. Medications dis-posed of by the public through their bodywaste and disposing of excess medicationvia the toilet or sink drain are passed ontothe wastewater treatment plant. The wateris treated before being discharged intoreservoirs, rivers or lakes. This same water isthen cleansed again at drinking water treat-ment plants and piped back to consumers,but most treatment plants do not remove allof the drug residue.
Most people, when interviewed, thoughtthat it was acceptable to either flushunwanted medications down the toilet orwash them down the sink drain. The extentof the problem is further exemplified by a2002 study in which 80 percent of 139streams tested were positive for pharmaceu-ticals and other common household products. The concentrations of these phar-maceuticals are small, measuring in theparts per billion or trillion, far below amedical dose. The federal government doesnot require any testing and has not set safe-ty limits for drugs in water.
Consumers who use well water, bottledwater or home filtration systems are not freefrom exposure. Vendors of bottled waterand home filtration systems do not testtheir final product for pharmaceuticals. Theproblem is so widespread that areasthroughout the world have also found phar-
Medical W
10 Correct Rx

maceuticals in their water. Forty percent ofthe nation’s water supply comes fromaquifers. These too have been permeatedwith pharmaceuticals. Federal scientists,who drew water in 24 states from aquifersnear contaminant sources, such as landfillsand animal feed lots, found minuscule levelsof hormones, antibiotics and other drugs.“We recognize it is a growing concern, andwe’re taking it very seriously,” saidBenjamin H. Grumbles, assistant adminis-trator for water at the EPA. He alsoacknowledged that the EPA developed threenew methods to detect and quantify med-ications in wastewater.
The pharmaceuticals that are being detectedin the environment, even though they are inlow concentrations, could, over time, beproblematic to human health or to aquaticanimals. Recent research has found thatsmall amounts of medication have affectedhuman embryonic kidney cells, humanblood cells and human breast cancer cells.The cancer cells proliferated more quickly,the kidney cells grew more slowly, and theblood cells showed biological activity associ-ated with inflammation. Research alsoshows that male fish are feminized by estro-gen, creating egg yolk proteins, a processusually restricted to females. Pharm-aceuticals are also affecting sentinel speciesat the foundation of the pyramid of life, i.e.,earthworms in the wild and zooplankton inthe laboratory. The experiments have thusfar been limited, and there are many
unknowns, but the documented healthproblems in wildlife are disconcerting.
Many states prohibit the return of unusedmedications to pharmacies. In addition, theControlled Substance Act (CSA) prohibitsthe return of controlled substances andstates that only law enforcement personnelmay receive controlled substances fromhousehold consumers. This also includesnursing homes. The CSA also states that forpharmacists or pharmacies to acceptreturned medications, they must verify thereare no scheduled substances in the returns.A reverse distributor may not accept med-ications from patients, as this is consideredhousehold waste, which their license doesnot cover.
Hospitals and other health care facilitiesmainly contract with companies that arelicensed to pick up and then dispose ofmedical waste by incineration. There arestill some hospitals that own their own med-ical waste-incinerator, but with the strictemission regulations of the EPA, whichmake it very expensive to run such an incin-erator, more of these hospitals are turning tothe medical-waste-disposal contractors forwaste removal.
Consumers have limited options and shouldcontact their local solid-waste-disposalagency for the local regulations. Some coun-ties run a household hazardous waste dump;however, some of these county waste dumps
may not accept pharmaceuticals if they lackthe training or necessary security to handlethem. Law enforcement can legally acceptthe medications but may not have the man-power or the space for storage. Some locali-ties suggest that the unwanted items bemixed with garbage that would make themedication less appealing to abusers. Inaddition, coffee grounds and used kitty litter have been suggested. Wetting the medication with enough water to cause dis-integration before adding to the garbage hasalso been suggested. Even though thiswould end up in a land fill and subsequent-ly the aquifer, it is preferable to adding themedicines directly into the sewage system.
To keep unwanted medications and otherchemicals out of the water supply, the rec-ommendation is that the waste be incinerat-ed by a company licensed for destruction ofbiomedical waste. There have been localefforts to do this by creating community-run collection sites with proper law enforce-ment present. It seems that EPA regulationwould be needed to address environmentalissues on how medications should be dis-posed and how to monitor the removal ofharmful chemicals in our processed sewage.
aste by Barry Hommerbocker
References:1) EPA Web site: http://www.epa.gov/.2) Prescription Drugs Found In Drinking Water Across U.S., AP National Investigative Team, http://cnn.com.3) The Collection and Disposal of Waste Medications, U.S. Pharmacist, Vol. No. 33:6.
Alcohol WithdrawalSyndrome
by Sankung Sise,Pharm.D.
Alcoholism is thought to be a chronic disease of unknown etiology. About 70percent of the population consumes alcohol in one form or the other; however,only 10 percent are reported to be alcoholics. Consumption of large amounts ofethanol (alcohol) may cause significant clinical toxicity and lead to tissue dam-age. Patients can also develop a physical dependence, thereby resulting in apotentially dangerous withdrawal syndrome. Alcoholism also leads to socialimpairment in the lives of alcoholics and their loved ones.
12 Correct Rx
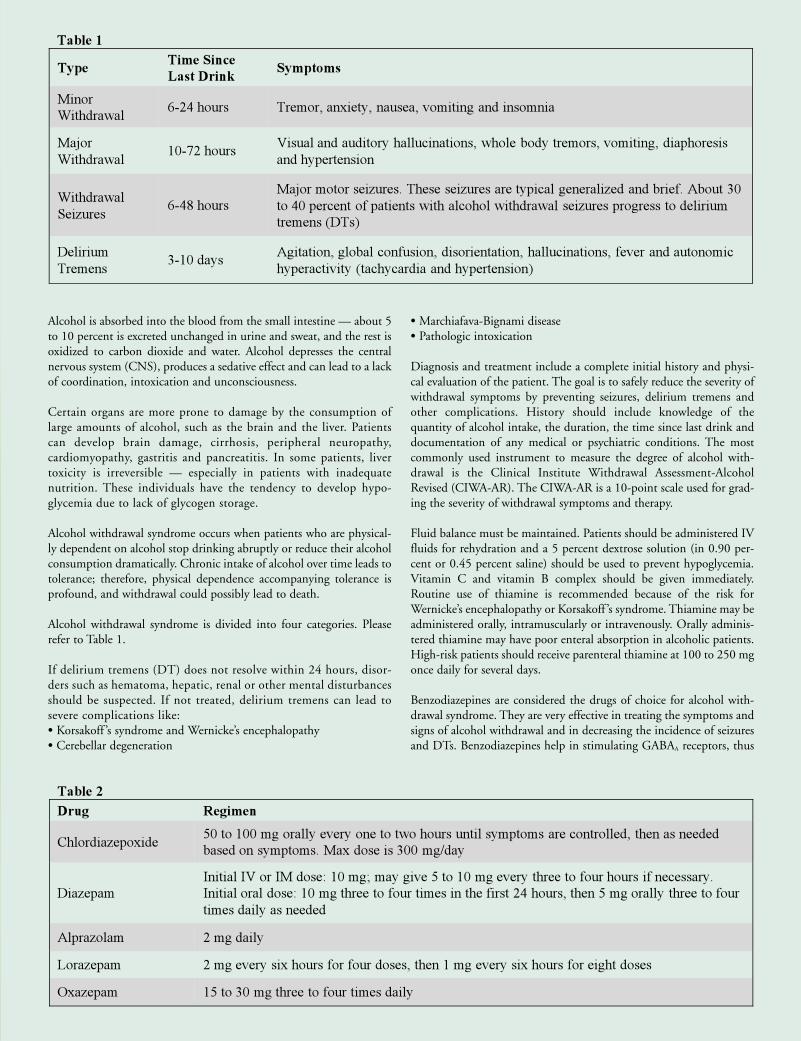
Table 1
TypeTime Since
Last DrinkSymptoms
Minor
Withdrawal6-24 hours Tremor, anxiety, nausea, vomiting and insomnia
Major
Withdrawal10-72 hours
Visual and auditory hallucinations, whole body tremors, vomiting, diaphoresis
and hypertension
Withdrawal
Seizures6-48 hours
Major motor seizures. These seizures are typical generalized and brief. About 30
to 40 percent of patients with alcohol withdrawal seizures progress to delirium
tremens (DTs)
Delirium
Tremens3-10 days
Agitation, global confusion, disorientation, hallucinations, fever and autonomic
hyperactivity (tachycardia and hypertension)
Table 2
Drug Regimen
Chlordiazepoxide50 to 100 mg orally every one to two hours until symptoms are controlled, then as needed
based on symptoms. Max dose is 300 mg/day
Diazepam
Initial IV or IM dose: 10 mg; may give 5 to 10 mg every three to four hours if necessary.
Initial oral dose: 10 mg three to four times in the first 24 hours, then 5 mg orally three to four
times daily as needed
Alprazolam 2 mg daily
Lorazepam 2 mg every six hours for four doses, then 1 mg every six hours for eight doses
Oxazepam 15 to 30 mg three to four times daily
Alcohol is absorbed into the blood from the small intestine — about 5to 10 percent is excreted unchanged in urine and sweat, and the rest isoxidized to carbon dioxide and water. Alcohol depresses the centralnervous system (CNS), produces a sedative effect and can lead to a lackof coordination, intoxication and unconsciousness.
Certain organs are more prone to damage by the consumption oflarge amounts of alcohol, such as the brain and the liver. Patientscan develop brain damage, cirrhosis, peripheral neuropathy, cardiomyopathy, gastritis and pancreatitis. In some patients, livertoxicity is irreversible — especially in patients with inadequatenutrition. These individuals have the tendency to develop hypo-glycemia due to lack of glycogen storage.
Alcohol withdrawal syndrome occurs when patients who are physical-ly dependent on alcohol stop drinking abruptly or reduce their alcoholconsumption dramatically. Chronic intake of alcohol over time leads totolerance; therefore, physical dependence accompanying tolerance isprofound, and withdrawal could possibly lead to death.
Alcohol withdrawal syndrome is divided into four categories. Pleaserefer to Table 1.
If delirium tremens (DT) does not resolve within 24 hours, disor-ders such as hematoma, hepatic, renal or other mental disturbancesshould be suspected. If not treated, delirium tremens can lead tosevere complications like:• Korsakoff ’s syndrome and Wernicke’s encephalopathy• Cerebellar degeneration
• Marchiafava-Bignami disease• Pathologic intoxication
Diagnosis and treatment include a complete initial history and physi-cal evaluation of the patient. The goal is to safely reduce the severity ofwithdrawal symptoms by preventing seizures, delirium tremens andother complications. History should include knowledge of the quantity of alcohol intake, the duration, the time since last drink anddocumentation of any medical or psychiatric conditions. The mostcommonly used instrument to measure the degree of alcohol with-drawal is the Clinical Institute Withdrawal Assessment-AlcoholRevised (CIWA-AR). The CIWA-AR is a 10-point scale used for grad-ing the severity of withdrawal symptoms and therapy.
Fluid balance must be maintained. Patients should be administered IVfluids for rehydration and a 5 percent dextrose solution (in 0.90 per-cent or 0.45 percent saline) should be used to prevent hypoglycemia.Vitamin C and vitamin B complex should be given immediately.Routine use of thiamine is recommended because of the risk forWernicke’s encephalopathy or Korsakoff ’s syndrome. Thiamine may beadministered orally, intramuscularly or intravenously. Orally adminis-tered thiamine may have poor enteral absorption in alcoholic patients.High-risk patients should receive parenteral thiamine at 100 to 250 mgonce daily for several days.
Benzodiazepines are considered the drugs of choice for alcohol with-drawal syndrome. They are very effective in treating the symptoms andsigns of alcohol withdrawal and in decreasing the incidence of seizuresand DTs. Benzodiazepines help in stimulating GABAA receptors, thus
14 Correct Rx
References:1) U.S. Department of Health and Human Services, National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism. Helping Patients Who Drink TooMuch: A Clinician’s Guide, December 2007 Update. National Institute on Alcohol Abuse and Alcoholism (www.niaaa.nih.gov/guide). 2) Rathlev NK, Ulrich AS, Delanty N, D’Onofrio G. Alcohol-related seizures. J Emerg Med. Aug 2006; 31(2): 157-63.3) Olmedo R, Hoffman RS. Withdrawal syndromes. Emerg Med Clin North Am. May 2000; 18(2): 273-88.4) Mayo-Smith MF, Beecher LH, Fischer TL, Gorelick DA, Guillaume JL, Hill A, et al. Management of alcohol withdrawal delirium. An evidence-based practice guide-line. Arch Intern Med. Jul 12 2004; 164(13): 1405-12.5) Addolorato G, Caputo F, Capristo E, et al: Rapid suppression of alcohol syndrome by baclofen. Am J Med 2002; 112 (3): 226-229.
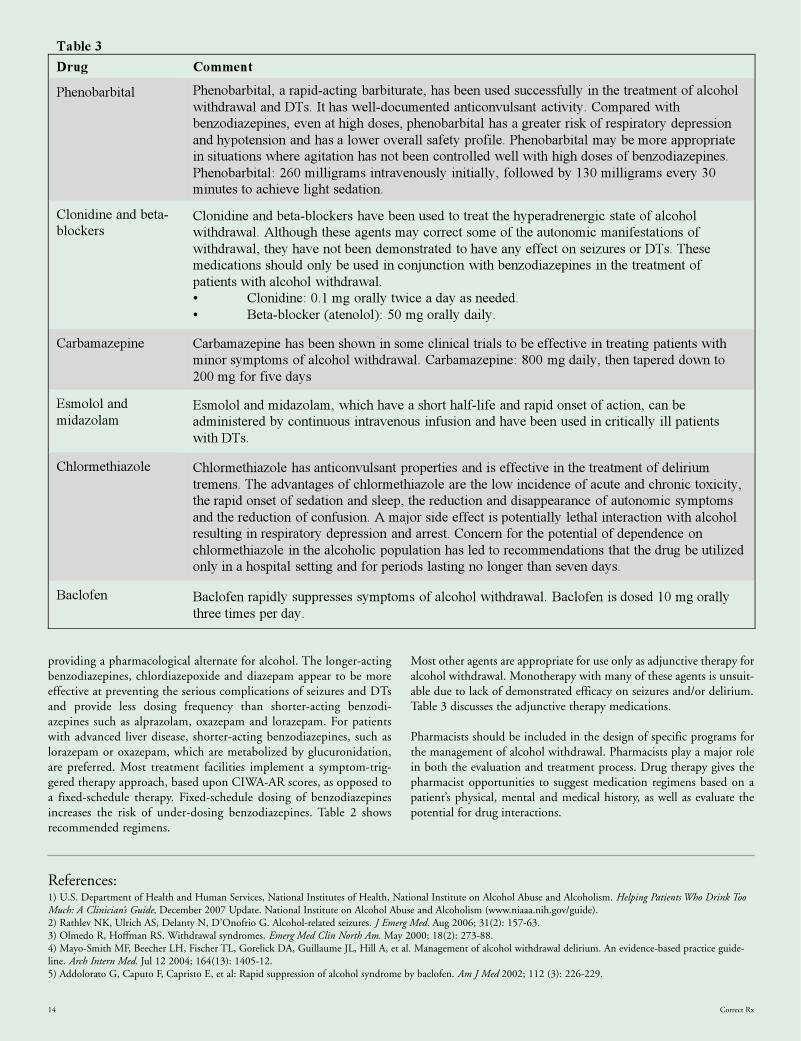
Table 3
Drug Comment
Phenobarbital Phenobarbital, a rapid-acting barbiturate, has been used successfully in the treatment of alcohol
withdrawal and DTs. It has well-documented anticonvulsant activity. Compared with
benzodiazepines, even at high doses, phenobarbital has a greater risk of respiratory depression
and hypotension and has a lower overall safety profile. Phenobarbital may be more appropriate
in situations where agitation has not been controlled well with high doses of benzodiazepines.
Phenobarbital: 260 milligrams intravenously initially, followed by 130 milligrams every 30
minutes to achieve light sedation.
Clonidine and beta-
blockersClonidine and beta-blockers have been used to treat the hyperadrenergic state of alcohol
withdrawal. Although these agents may correct some of the autonomic manifestations of
withdrawal, they have not been demonstrated to have any effect on seizures or DTs. These
medications should only be used in conjunction with benzodiazepines in the treatment of
patients with alcohol withdrawal.
• Clonidine: 0.1 mg orally twice a day as needed.
• Beta-blocker (atenolol): 50 mg orally daily.
Carbamazepine Carbamazepine has been shown in some clinical trials to be effective in treating patients with
minor symptoms of alcohol withdrawal. Carbamazepine: 800 mg daily, then tapered down to
200 mg for five days
Esmolol and
midazolamEsmolol and midazolam, which have a short half-life and rapid onset of action, can be
administered by continuous intravenous infusion and have been used in critically ill patients
with DTs.
Chlormethiazole Chlormethiazole has anticonvulsant properties and is effective in the treatment of delirium
tremens. The advantages of chlormethiazole are the low incidence of acute and chronic toxicity,
the rapid onset of sedation and sleep, the reduction and disappearance of autonomic symptoms
and the reduction of confusion. A major side effect is potentially lethal interaction with alcohol
resulting in respiratory depression and arrest. Concern for the potential of dependence on
chlormethiazole in the alcoholic population has led to recommendations that the drug be utilized
only in a hospital setting and for periods lasting no longer than seven days.
Baclofen Baclofen rapidly suppresses symptoms of alcohol withdrawal. Baclofen is dosed 10 mg orally
three times per day.
providing a pharmacological alternate for alcohol. The longer-actingbenzodiazepines, chlordiazepoxide and diazepam appear to be moreeffective at preventing the serious complications of seizures and DTsand provide less dosing frequency than shorter-acting benzodi-azepines such as alprazolam, oxazepam and lorazepam. For patientswith advanced liver disease, shorter-acting benzodiazepines, such aslorazepam or oxazepam, which are metabolized by glucuronidation,are preferred. Most treatment facilities implement a symptom-trig-gered therapy approach, based upon CIWA-AR scores, as opposed toa fixed-schedule therapy. Fixed-schedule dosing of benzodiazepinesincreases the risk of under-dosing benzodiazepines. Table 2 showsrecommended regimens.
Most other agents are appropriate for use only as adjunctive therapy foralcohol withdrawal. Monotherapy with many of these agents is unsuit-able due to lack of demonstrated efficacy on seizures and/or delirium.Table 3 discusses the adjunctive therapy medications.
Pharmacists should be included in the design of specific programs forthe management of alcohol withdrawal. Pharmacists play a major rolein both the evaluation and treatment process. Drug therapy gives thepharmacist opportunities to suggest medication regimens based on apatient’s physical, mental and medical history, as well as evaluate thepotential for drug interactions.
Correct Rx 15
Tardive dyskinesia (TD) is a neurological syndromethat is not well understood. TD is severely debilitatingand often warrants the discontinuation of the neu-roleptic treatment that has provided control of psy-chotic symptoms. Management of TD is especiallychallenging in schizophrenic patients who have found,after a potentially long process of trial and error, aneuroleptic that offers control for their psychoticsymptoms with very few alternatives remaining.
The presentation of TD symptoms is highly stigmatizing and hassocial implications for patients treated with antipsychotic medica-tion. The classic description of TD is the Buccal-Lingual-Masticatory Syndrome, or oral-facial movements. The firstdetectable signs may be a slight back and forward movement of thetongue, then progression to a more pronounced thrusting or rollingof the tongue with or without chewing or lateral jaw movements.
Treatmentof Tardive
Dyskinesia
by Hui W. Seo,Pharm.D.

TD symptoms can interfere with a patient’sability to eat; malnutrition becomes a seri-ous concern. Facial movements include frequent blinking, brow-arching, grimacing,upward deviation of the eyes and lip-smack-ing. Upper- and lower-extremity involve-ment is exhibited by restless choreiform or,conversely, a slow, writhing movement oflimbs in twisting, spreading and bendingmotions. Unusual posture, hyperextension,pelvic thrusting, excessive muscular activityof the head and trunk, jerking, shaking,rocking and swaying are observed. TD canbe worsened by stress and diminished bysedation or sleep.
The pathophysiologic mechanism that causesTD and why it occurs have not been conclu-sively uncovered. There are numerous proposed mechanisms based upon publishedmanagement strategies and anecdotal casereports: dopamine receptor super-sensitivitydue to up-regulation, catecholamine hyperac-tivity, gamma-aminobutyric acid (GABA) hypo-activity and free radical damage of neurons.
The most discussed mechanism is the com-pensatory up-regulation of dopamine (D2-type) receptors or the increased sensitivityof the receptors in the basal ganglia due tolong-term administration of neuroleptics.This hypothesis explains the delayed onsetof TD and worsening of TD when antipsychotic agents are discontinued.Additionally, the lower incidence of TDassociated with second-generation antipsy-chotic agents (SGA) compared to first-gen-eration antipsychotic agents (FGA). SGAsbind to serotonergic, alpha, histaminic,muscarinic and have higher affinity for D4-and D5-type dopamine receptors asopposed to D2-type receptors.
FGA agents are reported to have an inci-dence rate between 0.5 percent and 62 per-cent in earlier studies. In a first episode ofschizophrenia, the incidence is estimated atabout 5 percent a year, with overall preva-lence ranging from 20 to 25 percent withlong-term treatment.1 A 2004 review byCorrell CU, Leucht S, and Kane JM exam-ined 11 studies where SGAs were used for atleast one year and found an overall risk ofTD to be approximately 0.8 percent per yearin adults less than 65 years of age.1 Theiranalyses also suggest that FGAs should notbe used in adults older than 65 years of agedue to a fivefold increase in TD rates com-pared to SGAs.
The risk of TD with second-generationantipsychotics is significantly lower basedupon comparisons with first-generationantipsychotics (FGA). In most studies,haloperidol, usually in high doses (haloperi-dol > 10 mg/day), was the representativeFGA. TD incidence rates with medium-potency neuroleptics, such as fluphenazine ortrifluoperazine, have not been well-studied.Unfortunately, there is inconclusive data tosuggest variances between SGAs (excludingclozapine). There have been no proven casesof TD associated with the use of clozapine.Clozapine has been shown to reduce TDseverity in patients who have failed or shown
intolerance to trials of three or more antipsy-chotic agents. Nevertheless, the clinician mustbalance the risk of agranulocytosis associatedwith clozapine when considering use.
The dopamine up-regulation and increasedsensitivity model for TD is the basis for cur-rent investigative clinical trials of reserpine,tetrabenazine and dopamine-depletingagents.2 Interestingly, increasing the dose of adopamine antagonis t or adding an additional neuroleptic has been investigat-ed for treating TD. This strategy remains highly controversial.
Another theory is that free radicals damageneurons in the basal ganglia. This theory isthe basis for the use of antioxidants and vita-min E for the treatment of TD. Hydrogenperoxide is a byproduct of dopamine metab-olism by monoamine oxidase.3 Hydrogenperoxide is a potent oxidant and generatesfree radicals to damage neuronal cells.4
Anecdotal treatment with vitamin E 400 to1,600 units/day has been used to alleviateTD symptoms. Clinical trial results withvitamin E provide conflicting evidence.
There is growing interest in the role of theGABA system in TD and other movementdisorders. GABA neurons in the subcorticalregions of the brain play a crucial role in
Table 1: Tardive Dyskinesia Presentation
Affected Anatomy Involuntary Dyskinetic Manifestations
General Unusual posture
Hyperextension
Bending backward
Rocking
Swaying
Facial Frequent blinking
Upward deviation of the eyes
Brow-arching
Buccal-Lingual-Masticatory (BLM) Syndrome
• Forward, backward, lateral tongue movements
• Tongue thrusting, rolling or “fly-catching” movements
• False chewing or lateral jaw movements
Grimacing
Lip-smacking
Upper Extremity Restless choreiform (irregular and spasmodic) movements
Slow, writhing movements of the limbs
Twisting, spreading, bending and extension of the fingers
Trunk and hips Hyperkinesias of the trunk and neck
Pelvic thrusting
Lower Extremity Toe-tapping
Toe dorsiflexion
T bl 2 Ri k F t f T di D ki i
18 Correct Rx
Correct Rx 19
abnormal movement disorders.5 TD may beassociated with decreased glutamic aciddecarboxylase, which is the GABA-synthe-sizing enzyme found in various parts of thebrain; however, GABA-enhancing medica-tions have failed to provide significant benefit in controlling TD symptoms.6 Thereare reports that clonazepam has alleviatedoral dyskinesia associated with TD.7
Other treatment strategies under investiga-tion include: levodopa, benzodiazepines,botulinum toxins, acetylcholinesteraseinhibitors, ondansetron and calcium chan-nel blockers.2 Currently, the mechanism of
how these agents may improve TD effectsis not clear.
Risk factors include an age greater than 65years, the occurrence of acute extrapyrami-dal side effects, poor antipsychotic drugresponse, diagnosis of organic mental disor-der, diabetes mellitus, mood disorders,female gender and the use of high-dosefirst-generation antipsychotic agents.9 Theduration of antipsychotic therapy, the dailydosage and possibly the total cumulativedosage are probably the most significantrisk factors.2
There is no standardized diagnostic toolavailable for identifying or monitoring TD.The most commonly used rating scale is theAbnormal Involuntary Movement Scale(AIMS) and the Dyskinesia IdentificationSystem: Condensed User Scale (DISCUS).Both assessments are relatively quick to per-form (five to 10 minutes); however, theymust be performed by a trained clinician. 2
Identification and prevention strategies forTD are vital in managing medication therapyfor TD. The chance of reversing TD is great-est when discovered early with discontinua-tion of the offending medication. Despite
Other treatment strategies under investigation include: levodopa,
benzodiazepines, botulinum toxins, acetylcholinesterase inhibitors,
ondansetron and calcium channel blockers.

reports that TD is not always permanent,with remission of symptoms observed in 25percent of patients after five years of contin-ued treatment, if TD is allowed to persist, TDmay be irreversible even after discontinuationof the neuroleptic.
The first consideration for managing TD isthe withdrawal of the causative agent andinitiation of an alternative antipsychotic.2 Ifthe offending agent is an FGA, trial of anSGA should be considered. If withdrawal isnot feasible when treating a chronic schizo-phrenic patient, due to the risk of relapse or
exacerbation of psychotic symptoms, anattempt at a dosage reduction is a reasonableoption. Caution should be exercised whenmaking transitions. The absence ofdopaminergic blockade may aggrevate TDeffects. The addition of vitamin E early mayprovide benefit in reducing TD symptoms.Clozapine should be considered after failureof three or more antipsychotic agents.1,2
The role of medium potency FGAs in themanagement of psychosis is not clear at thistime. The CATIE Trial showed no differencein therapeutic outcomes and side effects,
including TD, between fluphenazine andSGAs.9 More research on TD mechanismand treatment strategies are warranted.Currently, there are numerous clinical trialsongoing at the National Institute for MentalHealth on treatment modalities for TD.
TD is a potentially irreversible side effectassociated with antipsychotic agents if it isunrecognized. It follows that judicious mon-itoring for TD is critical in treating patientswith antipsychotic medications.
References:1. Correll CU, Leucht S, Kane JM. Lower Risk for Tardive Dyskinesia Associated with Second-Generation Antipsychotics: A Systematic Review of 1-Year Studies. Am JPsych 161:3, March 2004.2. Brasic JR. Tardive Dyskinesia. EMedicine. Last Updated March 2007.3. Lohr JB, Caliguri MP. A double-blind placebo-controlled study of vitamin E treatment of tardive dyskinesia. J Clin Psych 1996; 57: 167-73.4. Yamada K, Kanba S, Anamizu S, et al. Low superoxide dismutase activity in schizophrenic patients with tardive dyskinesia. Psychol Med. Sep 1997; 27(5):1223-5.5. Tsai G, Goff DC, Chang RW, et al. Markers of glutamatergic neurotransmission and oxidative stress associated with tardive dyskinesia. Am J Psychiatry. Sep 1998; 155(9):1207-13.6. Thaker GK, Nguyen JA, Strauss ME, et al. Clonazepam treatment of tardive dyskinesia: a practical GABAmimetic strategy. Am J Psychiatry. Apr 1990; 147(4):445-51.7. Watts RL, Koller WC. Movement Disorders: Neurologic Principles and Practice. New York, NY. McGraw-Hill; 1997.8. Walters VL, Tognolini RZ, Rueda HM, et al. New strategies for old problems: tardive dyskinesia (TD). Review and report on severe TD cases treated with clozapine, with 12, 8 and 5years of video follow-up. Schizophr Res. Dec 19 1997; 28(2-3):231-46.9. Rosenheck RA, Leslie DL, Sindelar J, Miller EA, Lin H, Stroup TS, McEvoy J, Davis S, Keefe R, Swartz M, Perkins D, Hsiao JK, Lieberman J. Cost-effectiveness of Second GenerationAntipsychotics and Perphenazine in a Randomized Trial of Treatment for Chronic Schizophrenia. Journal of Psychiatry. 2006 Dec; 163 (12): 2080-89.
20 Correct Rx
Bridging the GapOpioid Treatment Program in Corrections
In the American correctional system, drug addiction is a major concern. According to the Department
of Justice, approximately 1.7 million individuals arrested are involved with drugs and/or alcohol. In
2000, a median of 5.8 percent of adult men and 6.6 percent of adult women tested positive for opiates
upon incarceration. In jails located in urban areas, 10 to 27 percent of arrestees have opioids in their sys-
tem when taken into custody. For those who are incarcerated for drug-related crimes or for those who
succumb to the perils of opioid dependence, there are limited programs available that offer much-needed
support and care. Ideally, these programs should concentrate efforts to help those who are incarcerated
maintain treatment for opioid dependence and transition care when they are released. Nationally, there
are approximately 300,000 individuals who participate in such programs; unfortunately, roughly 10
percent of these individuals are arrested yearly.
by Kesha N. O’Reilly,Pharm.D.

One such program is an Opioid TreatmentProgram (OTP) with methadone used as itsprimary treatment medication. OTPs are cer-tified by the Substance Abuse and MentalHealth Services Administration (SAMHSA).In addition, OTP programs must meet U.S.Drug Enforcement Agency (DEA) mandatesand state regulations. Furthermore, correc-tional OTP programs must be accredited bythe National Commission on CorrectionalHealthcare (NCCHC). The majority of jailsthroughout the United States do not provideOTPs. In jails without OTPs, when an opioid-dependent individual is arrested, he orshe may experience severe withdrawal. Thesewithdrawal symptoms are generally treatedwith clonidine, acetaminophen, NSAIDs andantiemetic medications.
In February 2008, an OTP program wasestablished in a mid-Atlantic metropolitan jailfacility. This program addressed the needs ofinmates who were arrested and were detoxingfrom opioids, as well as inmates who wereenrolled in a community methadone treat-ment program. The correctional OTP has twosignificant benefits. It keeps patients shieldedfrom life-threatening detoxing events, and itensures that individuals who are participantsin community methadone programs will notforfeit their enrollment. Prior to the creationof the correctional OTP, an arrest wouldmean a person’s removal from his or her out-patient treatment program. Many would bereleased from jail within a couple of days orweeks with no treatment options, thusincreasing the risk of relapse.
Continual service and extensive care are cor-nerstones to any successful methadone/detoxprogram. To support these measures in a jailsetting, the medical personnel must be avail-able 24 hours a day to ensure individualswho self-report participation in a methadoneprogram would be assessed extensively. Onceverification of participation in a communityprogram is made, individuals would receivemethadone on a daily basis. Patients receiv-ing methadone would be on a different medication administration schedule thanother patients to reduce manipulation andcoercion by other inmates and maintain a safe environment.
From its implementation, there was an imme-diate and high level of participation. Initially,the correctional OTP was expected to servesix to seven individuals per week. In actuality,45 individuals receive methadone daily,
exceeding estimates used in planning for theprogram. More than 95 percent of these indi-viduals received methadone for maintenanceand not detox.
The correctional OTP numbers mirror theinterest within the served communities. Uponlearning about the planned rollout in the met-ropolitan correctional facility, reaction rangedfrom excitement to concern. Communityhealth care professionals thought the programwould keep participants fully vested in theservices, decreasing the possibility that indi-viduals would be lost if arrested and released.
Although most people saw the immediatebenefits from the program, several issues wereraised. Many were skeptical about the jail pro-viding the services, doubting the quality ofcare in counseling. Some also pointed to theconstant concerns about safety, specificallyinmate behavior that is already volatile. Dueto the pre-existing stigma of methadone inboth the community and in corrections, ini-tiating a methadone program appeared to be arecipe for disaster. Those involved wantedassurances that methadone would be part ofmaintenance or detox and not used byinmates as an agent for overdosing.
In order for the program to be certified, med-ical staff members had to follow state and fed-eral laws and regulations. Both medical andcustody staff were briefed by DEA agents andSAMHSA representatives on how the OTP
would operate and new policies and proce-dures associated with methadone use. Addingoversight capabilities helped medical staffmembers provide the service in the correctway, lessening the chance of possible inci-dents. For example, nursing staff membersmade sure to properly document every facetof the program, including separatingmethadone used for the program from othercontrolled substances.
Although the program was certified, therewere additional obstacles. Educating staff onthe state and federal laws and regulationsproved to be a daunting task. Training ses-sions were set up on a weekly basis, whichconsisted of pre- and post-testing, roundtablediscussions and work-flow analysis. Also,medical administrators had to work extreme-ly hard to convince custody that methadonehad positive uses. The negative connotationneeded to be minimized in order for the pro-gram to have full support both openly andbehind the scenes.
Overall, the correctional OTP created a need-ed infrastructure in the rehabilitation of thosesaddled with drug dependency. The cohesiverelationship with the community programand correctional staff was a vital part of theOTP success. Hopefully, more metropolitanareas will follow and establish correctionalOTPs that bridge the need of opioid depend-ence between the community and jails.
22 Correct Rx
Correct Rx 23
“If it’s the right way, it’s the correct way.”





























