Embed Size (px)
Citation preview
60 inside dentistry | July 2013 | www.insidedentistry.net
Sleep Prosthodontics: A New Vision for DentistryPart 1 of this 2-part series focuses on the snoring child Jeffrey S. Rouse, DDS
InsideContinuing eDuCation eSthetiCS | ReStoRative
• Describethedifference betweensleepprosthodontics andsleepdentistry.
• Explaintheuniqueimpactofsleep fragmentationandobstructive apneaonchildren.
• Correlatedentalabnormalities toairwaydeficienciesin pediatricpatients.
Toreceiveupto2creditsforthisarticle,logonto
www.insidedentistryCE.com totakethequiz.
LEarning ObjECtivEs
abstraCt
the purpose of this article is to introduce a new term, sleep prosthodontics, to the den-tal community and to differentiate airway analytics from sleep dentistry. sleep dentistry may be thought of as the study of an oral appliance and its impact on the airway. sleep prosthodontics is the study of airway and its impact on the stomatognathic system. in other words, sleep dentistry addresses the how (ie, how does an appliance assist noctur-nal breathing?), whereas sleep prosthodontics addresses the why (ie, why are patients developing malocclusions, creating myofacial pain symptoms, and wearing their den-tition?) this article will focus on the impact of sleep disordered breathing on the grow-ing child and the unique role dentistry plays in screening and treating these patients.
S leep disordered breath-ing (sdB) encompasses a spectrum of dysfunctional sleep breathing, including occasional snoring, habitu-al snoring, upper airway re-sistance syndrome (UArs),
sleep apnea, and hypoventilation. the medi-cal community has traditionally focused on obstructive sleep apnea (OsA) and obesity hypoventilation syndrome. Unfortunately, many sleep-related breathing disorders, es-pecially those predominately found in women
Jeffrey S. rouSe, DDSPrivate Practice ProsthodontistSan Antonio, Texas
uArS and oSA: A Comparison Although many clinicians describe UArs and OsA as the same disease with a slight variance in severity, their pathophysiologies appear to be different.4 OsA is characterized by com-plete upper airway obstructions lasting longer than 10 seconds with an associated 4% oxygen desaturation. it is most commonly attribut-ed to a hypotonia of the soft palate or base of tongue. Partial airway obstructions that lead to desaturation or brief awakenings from sleep are classified as hypopneas. Continued desatu-rations over time may cause excessive daytime sleepiness and hypertension. they have been correlated to endothelial dysfunction, myo-cardial infarction, and cerebrovascular acci-dents. the level of severity of OsA has been associated with an increased mortality.5,6
Anatomic irregularities or minor breath-ing impairments can create UArs.7 Patients with UArs may have a more collapsible air-way because of abnormal inspiratory flow dynamics8 or increased collapsibility on expiration due to atypical anatomy.9 UArs patients have more sensitivity to restricted breathing or negative oropharyngeal pres-sure. the airway constriction is recognized
and children, have been ignored because of the focus on OsA.
snoring typically occurs when air passes between the tongue and soft palate, caus-ing a vibration of the soft palate. A snor-ing sound may also be produced from the nose during inhalation. Children can pro-duce the same loud snoring sound as an adult, but typically their snoring is more of an effortful breathing, making recogni-tion and diagnosis more challenging in this population.
the consequences of snoring can be seri-ous. Habitual snoring, defined as three times per week or more, has been associated with hyperactive behavior in children as young as 3 years of age1 and poor academic perfor-mance.2 sleep fragmentation or disruption caused by snoring appears to play a role as important as hypoxia in causing dysfunction. Benign snoring in adults has been implicat-ed in an increase risk of stroke.3
Peer Reviewed

62 inside dentistry | July 2013 | www.insidedentistry.net
for OsA, women with UArs and the majority of children are eliminated from the purview of the dental practitioner.
Sleep Prosthodonticssleep dentistry can be thought of as the study of an OA and its impact on the airway. sleep prosthodontics is the study of the airway and its impact on the stomatognathic system. the stomatognathic system encompasses the mouth, jaws, and the closely related struc-tures of the oro-pharynx and fauces. dentists deal with this system during its development and maintain it throughout a lifetime.
Although a physician must make the diag-nosis of sdB, the dentist plays a critical “diag-nostic” role. Many times the lack of witnessed apneic episodes or the lack of particularly egregious daytime symptoms may lead to a delay in care by the medical community. the impact of a poor airway can many times be detected in the patient’s craniofacial devel-opment, oral impairment, and occlusal dys-function well before the clinical presentation of systemic disease.15
sleep prosthodontics is not restricted to an appliance, but instead has a single-minded focus on the patient’s health. it also encour-ages a patient-centered, interdisciplinary so-lution that includes a wide range of options, including orthodontics, oral mycology, nutri-tion/diet counseling, orthognathics, CPAP, MAA, and otolaryngologic surgeries.
The Snoring Child in the general population, 2% to 3% of chil-dren have apnea.16 that proportion is grow-ing given the increase in childhood obesity.17 Apneas and hypopneas are defined in chil-dren as events lasting longer than two missed breaths and most commonly associated with some change in oxygen saturation or end tidal CO2 increase. UArs presents in children dur-ing polysomnography (PsG) as an increased respiratory effort with no apnea and little oxy-gen saturation change (Figure 2). the charac-teristic signs and symptoms of UArs vary with the age of the child, as will treatment options.18
the prevalence of snoring in children rang-es from 10% to 21% from 6 to 81 months.19 Habitual snoring has been reported in 9% of infants aged 0 to 3 months.20 in a general pediatric clinic, habitual snoring was docu-mented in 17% of patients, with that rising to 29% of the children reporting for neurolog-ic indications such as headaches and 56% of the children diagnosed with psychiatric dis-orders (half with anxiety/mood disorders).21,22 in a 2-year follow-up on habitually snoring children, 30% of subjects had worsened from baseline. OsA developed more often in boys, especially if adenotonsillar hypertrophy or an increase in waist circumference was present.23
snoring and mouth breathing in children were initially thought of as unreliable markers for OsA and not as potential problems in their own right. More recently, it is believed that snor-ing independent of OsA may cause neurocogni-tive dysfunction and impaired daytime perfor-mance.24,25 Habitually snoring children are at higher risk for social problems, poor academic performance, decreased attention, and anxiety/depression issues.26-28 Children who are chron-ic snorers have abnormal slow-wave sleep pat-terns and experience more fragmentation. this sleep instability may explain the detrimental effects of non-apneic snoring.29 studies of oc-casionally snoring children who otherwise have normal sleep demonstrated altered brain func-tion and more delayed and effortful processing. these children also experienced more behav-ioral problems than non-snoring children.30
Children who snore are not likely to “grow out of it” without experiencing cognitive impairment.
and responded to more quickly, preventing obstruction. these respiratory effort–related arousals (rerAs) and sleep fragmentations lead to activation of the autonomic nervous system—in particular, increased sympathetic nerve activity.10
Sleep DentistryContinuous positive airway pressure (CPAP) was introduced in 1981.11 CPAP is still the standard of care today for OsA.12 even with significant improvements in CPAP technol-ogy, it is unpopular with patients, rarely worn throughout an entire night,13 and has less than optimal long-term compliance.14
Oral appliances (OA) were introduced in the 1980s in an attempt to provide an alter-native to the unpopular CPAP. OAs act by protruding the mandible and attempting to position the tongue out of the oropharyn-geal region. OAs are currently divided by their manner of therapy. tongue-retaining devices utilize negative pressure from a bulb attached to the tip of the tongue to reposition the tongue. Mandibular advancing appliances (MAAs) are attached to the dental arch (Figure 1). the mandible is held in a protruded posi-tion. the protrusion is either fixed or titratable.
Although the quest to create an alternative to CPAP is understandable, sleep dentistry has become single-minded in its treatment of adult apnea with an appliance. if dentistry compartmentalizes itself on OA fabrication
DisorDereD sleep (1.) Titratable mandibular advancing appliance. (2.) Preparing for polysomnography (PSG). Monitoring and scoring is unique for pediatric sleep studies.
fig. 1 fig. 2
inside Continuing eDuCation

inside Continuing eDuCation
the neurocognitive and behavioral damage from snoring in children appears to be related to the fact that their brains are still developing. A confounding issue is that the impact of the snoring may not be detected for years, even after the snoring has resolved. the genesis of the long-term neurocognitive effect in snor-ing children may be during a critical devel-opmental period—at or before 3 years of age.
Bonuck and colleagues31 examined 7 years of epidemiologic data from more than 11,000 children followed from birth. Cognitive and behavioral assessments were conducted when the children reached 4 and 7 years of age. By 4 years old, children who had a history of sdB were 20% to 60% more likely to exhib-it behavioral difficulties; by 7 years, they were 40% to 100% more likely. the more severe sdB was linked to the poorest behavioral out-comes. the “Worst Case” cluster had a peak
of sdB symptoms at 30 months that abated. nonetheless, at 7 years the cluster displayed hyperactivity and conduct and peer difficul-ties. inclusion in the “Later sdB symptom” cluster, with a peak at 42 through 69 months, was predictive of emotional difficulties and hyperactivity at both 4 and 7 years.
Bonuck’s work underscores that the pres-ence of irregular sleep breathing may not be directly linked to the academic and behavior-al symptoms. instead, sdB during periods of brain development is very predictive of later damage. the neurocognitive damage in areas such as academic performance and executive functioning is not reversible, so early iden-tification and treatment are paramount.32-34
Metabolic ConsequencesBecause of the close link between sleep, the immune system, and inflammation, children
with sdB are prone to many of the same sys-temic inflammatory conditions that as adults lead to high blood pressure, arrhythmias, and congestive heart failure.35 sleep disturbances in children lead to aberrant sympathetic ner-vous activation that creates cardiovascular and metabolic injury.36 Pediatric apnea is connect-ed with endothelial microvascular dysfunction: a marker of subclinical cardiovascular disease, systemic hypertension, pulmonary hyperten-sion, and myocardial left ventricular remodel-ing.37 in the presence of obesity, the metabolic consequences are exacerbated. treatment of the sdB is mandatory to prevent complica-tions.38 if the child’s sdB is resolved, the sys-temic inflammation in non-obese subjects appears to be reversible.39 the unanswered question is whether the childhood autonom-ic disturbance promotes metabolic morbid-ity later in life even after sdB resolution.35
(Circle70onReaderServiceCard)
64 inside dentistry | July 2013 | www.insidedentistry.net
inside Continuing eDuCation
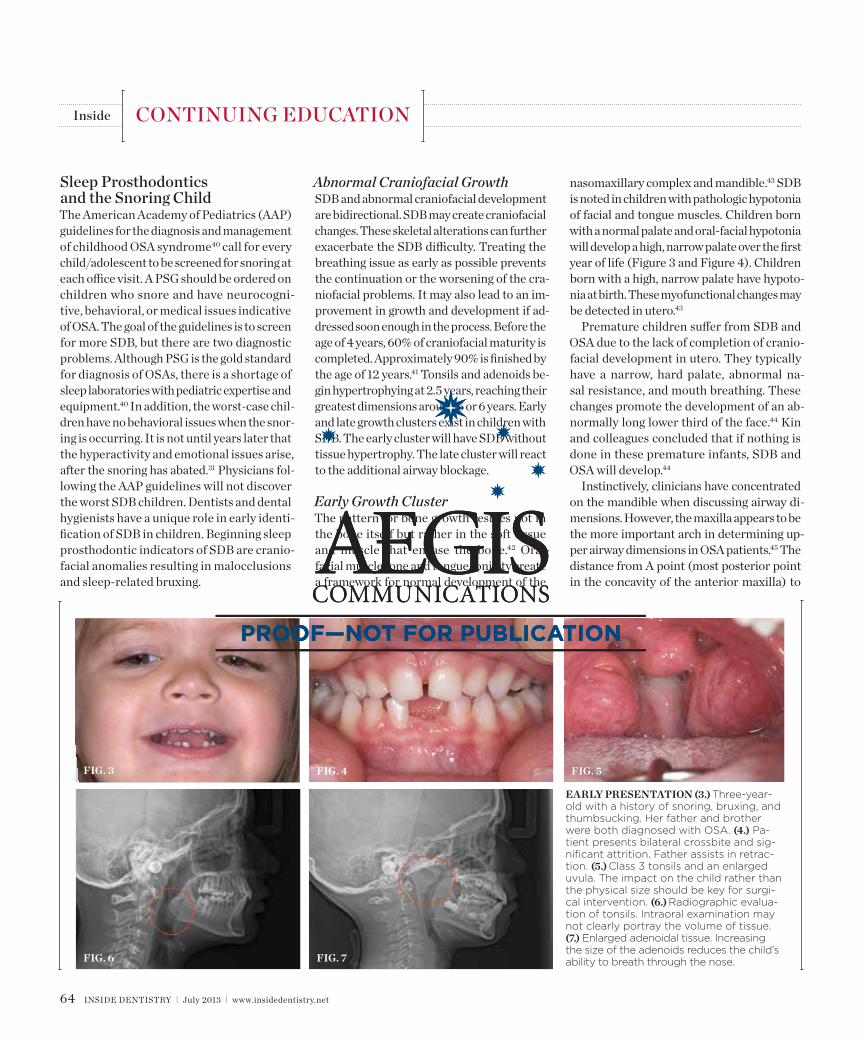
early presentation (3.) Three-year-old with a history of snoring, bruxing, and thumbsucking. Her father and brother were both diagnosed with OSA. (4.) Pa-tient presents bilateral crossbite and sig-nificant attrition. Father assists in retrac-tion. (5.) Class 3 tonsils and an enlarged uvula. The impact on the child rather than the physical size should be key for surgi-cal intervention. (6.) Radiographic evalua-tion of tonsils. Intraoral examination may not clearly portray the volume of tissue. (7.) Enlarged adenoidal tissue. Increasing the size of the adenoids reduces the child’s ability to breath through the nose.
fig. 3 fig. 4 fig. 5
fig. 6 fig. 7
Abnormal Craniofacial GrowthsdB and abnormal craniofacial development are bidirectional. sdB may create craniofacial changes. these skeletal alterations can further exacerbate the sdB difficulty. treating the breathing issue as early as possible prevents the continuation or the worsening of the cra-niofacial problems. it may also lead to an im-provement in growth and development if ad-dressed soon enough in the process. Before the age of 4 years, 60% of craniofacial maturity is completed. Approximately 90% is finished by the age of 12 years.41 tonsils and adenoids be-gin hypertrophying at 2.5 years, reaching their greatest dimensions around 5 or 6 years. early and late growth clusters exist in children with sdB. the early cluster will have sdB without tissue hypertrophy. the late cluster will react to the additional airway blockage.
Early Growth Clusterthe pattern for bone growth resides not in the bone itself but rather in the soft tissue and muscle that encase the bone.42 Oral-facial muscle tone and tongue tonicity create a framework for normal development of the
nasomaxillary complex and mandible.43 sdB is noted in children with pathologic hypotonia of facial and tongue muscles. Children born with a normal palate and oral-facial hypotonia will develop a high, narrow palate over the first year of life (Figure 3 and Figure 4). Children born with a high, narrow palate have hypoto-nia at birth. these myofunctional changes may be detected in utero.43
Premature children suffer from sdB and OsA due to the lack of completion of cranio-facial development in utero. they typically have a narrow, hard palate, abnormal na-sal resistance, and mouth breathing. these changes promote the development of an ab-normally long lower third of the face.44 Kin and colleagues concluded that if nothing is done in these premature infants, sdB and OsA will develop.44
instinctively, clinicians have concentrated on the mandible when discussing airway di-mensions. However, the maxilla appears to be the more important arch in determining up-per airway dimensions in OsA patients.45 the distance from A point (most posterior point in the concavity of the anterior maxilla) to
Sleep Prosthodontics and the Snoring Childthe American Academy of Pediatrics (AAP) guidelines for the diagnosis and management of childhood OsA syndrome40 call for every child/adolescent to be screened for snoring at each office visit. A PsG should be ordered on children who snore and have neurocogni-tive, behavioral, or medical issues indicative of OsA. the goal of the guidelines is to screen for more sdB, but there are two diagnostic problems. Although PsG is the gold standard for diagnosis of OsAs, there is a shortage of sleep laboratories with pediatric expertise and equipment.40 in addition, the worst-case chil-dren have no behavioral issues when the snor-ing is occurring. it is not until years later that the hyperactivity and emotional issues arise, after the snoring has abated.31 Physicians fol-lowing the AAP guidelines will not discover the worst sdB children. dentists and dental hygienists have a unique role in early identi-fication of sdB in children. Beginning sleep prosthodontic indicators of sdB are cranio-facial anomalies resulting in malocclusions and sleep-related bruxing.
66 inside dentistry | July 2013 | www.insidedentistry.net
inside Continuing eDuCation
Porion vertical (vertical line drawn from the most superior part of the external auditory me-atus) was the most contributory cephalometric marker for airway patency. Appropriate posi-tioning of the maxilla opens the velopharyn-geal and orophayngeal airways. Additionally, proper maxillary positioning enhances man-dibular growth. thus, the lack of facial mus-cle activity and ideal tongue tone constrains the premaxilla, producing an abnormal airway dimension and amplifying the threat of sdB.
Late and Mixed Growth Clustertonsils and adenoids occupy space, increase airway resistance, and create turbulent na-sal airflow. the period of tissue hypertrophy is especially damaging to mixed cluster pa-tients. these children are undiagnosed early growth cluster children who become further compromised due to enlargement of oral and nasal tissues.
tonsils and adenoids should be judged against the relative size of the airway rather than the absolute size of the lymphoid tis-sue46 (Figure 5 and Figure 6). Adenoids are located at the posterior of the nasal cavity on
the roof of the nasopharynx (Figure 7). the normal distance from the adenoids to the soft palate for an acceptable airway should be at least 12 mm. For each millimeter de-crease, the odds of the child snoring increase 1.61 times. Mouth breathers typically show a smaller upper airway dimension as well.47 the adenoid and tonsillar obstruction cre-ates the trigger, but the deviate facial and neck muscle recruitment and tongue hypo-tonia cause the maldevelopment.48
the point of obstruction tends to determine the type of skeletal impact. nasal obstruc-tion from enlarged turbinates, blocked osti-um maxillare, deviated septum, or nasal valve stenosis creates Angle occlusions of Class i, ii, and iii equally (Figure 8). the maxilla in these cases is positioned posteriorly and the mandible is posterior-inferior. the facial type is most commonly dolicocephalic. Blockage of the airway predominately by the adenoids will create growth patterns that yield mostly Class ii occlusions and anterior open bite with both jaws located posterior-inferiorly. Facial type is again dolicocephalic with the typical long-thin “adenoidal” face49 (Figure 9 through
Figure 12). if the tonsillar tissue is responsi-ble for the airway obstruction, the tongue will have an abnormal resting posture. Class iii occlusions will be more common with the maxilla normal or posterior placed (Figure 13 through 15). the tongue may direct the mandible anteriorly or, because the tongue is not in the roof of the mouth driving A point anterior, the maxilla will become bimaxillary retrusive.50 in some cases, the anterior pos-ture of the tongue will create an open bite. this is incorrectly referred to as a tongue thrust. the impact from a thrust does not alter the tooth position. Long-term, low forces cause tooth movement. the posture of the tongue against or between the anterior teeth due to the excessive tonsillar size creates the open bite (Figure 16 and Figure 17). Facial types in this group are more brachyfacial. Lastly, if the airway is blocked through a combination of factors, the Angle classification will be either Class ii or iii. the maxilla will be in a normal location and the mandible will be the affected arch (Figure 18). these craniofacial changes are not restricted to OsA; all sdB will create unique alterations depending on the patient
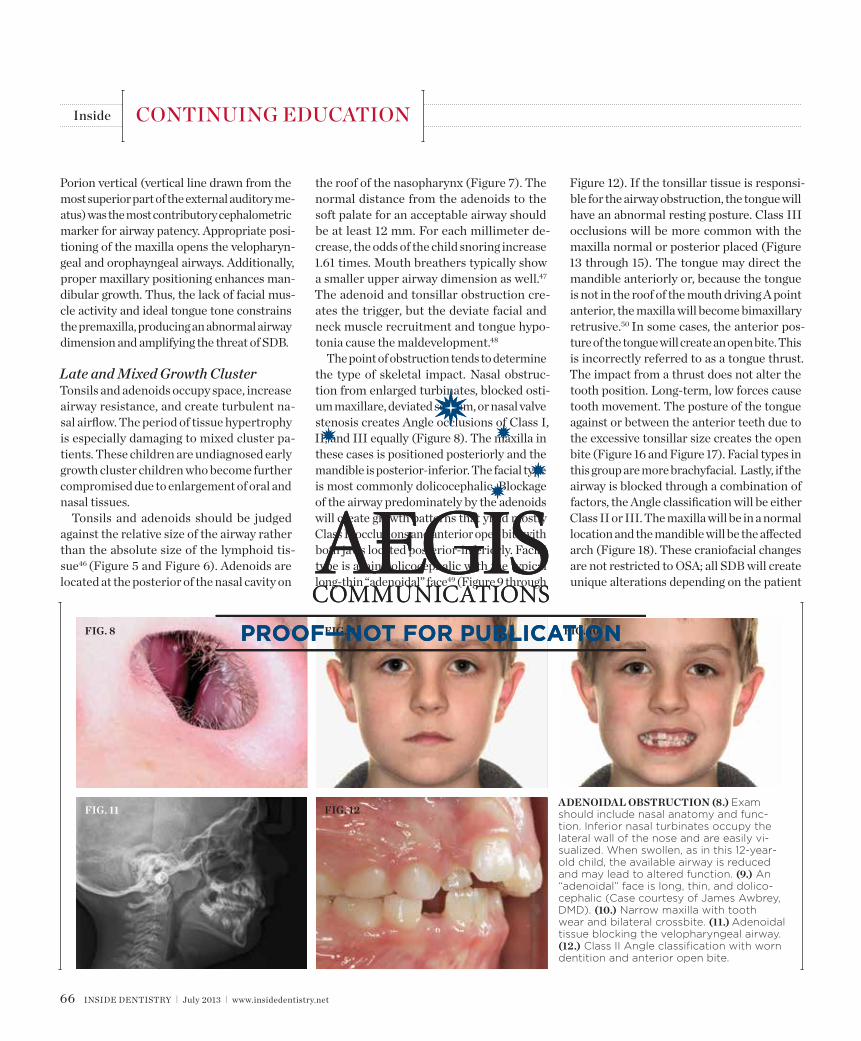
aDenoiDal obstruction (8.) Exam should include nasal anatomy and func-tion. Inferior nasal turbinates occupy the lateral wall of the nose and are easily vi-sualized. When swollen, as in this 12-year-old child, the available airway is reduced and may lead to altered function. (9.) An “adenoidal” face is long, thin, and dolico-cephalic (Case courtesy of James Awbrey, DMD). (10.) Narrow maxilla with tooth wear and bilateral crossbite. (11.) Adenoidal tissue blocking the velopharyngeal airway. (12.) Class II Angle classification with worn dentition and anterior open bite.
fig. 11
fig. 8 fig. 10
fig. 12
fig. 9
68 inside dentistry | July 2013 | www.insidedentistry.net
inside Continuing eDuCation
mouth breathing with the tongue in the roof of the mouth directed ideal growth.
in some children, t&A alone may not com-pletely resolve the OsA (Figure 19 and Figure 20). the longer the airway dysfunction, the greater the structural impact on the airway. An interdisciplinary clinical study54 was con-ducted on children approximately 6.5 years old with inclusion criteria of OsA, large tonsils, vi-sually constricted airway, and high and narrow palate. Group 1 was treated with rapid maxil-lary expansion (rMe) and Group 2 with t&A. Maxillary expansion has been shown to cre-ate improved nasal resistance and an increase nasal cavity volume. in cases without exces-sive lymphoid hypertrophy, rMe can resolve significant levels of OsA.55,56 After the original therapy, only one child had been completely resolved (apnea-hypopnea index [AHi] <1). the remaining subjects switched groups and received the opposite treatment. After receiv-ing both treatments, 29 of the 31 children were cured. it can be concluded that many children must be treated with multiple therapies before resolution, especially if the sdB has previously altered the airway to a significant degree.
Sleep Bruxismnot only are dentists in the best position to detect and intercede in cases of abnormal cra-niofacial development, but they are also the best judges of aberrant tooth wear. Bruxism occurs in up to 30% of children, often around 5 and 6 years during late cluster adenoid and tonsillar hypertrophy.57 Carlsson and col-leagues58 determined in a 20-year prospec-tive study that bruxism in childhood may be a persistent trait. early tooth wear was pre-dictive of increased tooth wear 20 years lat-er. the results emphasize that the triggering mechanism for sleep bruxism is present as a child and does not develop over time.
For restorative dentists, it is significant-ly more important to locate what elicits the action than the “genetic code” that produc-es a bruxer. Historically, popular theories have postulated that the generator for brux-ism was stress, neurochemical, or occlusion. PsG-based research has disproven these theories. stress leads to awake bruxism, not sleep bruxism.59,60 Most chemical irregulari-ties in bruxers are linked to sleep fragmen-tation.61,62 Finally, bruxism is a centrally, not
compensation. Children with UArs have been reported to display high, narrow palates, doli-cofacial form, and a Class ii malocclusion, in-dicative of largely adenoidal blockage.51
dentists identifying craniofacial changes early in development may resolve the mal-occlusion by simply referring for adenoton-sillectomy (t&A). the impact of t&A on the pediatric immune system is controver-sial. A recent 5-year longitudinal, prospective study demonstrated that adenotonsillectomy does not pose adverse short- or long-term im-pact on the cellular or humoral immunity.52 Cephalametric changes (eg, posterior incline to the mandible, anterior incline to the maxil-la, longer anterior and shorter posterior face height, and upper and lower teeth more retro-clined than a normal matched control) were detected in 5-year-old subjects with adenoid-induced OsA.53 t&A resolved the OsA in all subjects. At the 5-year recall, cephalomet-ric evaluation demonstrated that the man-dibular plane angle and incisor relationship was similar to the control. early resolution of the sdB allowed time for the proper use of the oral-facial and tongue muscles. Closed
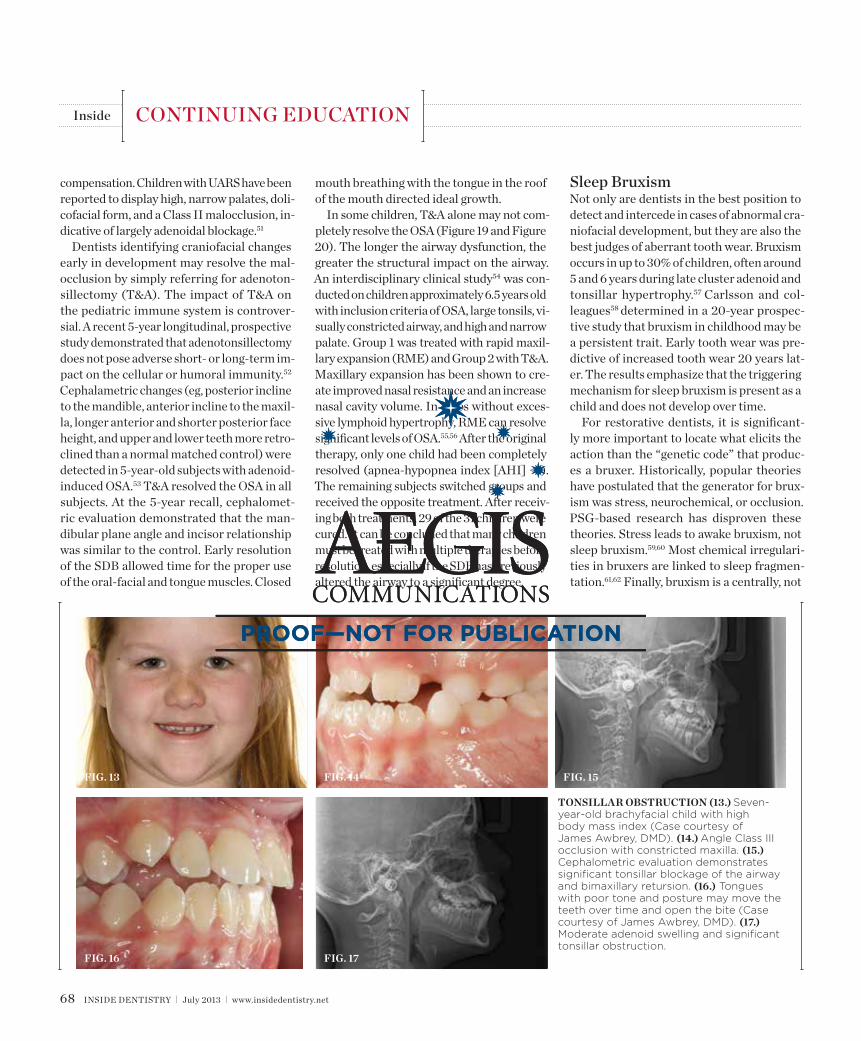
tonsillar obstruction (13.) Seven-year-old brachyfacial child with high body mass index (Case courtesy of James Awbrey, DMD). (14.) Angle Class III occlusion with constricted maxilla. (15.) Cephalometric evaluation demonstrates significant tonsillar blockage of the airway and bimaxillary retursion. (16.) Tongues with poor tone and posture may move the teeth over time and open the bite (Case courtesy of James Awbrey, DMD). (17.) Moderate adenoid swelling and significant tonsillar obstruction.
fig. 16
fig. 13 fig. 15
fig. 17
fig. 14
70 inside dentistry | July 2013 | www.insidedentistry.net
peripherally, mediated event.63 idealizing oc-clusions may control the impact of bruxism and improve chewing function, but it will not resolve sleep bruxism.64
Bruxism occurs during microarousals from regular sleep patterns.64,65 Many fac-tors may introduce microarousals, including reflux and tactile and auditory stimuli.66,67 the most common reason for these brux-ism-related microarousals appears to be re-spiratory effort. it is the author’s assertion that sleep bruxism serves a functional role in protecting and improving the airway during episodes of inspiratory flow limitation and obstruction. the activity of increasing ge-nioglossal and infrahyoid muscle tone along with the lateral movement of the mandible
dilates the upper airway, raises inspiratory flow, and reduces upper airway resistance.68
sleep bruxism is classified as a sleep-related movement disorder similar to restless leg syn-drome and is routinely referred to as a possi-ble indicator of sdB. the majority of bruxism occurs during light non–rapid eye movement sleep.69 With traditional PsG, 80% or more of the bruxing episodes have related respirato-ry events.68,70 Linking bruxism and airway re-sistance causally is difficult, given that many abnormal breathing patterns are not neces-sarily conspicuous on PsG. sleep apneas are more easily recognized, but the rerAs can be a challenge to identify, especially in children who do not desaturate like adults. Additionally, bruxism minimizes the degree of obstruction
and flow restriction.71,72 A healthy autonomic nervous system of a bruxing child can fix the airway before it can be detected within the framework of a normal PsG.
Without esophageal pressure monitoring to demonstrate the increase respiratory ef-fort, bruxism activity may not be recognized as being associated with a respiratory event.71,72 this rerA-related phenomenon was verified in a study of 50 pediatric subjects with an in-clusion criteria of sleep-related tooth wear.73 no significant statistical association was found between AHi and the severity of brux-ism. However, when respiratory effort–related arousals were added to the AHi, a statistically significant association was found. the bruxing events acted to protect the airway rather than
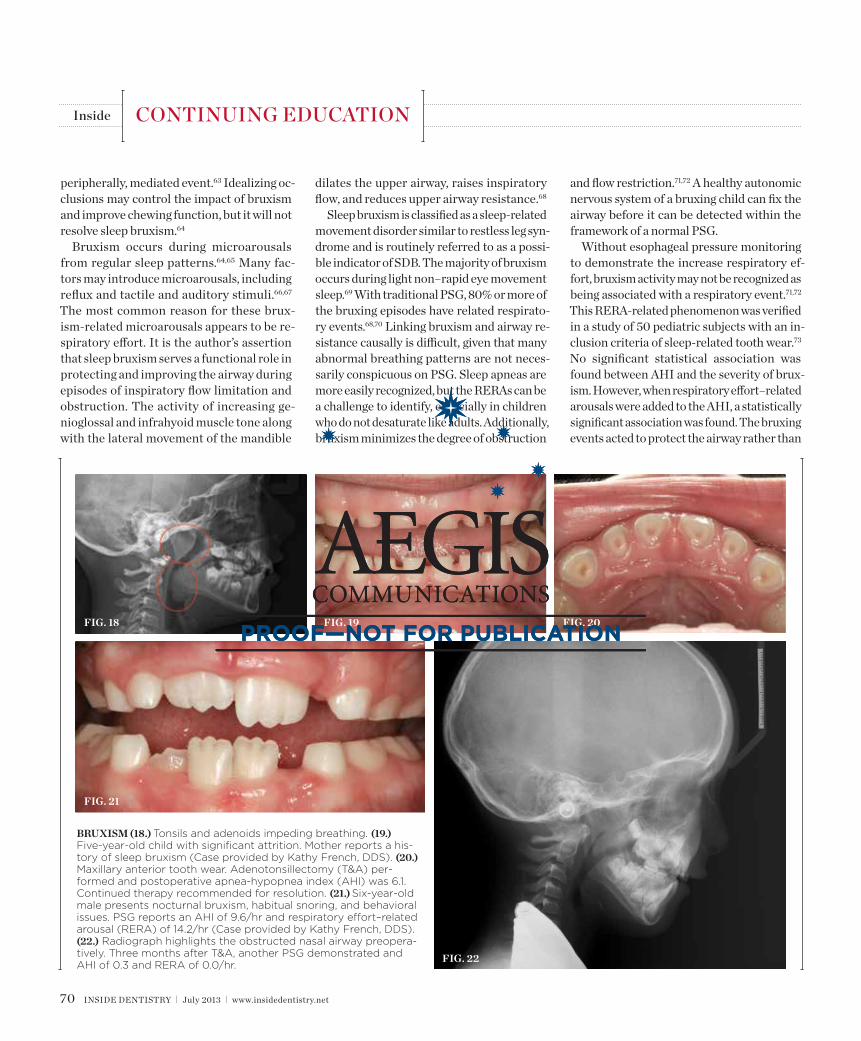
bruxism (18.) Tonsils and adenoids impeding breathing. (19.) Five-year-old child with significant attrition. Mother reports a his-tory of sleep bruxism (Case provided by Kathy French, DDS). (20.) Maxillary anterior tooth wear. Adenotonsillectomy (T&A) per-formed and postoperative apnea-hypopnea index (AHI) was 6.1. Continued therapy recommended for resolution. (21.) Six-year-old male presents nocturnal bruxism, habitual snoring, and behavioral issues. PSG reports an AHI of 9.6/hr and respiratory effort–related arousal (RERA) of 14.2/hr (Case provided by Kathy French, DDS). (22.) Radiograph highlights the obstructed nasal airway preopera-tively. Three months after T&A, another PSG demonstrated and AHI of 0.3 and RERA of 0.0/hr.
fig. 18
fig. 21
fig. 20
fig. 22
fig. 19
inside Continuing eDuCation

72 inside dentistry | July 2013 | www.insidedentistry.net
inside Continuing eDuCation
4. Bao G, Guilleminault C. Upper airway resistance syndrome—one decade later. Curr Opin Pulm Med. 2004;10(60):461-467.5. shahar e, Whitney CW, redline s, et al. sleep-disordered breathing and cardiovascular disease: cross-sectional results of the sleep heart health study. Am J Respir Crit Care Med. 2001;163(1):19-25.6. redline s. Morbidity, mortality, and public health burden of sleep apnea. in: Mcnicholas Wt, Phillipson eA, eds. Breathing Disorders in Sleep. London: WB saunders; 2002:222-235.7. Chen W, Kushida CA. nasal obstruction in sleep-disor-dered breathing. Otolaryngol Clin North Am. 2003;36(3) :437-460.8. Gold Ar, dipalo F, Gold Ms, Broderick J. inspiratory airflow dynamics during sleep in women with fibromyalgia. Sleep. 2004;27(3):459-466.9. Woodson Bt. expiratory pharyngeal airway ob-struction during sleep: a multiple element model. Laryngoscope. 2003;113(9):1450-1459.10. Walter LM, Foster AM, Patterson rr, et al. Cardiovascular variability during periodic leg movements in sleep in children. Sleep. 2009;32(8): 1093-1099.11. sullivan Ce, issa FG, Berthon-Jones M, eves L. reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;1(8225):862-865.12. Giles tL, Lasserson tJ, smith BJ, et al. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006;19(3): Cd001106.13. somiah M, taxin Z, Keating J, et al. sleep quality, short-term and long-term CPAP adherence. J Clin Sleep Med. 2012;8(5):489-500.14. tokunaga t, ninomiya t, Kato y, et al. Long-term compliance with nasal continuous positive airway pressure therapy for sleep apnea syndrome in an otorhinolaryngological office [published online ahead of print April 9 2013]. Eur Arch Otorhinolaryngol. http://link.springer.com/article/10.1007/s00405-013-2483-3#page-1. Accessed May 23, 2013.15. rouse Js. the bruxism triad: sleep bruxism, sleep disturbance, and sleep-related Gerd. Inside Dentistry. 2010;6(5):33-44.16. Lumeng JC, Chervin rd. epidemiology of pedi-atric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242-252.17. Chervin rd, Clarke dF, Huffman JL, et al. school performance, race, and other correlates of
sleep-disordered breathing in children. Sleep Med. 2003;4(1):21-27.18. Guilleminault C, Khramtsov A. Upper airway resistance syndrome in children: a clinical review. Semin Pediatr Neurol. 2001;8(4):207-215.19. Bonuck KA, Chervin rd, Cole tJ, et al. Prevalence and persistence of sleep disordered breathing symp-toms in young children: a 6-year population-based cohort study. Sleep. 2011;34(7):875-884.20. Piteo AM, Lushington K, roberts rM, et al. Prevalence of snoring and associated factors in in-fancy. Sleep Med. 2011;12(8):787-792.21. Archbold KH, Pituch KJ, Panahi P, Chervin rd. symptoms of sleep disturbances among chil-dren at two general pediatric clinics. J Pediatr. 2002;140(1):97-102.22. ivanenko A, Crabtree VM, Obrien LM, Gozal d. sleep complaints and psychiatric symptoms in chil-dren evaluated at a pediatric mental health clinic. J Clin Sleep Med. 2006;2(1):42-48.23. Li AM, Au Ct, ng sK, et al. natural history and predictors for progression of mild childhood obstruc-tive sleep apnoea. Thorax. 2010;65(1):27-31.24. O’Brien LM, Mervis CB, Holbrook Cr, et al. neurobehavioral correlates of sleep-disordered breathing in children. J Sleep Res. 2004;13(2):165-172.25. Barnes Me, Huss eA, Garrod Kn, et al . impairments in attention in occasionally snoring children: an event-related potential study. Dev Neuropsychol. 2009;34(5):629-649.26. Blunden s, Lushington K, Lorenzen B, et al. neuropsychological and psychosocial function in children with a history of snoring or behavioral sleep problems. J Pediatr. 2005;146(6):780-786.27. O’Brien LM, Mervis CB, Holbrook Cr, et al. neurobehavioral implications of habitual snoring in children. Pediatrics. 2004;114(1):44-49.28. Urschitz Ms, eitner s, Guenther A, et al. Habitual snoring, intermittent hypoxia, and impaired behavior in primary school children. Pediatrics. 2004;114(4): 1041-1048.29. Lopes MC, Guilleminault C. Chronic snoring and sleep in children: a demonstration of sleep disruption. Pediatrics. 2006;118(3);e741-e746.30. Barnes Me, Huss eA, Garrod Kn, et al . impairments in attention in occasionally snoring children: an event-related potential study. Dev Neuropsychol. 2009;34(5):629-649.31. Bonuck K, Freeman K, Chervin rd, Xu L. sleep-disordered breathing in a population-based cohort:
to resolve an obstruction. Bruxism should rise with UArs, habitual snoring, and occasion-al snoring, because negative pressure and respiratory effort drives the action. the re-searchers concluded that pediatric sleep-re-lated tooth wear could be used as a marker for sdB. Currently, no other healthcare provider is more equipped to evaluate and monitor pe-diatric nocturnal tooth wear than the dental practitioner (Figure 21 and 22).
Conclusionthe impact of sdB on the growing, snoring child can be serious, and sleep prosthodon-tics plays a unique role in screening and treat-ing these patients. dentists should screen children based on history and pediatric sleep questionnaire, as well as physical, intraoral, airway, and radiographic examination. it is important to note that dentists should not consider treatment in these children with-out a medical evaluation and possibly a sleep study. interdisciplinary treatment options must be reviewed within the context of the particular sleep breathing disorder, age of the patient, and level of cooperation of the child and the parents. Given its focus on MAAs, sleep dentistry is limited in treating the snor-ing child. sleep prosthodontics screens possi-ble OsA/UArs in children and acts as a con-duit of care, placing the patient in the proper medical, orthodontic, orthognathic, nutri-tionist/dietician, and/or oral mycology care for the best possible results. dentistry has a bigger role to play in sdB, and sleep prosth-odontics encapsulates that role.
References 1. Gill Ai, schaughency e, Galland BC. Prevalence and factors associated with snoring in 3-year olds: early links with behavioral adjustment. Sleep Med. 2012;13(9):1191-1197.2. Kurnatowski P, Putyński L, Lapienis M, Kowalska B. neurocognitive abilities in children with adeno-tonsillar hypertrophy. Int J Pediatr Otorhinolaryngol. 2006;70(3):419-424.3. Cho JG, Witting PK, Verma M, et al. tissue vibra-tion induces carotid artery endothelial dysfunction: a mechanism linking snoring and carotid atheroscle-rosis? Sleep. 2011;34(6):751-757.
inside Continuing eDuCation
behavioral outcomes at 4 and 7 years. Pediatrics. 2012;129(4):e857-e865.32. Gozal d, Pope dW Jr. snoring during early child-hood and academic performance at ages thirteen to fourteen years. Pediatrics. 2001;107(6):1394-1399.33. Bhattacharjee r, Kim J, Kheirandish-Gozal L, Gozal d. Obesity and obstructive sleep apnea syn-drome in children: a tale of inflammatory cascades. Pediatr Pulmonol. 2011;46(4):313-323. 34. Bhattacharjee r, Kheirandish-Gozal L, Pillar G, Gozal d. Cardiovascular complications of obstructive sleep apnea syndrome: evidence from children. Prog Cardiovasc Dis. 2009;51(5):416-433. 35. Kim J, Hakim F, Kheirandish-Gozal L, Gozal d. inflammatory pathways in children with insuf-ficient or disordered sleep. Respir Physiol Neurobiol. 2011;178(3):465-474.36. Hakim F, Gozal d, Kheirandish- Gozal L. sympathetic and catecholaminergic alterations in sleep apnea with particular emphasis on children. Front Neurol. 2012;3:7.37. Gozal d, Kheirandish-Gozal L, Bhattacharjee r, spruyt K. neurocognitive and endothelial dys-function in children with obstructive sleep apnea. Pediatrics. 2010;126(5):e1161-e1167.38. spicuzza L, Leonardi s, La rosa M. Pediatric sleep apnea: early onset of the ‘syndrome’? Sleep Med Rev. 2009;13(2):111-122. 39. Gozal d, serpero Ld, sans Capdevila O, Kheirandish- Gozal L. systemic inflammation in non-obese children with obstructive sleep apnea. Sleep Med. 2008;9(3):254-259. 40. Marcus CL, Brooks LJ, draper KA, et al. diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(5):576-584. 41. Guilleminault C, Khrammtsov A. Upper airway resistance syndrome in children: a clinical review. Semin Pediatr Neurol. 2001;8(4):207-215.42. enlow dH, Hans MG. Basic growth concepts. in: enlow dH, Hans MG, eds. Essentials of Facial Growth. Philadelphia, PA: WB saunders Company; 1996:18-38.43. Huang ys, Guilleminault C. Pediatric obstructive sleep apnea and the critical role of oral-facial growth: evidences. Front Neurol. 2012;3:1-7. 44. Kim JH, Guilleminault C. the nasomaxillary complex, the mandible, and sleep-disordered breath-ing. Sleep Breath. 2011;15(2):185-193.45. dempsey JA, skatrud JB, Jacques AJ, et al. Anatomic determinants of sleep-disordered breath-ing across the spectrum of clinical and nonclinical
Anything Else Means
COMPROMISE!
Though it's possible to get great results with some compositematerials, none exhibit the unique, patented, optical propertiesof HRi enamel. HRi eliminates the graying effect of increasedenamel thickness. It produces restorations with invisible marginsby design, while other systems involve complicated methodsthat still lead to metameric failure.
HRi makes it easier, faster and more predictableMaster technique, Basic technique and Enamel only technique,designed for all practices - for all composite restorations.
Todd C. Snyder, DDS, AAACDwww.drtoddsnyder.com
Laguna Niguel, CA
Intro kits starting at: $139www.micerium.synca.com
1 - 8 8 8 - 5 8 2 - 8 1 1 5i n C a n a d a : 1 - 8 0 0 - 6 6 7 - 9 6 2 2
by
HRi Inside Dentistry 2013-06_Layout 1 13-04-15 9:51 AM Page 1
(Circle75onReaderServiceCard)

male subjects. Chest. 2002;122(3):840-851.46. ruoff CM, Guilleminault C. Orthodontics and sleep-disordered breathing. Sleep Breath. 2012;16 (2):271-273.47. Juliano ML, Machado MA, de Carvalho LB, et al. Polysomnographic findings are associated with cephalometric measurements in mouth-breathing children. J Clin Sleep Med. 2009;5(6):554-561.48. Harvold eP, tomer Bs, Vargervik K, Chierici G. Primate experiments on oral respiration. Am J Orthod. 1981;79(4):359-372.49. solow B, skov s, Ovesen J, et al. Airway dimensions and head posture in obstructive sleep apnoea. Europ J Orthod. 1996;18(6):571-579.50. Güray e, Karaman Ai. effects of adenoidectomy on dentofacial structures: a 6-year longitudinal study. World J Orthod. 2002;3(1):73-81.51. Guilleminault C, stoohs r, Kim yd, et al. Upper airway sleep-disordered breathing in women. Ann Intern Med. 1995;122(7):493-501. 52. Marcus CL, Brooks LJ, draper KA, et al. diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(5):576-584.53. Zettergren-Wijk L, Forsberg CM, Linder-Aronson s. Changes in dentofacial morphology after adeno-/tonsillectomy in young children with obstructive sleep apnoea—a 5-year follow-up study. Eur J Orthod. 2006;28(4):319-326.54. Guilleminault C, Monteyrol PJ, Huynh nt, et al. Adeno-tonsillectomy and rapid maxillary distraction in pre-pubertal children, a pilot study. Sleep Breath. 2011;15(2):173-177.55. Oliveira de Felippe nL, da silveira AC, Grace Viana G, et al. relationship between rapid maxillary expansion and nasal cavity size and airway resistance: short- and long-term effects . Am J Orthod Dentofacial Orthop. 2008;134(3):370-382.56. Pirelli P, saponara M, Guilleminault C. rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004;27(4):761-766.57. Lavigne GJ, Manzini C, Kato t. sleep Bruxism. in: Kryger MH, roth t, dement WC, eds. Principles and Practice of Sleep Medicine. Philidelphia, PA: saunders; 2005:946-959.58. Carlsson Ge, egermark i, Magnusson t. Predictors of bruxism, other oral parafunctions, and tooth wear over a 20-year follow-up period. J Orofac Pain. 2003;17(1):50-57.59. van selms MK, Lobbezoo F, Wicks dJ, et al. Craniomandibular pain, oral parafunctions, and
www.e4d.com
SEE DENTISTRY IN A WHOLE NEW LIGHT.INTRODUCING
The Natural Evolution of Digital Dentistry
Super EasySuper AccurateSuper Fast
(Circle76onReaderServiceCard)

Rehabil. 2011;38(9):635-642.70. Kato t, thie nM, Huynh n, et al. topical review: sleep bruxism and the role of peripheral sensory influ-ences. J Orofac Pain. 2003;17(3):191-213.71. simmons JH, Prehn r. Airway protection: the missing link between nocturnal bruxism and obstructive sleep apnea. Paper presented at: 23rd Annual Meeting of the Associated Professional sleep societies; June 6-11, 2009; seattle, WA. Abstract A218.72. simmons JH, Prehn r. nocturnal bruxism as a protective mechanism against obstructive breathing during sleep. Paper presented at: 22rd Annual Meeting of the Associated Professional sleep societies; June 7-12, 2008; Baltimore, MA. Abstract A199.73. singh n, Chandwani B, Finkelmann M, et al. sleep bruxism-related tooth wear as a clinical marker for pediatric sleep-disordered breathing. Paper pre-sented at: 21st Annual American Academy of dental sleep Medicine Meeting; June 8, 2012; Boston, MA. Poster #015.
psychological stress in a longitudinal case study. J Oral Rehabil. 2004;31(8):738-745.60. Pierce CJ, Chrisman K, Bennett Me, Close JM. stress, anticipatory stress, and psychologic mea-sures related to sleep bruxism. J Orofac Pain. 1995;9 (1):51-56.61. seraidarian P, seraidarian Pi, das neves Cavalcanti B, et al. Urinary levels of catecholamines among individuals with and without sleep bruxism. Sleep Breath. 2009;13(1):85-88.62. Zhang J, Ma rC, Kong AP, et al. relationship of sleep quantity and quality with 24-hour urinary cate-cholamines and salivary awakening cortisol in healthy middle-aged adults. Sleep. 2011;34(2):225-233.63. Gastaldo e, Quatrale r, Graziani A, et al. the excitability of the trigeminal motor system in sleep bruxism: a transcranial magnetic stimula-tion and brainstem reflex study. J Orofac Pain. 2006;20(2):145-155.64. Lavigne GJ, Khoury s, Abe s, et al. Bruxism
physiology and pathology: an overview for clinicians. J Oral Rehabil. 2008;35(7):476-494. 65. Khoury s, rouleau GA, rompré PH, et al. A signifi-cant increase in breathing amplitude precedes sleep bruxism. Chest. 2008;134(2):332-337.66. Miyawaki s, Lavigne GJ, Pierre M, et al. Association between sleep bruxism, swallowing-related laryngeal movement, and sleep positions. Sleep. 2003;26(4):461-465.67. Kato t, Montplaisir Jy, Guitard F, et al. evidence that experimentally induced sleep bruxism is a consequence of transient arousal. J Dent Res. 2003;82(4):284-288.68. Krieger J. Breathing in normal subjects. in: Kryger MH, roth t, dement WC, eds. Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia, PA: WB saunders Company; 2000:229-241. 69. Carra MC, rompré PH, Kato t, et al. sleep brux-ism and sleep arousal: an experimental challenge to assess the role of cyclic alternating pattern. J Oral
inside Continuing eDuCation
* 10 miniMARK Implants need to be on the same invoice. Not to be combined with any other discounts or promotions. Offer expires August 31, 2013.
ACE Surgical Supply Co., Inc. 1.800.441.3100 miniMARKimplants.com
BUY 10 miniMARK IMPLANTS GET THE SURGICAL KIT FREE*
miniMARK® ® and
Now it’s possible for you to offer reliable, predictable, same-day small-diameter implants to your patients who are denture wearers. The miniMARK® Dental Implant System is an affordable option for denture wearers. Precision engineered by ACE Surgical, it is the world’s first small-diameter implant system to feature the renowned LOCATOR® Attachment.
Give your DeNTure weariNG paTieNTs The seCuriTy They Deserve wiTh every sMiLe.
(Circle78onReaderServiceCard)
78 inside dentistry | July 2013 | www.insidedentistry.net
COntinUinG edUCAtiOn quizto take this quiz, log on to www.insidedentistry.net
or fill out and mail the answer form on the next page.
aEgis Publications, LLC, is an aDa CErP recognized Provider. aDa CErP is a service of the american Dental association to assist dental professionals in identifying quality providers of continuing dental education. aDa CErP does not approve or endorse individual courses or instructors, nor does it imply accep-tance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to aDa CErP at www.ada.org/cerp. Program Approval for
Continuing Education
approved PaCE Program Provider FagD/MagD Credit approval does not imply acceptance by a state or provincial board of dentistry or agD endorsement 1/1/2013 to 12/31/2016. Provider iD# 20972
Sleep Prosthodontics: A New Vision for DentistryJeffrey S. Rouse, DDS
AeGis Publications, LLC, provides 2 hours of Continuing education credit for this article. We are pleased to offer two options for participating in this Ce lesson. By visiting www.insidedentistryCe.com, you can take the quiz for $16 and print your certificate immediately, or you can fill out and mail the Answer sheet on the next page for $32. (note: for the mail-in option the answer sheet must be completely filled out and include your name and payment information in order to be valid.) For more information, call 877-4-AeGis-1.
Please complete the answer Form on page 80, including your name and payment information.
sleep disordered breathing (sDb) encompasses a spectrum of dysfunctional sleep breathing, including:
a. habitualsnoring. b. upperairwayresistancesyndrome(UARS). C. sleepapnea. D. alloftheabove.
Osa is characterized by complete upper airway obstructions:
a. lastinglongerthan4secondswith10%oxygendesaturation. b. lastinglongerthan10secondswith4%oxygendesaturation. C. lastinglongerthan6secondswith6%oxygendesaturation. D. lastinglessthan15secondswith5%oxygendesaturation.
according to the author, sleep dentistry can be thought of as the study of:
a. anoralappliance(OA)anditsimpactontheairway. b. polysomnography(PSG). C. thewayocclusionaffectssleep. D. continuouspositiveairwaypressure(CPAP).
sleep prosthodontics is the study of:
a. UARS,butnotOSA. b. occlusionandcentricrelation. C. theairwayanditsimpactonthestomatognathicsystem. D. SDBinwomen.
in the general population, what percentage of children has apnea?
a. 2%to3% b. 4%to5% C. 6%to7% D. 8%to10%
Habitually snoring children are at higher risk for:
a. socialproblems. b. pooracademicperformance. C. decreasedattention. D. alloftheabove.
sleep disturbances in children lead to sympathetic nervous activation that creates:
a. cardiovascularandpulmonaryproblems. b. cardiovascularandmetabolicinjury. C. metabolicandpulmonarydevelopmentaldelays. D. growthproblemsandsocial-emotionalissues.
beginning sleep prosthodontics indicators of sDb are craniofacial anomalies resulting in:
a. alow,narrowpalate. b. congenitaledentulism. C. malocclusions. D. ankyloglossia.
the normal distance from the adenoids to the soft palate for an acceptable airway should be:
a. atleast15mm. b. between8and10mm. C. nomorethan10mm. D. atleast12mm.
With traditional Psg, what percentage of bruxing episodes is related to respiratory events?
a. 80% b. 65% C. 50% D. 35%
80 inside dentistry | July 2013 | www.insidedentistry.net
july 2013sleep Prosthodontics: a new vision for Dentistry
COntinUinG edUCAtiOn MaiL in ansWEr FOrM
to use our mail-in option, please completely fill out the Answer Form and mail it along with your payment of $32 to the address provided below. note: this form must be com-pletely filleD out anD incluDe your name anD payment information in orDer to be processeD anD creDit awarDeD. your test will be graded
and your certificate will be sent to you in the mail; please allow approximately 2 to 3 weeks for processing. Course valid from 7/2/13 to 8/31/16.
1 a b C D
2 a b C D
3 a b C D
4 a b C D
5 a b C D
6 a b C D
7 a b C D
8 a b C D
9 a b C D
10 a b C D
CHECk(payabletoAEGISCommunications) CrEDit CarDPleasecompleteinformationandsignbelow:
Card number Expiration Date: Month/Year Cvv Code:
visa Mastercard total amount ($32pertest)
signaturE DatE
Last 4 Digits OF ssn aDa number agD number
the Month and Day (notyear) of birth. Example, February 23 is 02/23 Month/Date of birth
NAmE
ADDRESS
CITy E-mAIlADDRESS
STATEzIPDAyTImEPhONE
Pleasemailcompletedformswithyourpaymentto:AEGISCommunicationsCEDepartment,104PheasantRun,Suite105,Newtown,PA18940
SCORINGSERVICES:Bymail|Fax:215-504-1502|Phone-in:877-423-4471(9am-5pmET,monday-Friday)CustomerServiceQuestions?PleaseCall877-423-4471
1.Clarityofobjectives 43210
2.Usefulnessofthecontent 43210
3.Benefittoyourclinicalpractice 43210
4.Usefulnessofthereferences 43210
5.Qualityofthewrittenpresentation 43210
6.Qualityoftheillustrations: 43210
7.Clarityofreviewquestions 43210
8.Relevanceofreviewquestions 43210
9.Didthislessonachieveitseducationalobjectives?yesNo
10.Didthisarticlepresentnewinformation? yesNo
11.howmuchtimedidittakeyoutocompletethislesson? min
/
PrOgraM EvaLuatiOn
Pleasecircleyourlevelofagreementwiththefollowingstatements.(4=StronglyAgree;0=StronglyDisagree)





























