Embed Size (px)
Citation preview
SEPTEMBER 2018 | INSERT TO RE TINA TODAY 37
INSERT TO
SEPTEMBER 2018 VOL. 16, NO. 6 SPONSORED BY TOPCON
INTRODUCTIONOCT imaging has become an indispensable tool in uveitis
practice. It is the standard diagnostic technique in the detection, monitoring of treatment, and determination of prognosis in uveitic macular edema (ME) as well as in other macular and extramacular inflammatory changes. OCT technology has evolved in the last 2 decades from time domain OCT (TD-OCT) to spectral domain OCT (SD-OCT) and recently to the enhanced-depth imaging OCT (EDI-OCT) and Topcon’s Swept Source OCT (SS-OCT).1
The innovation of SS-OCT, introduced in clinical practice in 2012, provides several advantages over SD-OCT.2 These include
1. higher resolution;2. improved penetration through opacities, including vitreous
haze and cataract;3. faster acquisition times; and4. greater depth and breadth of imaging. This allows the simultaneous detailed documentation of all
structures, including vitreoretinal interface, retinal layers, retinal pigment epithelium (RPE), and choroid.2
We have been using the Topcon high-resolution SS-OCT system in our department for more than 2 years. This allows for improved qualitative and quantitative assessment of uveitis-related posterior segment changes and for a better understanding of distinct chang-es at the vitreoretinal interface, inner and outer retinal layers, and choroid that are specific to various inflammatory entities.
SS-OCT FOR UVEITIC ME AND OTHER MACULAR COMPLICATIONSSS-OCT enables noninvasive, objective, and precise detection,
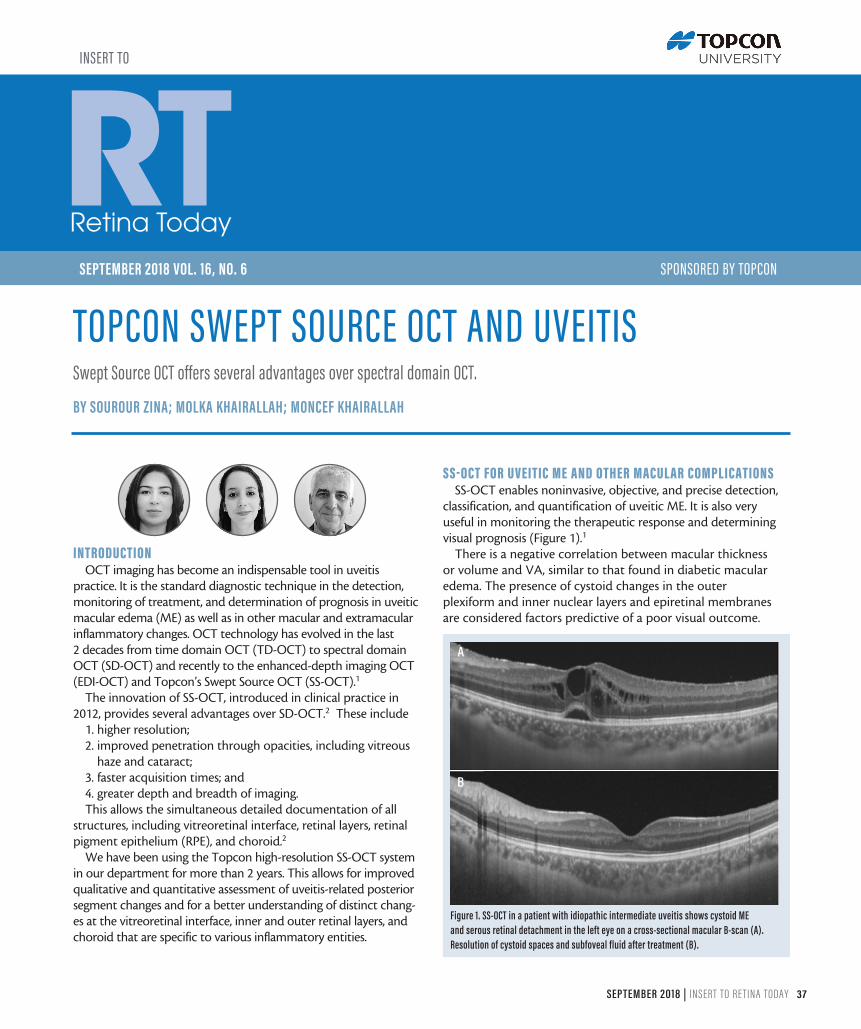
classification, and quantification of uveitic ME. It is also very useful in monitoring the therapeutic response and determining visual prognosis (Figure 1).1
There is a negative correlation between macular thickness or volume and VA, similar to that found in diabetic macular edema. The presence of cystoid changes in the outer plexiform and inner nuclear layers and epiretinal membranes are considered factors predictive of a poor visual outcome.
Figure 1. SS-OCT in a patient with idiopathic intermediate uveitis shows cystoid ME and serous retinal detachment in the left eye on a cross-sectional macular B-scan (A). Resolution of cystoid spaces and subfoveal fluid after treatment (B).
A
B
Swept Source OCT offers several advantages over spectral domain OCT.
BY SOUROUR ZINA; MOLKA KHAIRALLAH; MONCEF KHAIRALLAH
TOPCON SWEPT SOURCE OCT AND UVEITIS

TOPCON SWEPT SOURCE OCT AND UVEITIS
38 INSERT TO RE TINA TODAY | SEPTEMBER 2018
Exudative retinal detachment (ERD) is associated with lower initial VA but higher rates of ME resolution and VA increase. Loss or disruption of the ellipsoid zone (EZ, also called photoreceptor IS/OS junction line) is associated with increased risk of macular atrophy and worse VA.1,2
SS-OCT is also an essential tool for detecting uveitic macular changes other than ME, including epiretinal membrane forma-tion, vitreomacular traction, foveal atrophy, and lamellar or full-thickness macular hole. Macular atrophy is associated with longer disease duration and worse VA.1,2
DIAGNOSING AND MONITORING OF INFECTIOUS AND NONINFECTIOUS RETINITIS WITH SS-OCT
SS-OCT enables accurate detection, characterization, and monitoring of vitreous and retinal changes associated with infectious or noninfectious retinitis or retinochoroiditis, includ-ing toxoplasmosis, toxocariasis, viral retinitis, fungal retinitis, and Behçet uveitis (Figure 2).1,3
DIAGNOSING AND MONITORING OF OUTER RETINAL AND CHOROIDAL DISEASE WITH SS-OCT
Various specific changes in the outer retina can be clearly identified by SS-OCT in white dot syndromes, such as multiple evanescent white dot syndrome (MEWDS), acute posterior multifocal placoid pigment epitheliopathy (APMPPE), idio-pathic multifocal choroiditis, punctate inner choroiditis, and serpiginous choroiditis. They mainly include disruption of the EZ, hyperreflective areas overlying the RPE, and RPE alterations. Hyperreflective lesions gradually resolve over time, with partial or complete restoration of the EZ (Figure 3).1
SS-OCT is an essential tool in the diagnosis and monitoring of response to treatment in patients with acute Vogt-Koyanagi-Harada disease.4 Key SS-OCT findings include multifocal ERD,
subretinal hyperreflective dots, subretinal septa, retinal/RPE folds, and choroidal thickening (Figure 4).1,4 Accurate evaluation of choroidal inflammatory changes thanks to SS-OCT is also essen-tial for other inflammatory entities including sympathetic oph-thalmia, posterior scleritis, and Birdshot chorioretinopathy.1
ASSESSING AN INFLAMMATORY REACTION WITH SS-OCT Recent data show that SS-OCT may allow qualitative and
quantitative analysis of anterior chamber and vitreous inflam-matory reaction. It may be useful as a quantitative and objec-tive marker of disease activity and treatment response, espe-cially in eyes with corneal haze or edema.5
SS-OCT-A TECHNOLOGYOCT angiography (OCT-A) using SS technology (SS-OCT-A)
is a new noninvasive imaging modality, allowing the mapping of the retinal and choroidal microvasculature by calculating motion contrast in OCT B-scans acquired repeatedly at the same location. It is particularly useful in the diagnosis and management of retinal vasculitis, choriocapillaritis, and
Figure 2. Color fundus photograph in a patient with Behçet uveitis in the left eye shows an inferonasal macular retinal infiltrate (A). SS-OCT B-scan image shows a corresponding focal inner retinal hyperreflectivity and thickening (B). After complete resolution of the retinal infiltrate, there is no visible scar, but a focal retinal nerve fiber defect becomes evident (white arrows) (C), with a corresponding localized inner retinal atrophy on SS-OCT (white arrow) (D).
Figure 3. Color fundus photograph in a patient with MEWDS in the left eye shows coalescent deep white retinal lesions with macular granularity (A). SS-OCT of the same eye shows disruption of the EZ, irregularities of the RPE, and hyperreflective material resting on the RPE and extending anteriorly (yellow arrows) (B). Resolution of the hyperreflective material, with near complete restoration of the EZ, is observed 3 months after initial presentation (C).
Figure 4. SS-OCT of the left and right eyes in a patient with acute Vogt-Koyanagi-Harada disease shows multifocal exudative retinal detachment, subretinal hyperreflective dots, subretinal septa, and choroidal thickening leading to RPE undulations in both eyes (A and B). SS-OCT shows complete resolution of the ERD, RPE undulations, and choroidal thickening after high-dose systemic corticosteroid treatment (C and D).
A A
A
C
B B
B
D
C
C D

TOPCON SWEPT SOURCE OCT AND UVEITIS
SEPTEMBER 2018 | INSERT TO RE TINA TODAY 39
inflammatory choroidal neovascularization. SS-OCT-A was found to be better than fluorescein angiography in detecting and characterizing perifoveal microvascular changes in eyes with Behçet uveitis, with the deep capillary plexus being more severely affected than the superficial capillary plexus (Figure 5).6
CONCLUSION
OCT has become an essential component of the multimodal imaging approach for the diagnosis and management of inflam-matory chorioretinal diseases. The recent advent of SS-OCT has provided significant advantages over SD-OCT, allowing for improved qualitative and quantitative assessment of posterior segment changes associated with uveitis, including ME, other macular complications, inner and outer retinal structural altera-tions, and choroidal inflammation.
OCT-A using SS technology is a new noninvasive and dyeless imaging modality that provides a detailed, 3D mapping of retinal
and choroidal microvasculature. SS-OCT-A is particularly useful for the diagnosis and management of retinal vasculitis, chorio-capillaritis, and inflammatory choroidal neovascularization. n
1. Onal S, Tugal-Tutkun I, Neri P, P Herbort C. Optical coherence tomography imaging in uveitis. Int Ophthalmol. 2014;34(2):401-435.2. Lavinsky F, Lavinsky D. Novel perspectives on swept-source optical coherence tomography. Int J Retina Vitreous. 2016;2:25.3. Chen KC, Jung JJ, Engelbert M. Single acquisition of the vitreous, retina and choroid with swept source optical coherence tomography in acute toxoplasmosis. Retin Cases Brief Rep. 2016;10(3):217-220.4. Chee SP, Chan SN, Jap A. Comparison of enhanced depth imaging and swept source optical coherence tomography in assessment of choroidal thickness in Vogt-Koyanagi-Harada disease. Ocul Immunol Inflamm. 2017;25(4):528-532.5. Invernizzi A, Marchi S, Aldigeri R, et al. Objective quantification of anterior chamber inflammation: measuring cells and flare by anterior segment optical coherence tomography. Ophthalmology. 2017;124(11):1670-1677.6. Khairallah M, Abroug N, Khochtali S, et al. Optical coherence tomography angiography in patients with Behçet uveitis. Retina. 2017;37(9):1678-1691.
SOUROUR ZINAn Department of Ophthalmology, Fattouma Bourguiba University Hospital, Faculty of
Medicine, University of Monastir, Tunisian [email protected] Financial disclosure: None
MOLKA KHAIRALLAHn Department of Ophthalmology, Fattouma Bourguiba University Hospital, Faculty of
Medicine, University of Monastir, Tunisian [email protected] Financial disclosure: None
MONCEF KHAIRALLAH n Department of Ophthalmology, Fattouma Bourguiba University Hospital, Faculty of
Medicine, University of Monastir, Tunisian [email protected] Financial disclosure: Speaker (Topcon)
Figure 5. SS-OCT angiography of the right eye in a patient with Behçet uveitis showing well-delineated hypointense grayish areas of retinal capillary nonperfusion associated with capillary telangiectasias. The deep capillary plexus (B) is more severely involved than the superficial capillary plexus (A).
A B













![Welcome [] · 2019. 7. 31. · Shipper ID: 00000000 Insert #1 Insert #2 Shipping Method: 2ND DAY Insert #3 Insert #4 CARRIER: UPS Insert #5 Insert #6 Address: Insert #7 Insert #8](https://img.pdfslide.us/doc/110x75/606af0d80d38412add396492/welcome-2019-7-31-shipper-id-00000000-insert-1-insert-2-shipping-method.jpg)

![· Web view2020. 12. 29. · [insert 2018 plan name]3. Índice. Evidencia de cobertura de 2018 para [insert 2018 plan name] 154. Capítulo 6.Lo que le corresponde pagar por los](https://img.pdfslide.us/doc/110x75/613c86174c23507cb635703a/web-view-2020-12-29-insert-2018-plan-name3-ndice-evidencia-de-cobertura.jpg)
![Web view · 2018-02-15Dear Proponent, [if applicable, insert: Invitation N°..; Loan N° ..] [insert: Location and Date] [insert: Name and Address of Consultant] Dear Proponent.:](https://img.pdfslide.us/doc/110x75/5aa607377f8b9ae7438e4921/web-view2018-02-15dear-proponent-if-applicable-insert-invitation-n-loan.jpg)





![· Web view2020. 12. 29. · [insert 2018 plan name]50. Capítulo 2. Números de teléfono y recursos importantes. Evidencia de cobertura de 2018 para [insert 2018 plan name] 76](https://img.pdfslide.us/doc/110x75/613736180ad5d20676487946/web-view-2020-12-29-insert-2018-plan-name50-captulo-2-nmeros-de-telfono.jpg)

![[INSERT SPEAKER’S NAME] [INSERT TITLE] [INSERT DATE]](https://img.pdfslide.us/doc/110x75/56812c68550346895d90fff9/insert-speakers-name-insert-title-insert-date-5685c9ae3d2da.jpg)

![Facilitator: [Insert name] Date: [Insert] Venue: [Insert] Wellcome !](https://img.pdfslide.us/doc/110x75/56649dd05503460f94ac59be/facilitator-insert-name-date-insert-venue-insert-wellcome-.jpg)

![[Insert House of Worship Name] Emergency operations plan Template · 2018-11-07 · 1 | (insert name of house of worship) Emergency Operations Plan (Insert Year) TABLE OF CONTENTS](https://img.pdfslide.us/doc/110x75/5ed121eac910782603754f03/insert-house-of-worship-name-emergency-operations-plan-2018-11-07-1-insert.jpg)