Embed Size (px)
Citation preview

10/13/2017
1
The potential effects of exercise “dose” on functional recovery in patients with physical
disabilities: Introduction
T. George Hornby, PT, PhD
Research Scientist, Professor
Physical Medicine and Rehabilitation
Indiana University School of Medicine
Rehabilitation Hospital of Indiana
Acknowledgements• Locomotor Recovery Laboratory
• Abi Leddy, DPT, MSCI, NCS
• Jane Woodward, DPT, NCS
• Jennifer Kahn, DPT, NCS
• Kristan Leech DPT
• Mark Connolly, BS
• Catherine Kinnaird, MS
• Gordhan Mahtani, MS
• Collaborators/Colleagues• Michael Lewek, PT, PhD
• Catherine Lang, PT, PhD
• Darcy Reisman, PT, PhD
• RIC Physical Therapists• Nicole Williams DPT
• Ryan Pelo DPT
• Raquel Santiago DPT
• Mike Klonowski DPT, PCS
• Heather Scholten, DPT
• Holly Paczan, DPT
• Deb Tobias, DPT
• Administrators/Physicians• Elliot Roth, MD
• Richard Harvey, MD
• Linda Lovell, BS
• Kara Kozub, MS
• Jennifer Smith, MS
• Nicole Sedam, OTL/R
Walking the Walk . . .
• Introduction – Theory and Rationale
• Development and Application of a Training Paradigm
• Briefly . . . Knowledge Translation Strategies and Clinical Implementation

10/13/2017
2
Outline
• Introduction – Theory and Rationale• Patient’s goals• Constraints of PT practice• Rationale for specific training strategies• Fundamentals for application
• Development and Application of a Training Paradigm
• Knowledge Translation Strategies
• Implementation
Patient’s Goals
“I want to go out to the store on my own”
“My leg is weak, I want to get stronger”
“I’m not going to church with this cane!!”
“I can’t get my feet underneath me!!”
”I walk like a pimp . .. . … I’m not a pimp!!”
Constraints of PT Practice
COORDINATION
STRENGTH
BALANCE
SPASTICITY
FLEXIBILITY
Locomotion

10/13/2017
3
Constraints of PT Practice
COORDINATION
STRENGTH
BALANCE
SPASTICITY
FLEXIBILITY
Locomotion Standing StairsTransfersWheelchair
COORDINATION
STRENGTH
BALANCE
SPASTICITY
FLEXIBILITY
Locomotion Standing StairsTransfersWheelchair
Constraints of PT Practice
Constraints of PT Practice
We’re looking for someone who can stretch with this job? Are you flexible?
??

10/13/2017
4
Distribution of PT Activities• Practice of multiple activities to improve multiple impairments/functional limitations
• Derived from outpatient observations (Moore et al, 2010, Stroke)
• # specific task repetitions during clinical therapy (Lang et al 2009, APMR) Gait 357
Steps/stairs 36Balance 27
Active LE exercise 27
Passive LE exercise 12Transfers 11
UE exercise 12
• Minimize abnormal movement patterns– Normalize motor patterns
– Decrease Intensity = risk for cardiovascular event, decrease spasticity(Mackay 2003, Kline 2007)
• Standardized progression of task difficulty
Constraints of PT practice: tradition/education
Stability Mobility
Limited variability
Increased variability
Constrained environment
Unconstrained Environment
Outline
•Introduction – Theory and Rationale• Patient’s goals• Constraints of PT practice• Rationale for specific training strategies• Fundamentals for application
•Development and Application
•Knowledge Translation
• Implementation

10/13/2017
5
Rationale for specific training interventions• Specific factors that influence neuroplasticity (Kleim and Jones 2008)
1. Use it or lose it2. Use it and improve it3. Specificity Matters4. Repetition Matters5. Intensity Matters
6. Time Matters7. Salience Matters 8. Age Matters9. Transference10. Interference
Rationale for specific training interventions• Specific factors that influence neuroplasticity (Kleim and Jones 2008)
• Similar practice paradigms in fields of motor control and exercise physiology
• Similar determinants for cardiovascular and muscular plasticity
1. Use it or lose it2. Use it and improve it3. Specificity Matters4. Repetition Matters5. Intensity Matters
6. Time Matters7. Salience Matters 8. Age Matters9. Transference10. Interference
Common themes of previous and emerging evidence

10/13/2017
6
Common themes of previous and emerging evidence
Contributions of Specificity of Practice
• Stepping practice improves stepping performance • Animals (vs no interventions or standing): Deleon 1998, 1999
• Humans: SCI ‐ Wernig et al 1995, Stroke ‐ Hesse et al 1995
• Non‐stepping practice• Balance training improves balance (Au‐Yeung, Hui‐Chan et al 2009)
• Strength training improves strength (Patten et al 2004; Jayaraman et al 2013)
• Smaller effects on walking
Contributions of Amount of Practice
• Animal studies ‐ 1000 steps > 100 steps; Cha et al 2007
• Human studies – 2000‐6000 steps; Moore et al 2010, Pohl et al 2002, Sullivan et al 2002

10/13/2017
7
Contributions of Amount of Practice
• Animal studies ‐ 1000 steps > 100 steps; Cha et al 2007
• Human studies – 2000‐6000 steps; Moore et al 2010, Pohl et al 2002, Sullivan et al 2002
Dose Response
Clinical PT Locomotor Training
Contributions of Amount of Practice
• Animal studies ‐ 1000 steps > 100 steps; Cha et al 2007
• Human studies – 2000‐6000 steps; Moore et al 2010, Pohl et al 2002, Sullivan et al 2002
Clinical PT Locomotor Training
Dose Response
Contributions of Intensity of Practice
•Aerobic treadmill walking improves selected walking measures (Macko 2005, Moore 2010, Globas 2012)
• Fastest speeds (Sullivan 2002, Pohl 2002)• Greater neuromuscular demands (Hornby 2008, Holleran 2015)
• Lower stepping intensities may not generate sufficient gains in stepping (Duncan 2011)

10/13/2017
8
Implementation of large amounts of high intensity stepping practice•Benefits (Macko 2005, Moore 2010, Globas 2012)
• Consistent improvements in 6 min walk test• Consistent improvements in aerobic capacity or gait economy
• Limitations (Macko 2005, Moore 2010, Globas 2012)
• Inconsistent changes in comfortable walking speed and community stepping• Small improvements in balance• Limited improvements in transfers
What else you got?
• Errors and variability are important in learning − Variable vs Constant Practice− Random vs Blocked Practice (i.e., Contextual Interference)
− Greater errors associated with allowing variability
Other factors?
• Types of variability− Kinematic variability (Cai 2007; Hornby 2008, Lewek 2009)
Contributions of errors and variability to learning

10/13/2017
9
• Types of variability− Kinematic variability (Cai 2007; Hornby 2008, Lewek 2009)
Contributions of errors and variability to learning
Hornby et al Stroke 2008
• Types of variability− Kinematic variability (Cai 2007; Hornby 2008, Lewek 2009)
Contributions of errors and variability to learning
Hornby et al Stroke 2008
0
2
4
-2
-4
-6
0
2
4
-2
-4
6
**
% single limb stance Step length asymmetry
Therapist‐assisted Robotic‐assisted
• Types of variability− Kinematic variability (Cai 2007; Hornby 2008, Lewek 2009)
− Environmental variability – overground/stairs (van den Brand 2012)
− Task variability – forward vs sideways vs backwards (Shah 2012)
Contributions of errors and variability to learning

10/13/2017
10
• Augmenting errors during learning may enhance magnitude/accelerate learning (split‐belt treadmill stepping; Bastian 2006, Reisman 2010)
• Tailoring errors for other walking subcomponents?• Limb swing?• Propulsion?• Postural stability/balance?
Contributions of errors and variability to learning
Outline
• Introduction – Theory and Rationale• Patient’s goals• Constraints of PT practice• Rationale for specific training strategies• Fundamentals for application
•Development and Application
•Knowledge Translation
• Implementation
Outline
•Introduction – Theory and Rationale• Patient’s goals
• Constraints of PT practice
• Rationale for specific training strategies
• Fundamentals for application
•Development and Application
•Knowledge Translation
•Implementation

10/13/2017
11
How can we apply what we know?
Priorities and sacrifices If realistic goal is to improve walking function . . .
. . . need to focus on walking activities
Intensity of interventions High training intensity as safe as regular PT (Pang 2013) Does spasticity increase over long‐term? (Wirz 2005)
Allowing/encouraging errors and variability What they look like may be okay? Variable stepping may improve other functions (Horn 2005)
How can we apply what we know?
Intensity of interventions High training intensity as safe as regular PT (Pang 2013) Does spasticity increase over long‐term? (Wirz 2005)
Allowing/encouraging errors and variability What they look like may be okay? Variable stepping may improve other functions (Horn 2005)
How can we apply what we know?
Stability
Limited variability
Constrained environment
Mobility
Increased variability
Unconstrained Environment

10/13/2017
12
Outline
• Introduction – Theory and Rationale
• Development and Application of a Training Paradigm
• Knowledge Translation Strategies
• Implementation
Outline
• Introduction – Theory and Rationale
• Development and Application• Developing the Training Program
• Preliminary study
• Randomized Clinical Trial
• Knowledge Translation
• Implementation
Development of Training Paradigm
• Large Amounts of Task Specific Practice• Focus on continuous reciprocal stepping
• Focus only on continuous reciprocal stepping
• Aerobic intensity • Training HR zone (THR) = 70‐80% Heart Rate Reserve (HRR)
• 15‐18 BORG Ratings of Perceived Exertion (RPE)
• Variability • Multidirectional stepping
• Multiple environments
• Random order practice

10/13/2017
13
Focus Only on Stepping
• Biomechanical subcomponents of walking
(Holleran, NNR 2014, appendix)
• Defining Successful walking
Success = Continuous steppingFailure= 3‐5 consecutive errors
Gait kinematics were not a primary concern
– Positive step length
– Directional advancement
– Preventing limb/trunk collapse
– Lateral/frontal stability – Maintain upright
– Limb swing advancement
– Propulsion
– Stance control
Progressing Biomechanical Subcomponents of Walking
PropulsionLimb
AdvancementStability & Balance
Stance Control
Outline
• Introduction – Theory and Rationale
• Development and Application• Developing the Training Program
• Preliminary study• Study Design
• Intervention description
• Results
• Randomized Clinical Trial
• Knowledge Translation
• Implementation

10/13/2017
14
• Subjects: • Subacute (1‐6mo) and chronic stroke (>6mo) • 18‐75yo• MMSE score ≥23/30• Moderate assistance or better to ambulate < 0.9
m/s self‐selected walking speed (SSV)
(Holleran, NNR 2014)
Feasibility and Efficacy of High Intensity Variable Stepping Training : Pilot Study
Pilot Study: Intervention Protocol
• Target 40 1hour sessions over 8‐10 weeks
• Week 1‐2: Forward treadmill training
• Weeks 3‐8: Variable, multi‐directional training• Half treadmill: 25% speed training, 25% dynamic balance
• Half overground: 25% speed/balance, 25% stairs
Methods: Design & Outcome Measures
• 6 Minute Walk Test (6MWT)
• Overground gait speed
• Self‐selected velocity (SSV)
• Fastest velocity (FV)
• Spatiotemporal gait symmetry
• Single limb stance time (%)
• Step length symmetry (%)
• Daily stepping activity
• Stepwatch Accelerometers worn during all waking hours
• 5‐14 days Pre/Post intervention
• Within‐session intensity measures(HR, RPE)
Chronic
Subacute

10/13/2017
15
Progressing Biomechanical Subcomponents of Walking
PropulsionLimb
AdvancementStability & Balance
Stance Control
Progressing Biomechanical Subcomponents of Walking
Limb Advancement
PropulsionStability & Balance
Stance Control
Progressing Biomechanical Subcomponents of Walking
Limb Advancement
PropulsionStability & Balance
Stance Control

10/13/2017
16
Progressing Biomechanical Subcomponents of Walking
Limb Advancement
PropulsionStability & Balance
Stance Control
Progressing Biomechanical Subcomponents of Walking
Limb Advancement
PropulsionStability & Balance
Stance Control
Results: Stepping Activity
Average step/session chronic (n=12) : 2967 ± 722
Average step/session sub‐acute (n=10) : 2845 ± 869
Significant changes in “real world” stepping (Pre‐BSL to F/U testing)
10/13/2017
17
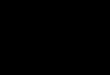
Primary locomotor outcomes
•SSV: chronic = 0.23 m/s; subacute = 0.33 m/s (ES=1.34, 1.64)
•MCID= 0.16m/s
• 6MWT: chronic = 90m subacute = 144m, (ES=1.49, 1.47)•MCID=50m
Primary locomotor outcomes
No relation between initial walking status and improvements
Relationship between stepping dosage vs primary outcomes
Gait kinematics (spatiotemporal and joint excursions)• Improved stride length/cadence and gait symmetry• Δ paretic single limb stance (% gait cycle; FV); 21±8.7 to 27±7.1** (normal is 40%)
• Average Δ step length symmetry (FV): 63±35 to 82±10%* (normal is 100%)
• Increased hip/knee ROM, consistency
• Frontal plane• increase in swing‐phase hip abduction (p<0.05)
• greatest increase in those with higher gait speed gains and lower initial Fugl‐Meyer
10/13/2017
18
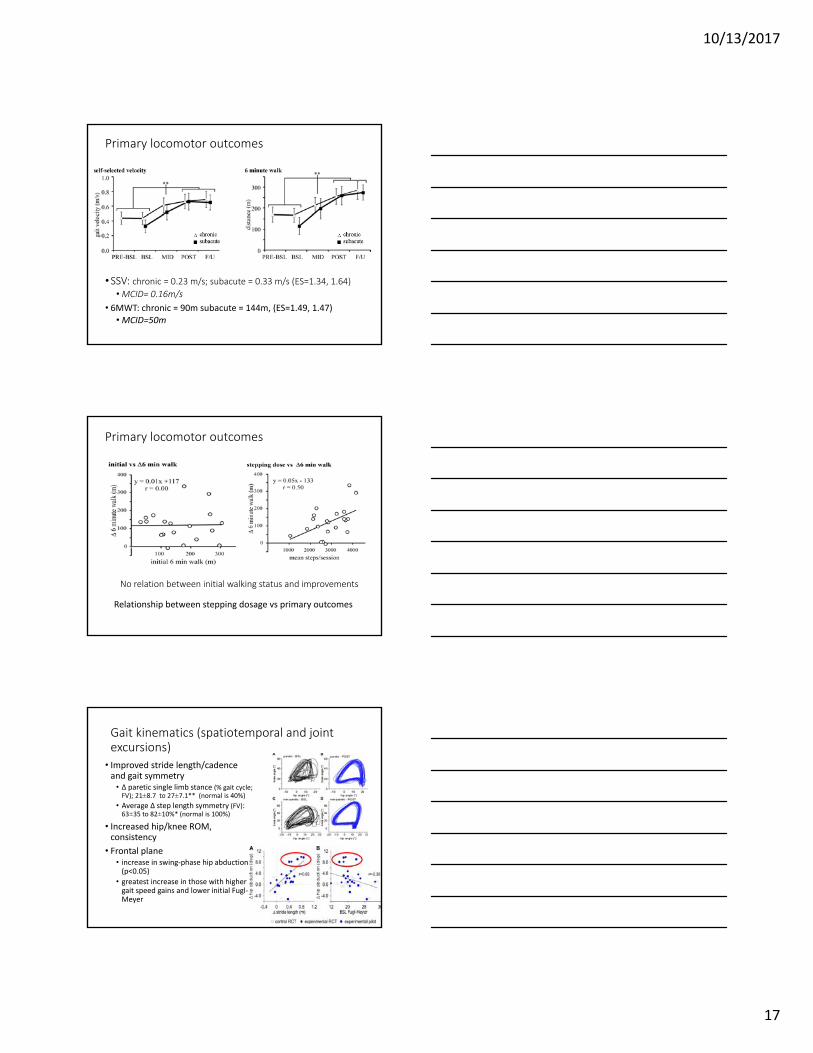
Non‐locomotor Improvements
• Berg Balance Scale Improvements
• Chronic: 6 pts (MDC=2.5)
• Subacute: 8 pts (MDC=6.0)
• Non‐ambulatory patients (n=3): 21 points
(Straube et al, PTJ 2014)
• Five Times Sit to Stand Improvements• 25% or 12.0 seconds chronic (MDC=3.6seconds)
• 40% or 5.9 seconds subacute (MDC=3.6seconds)
Outline
• Introduction – Theory and Rationale
• Development and Application• Developing the Training Program
• Preliminary study
• Randomized Clinical Trial – Very Intensive Early Walking post‐Stroke (VIEWS –submitted)
• Knowledge Translation
• Implementation
Randomized Controlled Trial:
• Subjects:• Subacute* • Age 18‐75• Single unilateral stroke• MMSE ≥ 23
• mod A or ambulate < 0.9 m/s (SSV)
• Stratification prior to randomization (walking speed)*
• N=32 required from effect sizes
• Intervention• ≤ 40 1hour sessions over 8‐10 weeks
• 1 week forward TM training*
• 7 weeks variable training
• Outcomes assessment• Primary: SSV & 6MWT
• Secondary: 5X sit‐to‐stand, Berg Balance Scale
(Hornby et al, submitted)

10/13/2017
19
VIEWS: Design
Experimental• Focused stepping training up to 40 1 hr sessions
• High aerobic intensity (70‐80%HRR)
• Skilled variable task practice on treadmill and overground
• No concurrent physical therapy
Control• Encouraged to continued physical therapy
• Supplemental sessions to achieve 40sessions
• Multiple activities, limited practice of any single task (Lang, 2009)
• Balance, Strength, PROM,Transfers
• Walking: 800‐1000 steps/session formula based on gait speed
• steps/session=200 +1500 steps (initial walking speeds) (Moore, 2010)
• 30‐40%HRR (Mackay‐Lyons 2003)
Baseline Experimental Control p‐value
Demographics N=15 N=17
Age 57±12 60±9.2 0.31
Days post-stroke 114±56 89±44 0.16
Impairments
LE Fugl-Meyer 20±5.8 21±6.2 0.63
PHQ-9 4.3±3.5 3.2±3.3 0.74
Training
sessions, n 34±8.9 33±8.9 0.31
steps/day 4046±2596 2572±1689 <0001
steps/session 2358±860 948±489 <0.001
average peak RPE 18±1.2 15±1.8 0.03
average peak HRR 74±8.7 40±5.4 <0.001
VIEWS: Group Comparisons
VIEWS: Group Comparisons
Self‐selected velocity (0.27±0.22 vs 0.09±0.09 m/s)
Fastest possible velocity (0.28±0.20 vs 0.11±0.15 m/s)
Significant difference in walking measures (p<0.01)
6 min walk test (114±111 vs 29±32 m)
Between group differences well above MCID for walking outcomes

10/13/2017
20
VIEWS: Results
Only control group practiced transfers and balance, but demonstrated no greater outcomes gains than experimental
group
No significant changes in non‐walking measures
(p=0.66) (p=0.95)
VIEWS: Results
Relationship between stepping dosage vs outcomes
Amount of practice related to improvements in walking
Gait kinematics (spatiotemporal and joint excursions)• Improved stride length/cadence and gait symmetry• Δ paretic single limb stance (% gait cycle; FV); 21±8.7 to 27±7.1** (normal is 40%)
• Average Δ step length symmetry (FV): 63±35 to 82±10%* (normal is 100%)
• Increased hip/knee ROM, consistency
• Frontal plane• increase in swing‐phase hip abduction (p<0.05)
• greatest increase in those with higher gait speed gains and lower initial Fugl‐Meyer

10/13/2017
21
Outline
• Introduction – Theory and Rationale
• Development and Application
• Knowledge Translation
• Implementation
Outline
• Introduction – Theory and Rationale
• Development and Application
• Knowledge Translation
• Implementation
The Challenge of Knowledge Translation (KT)
• > 17 years for evidence to be used clinical practice (Morris, 2011)
• KT is multi‐faceted (Strauss, 2009)• Patient
• Individual Clinician
• Organizational leaders/stakeholders
• Political
• Economic
63

10/13/2017
22
MonitorKnowledgeUse
SustainKnowledgeUse
EvaluateOutcomes
AdaptKnowledgeto Local Context
AssessBarriers to Knowledge Use
Select, Tailor,ImplementInterventions
Identify Problem
Identify, Review,Select Knowledge
Products/Tools
Synthesis
Knowledge Inquiry
KNOWLEDGE CREATION
Graham 2006Knowledge-to-Action Framework
Study Sample and Design
• Retrospective data analysis• Implementation of clinical initiative over 16 month period• No control group
• Inclusion• Initial diagnosis of stroke (<6 months)• 18-89 years of age
• Exclusion• Pregnant• HIV or AIDS• Incarceration• Lower extremity fracture or amputation
Implementation – Clinician Driven• Physical Therapy Staff• Prioritizing walking
• Perform outcome measurements
• Occupational Therapy• Continuing to address transfers
• Therapy Aides • Assist with increased stepping under PT guidance
• Nursing/PCT Staff • Consistently ready for therapy
• Carry over of transfers
• Administrative/Physician Support• Group scheduling
• Moral support
• Research Support • Assisted with initiation of program and performed data analysis

10/13/2017
23
Implementation ‐ Stepwatch• StepWatch3TM
• Worn 7:30 am to 5:00 pm• Paretic leg• Matched with medical records and de-
identified for research analysis
Results ‐ DemographicsDemographics Median (IQR; N)) or N (%)
age 64 (55-75; 201)
gender: male/female 114/87
lesion location: right 74 (39%)
left 88 (44%)
bilateral 32 (17%)
lesion distribution: cortical 98 (49%)
subcortical 32 (16%)
subtentorial 21 (15%)
multiple/unknown 40 (20%)
lesion type: ischemic 142 (71%)
hemorrhagic/unknown 59 (29%)
duration post-stroke 13 (8-25; 201)
Charlson Comorbidity Index 1 (0-3; 201)
Results ‐ Stepping Activity

10/13/2017
24
Results ‐ Stepping Activity
249 steps (Lang et al, 2009)
1516 steps
Results ‐ Correlations
Results ‐ Correlations

10/13/2017
25
Summary• Rationale and Development of Interventions based on well‐established principles of exercise physiology and motor control
• Proof‐of‐concept for smaller populations, ongoing studies in larger trials
• Implementation strategies – can we figure out how to get these and other effective strategies to therapists
• Thanks and questions . . .