Embed Size (px)
Citation preview
C
ITa
Y
a
b
c
A
1f
0h
omplementary Therapies in Medicine (2013) 21, 200—206
Available online at www.sciencedirect.com
j ourna l ho me pa g e: www.elsev ierhea l th .com/ journa ls /c t im
npatient treatment for severe atopic dermatitis in araditional Korean Medicine hospital: Introductionnd retrospective chart review
ounghee Yuna, Seungdeok Leeb, Sehyun Kimc, Inhwa Choia,∗
Department of Oriental Dermatology, College of Korean Medicine, Kyung Hee University, Seoul, Republic of KoreaDepartment of Acupuncture & Moxibustion, Dongguk University Hospital at Ilsan, Gyunggi-do, Republic of KoreaGraduate School of East-West Medical Science, Kyung Hee University, Yongin-Si, Republic of Koreavailable online 11 January 2013
KEYWORDSAtopic dermatitis;Hospitalisation;Traditional KoreanMedicine;Herbs;Acupuncture;SCORAD
SummaryObjectives: Patients with atopic dermatitis increasingly seek complementary and alternativemedical treatment. A number of studies have demonstrated the efficacy of herbs and acupunc-ture in the treatment of atopic dermatitis. Some patients with extensive disease, outpatienttreatment failure, acute deterioration or highly impaired everyday functioning require inpa-tient care. The aim of this study was to introduce and evaluate inpatient treatments for severeatopic dermatitis patients at a Traditional Korean Medicine hospital.Design and subjects: We performed a retrospective chart review of inpatients with severe atopicdermatitis between March 2008 and October 2011. Eligibility criteria for inclusion were: (1) adiagnosis of atopic dermatitis according to the criteria established by Hanifin and Rajka and(2) hospitalisation because of severe atopic dermatitis (objective scoring atopic dermatitis(SCORAD) score ≥ 40).Main outcome measurement: The SCORAD score was assessed by trained investigators at admis-sion and discharge.Results: Among 37 inpatients, there were 29 patients who met the criteria. Patients receivedtreatments including acupuncture, herbal medicine and herbal wet wrap dressings. The meantotal scoring SCORAD decreased from 60.63 to 37.37 during hospitalisation. Despite the rela-
tively small sample size, these findings were statistically significant.Conclusion: In atopic dermatitis, Traditional Korean Medicine effectively decreased clinicaldisease severity. This study’s weaknesses include the relatively small number of patients, someaspects of the study design, lack of follow-up assessment and lack of second measurement.hts re
© 2012 Elsevier Ltd. All rig∗ Corresponding author at: #149 Sangil-dong, Gangdong-gu, Seoul34-090, Republic of Korea. Tel.: +82 2 440 6235;ax: +82 2 440 7143; mobile: +82 18 344 1739.
E-mail address: [email protected] (I. Choi).
I
Wcoo
965-2299/$ — see front matter © 2012 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.ctim.2012.12.002
served.
ntroduction
hile most cases of atopic dermatitis (AD) are effectivelyontrolled with emollients and topical treatments in theutpatient setting, some patients with extensive disease,utpatient treatment failure, acute deterioration or highly

onal
AADswT1ld
HTrgtsbiatpTe
HPeoflt2bta(
CWmWottocstwt
S
DeI
Inpatient treatment for severe atopic dermatitis in a Traditi
impaired everyday functioning require inpatient care.1 Theaim of inpatient treatment for AD is not to provide com-plete clearance, but to improve the condition sufficiently toallow outpatient treatment. To date, there are few objec-tive data about the effectiveness of inpatient treatment ofAD in conventional medicine, but hospitalisation improvesclinical disease symptoms in patients with AD.1—3
Complementary and alternative medicine (CAM) isbecoming increasingly popular for the treatment of inflam-matory skin diseases, especially AD,4 since effective medicaltreatments for AD are limited.5,6 At Traditional KoreanMedicine (TKM) hospitals in Korea, patients receive acupunc-ture, herbal medicine and herbal wet wrap dressing dailyduring hospitalisation.
A number of randomised, controlled studies have demon-strated the efficacy of CAM in treating AD.4,7—9 However, nostudies have reported the outcomes of inpatient treatmentwith CAM or TKM medicine.
The aim of this study was to determine the effectsof TKM hospitalisation on AD. We conducted a retrospec-tive chart review of patients with severe AD treated at aTKM hospital. Objective and subjective scoring atopic der-matitis (SCORAD) scores were assessed at admission anddischarge.
Methods
Patients
We performed a retrospective chart review of inpatientswith severe AD treated in the Department of Oriental Derma-tology, Kyung Hee University Hospital at Gangdong, Collegeof Oriental Medicine, Kyung Hee University, Seoul, Republicof Korea between March 2008 and October 2011. The eli-gibility criteria for inclusion were: (1) diagnosis with ADaccording to the criteria established by Hanifin and Rajka10
and (2) hospitalisation for severe AD (objective SCORADscore ≥ 40).
This study was approved by the Institutional ReviewBoard, Kyung Hee University Hospital at Gangdong. Informedconsent was obtained from all patients, or from their parentsor guardians for patients under 18 years of age.
Outcome measurements
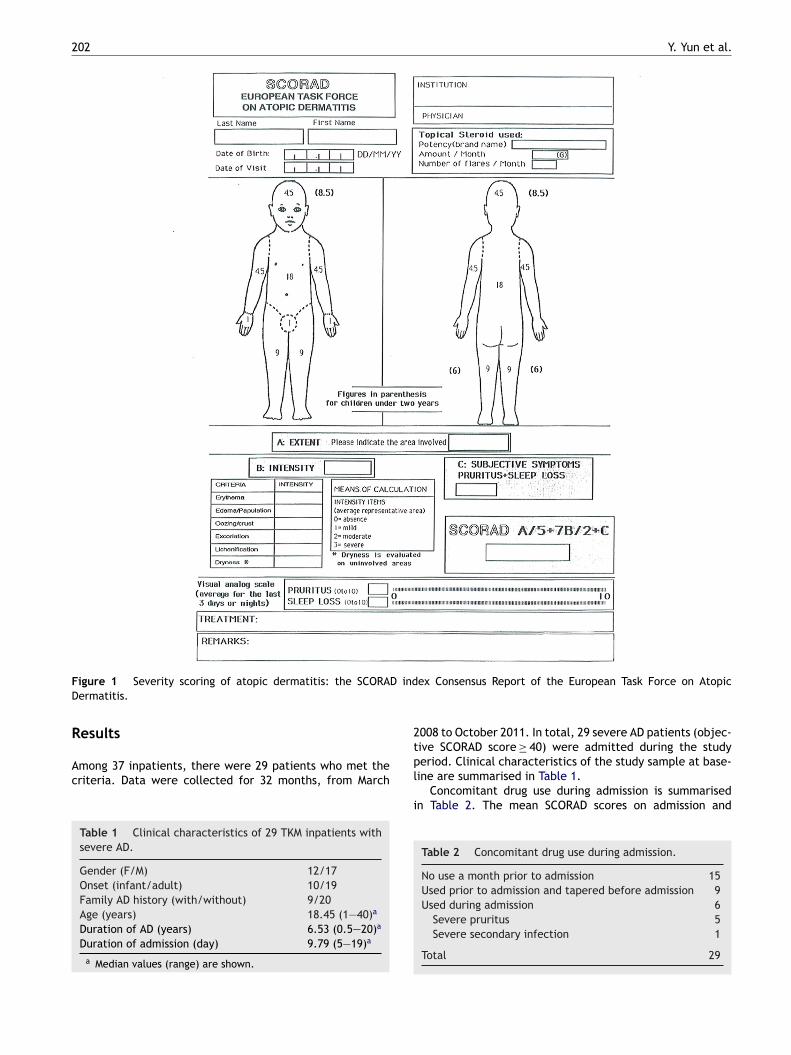
To assess the efficacy of treatments, the severity of ADwas evaluated using the SCORAD score11 (Fig. 1) on bothadmission and discharge day by a TKM doctor specialising indermatology.
Treatment
Patients received treatments including acupuncture, herbalmedicine and herbal wet wrap dressings. All treatments
were prepared and administered by a practitioner who hadcompleted a 6-year full-time didactic and practicum coursein CAM, with further clinical and research experience in thesame field for 20 years.mtsp
Korean Medicine hospital 201
cupuncturecupuncture needles (0.25 mm diameter and 40 mm length,ong Bang, Gyeonggi-do, Korea) were manually insertedubcutaneously or intramuscularly. Needle retention timeas 15 min. Acupuncture points included EX-HN3, LI4, LI11,E5, ST36, SP6 and LR3 on both sides of the body. About0 local points of acupuncture were also used on eczemaesions. Acupuncture treatment was provided twice per dayuring inpatient treatment.
erbal decoctionhe herbal medicine used was a decoction of plant mate-ial, including Rehmannia glutinosa, Talcum, Glycyrrhizalabra, Atractylodes chinensis, Plantago asiatica L., Gen-iana scabra Bunge, Akebia quinata Decaisne, Raphanusativus, Adenophora triphylla, Smilax china L., Scutellariaaicalensis Georgi and Angelica gigas. This herbal formulas known to be effective for reducing erythema, pruritusnd exudates in AD and has no known hepatic or renaloxicities.12 We decocted 0—20 g of each plant material withurified water as a daily dose according to patient progress.his medication was administered three times per day, afterach meal.
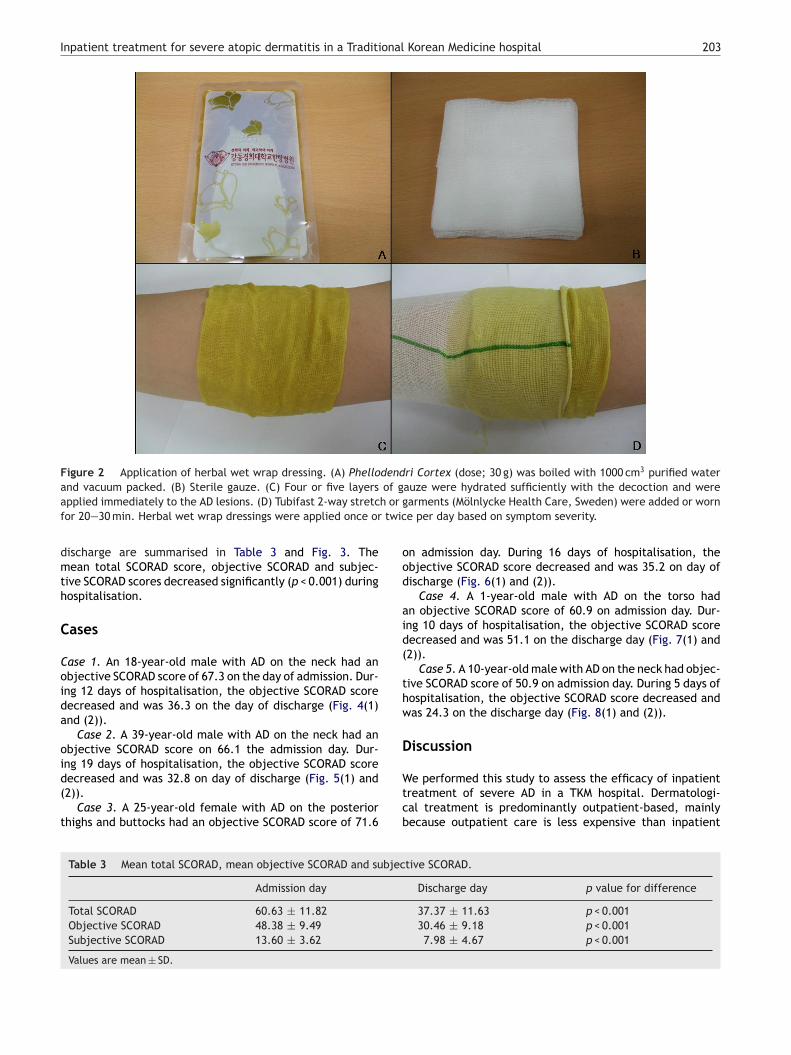
erbal wet wrap dressinghellodendri Cortex is known to have antibacterialffects.13 This herb (dose; 30 g) was boiled with 1000 cm3
f purified water in a large, open pot and vacuum packed toorm two packs of 120 cm3 for each treatment. Four or fiveayers of gauze were hydrated sufficiently with the decoc-ion and applied immediately to the AD lesions, and Tubifast-way stretch or garments (Mölnlycke Health Care, Göte-org, Sweden) were added and the dressings were worn byhe patients for 20—30 min. Herbal wet wrap dressings werepplied once or twice per day based on symptom severityFig. 2).
oncomitant medicationse allowed patients to use only emollients, lotions and oint-ents that do not contain steroids during hospitalisation.e requested patients not to use antihistamines, steroidsr immune-suppressant treatment during hospitalisation. Inhe cases of patients who were using these medications prioro treatment, the TKM doctors decided whether to taper offr continue using this medication according to the patient’sondition. In five cases with uncontrolled itching, we con-ulted with allopathic medical doctors for antihistaminereatment. In one case with severe secondary infection,e consulted with allopathic medical doctors for antibiotic
reatment.
tatistical analysis
ata were analysed using Statistical Package for Social Sci-nces (SPSS) version 13.0 for Windows (SPSS Inc., Chicago,L, USA). Continuous variables were characterised using
ean ± SD. A paired t-test test was used to determine ifhere was a statistically significant change in the SCORADcore. Results were considered statistically significant at
< 0.05.
202 Y. Yun et al.
F D indD
R
Ac
2
igure 1 Severity scoring of atopic dermatitis: the SCORAermatitis.
esults
mong 37 inpatients, there were 29 patients who met theriteria. Data were collected for 32 months, from March
Table 1 Clinical characteristics of 29 TKM inpatients withsevere AD.
Gender (F/M) 12/17Onset (infant/adult) 10/19Family AD history (with/without) 9/20Age (years) 18.45 (1—40)a
Duration of AD (years) 6.53 (0.5—20)a
Duration of admission (day) 9.79 (5—19)a
a Median values (range) are shown.
tpl
i
ex Consensus Report of the European Task Force on Atopic
008 to October 2011. In total, 29 severe AD patients (objec-ive SCORAD score ≥ 40) were admitted during the studyeriod. Clinical characteristics of the study sample at base-
ine are summarised in Table 1.Concomitant drug use during admission is summarisedn Table 2. The mean SCORAD scores on admission and
Table 2 Concomitant drug use during admission.
No use a month prior to admission 15Used prior to admission and tapered before admission 9Used during admission 6
Severe pruritus 5Severe secondary infection 1
Total 29
Inpatient treatment for severe atopic dermatitis in a Traditional Korean Medicine hospital 203
Figure 2 Application of herbal wet wrap dressing. (A) Phellodendri Cortex (dose; 30 g) was boiled with 1000 cm3 purified waterand vacuum packed. (B) Sterile gauze. (C) Four or five layers of gauze were hydrated sufficiently with the decoction and were
h or g twic
ood
aid(
thw
D
applied immediately to the AD lesions. (D) Tubifast 2-way stretcfor 20—30 min. Herbal wet wrap dressings were applied once or
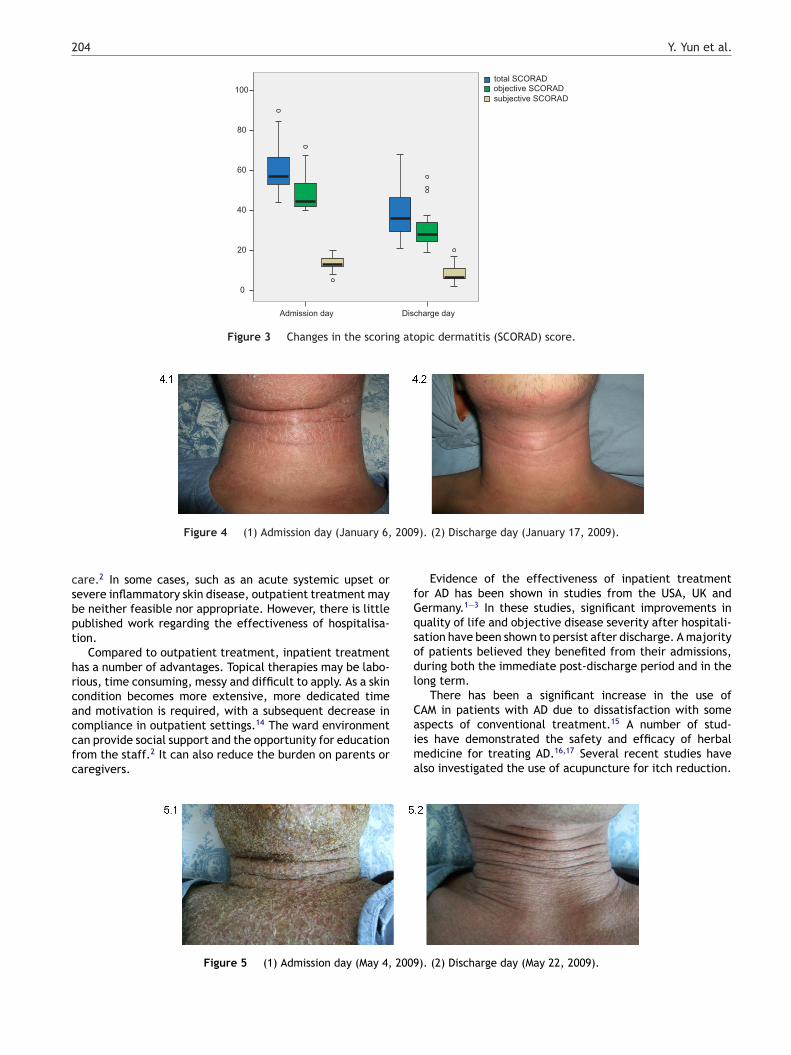
discharge are summarised in Table 3 and Fig. 3. Themean total SCORAD score, objective SCORAD and subjec-tive SCORAD scores decreased significantly (p < 0.001) duringhospitalisation.
Cases
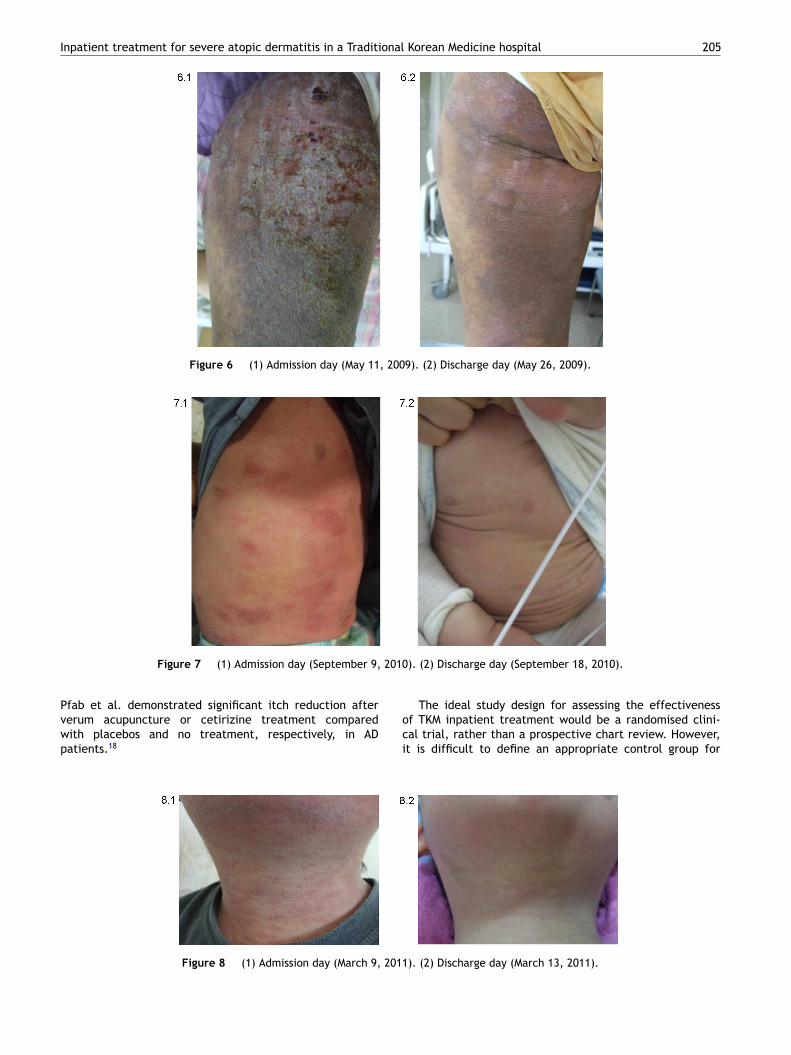
Case 1. An 18-year-old male with AD on the neck had anobjective SCORAD score of 67.3 on the day of admission. Dur-ing 12 days of hospitalisation, the objective SCORAD scoredecreased and was 36.3 on the day of discharge (Fig. 4(1)and (2)).
Case 2. A 39-year-old male with AD on the neck had anobjective SCORAD score on 66.1 the admission day. Dur-ing 19 days of hospitalisation, the objective SCORAD score
decreased and was 32.8 on day of discharge (Fig. 5(1) and(2)).Case 3. A 25-year-old female with AD on the posteriorthighs and buttocks had an objective SCORAD score of 71.6
Wtcb
Table 3 Mean total SCORAD, mean objective SCORAD and subjec
Admission day
Total SCORAD 60.63 ± 11.82
Objective SCORAD 48.38 ± 9.49
Subjective SCORAD 13.60 ± 3.62
Values are mean ± SD.
arments (Mölnlycke Health Care, Sweden) were added or worne per day based on symptom severity.
n admission day. During 16 days of hospitalisation, thebjective SCORAD score decreased and was 35.2 on day ofischarge (Fig. 6(1) and (2)).
Case 4. A 1-year-old male with AD on the torso hadn objective SCORAD score of 60.9 on admission day. Dur-ng 10 days of hospitalisation, the objective SCORAD scoreecreased and was 51.1 on the discharge day (Fig. 7(1) and2)).
Case 5. A 10-year-old male with AD on the neck had objec-ive SCORAD score of 50.9 on admission day. During 5 days ofospitalisation, the objective SCORAD score decreased andas 24.3 on the discharge day (Fig. 8(1) and (2)).
iscussion
e performed this study to assess the efficacy of inpatientreatment of severe AD in a TKM hospital. Dermatologi-al treatment is predominantly outpatient-based, mainlyecause outpatient care is less expensive than inpatient
tive SCORAD.
Discharge day p value for difference
37.37 ± 11.63 p < 0.00130.46 ± 9.18 p < 0.0017.98 ± 4.67 p < 0.001
204 Y. Yun et al.
100
80
60
40
20
0
Admission day Discharge day
total SCORADobjective SCORAD
subjective SCORAD
Figure 3 Changes in the scoring atopic dermatitis (SCORAD) score.
2009
csbpt
hrcaccfc
fGqsodl
C
Figure 4 (1) Admission day (January 6,
are.2 In some cases, such as an acute systemic upset orevere inflammatory skin disease, outpatient treatment maye neither feasible nor appropriate. However, there is littleublished work regarding the effectiveness of hospitalisa-ion.
Compared to outpatient treatment, inpatient treatmentas a number of advantages. Topical therapies may be labo-ious, time consuming, messy and difficult to apply. As a skinondition becomes more extensive, more dedicated timend motivation is required, with a subsequent decrease in
ompliance in outpatient settings.14 The ward environmentan provide social support and the opportunity for educationrom the staff.2 It can also reduce the burden on parents oraregivers.aima
Figure 5 (1) Admission day (May 4, 2009
). (2) Discharge day (January 17, 2009).
Evidence of the effectiveness of inpatient treatmentor AD has been shown in studies from the USA, UK andermany.1—3 In these studies, significant improvements inuality of life and objective disease severity after hospitali-ation have been shown to persist after discharge. A majorityf patients believed they benefited from their admissions,uring both the immediate post-discharge period and in theong term.
There has been a significant increase in the use ofAM in patients with AD due to dissatisfaction with some
spects of conventional treatment.15 A number of stud-es have demonstrated the safety and efficacy of herbaledicine for treating AD.16,17 Several recent studies havelso investigated the use of acupuncture for itch reduction.
). (2) Discharge day (May 22, 2009).
Inpatient treatment for severe atopic dermatitis in a Traditional Korean Medicine hospital 205
Figure 6 (1) Admission day (May 11, 2009). (2) Discharge day (May 26, 2009).
2010
Figure 7 (1) Admission day (September 9,Pfab et al. demonstrated significant itch reduction after
verum acupuncture or cetirizine treatment comparedwith placebos and no treatment, respectively, in ADpatients.18oci
Figure 8 (1) Admission day (March 9, 2011
). (2) Discharge day (September 18, 2010).
The ideal study design for assessing the effectiveness
f TKM inpatient treatment would be a randomised clini-al trial, rather than a prospective chart review. However,t is difficult to define an appropriate control group for). (2) Discharge day (March 13, 2011).

2
is
SmsaimAappsa6sc
slwctwistit
C
N
A
TKR
R
1
1
1
1
1
1
1
1
1
06
npatient treatment, and therefore we conducted a retro-pective chart review of inpatients.
This study included 29 patients with severe AD (objectiveCORAD score ≥ 40) who were hospitalised for approxi-ately 9.79 days (5—19 days) and assessed by SCORAD
cores on admission and discharge day. Inpatients receivedcupuncture, herbal medicine and herbal wet wrap dress-ng everyday during hospitalisation. Education about ADanagement was given to both patients and caregivers.mong the 29 patients, six patients used antihistamines orntibacterial agents during their admission. We allowed fiveatients to take antihistamines due to severe itching. Oneatient (case 2) received antibacterial therapy to treat sep-is. No steroidal agents were used by any patients duringdmission. The mean total SCORAD score decreased from0.63 to 37.37 during hospitalisation. Despite the relativelymall sample size, these findings were statistically signifi-ant.
This study has a number of limitations. Previoustudies1—3 assessed clinical disease severity using quality-of-ife scales such as Dermatology Life Quality Index. However,e did not assess any quality-of-life measures. We did notonduct any follow-up assessments. In addition, as men-ioned above, this was a retrospective chart review, andas essentially a pilot study that was completed in antic-
pation of a follow-up (prospective) study. However, thistudy expands upon previous research because it evaluateshe efficacy of hospitalisation in severe AD patients. Thiss the first report describing the effectiveness of inpatientreatment in a TKM hospital.
onflict of interest statement
o conflict of interest declared.
cknowledgement
his study was supported by a grant of the Traditionalorean medicine R&D Project, Ministry of Health & Welfare,epublic of Korea (B110017, B120014).
eferences
1. Schmitt J, Heese E, Wozel G, Meurer M. Effectiveness of inpa-tient treatment on quality of life and clinical disease severity inatopic dermatitis and psoriasis vulgaris — a prospective study.Dermatology 2007;214(1):68—76.
2. Ayyalaraju RS, Finlay AY, Dykes PJ, Trent JT, Kirsner RS, Kerdel
FA. Hospitalization for severe skin disease improves quality oflife in the United Kingdom and the United States: a compara-tive study. Journal of the American Academy of Dermatology2003;49(2):249—54.Y. Yun et al.
3. Kurwa HA, Finlay AY. Dermatology in-patient managementgreatly improves life quality. British Journal of Dermatology1995;133(4):575—8.
4. Boneberger S, Rupec RA, Ruzicka T. Complementary ther-apy for atopic dermatitis and other allergic skin diseases:facts and controversies. Clinics in Dermatology 2010;28(1):57—61.
5. Gardiner P, Kemper KJ. Herbs in pediatric and adolescentmedicine. Pediatrics in Review 2000;21(2):44—57.
6. Sidbury R, Hanifin JM. Old, new, and emerging thera-pies for atopic dermatitis. Dermatologic Clinics 2000;18(1):1—11.
7. Sheehan MP, Rustin MH, Atherton DJ, Buckley C, Harris DW,Brostoff J, et al. Efficacy of traditional Chinese herbal therapyin adult atopic dermatitis. Lancet 1992;340(8810):13—7.
8. Hon KL, Leung TF, Ng PC, Lam MCA, Kam WYC, WongKY, et al. Efficacy and tolerability of a Chinese herbalmedicine concoction for treatment of atopic dermati-tis: a randomized, double-blind, placebo-controlledstudy. British Journal of Dermatology 2007;157(2):357—63.
9. Salameh F, Perla D, Solomon M, Gamus D, Barzilai A, Green-berger S, et al. The effectiveness of combined Chinese herbalmedicine and acupuncture in the treatment of atopic der-matitis. Journal of Alternative and Complementary Medicine2008;14(8):1043—8.
0. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis.Acta Dermato-Venereologica (Stockholm) 1980;92:44—7.
1. Dermatitis ETFoA. Severity scoring of atopic dermatitis: theSCORAD index (Consensus report of the European task force onatopic dermatitis). Dermatology 1993;186(1):23—31.
2. Choi IH. Non-comparative study for the observation of clinicalefficacy and safety of CheungYeolYiSeup-tang and Hwangbaekexternal dressings on dampness-heat pattern atopic dermatitis.The Journal of Korean Oriental Medicine 2008;29:41—51.
3. Kim SI, Ahn YM, Ahn SY, Doo HK, Lee BC. The effects ofPhellodendri Cortex treatment on hematological and cyto-pathological alterations in non-bacterial prostatitis rat model.Journal of Korean Oriental Medical 2006;27(3):51—62.
4. Helbing I, Muston HL, Ferguson JE. Audit of admissions to der-matology beds in the northwest. British Journal of Dermatology2000;143:42.
5. Johnston GA, Bilbao RM, Graham-Brown RA. The use of com-plementary medicine in children with atopic dermatitis insecondary care in Leicester. British Journal of Dermatology2003;149(3):566—71.
6. Reuter J, Merfort I, Schempp CM. Botanicals in dermatology: anevidence-based review. American Journal of Clinical Dermatol-ogy 2010;11(4):247—67.
7. Zhang W, Leonard T, Bath-Hextall F, Chambers CA, Lee C,Humphreys R, et al. Chinese herbal medicine for atopic eczema.Cochrane Database of Systematic Reviews 2005;2:CD002291.
8. Pfab F, Kirchner MT, Huss-Marp J, Schuster T, Schalock PC,Fuqin J, et al. Acupuncture compared with oral antihis-
tamine for type I hypersensitivity itch and skin responsein adults with atopic dermatitis: a patient- and examiner-blinded, randomized, placebo-controlled, crossover trial.Allergy 2012;67(4):566—73.