Embed Size (px)
Citation preview

https://stolav.no/avdelinger/sentral-stab/fagavdelingen/hysnes-helsefort
Inpatient Multidiciplinary
Occupational Rehabilitation
(Slide design: Aasdahl)
Sigmund Gismervik MD, Ph.D. Candidate

DISCLOSURE: The presenter has not received and will not receive any commercial
support related to this presentation or the work presented in this presentation.
Background
Aims
Design
The rehabilitation model
Results
Concluding remarks

8 of 10 will experience back pain
1 of 3 report current pain lasting > 6 months.
1 of 2 will fulfil criteria for a mental disorder
1 of 5 will experience depression
1 of 2 will experience suicidal thoughts >14 days
1 of 4 will experience an alcohol or drug problem
(1 of 2 marriages will end with divorce)
> 60% of sick leave is caused by PAIN or CMD
(Norwegian HUNT studies, Harris 2010, Kessler-Berglund 2005, SSB)

Eliza Josolyne (Admitted Februar 1857)
Diagnosis: Insanity caused by overwork
http://www.dailymail.co.uk/home/you/article-2141741/Sent-asylum-The-Victorian-women-locked-suffering-stress-post-natal-depression-anxiety.html

http://tidsskriftet.no/2015/06/tidligere-i-tidsskriftet/lysslottet-i-luster

http://www.vest-telemark.no/OPPLEV/AiR-fyller-25-aar

3 ½ week
of
I-MORE
AIM
Outpatient
single-
component
program
vs.

Identified in the National SocialSecurity System Registry
Randomization 1
Invitation«short study»
Randomization 2
Short inpatientprogram
OutpatientACT
Invitation«long study»
Untouched controlgroup
Long inpatientprogram(I-MORE)
Screening
Randomization 2
Sicknessabsence
Screening

Identified in the National SocialSecurity System Registry
Randomization 1
Invitation«short study»
Randomization 2
Short inpatientprogram
OutpatientACT
Invitation«long study»
Untouched controlgroup
Long inpatientprogram (I-MORE)
Screening
Randomization 2
Sicknessabsence
Screening

Participants
Sick listed2-12 months
At least 50%
18-60 years oldMusculoskeletal
Psycological(Fatigue)
http://genius.com/http://www.fastcompany.com/ http://www.redbubble.com http://medicalnegligence.center
(Slide design: Aasdahl)

Diagnosis
57 %
43 %
43 %
Pain Mental disorders(including fatigue)


ACT1
CO-
ORDINATE
EXERCISE
REHABILITATION MODEL
1 A-Tjak et.al. 2015 Meta-Analysis of Efficacy of
Acceptance and Commitment Therapy (ACT)


RESULTS• N= 166• 79% Female• 40 % Higher education• 10% Had no employer• Median days on sick leave
> 200• Similar baseline
86 I-MORE (3 ½ weeks)80 O-ACT (6 weeks)

http://www.blog.friskbrisrc.com/sick-leave-benefits-norway/

Days on sick-leave(cumulativ median)
Inpatient rehabilitation 85 (IQR 33-149)*
Outpatient ACT 117 (IQR 59-189)
*(Mann-Whitney U test, p=0.034)

RETURN TO WORK
(4 weeks without receiving any benefits)
http://all-free-download.com/free-photos/stairs_silhouettes_human_214194.html
Hazard ratio 1.9 (95% CI 1.2-3.0, p=0.009)

http://www.thesil.ca/the-sad-state-of-mental-health
* Anxiety/Depression (HADS)
* Level of pain (BPI)
* Quality of life (15D)
* Subjective health (SHC)
SELF REPORTED OUTCOMES

Pain improved in outpatient ACT at 12 months follow up (-1 on 1-10 numeric rating scale)
No other statistical significant differences found
http://isha.sadhguru.org/blog/podcast/action-receptivity-right-balance/

Identified in the National SocialSecurity System Registry
Randomization 1
Invitation«short study»
Randomization 2
Short inpatient(4+4 days)
OutpatientACT
Invitation«long study»
Untouched controlgroup
Long inpatientprogram
Screening
Randomization 2
Sicknessabsence
Screening

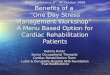
0.6
0.7
0.8
0.9
1.0
Hea
lth-r
ela
ted q
ualit
y o
f lif
e
start 3 months 6 months 12 months
Inpatient program
Outpatient program
Health-related quality of life 15D (0-1)
Aasdahl et al. Journal of Occupational Rehabilitation 2016

Summary (4+4 study)
No difference between a 4+4 days inpatient multimodal
occupational rehabilitation program and a 6 weeks of
outpatient ACT on sickness absence or health outcomes.
No evidence supporting implementation of the 4+4 days
inpatient program in ordinary practice.

Concluding remarks
3 ½ weeks of inpatient multimodal rehabilitation significantly
reduced sick-leave compared to 6 weeks of outpatient ACT.
Longer term health economic assessments are needed.
Integrating care for individuals with common mental and/or
pain disorders is a workable strategy within an ACT based
approach.

Thanks to all collaborators!

REFERENCES
• Fimland, M. S., et al. (2014). "Occupational rehabilitation programs for musculoskeletal pain and common mental health disorders: study protocol of a randomized controlled trial." BMC Public Health 14: 9.
• Aasdahl, L., et al. (2017). "Effect of Inpatient Multicomponent Occupational Rehabilitation Versus Less Comprehensive Outpatient Rehabilitation on Sickness Absence in Persons with Musculoskeletal- or Mental Health Disorders: A Randomized Clinical Trial." J Occup Rehabil.
• Aasdahl, L., et al. (2016). "Effects of Inpatient Multicomponent Occupational Rehabilitation versus Less Comprehensive Outpatient Rehabilitation on Somatic and Mental Health: Secondary Outcomes of a Randomized Clinical Trial." J Occup Rehabil.
• Hara, K. W., et al. (2017). "Transdiagnostic group-based occupational rehabilitation for participants withchronic pain, chronic fatigue and common mental disorders. A feasibility study." Disabil Rehabil: 1-11.
• Gismervik, S. O., et al. (2018). "The acceptance and commitment therapy model in occupational rehabilitationof musculoskeletal and common mental disorders: a qualitative focus group study." Disabil Rehabil: 1-11.

THERE IS A CRACK IN EVERYTHING
…that’s how the light gets in
(Leonard Cohen)