Embed Size (px)
Citation preview

Innovative Spine Technology to Differentiate and Grow Your Practice at Any Site of Service

Our Speakers for Today
Kevin N. Ammar, MDNeurosurgeonNeurological Institute of Savannah and Center for SpineSavannah, Georgia
Jeff HayesDirector of Field Training and Support Paradigm Spine, LLC
Sponsored By:
Saul EpsteinASC AdministrationParkCreekSurgery CenterDelray Beach Surgery Center
Moderator:Raymond Golish, MDOrthopedic Spine SurgeonJupiter, Florida

Overview • Introduction and Opportunity in Spine
• Stenosis Disease and Treatment Options
• Interlaminar Stabilization Overview
• Surgeon Clinical Experience
• Case Studies
• ASC Administration Experience
• Implementing New Technology in the ASC
• Differentiating Your Practice with InterlaminarStabilization
• Closing

Are you seeing them in your practice?
° National Profile Database (NPP) , IMS Health. 2015

Historically, Surgical Treatment was a Binary Choice
What if you could provide an additional treatment option to your stenosis patients that allows you to grow and differentiate your spine practice?

Grow and Differentiate Your Practice in Any Setting
Decompression with coflex® is a smart option between the two typical lumbar spinal stenosis surgical treatments

Coding Clarity for Interlaminar Stabilization

Lumbar Spinal Stenosis Disease and Treatment Overview
Jeff HayesDirector of Field Training and Support Paradigm Spine, LLC

Lumbar Spinal Stenosis Disease
• Lumbar spinal stenosis is the narrowing of spaces in the lower area of the spine that results in pressure on the spinal cord and/or nerve roots
• This narrowing can be the result of one or more several causes
• Lumbar spinal stenosis is a common cause of leg and back pain, and symptoms include pain and/or numbness, weakness, tingling in the legs brought on by walking and standing, and is relieved by sitting, leaning forward, or lying down

Symptoms of Lumbar Spinal Stenosis
• Pain and/or numbness in the legs brought on by walking and standing, and relieved by leaning forward, sitting or lying down
• The leg pain is frequently associated with lower back pain
• The cardinal symptom of lumbar stenosis is intermittent neurogenic claudication

Lumbar Spinal Stenosis is a Degenerative Process
• Lumbar spinal stenosis usually occurs over time as the spine gets more degenerated
• The more each spinal segment degenerates, the spine may become more unstable
• If the spinal segment is not aligned and “slips” forward, it is called a spondylolisthesis
• May not be treated with conservative care effectively – needs surgical intervention
Normal Alignment Spondylolisthesis
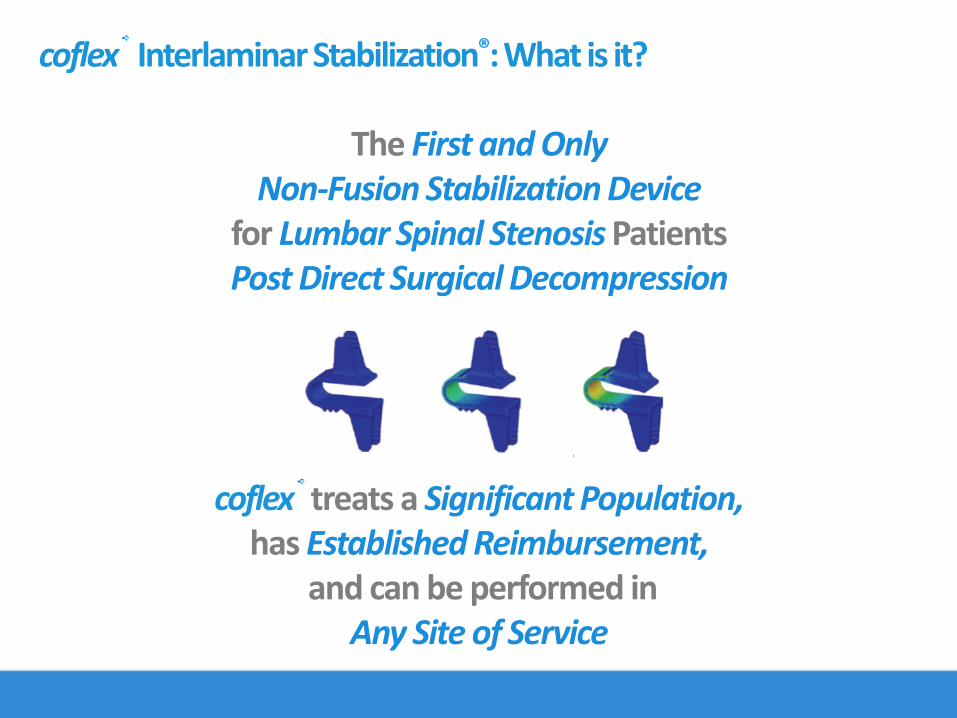
coflex® Interlaminar Stabilization®: What is it?
The First and OnlyNon-Fusion Stabilization Device
for Lumbar Spinal Stenosis Patients Post Direct Surgical Decompression
coflex® treats a Significant Population,has Established Reimbursement,
and can be performed in Any Site of Service

• The coflex® device offers a new option for treating lumbar spinal stenosis patients who may need more than a decompression alone, but not require the extensiveness of a fusion, and is available in any setting of care
Disease Severity Continuum
Surgical Treatment Options: Where Does coflex® Fit?

• Supports decompression• Preserves motion• Addresses leg and back pain• Maintains foraminalheight• Preserves normal motion
at operative and adjacent levels
coflex® Interlaminar Stabilization®: How it Works
coflex® loads on laminar bone NOT the spinousprocess
Allows for flexion Allows for extension through device compression
*Claims based on US FDA PMA P110008. October 2012.http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm327502.htm

Surgical Procedure for Decompression with coflex®

Address Leg Pain with Necessary Decompression
Decompression with up to 50% bilateral partial medial facetectomies can be performed before insertion of coflex®
coflex®provides similar decompression value compared to fusion through five years
*Claims based on US FDA PMA P110008. October 2012.http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm327502.htm
coflex® Immediately Decreases Leg Pain Through 5 Years

coflex® Bears Load on InterlaminarRidge
Provide Non-Fusion Stabilization After Decompression
Preoperative stenoticspine Postoperative spine with coflex®

Address Back Pain with Motion Preservation
Deep interlaminarpositioning allows for facet offloading
coflex® Immediately Decreases Back Pain Through 5 Years
*Claims based on US FDA PMA P110008. October 2012.http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm327502.htm

For Patients with Lumbar Spinal Stenosis
coflex® Provides Durable and Sustainable Treatment
*Claims based on US FDA PMA P110008. October 2012.http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm327502.htm

Clinical Experience & Case Studies
Kevin N. Ammar, MDNeurosurgeonNeurological and Spine InstituteSavannah, Georgia

Clinical Experience
Education• University of Virginia, BA 1995• University of Florida, MD 2000• University of Alabama-Birmingham, Neurosurgical Internship and Residency 2000-2006• Cedars-Sinai Medical Center, Los Angeles, Spine Fellowship 2006-2007
Practice• Memorial University Medical Center, Savannah, GA• St. Joseph’s / Candler Hospitals, Savannah, GA• East Georgia Regional Medical Center, Statesboro, GA• Wayne Memorial Hospital, Jesup, GA• Neurological and Spine Institute ASC, Savannah, GA

How I first found out about coflex®
• Attending a local seminar / course introducing coflex®
How I used to think about coflex®
• A modest technical extrapolation from Medtronic’s X-Stop with likely similar deficiencies of durable results, and limited insurance acceptance
How I now think about coflex®
• A durable solution for one or two level lumbar stenosis• A simple, but efficacious option that warrants consideration for certain cases of, Grade 1
spondylolisthesis, radiculopathy.
What I know now that I didn’t know back then about coflex®
• It is very easy to use –modest technical nuances• Excellent results so far• Patients are happy!
Adopting coflex® into My Practice

Selecting coflex® patients for Inpatient (hospital)• Medical comorbidities that may necessitate overnight observation• Poor support at home• 2 level cases with anticipated need for overnight drain
Selecting coflex® patients for Outpatient (hospital)• Those with hospital preference
Selecting coflex® patients for the ASC• Everyone else
Essentially the same considerations as for laminectomy alone
Determining Patients for coflex® in All Settings of Care

Started simple• Single-level case
How coflex® helps differentiate and grow my ASC• An entire new population of patients can now become potentially outpatient• Offers a non-fusion alternative
For those considering bringing coflex® to their ASC setting• Start simple• Build appropriate expectations pre-operatively• Consider paraspinal musculature local anesthetic or “cocktail”
• i.e. Toradol, Depo-Medrol, Marcaine• Consider polymerized gelfoam, temporary drain
Integrating coflex® into My ASC

coflex®Patient Cases
27 patients treated with coflex® InterlaminarStabilization®
• One removed due to recurrent radicular symptoms after initial period of improvement

coflex®Case Examples
Exam
Normal
Preop
• 69 year old male
• Moderately obese (BMI<40)
• No prior surgery
• > 1yr progressive BLE pain increased with standing/walking, improvedwith sitting
• Transient benefit from LESI

coflex®Case Examples
Exam
Normal
Postop
• Surgery 3/17
• Follow-up 8/17
• Resolved lower extremity pain, modest lower back pain
• Referred to PT

coflex®Case Examples
Exam
Normal
Preop
• 70 year old female
• > 1yr progressive back and BLE symptoms
• L5 distribution
• Improved with sitting
• +PT/LESI’s/RFA
• Grade 1 degenerative spondy– non-mobile
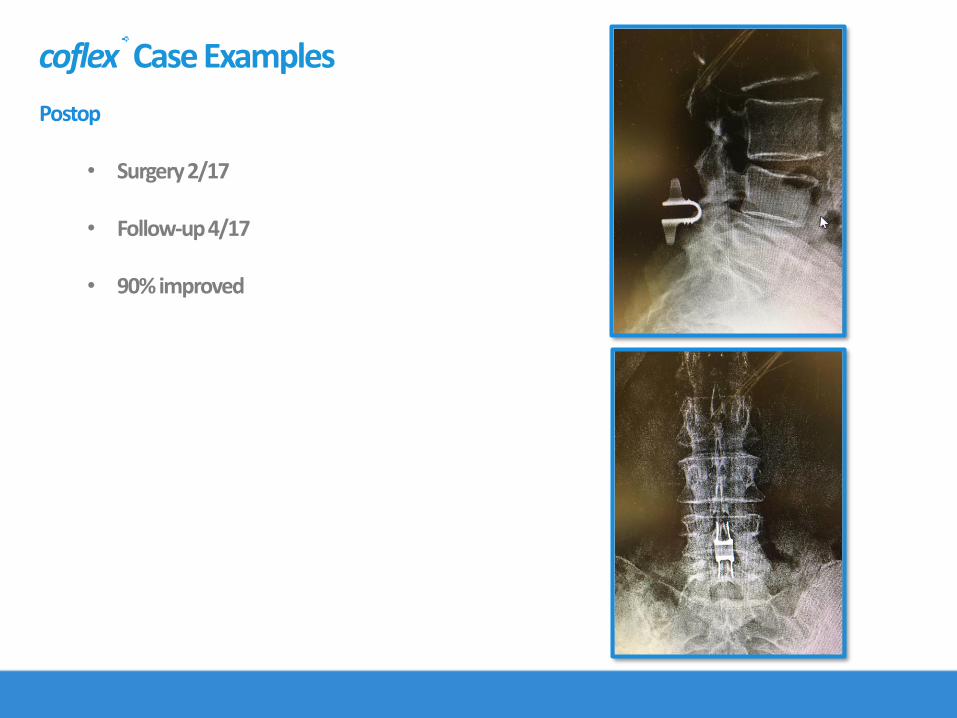
coflex®Case Examples
Exam
Normal
Postop
• Surgery 2/17
• Follow-up 4/17
• 90% improved

coflex®Case Examples
Exam
Normal
Preop
• 44 year old male
• Runner, bilateral UE amputations
• No prior back surgery
• Severe BLE, worse with standing
• Failed PT/LESI’s

coflex®Case Examples
Exam
Normal
The anatomy dictates the best orientation of the coflex® device
Make sure to not block out the coflex®
device in a 2-level case
Postop
• 2 months follow-up
• No leg or back pain

coflex®Case Examples
Exam
Normal
Preop
• 52 year old female
• Bilateral L4 distribution pain
• Worse pain when standing/walking
• No prior back surgery
• Failed PT/LESI’s
• Non-mobile degenerative spondyL4-5

coflex®Case Examples
Exam
Normal
Postop
• Resolved lower extremity symptoms
• Follow-up at 5 months
Experience from ASC Administration
Saul EpsteinASC Administration
Park Creek Surgery CenterCoconut Creek, Florida
Delray Beach Surgery CenterDelray Beach, Florida

Experience as ASC Administration
Saul Epstein, 20 years experience as ASC Administration • ParkCreekSurgery Center• Delray Beach Surgery Center• President of Florida Society of Ambulatory Surgery Centers (FSASC)
• Introduced to coflex® in 2015 • The device was requested by a surgeon
• Expanded utilization and surgeon user base in 2017

2015• Spine surgeon requested coflex® procedure to be done in the ASC• ASC administration confirmed economic sensibility• ASC administration confirmed clinical ease of use
• A “simple add-on” to a basic decompression• Does not require additional post-op services• Minimally invasive, alternative to fusion• Not a complex surgery overall• Small instrument set
2017• CPT coding changes allowed procedure at ASC site of service• Due to these changes, case volume has increased• Provides opportunity for recruiting additional coflex®cases and surgeons to practice in the ASC
setting • Existing medical staff member doing coflex®Medicare cases at hospital, not knowing it could
be done at ASC as of 1/1/17
History of coflex® with ASC

Implementing coflex® into Spine Service at Surgery Center
After surgeon shows interest in procedure, the following steps occur:• coflex®case is identified • Economic analysis performed
• New 2017 CPT Code reimbursable by Medicare in ASC setting (bundled rate includes surgical procedure and implantable)
• Possibly reimbursable by private carriers• Surgical Code (22867) and implant cost• ASC contracts proactively verified prior to case
• Clinical evaluation of patient, confirming appropriate for the ASC• Coordination with Paradigm representative for instrumentation & coverage
on procedure day• Post case economic evaluation of case performed

Expansion of Services in the ASC with coflex®
Offering coflex ® at the ASC allows opportunity for• New type of spine procedure• Minimally invasive procedure • Offers an alternative to fusion• Serves new stenosis patient population• Potential new insurance base that wasn’t previously available prior to 2017
Clinical ease of use • OR time – similar to standard decompression• Instrumentation – small tray, no additional instrumentation required
Economically profitable
Recruitment opportunity for ASC• New spine surgeons • New cases & more volume of cases at the ASC

Interlaminar Stabilization Opportunity for the ASC
coflex® InterlaminarStabilization® is a smart fit for the ASC because:• Less invasive spine procedure• Recruitment tool• Economics
Patient out-of-pocket expenses are less than going to a hospital setting • Co-insurance percentage applied towards a lower reimbursement amount
Easy procedure to adopt when trying to grow spine in your ASC • Simple, minimally invasive, lumbar spine procedure • Less instrumentation, OR time, costs compared to a posterior lumbar fusion procedure• Reimbursement/coding clarity – 2017 Reimbursement pathway for ASC Setting
coflex® is a great way to get started with differentiating and growing your spine ASC from basic discectomy and laminectomy cases to implant cases

In Summary…• Offer a disease-state solution at any site of service
• There’s an opportunity in spine that can help differentiate your practice
• Patients with coflex® InterlaminarStabilization®FEEL BETTER with relief that LASTS

Appendix

Coding Clarity for Interlaminar Stabilization