Embed Size (px)
Citation preview
GA
TA
GC
GA
CG
AT
C-
GA
AA
GA
AG
TT
A
++
++
+
+
++
+PGR
GA
TA
GC
GA
CG
AT
C-
GA
AA
GA
AG
TT
A+
+
+
+ERBB2
GA
TA
GC
GA
C
GA
TA
GC
GA
CG
AT
C-
GA
AA
GA
AG
TT
A
+++
+ESR1
++
++
MKI67
molecular diagnostic test for quantitative determination of breast cancer biomarkers ER, PR, HER2, Ki-67 mRNA expression for any laboratory.
Innovation for your breast cancer diagnostics
High-performance
2 3
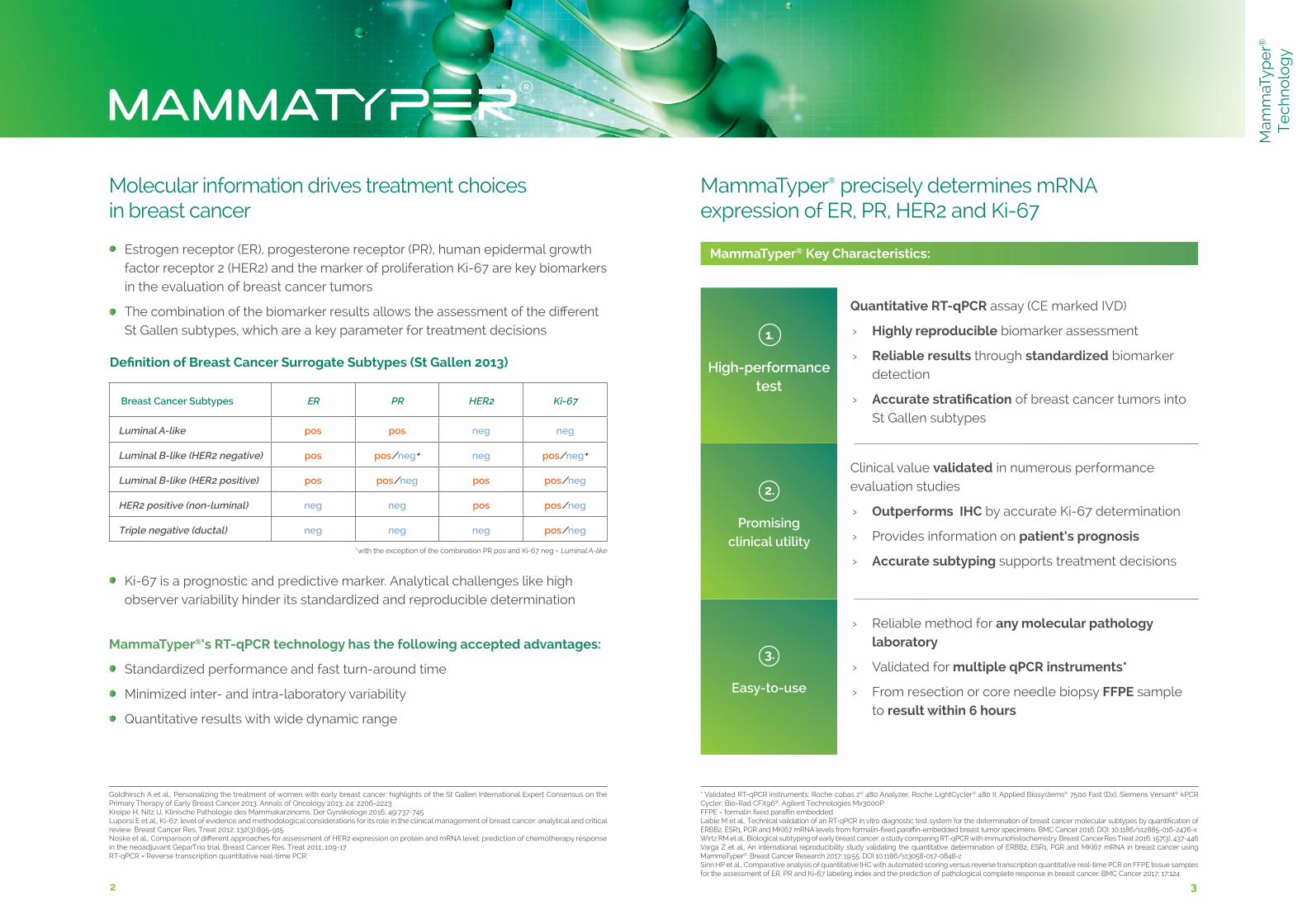
Breast Cancer Subtypes ER PR HER2 Ki-67
Luminal A-like pos pos neg neg
Luminal B-like (HER2 negative) pos pos/neg+ neg pos/neg+
Luminal B-like (HER2 positive) pos pos/neg pos pos/neg
HER2 positive (non-luminal) neg neg pos pos/neg
Triple negative (ductal) neg neg neg pos/neg
3
Molecular information drives treatment choices in breast cancer
Goldhirsch A et al., Personalizing the treatment of women with early breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Annals of Oncology 2013; 24: 2206-2223Kreipe H, Nitz U, Klinische Pathologie des Mammakarzinoms. Der Gynäkologe 2016; 49:737-745 Luporsi E et al., Ki-67: level of evidence and methodological considerations for its role in the clinical management of breast cancer: analytical and critical review. Breast Cancer Res. Treat 2012; 132(3):895-915 Noske et al., Comparison of different approaches for assessment of HER2 expression on protein and mRNA level: prediction of chemotherapy response in the neoadjuvant GeparTrio trial. Breast Cancer Res. Treat 2011; 109-17 RT-qPCR = Reverse transcription quantitative real-time PCR
Definition of Breast Cancer Surrogate Subtypes (St Gallen 2013)
*with the exception of the combination PR pos and Ki-67 neg = Luminal A-like
MammaTyper® precisely determines mRNAexpression of ER, PR, HER2 and Ki-67
Estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2) and the marker of proliferation Ki-67 are key biomarkers in the evaluation of breast cancer tumors
The combination of the biomarker results allows the assessment of the different St Gallen subtypes, which are a key parameter for treatment decisions
Ki-67 is a prognostic and predictive marker. Analytical challenges like high observer variability hinder its standardized and reproducible determination
Quantitative RT-qPCR assay (CE marked IVD)
› Highly reproducible biomarker assessment
› Reliable results through standardized biomarker detection
› Accurate stratification of breast cancer tumors into St Gallen subtypes
Clinical value validated in numerous performance evaluation studies
› Outperforms IHC by accurate Ki-67 determination
› Provides information on patient‘s prognosis
› Accurate subtyping supports treatment decisions
› Reliable method for any molecular pathology laboratory
› Validated for multiple qPCR instruments*
› From resection or core needle biopsy FFPE sample to result within 6 hours
High-performance test
Promising clinical utility
Easy-to-use
1.
2.
3.
MammaTyper® Key Characteristics:
MammaTyper®‘s RT-qPCR technology has the following accepted advantages:
Standardized performance and fast turn-around time
Minimized inter- and intra-laboratory variability
Quantitative results with wide dynamic range
* Validated RT-qPCR instruments: Roche cobas z® 480 Analyzer, Roche LightCycler® 480 II, Applied Biosystems® 7500 Fast (Dx), Siemens Versant® kPCR Cycler, Bio-Rad CFX96®, Agilent Technologies Mx3000PFFPE = formalin fixed paraffin embeddedLaible M et al., Technical validation of an RT-qPCR in vitro diagnostic test system for the determination of breast cancer molecular subtypes by quantification of ERBB2, ESR1, PGR and MKI67 mRNA levels from formalin-fixed paraffin-embedded breast tumor specimens. BMC Cancer 2016; DOI: 10.1186/s12885-016-2476-xWirtz RM et al., Biological subtyping of early breast cancer: a study comparing RT-qPCR with immunohistochemistry. Breast Cancer Res Treat 2016; 157(3), 437-446Varga Z et al., An international reproducibility study validating the quantitative determination of ERBB2, ESR1, PGR and MKI67 mRNA in breast cancer using MammaTyper®. Breast Cancer Research 2017; 19:55: DOI 10.1186/s13058-017-0848-zSinn HP et al., Comparative analysis of quantitative IHC with automated scoring versus reverse transcription quantitative real-time PCR on FFPE tissue samples for the assessment of ER, PR and Ki-67 labeling index and the prediction of pathological complete response in breast cancer. BMC Cancer 2017; 17:124
Mam
maT
ype
r®
Te
chn
olo
gy
4 5
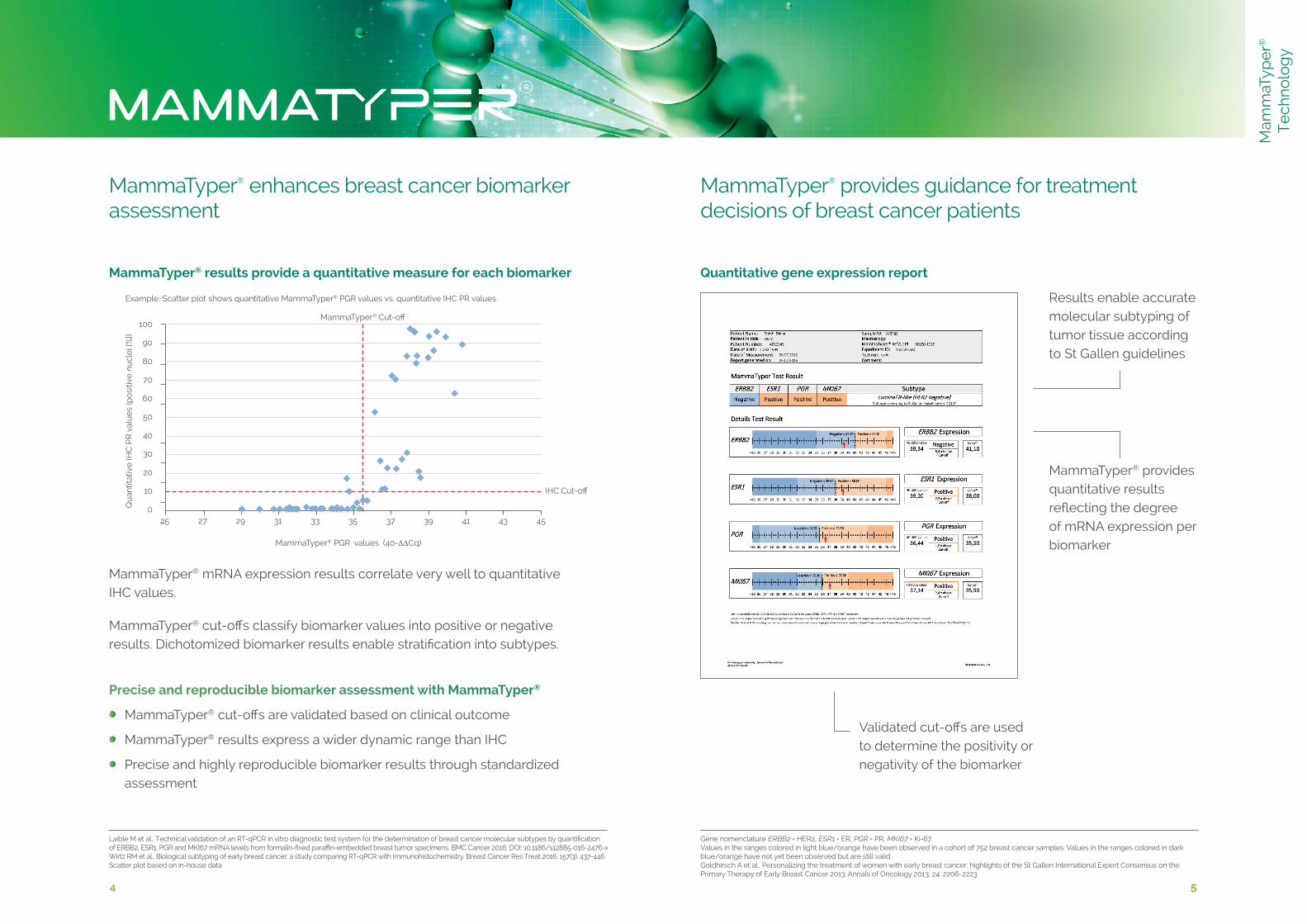
MammaTyper® cut-offs classify biomarker values into positive or negative results. Dichotomized biomarker results enable stratification into subtypes.
MammaTyper® mRNA expression results correlate very well to quantitative IHC values.
Precise and reproducible biomarker assessment with MammaTyper®
MammaTyper® cut-offs are validated based on clinical outcome
MammaTyper® results express a wider dynamic range than IHC
Precise and highly reproducible biomarker results through standardized assessment
MammaTyper® enhances breast cancer biomarker
assessment
Laible M et al., Technical validation of an RT-qPCR in vitro diagnostic test system for the determination of breast cancer molecular subtypes by quantificationof ERBB2, ESR1, PGR and MKI67 mRNA levels from formalin-fixed paraffin-embedded breast tumor specimens. BMC Cancer 2016; DOI: 10.1186/s12885-016-2476-xWirtz RM et al., Biological subtyping of early breast cancer: a study comparing RT-qPCR with immunohistochemistry. Breast Cancer Res Treat 2016; 157(3), 437-446Scatter plot based on in-house data
Gene nomenclature ERBB2 = HER2, ESR1 = ER, PGR = PR, MKI67 = Ki-67Values in the ranges colored in light blue/orange have been observed in a cohort of 752 breast cancer samples. Values in the ranges colored in dark blue/orange have not yet been observed but are still validGoldhirsch A et al., Personalizing the treatment of women with early breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Annals of Oncology 2013; 24: 2206-2223
MammaTyper® provides guidance for treatment decisions of breast cancer patients
5
Mam
maT
ype
r®
Te
chn
olo
gy
Results enable accurate molecular subtyping of tumor tissue according to St Gallen guidelines
MammaTyper® provides quantitative results reflecting the degree of mRNA expression per biomarker
Validated cut-offs are used to determine the positivity or negativity of the biomarker
Quantitative gene expression reportMammaTyper® results provide a quantitative measure for each biomarker
Example: Scatter plot shows quantitative MammaTyper® PGR values vs. quantitative IHC PR values
Qu
antit
ativ
e IH
C P
R v
alu
es
(po
sitiv
e n
ucl
ei [
%])
100
90
80
70
60
50
40
30
20
10
0
MammaTyper® Cut-off
IHC Cut-off
MammaTyper® PGR values (40-∆∆Cq)
27 29 31 33 35 37 39 41 43 4525
6 76 7
Varying tumor cell content has minimal influence on MammaTyper® performance*
Fluctuating tumor cell content (TCC) could possibly affect the validity of quantitative assessment of ER, PR, HER2 and Ki-67. Therefore, the performance of MammaTyper® was investigated under different scenarios of TCC.
Wirtz RM et al., Low influence of tumor cell content on mRNA expression levels of ERBB2, ESR1, PGR and MKI67 when performing the MammaTyper® RT-qPCR kit. Poster SABC 2014 Laible M et al., Technical validation of an RT-qPCR in vitro diagnostic test system for the determination of breast cancer molecular subtypes by quantification of ERBB2, ESR1, PGR and MKI67 mRNA levels from formalin-fixed paraffin-embedded breast tumor specimens. BMC Cancer 2016; DOI: 10.1186/s12885-016-2476-x* shown for HER2 negative tissue samples with TCC > 20 %; DCIS = ductal carcinoma in situ
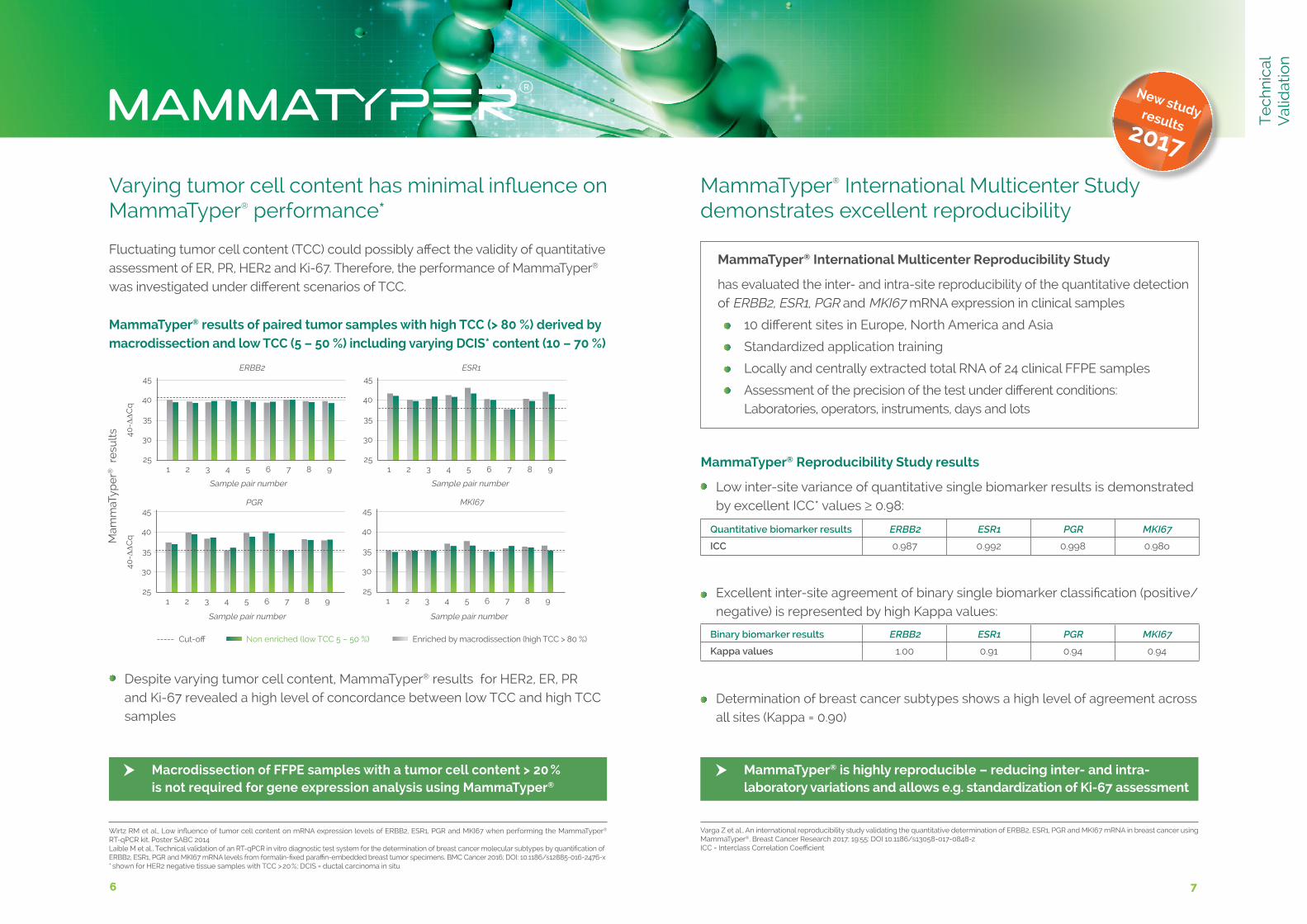
----- Cut-off Non enriched (low TCC 5 – 50 %) Enriched by macrodissection (high TCC > 80 %)
40-∆∆C
q
ERBB2
1 2 3 4 5 6 7 8 9
40-∆∆C
q
PGR45
40
35
30
25
1 2 3 4 5 6 7 8 91 2 3 4 5 6 7 8 9
ESR145
40
35
30
25
45
40
35
30
25
1 2 3 4 5 6 7 8 9
MKI6745
40
35
30
25
Sample pair number
Sample pair number
Sample pair number
Sample pair number
Mam
maT
ype
r® r
esu
lts
MammaTyper® results of paired tumor samples with high TCC (> 80 %) derived by macrodissection and low TCC (5 – 50 %) including varying DCIS* content (10 – 70 %)
Binary biomarker results ERBB2 ESR1 PGR MKI67
Kappa values 1.00 0.91 0.94 0.94
Quantitative biomarker results ERBB2 ESR1 PGR MKI67
ICC 0.987 0.992 0.998 0.98o
Varga Z et al., An international reproducibility study validating the quantitative determination of ERBB2, ESR1, PGR and MKI67 mRNA in breast cancer using MammaTyper®. Breast Cancer Research 2017; 19:55: DOI 10.1186/s13058-017-0848-z ICC = Interclass Correlation Coefficient
Low inter-site variance of quantitative single biomarker results is demonstrated by excellent ICC* values ≥ 0.98:
Excellent inter-site agreement of binary single biomarker classification (positive/negative) is represented by high Kappa values:
Determination of breast cancer subtypes shows a high level of agreement across all sites (Kappa = 0.90)
MammaTyper® Reproducibility Study results
MammaTyper® International Multicenter Reproducibility Study
has evaluated the inter- and intra-site reproducibility of the quantitative detection of ERBB2, ESR1, PGR and MKI67 mRNA expression in clinical samples
10 different sites in Europe, North America and Asia
Standardized application training
Locally and centrally extracted total RNA of 24 clinical FFPE samples
Assessment of the precision of the test under different conditions: Laboratories, operators, instruments, days and lots
Despite varying tumor cell content, MammaTyper® results for HER2, ER, PR and Ki-67 revealed a high level of concordance between low TCC and high TCC samples
Macrodissection of FFPE samples with a tumor cell content > 20 % is not required for gene expression analysis using MammaTyper®
MammaTyper® is highly reproducible – reducing inter- and intra- laboratory variations and allows e.g. standardization of Ki-67 assessment
New study results 2017
MammaTyper® International Multicenter Study demonstrates excellent reproducibility
Te
chn
ical
V
alid
atio
n
8 98 9
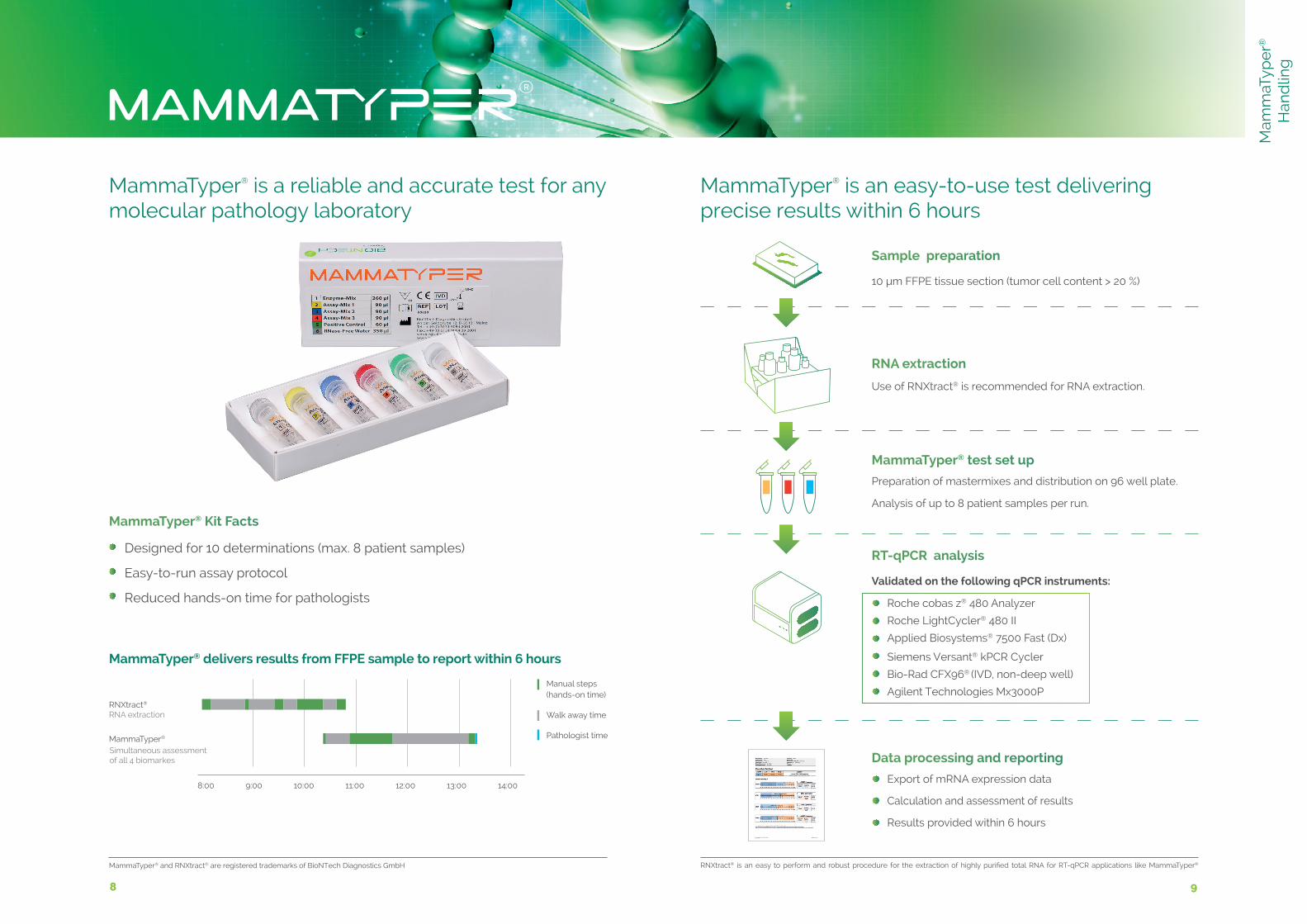
MammaTyper® is a reliable and accurate test for any molecular pathology laboratory
MammaTyper® is an easy-to-use test delivering precise results within 6 hours
Sample preparation
10 µm FFPE tissue section (tumor cell content > 20 %)
RNA extraction
Use of RNXtract® is recommended for RNA extraction.
MammaTyper® test set up
Preparation of mastermixes and distribution on 96 well plate.
Analysis of up to 8 patient samples per run.
Data processing and reporting
Export of mRNA expression data
Calculation and assessment of results
Results provided within 6 hours
RT-qPCR analysis
Validated on the following qPCR instruments:
Roche cobas z® 480 Analyzer
Roche LightCycler® 480 II
Applied Biosystems® 7500 Fast (Dx)
Siemens Versant® kPCR Cycler
Bio-Rad CFX96® (IVD, non-deep well)
Agilent Technologies Mx3000P
MammaTyper® Kit Facts
Designed for 10 determinations (max. 8 patient samples)
Easy-to-run assay protocol
Reduced hands-on time for pathologists
MammaTyper® delivers results from FFPE sample to report within 6 hours
RNXtract®
RNA extraction
MammaTyper®
Simultaneous assessment of all 4 biomarkes
Manual steps (hands-on time)
Walk away time
Pathologist time
8:00 9:00 10:00 11:00 12:00 13:00 14:00
RNXtract® is an easy to perform and robust procedure for the extraction of highly purified total RNA for RT-qPCR applications like MammaTyper®MammaTyper® and RNXtract® are registered trademarks of BioNTech Diagnostics GmbH
Mam
maT
ype
r®
Han
dlin
g
10 1110 11
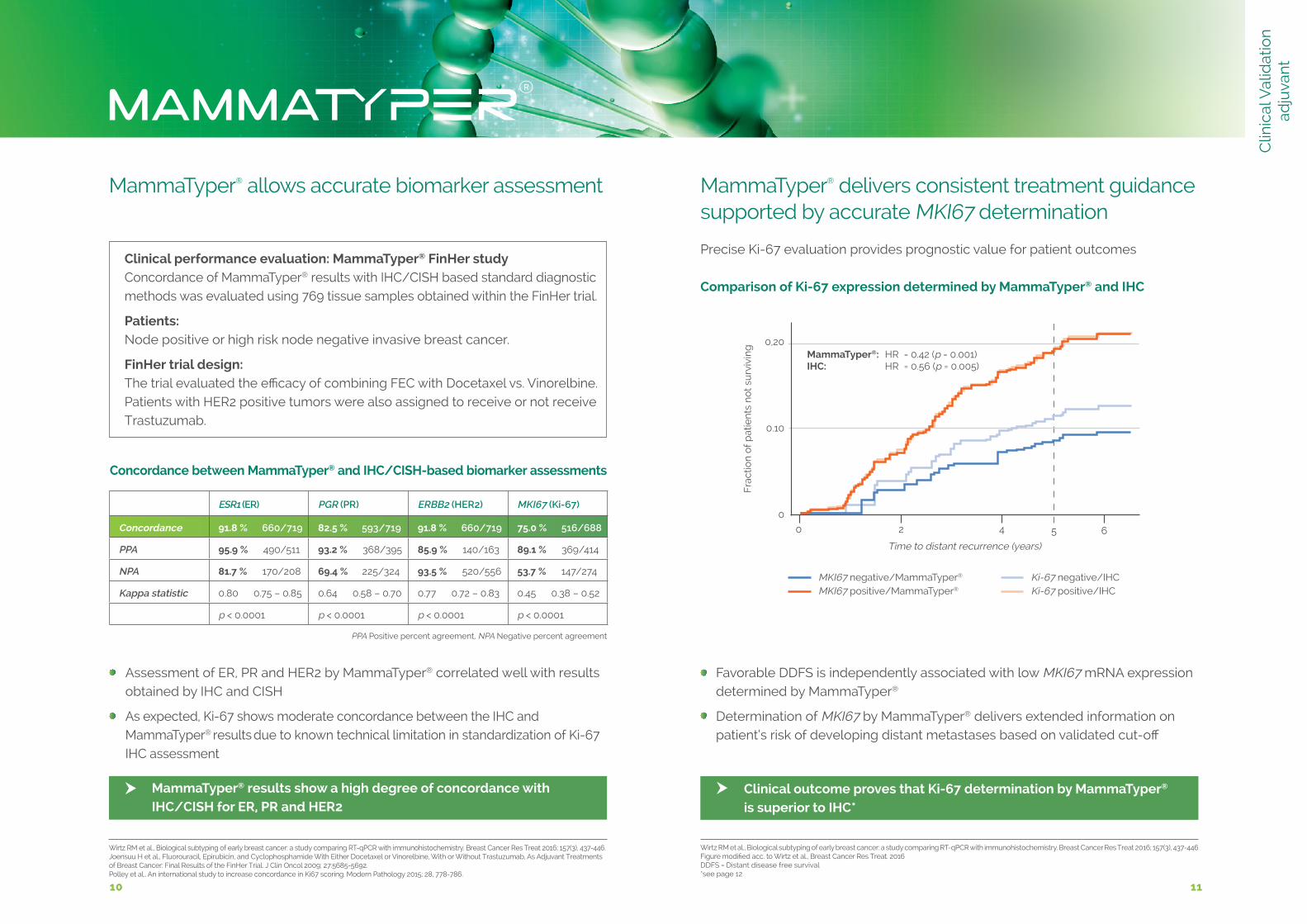
MammaTyper® delivers consistent treatment guidance supported by accurate MKI67 determination
Comparison of Ki-67 expression determined by MammaTyper® and IHC
Wirtz RM et al., Biological subtyping of early breast cancer: a study comparing RT-qPCR with immunohistochemistry. Breast Cancer Res Treat 2016; 157(3), 437-446Figure modified acc. to Wirtz et al., Breast Cancer Res Treat. 2016DDFS = Distant disease free survival *see page 12
0 2 4 6
Time to distant recurrence (years)
Fra
ctio
n o
f p
atie
nts
no
t su
rviv
ing
MKI67 negative/MammaTyper®
MKI67 positive/MammaTyper®
Ki-67 negative/IHCKi-67 positive/IHC
0,20
0.10
0
MammaTyper®: HR = 0.42 (p = 0.001)IHC: HR = 0.56 (p = 0.005)
5
Precise Ki-67 evaluation provides prognostic value for patient outcomes
Favorable DDFS is independently associated with low MKI67 mRNA expression determined by MammaTyper®
Determination of MKI67 by MammaTyper® delivers extended information on patient‘s risk of developing distant metastases based on validated cut-off
MammaTyper® allows accurate biomarker assessment
Clinical performance evaluation: MammaTyper® FinHer study Concordance of MammaTyper® results with IHC/CISH based standard diagnostic methods was evaluated using 769 tissue samples obtained within the FinHer trial.
Patients: Node positive or high risk node negative invasive breast cancer.
FinHer trial design: The trial evaluated the efficacy of combining FEC with Docetaxel vs. Vinorelbine. Patients with HER2 positive tumors were also assigned to receive or not receive Trastuzumab.
Wirtz RM et al., Biological subtyping of early breast cancer: a study comparing RT-qPCR with immunohistochemistry. Breast Cancer Res Treat 2016; 157(3), 437-446. Joensuu H et al., Fluorouracil, Epirubicin, and Cyclophosphamide With Either Docetaxel or Vinorelbine, With or Without Trastuzumab, As Adjuvant Treatments of Breast Cancer: Final Results of the FinHer Trial. J Clin Oncol 2009; 27:5685-5692. Polley et al., An international study to increase concordance in Ki67 scoring. Modern Pathology 2015; 28, 778-786.
Assessment of ER, PR and HER2 by MammaTyper® correlated well with results obtained by IHC and CISH
As expected, Ki-67 shows moderate concordance between the IHC and MammaTyper® results due to known technical limitation in standardization of Ki-67 IHC assessment
MammaTyper® results show a high degree of concordance with IHC/CISH for ER, PR and HER2
ESR1 (ER) PGR (PR) ERBB2 (HER2) MKI67 (Ki-67)
Concordance 91.8 % 660/719 82.5 % 593/719 91.8 % 660/719 75.0 % 516/688
PPA 95.9 % 490/511 93.2 % 368/395 85.9 % 140/163 89.1 % 369/414
NPA 81.7 % 170/208 69.4 % 225/324 93.5 % 520/556 53.7 % 147/274
Kappa statistic 0.80 0.75 – 0.85 0.64 0.58 – 0.70 0.77 0.72 – 0.83 0.45 0.38 – 0.52
p < 0.0001 p < 0.0001 p < 0.0001 p < 0.0001
PPA Positive percent agreement, NPA Negative percent agreement
Concordance between MammaTyper® and IHC/CISH-based biomarker assessments
Clinical outcome proves that Ki-67 determination by MammaTyper® is superior to IHC*
Clin
ical
Val
idat
ion
ad
juva
nt
12 13
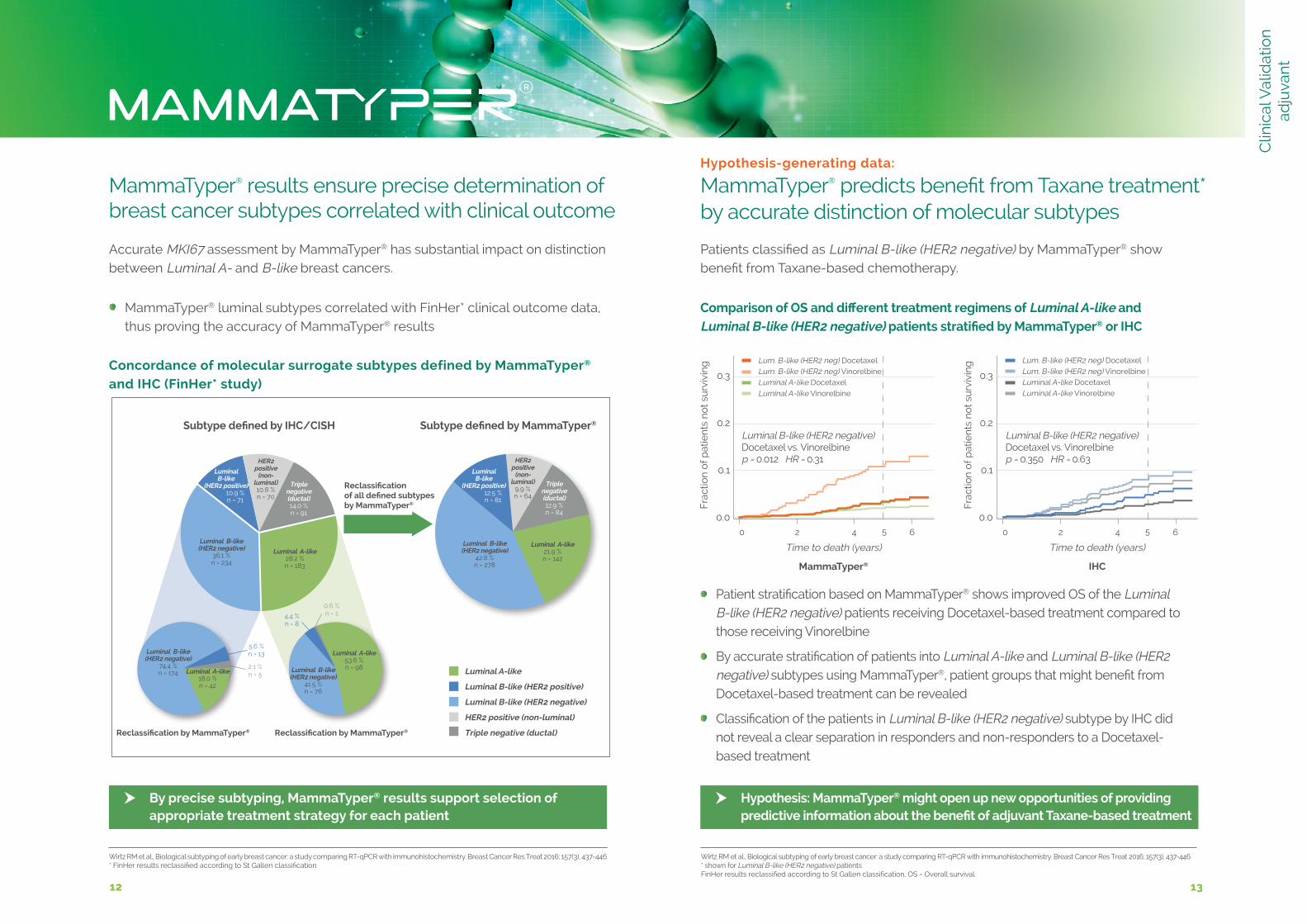
Triple negative (ductal)14.0 %n = 91
Luminal B-like (HER2 negative)
36.1 %n = 234
Luminal B-like
(HER2 positive)10.9 %n = 71
HER2 positive
(non- luminal)10,8 %n = 70
Luminal A-like28.2 %n = 183
Subtype defined by MammaTyper®
12 13
MammaTyper® results ensure precise determination of breast cancer subtypes correlated with clinical outcome
Concordance of molecular surrogate subtypes defined by MammaTyper® and IHC (FinHer* study)
Wirtz RM et al., Biological subtyping of early breast cancer: a study comparing RT-qPCR with immunohistochemistry. Breast Cancer Res Treat 2016; 157(3), 437-446* FinHer results reclassified according to St Gallen classification
Accurate MKI67 assessment by MammaTyper® has substantial impact on distinction between Luminal A- and B-like breast cancers.
MammaTyper® luminal subtypes correlated with FinHer* clinical outcome data, thus proving the accuracy of MammaTyper® results
Wirtz RM et al., Biological subtyping of early breast cancer: a study comparing RT-qPCR with immunohistochemistry. Breast Cancer Res Treat 2016; 157(3), 437-446 * shown for Luminal B-like (HER2 negative) patientsFinHer results reclassified according to St Gallen classification, OS = Overall survival
Subtype defined by IHC/CISH
Reclassification by MammaTyper® Reclassification by MammaTyper®
Reclassification of all defined subtypes by MammaTyper®
Luminal A-like
Luminal B-like (HER2 positive)
Luminal B-like (HER2 negative)
HER2 positive (non-luminal)
Triple negative (ductal)
By precise subtyping, MammaTyper® results support selection of appropriate treatment strategy for each patient
Hypothesis: MammaTyper® might open up new opportunities of providing predictive information about the benefit of adjuvant Taxane-based treatment
Triple negative (ductal)12.9 %n = 84
Luminal B-like (HER2 negative)
42.8 %n = 278
Luminal B-like
(HER2 positive)12.5 %n = 81
HER2 positive
(non- luminal)
9.9 %n = 64
Luminal A-like21.9 %n = 142
4.4 %n = 8
2.1 %n = 5
5.6 %n = 13
Comparison of OS and different treatment regimens of Luminal A-like and Luminal B-like (HER2 negative) patients stratified by MammaTyper® or IHC
Lum. B-like (HER2 neg) Docetaxel Lum. B-like (HER2 neg) Vinorelbine Luminal A-like Docetaxel Luminal A-like Vinorelbine
Luminal B-like (HER2 negative) Docetaxel vs. Vinorelbinep = 0.012 HR = 0.31
Luminal B-like (HER2 negative) Docetaxel vs. Vinorelbinep = 0.350 HR = 0.63
Lum. B-like (HER2 neg) Docetaxel Lum. B-like (HER2 neg) Vinorelbine Luminal A-like Docetaxel Luminal A-like Vinorelbine
MammaTyper® IHC
Fra
ctio
n o
f p
atie
nts
no
t su
rviv
ing
0 2 4 6
Time to death (years)
0.3
0.2
0.1
0.05
Time to death (years)
Fra
ctio
n o
f p
atie
nts
no
t su
rviv
ing
0 2 4 65
0.3
0.2
0.1
0.0
Patient stratification based on MammaTyper® shows improved OS of the Luminal B-like (HER2 negative) patients receiving Docetaxel-based treatment compared to those receiving Vinorelbine
By accurate stratification of patients into Luminal A-like and Luminal B-like (HER2 negative) subtypes using MammaTyper®, patient groups that might benefit from Docetaxel-based treatment can be revealed
Classification of the patients in Luminal B-like (HER2 negative) subtype by IHC did not reveal a clear separation in responders and non-responders to a Docetaxel- based treatment
Hypothesis-generating data: MammaTyper® predicts benefit from Taxane treatment* by accurate distinction of molecular subtypes
Patients classified as Luminal B-like (HER2 negative) by MammaTyper® show benefit from Taxane-based chemotherapy.
Luminal B-like (HER2 negative)
74.4 %n = 174 Luminal A-like
18.0 %n = 42
Luminal B-like (HER2 negative)
41.5 %n = 76
Luminal A-like53.6 %n = 98
0.6 %n = 1
Clin
ical
Val
idat
ion
ad
juva
nt
14 15
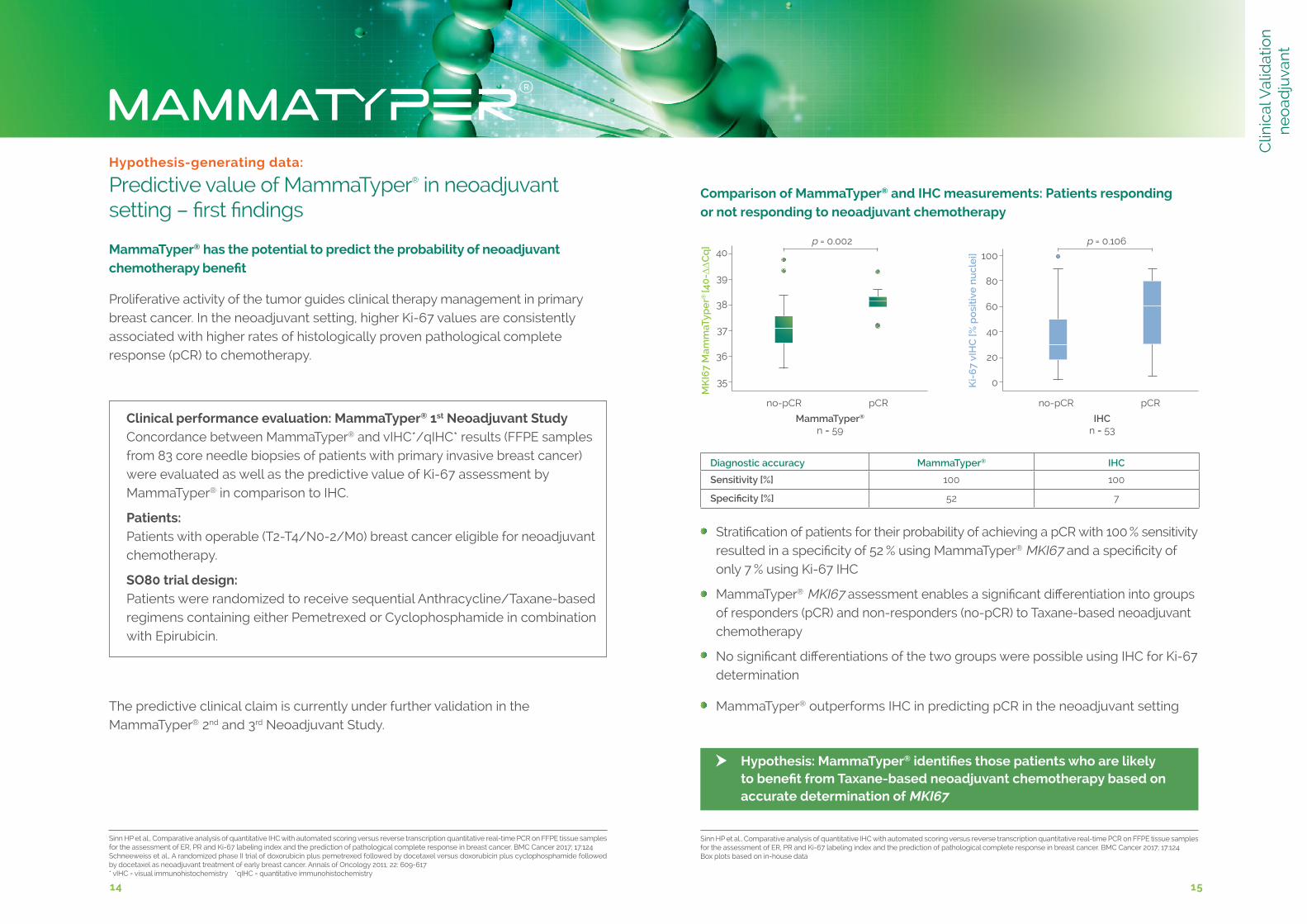
Sinn HP et al., Comparative analysis of quantitative IHC with automated scoring versus reverse transcription quantitative real-time PCR on FFPE tissue samples for the assessment of ER, PR and Ki-67 labeling index and the prediction of pathological complete response in breast cancer. BMC Cancer 2017; 17:124 Box plots based on in-house data
Comparison of MammaTyper® and IHC measurements: Patients responding or not responding to neoadjuvant chemotherapy
Stratification of patients for their probability of achieving a pCR with 100 % sensitivity resulted in a specificity of 52 % using MammaTyper® MKI67 and a specificity of only 7 % using Ki-67 IHC
MammaTyper® MKI67 assessment enables a significant differentiation into groups of responders (pCR) and non-responders (no-pCR) to Taxane-based neoadjuvant chemotherapy
No significant differentiations of the two groups were possible using IHC for Ki-67 determination
MammaTyper® outperforms IHC in predicting pCR in the neoadjuvant setting
Hypothesis: MammaTyper® identifies those patients who are likely to benefit from Taxane-based neoadjuvant chemotherapy based on accurate determination of MKI67
Hypothesis-generating data: Predictive value of MammaTyper® in neoadjuvant setting – first findings
Clinical performance evaluation: MammaTyper® 1st Neoadjuvant StudyConcordance between MammaTyper® and vIHC*/qIHC* results (FFPE samples from 83 core needle biopsies of patients with primary invasive breast cancer)were evaluated as well as the predictive value of Ki-67 assessment by MammaTyper® in comparison to IHC.
Patients: Patients with operable (T2-T4/N0-2/M0) breast cancer eligible for neoadjuvant chemotherapy.
SO80 trial design: Patients were randomized to receive sequential Anthracycline/Taxane-based regimens containing either Pemetrexed or Cyclophosphamide in combination with Epirubicin.
Sinn HP et al., Comparative analysis of quantitative IHC with automated scoring versus reverse transcription quantitative real-time PCR on FFPE tissue samples for the assessment of ER, PR and Ki-67 labeling index and the prediction of pathological complete response in breast cancer. BMC Cancer 2017; 17:124 Schneeweiss et al., A randomized phase II trial of doxorubicin plus pemetrexed followed by docetaxel versus doxorubicin plus cyclophosphamide followed by docetaxel as neoadjuvant treatment of early breast cancer. Annals of Oncology 2011; 22: 609-617* vIHC = visual immunohistochemistry *qIHC = quantitative immunohistochemistry
The predictive clinical claim is currently under further validation in the MammaTyper® 2nd and 3rd Neoadjuvant Study.
MammaTyper® has the potential to predict the probability of neoadjuvant chemotherapy benefit
Proliferative activity of the tumor guides clinical therapy management in primary breast cancer. In the neoadjuvant setting, higher Ki-67 values are consistently associated with higher rates of histologically proven pathological complete response (pCR) to chemotherapy.
Diagnostic accuracy MammaTyper® IHC
Sensitivity [%] 100 100
Specificity [%] 52 7
Ki-
67
vIH
C [%
po
siti
ve n
ucl
ei] 100
80
60
40
20
0
no-pCR pCR
IHCn = 53
MK
I67
Mam
maT
ype
r® [4
0-ΔΔ∆∆C
q]
40
39
38
37
36
35
no-pCR pCR
MammaTyper®
n = 59
p = 0.002 p = 0.106
Clin
ical
Val
idat
ion
n
eo
adju
vant
Service for Germany:BioNTech Diagnostics GmbH An der Goldgrube 12 55131 Mainz, Germany
Tel: +49 6131 9084 2001Fax: +49 6131 9084 39 2001E-Mail: [email protected]
Visit us online:+ biontech.de + mammatyper.com
Precise quantitative results for mRNA expression of HER2, ER, PR and Ki-67
Outperforms IHC by accurate Ki-67 determination
Accurate and reliable test to stratify breast cancer into surrogate subtypes acc. to St Gallen
Highly reproducible results with extremely low inter-/intra-laboratory variation
Clinical value has been validated in numerous performance evaluation studies
Extended information on patient‘s prognosis
Accurate subtyping supports treatment decisions
Reliable method for any pathology laboratory
Easy-to-use test which allows results within 6 hours
High-performance
Reproducible
Validated
Prognostic
Predictive
Optimized
Easy-to-use
To order MammaTyper® or for further information, please contact your local distributor:
Innovation for your breast cancer diagnostics
150
529
-01-
EN
Re
v. 2
.0
All scientific and technical information in this brochure is based on the MammaTyper® Instructions for Use Rev. 3.1 and Wirtz et al., Breast Cancer Res Treat. 2016; 157(3) 437-446; Laible et al., BMC Cancer 2016; DOI: 10.1186/s12885-016-2476-x; Varga Z et al., Breast Cancer Research 2017; 19:55: DOI 10.1186/s13058-017-0848-z; Sinn et al., BMC Cancer 2017; 17:124











![Introduction to Tokyo Climate Center (TCC) and TCC ...ds.data.jma.go.jp/tcc/tcc/library/library2015/... · Introduction to TCC and TCC training seminar 2015 / Plans for 2015 [1] In](https://img.pdfslide.us/doc/110x75/600dca8f9be1e172842925cf/introduction-to-tokyo-climate-center-tcc-and-tcc-dsdatajmagojptcctcclibrarylibrary2015.jpg)

















