Embed Size (px)
Citation preview

10/22/2018
1
INNOVATE
INTEGRATE
TRANSFORMBarbara Martin, RN, MSN, ACNP-BC, MPH,
Colorado State Innovation Model Director
CHA Patient Safety Conference, Oct. 23, 2018
Fund: The Colorado State Innovation Model (SIM) and Transforming Clinical
Practice Initiative are funded by the Centers for Medicare & Medicaid
Services with up to
$76 million to reform health care payment and delivery systems.
Collaborate: Colorado was the only SIM state to focus on integrated
behavioral and physical health in primary care settings with support from
public and private payers to help providers succeed with APMs.
TCPi rounds out the equation of providers, who have access to health reform
support and 80% are specialists working on business supports, process
changes for success with APMs.
Systems change: These Governor’s office initiatives are investing in
hundreds of providers, community mental health centers and local public
health agencies to set the stage for future success.
HEALTH REFORM
2

10/22/2018
2
WHY INTEGRATION MATTERS
> 50%
80%50%
Of referrals from primary care to an outpatient behavioral
health clinic do not make the 1st appointment
Of people with a behavioral
health disorder visit a primary
care at least once a yearOf behavioral health
disorders are treated in
primary care
WHY IT MATTERS TO YOU
Sources: https://www.cdc.gov/nchs/fastats/mental-health.htm
https://www.hcup-us.ahrq.gov/reports/statbriefs/sb216-Mental-Substance-Use-Disorder-ED-Visit-Trends.jsp
• Number of visits to physician offices with mental disorders as the primary
diagnosis: 59.8 million
• Number of visits to EDs with mental disorders as primary diagnosis: 5.7 million
• Between 2006 and 2013, the rate of ED visits increased across mental and
substance use disorders, but the increase was higher for mental disorders
(55.5% for depression, anxiety or stress reactions and 52.0% for psychoses
and bipolar disorders) than for SUDs (37.0%)

10/22/2018
3
5
BEHAVIORAL HEALTH IN THE HOSPITAL
Sources: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb225-Inpatient-US-Stays-Trends.pdf
https://www.hcup-us.ahrq.gov/reports/statbriefs/sb216-Mental-Substance-Use-Disorder-ED-Visit-Trends.jsp
• From 2005-2014 the total number of hospital stays for mental
health/substance use conditions
rose 12.2% in the U.S. In comparison, overall hospital stays for all conditions
dropped by 6.6%
• Driving the increase in hospitalizations were patients from 0-17 and 45-64
years of age
• In 2005 mood disorders were not found in the top 5 reasons for
hospitalization in these
populations yet in 2014 mood disorders were the top reason for
hospitalizations for these
ages 0-17 as well as 18-44 and it’s number 3 for 45-64

10/22/2018
4
7
System barrier and facilitators can influence
communication, collaboration and coordination
▪ Financing
▪ Data exchange
▪ A culture of communication collaboration and
coordination
▪ Recognizing an evolving landscape—older population, co-
morbid disease, increasing severity of behavioral health
BREAKING THE CYCLE
8

10/22/2018
5
SYSTEM BARRIERS
9
Effective communication exists when each clinician or treatment
provider caring for patients shares needed treatment information
with other clinicians and providers caring for that patient.
Information can be shared verbally, manually in writing or through
information technology, such as a shared electronic health record.
Collaboration is multidimensional and requires the aggregation of
several behaviors, including:
▪ A shared understanding of goals and roles
▪ Effective communication
▪ Shared decision making
CHANGING THE SYSTEM
10

10/22/2018
6
THE SIM APPROACH
Public
Health
Behavior
al Health
Providers
Consumers
Consumer Engagement Policy Workforce Evaluation
Practice
Transformation
Payment
ReformPopulation
HealthHIT
Increase access
to integrated care in coordinated
systems supported by value-based payment
Support for
practices as they
accept new
payment models
and integrate
behavioral and
physical healthcare.
Engaging
communities in
prevention,
education, and
improving access
to integrated
care.
Development and
implementation of
value-based
payment models
that incentive
integration and
improve quality
of care.
Secure and
efficient use of
technology across
health and non-
health sectors in
order to advance
integration and
improving health.
11
12
KEY
RHC = Regional Health
Connector
CHITA = Clinical HIT Advisor
PF = Practice Facilitator
Grants to Practices
Each practice can apply for
competitive small grants of up
to $40,000 to offset initial costs
of integration. Alternative Payment Models
Each practice will be supported
with value-based payments from
at least one of the seven payers
that signed the SIM MOU.
Achievement-Based Payments
Each practice participating in
SIM is eligible to receive
achievement-based payments.
Regional Health Connectors
Each SIM practice will be
matched with a regional health
connector, who will serve as a
dedicated resource for
connecting the practice to
relevant resources.
Business Consultation
MGMA provides resources and
assistance to help practices
improve business processes and
accept alternative payment
models.
Practice Facilitators and CHITAs
Each SIM practice is matched
with an appropriate practice
transformation organization that
provides them with a practice
facilitator (PF) and/or a clinical
health information technology
advisor (CHITA), as well as other
technical assistance.

10/22/2018
7
BI-DIRECTIONAL PILOT
SIM is helping providers integrate behavioral and physical
health in primary care settings to ID all health issues
early and help ensure that patients get the care when
and where they need it.
The key is effective collection, analysis and use of data.
REFORMING CARE
14

10/22/2018
8
▪MACRA/QPP and other emerging alternative payment models include measures of cost control, either as an adjustment to practice payments or through shared savings and/or shared risk
▪ Practices have had little to no data to help
them work on this
▪ It is critically important for practices to begin
to learn how to use cost data to reduce
unnecessary costs and improve patient care
and safety
HELPING PROVIDERS USE DATA
COST & UTILIZATION MEASURES
▪ Out of Pocket Expenditures for Consumers
▪ Total Cost of Care Population based Per member per-month (PMPM) Index
▪ Admissions
▪ Emergency Department (ED) Rate
▪ Follow-Up after Hospitalization for Mental Illness
▪ Readmissions
▪ PsychiatricAdmissions
▪ Psychiatric ED Rate
▪ Psychiatric Readmissions

10/22/2018
9
APCD DATA ATTRIBUTION
▪ All Payer Claims Database (APCD) data
▪ Medicare, Medicaid, commercial claims
▪ Includes detailed membership and claims data for inpatient facility, outpatient facility, professional services, ancillary services and prescription drugs (all healthcare costs)
▪ Attribution based on NPIs reported by practices on SIM practice roster
USING DATA EFFECTIVELY
▪ Sample SIM practice cost and utilization report

10/22/2018
10
OTHER DATA SOURCES
Milliman cost & utilization reports StratusTM data aggregationtool
APCD data Payers submit directly or via APCD
All payers 6 payers that support the tool
SIM standard attribution methodology Proprietary payer attribution
Methodology
9 SIM cost and utilization measures
(aligned with CMMI report)
3 HEDIS measures; filters & custom reports
on claims data; gaps in care
6 month – 1 year time lag Might be more recent if payers submit
directly
Quarterly reports Monthly – quarterly data refreshes
IMPROVING PATIENT HEALTH
20
SIM practices are screening more patients to ID and
address issues early. In 2017 SIM practices screened:
• 59% of eligible moms for maternal depression
• 81% of eligible children for developmental issues
• 86% of eligible adolescents for obesity
• 98% of eligible patients for tobacco use
• 20% of patients with diabetes had poor HBA1c levels*

10/22/2018
11
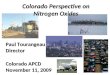
49.71%56.32%
65.71%
36.02%
61.2…62.49%
52%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
2017 Q2 2017 Q3 2017 Q4 2018 Q1 2018 Q2
Cohort 2 Cohort 3 CMHCs Primary care target
21
Aggregate percent of eligible patients screened for depression
as reported by the CMHCs and cohorts 2 and 3
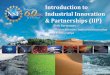
37.50%
28.64% 32.17%
8.98%
21.70%
22.80%
29.80%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
2017 Q2 2017 Q3 2017 Q4 2018 Q1 2018 Q2
Cohort 2 Cohort 3 CMHCs Primary care targets
22
Lower values are desired for this measure
Aggregate percent of patients with diabetes and who have poor HbA1c
control in cohort practices sites and CMHCs

10/22/2018
12
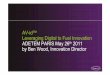
595.14
568.15
550.00
555.00
560.00
565.00
570.00
575.00
580.00
585.00
590.00
595.00
600.00
Q4 (2015) Q4 (2016)
ED rate for primary care disorders for patients attributed to
SIM cohort-1 primary care practices (per 1,000 population)
▪ SIM launched a service to help primary care practice sites extract electronic clinical quality measures (eCQMs) once and report to several approved entities.
▪The first phase includes 11 practices and 90 providers and the second phase will include 190 practices.
▪The application for phase 2 of the SIM eCQM solution is open: www.surveymonkey.com/r/5CYV5CW.
24
SIM SUPPORTS

10/22/2018
13
ECQM PROJECT
▪ Three organizations contracted with SIM and formed Health Data Colorado (HDCo)
▪ CORHIO (front range, eastern plains)
▪ QHN (western slope)
▪ CCMCN (safety net providers)
▪ Phase 1 — Initial phase
▪ Completed July 31, 2018
▪ All 3 organizations worked with about 12 practices in total
▪ Collected 3 eCQMs
▪ Phase 2 — full implementation — HDCO will work with CHITAs
▪ Working with SIM practices — open to 190
▪ Collecting 9 SIM measures
▪ Field-level data through custom extracts or other methods
25
While SIM is helping primary care providers deliver whole-
person care, TCPi is focused on helping providers (mainly
specialists) ensure the delivery of patient-centered, team-
based care.
By intervening early—patients avoid unnecessary ED visits
that do not lead to better health outcomes and have a
negative effect on your bottom line.
SIM is also investing in local public health agencies and
created a new workforce to help ensure that providers know
about community resources to avoid duplication of efforts.
EFFECTIVE, EFFICIENT CARE
26

10/22/2018
14
Q3 AND Q4 2017 FEEDBACK
27
11.8%
29.4%
52.9%
5.9%
4.2%
45.8%
37.5%
12.5%
0% 20% 40% 60% 80% 100%
Awareness
Cooperating
Coordinating
Integrating
LPHA/BHTC
SIM-funded LPHAs, BHTCs and RHCs
report positive progress:
▪ RHCs are forming important
partnerships in their communities
that link health systems with
community partners
▪ LPHA education/outreach efforts
reached 12,108,987 individuals
during Q2–Q3 2017
▪ BHTCs referred 3,283 participants
to behavioral health resources
28

10/22/2018
15
• Commitment: 2,000 clinicians
• Enrolled: 1,972
• 99% progress toward goal
Aim 1: Engagement
• Commitment: Improve 28,904 lives
• Lives Improved: 24,823 lives
• 85% progress toward goal
Aim 2:Improve health
outcomes
• Commitment: 1,704
• Admissions avoided: 6,169
• 360% progress toward goal
Aim 3: Reduce unnecessary
hospitalizations
TCPI COMMITMENTS AND RESULTS
• Commitment: $85.6 million
• $42 million
• 49% progress toward goal
Aim 4: Save dollars for the health care system
• Commitment: 4,000 tests reduced
• Test reduced: 3,267
• 85% progress toward goal
Aim 5: Reduce unnecessary tests and procedures
• Commitment: 410 clinicians
• Graduated: 363 clinicians to CPC+ and MSSP Track 3 (18%)
• 20% progress toward goal
Aim 6: Graduate to APM
TCPI COMMITMENTS AND RESULTS

10/22/2018
16
31
PROVIDER SPECIALTIES
Anesthesiology
Bariatric Medicine
Behavioral Health
Cardiology
Colon and Rectal
Surgery
Dermatology
Emergency Medicine
Family Medicine
Fetal Medicine
Gastroenterology
General Surgery
Hospice
Infectious Disease
Internal Medicine
Interventional
Radiology
Nephrology
Neurology
Neurosurgery
OB/GYN
Oncology
Ophthalmology
Orthopaedics
Otolaryngology
Pain Management
Pediatric Medicine
Pediatric Surgery
Physical Therapy
Plastic &
Reconstructive
Surgery
Podiatry
Psychiatry
Pulmonology
Radiology
Rheumatology
Surgery
Urology
Primary Care Other Specialists
Behavioral Health
204 Practices
1,972 Clinicians
87% Specialty Care
USING DATA TO BRIDGE THE GAP
▪ Colorado providers have recognized the value of effective communication (and the processes that back it up)
▪ Optimization of EHRs, health information exchanges
▪ Effective huddles, actionable referrals
▪ Patient education, discussion, follow-up
▪ Working as a team that extends beyond the four-walls of a clinic, providers and hospitals can improve patient outcomes, lower costs and succeed financially

10/22/2018
17
INFLUENCING PATIENT CARE, SAFETY
▪ TCPi helps providers retool processes, which results in cost-savings and cost avoidance. One example:▪ A small, specialty practice improved access via same-day appointments
and “special alert” phone protocols, which helped endocrine patients avoid more than 300 ED visits per year
▪ Avoided unnecessary duplicative testing by routine use of HIE
▪ Provided ongoing patient education, teach-back and shared decision making, medication management and use of patient portal for communication and follow-up
SUCCESS WITH APMS
34
• Prepare providers for success in the Medicare Quality Payment Program
and Merit-Based Incentive Program
• 323 MIPS- eligible providers in 2017 reporting year
• More than 97% of Colorado TCPi eligible providers reported
• Practices are preparing for alternative payment models (APMs) and using
TCPi to understand data
• Expect to transition 400+ providers to APMs
• TCPi national goal of to move 75% of providers into value-based
contracts
• Limited availability of APMs for specialists could affect Colorado’s
ability to transition specialists to APMs

10/22/2018
18
• Solo Obstetrics/Gynecology
• Serving 4,189 patients
• Avoided 302 ED visits, which saved $257,908 annually
by offering same-day appointments
• Saved $120,000 per year by assessing surgical trays;
went from $3,000 to $106 per surgery
EXEMPLAR PRACTICE
• Largest retina practice in the Rocky Mountain region
• Number of patients served: 18,046
• 12 providers
• Reduced ED visits by 231
• $197,914 in savings by offering same day appointments
• Saved $20 million by changing injectables compared with national average of peers
EXEMPLAR PRACTICES

10/22/2018
19
• Part of large safety-net health system
• 3,500 patients served per year
• 4 providers
• Reduced ED visits <14 days of surgery by 33%
• Estimated cost savings: $16,275/year
• Successful process change spreading to other clinics in the system
EXEMPLAR PRACTICES
LESSONS LEARNED
38

10/22/2018
20
SUSTAINING INNOVATION
Payment reform to achieve a healthier Colorado
Support for value-based payments and coordination across providers and stakeholders to encourage patient-centered, team-based care that improves
health outcomes and reduces or avoids unnecessary costs
39
• Advance primary care engagement and success in alternative payment models; incremental steps toward participation
• Support integration of physical and behavioral health
• Bolster primary care infrastructure and build off success and lessons learned in SIM and CPC+
Multi-payer advanced alternative payment model for primary care
• Provide flexibility and financial stability for hospitals to best serve their communities and align with other service providers
• Population health objectives and health goals related to quality and performance
• Voluntary participation for rural hospitals
Global budgets for some rural hospitals
TELEHEALTH: EXPANDING ACCESS TO CARE
▪ SIM will fund three health systems with up to $250,000 each to develop an implementation model for an e-Consult program.
▪ Up to $100,000 can be spent on technology.
▪ RFP released by the Department of Health Care Policy & Financing Oct. 18: https://lnkd.in/ee_HAZ6. Interested parties must apply by Nov. 19, 2018.
▪ UHAA 2019000083 e-Consult Planning and Implementation Project seeks a Contractor to solicit competitive, responsive proposals from experienced and financially sound health care entities to plan for and test electronic consultations (e-Consults).
40

10/22/2018
21
QUESTIONS AND DISCUSSION
The project described was supported by Funding Opportunity Number CMS-1G1-14-001 from the U.S Department of Health and Human
Services (HHS), Centers for Medicare & Medicaid Services (CMS). The Colorado State Innovation Model (SIM), a four-year initiative, is
funded by up to $65 million from CMS. The content provided is solely the responsibility of the authors and does not necessarily
represent the official views of HHS or any of its agencies.