Embed Size (px)
Citation preview

Injuries To The Hand Injuries To The Hand And DigitsAnd Digits
Chrisnel Jean, D.O.Chrisnel Jean, D.O.May 30, 2006May 30, 2006
Reviewed by Dr. BatizyReviewed by Dr. Batizy

OutlineOutline
AnatomyAnatomy Principles of EvaluationPrinciples of Evaluation
General Hand ExaminationGeneral Hand Examination Anesthesia and Direct Wound Anesthesia and Direct Wound
ExaminationExamination Radiographs, Consultation, Radiographs, Consultation,
and Dispositionand Disposition
Tendon InjuriesTendon Injuries Flexor / Extensor TendonsFlexor / Extensor Tendons
Ligaments And Dislocation Ligaments And Dislocation InjuriesInjuries
Compartment SyndromeCompartment Syndrome High-Pressure Injection InjuryHigh-Pressure Injection Injury

Hand AnatomyHand Anatomy Hand consist of 27 Hand consist of 27
bones:bones: 14 Phalangeal bones14 Phalangeal bones 5 Metacarpal bones5 Metacarpal bones 8 Carpal bones8 Carpal bones
Carpal bones are Carpal bones are made up of two rows of made up of two rows of four bones bridged by four bones bridged by flexor retinaculum flexor retinaculum which forms the carpal which forms the carpal tunnel.tunnel.
Carpal tunnel consist Carpal tunnel consist of the median nerve of the median nerve and the nine long and the nine long flexor of the fingersflexor of the fingers

Hand AnatomyHand Anatomy Intrinsic muscle of the Intrinsic muscle of the
hand:hand: Have their origins and Have their origins and
insertions within the insertions within the hand.hand.
Consist the following:Consist the following: Thenar, Hypothenar, Thenar, Hypothenar,
adductor pollicies, the adductor pollicies, the interossei and the interossei and the lumbricalslumbricals. (Refer to pg . (Refer to pg 1665 for anatomical 1665 for anatomical description)description)

Hand AnatomyHand Anatomy
Extensor Tendons:Extensor Tendons: Courses over the dorsal side of the forearm, Courses over the dorsal side of the forearm,
wrist and hand.wrist and hand. 9 extensor tendons pass under the extensor 9 extensor tendons pass under the extensor
retinaculum and separate into 6 retinaculum and separate into 6 compartmentscompartments

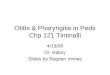
Surface anatomy of the hand.
The tendons that are palpated with thumb abducted and extended form an anatomic snuff-box.

Hand AnatomyHand Anatomy
Extensor Tendons:Extensor Tendons:
The extensor tendons gain entrance to the hand from the forearm through a series of six canals, five fibroosseous and one fibrous The communis tendons are joined distally near the MP joints by fibrous interconnections called juncturae tendinum. Beneath the retinaculum, the extensor tendons are covered with a synovial sheath.

Hand AnatomyHand Anatomy
Extensors digitorum communis are Extensors digitorum communis are connected by junctura.connected by junctura.
Because of this, a complete tendon Because of this, a complete tendon laceration proximal to the junction may laceration proximal to the junction may still result in normal extensor fuction.still result in normal extensor fuction.

Hand AnatomyHand Anatomy
Flexor Tendons:Flexor Tendons: Courses over the volar side of the forearm, wrist, Courses over the volar side of the forearm, wrist,
and hand.and hand.
Unlike the extensor tendons, the flexor tendons are Unlike the extensor tendons, the flexor tendons are enclosed in synovial sheaths making them prone enclosed in synovial sheaths making them prone to deep space infections.to deep space infections.

Hand AnatomyHand Anatomy
Flexor Tendons:Flexor Tendons: Flexor carpi Flexor carpi
radialis, flexor radialis, flexor carpi ulnaris, carpi ulnaris, and palmaris and palmaris longus primarily longus primarily flex the wristflex the wrist

Hand AnatomyHand Anatomy

Hand AnatomyHand Anatomy
9 flexor tendons pass through the carpel 9 flexor tendons pass through the carpel tunnel:tunnel:
1 tendon go to the base of the dist. Phalanx of the 1 tendon go to the base of the dist. Phalanx of the thumbthumb
The other 4 digit has 2 tendon each (FDS / FDP).The other 4 digit has 2 tendon each (FDS / FDP).

Hand AnatomyHand Anatomy Flexor digitorum Flexor digitorum
superficialis (FDS) superficialis (FDS) insert into middle insert into middle phalanx.phalanx.
Flexor digitorum Flexor digitorum profundus (FDP) runs profundus (FDP) runs deep to the FDS until deep to the FDS until the level of the MP joint the level of the MP joint where FDS bifurcates.where FDS bifurcates.
FDP inserts at the base FDP inserts at the base of the distal phalanx of the distal phalanx and acts primarily to and acts primarily to flex the DIP joint as well flex the DIP joint as well as all other joints flexed as all other joints flexed by FDS. (Figure 268-5).by FDS. (Figure 268-5).

Hand AnatomyHand Anatomy Blood supply (BS):Blood supply (BS):
Hand and digits has Hand and digits has dual (BS) with dual (BS) with contributions from contributions from the radial and ulnar the radial and ulnar arteries.arteries.

Hand AnatomyHand Anatomy
Blood supply (BS):Blood supply (BS):
Proximal portions of the hand (BS) come from Proximal portions of the hand (BS) come from the deep and superficial arches on the palmar the deep and superficial arches on the palmar and dorsal side.and dorsal side.
BS of the fingers is distributed by the digital BS of the fingers is distributed by the digital arteries that arises from the superficial palmer arteries that arises from the superficial palmer arch.arch.

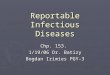
Hand Anatomy - Blood supplyHand Anatomy - Blood supply
The Allen's test.

Hand AnatomyHand Anatomy
The cutaneous nerve supply in the hand. M, median; R, radial; U, ulnar; PCM, palmar cutaneous branch of median nerve; DCU, dorsal cutaneous branch of ulnar nerve

Principles of EvaluationPrinciples of Evaluation
History:History: Should include the time, the cause of the Should include the time, the cause of the
injury and eval for the possibility of crush, injury and eval for the possibility of crush, burn, or chemical exposure. burn, or chemical exposure.
The patient’s occupation, prior hand injuries, The patient’s occupation, prior hand injuries, and handedness should be documentedand handedness should be documented

Principles of EvaluationPrinciples of Evaluation
The position of the hand at the time of The position of the hand at the time of injury should be determined.injury should be determined.
Injuries with the digits in flexion may Injuries with the digits in flexion may result in retraction of the cut end of the result in retraction of the cut end of the tendon when the digit is examined in tendon when the digit is examined in neutral position.neutral position.

Principles of EvaluationPrinciples of Evaluation
Physical ExamPhysical Exam Should detail the extent of injury by Should detail the extent of injury by
documenting the following:documenting the following: Amount of devascularizationAmount of devascularization Status of the skinStatus of the skin Posture of the fingersPosture of the fingers Presence of deformityPresence of deformity Active bleedingActive bleeding B/L grip strength B/L grip strength

Principles of EvaluationPrinciples of Evaluation
Physical ExamPhysical Exam ROM and strength should be tested against ROM and strength should be tested against
resistance.resistance.
Nerve testing: Nerve testing: Test Test median nervemedian nerve: :
Have the pt flex the distal phalanx of the thumb against Have the pt flex the distal phalanx of the thumb against resistanceresistance
Test opposition by touching the tip of the thumb to the tip of Test opposition by touching the tip of the thumb to the tip of the little fingerthe little finger
The pt will be unable to oppose against resistence if The pt will be unable to oppose against resistence if median nerve function is lost.median nerve function is lost.

Principles of EvaluationPrinciples of Evaluation
Nerve testingNerve testing
Test Test median nervemedian nerve: : Test thumb abduction by placing the hand palm up Test thumb abduction by placing the hand palm up
and raising the thumb to the perpendicular while and raising the thumb to the perpendicular while palpating the belly of the abductor pollicis muscle palpating the belly of the abductor pollicis muscle to insure it is contracting.to insure it is contracting.

Principles of EvaluationPrinciples of Evaluation
Nerve testing:Nerve testing: To test To test ulnar nerveulnar nerve
Spread the fingers apart against resistance and Spread the fingers apart against resistance and then push them together against resistance.then push them together against resistance.
Test the hypothenar muscle, extend the fingers Test the hypothenar muscle, extend the fingers and then move the fifth finger away from the othersand then move the fifth finger away from the others
Test thumb adduction (ulnar nerve innervates the Test thumb adduction (ulnar nerve innervates the adductor pollicis muscles) bring the thumb tightly adductor pollicis muscles) bring the thumb tightly against the side of the index finger.against the side of the index finger.

Principles of EvaluationPrinciples of Evaluation
Nerve testing:Nerve testing: To test To test ulnar nerveulnar nerve
Adductor strength can be further tested by Adductor strength can be further tested by interposing a piece of paper between the thumb interposing a piece of paper between the thumb and the side of the index finger and then trying to and the side of the index finger and then trying to pull the paper away.pull the paper away.
To test To test radial nerveradial nerve:: Extend the fingers and wrist.Extend the fingers and wrist. With the thumb in the hitchhiking position, test its With the thumb in the hitchhiking position, test its
resistance to further extension.resistance to further extension.

Principles of EvaluationPrinciples of Evaluation
Nerve testing: SensationNerve testing: Sensation Determined by 2-point discrimination.Determined by 2-point discrimination.
Normal 2-point discrimination is <6 mm at the Normal 2-point discrimination is <6 mm at the fingertips and is often <2 mm. Both injured fingertips and is often <2 mm. Both injured and non-injured fingers must be compared.and non-injured fingers must be compared.
Repeat 2-point discrimination testing 2 – 4 Repeat 2-point discrimination testing 2 – 4 times on each side of the digit (80% accuracy times on each side of the digit (80% accuracy is considered acceptable)is considered acceptable)

Principles of EvaluationPrinciples of Evaluation
Nerve testing: SensationNerve testing: Sensation A sensory deficit implies a potential digital A sensory deficit implies a potential digital
artery laceration because of the close artery laceration because of the close proximity of the two.proximity of the two.
Tendon testing:Tendon testing: Full ROM of each tendon against resistance Full ROM of each tendon against resistance
should be assessed and compared with the should be assessed and compared with the uninjured side. uninjured side.

Principles of EvaluationPrinciples of Evaluation
Tendon testing:Tendon testing: Important to test resistance because up to Important to test resistance because up to
90 % of a tendon can be lacerated with 90 % of a tendon can be lacerated with preservation of ROM without resistance.preservation of ROM without resistance.
Pain along the course of the tendon during Pain along the course of the tendon during resistance testing suggests a partial resistance testing suggests a partial laceration even if the strength appears laceration even if the strength appears adequate.adequate.

Principles of EvaluationPrinciples of Evaluation
Tendon testing:Tendon testing: FDP is tested by flexing the DIP against FDP is tested by flexing the DIP against
resistance while the MP and PIP are held in resistance while the MP and PIP are held in extension.extension.
FDS is tested by flexing the PIP against FDS is tested by flexing the PIP against resistance while the remaining fingers are resistance while the remaining fingers are held.held.

Principles of EvaluationPrinciples of Evaluation
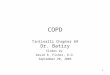
FDP is testedFDP is tested
To test for an intact profundus tendon, the examiner maintains the digit in extension while the patient attempts to flex the terminal phalanx.

Principles of EvaluationPrinciples of Evaluation
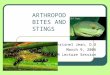
FDS is testedFDS is tested
Examination to assess function of flexor digitorum superficialis.

Principles of EvaluationPrinciples of Evaluation
Anesthesia and Direct Wound Anesthesia and Direct Wound Examination:Examination: Sensation and ROM should be tested before Sensation and ROM should be tested before
anesthesia applied.anesthesia applied.
Exam should be done under a bloodless field Exam should be done under a bloodless field by applying local tourniquet or penrose drain by applying local tourniquet or penrose drain around the base of the finger.around the base of the finger.

Principles of EvaluationPrinciples of Evaluation
Radiographs, Consultation, and Radiographs, Consultation, and Disposition:Disposition: XRAY: should include a PA, lateral , and XRAY: should include a PA, lateral , and
oblique view.oblique view. Injuries requiring immediate and delayed Injuries requiring immediate and delayed
follow-up by a hand surgeon are listed in follow-up by a hand surgeon are listed in Tables 268-1 and 268-2.Tables 268-1 and 268-2.
Guidelines for adequate immobilization and Guidelines for adequate immobilization and follow-up for specific hand injuries are listed in follow-up for specific hand injuries are listed in Tables 268-3Tables 268-3

Principles of EvaluationPrinciples of Evaluation
Tendon injuries: Flexor tendonsTendon injuries: Flexor tendons Most common cause of flexor tendon injury is Most common cause of flexor tendon injury is
a laceration.a laceration.
A distal to proximal five zone (I – V) A distal to proximal five zone (I – V) classification system for flexor tendon injuries classification system for flexor tendon injuries has been developed based on location, has been developed based on location, treatment considerations, and prognosis. treatment considerations, and prognosis.
Refer to pg 1670 for specific descriptions.Refer to pg 1670 for specific descriptions.

Principles of EvaluationPrinciples of Evaluation Tendon injuries: Extensor tendonsTendon injuries: Extensor tendons
Are the most common site of tendon injuries Are the most common site of tendon injuries because of the superficial nature of the because of the superficial nature of the tendons on the dorsum of the hand.tendons on the dorsum of the hand.
A separate zone classification system (I – A separate zone classification system (I – VIII) has been developed for assessing injury VIII) has been developed for assessing injury patterns, repair techniques, and rehabilitation.patterns, repair techniques, and rehabilitation.
Refer to pages 1670 – 1671 for specific Refer to pages 1670 – 1671 for specific description.description.

Ligament and Dislocation injuriesLigament and Dislocation injuries
DIPDIPDislocation at DIP are uncommon because of Dislocation at DIP are uncommon because of
the firm attachments of the skin and subq the firm attachments of the skin and subq tissue to the underlying bone.tissue to the underlying bone.
Dislocations at the DIP are usually dorsal.Dislocations at the DIP are usually dorsal.Reduction can be done by longitudinal Reduction can be done by longitudinal
traction and hyperextension, followed by traction and hyperextension, followed by direct dorsal pressure to the base of the distal direct dorsal pressure to the base of the distal phalanx after a digital block.phalanx after a digital block.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Volar dislocation of DIP joint of little finger.
Dorsal dislocation at the DIP jt without associated fracture

Ligament and Dislocation injuriesLigament and Dislocation injuries
PIP Dislocation:PIP Dislocation:One of the most common ligamentous injuriesOne of the most common ligamentous injuriesMechanism: Mechanism:
Usually due to axial load and hyperextension. Usually due to axial load and hyperextension. Dorsal dislocation occurs when the volar plate Dorsal dislocation occurs when the volar plate
ruptures.ruptures.Lateral dislocation occurs when one of the Lateral dislocation occurs when one of the
collateral ligaments ruptures with at least a partial collateral ligaments ruptures with at least a partial avulsion of the volar plate form the middle phalanx.avulsion of the volar plate form the middle phalanx.
Volar dislocations are rare.Volar dislocations are rare.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Lateral dislocation of middle finger PIP joint.

Ligament and Dislocation injuriesLigament and Dislocation injuries
PIP Dislocation:PIP Dislocation: ReductionReduction
Perform similarly to DIP dorsal dislocationsPerform similarly to DIP dorsal dislocationsActive ROM and strength should be tested after Active ROM and strength should be tested after
reduction.reduction.If testing is normal, then splint in 30-degree flexion If testing is normal, then splint in 30-degree flexion
for 3 wks.for 3 wks.If the joint is irreducible or there is evidence of If the joint is irreducible or there is evidence of
complete ligamentous disruption, operative repair complete ligamentous disruption, operative repair is required.is required.

Ligament and Dislocation injuriesLigament and Dislocation injuries
MP dislocation:MP dislocation:Less common than at the PIP jtLess common than at the PIP jtMechanism:Mechanism:
Usually due to hyperextension forces that rupture Usually due to hyperextension forces that rupture the volar plate causing dorsal dislocation.the volar plate causing dorsal dislocation.
In subluxation (simple dislocation) – the jt appears In subluxation (simple dislocation) – the jt appears to be hyperextended 60 – 90 degrees and the to be hyperextended 60 – 90 degrees and the articular surfaces are still in contact.articular surfaces are still in contact.
Volar dislocation are rare and usually require Volar dislocation are rare and usually require operative reduction.operative reduction.

Ligament and Dislocation injuriesLigament and Dislocation injuries
MP dislocation:MP dislocation:Reduction:Reduction:
Does not involve hyperextension (this might Does not involve hyperextension (this might convert it from a simple to a complex dislocation)convert it from a simple to a complex dislocation)
Performed with the wrist flexed to relaxed the Performed with the wrist flexed to relaxed the flexor tendon and applying pressure over the flexor tendon and applying pressure over the dorsum of the proximal phalanx in a distal and dorsum of the proximal phalanx in a distal and volar direction.volar direction.
Splint the MP jt in flexion after reduction.Splint the MP jt in flexion after reduction.

Ligament and Dislocation injuriesLigament and Dislocation injuries
CMC jt dislocation:CMC jt dislocation:
Are uncommon because the jt is supported by Are uncommon because the jt is supported by strong dorsal, volar, and interosseous strong dorsal, volar, and interosseous ligaments and reinforced by the broad ligaments and reinforced by the broad insertions of the wrist flexions and extensors.insertions of the wrist flexions and extensors.

Ligament and Dislocation injuriesLigament and Dislocation injuries
CMC jt dislocation:CMC jt dislocation: Mechanism:Mechanism:
Usually due to high-speed mechanisms (MVC, Usually due to high-speed mechanisms (MVC, falls, crushes, or clenched fist trauma).falls, crushes, or clenched fist trauma).
Usually occurs via dorsal and with associated Usually occurs via dorsal and with associated fractures.fractures.

Ligament and Dislocation injuriesLigament and Dislocation injuries
CMC jt dislocation:CMC jt dislocation: Reduction:Reduction:
Attempt after regional anesthesia with traction and Attempt after regional anesthesia with traction and flexion with simultaneous longitudinal pressure on flexion with simultaneous longitudinal pressure on the metacarpal base.the metacarpal base.
Pt need early referral after reduction to determine Pt need early referral after reduction to determine if further fixation is needed.if further fixation is needed.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb IP dislocationThumb IP dislocationAre rare but, if present, usually open.Are rare but, if present, usually open.Mechanism:Mechanism:
Usually hyperextension with rupture of the volar Usually hyperextension with rupture of the volar plate.plate.
Reduction:Reduction:Similar to the IP jt of the other digitsSimilar to the IP jt of the other digitsImmobilized for 3wks in mild flexion.Immobilized for 3wks in mild flexion.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb MP dislocation:Thumb MP dislocation:
Usually dorsalUsually dorsal
Can be simple (subluxation) or complexCan be simple (subluxation) or complex
Mechanism:Mechanism:Hyperextension force causing rupture of the volar Hyperextension force causing rupture of the volar
plate.plate.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb MP dislocation:Thumb MP dislocation:Reduction:Reduction:
After a radial nerve block.After a radial nerve block.
Performed with pressure directed distally on the Performed with pressure directed distally on the base of the proximal phalanx with the metacarpal base of the proximal phalanx with the metacarpal flexed and abducted.flexed and abducted.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb MP Collateral Ligament Rupture:Thumb MP Collateral Ligament Rupture:Rupture of the ulnar collateral ligament Rupture of the ulnar collateral ligament
(gamekeeper’s thumb, skier’s thumb) (gamekeeper’s thumb, skier’s thumb) Occurs when the mechanism causes radial Occurs when the mechanism causes radial
deviation (abduction) of the MP jt.deviation (abduction) of the MP jt.
Tear usually occur at the insertion into the Tear usually occur at the insertion into the proximal phalanx.proximal phalanx.
Significant injury occurs to the dorsal capsule and Significant injury occurs to the dorsal capsule and volar plate.volar plate.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb MP Collateral Ligament Rupture:Thumb MP Collateral Ligament Rupture:Rupture of the ulnar collateral ligament Rupture of the ulnar collateral ligament
(gamekeeper’s thumb, skier’s thumb) (gamekeeper’s thumb, skier’s thumb)
Type 1 Avulsion fracture, nondisplaced Type 1 Avulsion fracture, nondisplaced Type 2 Avulsion fracture, displaced Type 2 Avulsion fracture, displaced Type 3 Torn ligament, stable in flexion Type 3 Torn ligament, stable in flexion Type 4 Torn ligament, unstable in flexion Type 4 Torn ligament, unstable in flexion

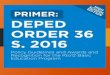
Ligament and Dislocation injuriesLigament and Dislocation injuries
Gamekeeper's thumb. Gamekeeper's thumb. (1.) The normal thumb (1.) The normal thumb MCP jt ulnar collateral MCP jt ulnar collateral ligament. (2.)Tear in the ligament. (2.)Tear in the extensor mechanism extensor mechanism overlying the disrupted overlying the disrupted ligament acts as a ligament acts as a buttonhole and (3.) traps buttonhole and (3.) traps the ligament end. In this the ligament end. In this position, spontaneous position, spontaneous healing and recovery of healing and recovery of stability is prevented. stability is prevented.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb MP Collateral Ligament Rupture:Thumb MP Collateral Ligament Rupture:
Rupture of the ulnar collateral ligamentRupture of the ulnar collateral ligamentHand surgery referral is recommended for all Hand surgery referral is recommended for all
patients with weakness of pincer function and patients with weakness of pincer function and point tenderness at the volar – ulnar aspect of point tenderness at the volar – ulnar aspect of the thumb MCP jtthe thumb MCP jt resulting from a forced resulting from a forced abduction mechanism of injury.abduction mechanism of injury.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb MP Collateral Ligament Rupture:Thumb MP Collateral Ligament Rupture:Rupture of the ulnar collateral ligamentRupture of the ulnar collateral ligament
If XRAY negative for fracture, then abduction If XRAY negative for fracture, then abduction stress testing of the ulnar collateral ligament stress testing of the ulnar collateral ligament maybe performed for added information.maybe performed for added information.
Test the thumb MCP both in full extension and 30-Test the thumb MCP both in full extension and 30-degree flexion, by stabilizing the metacarpal with degree flexion, by stabilizing the metacarpal with one hand while applying lateral (radial) stress on one hand while applying lateral (radial) stress on the proximal phalanx with the other.the proximal phalanx with the other.

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb MP Collateral Ligament Rupture:Thumb MP Collateral Ligament Rupture: Rupture of the ulnar collateral ligamentRupture of the ulnar collateral ligament
More than 40 degrees radial angulation indicates More than 40 degrees radial angulation indicates complete rupture and requires surgical complete rupture and requires surgical consultation.consultation.
Repair best accomplished in 1 wk.Repair best accomplished in 1 wk.
Rupture of the radial collateral ligamentRupture of the radial collateral ligament Not as commonNot as common Mechanism is forced adductionMechanism is forced adduction

Ligament and Dislocation injuriesLigament and Dislocation injuries
Thumb CMC:Thumb CMC: Isolated dislocation is rare compared to the Isolated dislocation is rare compared to the
more common Bennett fracture dislocation.more common Bennett fracture dislocation. Easy to reduce but unstable after reduction.Easy to reduce but unstable after reduction. Apply thumb spica splint after reduction.Apply thumb spica splint after reduction. Need surgical referral.Need surgical referral.

ROM of the ThumbROM of the Thumb

FracturesFractures
Distal Phalanx:Distal Phalanx: Account for 15 – 30 present of all hand Account for 15 – 30 present of all hand
fractures.fractures. Are usually from crush or shearing forces.Are usually from crush or shearing forces. Can be classified as tuft, shaft, or Can be classified as tuft, shaft, or
intraarticular.intraarticular. Tuft fractures – can be associated with nail Tuft fractures – can be associated with nail
bed lacerationsbed lacerations

FracturesFractures
Distal Phalanx:Distal Phalanx: Fractures at the base Fractures at the base
may be associated may be associated with flexor or extensor with flexor or extensor tendon involvement.tendon involvement.
These fractures are These fractures are treated as soft tissue treated as soft tissue injuries with protective injuries with protective splinting.splinting.

FracturesFractures
Proximal and Middle PhalanxProximal and Middle Phalanx Proximal phalanxProximal phalanx
Has no tendinous attachmentsHas no tendinous attachments Fractures frequently have volar angulation from the Fractures frequently have volar angulation from the
forces of the extensor and interosseous muscles.forces of the extensor and interosseous muscles.

FracturesFractures
Proximal and Middle PhalanxProximal and Middle Phalanx Middle Phalanx:Middle Phalanx:
Has the FDS insert on the entire volar surface and Has the FDS insert on the entire volar surface and the extensor tendon insert at the proximal basethe extensor tendon insert at the proximal base
Fractures at the base have dorsal angulation and Fractures at the base have dorsal angulation and fractures at the neck result in volar angulation.fractures at the neck result in volar angulation.
Most often these fractures are stable and Most often these fractures are stable and nondisplaced.nondisplaced.
Can be treated with early protected motion by Can be treated with early protected motion by buddy taping.buddy taping.

FracturesFractures
Proximal and Middle PhalanxProximal and Middle Phalanx Unstable fractures amenable to closed Unstable fractures amenable to closed
reduction can be splinted from the elbow to reduction can be splinted from the elbow to the DIP with the wrist at 20-degree extension the DIP with the wrist at 20-degree extension and the MP jt in 90-degree flexion.and the MP jt in 90-degree flexion.
Midshaft transverse fractures, spiral fractures Midshaft transverse fractures, spiral fractures and intraarticular fractures often require and intraarticular fractures often require internal fixation.internal fixation.

FracturesFractures
Metacarpal (II to V) FracturesMetacarpal (II to V) Fractures 22ndnd and 3 and 3rdrd metacarpals are relatively immobile metacarpals are relatively immobile
and fractures require anatomic reduction.and fractures require anatomic reduction. 44thth and 5 and 5thth MC have 15 to 20-degree AP MC have 15 to 20-degree AP
motion, which allows for some compensation.motion, which allows for some compensation. MC fractures are categorized as head, neck, MC fractures are categorized as head, neck,
shaft, or base fractures.shaft, or base fractures.

FracturesFractures
Metacarpal (II to V) FracturesMetacarpal (II to V) Fractures Head:Head:
Usually caused by a direct blow, crush or missile.Usually caused by a direct blow, crush or missile. Fractures are distal to the insertion of the collateral Fractures are distal to the insertion of the collateral
ligaments and are often comminuted.ligaments and are often comminuted. If a laceration is present a human bite must be If a laceration is present a human bite must be
considered.considered. Treatment:Treatment:
Ice, elevation, immobilization, and referral to a hand Ice, elevation, immobilization, and referral to a hand surgeon.surgeon.

FracturesFractures
Metacarpal (II to V) FracturesMetacarpal (II to V) Fractures Neck:Neck:
Usually caused by a directed impaction force.Usually caused by a directed impaction force. Fracture of the fifth MC neck is often referred to as Fracture of the fifth MC neck is often referred to as
a boxer’s fracturea boxer’s fracture Fracture are usually unstable with volar angulation.Fracture are usually unstable with volar angulation. Angulation of < 20 degrees in the 4Angulation of < 20 degrees in the 4thth and 40 and 40
degrees in the 5degrees in the 5thth MC will not result in functional MC will not result in functional impairmentimpairment

FracturesFractures
Metacarpal (II to V) FracturesMetacarpal (II to V) Fractures Neck:Neck:
If greater angulation in these MC occur, reduction If greater angulation in these MC occur, reduction should be attemptedshould be attempted
Fractures should be splinted with the wrist in 20-Fractures should be splinted with the wrist in 20-degree extension and the MP flexed at 90 degree extension and the MP flexed at 90 degrees.degrees.
In the 2In the 2ndnd and 3 and 3rdrd MC, angulation of <15 degrees is MC, angulation of <15 degrees is acceptable. If significantly displaced or angulated acceptable. If significantly displaced or angulated then anatomic reduction and surgical fixation is then anatomic reduction and surgical fixation is neededneeded

FracturesFractures
Metacarpal (II to V) FracturesMetacarpal (II to V) Fractures Shaft:Shaft:
Usually occur via a direct blowUsually occur via a direct blow Rotational deformity and shortening are more often Rotational deformity and shortening are more often
in shaft fractures than in neck fractures.in shaft fractures than in neck fractures. If reduction is needed, than operative fixation is If reduction is needed, than operative fixation is
usually indicated.usually indicated.

FracturesFractures
Metacarpal (II to V) FracturesMetacarpal (II to V) Fractures BaseBase
Usually caused by a direct blow or axial force.Usually caused by a direct blow or axial force. They are often associated with carpal bone They are often associated with carpal bone
fractures.fractures. Fractures at the base of the 4Fractures at the base of the 4thth and 5 and 5thth MC can MC can
result in paralysis of the motor branch of the ulnar result in paralysis of the motor branch of the ulnar nerve.nerve.

FracturesFractures
Thumb MCThumb MC Because of the mobility of the thumb MC, Because of the mobility of the thumb MC,
shaft fractures are uncommonshaft fractures are uncommon Fractures usually involve the base.Fractures usually involve the base. Two type:Two type:
ExtraarticularExtraarticular Intraarticular Intraarticular

FracturesFractures
Thumb MCThumb MC Extraarticular:Extraarticular:
Are caused by a direct blow or impaction Are caused by a direct blow or impaction mechanism.mechanism.
Mobility of the CMC jt can allow for 20-degree Mobility of the CMC jt can allow for 20-degree angular deformity. Angulation greater than this angular deformity. Angulation greater than this requires reduction and thumb spica splint for 4 requires reduction and thumb spica splint for 4 wks.wks.
Spiral fractures often require fixation.Spiral fractures often require fixation.

FracturesFractures
Thumb MCThumb MC IntraarticularIntraarticular
Caused by impaction from striking a fixed object Caused by impaction from striking a fixed object (two type)(two type)
Bennett fx Bennett fx Is an intraarticular fx with associated subluxation or Is an intraarticular fx with associated subluxation or
dislocation at the CMC jt.dislocation at the CMC jt. The ulnar portion of the MC usually remains in place.The ulnar portion of the MC usually remains in place. The distal portion usually subluxes radially and dorsally The distal portion usually subluxes radially and dorsally
from the pull of abduction pollicis longus and the from the pull of abduction pollicis longus and the adductor pollicisadductor pollicis
Treatment – thumb spica and referralTreatment – thumb spica and referral

FracturesFractures
Bennett's fracture Bennett's fracture Avulsion fracture of Avulsion fracture of
the articular surface the articular surface of the first of the first metacarpal with metacarpal with subluxation at the subluxation at the CMC jt. CMC jt.

FracturesFractures
Thumb MCThumb MC IntraarticularIntraarticular
Rolando fractureRolando fracture An intraarticular comminuted fracture at the base of the An intraarticular comminuted fracture at the base of the
metacarpal.metacarpal. Mechanism of injury is similar to the Bennett fracture, but Mechanism of injury is similar to the Bennett fracture, but
less common.less common. Treatment – thumb spica splint and surgery consultation.Treatment – thumb spica splint and surgery consultation.

COMPARTMENT SYNDROMECOMPARTMENT SYNDROME
May occur in crush injury of the hand with May occur in crush injury of the hand with or without associated fracture.or without associated fracture.
Involved compartments of the hand Involved compartments of the hand includes:includes: ThenarThenar HypothenarHypothenar Adductor pollicisAdductor pollicis Four interosseiFour interossei

COMPARTMENT SYNDROMECOMPARTMENT SYNDROME
Cross section Cross section through the palm through the palm showing showing compartments of compartments of the handthe hand

COMPARTMENT SYNDROMECOMPARTMENT SYNDROME
Edema of tissues or hemorrhage within Edema of tissues or hemorrhage within any of these compartments may lead to any of these compartments may lead to elevated pressures that result in tissue elevated pressures that result in tissue necrosis and subsequent loss of hand necrosis and subsequent loss of hand function due to contracture.function due to contracture.
Sign and symptoms:Sign and symptoms: Pain and paresthesias occur earlyPain and paresthesias occur early Paralysis and pulselessness occurring laterParalysis and pulselessness occurring later

COMPARTMENT SYNDROMECOMPARTMENT SYNDROME
Sign and symptoms:Sign and symptoms: Pain Pain
Most consistent clinical signMost consistent clinical sign usually described as deep, constant, poorly usually described as deep, constant, poorly
localized and disproportionate to clinical findings.localized and disproportionate to clinical findings.
PE findings:PE findings: ““intrinsic minus” position at rest (MCP intrinsic minus” position at rest (MCP
extended with PIP slightly flexed)extended with PIP slightly flexed) Pain with passive stretch of the involved Pain with passive stretch of the involved
compartmental musclecompartmental muscle

COMPARTMENT SYNDROMECOMPARTMENT SYNDROME
PE findings:PE findings: Pain with passive stretch of the involved Pain with passive stretch of the involved
compartmental musclecompartmental muscle Interosseous: performed with MCP extended and Interosseous: performed with MCP extended and
PIP fully flexed with slight radial ulnar deviationPIP fully flexed with slight radial ulnar deviation Thenar / Hypothenar: performed by extension of Thenar / Hypothenar: performed by extension of
MCPMCP
Tense swelling of the affected compartmentTense swelling of the affected compartment

COMPARTMENT SYNDROMECOMPARTMENT SYNDROME
DiagnosisDiagnosis Confirmed by compartment pressure Confirmed by compartment pressure
measurement – high rate of false readings.measurement – high rate of false readings. In the setting of severe crush injury with signs In the setting of severe crush injury with signs
and symptoms suggestive of compartment and symptoms suggestive of compartment syndrome, emergent hand surgeon syndrome, emergent hand surgeon consultation for fasciotomy is mandatory.consultation for fasciotomy is mandatory.

High – Pressure Injection InjuryHigh – Pressure Injection Injury
The initial dissipation of kinetic energy The initial dissipation of kinetic energy through the soft tissue of the hand through the soft tissue of the hand produce tissue edema and resultant produce tissue edema and resultant ischemia of the tissue.ischemia of the tissue.
Most common injected substances include Most common injected substances include grease, paint, hydraulic fluid, diesel fuel, grease, paint, hydraulic fluid, diesel fuel, paint thinner, and water.paint thinner, and water.

High – Pressure Injection InjuryHigh – Pressure Injection Injury
Definitive treatment of high – pressure injection Definitive treatment of high – pressure injection injuries is early surgical decompression and injuries is early surgical decompression and debridement of injected areas.debridement of injected areas.
These must be recognized as surgical These must be recognized as surgical emergency and obtain immediate hand surgery emergency and obtain immediate hand surgery consultation, immobilize and elevate the affected consultation, immobilize and elevate the affected hand, initiate tetanus prophylaxis, broad-hand, initiate tetanus prophylaxis, broad-spectrum antibiotics and provide adequate spectrum antibiotics and provide adequate analgesia.analgesia.