-
8/3/2019 Injuries of Wrist and Hand
1/34
Injuries of Wristand Hand
-
8/3/2019 Injuries of Wrist and Hand
2/34
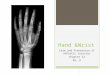
Some anatomiclandmarks on a wrist
and hand
-
8/3/2019 Injuries of Wrist and Hand
3/34
SCAPHOID FRACTURES
Mechanism of trauma is direct and indirect
fall onto outstretched handor direct blow on palm
punch or fallonto clinched fist
-
8/3/2019 Injuries of Wrist and Hand
4/34
Direct mechanism of trauma
-
8/3/2019 Injuries of Wrist and Hand
5/34
CLASSIFICATION
(Herbert)
-
8/3/2019 Injuries of Wrist and Hand
6/34
Variants of fracturesof a navicular bone
1, 2 splinters atfracture;
3 fracture of
tubercle of navicularbone
-
8/3/2019 Injuries of Wrist and Hand
7/34
-
8/3/2019 Injuries of Wrist and Hand
8/34
Clinical presentation
slight edema and palpatory tenderness inregion of radiocarpal
articulation (especially in
region of anatomic snuffbox) axial load along I and II fingers
is painful
movements in a joint are painful and limited,
especially in dorsal and radial direction weakness of a catch of
objects by the hand
impossibility of complete compression hand to
fist
-
8/3/2019 Injuries of Wrist and Hand
9/34
-
8/3/2019 Injuries of Wrist and Hand
10/34
The wrist positioning toradiography in lateral projection
1 -
2 -
5 -
9 -
navicular bone
lunate bone
trapezium bone
1 metacarpal bone
-
8/3/2019 Injuries of Wrist and Hand
11/34
The wrist positioning toradiography in slantingulnar dorsal
projection
1 -
2 -
3 -
4 -
7 -
8 -
9 -
10 -
navicular bone
lunate bone
triangular bone
pisiform bone
capitate bone
hamate bone
1 metacarpal bone
5 metacarpal bone
-
8/3/2019 Injuries of Wrist and Hand
12/34
The wrist positioning toradiography in slantingulnar palmar
projection
1 -
2 -
3 -
4 -
5 -
6 -
7 -
8 -
9 -
10 -
navicular bone
lunate bone
triangular bone
pisiform bone
trapezium bone
trapezoid bone
capitate bone
hamate bone
1 metacarpal bone
5 metacarpal bone
-
8/3/2019 Injuries of Wrist and Hand
13/34
X-ray
fracture of the navicular bone in middle part(direct and three
fourth projections)
-
8/3/2019 Injuries of Wrist and Hand
14/34
SCAPHOID FRACTURES
Non-union and AVN
-
8/3/2019 Injuries of Wrist and Hand
15/34
Treatment of a navicular fractures
without displacement of splinters
fracture of tubercle of a navicular bone:immobilization 4 6
weeks
fracture of body and distal one-third of anavicular bone:
immobilization 10 12 weeks
The hand is in position ofslight flexion and radial
deviation. The first fingeris fixated in position of
moderate abduction.
-
8/3/2019 Injuries of Wrist and Hand
16/34
Complications, such as a delayed union, a falsejoint or aseptic
necrosis, may be even at
absent of a displacement of splinters and at
sufficient immobilization. It depends on adegree of blood supply
disturbance ofa navicular.
Complications
Variants of circulation at
fractures of a navicular bone
-
8/3/2019 Injuries of Wrist and Hand
17/34
Indications to operativetreatment
fractures of a navicular bone withconsiderable displacement
a delayed union
a false joint
aseptic necrosis
-
8/3/2019 Injuries of Wrist and Hand
18/34
The methods ofosteosynthesis
Autologous bone grafting bya bone nail
Osteosynthesisby wires
-
8/3/2019 Injuries of Wrist and Hand
19/34
Postoperative treatment
Immobilization of a hand in medium-physiological position during
6 8
weeks exercise therapy
physiotherapy
-
8/3/2019 Injuries of Wrist and Hand
20/34
SEQUELAE OF SCAPHOIDFRACTURES
1. Delayed union
2. Non-union
3. Avascular necrosis
4. Scaphoid Non-union Advanced
Collapse (SNAC)
demigauntlet bandage
-
8/3/2019 Injuries of Wrist and Hand
21/34
-
8/3/2019 Injuries of Wrist and Hand
22/34
The kinds ofperilunate
dislocations in dorsal-palmar direction
1 - perilunar dislocation
2 - transscaphoperilunate d.
3 - transscaphoid-transtriquetral dislocation
4 - periscaphoperilunate d.
5 - transtriquetralperilunate d
6 - peritriquetralperilunate dislocation
7 - transscaphoid-transcapitate-perilunate d.
8 - transcapitate-perilunate dislocation
-
8/3/2019 Injuries of Wrist and Hand
23/34
Perilunate dislocations anddislocations of a lunate bone
- perilunate dislocation, - perilunate dislocation
withsubluxation of a lunate bone. Dislocations of lunate bone: - I,
- II, - III degree (enucleation of a lunate bone)
-
8/3/2019 Injuries of Wrist and Hand
24/34
-
8/3/2019 Injuries of Wrist and Hand
25/34
-
8/3/2019 Injuries of Wrist and Hand
26/34
The mechanism of a rupture of the metacarpophalangealjoints
ligaments at skiers, cyclists, motorcyclists and the like
outstretched
-
8/3/2019 Injuries of Wrist and Hand
27/34
Fractures of 1 metacarpalbone
Mechanism of trauma
direct
indirect
-
8/3/2019 Injuries of Wrist and Hand
28/34
Kinds of fractures of the firstmetacarpal bone
a. Benets fracture,b. Rolands fracture,
c. transverse
fracture of a shaft,d. oblique fracture of
a shaft.
a. b.
c. d.
-
8/3/2019 Injuries of Wrist and Hand
29/34
Flexible Thumb Splint
-
8/3/2019 Injuries of Wrist and Hand
30/34
Fracture of a shaft of a
metacarpal bone, as a rule,
is result of a directmechanism of a trauma.
The fracture is astable with
volar angular displacementbecause of prevalence of a
tonus of palmar
interosseous muscles.
-
8/3/2019 Injuries of Wrist and Hand
31/34
Usually fractures of a neck of a
metacarpal bone are instable as
they have small splinters of acortical bone on volar
surface.
Here, as a rule, it is established
indications to a little invasive
osteosynthesis.
So-called 90 90 themethod of reduction
allows reducing and
holding splinters, but it
cannot be used as the
method of fixation
Splintered fractures of heads of metacarpal
-
8/3/2019 Injuries of Wrist and Hand
32/34
Splintered fractures of heads of metacarpalbones are a subject
to open anatomical reduction
and little invasive osteosynthesis by wires
B i h d f i i i i
-
8/3/2019 Injuries of Wrist and Hand
33/34
Basic methods of minimum invasiveosteosynthesis after closed
reduction
Minimuminvasive
osteosynthesis is
an atraumatic
technique of afixation with the
purpose of
preservation of
thevascularization of
bony fragments
The lose reduction is one of the principles of an
osteosynthesis
-
8/3/2019 Injuries of Wrist and Hand
34/34