Embed Size (px)
Citation preview

ARTICLESPUBLISHED ONLINE: 30MARCH 2014 | DOI: 10.1038/NMAT3922
Injectable and bioresponsive hydrogels foron-demand matrix metalloproteinase inhibitionBrendan P. Purcell1, David Lobb2, Manoj B. Charati1, Shauna M. Dorsey1, Ryan J. Wade1,Kia N. Zellars2, Heather Doviak2, Sara Pettaway2, Christina B. Logdon2, James A. Shuman2,Parker D. Freels2, Joseph H. Gorman III3, Robert C. Gorman3, Francis G. Spinale2
and Jason A. Burdick1*
Inhibitors of matrix metalloproteinases (MMPs) have been extensively explored to treat pathologies where excessive MMPactivity contributes to adverse tissue remodelling. Although MMP inhibition remains a relevant therapeutic target, MMPinhibitors have not translated to clinical application owing to the dose-limiting side e�ects following systemic administrationof the drugs. Here, we describe the synthesis of a polysaccharide-based hydrogel that can be locally injected into tissuesand releases a recombinant tissue inhibitor of MMPs (rTIMP-3) in response to MMP activity. Specifically, rTIMP-3 issequestered in the hydrogels through electrostatic interactions and is released as crosslinks are degraded by active MMPs.Targeted delivery of the hydrogel/rTIMP-3 construct to regions of MMP overexpression following a myocardial infarctionsignificantly reduced MMP activity and attenuated adverse left ventricular remodelling in a porcine model of myocardialinfarction. Our findings demonstrate that local, on-demand MMP inhibition is achievable through the use of an injectable andbioresponsive hydrogel.
Excessive extracellular matrix (ECM) proteolysis by MMPs isa hallmark of many human disease states including chronicinflammation, tumour progression and cardiovascular
disease1. MMPs hydrolyse peptide bonds with a high level ofamino-acid specificity, and under normal physiological conditionsMMP activity is precisely controlled—such as through tissueinhibitors of MMPs (TIMPs)—to maintain a low level of structuralprotein, cell receptor, and growth factor turnover. However, underpathophysiological conditions, there is a persistence of MMPactivity that causes maladaptive changes to tissue architecturesand functions, contributing to disease progression2. Towards thedevelopment of therapies to treat this, the design and developmentof molecules that inhibit MMP activity has been a widely exploredarea of research over the past 25 years1,3; however, none hastranslated to clinical application owing to the dose-limiting sideeffects following systemic administration of these pharmacologicalMMP inhibitors4. To limit off-target effects of therapeutics,biomaterials—including injectable and water-swollen polymernetworks or hydrogels—have acted as depots to locally delivertherapeutics through diffusion and degradation mechanisms5–7.Typically, these material systems are engineered to achieve a releaseprofile to adequately dose patients within a therapeutic windowspecific to a disease. However, the absolute magnitude and temporalvariation of MMP activity in patients is highly variable8,9; therefore,one hydrogel formulation and inhibitor dose may not be widelyapplicable across patient populations.
As an alternative to passive delivery, the recent developmentof stimuli-responsive polymers has improved our ability to delivertherapeutics using a trigger, such as light, pH, temperature or the
presence of an enzyme10, including MMPs (refs 11–16). We presenthere the development of an MMP-degradable hydrogel that is bothinjectable and sequesters TIMPs through charge interactions, sothat local MMP activity regulates the release of a recombinantTIMP. This approach has not been previously used; yet, it hasimplications in numerous applications where MMP dysregulationleads to disease progression and where heterogeneity inMMP levelsmakes uniform therapeutic dosing difficult.
One specific area where MMP induction is associated withdisease progression is the adverse left ventricle (LV) remodelling inpatients following a myocardial infarction9,17 (MI). Experimentalmodels involving transgenic deletion of specific MMPs andsystemic administration of pharmacologic MMP inhibitors havedemonstrated that MMPs are important contributors to adverseglobal LV remodelling including LV wall thinning, chamberdilation, and ultimately dysfunction18–21. Although systemicadministration of pharmacologic MMP inhibitors has shownefficacy in attenuating post MI remodelling in pre-clinical animalmodels of MI (refs 20,22), off-target effects have limited theirsuccess in recent clinical trials23,24. Further, recent studies haveshown that MMP elevation is highly localized to ischaemic tissuewithin the MI region following experimental MI in large animalmodels25,26. While MMP levels increased markedly, levels of TIMPsdecreased significantly within the MI region26. With the exceptionof TIMP-1, TIMPs are known to inhibit all of the 25 known MMPs,and studies have identified unique roles and functionalities for eachof the four TIMPs (ref. 27). Regarding TIMP-3, myocardial TIMP-3levels were significantly reduced in contradistinction to elevatedmyocardial MMP levels in patients with end-stage heart failure28
1Department of Bioengineering, University of Pennsylvania, Philadelphia, Pennsylvania 19104, USA, 2Cardiovascular Translational Research Center,University of South Carolina School of Medicine and the WJB Dorn Veteran A�airs Medical Center, Columbia, South Carolina 29208, USA, 3GormanCardiovascular Research Laboratory, Department of Surgery, University of Pennsylvania, Philadelphia, Pennsylvania 19104, USA.*e-mail: [email protected]
NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials 1© 2014 Macmillan Publishers Limited. All rights reserved.

ARTICLES NATUREMATERIALS DOI: 10.1038/NMAT3922
and transgenic TIMP-3 deletion in experimental animal modelscaused adverse LV remodelling and accelerated progression to heartfailure following MI (refs 29–31). Therefore, strategies that localizeTIMP-3 to regions of MMP overexpression and limit spill over intothe systemic circulation could safely target post MI remodelling byrestoring MMP/TIMP imbalance within the MI region.
Hydrogels that form on injection into the myocardium haverecently been developed and applied post MI (refs 32–36). Buildingon these advances, we designed an injectable hydrogel with MMP-degradable crosslinks to encapsulate a recombinant TIMP-3 andrelease the inhibitor in response to elevated MMP expressionwithin the myocardium following MI. One challenge towardsrealizing on-demand TIMP-3 delivery is tominimize passive TIMP-3 release from the hydrogels (that is, in the absence of MMPactivity). TIMP-3 is unique among the TIMPs in that it is foundbound to the ECM of tissues whereas the other three TIMPsare presented as soluble proteins37. Specifically, TIMP-3 binds tosulphated glycosaminoglycans (GAGs) with a high affinity throughan abundance of positively charged lysine and arginine residuesexposed on the protein surface38,39. TIMP-3 binding to the ECMis thought to facilitate local MMP inhibition in tissues, and recentstudies have shown that sulphated polymers enhance TIMP-3binding affinity for specificMMPs (ref. 40). Therefore, we developedinjectable hydrogels with a negatively charged polysaccharidebackbone to mimic native TIMP-3/ECM interactions andminimizepassive diffusion of TIMP-3 from the hydrogels. MMP-cleavablecrosslinks were incorporated to liberate bound TIMP-3 in thepresence of localMMP activity. Further, we utilized conjugation andcrosslinking chemistries to form hydrogels rapidly on injection intothe myocardium that are stable in the absence of MMP activity tofurther prevent the passive release of TIMP-3 from the injectionsite.Wedemonstrate that this TIMP-3 delivery strategy is responsiveto elevated MMP activity post MI, and effectively inhibits MMPactivity within the MI region without raising systemic TIMP-3 levels. Importantly, locally inhibiting MMP activity within themyocardium attenuated post MI remodelling as evidenced throughsignificant improvements in LV geometry and function in a largeanimal model of MI.
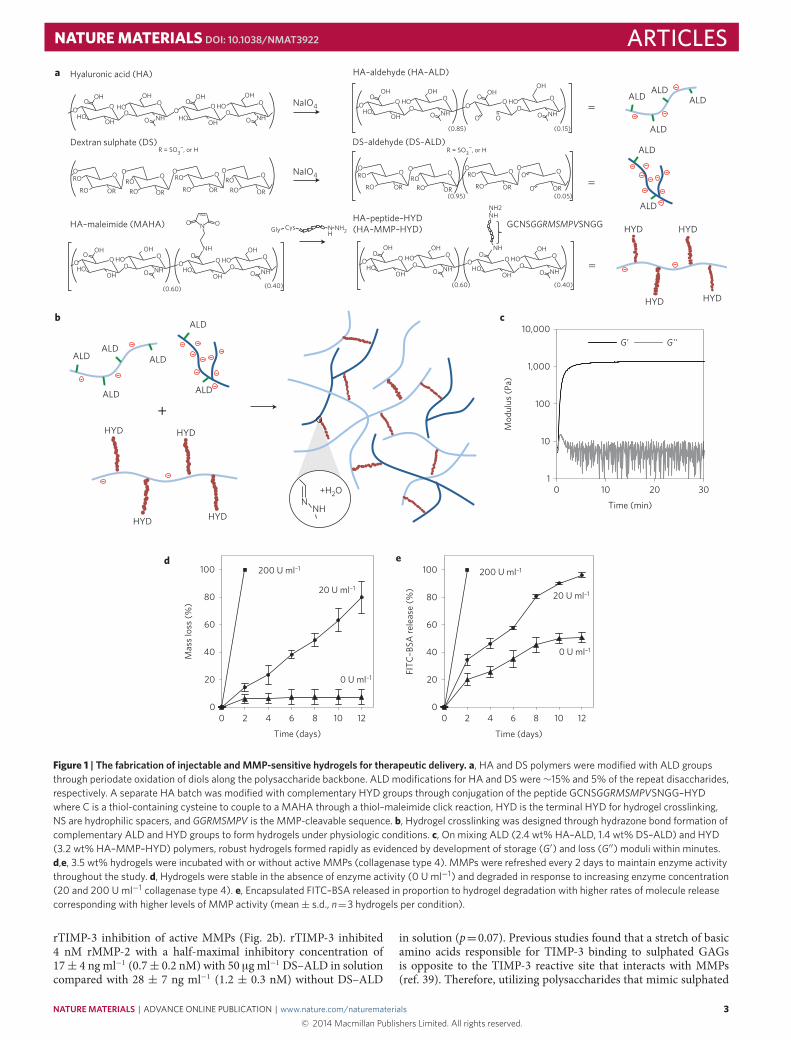
Injectable and bioresponsive hydrogel designThe main criteria used in designing a hydrogel formulation forrTIMP-3 delivery were to form hydrogels following injection ofmacromolecules through a syringe, have the hydrogels degradeonly in the presence of MMPs, and minimize passive releaseof encapsulated rTIMP-3. Towards this goal, we developeda three-macromer system that utilizes the chemical versatilityof polysaccharide backbones (Fig. 1a). Polysaccharides werechemically modified to contain either aldehyde (ALD) or hydrazide(HYD) functional groups to form hydrogels in a one-stepcondensation reaction, with water as the only byproduct (Fig. 1b).Hyaluronic acid (HA)was used as a template for bothALDandHYDmodifications owing to the well-defined size ranges of commerciallyavailable HA, the previous use of HA in biomedical applications,and the abundance of diol and carboxylic acid groups necessary forALD andHYDmodifications, respectively41. Dextran sulphate (DS)was also incorporated into the hydrogels throughALDmodificationof its diol groups to act as a heparin mimetic to immobilizeencapsulated heparin-binding TIMP-3 (ref. 42).
ALD modification of HA and DS was evaluated separately aseach polysaccharide contains a different number of diol groupsamendable to ALD modification (Supplementary Fig. 1). Further,converting diols to ALDs through periodate oxidation is knownto degrade polysaccharides, so a large-molecular-weight HA (∼350kDa) was chosen to provide sufficient HA–ALD molecular weightto allow formation of robust hydrogels for rTIMP-3 encapsulation.Reaction conditions for HA–ALD were chosen to balance ALD
modification and macromer MW as periodate concentration bothincreased ALD modification and decreased HA MW in a dose-dependent manner (Supplementary Fig. 2). Reaction conditions forDS–ALD were chosen to provide sufficient ALD modification tocrosslink DS–ALD into the hydrogel.
MMP sensitivity was incorporated into the hydrogels bygenerating the MMP-cleavable peptide GGRMSMPV with func-tional groups at both ends for chemical conjugations using solid-phase peptide synthesis. The peptide was synthesized with aHYD group at the amino terminus to react with ALD-containingpolymers for hydrogel crosslinking, and a thiol group at thecarboxy terminus through incorporation of a cysteine amino acidto facilitate thioether linkage to a maleimide-functionalized HA(MAHA) in a one-step click reaction (Fig. 1a). Finally, to improvesolubility for passage of the polymer solution through a syringe,hydrophilic serine (S) and asparagine (N) spacers were incorporatedbetween the functional groups and the MMP-cleavable sequence.Successful synthesis of the designed peptide was verified withmass spectroscopy (Supplementary Fig. 3) and peptide couplingto MAHA was verified using 1H NMR spectroscopy, as indicatedby the complete consumption of the characteristic maleimide peak(Supplementary Fig. 4). The thioether coupling chemistry waschosen for its stability in water to prevent nonspecific hydrolysis ofthe hydrogels.
The designed macromers rapidly formed hydrogels on mixingALD- and HYD-modified macromers over a range of macromerweight percentages (1–5 wt%) as evidenced by development of theelastic component (G′) of the complex modulus using rheometry(Supplementary Fig. 5). The time to gelation and the ultimatemodulus decreased and increased, respectively, with an increasein macromer concentrations. At 3.5 wt%, the hydrogels formedsolid gels (G′ >G′′) in less than 1 min and reached a final G′ ofapproximately 1.5 kPa within 10 min, at which point the hydrogelswere robust, nearly elastic solids (Fig. 1c). To demonstrate MMPsensitivity, hydrogels were incubated in buffer with varying concen-trations of active MMPs and uronic acid content in the buffer wasmeasured over time to calculate hydrogel mass loss. In the absenceof active MMPs, the 3.5 wt% hydrogels were stable over the 12-daystudy (Fig. 1d). However, with 20 Uml−1 enzyme concentration, thehydrogels degraded in a near-linear fashion with very little hydrogelremaining after 12 days, and with 200 U ml−1, the hydrogelscompletely degraded in 2 days. In addition to enzyme concentration,hydrogel degradation rate was also controlled by macromerconcentration (Supplementary Fig. 6). Hydrogel degradation ratesscaled inversely with macromer concentration and therefore thenumber of crosslinks in the hydrogel. To evaluate the applicability ofthe hydrogels forMMP-triggered release of encapsulatedmolecules,fluorescein-isothiocyanate-labelled bovine serum albumin (FITC–BSA) was encapsulated in 3.5 wt% hydrogels and release wasquantified in buffer with varying concentrations of active MMPs.Encapsulated FITC–BSA release followed the hydrogel degradationbehaviour in a similar MMP-dependent manner (Fig. 1e).
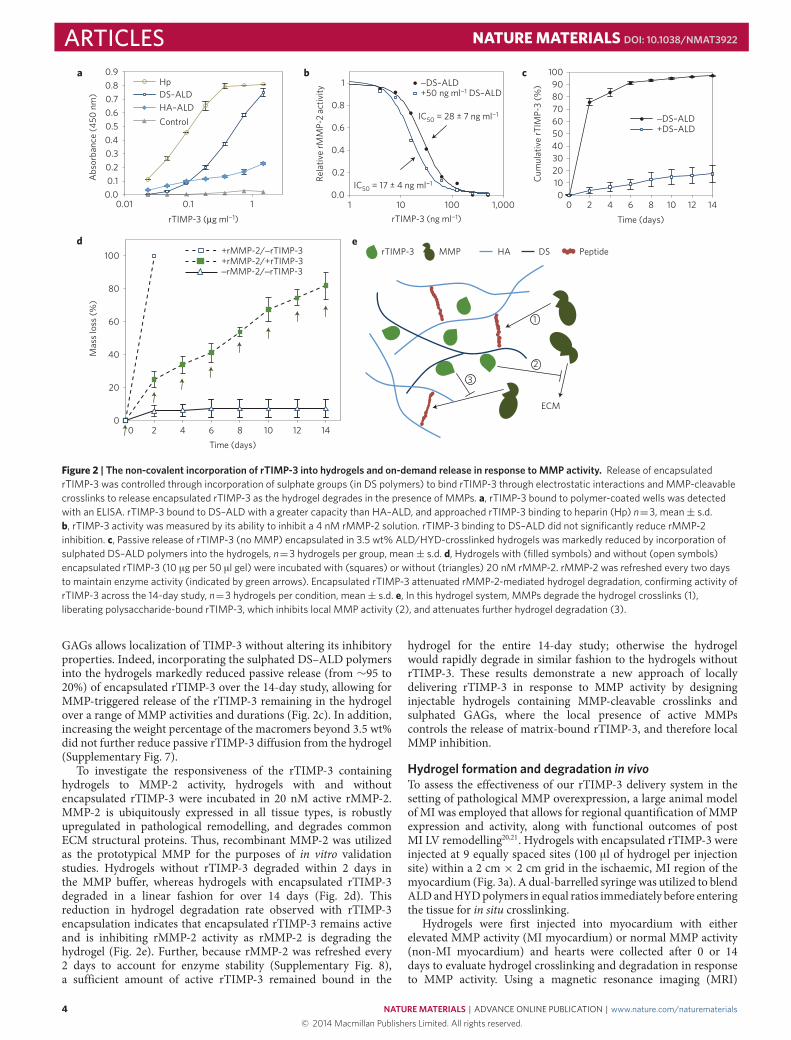
MMP triggered rTIMP-3 releaseTIMP-3 was chosen for local delivery post-MI in part becauseof its unique ECM-binding property. This allowed us to designECM mimetic hydrogels to encapsulate and bind rTIMP-3 untilreleased by MMP-mediated hydrogel degradation. To this end,DS was incorporated into the hydrogel formulation to mimicsulphated GAGs, the main component of the ECM responsible forTIMP-3 binding, owing to its susceptibility to ALD modificationthrough diol oxidation. Binding of rTIMP-3 to DS–ALD wasevaluated using a solid-phase binding assay. rTIMP-3 boundto DS–ALD with a much greater capacity than to HA–ALD,and approached the capacity of rTIMP-3 binding to heparin(Fig. 2a). Importantly, rTIMP-3 binding to DS–ALD did not reduce
2 NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials© 2014 Macmillan Publishers Limited. All rights reserved.
NATUREMATERIALS DOI: 10.1038/NMAT3922 ARTICLES
DS–aldehyde (DS–ALD)
HYD
HYD HYD
HYD
ALD
ALD
ALD
ALD
ALDALD
a
HA–peptide–HYD(HA–MMP–HYD) GCNSGGRMSMPVSNGG
O
OHHO
OO O
NHO
HO
O
OH
(0.60) (0.40)
O
OHHO
O
OHO O
NHOHO
O
OH NH
NHNH2
HA–maleimide (MAHA)
O
OHHO
OO O
NHO
HO
O
OH
(0.60) (0.40)
O
OHHO
O
OHO O
NHOHO
O
OH NH
N OO
OH
HA–aldehyde (HA–ALD)
OO
OHO O
NHO
HO
O
OHO
OO
O
OHO O
NHO
HO
O
OH
(0.85) (0.15)
HOOH
O OO
OR
RO
RO
O
OR
R = SO3−, or H
O OOO
OR
RO
RO O
O
OR(0.95) (0.05)
RORO
R = SO3−, or H
NaIO4O OO
OR
RO
RO
O
OR
O OO
OR
RO
RO
O
ORRORO
RORO
HN NH2CysGly
Hyaluronic acid (HA)
NaIO4OO
OHO O
NHO
HO
O
OHO
O
OHO O
NHO
HO
O
OH
HOOH HO
0
20
40
60
80
100
0 2 4 6 8 10 12
Mas
s lo
ss (%
)
Time (days)
200 U ml–1
20 U ml–1
0 U ml–1
d
0
20
40
60
80
100
0 2 4 6 8 10 12
FITC
–BSA
rele
ase
(%)
Time (days)
200 U ml–1
20 U ml–1
0 U ml–1
e
b
ALD
ALD
ALD
ALD
HYD
HYD HYD
HYD
ALD
ALD
1
10
100
1,000
10,000
0 10 20 30
Mod
ulus
(Pa)
Time (min)
G’ G’’
c
NNH
+H2O
Dextran sulphate (DS)
Figure 1 | The fabrication of injectable and MMP-sensitive hydrogels for therapeutic delivery. a, HA and DS polymers were modified with ALD groupsthrough periodate oxidation of diols along the polysaccharide backbone. ALD modifications for HA and DS were∼15% and 5% of the repeat disaccharides,respectively. A separate HA batch was modified with complementary HYD groups through conjugation of the peptide GCNSGGRMSMPVSNGG–HYDwhere C is a thiol-containing cysteine to couple to a MAHA through a thiol–maleimide click reaction, HYD is the terminal HYD for hydrogel crosslinking,NS are hydrophilic spacers, and GGRMSMPV is the MMP-cleavable sequence. b, Hydrogel crosslinking was designed through hydrazone bond formation ofcomplementary ALD and HYD groups to form hydrogels under physiologic conditions. c, On mixing ALD (2.4 wt% HA–ALD, 1.4 wt% DS–ALD) and HYD(3.2 wt% HA–MMP–HYD) polymers, robust hydrogels formed rapidly as evidenced by development of storage (G′) and loss (G′′) moduli within minutes.d,e, 3.5 wt% hydrogels were incubated with or without active MMPs (collagenase type 4). MMPs were refreshed every 2 days to maintain enzyme activitythroughout the study. d, Hydrogels were stable in the absence of enzyme activity (0 U ml−1) and degraded in response to increasing enzyme concentration(20 and 200 U ml−1 collagenase type 4). e, Encapsulated FITC–BSA released in proportion to hydrogel degradation with higher rates of molecule releasecorresponding with higher levels of MMP activity (mean± s.d., n=3 hydrogels per condition).
rTIMP-3 inhibition of active MMPs (Fig. 2b). rTIMP-3 inhibited4 nM rMMP-2 with a half-maximal inhibitory concentration of17± 4 ng ml−1 (0.7± 0.2 nM) with 50 µg ml−1 DS–ALD in solutioncompared with 28 ± 7 ng ml−1 (1.2 ± 0.3 nM) without DS–ALD
in solution (p=0.07). Previous studies found that a stretch of basicamino acids responsible for TIMP-3 binding to sulphated GAGsis opposite to the TIMP-3 reactive site that interacts with MMPs(ref. 39). Therefore, utilizing polysaccharides that mimic sulphated
NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials 3© 2014 Macmillan Publishers Limited. All rights reserved.
ARTICLES NATUREMATERIALS DOI: 10.1038/NMAT3922
3
2
1
rTIMP-3 MMP HA DS Peptide
ECM
e
0
20
40
60
80
100
0 2 4 6 8 10 12 14
Mas
s lo
ss (%
)
Time (days)
d+rMMP-2/−rTIMP-3+rMMP-2/+rTIMP-3−rMMP-2/−rTIMP-3
0.0
0.2
0.4
0.6
0.8
1
1 10 100 1,000
Rela
tive
rMM
P-2
activ
ity
rTIMP-3 (ng ml−1)
+50 ng ml−1 DS–ALD−DS–ALD
IC50 = 17 ± 4 ng ml−1
IC50 = 28 ± 7 ng ml−1
b c
0102030405060708090
100
0 2 4 6 8 10 12 14
Cum
ulat
ive
rTIM
P-3
(%)
Time (days)
−DS–ALD+DS–ALD
0.00.10.20.30.40.50.60.70.80.9
0.01 0.1 1
Abs
orba
nce
(450
nm
)
rTIMP-3 (µg ml−1)
HpDS–ALDHA–ALDControl
a
Figure 2 | The non-covalent incorporation of rTIMP-3 into hydrogels and on-demand release in response to MMP activity. Release of encapsulatedrTIMP-3 was controlled through incorporation of sulphate groups (in DS polymers) to bind rTIMP-3 through electrostatic interactions and MMP-cleavablecrosslinks to release encapsulated rTIMP-3 as the hydrogel degrades in the presence of MMPs. a, rTIMP-3 bound to polymer-coated wells was detectedwith an ELISA. rTIMP-3 bound to DS–ALD with a greater capacity than HA–ALD, and approached rTIMP-3 binding to heparin (Hp) n=3, mean± s.d.b, rTIMP-3 activity was measured by its ability to inhibit a 4 nM rMMP-2 solution. rTIMP-3 binding to DS–ALD did not significantly reduce rMMP-2inhibition. c, Passive release of rTIMP-3 (no MMP) encapsulated in 3.5 wt% ALD/HYD-crosslinked hydrogels was markedly reduced by incorporation ofsulphated DS–ALD polymers into the hydrogels, n=3 hydrogels per group, mean± s.d. d, Hydrogels with (filled symbols) and without (open symbols)encapsulated rTIMP-3 (10 µg per 50 µl gel) were incubated with (squares) or without (triangles) 20 nM rMMP-2. rMMP-2 was refreshed every two daysto maintain enzyme activity (indicated by green arrows). Encapsulated rTIMP-3 attenuated rMMP-2-mediated hydrogel degradation, confirming activity ofrTIMP-3 across the 14-day study, n=3 hydrogels per condition, mean± s.d. e, In this hydrogel system, MMPs degrade the hydrogel crosslinks (1),liberating polysaccharide-bound rTIMP-3, which inhibits local MMP activity (2), and attenuates further hydrogel degradation (3).
GAGs allows localization of TIMP-3 without altering its inhibitoryproperties. Indeed, incorporating the sulphated DS–ALD polymersinto the hydrogels markedly reduced passive release (from ∼95 to20%) of encapsulated rTIMP-3 over the 14-day study, allowing forMMP-triggered release of the rTIMP-3 remaining in the hydrogelover a range of MMP activities and durations (Fig. 2c). In addition,increasing the weight percentage of the macromers beyond 3.5 wt%did not further reduce passive rTIMP-3 diffusion from the hydrogel(Supplementary Fig. 7).
To investigate the responsiveness of the rTIMP-3 containinghydrogels to MMP-2 activity, hydrogels with and withoutencapsulated rTIMP-3 were incubated in 20 nM active rMMP-2.MMP-2 is ubiquitously expressed in all tissue types, is robustlyupregulated in pathological remodelling, and degrades commonECM structural proteins. Thus, recombinant MMP-2 was utilizedas the prototypical MMP for the purposes of in vitro validationstudies. Hydrogels without rTIMP-3 degraded within 2 days inthe MMP buffer, whereas hydrogels with encapsulated rTIMP-3degraded in a linear fashion for over 14 days (Fig. 2d). Thisreduction in hydrogel degradation rate observed with rTIMP-3encapsulation indicates that encapsulated rTIMP-3 remains activeand is inhibiting rMMP-2 activity as rMMP-2 is degrading thehydrogel (Fig. 2e). Further, because rMMP-2 was refreshed every2 days to account for enzyme stability (Supplementary Fig. 8),a sufficient amount of active rTIMP-3 remained bound in the
hydrogel for the entire 14-day study; otherwise the hydrogelwould rapidly degrade in similar fashion to the hydrogels withoutrTIMP-3. These results demonstrate a new approach of locallydelivering rTIMP-3 in response to MMP activity by designinginjectable hydrogels containing MMP-cleavable crosslinks andsulphated GAGs, where the local presence of active MMPscontrols the release of matrix-bound rTIMP-3, and therefore localMMP inhibition.
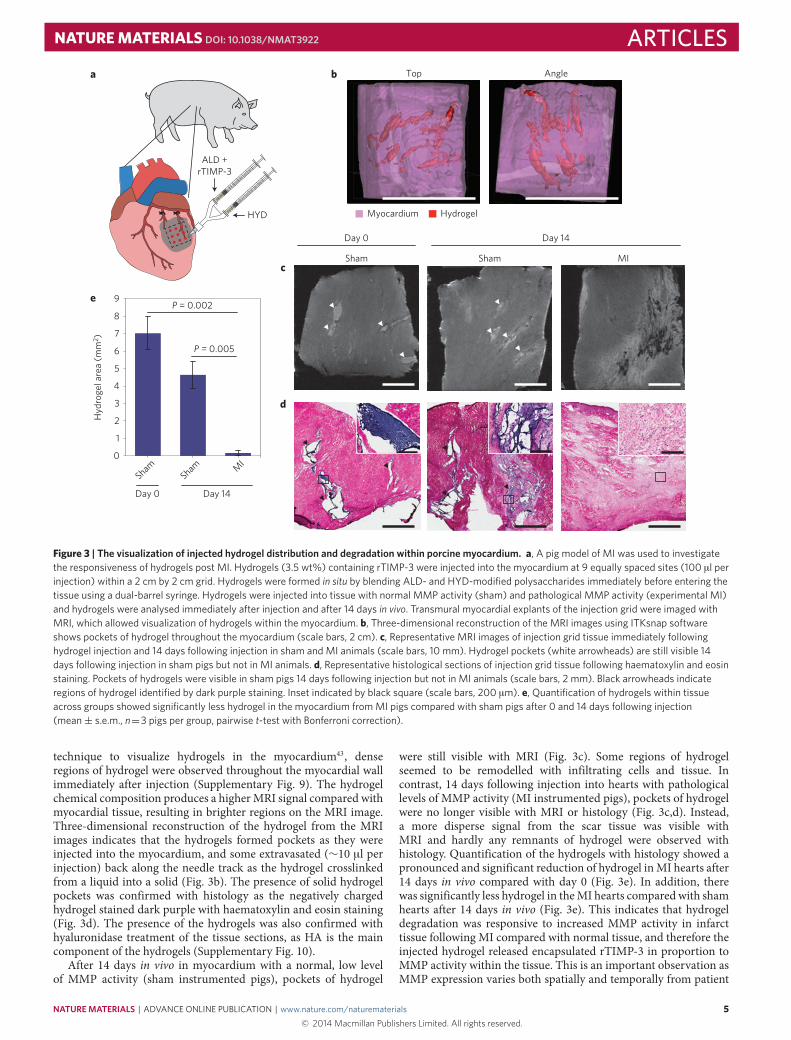
Hydrogel formation and degradation in vivoTo assess the effectiveness of our rTIMP-3 delivery system in thesetting of pathological MMP overexpression, a large animal modelof MI was employed that allows for regional quantification of MMPexpression and activity, along with functional outcomes of postMI LV remodelling20,21. Hydrogels with encapsulated rTIMP-3 wereinjected at 9 equally spaced sites (100 µl of hydrogel per injectionsite) within a 2 cm × 2 cm grid in the ischaemic, MI region of themyocardium (Fig. 3a). A dual-barrelled syringewas utilized to blendALDandHYDpolymers in equal ratios immediately before enteringthe tissue for in situ crosslinking.
Hydrogels were first injected into myocardium with eitherelevated MMP activity (MI myocardium) or normal MMP activity(non-MI myocardium) and hearts were collected after 0 or 14days to evaluate hydrogel crosslinking and degradation in responseto MMP activity. Using a magnetic resonance imaging (MRI)
4 NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials© 2014 Macmillan Publishers Limited. All rights reserved.
NATUREMATERIALS DOI: 10.1038/NMAT3922 ARTICLESb Top Angle
Myocardium Hydrogel
Day 0 Day 14
Sham Sham MIc
d
0
1
2
3
4
5
Hyd
roge
l are
a (m
m2 )
6
7
8
9e
Day 0 Day 14
P = 0.005
P = 0.002
ShamSham M
I
ALD +rTIMP-3
HYD
a
Figure 3 | The visualization of injected hydrogel distribution and degradation within porcine myocardium. a, A pig model of MI was used to investigatethe responsiveness of hydrogels post MI. Hydrogels (3.5 wt%) containing rTIMP-3 were injected into the myocardium at 9 equally spaced sites (100 µl perinjection) within a 2 cm by 2 cm grid. Hydrogels were formed in situ by blending ALD- and HYD-modified polysaccharides immediately before entering thetissue using a dual-barrel syringe. Hydrogels were injected into tissue with normal MMP activity (sham) and pathological MMP activity (experimental MI)and hydrogels were analysed immediately after injection and after 14 days in vivo. Transmural myocardial explants of the injection grid were imaged withMRI, which allowed visualization of hydrogels within the myocardium. b, Three-dimensional reconstruction of the MRI images using ITKsnap softwareshows pockets of hydrogel throughout the myocardium (scale bars, 2 cm). c, Representative MRI images of injection grid tissue immediately followinghydrogel injection and 14 days following injection in sham and MI animals (scale bars, 10 mm). Hydrogel pockets (white arrowheads) are still visible 14days following injection in sham pigs but not in MI animals. d, Representative histological sections of injection grid tissue following haematoxylin and eosinstaining. Pockets of hydrogels were visible in sham pigs 14 days following injection but not in MI animals (scale bars, 2 mm). Black arrowheads indicateregions of hydrogel identified by dark purple staining. Inset indicated by black square (scale bars, 200 µm). e, Quantification of hydrogels within tissueacross groups showed significantly less hydrogel in the myocardium from MI pigs compared with sham pigs after 0 and 14 days following injection(mean± s.e.m., n=3 pigs per group, pairwise t-test with Bonferroni correction).
technique to visualize hydrogels in the myocardium43, denseregions of hydrogel were observed throughout the myocardial wallimmediately after injection (Supplementary Fig. 9). The hydrogelchemical composition produces a higherMRI signal compared withmyocardial tissue, resulting in brighter regions on the MRI image.Three-dimensional reconstruction of the hydrogel from the MRIimages indicates that the hydrogels formed pockets as they wereinjected into the myocardium, and some extravasated (∼10 µl perinjection) back along the needle track as the hydrogel crosslinkedfrom a liquid into a solid (Fig. 3b). The presence of solid hydrogelpockets was confirmed with histology as the negatively chargedhydrogel stained dark purple with haematoxylin and eosin staining(Fig. 3d). The presence of the hydrogels was also confirmed withhyaluronidase treatment of the tissue sections, as HA is the maincomponent of the hydrogels (Supplementary Fig. 10).
After 14 days in vivo in myocardium with a normal, low levelof MMP activity (sham instrumented pigs), pockets of hydrogel
were still visible with MRI (Fig. 3c). Some regions of hydrogelseemed to be remodelled with infiltrating cells and tissue. Incontrast, 14 days following injection into hearts with pathologicallevels of MMP activity (MI instrumented pigs), pockets of hydrogelwere no longer visible with MRI or histology (Fig. 3c,d). Instead,a more disperse signal from the scar tissue was visible withMRI and hardly any remnants of hydrogel were observed withhistology. Quantification of the hydrogels with histology showed apronounced and significant reduction of hydrogel inMI hearts after14 days in vivo compared with day 0 (Fig. 3e). In addition, therewas significantly less hydrogel in theMI hearts compared with shamhearts after 14 days in vivo (Fig. 3e). This indicates that hydrogeldegradation was responsive to increased MMP activity in infarcttissue following MI compared with normal tissue, and therefore theinjected hydrogel released encapsulated rTIMP-3 in proportion toMMP activity within the tissue. This is an important observation asMMP expression varies both spatially and temporally from patient
NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials 5© 2014 Macmillan Publishers Limited. All rights reserved.
ARTICLES NATUREMATERIALS DOI: 10.1038/NMAT3922
aMI region TIMP-3
rTIM
P-3
Sham
MI
MI/
hydr
ogel
MI/
hydr
ogel
/rT
IMP-
3rT
IMP-
3
bMIMI/hydrogelMI/hydrogel/rTIMP-3
Sham
Plas
ma
TIM
P-3
(ng
ml−1
)
Time (days)
15
10
5
0
20
0 4 8 122 6 10 14
Glo
bal M
MP
activ
ity
∗ ∗
MI region Remote regiond
0
0.5
1.0
1.5
2.0
0
0.5
1.0
1.5
2.0
2.5
MT1
-MM
P ac
tivity
∗∗
Sham M
IM
I/hyd
roge
l
MI/h
ydro
gel/r
TIMP-3
c
∗
+
0
1
2
3
Inte
rstit
ial M
MP
activ
ity (n
orm
)
MI region
Sham M
I
MI/h
ydro
gel
MI/h
ydro
gel/r
TIMP-3
∗ +
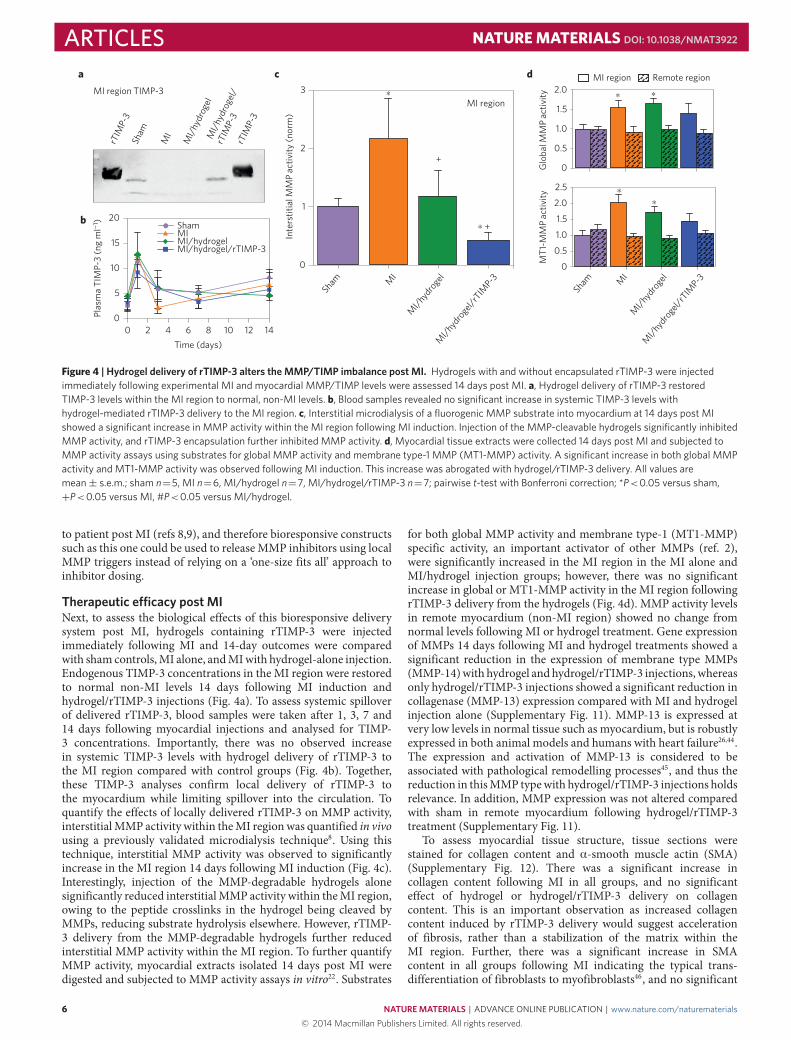
Figure 4 | Hydrogel delivery of rTIMP-3 alters the MMP/TIMP imbalance post MI. Hydrogels with and without encapsulated rTIMP-3 were injectedimmediately following experimental MI and myocardial MMP/TIMP levels were assessed 14 days post MI. a, Hydrogel delivery of rTIMP-3 restoredTIMP-3 levels within the MI region to normal, non-MI levels. b, Blood samples revealed no significant increase in systemic TIMP-3 levels withhydrogel-mediated rTIMP-3 delivery to the MI region. c, Interstitial microdialysis of a fluorogenic MMP substrate into myocardium at 14 days post MIshowed a significant increase in MMP activity within the MI region following MI induction. Injection of the MMP-cleavable hydrogels significantly inhibitedMMP activity, and rTIMP-3 encapsulation further inhibited MMP activity. d, Myocardial tissue extracts were collected 14 days post MI and subjected toMMP activity assays using substrates for global MMP activity and membrane type-1 MMP (MT1-MMP) activity. A significant increase in both global MMPactivity and MT1-MMP activity was observed following MI induction. This increase was abrogated with hydrogel/rTIMP-3 delivery. All values aremean± s.e.m.; sham n=5, MI n=6, MI/hydrogel n=7, MI/hydrogel/rTIMP-3 n=7; pairwise t-test with Bonferroni correction; *P<0.05 versus sham,+P<0.05 versus MI, #P<0.05 versus MI/hydrogel.
to patient post MI (refs 8,9), and therefore bioresponsive constructssuch as this one could be used to releaseMMP inhibitors using localMMP triggers instead of relying on a ‘one-size fits all’ approach toinhibitor dosing.
Therapeutic e�cacy post MINext, to assess the biological effects of this bioresponsive deliverysystem post MI, hydrogels containing rTIMP-3 were injectedimmediately following MI and 14-day outcomes were comparedwith sham controls,MI alone, andMIwith hydrogel-alone injection.Endogenous TIMP-3 concentrations in the MI region were restoredto normal non-MI levels 14 days following MI induction andhydrogel/rTIMP-3 injections (Fig. 4a). To assess systemic spilloverof delivered rTIMP-3, blood samples were taken after 1, 3, 7 and14 days following myocardial injections and analysed for TIMP-3 concentrations. Importantly, there was no observed increasein systemic TIMP-3 levels with hydrogel delivery of rTIMP-3 tothe MI region compared with control groups (Fig. 4b). Together,these TIMP-3 analyses confirm local delivery of rTIMP-3 tothe myocardium while limiting spillover into the circulation. Toquantify the effects of locally delivered rTIMP-3 on MMP activity,interstitialMMP activity within theMI regionwas quantified in vivousing a previously validated microdialysis technique8. Using thistechnique, interstitial MMP activity was observed to significantlyincrease in the MI region 14 days following MI induction (Fig. 4c).Interestingly, injection of the MMP-degradable hydrogels alonesignificantly reduced interstitialMMP activity within theMI region,owing to the peptide crosslinks in the hydrogel being cleaved byMMPs, reducing substrate hydrolysis elsewhere. However, rTIMP-3 delivery from the MMP-degradable hydrogels further reducedinterstitial MMP activity within the MI region. To further quantifyMMP activity, myocardial extracts isolated 14 days post MI weredigested and subjected to MMP activity assays in vitro22. Substrates
for both global MMP activity and membrane type-1 (MT1-MMP)specific activity, an important activator of other MMPs (ref. 2),were significantly increased in the MI region in the MI alone andMI/hydrogel injection groups; however, there was no significantincrease in global or MT1-MMP activity in the MI region followingrTIMP-3 delivery from the hydrogels (Fig. 4d). MMP activity levelsin remote myocardium (non-MI region) showed no change fromnormal levels following MI or hydrogel treatment. Gene expressionof MMPs 14 days following MI and hydrogel treatments showed asignificant reduction in the expression of membrane type MMPs(MMP-14)with hydrogel andhydrogel/rTIMP-3 injections, whereasonly hydrogel/rTIMP-3 injections showed a significant reduction incollagenase (MMP-13) expression compared with MI and hydrogelinjection alone (Supplementary Fig. 11). MMP-13 is expressed atvery low levels in normal tissue such as myocardium, but is robustlyexpressed in both animal models and humans with heart failure26,44.The expression and activation of MMP-13 is considered to beassociated with pathological remodelling processes45, and thus thereduction in thisMMP typewith hydrogel/rTIMP-3 injections holdsrelevance. In addition, MMP expression was not altered comparedwith sham in remote myocardium following hydrogel/rTIMP-3treatment (Supplementary Fig. 11).
To assess myocardial tissue structure, tissue sections werestained for collagen content and α-smooth muscle actin (SMA)(Supplementary Fig. 12). There was a significant increase incollagen content following MI in all groups, and no significanteffect of hydrogel or hydrogel/rTIMP-3 delivery on collagencontent. This is an important observation as increased collagencontent induced by rTIMP-3 delivery would suggest accelerationof fibrosis, rather than a stabilization of the matrix within theMI region. Further, there was a significant increase in SMAcontent in all groups following MI indicating the typical trans-differentiation of fibroblasts to myofibroblasts46, and no significant
6 NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials© 2014 Macmillan Publishers Limited. All rights reserved.
NATUREMATERIALS DOI: 10.1038/NMAT3922 ARTICLESMI MI/hydrogel MI/hydrogel/rTIMP-3Sham
e
Sham MI MI/hydrogelMI/hydrogel/
rTIMP-3
Day 14
PWPW PW PW
30
35
40
45
50
55
60
65
0 2 4 6 8 10 12 14 16
EF (%
)
Time (days)
a
∗
∗∗
∗+
∗∗
∗+# ∗+#
∗∗ ∗
∗
30
40
50
60
70
80
90
0 2 4 6 8 10 12 14 16
LVED
V (m
l)
b
∗
∗∗∗
∗∗∗#
∗∗∗#
Time (days)
2
4
6
8
10
12
14
0 2 4 6 8 10 12 14 16
PCW
P (m
mH
g)
++#
Time (days)
∗+#
∗+#∗∗
∗∗
∗∗
∗
d
0.35
0.45
0.55
0.65
0.75
0.85
0 2 4 6 8 10 12 14 16
LVPW
Thd
(cm
)
+
Time (days)
c
∗+
∗+∗+#
∗∗
∗
∗
∗ ∗
f
0
20
40
60
EF (%
) ∗ ∗ ∗+#
LVED
V (m
l)
∗ ∗
∗+
0
50
100
150
0
5
10
15
PCW
P (m
mH
g) ∗ ∗∗
0
0.2
0.4
0.6
0.8
LVPW
Thd
(cm
) +#∗ ∗
*
Day 28
MI/hydroge
l/rTIMP-3MI
MI/hydroge
l
MI/hydroge
l/rTIMP-3MI
MI/hydroge
l
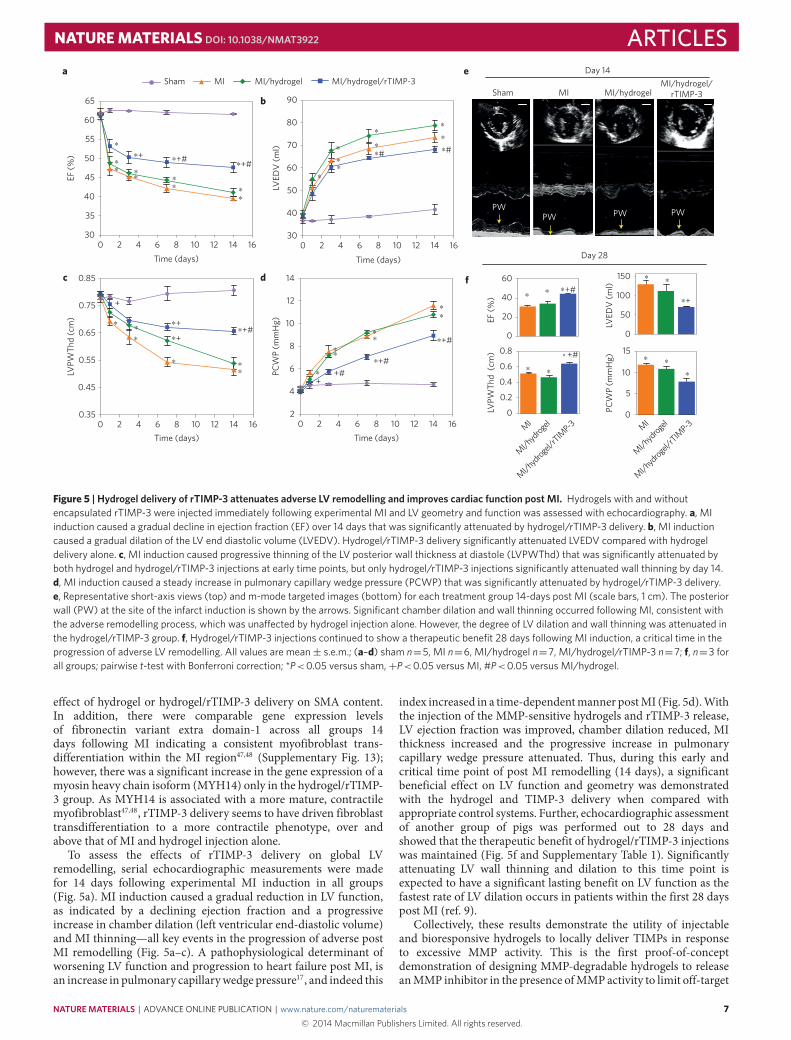
Figure 5 | Hydrogel delivery of rTIMP-3 attenuates adverse LV remodelling and improves cardiac function post MI. Hydrogels with and withoutencapsulated rTIMP-3 were injected immediately following experimental MI and LV geometry and function was assessed with echocardiography. a, MIinduction caused a gradual decline in ejection fraction (EF) over 14 days that was significantly attenuated by hydrogel/rTIMP-3 delivery. b, MI inductioncaused a gradual dilation of the LV end diastolic volume (LVEDV). Hydrogel/rTIMP-3 delivery significantly attenuated LVEDV compared with hydrogeldelivery alone. c, MI induction caused progressive thinning of the LV posterior wall thickness at diastole (LVPWThd) that was significantly attenuated byboth hydrogel and hydrogel/rTIMP-3 injections at early time points, but only hydrogel/rTIMP-3 injections significantly attenuated wall thinning by day 14.d, MI induction caused a steady increase in pulmonary capillary wedge pressure (PCWP) that was significantly attenuated by hydrogel/rTIMP-3 delivery.e, Representative short-axis views (top) and m-mode targeted images (bottom) for each treatment group 14-days post MI (scale bars, 1 cm). The posteriorwall (PW) at the site of the infarct induction is shown by the arrows. Significant chamber dilation and wall thinning occurred following MI, consistent withthe adverse remodelling process, which was una�ected by hydrogel injection alone. However, the degree of LV dilation and wall thinning was attenuated inthe hydrogel/rTIMP-3 group. f, Hydrogel/rTIMP-3 injections continued to show a therapeutic benefit 28 days following MI induction, a critical time in theprogression of adverse LV remodelling. All values are mean± s.e.m.; (a–d) sham n=5, MI n=6, MI/hydrogel n=7, MI/hydrogel/rTIMP-3 n=7; f, n=3 forall groups; pairwise t-test with Bonferroni correction; *P<0.05 versus sham,+P<0.05 versus MI, #P<0.05 versus MI/hydrogel.
effect of hydrogel or hydrogel/rTIMP-3 delivery on SMA content.In addition, there were comparable gene expression levelsof fibronectin variant extra domain-1 across all groups 14days following MI indicating a consistent myofibroblast trans-differentiation within the MI region47,48 (Supplementary Fig. 13);however, there was a significant increase in the gene expression of amyosin heavy chain isoform (MYH14) only in the hydrogel/rTIMP-3 group. As MYH14 is associated with a more mature, contractilemyofibroblast47,48, rTIMP-3 delivery seems to have driven fibroblasttransdifferentiation to a more contractile phenotype, over andabove that of MI and hydrogel injection alone.
To assess the effects of rTIMP-3 delivery on global LVremodelling, serial echocardiographic measurements were madefor 14 days following experimental MI induction in all groups(Fig. 5a). MI induction caused a gradual reduction in LV function,as indicated by a declining ejection fraction and a progressiveincrease in chamber dilation (left ventricular end-diastolic volume)and MI thinning—all key events in the progression of adverse postMI remodelling (Fig. 5a–c). A pathophysiological determinant ofworsening LV function and progression to heart failure post MI, isan increase in pulmonary capillarywedge pressure17, and indeed this
index increased in a time-dependentmanner postMI (Fig. 5d).Withthe injection of the MMP-sensitive hydrogels and rTIMP-3 release,LV ejection fraction was improved, chamber dilation reduced, MIthickness increased and the progressive increase in pulmonarycapillary wedge pressure attenuated. Thus, during this early andcritical time point of post MI remodelling (14 days), a significantbeneficial effect on LV function and geometry was demonstratedwith the hydrogel and TIMP-3 delivery when compared withappropriate control systems. Further, echocardiographic assessmentof another group of pigs was performed out to 28 days andshowed that the therapeutic benefit of hydrogel/rTIMP-3 injectionswas maintained (Fig. 5f and Supplementary Table 1). Significantlyattenuating LV wall thinning and dilation to this time point isexpected to have a significant lasting benefit on LV function as thefastest rate of LV dilation occurs in patients within the first 28 dayspost MI (ref. 9).
Collectively, these results demonstrate the utility of injectableand bioresponsive hydrogels to locally deliver TIMPs in responseto excessive MMP activity. This is the first proof-of-conceptdemonstration of designing MMP-degradable hydrogels to releaseanMMP inhibitor in the presence ofMMPactivity to limit off-target
NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials 7© 2014 Macmillan Publishers Limited. All rights reserved.

ARTICLES NATUREMATERIALS DOI: 10.1038/NMAT3922
effects of MMP inhibitors, which have been clinically problematic,and to provide on-demand presentation of an inhibitor based onlocalMMPactivity. The successful demonstration of this technologyin attenuating postMI remodelling in a large animalmodel warrantsfurther pre-clinical investigation as it could ultimately provide asafe and effective therapy to treat patients in the clinical settingof acute MI. Ultimately, this strategy can be used for any diseasewhere the local imbalance of MMPs and their inhibitors leads todisease progression.
MethodsSolid-phase peptide synthesis. Peptides were synthesized with theMMP-cleavable sequence GCNSGGRMSMPVSNGG–HYD where C is thecysteine containing a thiol group that was used for coupling to a MAHA andHYD is the HYD for hydrogel crosslinking with an ALD-functionalized HA(Supplementary Methods).
Synthesis and characterization of polymers. HA–peptide–HYD polymers weresynthesized by coupling a cysteine-terminated peptide to MAHA (SupplementaryMethods) by mixing in a 4:1 molar ratio, cysteine/maleimide in PBS for 4 h at4 ◦C. The polymer was purified by dialysis against a 20 mM NaCl solution for 5days and then deionized water for 3 days, frozen and lyophilized. HA–ALD wassynthesized by mixing NaHy (350 kDa, Lifecore) at 1% (w/v) and sodiumperiodate (NaIO4) in deionized water at a molar ratio of 2:1 HA/IO4 for 2 h atroom temperature. The reaction was stopped by adding 10% (v/v) ethylene glycolto the reaction, dialysing against deionized water for 5 days, freezing andlyophilizing. DS–ALD was synthesized in a similar fashion except DS (Sigma)was reacted with NaIO4 at a molar ratio of 1:2 DS/IO4 for 5 h at roomtemperature. The percentage of ALD modification was quantified using a TNBScolorimetric assay as previously described49.
Rheometry. To form 3.5 wt% hydrogels, ALD (2.4% HA–ALD, 1.4% DS–ALD(w/v)) and HYD (3.2% (w/v) HA–MMP–HYD)-modified polymers were dissolvedin PBS, mixed 1:1 (v/v) for 1:1 ALD/HYD and gelation characteristics werequantified by monitoring the storage (G′) and loss (G′′) moduli with time usingan AR2000ex Rheometer (TA Instruments) at 37 ◦C under 1% strain and 1 Hz.
Hydrogel degradation and molecule release studies. FITC–BSA or rTIMP-3 wasmixed with the ALD precursor solution and hydrogels were formed as describedabove in cylindrical moulds for 30 min at 37 ◦C. Hydrogels were incubated inPBS supplemented with 1% BSA for FITC–BSA studies or TTC buffer (50 mMTris-HCl, 1 mM CaCl2 and 0.05% Triton X-100, at pH 7.5) for rTIMP-3 studies at37 ◦C. Enzymes (collagenase type 4, Worthington or rMMP-2, R&D Systems)were added every 2 days and buffers were collected and stored at −20 ◦C beforeanalysis. Uronic acid content was analysed to calculate hydrogel mass loss33,FITC–BSA fluorescence was analysed to measure release, and an enzyme-linkedimmunosorbent assay (ELISA) was used to measure rTIMP-3 content(R&D Systems).
rTIMP-3 activity and binding assays. rTIMP-3–His (Amgen) activity wasquantified by its ability to inhibit rMMP-2 (R&D Systems) activity using anMMP-cleavable fluorogenic substrate (R&D Systems). Serial dilutions of rTIMP-3were added to 4 nM activated rMMP-2 in TTC buffer, incubated for 2 h at 37 ◦C,and then the fluorogenic substrate was added and fluorescence kinetics weremeasured over 5 min with a microplate reader (Tecan). rTIMP-3 binding topolysaccharide polymers was evaluated with a solid-phase binding assay(Supplementary Methods).
MI induction and hydrogel injections. Yorkshire pigs (n=43, 25 kg, HamboneFarms) were anaesthetized with isoflurane (2%) and the LV free wall was exposedthrough a left thoracotomy. All animals were treated and cared for in accordancewith the National Institutes of Health Guide for the Care and Use of LaboratoryAnimals, and all protocols were approved by the University of South Carolina’sInstitutional Animal Care and Use Committee. A square calibrated grid wassutured below the origin of the first two obtuse marginal arteries of thecircumflex artery (OM1 and OM2), which provided for a total of 9 distinctinjection sites within a targeted 2 × 2 cm region of myocardium (Fig. 3a). OM1and OM2 were ligated to induce an MI, and characteristic electrocardiogramchanges occurred, but electrical cardioversion and/or defibrillation were notrequired. Past studies demonstrated that this technique creates a uniform andconsistent MI (ref. 20). Sham controls were instrumented in a similar fashionwith the exception of coronary artery ligation. In addition, a vascular accesscatheter was placed in the descending aorta and connected to a subcutaneousport (6 Fr., SlimPort, Bard Access Systems). Pigs were randomized to receiveinjections of saline, hydrogel alone, or hydrogel with rTIMP-3 immediately
following MI induction. For hydrogel injections, the ALD (2.4% HA–ALD, 1.4%DS–ALD (w/v)) and HYD (3.2% (w/v)) precursor solutions were mixed in asterile fashion, drawn into separate 1 ml syringes, and injected into themid-myocardium of each target site using a FibriJet blending connector (NordsonMicromedics, SA-3670) with a 27G needle. Hydrogels were injected immediatelyfollowing MI induction. For the MI/hydrogel/rTIMP-3 group, rTIMP-3 wasmixed into the ALD precursor (20 µg rTIMP-3/100 µl ALD). Successful injectionswere confirmed by visualization of an opacification of the epicardial surface atthe point of myocardial injection.
Blood analysis. Blood samples (5 ml) were collected from the subcutaneous port1, 3, 7 and 14 days post MI. The collected blood samples were centrifuged andthe decanted plasma subjected to ELISA for TIMP-3.
LV assessment with echocardiography. Animals were sedated (20 mg valium,PO, Elkin-Sinn) and two-dimensional echocardiographic studies (GE VIVID 7Dimension Ultrasound System: M4S 1.5–4.3 MHz active matrix array sectortransducer probe) were performed to calculate LV dimensions and ejectionfraction. Echocardiography measurements were taken 1 day before MI induction,and then again 1, 3, 7 and 14 days following MI in a subset of animals (n=25),and 3, 7, 14 and 28 days following MI in another subset of animals (n=9).
Interstitial MMP activity. After 14 days post MI, the pigs were anaesthetizedwith sufentanyl (2 µg kg−1 IV, Baxter Healthcare), morphine sulphate (3 mgkg−1 h−1 IV, Elkin-Sinn) and isoflurane (1%, 3 l min−1 O2, Baxter Healthcare),and mechanically ventilated. The LV was exposed through a sternotomy, amicrodialysis probe (20 kDa, outer diameter of probe shaft 0.77 mm;CMA/Microdialysis) placed within the MI region, and infused with the MMPfluorescent substrate (5 µl min−1) as previously validated8,9. The dialysate wasthen subjected to fluorometry, which reflected interstitial MMP activity, and thesevalues were normalized to referent control values and expressed as a percentage.Following these measurements, the LV was collected, separated into MI andremote regions (area served by left anterior descending artery), and prepared forbiochemical analysis.
Myocardial biochemical analysis. Immunoblotting was performed for totalmyocardial TIMP-3 using approaches described previously20 (SupplementaryMethods). To determine ex vivo MMP activity, LV myocardial extracts (50 µg)were incubated with the global MMP substrate described in the previous section.The steady-state maximal fluorescence units were recorded and all assays wereperformed in triplicate. Expression of key determinants of ECM remodelling wereanalysed using PCR (Supplementary Methods).
MRI analysis. Full-thickness LV myocardial sections were cut from cardiacexplants around the 2 cm hydrogel injection grid and imaged on a 9.4T MRIscanner (Siemens). A T2-weighted spin-echo pulse sequence was employed withthe following imaging parameters: echo time, 40 ms; repetition time, 4,000 ms;averages, 4; matrix size, 256 × 256 × 88; field of view, 35 × 35 mm2; voxel size,= 0.14 × 0.14 × 0.25 mm3. MRI images were converted into NIFTI files usingImageJ software and imported into ITK-SNAP segmentation software as a stackof two-dimensional images. Three-dimensional reconstructions of the hydrogelwere performed using an automated segmentation algorithm in ITK-SNAP(ref. 50). Briefly, the images were contrasted and hydrogel pockets were seededfor the algorithm (Supplementary Fig. 9). Presence of the hydrogel was confirmedwith histology (Supplementary Methods).
Data and statistical analysis. Statistical analyses were performed using STATAstatistical software (Supplementary Methods).
Received 11 September 2013; accepted 20 February 2014;published online 30 March 2014
References1. Fingleton, B. Matrix metalloproteinases as valid clinical targets. Curr. Pharm.
Des. 13, 333–346 (2007).2. Visse, R. & Nagase, H. Matrix metalloproteinases and tissue inhibitors of
metalloproteinases: Structure, function, and biochemistry. Circ. Res. 92,827–839 (2003).
3. Abbenante, G. & Fairlie, D. P. Protease inhibitors in the clinic.Med. Chem. 1,71–104 (2005).
4. Turk, B. Targeting proteases: Successes, failures and future prospects. NatureRev. Drug Discov. 5, 785–799 (2006).
5. Hao, X. J. et al. Angiogenic effects of sequential release of VEGF-A(165) andPDGF-BB with alginate hydrogels after myocardial infarction. Cardiovasc. Res.75, 178–185 (2007).
8 NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials© 2014 Macmillan Publishers Limited. All rights reserved.
NATUREMATERIALS DOI: 10.1038/NMAT3922 ARTICLES6. Ruvinov, E., Leor, J. & Cohen, S. The promotion of myocardial repair
by the sequential delivery of IGF-1 and HGF from an injectable alginatebiomaterial in a model of acute myocardial infarction. Biomaterials 32,565–578 (2011).
7. Peppas, N. A., Bures, P., Leobandung, W. & Ichikawa, H. Hydrogels inpharmaceutical formulations. Eur. J. Pharm. Biopharm. 50, 27–46 (2000).
8. Spinale, F. G., Koval, C. N., Deschamps, A. M., Stroud, R. E. & Ikonomidis, J. S.Dynamic changes in matrix metalloproteinase activity within the humanmyocardial interstitium during myocardial arrest and reperfusion. Circulation118, 16–23 (2008).
9. Webb, C. S. et al. Specific temporal profile of matrix metalloproteinase releaseoccurs in patients after myocardial infarction: Relation to left ventricularremodeling. Circulation 114, 1020–1027 (2006).
10. Stuart, M. A. C. et al. Emerging applications of stimuli-responsive polymermaterials. Nature Mater. 9, 101–113 (2010).
11. Lutolf, M. P. et al. Synthetic matrix metalloproteinase-sensitive hydrogels forthe conduction of tissue regeneration: Engineering cell-invasion characteristics.Proc. Natl Acad. Sci. USA 100, 5413–5418 (2003).
12. Burdick, J. A. & Murphy, W. L. Moving from static to dynamic complexity inhydrogel design. Nature Commun. 3 (2012).
13. Phelps, E. A., Landazuri, N., Thule, P. M., Taylor, W. R. & Garcia, A. J.Bioartificial matrices for therapeutic vascularization. Proc. Natl Acad. Sci. USA107, 3323–3328 (2010).
14. Kim, S. & Healy, K. E. Synthesis and characterization of injectablepoly(N-isopropylacrylamide-co-acrylic acid) hydrogels with proteolyticallydegradable cross-links. Biomacromolecules 4, 1214–1223 (2003).
15. West, J. L. & Hubbell, J. A. Polymeric biomaterials with degradation sites forproteases involved in cell migration.Macromolecules 32, 241–244 (1999).
16. Lutolf, M. P. et al. Repair of bone defects using synthetic mimetics ofcollagenous extracellular matrices. Nature Biotechnol. 21, 513–518 (2003).
17. Spinale, F. G. & Zile, M. R. Integrating the myocardial matrix into heart failurerecognition and management. Circ. Res. 113, 725–738 (2013).
18. Ducharme, A. et al. Targeted deletion of matrix metalloproteinase-9 attenuatesleft ventricular enlargement and collagen accumulation after experimentalmyocardial infarction. J. Clin. Invest. 106, 55–62 (2000).
19. Rohde, L. E. et al.Matrix metalloproteinase inhibition attenuates early leftventricular enlargement after experimental myocardial infarction in mice.Circulation 99, 3063–3070 (1999).
20. Mukherjee, R. et al.Myocardial infarct expansion and matrixmetalloproteinase inhibition. Circulation 107, 618–625 (2003).
21. King, M. K. et al. Selective matrix metalloproteinase inhibition with developingheart failure: Effects on left ventricular function and structure. Circ. Res. 92,177–185 (2003).
22. Spinale, F. G. et al. Cardiac-restricted overexpression of membrane type-1matrix metalloproteinase in mice: Effects on myocardial remodeling withaging. Circ. Heart Fail 2, 351–360 (2009).
23. Peterson, J. T. The importance of estimating the therapeutic index in thedevelopment of matrix metalloproteinase inhibitors. Cardiovasc. Res. 69,677–687 (2006).
24. Overall, C. M. & Kleifeld, O. Tumour microenvironment—opinion: Validatingmatrix metalloproteinases as drug targets and anti-targets for cancer therapy.Nature Rev. Cancer 6, 227–239 (2006).
25. Sahul, Z. H. et al. Targeted imaging of the spatial and temporal variation ofmatrix metalloproteinase activity in a porcine model of postinfarct remodeling:relationship to myocardial dysfunction. Circ. Cardiovasc. Imaging 4,381–391 (2011).
26. Wilson, E. M. et al. Region- and type-specific induction of matrixmetalloproteinases in post-myocardial infarction remodeling. Circulation 107,2857–2863 (2003).
27. Brew, K. & Nagase, H. The tissue inhibitors of metalloproteinases (TIMPs): Anancient family with structural and functional diversity. Biochim. Biophys. Acta1803, 55–71 (2010).
28. Fedak, P. W. et al.Matrix remodeling in experimental and human heart failure:A possible regulatory role for TIMP-3. Am. J. Physiol. Heart Circ. Physiol. 284,H626–H634 (2003).
29. Fedak, P. W. et al. TIMP-3 deficiency leads to dilated cardiomyopathy.Circulation 110, 2401–2409 (2004).
30. Tian, H. et al. TIMP-3 deficiency accelerates cardiac remodeling aftermyocardial infarction. J. Mol. Cell Cardiol. 43, 733–743 (2007).
31. Kassiri, Z. et al. Simultaneous transforming growth factor beta-tumor necrosisfactor activation and cross-talk cause aberrant remodeling response andmyocardial fibrosis in Timp3-deficient heart. J. Biol. Chem. 284,29893–29904 (2009).
32. Seif-Naraghi, S. B. et al. Safety and efficacy of an injectable extracellular matrixhydrogel for treating myocardial infarction. Sci. Trans. Med. 5 (2013).
33. Wall, S. T., Yeh, C. C., Tu, R. Y. K., Mann, M. J. & Healy, K. E. Biomimeticmatrices for myocardial stabilization and stem cell transplantation. J. Biomed.Mater. Res. Part A 95A, 1055–1066 (2010).
34. Ifkovits, J. L. et al. Injectable hydrogel properties influence infarct expansionand extent of postinfarction left ventricular remodeling in an ovine model.Proc. Natl Acad. Sci. USA 107, 11507–11512 (2010).
35. Segers, V. F. et al. Local delivery of protease-resistant stromal cell derivedfactor-1 for stem cell recruitment after myocardial infarction. Circulation 116,1683–1692 (2007).
36. Nelson, D. M., Ma, Z. W., Leeson, C. E. & Wagner, W. R. Extended andsequential delivery of protein from injectable thermoresponsive hydrogels.J. Biomed. Mater. Res. Part A 100A, 776–785 (2012).
37. Leco, K. J., Khokha, R., Pavloff, N., Hawkes, S. P. & Edwards, D. R. Tissueinhibitor of metalloproteinases-3 (TIMP-3) is an extracellularmatrix-associated protein with a distinctive pattern of expression in mousecells and tissues. J. Biol. Chem. 269, 9352–9360 (1994).
38. Yu, W. H., Yu, S., Meng, Q., Brew, K. &Woessner, J. F. Jr TIMP-3 binds tosulfated glycosaminoglycans of the extracellular matrix. J. Biol. Chem. 275,31226–31232 (2000).
39. Lee, M. H., Atkinson, S. & Murphy, G. Identification of the extracellular matrix(ECM) binding motifs of tissue inhibitor of metalloproteinases (TIMP)-3 andeffective transfer to TIMP-1. J. Biol. Chem. 282, 6887–6898 (2007).
40. Troeberg, L. et al. Pentosan polysulfate increases affinity between ADAMTS-5and TIMP-3 through formation of an electrostatically driven trimolecularcomplex. Biochem. J. 443, 307–315 (2012).
41. Burdick, J. A. & Prestwich, G. D. Hyaluronic acid hydrogels for biomedicalapplications. Adv. Mater. 23,H41–H56 (2011).
42. Huang, M., Vitharana, S. N., Peek, L. J., Coop, T. & Berkland, C. Polyelectrolytecomplexes stabilize and controllably release vascular endothelial growth factor.Biomacromolecules 8, 1607–1614 (2007).
43. Kichula, E. T. et al. Experimental and computational investigation of alteredmechanical properties in myocardium after hydrogel injection. Ann. Biomed.Eng. (2013).
44. Spinale, F. G. et al. A matrix metalloproteinase induction/activation systemexists in the human left ventricular myocardium and is upregulated in heartfailure. Circulation 102, 1944–1949 (2000).
45. Troeberg, L. & Nagase, H. Proteases involved in cartilage matrix degradation inosteoarthritis. Biochim. Biophys. Acta 1824, 133–145 (2012).
46. Zeisberg, E. M. et al. Endothelial-to-mesenchymal transition contributes tocardiac fibrosis. Nature Med. 13, 952–961 (2007).
47. Tomasek, J. J., Gabbiani, G., Hinz, B., Chaponnier, C. & Brown, R. A.Myofibroblasts and mechano-regulation of connective tissue remodelling.Nature Rev. Mol. Cell Biol. 3, 349–363 (2002).
48. Goldsmith, E. C., Bradshaw, A. D. & Spinale, F. G. Cellular mechanisms oftissue fibrosis 2 Contributory pathways leading to myocardial fibrosis: Movingbeyond collagen expression. Am. J. Physiol. Cell Physiol. 304,C393–C402 (2012).
49. Su, W. Y., Chen, Y. C. & Lin, F. H. Injectable oxidized hyaluronic acid/adipicacid dihydrazide hydrogel for nucleus pulposus regeneration. Acta Biomater. 6,3044–3055 (2010).
50. Yushkevich, P. A. et al. User-guided 3D active contour segmentation ofanatomical structures: Significantly improved efficiency and reliability.Neuroimage 31, 1116–1128 (2006).
AcknowledgementsThe authors would like to thank T. Lee from Amgen, for supplying the rTIMP-3 peptideused in this study, and W. Liu, S. Pickup and W. Witschey, from Penn Medicine, for MRItechnical expertise. This work was financially supported by the National Institutes ofHealth (R01 HL107938, HL111090, HL095608,T32 HL007954), and a Veterans’ AffairsHealth Administration Merit Award (5101BX000168-03) to F.G.S.
Author contributionsB.P.P., M.B.C., R.C.G., F.G.S. and J.A.B. conceived the ideas and designed theexperiments. B.P.P., D.L., M.B.C., S.M.D., R.J.W., K.N.Z., H.D., S.P., C.B.L., J.A.S. andP.D.F. conducted the experiments and analysed the data. B.P.P., J.H.G., R.C.G, F.G.S. andJ.A.B. interpreted the data and wrote the manuscript.
Additional informationSupplementary information is available in the online version of the paper. Reprints andpermissions information is available online at www.nature.com/reprints.Correspondence and requests for materials should be addressed to J.A.B.
Competing financial interestsThe authors declare no competing financial interests.
NATUREMATERIALS | ADVANCE ONLINE PUBLICATION | www.nature.com/naturematerials 9© 2014 Macmillan Publishers Limited. All rights reserved.





























