Embed Size (px)
Citation preview

Initial management of TMA syndromes
Elie Azoulay,
Saint-Louis Hospital, Medical Intensive Care Unit
Paris Diderot Sorbonne UniversityGroupe de Recherche Respiratoire en Réanimation Onco-Hématologique (GRRR-OH)

C3B factorC5
TTPHUS
T
M
A
Steroids?
Rituximab
Hypertension
AKI
Renal
Neurological
CARDIAC
ADAMTS 13
Complement
Ischemia
Thrombosis
Hemorrhage
STEC
aHUS
ICU Renal replacement therapy
Coma
Stroke
Medical emergency
Auto-immunity
OUTCOMES Genetic
Elie Azoulay, Do-Not-replicate
Differential diagnosesEvans, B12 deficiency, sepsis, HIT
Seizures
Eculizumab
Unresponsive
First line therapy
Second line therapy
H
E
M
O
L
Y
S
I
S
T
H
R
O
M
B
O
C
Y
T
O
P
E
N
I
A
Multiple Organ Failure
Drug-TransplantationCancerInfection
H FactorCD46 (MCP)I Factor
S
C
H
I
S
T
O
C
Y
T
E
S
Idiopathic
COOMBS TEST
Pregnancy
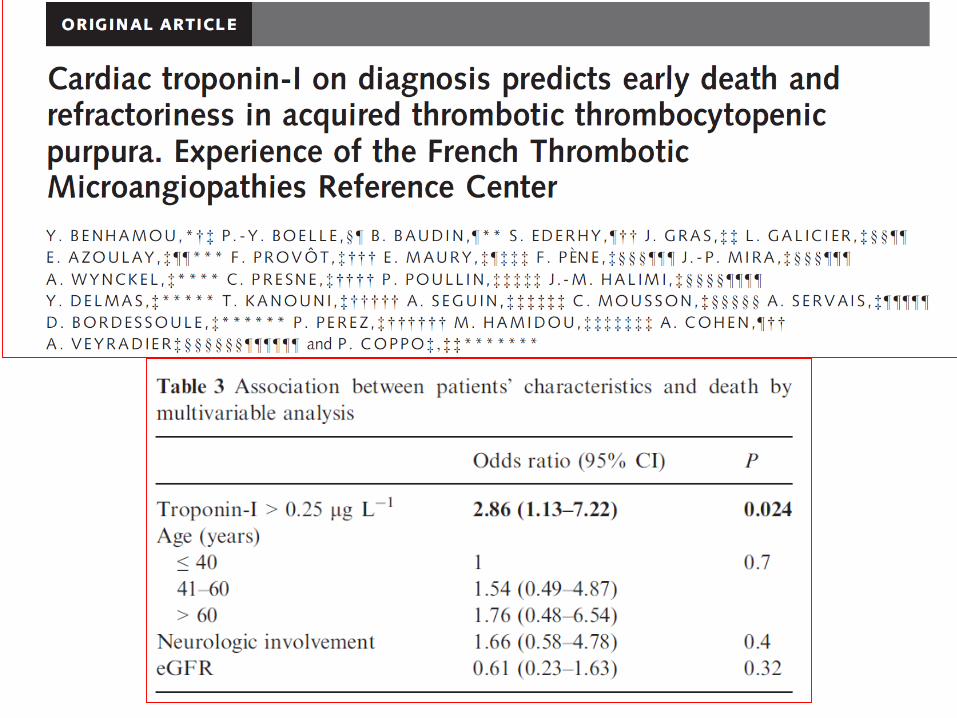
Troponin
Plasma exchange
Sudden death

TMA ?
Understanding TMAs

Normal erythrocytes
Mechanical (non-immune) haemolysis
Microvascular thrombosis
Aggregation of platelets
Ischaemia
Thrombotic microangiopathies

3. Microvascular occlusive disorders by platelet aggregation
TTP, ischaemia in the brain, heart, etc… and most organs
HUS, platelet–fibrin thrombi occlude predominantly, but not only, the renal circulation
1. Mechanical
(non-
immune)
injury to
normal
erythrocytes
2. Consumption
(Peripheral )
thrombocytopenia
TMA diagnosis: basics
Fremeaux-Bacchi V, et al. Clin J Am Soc Nephrol 2013;8:554-61
George JN, et al. N Engl J Med 2014;371:654–66
Scully M, et al. Br J Haematol 2014;164:759–66


TMA= a Multiple Organ Dysfunction
TMA
• Severe
• Reversible
• Prognostic factors hardly apply
• Duration of life support
• Impact of early appropriate management
▪Myocardial infarction▪Thromboembolism▪Cardiomyopathy▪Diffuse vasculopathy
▪Elevated creatinine▪Edema▪Malignant hypertension▪Renal failure▪Dialysis▪Transplant
▪Confusion▪Seizures▪Stroke▪Encephalopathy▪Diffuse cerebral dysfunction
▪Liver necrosis▪Pancreatitis▪Diabetes Mellitus▪Colitis▪Diarrhea▪Nausea/vomiting▪Abdominal pain
▪ Hemolysis▪ Decreased platelets▪ Fatigue▪ Transfusions
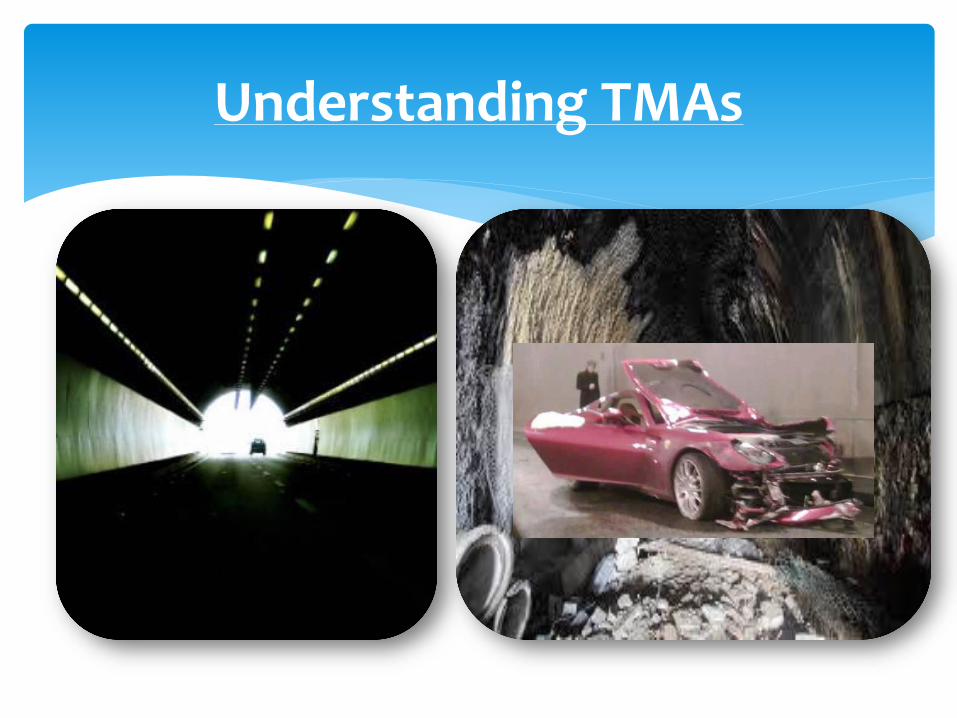
TMA
PEX
60ml/kg/d
Corticosteroids
1mg/kg/dayBP control
Differential diagnosesADAMTS13, Complement
TTP HUS
Platelet countCreatinine
ADAMTS 13
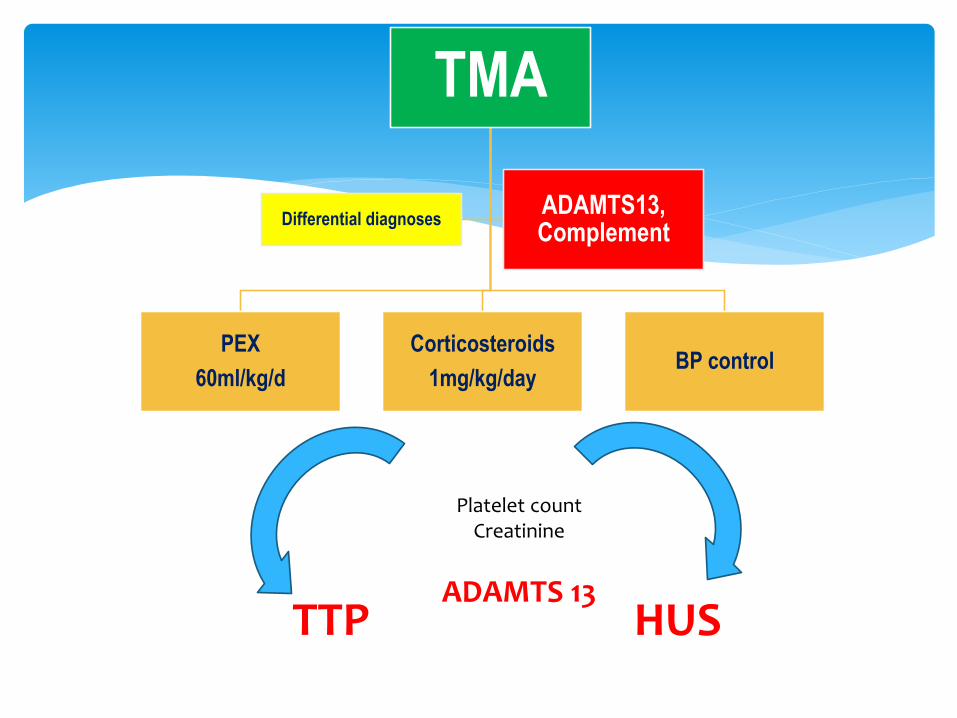
Noris M, et al. N Engl J Med 2009;361:1676–87
Tsai H, et al. Am J Med 2013;126:200–9
Orth D, et al. J Immunol 2009;182:6394–400
Johnson S, et al. Immunobiology 2012;217:235–43
TTP, atypical HUS and STEC-HUS
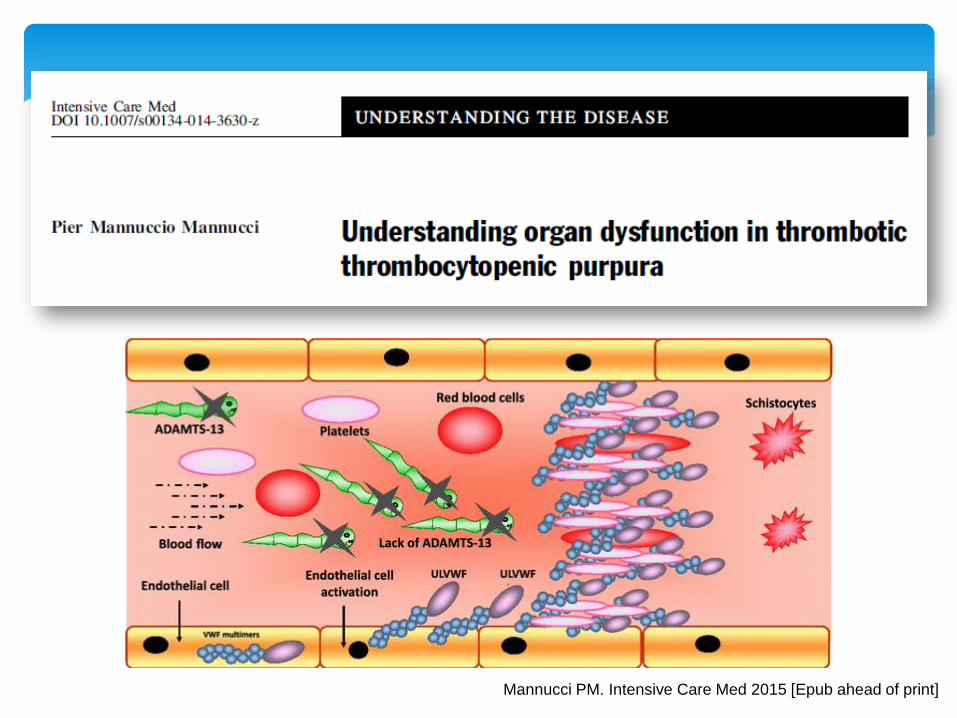
Mannucci PM. Intensive Care Med 2015 [Epub ahead of print]

Mesentericischaemia
Stroke
Myocardial
Infarction
Hospitalacquiredinfection
Varia
- AKI
- Alveolarhaemorrhage
Thrombosis>
Haemorrhage
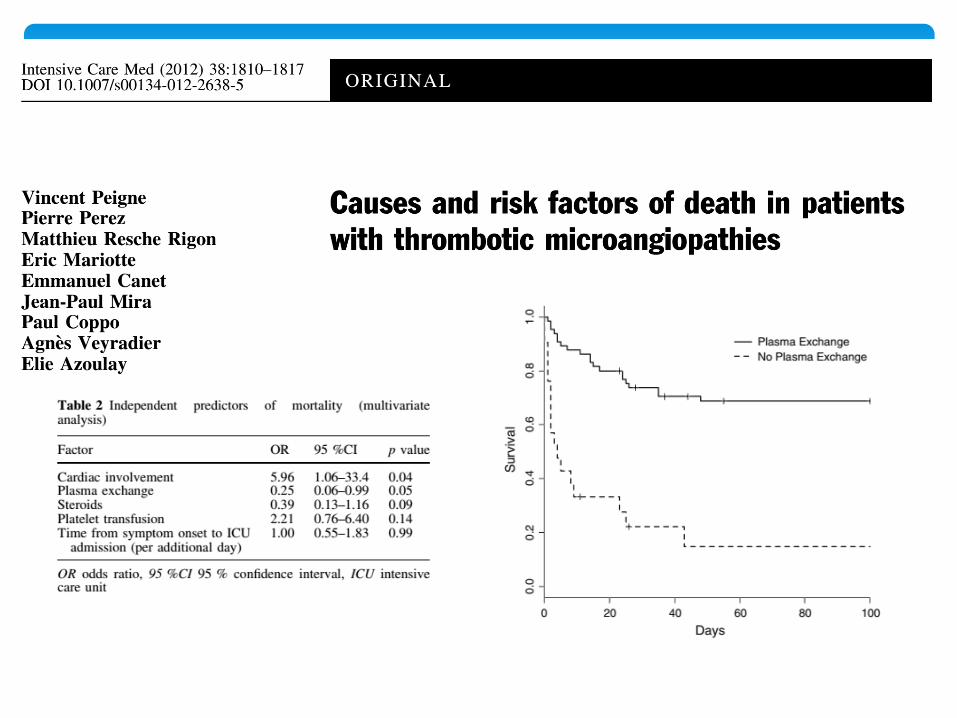
Peigne V, et al. Intensive Care Med 2012;38:1810–7
No platelet transfusion
a 77-yo Japanese man diagnosed with TTP. The patient suddenly died. On autopsy, myocardial infarction manifested as petechiae and fibrotic foci.
The microthrombi in the small arterioles and capillaries were platelet thrombi, which showed positive results for periodic acid-Schiff stain and factor VIII on immunohistochemical staining.
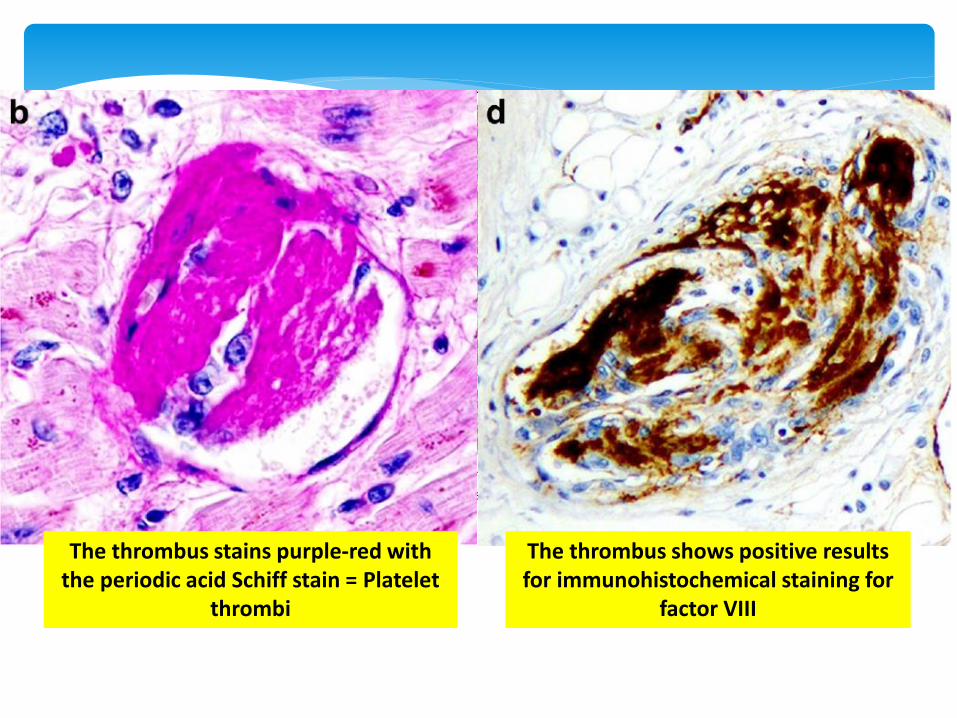
The thrombus stains purple-red with the periodic acid Schiff stain = Platelet
thrombi
The thrombus shows positive results for immunohistochemical staining for
factor VIII

2001-2010 Nationwide Inpatient Sample
database 4032 TTP patients
Mortality 11%
Independent predictors of hospital mortality were older age (OR 1.03 (1.02-1.04), acute
myocardial infarction (OR 1.89 (1.24-2.88), acute renal failure (OR 2.75 (2.11-3.58), congestive
heart failure (OR 1.66 (1.17-2.34), acute cerebrovascular disease (OR 2.68 (1.87-3.85), cancer
(OR 2.49 (1.83-3.40), and sepsis (OR 2.59 (1.88-3.59).
Independent predictors of acute myocardial infarction were older age (OR 1.03 (1.02-1.04),
smoking (OR 1.60 (1.14-2.24), known coronary artery disease (OR 2.59 (1.76-3.81), and
congestive heart failure (OR 2.40 (1.71-3.37).

Cases with higher Troponin T levels (>0.1 µg/L) had higher IgG level at presentation (p=0.03)
<0. 01n=13
0. 01-0. 09n=11
>0. 1n=14
0
25
50
75
100
125
150
175
200
An
ti-A
DA
MTS
13 Ig
G (
%)
Troponin T (µg/L)
Median IgG: 35% Median IgG: 45% Median IgG: 69.5%
Scully M et al. J Thromb Haemost 2009
Anti-ADAMTS13 IgG antibodies and Troponin T levels during acute TTP

Takotsubo cardiomyopathy
Two-chamber view of the left ventricle, obtained in diastole (A) and systole (B). Panel B demonstrates the akinetic and balloon apex in systole with a hypercontractile base.
Ventriculogram


Management of TTP
Admission to an ICU/HDU (intense needs, lines, PEX).
Urgent (within 4-8h) PEX 60ml/kg: ADAMTS13 sup + AB removal,
daily and until 2 days after platelet count normalizes. 100% plasma.
Corticosteroids 1mg/kg/day (high doses for 3 days?)
Low-dose aspirin, DVT prophylaxis, central venous access without
platelet transfusion, and Folic acid.
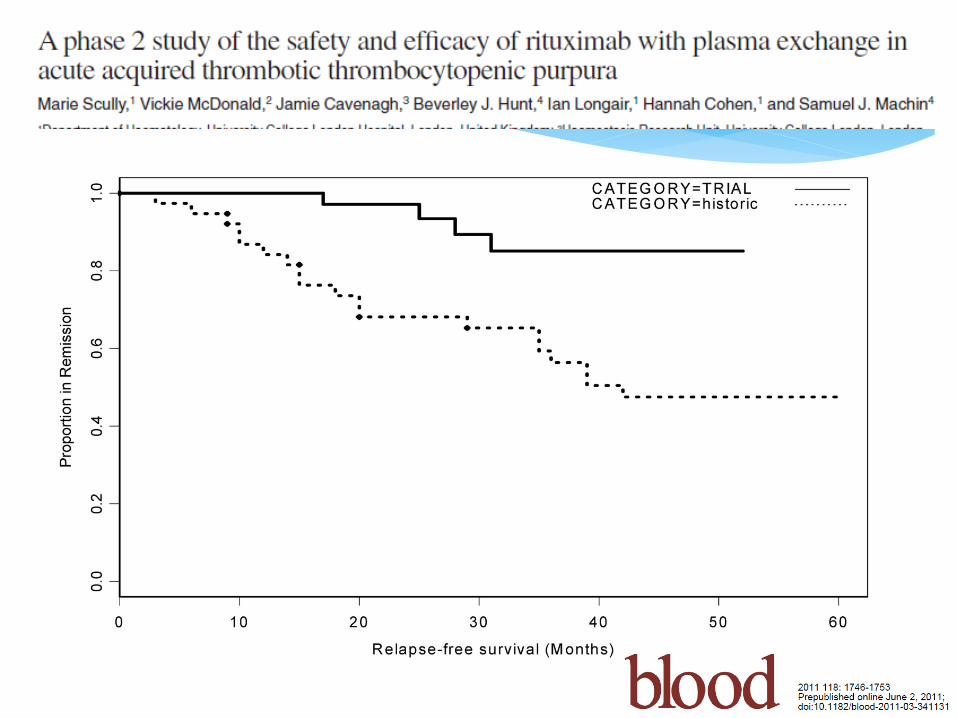
Rituximab is safe and effective for newly diagnosed TTP: decrease
the number of PEX. Early?

• Plasma 40-60 ml/kg (1-1,5 blood mass)
• Within 6h of admission
• Massive transfusion of functionnal ADAMTS13
• Clear anti-ADAMTS13 antibody
• Clear UL Wb factor

Rock et al. The Canadian Apheresis Group
103 pts, 7 y, 18 centers
PEX vs. Plasma transfusion
Group 1: 15.8 EP (3 à 36), 21.5+7.8 liters PVI
Group 2: 7.7 jours de PVI. 6.7+3.3 liters PVI
0
,2
,4
,6
,8
1
0 5 10 15 20 25 30 35
G1: Plasma exchange
G2: Plasma infusion
Weeks
P=0,03
Survival
N Engl J Med. 1991 Aug 8;325(6):393-7.

Darmon M, et al. Crit Care Med 2006;34:2127–33

Management of unresponsive TTP
Unresponsive to PEX + steroids
Check everything, avoid differential diagnoses
Rituximab
High dose steroids
Vincristine, other IS agents (cyclophosphamide etc…)
Splenectomy: late line option
…

OR 95% CI P value
Age >60y 7.90 1.06-78.34 0.04
Neurological symptoms
- Headaches
- Severe symptoms
8.04
1.71
1.27-51.03
0.42-7.09
0.02
0.45
Cardiac signs at presentation 3.44 1.63-16.39 <0.01
Platelet rate at day 2<15 G/L 3.88 1.30-11.62 0.01
Mariotte E, et al. Intensive Care Med 2013;39:1272–81

HUS: Mesangiolysis, fibrin thrombi and fibrinoidnecrosis involving the glomerular vascular pole
Mesangiolysis
Fibrin thrombi Fibrinoid necrosis
El Husseini et al. Am J Kidney Dis. 65(1):127-130
Arteriolar & capillary microthrombi (white clots, platelet-rich fibrin-poor)
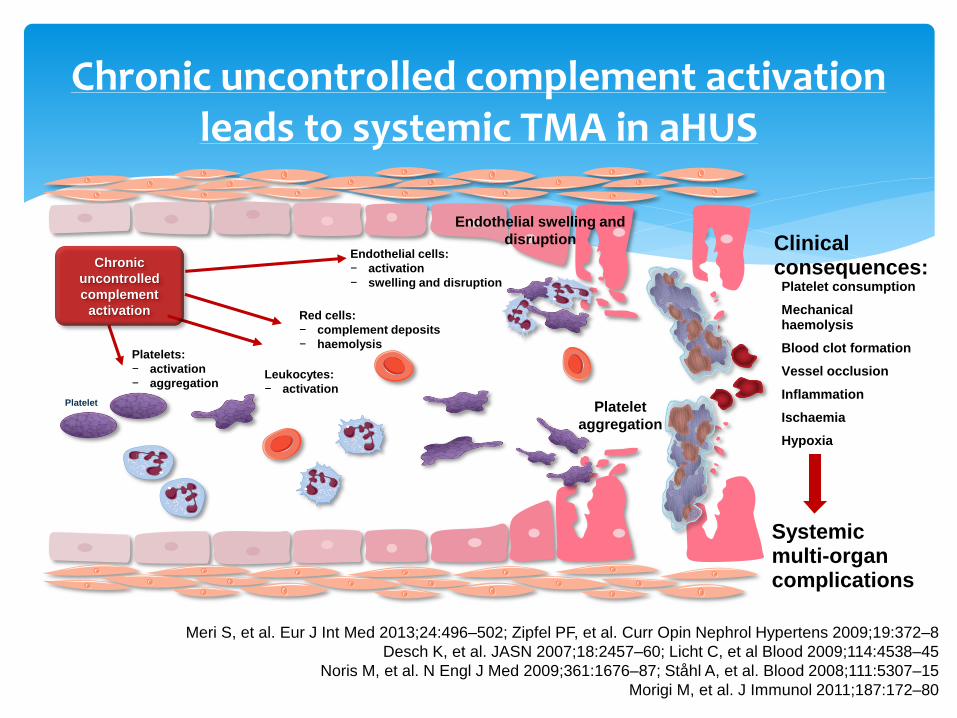
Chronic uncontrolled complement activationleads to systemic TMA in aHUS
Platelet
Platelets:
− activation
− aggregation
Chronic
uncontrolled
complement
activation
Endothelial swelling and
disruption Clinical consequences:
Platelet consumption
Mechanical haemolysis
Blood clot formation
Vessel occlusion
Inflammation
Ischaemia
Hypoxia
Platelet
aggregation
Systemic multi-organ complications
Leukocytes:
− activation
Red cells:
− complement deposits
− haemolysis
Endothelial cells:
− activation
− swelling and disruption
Meri S, et al. Eur J Int Med 2013;24:496–502; Zipfel PF, et al. Curr Opin Nephrol Hypertens 2009;19:372–8
Desch K, et al. JASN 2007;18:2457–60; Licht C, et al Blood 2009;114:4538–45
Noris M, et al. N Engl J Med 2009;361:1676–87; Ståhl A, et al. Blood 2008;111:5307–15
Morigi M, et al. J Immunol 2011;187:172–80

aHUS confirmed clinically
ADAMTS13>10% (result within 24 hours) Samples for complement (serum & EDTA)
DO NOT WAIT FOR RESULTS Complement analysis does not support diagnosis of aHUS, Diagnosis of aHUS does not require identification of a genetic
mutation
Vaccinations: tetravalent meningococcal and Bexsero(meningococcal B)
Antibiotics: penicillin based Eculizumab:
900 mg x 4 weeks 1200 mg every 2 weeks Monitor effect : CH50/CH100
Eculizumab Summary of Product Characteristics. Alexion Europe SAS, 2014Legendre CM et al. N Engl J Med 2013;368:2169–81

23-27%
5-7%
4-8%
1-4%
2-8%3%
X Eculizumab (SOLIRIS®)

37 patients (2 cohorts)
with PEX observation
followed by Eculizumab
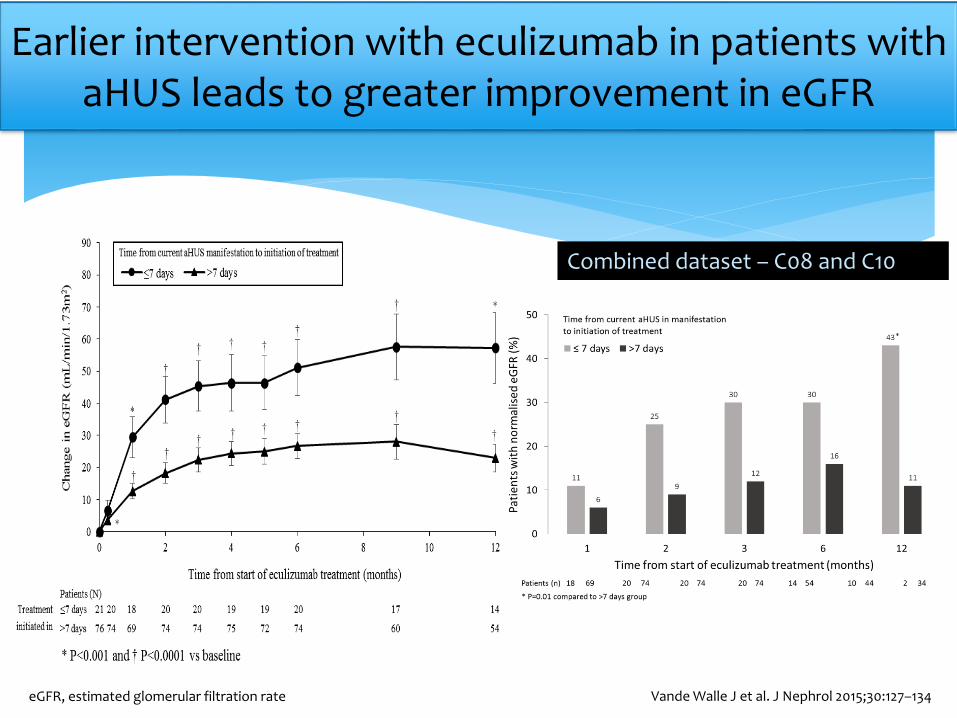
Earlier intervention with eculizumab in patients with aHUS leads to greater improvement in eGFR
Combined dataset – C08 and C10
Vande Walle J et al. J Nephrol 2015;30:127–134 eGFR, estimated glomerular filtration rate

• Open-label single-arm phase 2 trial. Multicenter multinational study of aHUS patients.
• 41 patients were treated with IV eculizumab for 26 weeks. 30 (73%) had complete TMA response.
• All 35 patients on baseline plasma exchange/plasmainfusion discontinued by week 26.
• Of 24 patients requiring baseline dialysis, 5 recovered kidney function before eculizumab initiation and 15 of the remaining 19 (79%) discontinued dialysis during eculizumab treatment.
• Two patients developed meningococcal infections

Dialysis could be discontinued
▪ 20/24 (83%) of patients on dialysis at baseline could discontinue dialysis
▪ 15/17 (88%) patients not on dialysis at baseline, remained dialysis-free through the study evaluation period
Evolution of eGFR under eculizumab treatment in adults with aHUS29.3 mL/min/1.73m2: mean change from baseline in eGFR at Week 26

1. Diagnostic challenges exist even for seniors/specialists.
2. Delayed diagnosis and treatment impacts on survival
3. Sudden deterioration.
4. Access to resuscitation facilities.
5. Adjuvant/novel therapies may be required.
6. Lack of awareness of intervention required to differentially
diagnose TMA cause
7. Organ involvement = severe and poor prognosis.
8. Treatment should not be delayed.
9. Specialist-led, multi-specialty input achieves high-quality care
10. There is the need for both acute and long-term care for a
condition that carries a significant risk of relapse.
Dutt T, et al. BJH 2015;170:737–42
Key points: TMA and the intensivists
Thank you for your attention












![TMA Standard Operating Procedure [Updated April 30, 2015]TMA+_updated+April+30+2015_.pdf · TMA Standard Operating Procedure [Updated April 30, 2015] Calibrating the TMA To obtain](https://img.pdfslide.us/doc/110x75/5e53ad55883f92255623d6b9/tma-standard-operating-procedure-updated-april-30-2015-tmaupdatedapril302015pdf.jpg)