Embed Size (px)
Citation preview

Infant Mental Health Journal, Vol. 16, No. 2, Summer 1995
Initial Adaptation in Mothers and Fathers Following Perinatal Loss
CHARLES H. ZEANAH Division of Infant, Child & Adolescent Psychiatry
Louisiana State University School of Medicine New Orleans, Louisiana
BARBARA DANIS Department of Psychology
University of Denver Denver, Colorado
LAURENCE HIRSHBERG Division of Child & Adolescent Psychiatry
Brown University School of Medicine Providence, Rhode Island
LAURA DIETZ Division of Child & Adolescent Psychiatry
Brown University School of Medicine Providence, Rhode Island
ABSTRACT: Two months following perinatal loss, 82 mothers out of a total of 205 whose infants died at a tertiary referral obstetrical hospital and 47 of their partners were assessed with regard to their re- actions to the deaths of their infants. Sample to population comparisons indicated that those who participated in the investigation were more likely to be socially advantaged. Intensity of mothers’ grief exceeded fathers’, but in roughly 25% of cases fathers’ grief exceeded mothers. Mothers with higher self-reports of ego strength reported lower intensity of grief. Fathers with less ego strength, less social support, and more stressful life events had significantly higher self-reported grief. A subgroup of parents who reported minimal grief was identified and characterized. Implitions of these findings for research on reactions to perinatal loss are discussed.
R&SUM6: Deux mois aprhs la perte perinatale, 82 meres sur un total de 205 dont les nourrissons Ctaient d&bdCs dans un service hospitalier d‘obstktrique et 47 de leurs partenaires furent CvaluCs pour ce qui con- cerne leurs rbctions 1 la mort de leurs nourrissons. Des comparaisons effectuks entre 1’6chantillon et la population indiqutrent que ceux qui participhrent ?i l’enquae Ctaient plus 1 m2me de provenir d‘un milieu social favorid. L’intensitC de la douleur des meres exfedait celle des +res, mais dans 25Yo des cas la douleur
The authors acknowledge the assistance of Daisy Broudy with the early phases of this project and of Sherry Heller with data analysis. This research was supported in part by a Research Scientist Develop- ment Award (MH00691) to Dr. Zeanah. Address correspondence to Charles H. Zeanah, M.D., Division of Infant, Child & Adolescent Psychiatry, Louisiana State University School of Medicine, 1542 Tulane Avenue, New Orleans, Louisiana 701 12-2822.
80 @Michigan Association
for Infant Mental Health
C. H. Zeanah, B. Dank, L. Hirshberg, and L. Dietz 81
des pbres exctdait celle des mtres. Les mtres s’ttant elles-memes dkrites comme ayant une plus grande force d’kgo ont rendu compte d’une plus faible intensitt dans leur douleur. Les pkres ayant moins de force d‘kgo, un soutien social moindre et une vie plus stressante ont rendu compte d‘une douleur plus impor- tante. Un sous-groupe de parents ayant fait &at d’une douleur minimale fut identifit et caracttrisk. Les implications de ces rtsultats pour la recherche sur les rtactions B la perte ptrinatale sont discutks.
RESUMEN: Dos meses despuks de una pkrdida perinatal, 82 madres de un total de 205 cuyos infantes murieron en un hospital de obstetricia de referencia terciaria y 47 de sus parejas fueron evaluados con respecto a sus reacciones en cuanto a la muerte de sus infantes. Muestras comparativas indicaron que quienes participaron en la investigaci6n presentaban probablemente m b ventajas sociales. La intensidad del dolor materno excedi6 a la de 10s padres, y s610 en el 25% de 10s casos el dolor de 10s padres fue mAs intenso. Aquellas madres cuyos propios reportes de su fuerza interior eran m8s altos, presentaron una menor intensidad de allicci6n. Los padres con una fuerza interior baja, rnenos apoyo social y una vida llena de tensiones, presentaron reportes propios de tener una mayor intensidad de dolor. Un sub- grupo de padres que reportaron una aflicci6n minima fue identificado y caracterizado. En el ensayo se discuten las implicaciones de estos hallazgos sobre las reacciones a pkrdidas perinatales.
Although a great deal has been learned about parents’ psychological reactions to perinatal loss, much remains to be clarified (Leon, 1992; Zeanah, 1989). A number of methodological problems in research in this area have made some findings about reactions to perinatal loss questionable. These include lack of validated instruments for assessing symptoms of grief, variable periods of time following the loss when assessments were conducted, and the use of instruments not specific to symptoms of grief. In addition, many previous studies were conducted before, or concurrent with, sweeping changes in hospital management of perinatal loss that occurred in the late 1970s and early 1980s. In the past 15 years, hospital staffs have developed systematic protocols designed to make the baby who died and the experience of loss more real for parents. Thus, results from some earlier studies may not necessarily reflect the contemporary experience of couples whose infants have died.
For example, although perinatal loss has been associated with significant grief for most parents, particularly in the initial months following the infant’s death, little is known about individual differences in response to the loss and what factors are associated with more or less intense reactions. A first question about parents’ adap- tation is which factors might make them more vulnerable to the effects of the loss.
Infant-related variables, such as gestational age at the time of the loss and whether the infant was stillborn or liveborn, have yielded mixed results in previous research. In a retrospective investigation, Peppers and Knapp (1980) found no differences in reactions to miscarriage, stillbirth, and neonatal death among 65 women. Lasker and colleagues (Goldbach, Dunn, Toedter, & Lasker, 1991; Toedter, Lasker, & Aldaheff, 1988), on the other hand, found that 2 months following the loss, mothers in their sample had grief reactions that were significantly correlated with gestational age. Theut
82 Infant Mental Health Journal
and colleagues also found that losses after 20 weeks were associated with more in- tense grief than losses prior to 20 weeks gestation (Theut et al., 1989). Problems with the retrospective design and the range of times since the loss that occurred in the first investigation, and the large number of early pregnancy losses in the latter two, leave undetermined the question of whether infant-related variables are significantly related to intensity of parents’ grief following perinatal loss.
Parent psychological variables have been little explored in research on perinatal loss (Leon, 1992). Personality characteristics, for example, have not been examined at all. Effects of previous losses have been investigated more than other variables in this area, and results have proven consistent. Having experienced previous losses has not been associated with intensity of grief in previous research (Benfield, Leib, & Vollman, 1978; Toedter et al., 1988).
Previous investigations also have assessed social contextual variables in relation to reactions following perinatal loss. For example, lack of or problematic social sup- port (LaRoche et al., 1984; Rowe et a]., 1978), more stressful life events, and marital dissatisfaction (LaRoche et al., 1984) all have been associated with more intense grief reactions.
Another question that has not been answered fully concerns similarities and differences in mothers’ and fathers’ reactions. For example, although all previous in- vestigations that have compared mothers’ and fat hers’ reactions have determined that mothers’ grief exceeds fathers’ (Benfield et al., 1978; Theut et al., 1989; Tudelope, Iredell, Rodgers, & Gunn, 1986; Wilson, Fenton, Stevens, & Soule, 1982), in one study, 22% of the time intensity of fathers’ grief exceeded that of their partners (Benfield et al., 1978). Although it has been suggested that fathers grieve differently from mothers (Wilson et al., 1982), this has been too little explored to reach any conclusions. There is some evidence of a more minimizing style in fathers in response to perinatal loss, although the evidence is largely anecdotal (Benfield et al., 1978; Kennell, Slyter, & Klaus, 1970). The paucity of data regarding correlates of intensity of grief in parents following perinatal loss leaves the possibility of different patterns in mothers and in fathers inadequately explored.
Finally, one of the most important unexplored questions regarding studies of perinatal loss concerns sampling bias. Most previous investigations have provided little to no information about how many subjects refused to participate and how they compared to those who did participate (Zeanah, 1989). One of the few studies that examined refusers found that they were less likely to be married, more likely to have a baby who died on the first day, and less likely to consent to an autopsy (Tudelope et al., 1986). Other studies have found that fewer than half of parents eligible for participation actually completed research protocols (Benfield et al., 1978; Rowe et al., 1978). Further, subjects from lower social classes have been noted to be under- represented in investigations of all types of losses (Osterweis, Solomon, & Green, 1987). Given that agreeing to participate in these types of investigations requires that subjects re-live a painful experience suggests that those who have more dismissing responses to painful experiences may be underrepresented. All of this raises ques- tions of sample bias and to whom results of extant research can be generalized. The question of who volunteers and who does not volunteer for research on perinatal
C. H. Zeanah, B . Danis, L. Hirshberg, and L. Diet2 83
loss is a difficult, important, and heretofore largely unaddressed issue in the literature on perinatal loss.
The purpose of the current investigation, which is the first report of a longitudinal investigation of perinatal loss, is to address many of the above issues in a single study. First, we predict that subjects who participated in the investigation will be distinguished from those who refused to participate and those who were not contacted by being more socially advantaged. Of those parents who participated, we hypothesize that as a group, mothers’ intensity of grief will exceed fathers’ 2 months after the loss, although we anticipate considerable variability. Further, we propose to explore cor- relates of parents’ intensity of grief that may shed light on individual differences. Specifically, we will examine relationship support, personality characteristics, other stressors, and demographic variables as predictors of grief intensity. Finally, based on our clinical experiences, we predict for both mothers and fathers no relationship between intensity of grief and characteristics of the loss such as infant gender, gesta- tional age, or whether the infant was stillborn or liveborn.
METHODS
Subjects
Between December of 1988 and April of 1990,205 infants died at between 20 and 44 weeks gestation at a single tertiary referral hospital in New England. Of these, 156 (76%) mothers were contacted and invited to participate in a study of families whose baby had died. Of the 156 who were approached about participating, 82 (40010) consented and 74 (36%) refused to participate. Of the 49 mothers who were not con- tacted, 10 (5%) were purposely not contacted because they did not speak English, but another 39 (19%) were unable to be reached because of an incorrect address, disconnected phone, etc.
The 82 mothers who participated were largely middle class (95% Hollingshead I- 111), older (28.7 f 5.4 years), and well-educated (13.8 f 2.5 years of education). A subgroup of 23 of the Participants were included as a comparison group in an investigation of women who terminated pregnancies because of fetal anomalies (Zeanah, Dailey, Rosenblatt, & Saller, 1993), but the entire group has not been reported elsewhere.
A total of 47 fathers participated in the investigation. They were also older (30.1 f 6.3 years) and well-educated (13.8 f 3.0 years). There were no differences in age, education, or social class in mothers whose partners participated and mothers whose partners did not participate in the study.
Measures
Parental Personality Measures Ego Strength Scale (Epstein & O’Brien, 1982): This 42-item, self-report scale uses
a 5-point Likert format ranging from “completely false” to “completely true.” The scale is used to determine a subject’s ego strength and defensiveness or tendency to minimize or dismiss distress. Internal consistencies of these subscales were 0.83 and 0.77, respectively. Both convergent and discriminant validity have been demonstrated
84 Infant Mental Health Journal
for the scale (Epstein & O’Brien, 1982). Measures of both ego strength and defen- siveness were used in the current investigation.
Parental Social Characteristics Measures Nethelp (Boukydis, Lester, & Hoffman, 1989): This is a measure of social support
in which subjects list individuals who have provided them with help and support and rate their satisfaction with the help provided on a 7-point scale. For this investiga- tion, we derived social support by totaling the number of individuals listed as sup- portive and rated as high (5-7) in degree of satisfaction. Two variables were deter- mined for the current investigation: Family Support, consisting of all family members listed as supportive, and Non-Family Support, consisting of all individuals listed as supportive who were not family members. This scale has been used in another in- vestigation of perinatal loss (Zeanah et al., 1993).
Dyadic Adjustment Scale (Spanier, 1976): This is a well-known and widely used 32-item scale for assessing self-reported marital adjustment. Internal consistency for the total score was 0.96. The scale has been extensively validated. Total scores of less than 100 are thought to indicate relationship distress. Only the total score for perceived Marital (Partner) Adjustment was used in the current investigation.
Life Experiences Survey (Sarason, Johnson, & Siegel, 1978): This is a frequently used questionnaire designed to measure stressful life events. From a list of 47 possible events, subjects select those that have been positive and negative during the past 12 months and the degree to which they have been affected by the events. We obtained scores of negative events that reflect both the number and magnitude of these events and report this single score as a measure of Stressful Life Events.
Measures of Grief and Mective Symptomatology Beck Depression Inventory (BDI, Beck, Ward, Mendelsohn, Mock & Erbaugh,
1961): The BDI is a widely used and well-validated self-report scale for assessing depressed mood or distress. Scores range from 0-63 and, according to Beck, Steer, and Garbin (1988), scores of 0-10 represent none to minimal depression, scores of 11-18 mild to moderate depression, scores of 19-29 moderate to severe depression, and scores of greater than 30 severe to extreme depression. We used the score as a measure of depressed mood.
Grief Experience Inventory -perinatal version (Sanders, Mauger, & Strong, 1979): This is a 135-item questionnaire for self-report of symptoms of grief following the loss of a baby. The original instrument has been used to report on grief following loss of a spouse or loss of a child (Sanders, Mauger, & Strong, 1979). Wording was changed slightly from the original instrument with permission of the publisher to make it more appropriate for perinatal loss. For example, in place of the GEI item that reads, “I am strongly preoccupied with a picture in my head of the deceased,” we substituted, “I am strongly preoccupied with a picture in my head of my baby.”
Perinatal Grief Scale (PGS, Potvin, Lasker, & Toedter, 1989; Toedter et al., 1988): The PGS (short version) is a self-report scale for measuring intensity of affective symp tomatology following the loss of a baby. Three factor-analyzed scales have been derived that assess grief, difficulty coping, and despair. Scores for each scale range from 1-5 and in this report are reversed for clarity, so that higher scores represent more grief, more difficulty coping, and more despair. The scale has been validated
C. H. Zeanah, B. Donis, L. Hirshberg, and L. Dietz 85
by moderate to high correlations with the Symptom Checklist-90 depression subscale (Toedter et al., 1988) and by convergence with other measures of parental distress (Zeanah et al., 1993).
Procedures
A list of names and addresses of parents whose babies died at the hospital were forwarded daily to the investigators. About 6 weeks following the loss, the investigators sent families a letter offering condolences and informing families that a member of the research team would be contacting them about a study of families whose baby had died. Many of the families had been informed about the study by one of the hospital social workers, who are routinely consulted in cases of perinatal death.
About 7 to 8 weeks after the death, a member of the team contacted the family by phone and invited them to participate in the study. They were informed that it would involve one interview now and another interview in a little over a year. In- formed consent was obtained at the time of the first visit. This paper reports results from the assessments obtained 2 months after the loss of the baby.
Most data collection appointments were conducted in the family's home (>90%), unless the family preferred to meet at the hospital. If both members of the couple participated in the investigation, interviews with each parent were conducted separately and all questionnaires were completed independently.
RESULTS
Comparisons of Participants, Re fusers, and Nonparticipants
In order to characterize the Participants in the current investigation, they were com- pared to Refusers and to the Not Contacted (excluding the non-English group) on variables that could be garnered from a chart review of the mothers' and infants' medical records. Results comparing the three groups indicated that mothers who par- ticipated were different in important ways from mothers who refused to participate or mothers who were never contacted.
Compared to Refusers, Participants were from higher social classes (2.25 vs. 3.00, F = 1 8 . 3 , ~ < .OOO) and better educated (13.8 yrs. vs. 12.1 yrs., F = 1 8 . 8 , ~ < .OOO). Participants were also more likely than Refusers to be married (88% vs. 63%, x2 = 6.10, p < .047) and less likely than Refusers to have a medically complicated pregnancy (53% vs. 60'7'0, x2 = 12.8, p < .000).
Compared to mothers who were not contacted, mothers who participated in the investigation were older (28.8 vs. 25.2 years, F = 4.94, p < .008), were better educated (13.8 vs. 11.4 years, F = 18.8, p < .OOO), were from higher social classes (2.25 vs. 3.65, F = 18.3, p < .OW), had had fewer previous pregnancies (1.44 vs. 2.36, F = 3.81, p < .024), were more likely to be White (91Vo vs. 64%, x2 = 12.2, p < .002), more likely to have been married (88% vs. 53%, xz = 10.8, p < .001), and less likely to have a stillborn infant (39% vs. 49%, x2 = 6.39, p < .01).
These results suggest a number of differences in subjects who agreed to participate and those who refused or were not contacted. Although multiple comparisons were made, thereby lowering confidence in any single finding, the overall pattern of these results is clear. In general, subjects of the investigation who agreed to participate
86 Infant Mental Health Journal
were older, better educated, more advantaged socially, and had fewer medical com- plications in pregnancy than those who refused to participate or those who were never contacted.
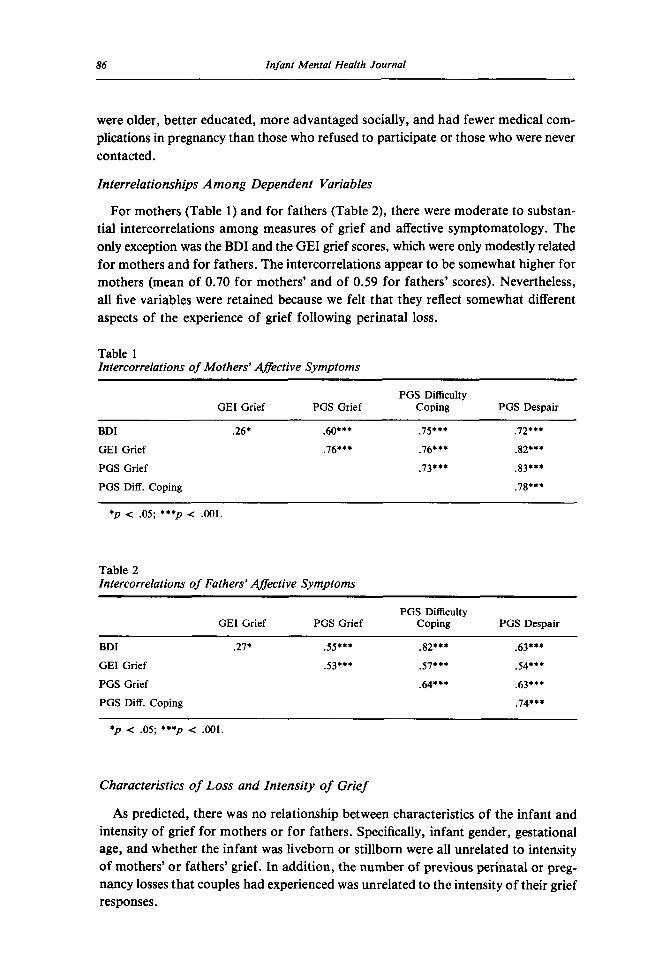
Interrelationships Among Dependent Variables
For mothers (Table 1) and for fathers (Table 2), there were moderate to substan- tial intercorrelations among measures of grief and affective symptomatology. The only exception was the BDI and the GEI grief scores, which were only modestly related for mothers and for fathers. The intercorrelations appear to be somewhat higher for mothers (mean of 0.70 for mothers’ and of 0.59 for fathers’ scores). Nevertheless, all five variables were retained because we felt that they reflect somewhat different aspects of the experience of grief following perinatal loss.
Table 1 Intercorrelations of Mothers’ Affective Symptoms
PGS Difficulty GEI Grief PGS Grief Coping PGS Despair
BDI .26* .60*** . I S * * * ,72***
GEI Grief .76*** .76*** .82***
PGS Grief .73*** .83***
PGS Diff. Coping .78***
*p < .05; ***p c .001.
Table 2 Intercorrelations of Fathers’ Affective Symptoms
PGS Difficulty GEI Grief PGS Grief Coping PGS Despair
BDI .27+ .55*** .82*** .63***
GEI Grief .53*** .57*** .54***
PGS Grief .64*** .63***
PGS Diff. Coping .74***
* p < .05; ***p < .001.
Characteristics of Loss and Intensity of Grief
As predicted, there was no relationship between characteristics of the infant and intensity of grief for mothers or for fathers. Specifically, infant gender, gestational age, and whether the infant was liveborn or stillborn were all unrelated to intensity of mothers’ or fathers’ grief. In addition, the number of previous perinatal or preg- nancy losses that couples had experienced was unrelated to the intensity of their grief responses.
C. H. Zeanah, B. Danis, L . Hirshberg, and L. Dietz 87
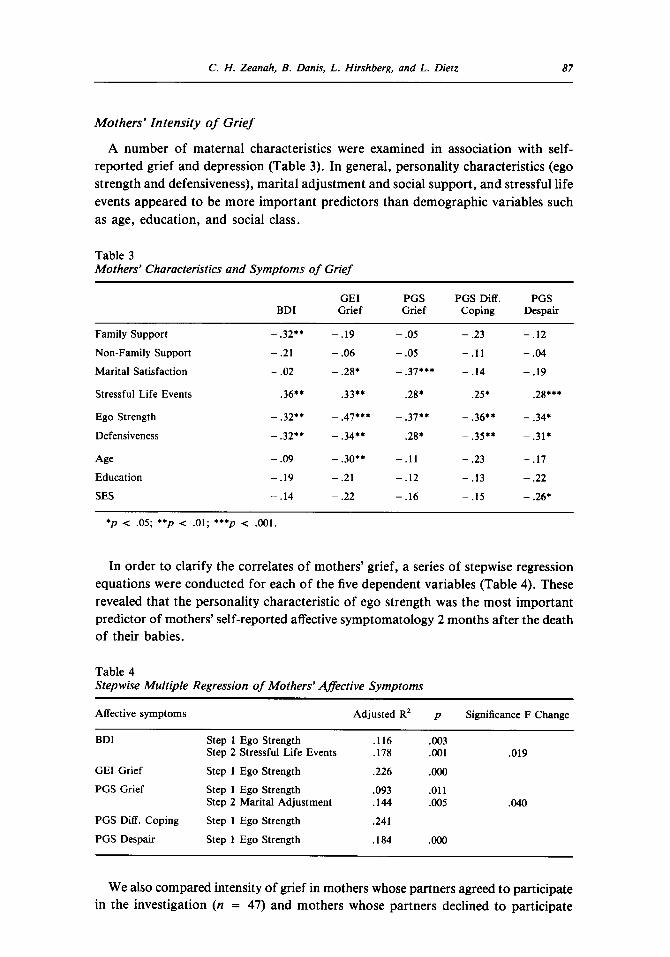
Mothers’ Intensity of Grief
A number of maternal characteristics were examined in association with self- reported grief and depression (Table 3). In general, personality characteristics (ego strength and defensiveness), marital adjustment and social support, and stressful life events appeared to be more important predictors than demographic variables such as age, education, and social class.
Table 3 Mothers’ Characteristics and Symptoms of Grief
GEI PGS PGS Diff. PGS BDI Grief Grief Coping Despair
Family Support
Non-Family Support
Marital Satisfaction
Stressful Life Events
Ego Strength
Defensiveness
Age Education
SES
- .32**
- .21
- .02
.36**
- .32**
- .32**
- .09
- .19
- .14
- .19
- .06
- .28*
.33**
- .05
- .05
- .37***
.28*
- .47***
- .34**
- .30**
- .21
- .22
- .37**
.28*
- . l l
- .12
- .16
~~
- .23
- . 1 1
- .14
.25*
- .36**
- .35**
- .23
- .13
- .15
- .I2
- .04
- .19
.28***
- .34*
- .31*
- .17
- .22
- .26*
*p < .05; **p < .01; ***p < .001.
In order to clarify the correlates of mothers’ grief, a series of stepwise regression equations were conducted for each of the five dependent variables (Table 4). These revealed that the personality characteristic of ego strength was the most important predictor of mothers’ self-reported affective symptomatology 2 months after the death of their babies.
Table 4 Stepwise Multiple Regression of Mothers’ Affective Symptoms
Affective symptoms Adjusted R2 p Significance F Change
BDI Step 1 Ego Strength .116 .003
GEI Grief Step 1 Ego Strength .226 .Ooo
PGS Grief Step 1 Ego Strength .093 .011
Step 2 Stressful Life Events ,178 .001 .019
Step 2 Marital Adjustment .I44 .005 .040
PGS Diff. Coping Step 1 Ego Strength .241
PGS Despair Step 1 Ego Strength .184 .Ooo
We also compared intensity of grief in mothers whose partners agreed to participate in the investigation (n = 47) and mothers whose partners declined to participate
88 Infant Mental Health Journal
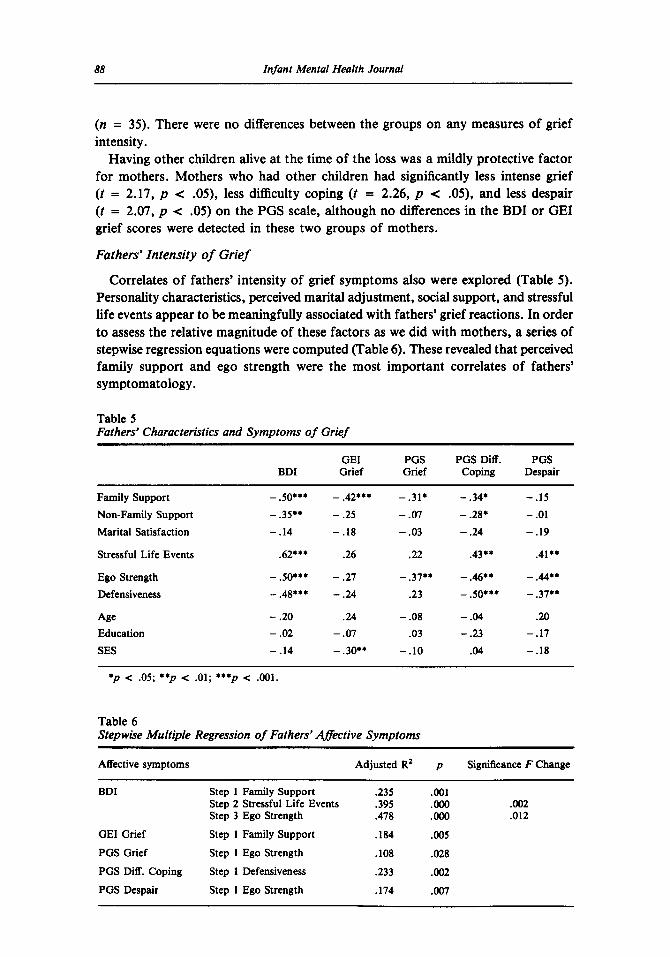
(n = 35). There were no differences between the groups on any measures of grief intensity.
Having other children alive at the time of the loss was a mildly protective factor for mothers. Mothers who had other children had significantly less intense grief (t = 2.17, p < .05), less difficulty coping ( t = 2.26, p < .05), and less despair (t = 2.07, p < .05) on the PGS scale, although no differences in the BDI or GEI grief scores were detected in these two groups of mothers.
Fathers’ Intensity of Grief
Correlates of fathers’ intensity of grief symptoms also were explored (Table 5) . Personality characteristics, perceived marital adjustment, social support, and stressful life events appear to be meaningfully associated with fathers’ grief reactions. In order to assess the relative magnitude of these factors as we did with mothers, a series of stepwise regression equations were computed (Table 6). These revealed that perceived family support and ego strength were the most important correlates of fathers’ symptomatology .
Table 5 Fathers’ Characteristics and Symptoms of Grief
GEI PGS PGS Diff. PGS BDI Grief Grief Coping Despair
Family Support Non-Family Support Marital Satisfaction
Stressful Life Events
Ego Strength Defensiveness
Age Education SES
-.50***
- .35** - .14
.62*+*
- so*** - .48**’ - .20 - .02 - .14
- .42+** - .25 - .18
.26
- .27 - .24
.24 - .07
- .30**
- .31* - .07 - .03
.22
- .37** .23
- .08 .03
- .10
- .34* - .28+ - .24
.43**
- .M*+
- .50***
- .04 - .23 .04
-.IS - .01 - .19
.41**
- .#** - .37**
.20 - .17 - .18
* p < .05; * p < .01; *+*p < .001.
Table 6 Stepwise Multiple Regression of Fathers’ qffective Symptoms
Affective symptoms Adjusted R2 p Significance F Change
BDI ~~
Step 1 Family Support .235 .001 Step 2 Stressful Life Events .395 .Ooo .002 Step 3 Ego Strength .478 .Ooo .012
GEI Grief Step 1 Family Support .184 .005
PGS Grief Step 1 Ego Strength .lo8 .028 PGS Diff. Coping Step 1 Defensiveness .233 .002 PGS Despair Step 1 Ego Strength .I74 .007
C. H. Zeanah, B. Dank, L. Hirshberg, and L . Dietz 89
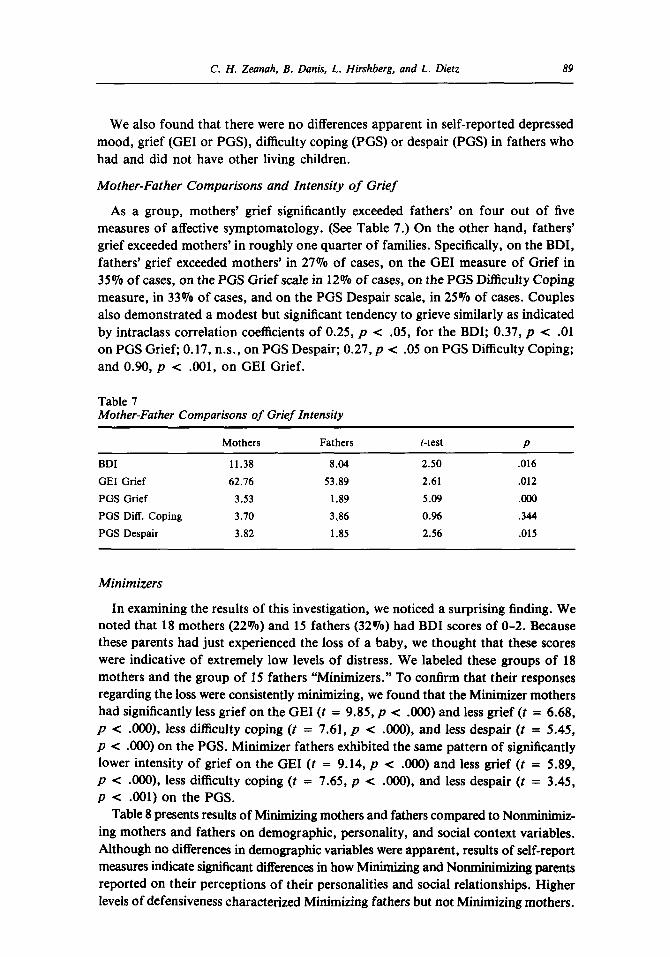
We also found that there were no differences apparent in self-reported depressed mood, grief (GEI or PGS), difficulty coping (PGS) or despair (PGS) in fathers who had and did not have other living children.
Mother-Father Comparisons and Intensity of Grief
As a group, mothers’ grief significantly exceeded fathers’ on four out of five measures of affective symptomatology. (See Table 7.) On the other hand, fathers’ grief exceeded mothers’ in roughly one quarter of families. Specifically, on the BDI, fathers’ grief exceeded mothers’ in 27% of cases, on the GEI measure of Grief in 35% of cases, on the PGS Grief scale in 12% of cases, on the PGS Difficulty Coping measure, in 33% of cases, and on the PGS Despair scale, in 25% of cases. Couples also demonstrated a modest but significant tendency to grieve similarly as indicated by intraclass correlation coefficients of 0.25, p < .05, for the BDI; 0.37, p < .01 on PGS Grief; 0.17, n.s., on PGS Despair; 0.27, p < .05 on PGS Difficulty Coping; and 0.90, p < .001, on GEI Grief.
Table 7 Mother-Father Comparisons of Grief Intensity
Mothers Fathers t-test P
BDI 11.38 8.04 2.50 ,016
GEI Grief 62.76 53.89 2.61 .012
PGS Grief 3.53 1.89 5.09 .ooo PGS Diff. Coping 3.10 3,86 0.96 .344
PGS Despair 3.82 1.85 2.56 .015
Minimizers
In examining the results of this investigation, we noticed a surprising finding. We noted that 18 mothers (22%) and 15 fathers (32%) had BDI scores of 0-2. Because these parents had just experienced the loss of a baby, we thought that these scores were indicative of extremely low levels of distress. We labeled these groups of 18 mothers and the group of 15 fathers “Minimizers.” To confirm that their responses regarding the loss were consistently minimizing, we found that the Minimizer mothers had significantly less grief on the GEI ( t = 9.85, p < .OOO) and less grief (t = 6.68, p < .OOO), less difficulty coping ( t = 7.61, p < .OOO), and less despair (t = 5.45, p < .OOO) on the PGS. Minimizer fathers exhibited the same pattern of significantly lower intensity of grief on the GEI ( t = 9.14, p < .OOO) and less grief (t = 5.89, p < .OOO), less difficulty coping ( t = 7.65, p < .OOO), and less despair ( t = 3.45, p < .001) on the PGS.
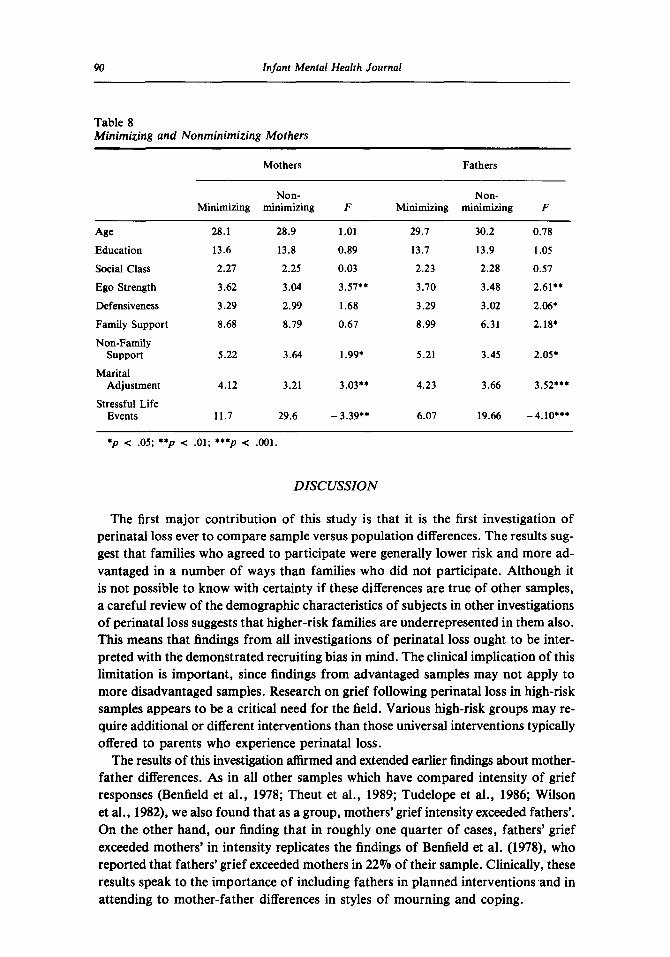
Table 8 presents results of Minimizing mothers and fathers compared to Nonminimiz- ing mothers and fathers on demographic, personality, and social context variables. Although no differences in demographic variables were apparent, results of self-report measures indicate significant differences in how Minimizing and Nonminimizing parents reported on their perceptions of their personalities and social relationships. Higher levels of defensiveness characterized Minimizing fathers but not Minimizing mothers.
90 Infant Mental Health Journal
Table 8 Minimizing and Nonminimizing Mothers
Mothers Fathers
Non- Non- Minimizing minimizing F Minimizing minimizing F
Age Education
Social Class
Ego Strength
Defensiveness
Family Support
Non-Family Support
Marital Adjustment
Stressful Life Events
28.1
13.6
2.27
3.62
3.29
8.68
5.22
4.12
11.7
28.9
13.8
2.25
3.04
2.99
8.79
3.64
3.21
29.6
1.01
0.89
0.03
3.57..
1.68
0.67
1.99.
3.03**
- 3.39**
29.7
13.7
2.23
3.70
3.29
8.99
5.21
4.23
6.07
30.2
13.9
2.28
3.48
3.02
6.31
3.45
3.66
19.66
0.78
1.05
0.57
2.61..
2.06.
2.18*
2.05.
3.52***
-4.10***
DISCUSSION
The first major contribution of this study is that it is the first investigation of perinatal loss ever to compare sample versus population differences. The results sug- gest that families who agreed to participate were generally lower risk and more ad- vantaged in a number of ways than families who did not participate. Although it is not possible to know with certainty if these differences are true of other samples, a careful review of the demographic characteristics of subjects in other investigations of perinatal loss suggests that higher-risk families are underrepresented in them also. This means that findings from all investigations of perinatal loss ought to be inter- preted with the demonstrated recruiting bias in mind. The clinical implication of this limitation is important, since findings from advantaged samples may not apply to more disadvantaged samples. Research on grief following perinatal loss in high-risk samples appears to be a critical need for the field. Various high-risk groups may re- quire additional or different interventions than those universal interventions typically offered to parents who experience perinatal loss.
The results of this investigation affirmed and extended earlier findings about mother- father differences. As in all other samples which have compared intensity of grief responses (Benfield et al., 1978; Theut et al., 1989; Tudelope et al., 1986; Wilson et al., 1982), we also found that as a group, mothers’ grief intensity exceeded fathers’. On the other hand, our finding that in roughly one quarter of cases, fathers’ grief exceeded mothers’ in intensity replicates the findings of Benfield et al. (1978), who reported that fathers’ grief exceeded mothers in 22% of their sample. Clinically, these results speak to the importance of including fathers in planned interventions ,and in attending to mother-father differences in styles of mourning and coping.
C. H. Zeanah, B . Dank, L. Hirshberg, and L. Dietz 91
Individual differences revealed somewhat different patterns of correlates of inten- sity of grief in mothers and fathers. Specifically, the personality characteristic of ego strength was the single most important predictor of the intensity of mothers’ grief responses. For fathers, support from family members and perceived stressful life events were also important. These findings are somewhat surprising given the clinical pic- ture of fathers as distant, underinvolved, and/or unaffected following perinatal loss. In fact, several fathers in this investigation talked about the lack of support available to them in contrast to that afforded to their wives or partners. It is interesting to note that defensiveness was the strongest predictor of difficulty coping in fathers, suggesting that fathers in this sample may have had more difficulty acknowledging difficulty coping than intensity of grief or distress. Nevertheless, the limited number of fathers who participated in this investigation reminds us that we can draw no con- clusions about the Nonparticipants, and that the cautions noted earlier about generalizability are even truer of fathers than of mothers.
Overall, personality characteristics were the strongest predictors of intensity of grief for both mothers and fathers. The Ego Strength variable, which purports to measure capacity for delayed gratification, lack of impulsivity, and emotional balance, was the single best predictor of grief responses 2 months after the death of a baby. The exploratory stepwise regression equations which highlighted the importance of this variable should be used to guide hypothesis testing about intensity of grief in future research.
Results also illuminated questions about the relationship between characteristics of the loss and grief intensity, which had had mixed findings in previous studies. The results of the current investigation suggest that when perinatal losses (those occurring between 20 and 44 weeks gestation) are examined, there are no differences in intensity of grief related to stillborn versus liveborn loss, nor any effect of gestational age for mothers or for fathers.
Another important finding in this investigation concerns Minimizers. This group had not been previously studied, although a minimizing style in response to perinatal loss has been noted in a number of clinical reports about perinatal loss (Kennel1 et al., 1970; Lewis, 1976, 1979). There are differing possible interpretations of their responses. It is possible that their more favorable ratings of their grief responses, their personality characteristics, their social support, and their experiencing of stressful events are indications that they are a well-adapted group who are coping well, hav- ing more desirable individual and social resources. In support of this interpretation is that mothers in the Minimizer group were not more defensive on the Ego Strength Scale. Another interpretation of the Minimizer group is that their responses are defen- sive and potentially indicative of the “prolonged absence of conscious grieving” (p. 138) pattern of disordered mourning described by Bowlby (1980). In support of this inter- pretation is the extremely low scores on the BDI and all other measures of grief only 2 months following the death of their child, and the fathers’ significantly more minimiz- ing responses on the Ego Strength Scale. The failure of mothers to be significantly different on the Ego Strength Scale measure of defensiveness could be explained as a failure of that measure to capture a defensiveness that is more specific to loss by a mother, or at least the loss of her baby, rather than a general personality style of defensiveness. This minimizing group is reminiscent of a group of mothers described
92 Infant Mental Health Journal
by Field and colleagues (Field et al., 1991) who scored zero on the BDI in the post- partum period. In that study, the zero BDI group interacted less optimally with their infants than did mothers who had even significantly elevated BDI scores.
We suggest that either explanation may be true for certain parents. The challenge for researchers and clinicians is the reliable and valid identification of healthy and unhealthy minimizers. Put another way, when parents are minimizing their affective responses following the loss of their baby, the question is when does the response indicate an adaptive coping style rather than mourning that is not progressing towards healthy resolution?
A response bias that reflects a minimizing style, of course, is only one possible distortion of responses in data derived from single informants, using self-report measures. Nevertheless, when what is of interest involves the individual’s own sub- jective experience and feelings, the self-report method is an important and valued source of data. The inclusion of interview data in future investigations would over- come the problem of shared method variance when multiple questionnaires are used, but even this would not overcome the problem of the lone informant.
Other limitations of the investigation are also evident. Despite the fact that the sample in this study was larger than in most previous investigations, its size was not as large as we would have liked, particularly for fathers. In addition to the impor- tant selection bias issues noted previously, there are also limitations of power with analyses involving fathers that larger samples may help to address. More important, this investigation focused somewhat narrowly on self-reported intensity of grief, which is only one aspect of the process of mourning. It is important that future research on perinatal loss attempt to grapple more fully with some of the complexities of the biological, behavioral, and social responses of bereaved parents. In addition, the initial adaptations of mothers and fathers that we described may become even more mean- ingful and revealing when they are considered longitudinally.
Much remains to be learned about the responses of families following perinatal losses. Future research should build upon these and other findings with longitudinal designs and other means of assessing mourning. Especially important will be follow- ups that address the effects of parents’ grief on surviving and subsequently born children.
REFERENCES
Beck, A. T., Steer, R. A., & Garbin, M. G. (1988). Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review, 8, 77-100.
Beck, A. T., Ward, C. H., Mendelsohn, M., Mock, J. E., & Erbaugh, J . (1961). An inventory for measur- ing depression. Archives of General Psychiatry, 4 , 561-571.
Elenfield, D. G., Leib, S. A., & Vollman, J . H. (1978). Grief response of parents to neonatal death and parent participation in deciding care. Pediatrics, 62, 171-177.
Boukydis, C. F. Z., Lester, B., &Hoffman, J . (1989). Parenting and social support: Network for parents of preterm and fullterm infants. In C. F. Z. Boukydis (Ed.), Research on support for parents and infants in the postnatal period (pp. 61-83). Norwood, NJ: Ablex.
Bowlby, J . (1980). Loss. New York: Basic Books. Epstein, S., & O’Brien, E. J . (1982). Ego Strength Scale. Unpublished manuscript. University of
Massachusetts, Amherst, Massachusetts.

C. ff. Zeanah, B. Dank, L. ffirshberg, and L. Dieiz 93
Field, T., Morrow, C., Healy, B., Foster, T., Adlestein, D., & Goldstein S. (1991). Mothers with zero Beck depression scores act more "depressed" with their infants. Development & Psychopathology,
Goldbach, K. R. C., Dunn, D. S., Toedter, L. J., & Lasker, J. N. (1991). The effects of gestational age and gender on grief after pregnancy loss. American Journal of Orthopsychiatry, 61, 461-467.
Kennel], J. H., Slyter, H., & Klaus, M. H. (1970). The mourning response of parents to the death of a newborn infant. New England Journal of Medicine, 283, 344-349.
LaRoche, C., Lalinec-Michaud, M., Engelsmann, F., Fuller, N., Copp, M., McQuade-Soldatos, P., & Azima, R. (1984). Grief reactions to perinatal death-A follow-up study. Canadian Journal of Psychiatry, 29, 14-19.
Leon, I. (1992). The psychoanalytic conceptualization of perinatal loss: A multidimensional model. American Journal of Psychiatry, 149, 1464-1472.
Lewis, E. (1976). The management of stillbirth: Coping with an unreality. Lancet, 2, 619-620. Lewis, E. (1979). Mourning by the family after stillbirth or neonatal death. Archives of Diseases of
Childhood, 54, 303-306. Osterweis, M., Solomon, F., & Green, M. (1987). Bereavement reactions, consequences and care. In
Biopsychosocial aspects of bereavement. Washington, DC: American Psychiatric Association. Peppers, L., & Knapp, R. J. (1980). Maternal reactions to involuntary fetalhnfant death. Psychiatry,
43, 155-159. Potvin, L., Lasker, J., & Toedter, L. (1989). Measuring grief: A short version of the Perinatal Grief
Scale. Journal of Psychopathology and Behavioral Assessment, 2, 29-45. Rowe, J., Clyman, R., Green, C., Mikkelson, C., Haight, J., & Ataide, L. (1978). Follow-up of families
who experience a perinatal death. Pediatrics, 62, 166-170. Sarason, I. G., Johnson, J. H., & Siege], J. M. (1978). Assessing the impact of life changes: Develop-
ment of the Life Experiences Survey. Journal of Consulting and Clinical Psychology. 46, 932-946. Sanders, C. M., Mauger, P. A., & Strong, P. N. (1979). Manual for the Grief Experience Inventory.
Unpublished manuscript. Sacred Heart College, Belmont, California. Spanier, G. B. (1976). Measuring dyadic adjustment: New scales for assessing the quality of marriage
and similar dyads. Journal of Marriage and the Family, 38, 15-20. Theut, S. K., Pederson, F. A., Zaslow, M. J., Cain, R. L., Rabinovich, B. A., & Morihisa, J. M.
(1989). Perinatal loss and parental bereavement. American Journal of Psychiatry, 146, 635-639. Toedter, L., Lasker, J., & Aldaheff, J. M. (1988). The Perinatal Grief Scale: Development and initial
validation. American Journal of Orthopsychiatry, 58, 435-449. Tudelope, D. I., Iredell, J., Rodgers, D., & Gunn, A. (1986). Neonatal death: Grieving families. Medical
Journal of Australia, 144, 290-292. Wilson, A. L., Fenton, L. J., Stevens, D. C., & Soule, D. J. (1982). The death of a newborn twin: An
analysis of parental bereavement. Pediatrics, 70, 587-591. Zeanah, C. H. (1989). Adaptation following perinatal loss: A critical review. Journal of the American
Academy of Child and Adolescent Psychiatry, 28, 467-480. Zeanah, C. H., Dailey, J., Rosenblatt, M. J., & Saller, N. (1993). Do women grieve following termina-
tion of pregnancy for fetal anomalies? A controlled investigation. Obstetrics and Gynecology, 82,
3, 253-262.
270-275.





























