Embed Size (px)
Citation preview

í.nAfí V , "" CONFERENCE PROCEEDINGS
THE 24™ DAYS OF ŔÁDIÄTI0N PRQTECTIpNJASNÁ POD ČHOPKpMi SÍQVÄKÍA
NOVEMBER 2óV 29, 2001
, 35 5 / * 5

Slovak Society of Nuclear Medicine and Radiation Hygiene(member of IRPA)
Czech Society for Radiation Protection(member of IRPA)
Institute of Preventive and Clinical Medicine, BratislavaNuclear Regulatory Authority of the Slovak Republic
Bohunice NPP, a.s., Jaslovské BohuniceState Institute of Public Health, Banská Bystrica
XXIV. DAYS OF RADIATIONPROTECTION
conference proceedings
November 26-29,2001 Demänovská dolina,Low Tatras, Slovak Republic
ISBN 80-88806-26-27

Slovak Society of Nuclear Medicine and Radiation Hygiene (member of IRPA)Czech Society for Radiation Protection (member of IRPA)Institute of Preventive and Clinical Medicine, Bratislava
Nuclear Regulatory Authority of the Slovak RepublicBohunice NPP, a.s., Jaslovské Bohunice
State Institute of Public Health, Banská Bystrica
Scientific committeeMUDr. Pavol AdámekIng. Jana DrábováIng. Jozef HuttaDoc. MUDr. Izabella Makaiová, CSc.RNDr. Denisa Nikodémova, CSc.RNDr. Josef Thomas, CSc.
Programme and organising committeeIng. Ľudmila AuxtováRNDr. Helena Cabáneková, Ph.D.Ing. Ľubomír DobišJitka GondováOľga MlynárovaEva Rýdza
Conference sponsorsCanberra Packard, s.r.o.VF s.r.o.Slovenské elektrárne, a.s.Úrad jadrového dozoru SRHUMA-LAB Apeco s.r.o.METEX CZ s.r.o.HEINEKEN Slovensko a.s.HEBEL Pórobetón Šaštín s.r.o.
THE EDITIONAL BOARD IS NOT RESPONSIBLE FOR THE CONTENT OF PAPERS, AS WELLAS FOR UNCORRECT ENGLISH TRANSLATION

PLEASE BE AWARE THATALL OF THE MISSING PAGES IN THIS DOCUMENT
WERE ORIGINALLY BLANK

C O N T E N T S
DOSIMETRIC AND MICRODOSIMETRIC APPROACH FOR THE ESTIMATIONOF RADON-INDUCED DAMAGES IN HUMAN LUNGS 9
Radoslav Bôhm, Denisa Nikodémova, Karol Holý
ATHMOSPHERIC RADIONUCLIDE DEPOSITS BIOMONITORING IN THENEIGHBOURHOOD OF NPP TEMELÍN IN THE YEAR 2000 13
Tomáš Čechák, Jaroslav Klusoň, Markéta Smejkalová, Lenka Thinová, Tomáš Trojek
NEW LEARNS AND NEW METHODS IN RADON DIAGNOSTICS 17Tomáš Čechák, Ladislav Moučka, Aleš Froňka, Karel Jílek
RADIATION PROTECTION IN BOHUNICE NPP 19Ľubomír Dobiš
IMPLEMENTATION OF PRE-OPERATIONAL VERSION OF RODOSIN SLOVAKIA 23
Tatiana Ďúranová
STUDIES OF ADSORPTION AND DESORPTION OF ZINC IONS ON ZEOLITESBY MEANS OF 6 5 ZN 27
M.Fôldesová, P.Dillinger, P.Lukáč
THE CASES OF INTERNAL CONTAMINATION WITH24 AM 32Štěpánka Foltánová, Irena Malátová, Věra Bečková, Radim Filgas
EXAMPLE OF USE OF QUANTITATIVE OPTIMIZATION OF RADIATIONPROTECTION IN OPERATION OF V-1 NPP 36
Marek Futas
RADIATION PROTECTION IN PET COMPLEX FOR PRODUCTION, RESEARCHAND UTILIZATION OF RADIOPHARMACEUTICALS 40
M.Fulop, A.Furiová, J.Malysák, J.Ďúran, J.Krišliak, F.Macásek, D.Nikodémová, K.Holý
ENVIRONMENTAL EFFECT OF PET COMPLEX EMISSION TO AIR 44M.Fulop, J.Ďúran, I.Gomola
48RADIOISOTOPES OF THE U, TH, PU, AM IN THE MUSHROOMS
D.Galanda, Ľ.Mátel
EXTERNAL AUDITS OF THERAPEUTIC PHOTON BEAMS IN NONREFERENCECONDITIONS. MAILED DOSIMETRY CHECKS WITH THE EC MULTIPURPOSEPHANTOM 49
Igor Gomola, Dominique Huyskens, Andrée Dutreix
QUALITY CONTROL OF RADIOTHERAPY CENTRES IN THE SLOVAKREPUBLIC: A DOSIMETRY INTERCOM?ARISON OF PHOTON AND ELECTRONBEAMS UNDER REFERENCE CONDITIONS 53
Igor Gomola, Gabriel Králik, Jan Van Dam, Viera Laginová
THE INFORMATION SYSTEM ON OCCUPATIONAL EXPOSURE ANDRELATED IAEA ACTIVITIES IN THE EUROPE REGION 57
Monica Gustafsson
FOUR-YEARS EXPERIENCE WITH MONITORING OF PERSONS AT THETREATMENT OF CHIDLREN PATIENTS WITH NEUROBLASTOMABY 13!I-MIBG COMBINATION WITH HYPERBARIC OXYGEN THERAPY .. 61
Jindřiška Heřmanská, Jaroslav Zimák, Hana Křížová, Zuzana Pásková

DETECTION SYSTEM FOR CONTINUOUS 2 2 2RN MONITORING IN WATERS 65Karol Holý, Eleonóra Patschová, Oľga Holá, Ivana Bosá, Anna Polášková
TEMPORAL VARIABILITY OF SOME RADON CHARACTERISTICSOF THE SOIL 68
Karol Holý, Anežka Ridziková, Anna Polášková, Tomas Stanys, Ivana Bosá, Oľga Holá
POSSIBLE RADIATION DOSE REDUCTION BY USING DIGITAL X-RAYEQUIPMENTS 78
Martina Horváthova, Denisa Nikodémova, Mariana Príkazská
DIAGNOSTIC REFERENCE LEVELS (DRLS) FOR RADIOPHARMACEUTICALSADMINISTERED IN NUCLEAR MEDICINE - FOUR - YEAR EXPERIENCEWITH THEIR USE .' 82
Václav Husák, Pavel Koranda, Zuzana Pásková, Karla Petrová, Zdeněk Prouza
COMPARISON OF VENTILATION MEASUREMENT TECHNIQUESIN REAL CONDITIONS 86
Karel Jílek, Ladislav Tomášek
DISCHARGE RADIONUCLIDES INTO THE ENVIRONMENT IN DIAMOS.P.-O.Z.GEAM DOLNÍ ROZINKA, O.Z. SUL 87
Miroslav Jurda, Jana Šeflová
PROGRAM "SVAZEK" FOR OPTIMISATION OF RADIATION PROTECTIONAT SHIELDING BARRIERS FOR X-RAY WORKPLACES 91
Martin Kadlec, Otto Kodl, Marcela Žákova
CONTRIBUTION TO THE PENETRATION OF RADIONUCLIDES ACROSSTHE SKIN. AGE DEPENDENCE OF PROMETHIUM THROUGH RAT SKIN INVITRO 93
Zoltán Kassai, Vasil Kopr da, Margita Harangozó, Petra Bendová, Katarína Bauerová
SIMULATION OF THE PHOTON FIELDS AND DOSE DISTRIBUTIONSFOR BRACHYTHERAPY SOURCES 97
J.Klusoň, P.Švihla, T.Čechák
ALARA PRINCIPLE IMPLEMENTATION ON THE TEMELÍN NPP 100Petr Koláček, Jaroslav Hak, Jiří Vokálek
ANALYSIS OF THE MORTALITY DEVELOPMENT OF THE POPULATIONIN THE SURROUNDINGS OF BOHUNICE NPP USING THE FUZZY LOGICMETHODS 103
Mária Letkovičová, Beáta Stehlíková, Martin Ďurov
STATISTICAL SURVEY OF THE CONSUMPTION OF THE PRODUCTS FROMSEMINATURAL ENVIRONMENT IN THE CZECH REPUBLIC 108
Irena Malátová, Josef Tecl
ADVANCED SEPARATION TECHNIQUES IN RADIOCHEMICAL ANALYSISOF ENVIRONMENTAL SAMPLES 112
Ľ.Mátel, P.Rajec, O.Rosskopfová
ACTUAL TRENDS IN PATIENT DOSE REDUCTION IN RADIODIAGNOSTIC 113Denisa Nikodémova, Igor Gomola, Martina Horváthova
DETERMINATION OF ABSORBED DOSE IN THE EXPERIMENTAL ANIMALIRRADIATED ON THE LEKSELL GAMMA KNIFE 121
Josef Novotný Jr., Josef Novotný, Václav Spěv áček, Pavel Dvořák, Tomáš Čechák, Román Liščák,Gustav Brožek, Jaroslav Tintěra, Josef Vymazal

DETERMINATION OF ALPHA RADIONUCLIDES IN FISH 1 2 5L.Pernická, Ľ.Mátel, O.Rosskopfová
THE SYSTEM OF REGISTRATION AND EVALUATION OF HIGHEROCCUPATIONAL DOSES IN THE CZECH REPUBLIC THE ANALYSISAND RESULTS 126
Karla Petrová
THE USE OF GEL DOSIMETER OF FRICKE TYPE IN THREE-DIMENSIONALDOSIMETRY 129
V.Spěváček, P.Dvořák, J.Novotný, T.Čechákml, M.Marek
AIRCREW RADIATION DOSIMETRY - LAST DEVELOPMENT 133František Spurný
SEMICONDUCTOR SPECTROMETER FOR RADIATION PROTECTIONFrantišek Spurný, Cvetan Dačev
MONITORING OF CARBON 14 IN ATMOSPHERIC CARBON DIOXIDE 141I.Světlík, V.Michálek, P.Rulík, L.Tomášková
AEROSOLS RADIOACTIVITY IN THE BRATISLAVA ATMOSPHERE 145I.Sýkora, M. Chudý, L.Ďurana, K.Holý, J.Merešová
TGF-BETA AND APOPTOSIS - RAT MODEL OF RADIATION PNEUMONITIS 148J.Škopek, J.Ůsterreicher, L.Navrátil, M.Králik, J.Vávrová, J.Knížek, A.Macela
SOIL-TO-PLANT TRANSFER FACTORS FOR RADIOCAESIUM MEASUREDIN DIFFERENT SOIL TYPES IN THE CZECH REPUBLIC 149
Josef Ted, Reza Mirchi, Irena Malátová, Vlasta Pešková, Eva Schlesingerová
EFFECTIVE DOSE ESTIMATION FROM THE Hp(10) VALUE MEASUREDBY FILM OR TL DOSEMETER LOCATED ABOVE THE LEAD APRON INMEDICAL DIAGNOSTIC AND INTERVENTION RADIOLOGY 152
Jaroslav Trousil, Jiří Plichta, Karla Petrová
NEW DEVELOPMENTS OF CZECH PERSONNEL NEUTRON DOSEMETERAND ITS APPLICATION 153
Jaroslav Trousil, František Spurný, Miroslav Králík, Zdeněk Zelenka
STATE METROLOGICAL CENTRE 157Magdaléna Vičanová
DETERMINATION OF 2 1 0PB IN WATER SAMPLES BY LIQUID SCINTILATIONSPECTROMETRY 161
Marta Vršková, Katarína Sedláčková
COLLECTIVE AND INDIVIDUAL EFFECTIVE DOSES IN DUKOVANY NPPDURING 1996-2000 166
Zdeněk Zelenka
QUALITY AUDITS OF THE REMOTE-CONTROLLED AUTOMATICALLY-DRIVEN GAMMA RAY AFTERLOADING EQUIPMENT USED INBRACHYTHERAPY IN THE CZECH REPUBLIC 167
Helena Žáčkova, Ivana Horáková

SK02K0165
PREFACE
The Organizing and Scientific Committee of the XXIV. Days of Radiation Protection,following the previous practice, submit to you the Proceedings of oral papers and postersintended to be presented during the meeting in Jasná. The meeting is supported by exhibitionswhich are regarded as an important integral part of the overal scientific programme.
Publication of the Proceedings in advance of the Conference has the advantage to givethe informations for the better discussion of the work, as well as, for immediate reference to theradiation protection community.
On behalf of organizing institutions we extend a very warm welcome to all participantsand sincere appreciation for participation in this important conference. We hope, that thepossibility to exchange the opinions of the specialists in the given topics will accelerate theimplementation of the new trends in radiation protection into the routine practice and improvethe future development in radiation protection.
We will take the oportunity to thank also to our colleaugues from abroad for theirvaluable contribution to the scientific level of our meeting.
The last revision of the Slovak Act on the Protection of Human Health(No.470/2000Coll.) had improved the national system of control in radiation protection andimplemented also the recommendations of the international organisations, as well as of theDirectives of European Commission. Supplemented by the New Regulations on Requrementsfor ensuring the Radiation Protection (No. 12/2001 Coll.) they lay down the measures ofkeeping the exposures of individuals to ionizing radiation as low as possible.
Despite of these, there are still many open radiation protection questions, which need tobe discussed and we hope that some of them will be during our meeting successfuly solved.
Finály we are sure that the nice environment of Low Tatras will also contribute to yourpleasant participation at XXIV. Days of Radiation Protection.
We would like to thank all members of the organizing and scientific committee forexcelent work during the conference preparation, the Slovak Medical Association for thesupport and colaboration, as well as all sponsoring organisations and exhibitors.
Denisa NikodémovaVicepresident of the IRPA associated Slovak Soc.
of Nuclear medcine and Radiation Hygiena

DOSIMETRIC AND MICRODOSIMETRIC APPROACH FOR THEESTIMATION OF RADON - INDUCED DAMAGES IN HUMAN
LUNGS.
Radoslav Bohm (1), Denisa Nikodémova (2), Karol Holý(1)
Faculty of Mathematics, Physics and Informatics of Comenius University, Mlynskádolina F I, 842 48 Bratislava, Slovak Republic, (2)Institute of Preventive & Clinical
Medicine, Limbová 14, 833 01 Bratislava, Slovak Republic
IntroductionExposure to radon is a well-documented cause of lung cancer among underground
miners, especially those who worked in uranium mines, where the radon was present in highconcentrations. While 222Rn is a gas, it decays with a half-life of 3.82 days into series of solidshort-lived radionuclides that are collectively referred as radon progeny, among which 214Po and
Po emit alpha particles during their decay. If the emission occurs after the radon progeny hasbeen inhaled and deposited within the lung, it may cause damage to the cells lining the airwaysand give rise to a malignant change.
The basal and secretory cells, located at the depth of 10-50 (im are assumed to be themost probable target cells from which lung cancer originates. Alpha particles emitted during thedecay of 214Po and 2I8Po have the range of 48 to 71pim and could damage these cells. For theestimation of radiation risk we can use dosimetric and microdosimetric approach.
Materials and methodsa. Dosimetric approach
The risk of occurrence of bronchial carcinomas following the inhalation of short-lived radondecay products is predominantly related to the concentration of the alpha particles, as well as totheir spatial distribution from the target cells. The total surface area activities of Rn progeny inthe different bronchial airways are determined by the aerosol deposition, radioactive decay,clearence of deposited nuclides through mucociliary action and absorption into the blood. Asthe Rn progeny concentrations cannot be at present directly measured, various modelingassumptions were made. In our work, the ICRP66 lung model [1] was applied. This modelallows calculation of the alpha particle distribution in a model structure of the lung tissue (inmucus layer, sol layer and particles sequestered by macrophages in the lamina propria).Our calculations were focused particularly onthe alpha particles distribution in the bronchial andbronchional region (BB, bb) because the results of recently provided epidemiological research[2] show the predominant occurence of bronchial carcinoma in this part of lungs.
To obtain radiation risk we supposed that the underground and home atmospherecharacteristics as they are given in Table 1,2
Table 1. Parameters of the aerosols in home (mine) atmosphere.
Description of parameter
FractionAerosol size (nm)DispersonHygroscopic growth factorunattached fractionradon to daughter ratio222Rn/218Po/2I4Pb/2MBi(214Po)
Mode
Unattached
1000.9(1.1)1.3(1.5)1.0(1.5)
AttachedNucleation | Accumulation28502.01.5
70 (100)250 (25012.0 (1.3)1.5 (1.5)
Coarse215001.51.5
fA(ZUiPo)=0.04, fB(zl4Pb)=0.004 (fA(^18Po)=0.35, fBf"4Pb)=0.035)1/0.61/0.29/0.21 (1/0.9/0.6/0.4)
XXIV DRO Demänovská dolina
SK02K0166

The estimation of the equivalent dose using parameters of the Table 1 is in thefollowing equation:
HAIAA1 0)where Hx is the equivalent dose to region X and Ax is the assigned fraction of w-r. For aheterogeneous radiation field, the quality factor Q, is usually estimated in terms of linealenergy y:
Q = — \Q(y)d(y)dy (2)
where d(y) is the normalised probability density of dose in lineal energy y. Again Q(y) is anempiricaly determined factor. We use the function QT [3] shown in Fig. exhibit the same
general feature as the function recommended inIGRU Report 40. The differences between thecurve at high y values turn out to be highlysignificant for the radon problem. Themicrodosimetric spectra d;(y) applied in Eq. 2were calculat by Monte Carlo method. In ourcalculations, 2 types of target nuclei depthdistributions were considered:• homogeneousfl] with basal cells locateduniformly in the depth of 35-50 jam andsecretory cells in 10-40 jj.m depth;• heterogeneous [4], with secretory nucleiremaining nearly constant in the depth of 20-50um, where the nuclei of basal cells have asignificant maximum between 40 and 50 jam.
10y [keV/|im]
Fig. 1 Weighting function Q. The QT
histogram is based the data [3] for oncogenictransformation in C3H 10T1/2 cells. TheQICRP curve is from ICRU Report 40.
b. microdosimetric approachThe microdosimetric approach to the problem of lung cancer risk estimation offers a
theoretical background for the interpretation of relations between the dose and the effects ofradiation. The interaction of alpha particles with target cells of lung tissue was simulated byMonte Carlo method. The starting position of alpha particles emitted during the decay of 214Poand 218Po was generated by generator of random numbers according to the particle distributiongiven by using ICRP66 lung model [1]. The target nuclei of bronchial epithelium wererepresented by spheres of 5 um diameter.
Energy deposition in the tissue and in the air gap as calculated by the Bethe-Blochequation [5,6]. We followed the fiuence rate spectra, as well as the microdosimetric spectra ofLET and the distribution of cells with a specific energy zo, greater than the boundary value of0.65 Gy, the so called glancing cells. These microdosimetric data are useful as input tobiological model of radon carcinogenesis. There are no corresponding experimental dataavailable on biological radiation effects in human epithelial bronchial cells, therefore the resultsof radiological experiments with cell lines (C3H10T1/2, V79) in vitro geometries were used inour calculations. Experimental survival data indicate that the response of human bronchialepithelial cells may be similar to those reported for a variety of cell lines [7], In the paper thefollowing microdosimetric models have been applied:• Track structure model [8] describes biological effects of charged particles using 4
radiosensitive cell parameters [9]:. These parameters of radiosensitivity can be obtainedfrom radiobiological in vitro studies [7].
• Model of threshold specific energy based on the assumption that the biological effect (e.g.the inactivation of cells) at a dose D will occur after exceeding a threshold value of specificenergy z0 in the target [10]
XXIV DRO Demänovská dolina 10

• State vector model, based on the assumption that the target cells must pass through 6distinct transitions in order to yield a fatal tumor [11]. These transitions are schematicallyshown in the Fig. 4. Transition rate constants given as the fraction of cells undergoing thetransition per unit time are explicit functions of the radiation dose rate.
• LET model - spectrum of alpha particles in cells is in this model are considered to be theparameter for the cell damage determination.
• Bystander effect model is incorporated a radiobiological bystander response, superimposedon a direct response due to the direct energy deposition in the cell nuclei. [12].
ResultsThe quality factor Q for Bronchial and Bronchional region were calculated according to theEq.2. Our results are summarised in Tab 3. We can see that quality factors of 20-25 for radonprogeny used currently may be too large. Our estimates are in the range of 13-18 in BB regionand 20 in the bb region. Based on the depth distribution factor Q (fig.2) we calculatedequivalent dose H in both region BB and bb.
Tab. 3 Quality Factor in the bronchial an bronchional region.
Position
all cellssecretory cells (BB)secretory cells (bb)basal cells
Quality Factor Q-Bronchial region BB, Bronchional bbC3H10T1/2
homogeneousdistribution
16.0216.7219.0912.70
heterogeneousdistribution
14.1113.2019.2616.20
ICRPhomogeneousdistribution
25.0726.3325.5125.29
heterogeneousdistribution
25.6425.4119.2626.32
I ' i ' I ' I ' I ' I ' I • I ' I ' I
0 5 10 15 2 0 2 5 3 0 3 5 4 0 4 5 5 0 5 5 6 0 6 5 7 0
Heterogeneous distributionHomopjncous distribution
10 20 30* 40
Fig. 2 Quality Factor Q and equivalent dose H for bronchiol and bronchional region.
The probabilities of biological effects were calculated for target cells as the functionof depth for different cumulative exposures.. These dependences were for all modelsapproximatly of the same shape. We present therefore in Fig 3 only the results obtained withstate vector model, giving the best agreement with the epidemilogical data.
We tried to correlate H(depth) factor and transformation probabilities T(depth) atdifferent exposures as H =a + fJT . The values of a and P as well as correlation parameter Rare presented in Table 3. It is obvious from Table 3 that the parameter R moves in homogeneousdistribution arround 0.9 but in homogeneus distribution is very small. Presented material is asource to our wide future research.
Conclusion• The factors quality of 20-25 for radon progeny used currently may be too large. Our
estimates are in the range of 13-18 in BB region and 20 in the bb region.• The homogeneous distribution of target nuclei depth dose underestimates the real
radiation risk, particularly in deeper locations.
XXIV DRO Demänovská dolina 11

The correlates H(depth) with the results of transformation probabilities at differentexposures quite well in case of homogeneous distribution target cells.
Table 4. The correlation coefficients obtained by linear regressionExpozícia
[WLM]
50100200300400500600700
homoA
-0.0,14±0,03-0,22±0,06-0,14±0,12-0,57±0,16-0,71+0,16-0,76±0,13-0,8+0,11
-0,74+0,08
geneous distributionB
0,25±0,021,49+0,010,77±0,130,55±0,100,44+0,070,34+0,040,2810,030,22+0,02
R0.980.960.920.910.930.950.970.98
heterogeneous distributionA
0,03±0,010,03±0,01_j0,04+0,010,04+0,010,04±0,010,05+0,010,05+0,010,05±0,01
B0,342±0,1210,081+0,0440,023±0,0120,011+0,0110,005+0,005O,0O3±0,0030,002±0,0030,002+0,002
R0.770.680.540.440.390.360.340.32
9.0x10'-
8.0x10 s -
7.0x10' -
g 6.0x10'1 "
g 5 .0x10 ' -
Oto 4.0x10 -cní£ 3.0x10"'-
2.0x10"'-
1.0x10°-
Homogeneous distribution—•— so WLM—O— 100 WLM—A—200 WLM—A— 300 WLM—T— 400 WLM—V— 500 WLM—O— 600 WLM
700 WLM
g 8.0X10
O 6.0x10"3
c
-í= 4.0x10 "
10 15 20 25 30 35 40 45 60 55
Heterogeneous distribution
—•— so WLM- O — 100 WLM—A— 200 WLM—A— 300 WLM—T— 400 WLM- V - 5 0 0 WLM—O— 600 WLM—•— 700 WLM
depth him] 10 15 20 25 30 35 40 45 50 55
depth [nm]
Fig. 2 The relative frequency of cell transformation for homogenous and heterogenous distribution ojtarget cells.
References:1. Human Respiratory Tract Model for Radiological Protection, ICRP66, 1994.2. National Research Council (NRC), Comparative Dosimetry Radon in Mines and Homes.
Washington, D.C., 1991.3. Brenner D.J., Miller R.C., Huang Y. The Biological Effectiveness of Radon-Progeny Alpha
Particles. III. Quality Factors., Radiat. Res. 142, 61-69 (1995)4. Mercer, R., Russel, M.L. and Crapo, J.D. Radon dosimetry based on the depth distribution of nuclei
in human and rat lung. Health Phys. 61(1), 117-131 (1991)5. Harley, N.H. Pasternack., B.S. Alpha absorption measurements applied to lung dose from
radon daughters, Health Phys. 23, 771-782 (1972).6. Kraft, G., Krämer, M., Scholz, M. LET, track structure and models, Radiat. Environ.
Biophys. 31, 161-180(1992)7. Hofmann, W. and Heistracher T. Track structure predictions of radon-induced biological
effects in human bronchial epithelium. Environmental International 22, 949-957 (1996).8. Katz, R. and Hofmann, W. Biological effects of low doses of ionizing radiations: particle
tracks in radiobiology. Nuclear Instr. and Meth. 203, 433-442 (1982)9. Katz, R., Zachariah, R., Cucinitta, F.A., Zhang, Ch. Survey of cellular radiosensitivity
parameters, Radiat. Res. 140, 356-365 (1994)10. Sedlák, A. Microdosimetric approach to the problem of lung cancer induced by radon
progeny, Health Phys. 70, 680-688 (1996).11. Crawford-Brown, DJ., Hofman W. Extension of a general state-vector model of radiation
carcinogenesis to consideration of dose rate. Math. Bios. 115, 123-144 (1993).12. Brenner D.J., Little J.B., Sachs R.K. The Bystander Effect in Radiation Oncogenesis: II, A
Quantitative Model, Radiat. Research 155, 402-408 (2001)
XXIV DRO Demänovská dolina 12

ATHMOSPHERIC RADIONUCLIDE DEPOSITSBIOMONITORING IN THE NEIGHBOURHOOD
OF NPP TEMELÍN IN THE YEAR 2000
Tomáš Čechák, Jaroslav Klusoň, Markéta Smejkalová, Lenka Thinová, Tomáš TrojekFJFIČVUT, Břehová 7, Praha 1, 115 19
Biomonitoring was conducted by employees of Czech Technical University (CVUT) inPrague based on requirements of Nuclear Power Plant Temelin.
Monitored area contained 29 sampled locations along eight radial profiles intersectingthe area of interest up to distance of 20 km from NPP Temelin (the measuring points are located2-5-10-20 km from NPP). GPS 45 Garmin measured the location of points. The samples weretaken from forest humus, surface pine bark, Shreber moss, edible mushrooms and forest berries.The pine bark and moss were sampled at the selected sites twice yearly, at spring and fall of2000, forest humus once in spring month of 2000, mushrooms and berries once in a growingseason of 2000. In total 203 samples were collected. For the determination of radionucleidpresence and their activity in samples was selected a method of laboratory gamma spectroscopy.The measuring equipment consists of HPGe detector with built-in preamplifier (mfg. by EG&GOrtec), amplifiers 2022 Canberra, Source VN31060 Canberra, ADC built-in analyzer, analyzermodel 4202 Canberra and PC.
Samples were enclosed in Marinelli containers with a volume of 0.5 I, surroundingduring the measurements coaxial HPG detector. Processing of measured spectra in the range upto 3 MeV provided mass related activity of naturally radioactive elements (4 0K, 2 2 6 Ra, and 2 3 2 Th)and contaminant U 7 C s .
For the elements of interest the following limits of detection were established:1 3 7Cs 2Bq/kg 2 3 6 Ra 10 Bq/kgI 3 4Cs 2 Bq/kg 2 3 2 Th 12 Bq/kg4 0 K 50 Bq/kg
Selected time intervals for sample measurement with 5% relative measurement error:Moss 40 000 - 80 000 secBark 14 000 - 40 000 secForest humus 14 000 secMushrooms 14 000 - 40 000 secBlueberries 40 000 sec
The results were statistically processed and individual results are listed in tables andgraphs (Fig. 1, 2, 3). The groups of measured quantities of mass-activity in Bq/kg (further Ah)are characterized by minimum, maximum, median, average value and standard deviation (fornormal deviation), arithmetic and geometric mean value, geometric standard deviation (forlogarithmic-normal spread). All values have assigned 95% tolerance intervals.
The measurement results confirm that in monitoring of biological plant samples a largerspread of measurement values is normal. For example contents of 13 Cs (resulting from nuclearweapon tests in the fifties of last century and from Černobyl accident fallout) in moss rangefrom 0 - 8 5 Bq/kg (maximum point 26, second maximum 83 Bq/kg point 3) in the spring and3-518 Bq/kg (maximum point 3, second maximum 117 Bq/kg point 26 ) in the fall, even thoughthe median of both points is nearly equal: 19.5 Bq/kg spring and 16 Bq/kg fall. High value of Aj,1 3 7Cs 518 Bq/kg (point 3 - fall) was verified by repeated measurement. Values Ah
1 3 7 C s in mosscorrespond well with content of mushrooms, where maxims Ai, were also measured at point 26and point 3 (5764 Bq/kg and 2182 Bq/kg). Minimum in mushrooms measured at a point 22
XXIV DRO Demänovská dolina 13
•IIISK02K0167

(88 Bq/kg) correspond to moss Aj, values that are among the lowest. The content of 137Cs in pinebark reached in the spring collection values in the range 1 3 - 9 9 Bq/kg, in the fall 11 - 121Bq/kg, median value 46 res. 48 Bq/kg, that confirms agreement among measured data in bothmeasurement periods of the year 2000. The 137Cs reach the bark surface by washing off from thecrowns of trees. It would be interesting to compare the contents of Cs in tree bark withcontents established by SURO in aerosols from the air in given area.
The measured content of 137Cs in blueberries is characterized by median value 40.5Bq/kg with a range 8 - 174 Bq/kg, while maximum was found again on the point number 3. Incase of forest humus the Ah
I37Cs is in range 83 - 736 Bq/kg (maximum point 1) while point 26and point 3 belong to the highest.
Very small values Ah 40K in the pine bark were mostly not reaching detection limits andthus correspond to values cited in literature. In case of moss is noticeable the growth of biomathfrom the spring (range from 0 - 234 Bq/kg, median 109 Bq/kg) until fall (range 63 - 333 Bq/kg,median 195 Bq/kg), that is given by the growth of moss during the season but also by theextreme dryness during the spring of 2000. There is no relation between Ah 40K in mushroomsrange 100 - 1183 Bq/kg (median 983 Bq/kg) and in forest humus with range 0 - 488 Bq/kg(median 118 Bq/kg). Blueberries or Raspberries contained 40K in quantities of 75 - 242 Bq/kgor 75 -351 Bq/kg.
Ah 226Ra and 232Th were above the deteption limits only in the samples of forest humus
where they ranged 0 - 5 1 Bq/kg and 0 - 5 5 Bq/kg.
The biomonitoring for year 2000 included assessment dosimetry and spectrometrycharacteristic of photon-fields (that is determination of reference background) at 15 selectedpoints. Two methods were selected with corresponding types of measurements:
1/ determination of air kerma rate (by direct measurement with device TESLA NB 3201and by calculation based on spectrometry data)
2/ measurement of photon-spectra by use of scintillation spectrometer MCA p. NOMADEG &G Ortec with scintillation detector Nal(Tl) diameter 3" by 3" in the energy range up to3 MeV.
All measurements were conducted in reference altitude 1 meter above surface. Total of99 measurements were conducted using device NB 3201 with integration interval of 100seconds. The spectra during spectrometry measurements were collected for 2700 seconds. Theresults of measurements using both methods are compared in Tab. 1 and Fig. 4. The measuredvalues corresponded to nominal values on natural background, depending mainly of geologicalsubstrata (soil contents), concentration of radon in soil or air etc. The methodology selectedenables identification of individual contaminants and their contribution or occurrence. With theexception of the identified 137Cs it is not possible to identify among the measured spectra anysignificant contribution of any other radionuclides.
XXIV DRO Demänovská dolina 14

Mass-activity 137Cs in the moss
150 n
•spring
-autum
10 15 20
number of point
Fig. 1
Bq/
kgm
ass-
acti
vity
140 -|120 -mn -80 -60 -40 -20 -0 -
c
Mass-activity 137Cs in the
) 5 10 15 20
number of point
pine
25
bark
M*ré
30
• spring—H— autum
Fig. 2
Mass-activily 137Cs in the mushrooms and in the humus
0 humus
B mushrooms
11 16 21
number of point
26
Fig. 3
XXIV DRO Demänovská dolina 15

In-situ monitoring of gamma ray background in reference altitude 1 meter(11.-12.7.2000)
Number of .point
010304060812141617202223252829
Mean
Spectrum
" \ - ; - \ - * • • ' - ' .
15011402050609121116101317-
03' ' • ' ' • , ; ' •
- ' ; / , - dKa/dt, (nGy/hJ,;
.•:, - •••mtíriitorNB3201'Tisla' '•>„ .,.„ total value.
10482
10410710189
12410112991
1451001138689
/ r <f .- >. 104
std[%J/2,22,42,16,52,83,4
1,11,51,82,2
1,12,81,32,22,3
. -ZA,
, spectrum NaI(Tl)3"x3"• • -terrestrial component
906093868671
11388
12174
1328697
-67
Tab. 1
Background in the points of the measurement 11.-12.7.2000
HNB3201HNal(Tl)
01 03 04 06 08 12 14 16 17 20 22 23 25 28 29
Number of point
Fig. 4
XXIV DRO Demänovská dolina 16

NEW LEARNS AND NEW METHODS IN RADON DIAGNOSTICS
Tomáš Čechák*, Ladislav Moučka, Aleš Froňka, Karel JílekStátní ústav radiační ochrany, Šrobárova 48,100 00 Praha 10
* ČVUT Fakulta jaderná a fyzikálně inženýrská, Břehová 7,11519Praha 1
It is well known, that the radon concentration in the certain volume is a result of the twocompetitive processes. The radon supply is a positive factor, while the ventilation causes radonconcentration decrease. As radon supply is concerned, the possible sources are geologicalstructures in the closest house surroundings, building materials, water supplied into the houseand radon released by combustion of the both solid and gaseous fuels. Practical results showthat most important radon sources are the geological structures and infiltration of the soil airinto the house.Dealing with the radon concentrations, it is useful to go into the infiltration and ventilationprocesses. Infiltration and ventilation are driven by stack effect, wind and mechanicalventilators.Neutral levels, see fig. 1, divide the room volume into two parts, the lower one, in which theroom air pressure is lower than outside air pressure and upper one, characteristic by the higherinside pressure an lower outside pressure.
Ventilation^ escapes
/ the house
Neutral level
Outdoor airinfiltrates thehouse
Soil air with radon infiltrates the housethrough the cracks
p0 (h) - outdoor air pressurePi (h) - indoor air pressure
Po(hn)=Pi(hn),p0 (h) > pi (h) pro h< K,p0 (h) < pi (h) pro h >ha,
Fig.l
Ventilation air enters the room through the untightnes at the lower part, below the neutral level,and leaves the room through the leaks situated in the upper levels.Radon supply from the ground soil is determined by the parameters of the cracks, that are incontact with the underground and by the pressure difference at both sides of the crack.
XXIV DRO Demänovská dolina 17
SK02K0168

That is, why methods for ventilation measurement are looked for and why parametersdescribing the radon supply are studied.The most important parameters are the air exchange rate (exchanged air volume per time unit, ornumber of air exchanges in unit time) and strength of the radon supply from the ground soil(usually radon activity per unit time).The air exchange rate is measured using radon as so-called trace gas. Measurement is carriedout with the constant source of radon, or with the short pulse of radon, measuring the timecourse of building up or decay of its activity. As the radon source is used the artificial radonsource, or natural radon source from the soil under the house.Measured radon exchange rates with compared with results acquired carbon monoxide tracegas.Radon supply delivered into the house interior with the soil gas passes through cracks andopenings in building constructions that are in contact with subsoil. Pressure difference betweenthe soil pores and interior of the house (at the floor level) controls the amount of the deliveredsoil gas. That is why the delivered radon activity versus air pressure difference is measured.One example of these measurements is presented in fig.2. The results belong to one of therooms situated on both sides of the central corridor of the one storey house. Timber floor is veryporous what results in very high radon supply.
Radon supplied activity rate versus pressuredifference
2
43
450040003500300025002000150010005000
10 15
Pressure difference [Pa]
20
Fig. 2
The blower doors technology is used and the radon concentration time characteristics areanalyzed and the radon supply is derived.The problem that is to be solved is the analysis of the ventilation processes and estimation ofpressure differences at different ventilation conditions.More actual results will be presented at the conferrence.Comment: To assess the quality of the house from the viewpoint of the mean radonconcentration the model of radon supply as the house parameter was used. Our work shows thatthis assumption is not correct. The value of radon supply is worthless without dates onventilation parameters.
XXIV DRO Demänovská dolina 18

SK02K0169
RADIATION PROTECTION IN BOHUNICE NPPDESCRIPTION OF PRESENT STATUS
Ing. Ľubomír DobišAtómové elektrárne Bohunice, o.z., 91931 Jaslovské Bohunice
1. Introduction
Bohunice NPP operates four units PWR type VVER 440 MW each. The unit first wasput in operation in 1972 and the last one in 1985. Bohunice Nuclear Power Plant is situated insouth - western part of Slovakia about 50 km away from Bratislava and approx. 120 km fromVienna
2. Organizational structure
PLANT DIRECTOR
TECHNICAL SUPPORT AND SAFETY DIVISION
LALARA GROUP SECRETARIAT
DOS1METRY SECTION
RADIATION PROTECTION V1
RADIACTION PROTECTION V2
MAINTENANCE SECTION
ENVIRONMENTAL LABORATORY
RP TECHN.SUPPORT AND CALIBRATION
The radiation protection department has the responsibility to control the radiation safety.It consists of 125 persons, 20 out of them with university degree
The department belongs to the Technical Support and Safety division and the head ofthe RP Department has direct access to the plant director.
3. Modification of RP instrumentation
The safety improvements at nuclear power plants is never ending process. The level ofhuman knowledge pushes the criterion of safety standards to the higher levels. Due to thecontinually updated international standards the new requirements rise and NPPs have toimplement them.
The original Russian design of the both NPPs came from seventies years of 20th century.It corresponded to the safety requirements as well as technical abilities of that time. A processof safety improvement and operation reliability has started immediately after units'commissioning. For example more than 1300 modifications have been implemented at VI NPPbefore 1993 followed later by large reconstruction works (1993 - 2000). Based on the results ofinternational review missions after the reconstruction of VI is obvious that VI NPP met all the
XXIV PRO Demänovská dolina 19

requirements defined by Slovak Nuclear Authority and by IAEA and thus VI NPP reached theinternationally acceptable level of nuclear safety.
The similar situation in the trend of safety improvement can be seen also at V2 but thebasic modernization process has started in this year
The original radiation protection systems at VI and V2 are very comprehensive andimportant measurements are doubled or even tripled (200% redundancy). Nevertheless not allthe monitors fulfilled the required technical parameters or resistance to the accident conditionsand some measurements were even missing.
Several areas for improvement in radiation protection had been recognized by RPexperts at the plant. The modifications of radiation protection systems have been done due tosafety improvements or simply due to the aging of instrumentation.
Table 2: List of main RP modifications
Due to the lack of space the list of main radiation modification will be provided during the oralpresentation
4. Occupational radiation exposure
Table 3: Collective and individual exposure
Collective exposure S [man mSv]Collective exposure
NPP staffcontractorstotal
Average individual exposure E [mSv]Average individual exposure
NPP staffcontractorstotal
Maximum individual exposure E [mSv]Maximum individual exposure
NPP staffcontractorstotal
Numbers of persons with the individualExposure interval
(5 - 10> mSv(10-15>mSv(15 - 20> mSvover 20 mSv
1.-6.VI
month 2001
356,61284,18640,79
1.-6.VI
0,2910,7030,393
1.-6.VI4,355,805,80
V272,5362,62135,15
month 2001V20,0590,1380,080
month 2001V21,634,414,41
exposure within the dose1.-6.month 2001 ,,V-l5000
V-20000
Bohunice NPP429,14346,80775,94
Bohunice NPP0,2740,5670,357
Bohunice NPP5,275,805,80
interval
Bohunice NPP7000
XXIV DRO Demänovská dolina 20

Unexpected events
199910.07 mSv individual dose during the transport of an internal part of reactor.
Due to the non standard situation the transport of the internal part of reactor lastedlonger than it is normal.
The plastic foil sticked to the container that is used for catching water drops from thereactor's internal part caught approx. 10 litre of contaminated water (more than usual) andstarted to loosen itself. Trying to protect the spread of contamination the worker bent himselfand got for 10-15 sec into the field of 1 Sv/h gamma radiation.
The worker was equipped with the legal film dosimeter and digital electronic dosimeter.The worker's annual dose including 10.07 mSv was less than 14 mSv. The work was done bypresence of radiation technician. The usual doses are less than lmSv for such a kind of job.
The root cause was the violation of the plant radiation rules when the operators knowingthe non standard situation did not elaborated the special procedure/program. Such a program hasto be approved by competent persons and contains the measures to solve probable accidentsituations.
2000Exceeding of internal individual dose limit at Unit 4 .
The event happened during the outage at the Unit 4 when the supply firm performed theinternal inspection of the reactor pressurized vessel. Three persons of that firm seriouslyviolated the NPP rules by• putting off the assigned operational personal electronic dosimeters,• entering the rooms without previous approval,• performing the unauthorized works.
One person of them got the month dose 29.48 mSv measured by legal film dosimeter.His total year's dose (obtained in different installations) was 32.66 mSv.
Both events were investigated by plant event committee and adequate correctivemeasures were taken.
5. Public radiation exposure due to the Bohunice NPP
Table 4: Gas and liquid effluentsVInoble gases [TBq]aerosols [MBq]m I [MBq]V2 ,noble gases [TBq]aerosols [MBq]I31I [MBq]
1st quarter1,66967,1782,779
1,3960,9590,510
2nd quarter5,79358,27818,086
2,0442,4720,530
1. - 6.20017,462125,45620,865
3,4393,4321,041
annual limit410018000067500
410018000067500
% of limit0,1820,0700,031
0,0840,0020,002
XXIV DRO Demänovská dolina 21

VIcorrosion andfission elements[MBq]JT [TBq]V2corrosion andfission elements[MBq]3T [TBq]
9,191
2,004
3,436
2,169
12,386
2,593
6,239
3,237
21,576
4,596
9,675
5,407
38000
43,7
38000
43,7
0,057
10,52
0,025
12,37
6. Conclusion
Radiation protection at Bohunice NPP has reached the high international standard. Thefact was approved by several independent international missions (OSART, WANO, WENRA,•••)
A lot of modifications have been done in order to improve the standard of radiationprotection. All the BSS requirements have been implemented into the plant regulations beforethe State Law No 290/1996 and 470/2000 came into the force.
Internal audits are regularly performed at NPP in order to reveal potential deficiencies.In 2001 there were 4 such audits focused on quality assurance, software operation, LBB conceptand limits and condition of safe operation.
State Health Institute, the regulatory body in the radiation protection, performs theinspection at least ones a month. Good relationship with the inspectors of State Health Institutealso contributes to the safe operation of the NPP
There were not any radiation accident. All anomalies or radiation events areinvestigated at a plant level. The results of root cause analysis and proposal of corrective actionsare provided to IAEA and WANO databases for the distribution.
The RP department of Bohunice NPP cooperates with the other Czech and SlovakNPPs. Regular meetings on radiation protection and lately also on emergency preparedness areorganized. The cooperation is excellent.
Occupational exposure is reviewed also with respect of ISOE data. Bohunice NPP (evenwith high dose burden caused by reconstruction of VI NPP) can be found in the first half ofworld PWR speaking about the collective exposure per reactor. V2 NPP itself reaches thelowest collective exposure in the world. All doses are below the limits and kept ALARA.ALARA system has been established already in 1997 at Bohunice NPP and its results areobvious for example looking at dose results during the reconstruction works at VI NPP.
The operation of Bohunice NPP has negligible influence to its surroundings. The valuesof gas and liquid effluents move within percents of annual limits. Results are published inquarter and annual reports and they also are provided to the EC/NEA database. The NEA annualreports are analyzed by plant RP experts providing good feedback to the operation.
The highest annual individual exposure calculated to the member of critical groupmoves in order 10"7Sv every year.
The annual reviews of plant radioactive releases, collective and individual exposure aswell as calculated exposure to the member of critical group in surroundings will be available atthe conference during the oral presentation.
XXIV DRO Demänovská dolina 22

SK02K0170IMPLEMENTATION OF PRE-OPERATIONAL VERSION
OF RODOS IN SLOVAKIA
Tatiana ĎúranováVÚJE Trnava, lne, Okružná 5, 918 64 Trnava
SummaryWith support from the European Commission's ECHO programme "Implementation of
the RODOS Decision Support System for Off-Site Emergency Preparation and response in theEmergency centres in Poland and the Slovak Republic", RODOS was implemented in theSlovak Republic. The main objective of the project which was implemented by the Consortiumof ENCONET and STUK, with participation of VUJE and IAE, was to accelerate theimplementation of the RODOS system within national emergency preparedness arrangements inPoland and the Slovak Republic. The main elements are: procure and install the computerhardware for the RODOS; establish dedicated communication lines; install and adapt RODOSsoftware; test and verify the operability of the whole system; develop and implement proceduresfor the pre-operational integration of RODOS into national emergency arrangements; developand implement maintenance procedures; develop and implement a training programme.
Objectives and Scope of the ProjectThe project ECHO/TPS/B7-219/97/303 "Implementation of RODOS in Poland and in the
Slovak Republic" with focus on the Slovak Republic was sponsored by the EuropeanCommission's ECHO (European Commission Humanitarian Office) within the assistanceprogramme to non EU countries. The implementation of this project was monitored byDirectorate Generals XII of the EC.
The overall objective of the project was to implement RODOS system Ver. 3.13 withinemergency arrangements in Poland and Slovakia.
The aim of the project was to establish RODOS in these two countries so it could be usedwithin emergency arrangements in a "pre-opérational" capacity. This means that it is theresponsibility of countries to, after initial experience has been gained, fully integrate RODOSinto their national emergency arrangements. Specific aim of the project was to establish all pre-conditions from computer hardware and communication links to procedures for normal andemergency operation and training of operators and users for the operation of a national RODOScentre. Within the project, RODOS was to be adapted to country specific local conditions. Forthis, the data collection needed to support that activity was part of the project beneficiaries'activities (i.e. formally separated from Contractor's tasks).
The scope of work performed within this project corresponds with full installation andcommissioning of two RODOS national centres. The scope of work comprised the followingtasks:0 Task 1: Computer hardware, software, and equipment procurement and
installationCommunication lines, design and establishmentSystem software installation and testing of RODOS operationSystem verificationOperating procedures and work plansMaintenance programTraining programme
000000
TaskTaskTaskTaskTaskTask
2:3:4:5:6:7:
XXIV DRO Demänovská dolina 23

Organisation of the ProjectThe project was implemented by an integrated team consisting of a Consortium of two
companies, supported by local sub-contractors. The leader of the Consortium was ENCONETConsulting Ges.m.b.H. from Vienna, Austria. The other Consortium member was STUK, theFinnish Radiation and Safety Authority in Helsinki.
The following local subcontractors were involved:0 VUJE, Trnava, Slovak Republic,0 IAE, Otwock-Swierk, Poland.
ENCONET had overall responsibility for the implementation of the project, includingthe project management. ENCONET was responsible for project tasks 1, 2, 4 and 6.
STUK, Finnish Radiation and Safety Authority shared the project managementresponsibility and was directly responsible for project tasks 3, 5 and 7.
Local subcontractors participated in all tasks in their respective countries, though theirmajor involvement was on verification and testing, as well as on adaptation of operatingprocedures and training to local conditions and needs.
Associated to the project, though not formally part of it, was ForschungszentrumKarlsruhe (FZK) under the separate ECHO contract ECHO/TPS/B7-219/97/0301.
Involved institutions and their role in the Slovak Republic within the project of RODOSimplementation:0 Nuclear Regulatory Authority of the Slovak Republic (NRA SR): National RODOS
Centrea Slovak Centre for Radiation Monitoring (SCRM):
passive userdata supplier - radiation monitoring and measuring systems
0 Nuclear Power Plants Research Institute (VUJE) Trnava:interactive usertechnical support organisation
0 Slovak Hydro-Meteorological Institute (SHMI):passive userdata supplier - real-time meteorological monitoring data, providing access to the nationalradiation monitoring network (NRIS) and to WMO
0 NPP, EBO Jaslovske Bohunice:passive userdata supplier - plant radiation monitoring system, source term data
0 NPP, EMO Mochovce:passive userdata supplier - plant radiation monitoring system, source term data
Tasks summaryComputer hardware, software, and equipment procurement and installation
I. equipment based on a cluster of 2 servers - HP type R 390II. "Service Guard" software - a commercial product from HP for mission-critical
applications which are running at a cluster of servers to allow a full operability of thesystem even in cases of failure of one of the servers or other equipment.
III. HP workstation - VUJEIV. 6 PC - 2x UJD, SURMS, SHMI, EBO, EMO
System software installation and testing of RODOS operation, system verificationFulfilled objective of this task was:
I. to adapt RODOS software to local conditionsII. install RODOSIII. test the operability of RODOS with simulated data in normal operation and
emergenciesIV. to test the whole installation of RODOS in all of its operating modes, including the
communication links
XXIV DRO Demänovská dolina 24

Communication lines, design and establishment
SHMI SCRM NPP EBONATIONAL RODOS CENTRE
NETWORKING (CS)
NPPRINPP EMOWANSDII
(3 x PL# 200U (1+2))
CENTRAL UNITS
ERC
Operating procedures and work plansSTUK proposed the staffing of national RODOS centres. STUK wrote standard working
procedures for each of the activities and staff within national centres. Procedures were preparedfor both normal operation and emergency operation. VUJE has written the procedures fordifferent tasks identified to be necessary for operating RODOS centre. The task relatedapproach in the Nuclear Regulatory Authority of the Slovak Republic fits better into existingemergency preparedness arrangements.
Training programmeThe training courses took place in the offices of the UJD SR:
17.-20.4.2000 Users Training Course2.-5.5.2000 Operators Training Course
Training materials contained:Final Report (English),Transparencies (Slovak),User Guide (Slovak),RODOS Test Concept: Application Software (Slovak)RODOS Test Concept: System SoftwareThe operating procedures developed by VUJE were used for the operators
courseTechnical preparation of courses in the UJD offices:
I. the five X-Terminals were made available for participants:A. one for demonstrations during both coursesB. four for participants of the operators course.
II. the participants of the operators course were divided into four groups (one X-Terminal for two participants). Four experienced specialists from VUJE wereproviding expert support.
Lessons LearnedAlthough never planned to be, this project turned out to be the first one where RODOS
was implemented in an emergency preparedness structure within a CEE country through an ECsponsored technical assistance project. As RODOS could become a standard tool foremergency preparedness in the EU and CEE region lesson learned within this project may be
XXIV DRO Demänovská dolina 25

expected to be a valuable contribution to other similar projects, but also to national projectswhere those are being planed.
Computer hardware and commercial software should be standardised, and should bebased on a cluster of two servers (i.e. HP 9000 series) with commercial mirroring software (i.e.Service Guard). This solution is more expensive than a workstation solution but is assuresstable operation.
After installation of operating system and commercial software, the installation should beextensively tested to assure full operability. For commercial software (like ALLBASE) patcheswhich are known to be needed should be simultaneously installed. Only after this is successfullycompleted, RODOS system should be installed.
Communication links with passive and interactive users and with data providers needs tobe optimised in each case. A solution with leased lines is an expensive one and apparently notcost-justified for passive or interactive users (except when additional development or remotemaintenance is envisaged by an interactive user). In normal (i.e. non-emergency) operationleased lines for data providers are an expensive undertaking. Solution with ISDN-basedguaranteed-call-completion may (currently) be the most cost beneficial way of establishingcommunication links for RODOS, for all users where own dedicated data links are notavailable.
Specialisation of RODOS with country-specific data should be initiated early in a projectand, if possible, completed even before installation of RODOS. One of subcontractors (i.e. theleading subcontractor) in a country shall be an organisation with long experience with RODOS(through participation in EC's research programmes) which should assume the responsibility foradjusting RODOS under FZK's guidance.
Testing of RODOS central unit and remote locations should be done as a single task. Thetesting procedure which was developed by FZK for this project may be retained and adjusted tolocal condition as needed.
Within this project, an outline of training courses and the training material covering basistopics was developed. The training provided was well accepted by users and operators in bothcountries. While this material could be used in the future, it has to be noted that the trainingmaterial needs to be adjusted, in both organisational aspects (who is trained and when) as wellas it contents (to reflect local conditions, organisation of National RODOS centre and thestructure of users). Training in national language also turned out to be important as it assuredfull understanding of all involved. Finally, training for users shall be concise yet informative asit needs to attract high level individuals who are usually members of Emergency commissions.
This project was the first implementation of RODOS in a national emergencypreparedness organisations in Europe. The project confirmed the participants' view on the factthat, on European scale, RODOS could be taken as a joint emergency management tool havingstandardised protocols for presentation and exchange of radiological data in and between thedifferent countries. In a long-term perspective, networking of RODOS with other decisionsupport systems outside Europe would provide better global exchange of data and informationin more harmonised way.
AcknowledgmentsThis work has been carried out with support from the European Commision's ECHO
under contract No. ECHO/TPS/B7-219/97/303.The author wish to acknowledge the great effort of all from an integrated team under the leadership ofENCONET Consulting Ges.m.b.H and STUK as a member of Consortium, supported by VUJE and IAEas a local subcontractors with close co-operation with FZK - RODOS team leader and beneficiaries -NRA SR and NAEA Poland, notably B. Tomic, R. Mustonen, J. Ehrhardt, S. Potempsky, R. Zelazny, M.Jurkowski, E. Metke. The author is very grateful to G. N. Kelly (EC DG XII) and W. Weiss (BfS, D) forsupervision and essential consultations within the project.
XXIV DRO Demänovská dolina 26

STUDIES OF ADSORPTION AND DESORPTION OF ZINC IONSON ZEOLITES BY MEANS OF 65ZN
M. Fôldesová, P. Dillinger, P. LukáčFaculty of Chemical and Food Technology, Slovak University of Technology,
Radlinského 9, SK-812 37 Bratislava, Slovak Republic,E-mail: [email protected]
The uptake of different metals by natural and chemically modified ionexchagers,including zeolites, were studied in order to minimize the contamination of environment withmetals in ionic form. In recent yers considerable attention has been devoted to the studies ofchemically modified zeolites their properties and applications. The used zeolite originated fromthe deposit Nižný Hrabovec, eastern Slovakia (NH) and from deposit of Ukraine (U). Thezeolite from Slovakia is a clinoptilolite /40 - 70%/ type, the zeolite from Ukraine is a mixedmordenite /75%/ and clinoptilolite /25%/ type. A fraction of 1.5 -2.5 mm was separated fromthe grained zeolite by sieving. The sedimentary zeolites, being the siliceous zeolites, shouldexhibit substantial nonselectivity for the divalent cations having a high hydration enthalpy,including zinc (-2026 kJ/g). Zinc is an essential trace element in all-living systems from bacteriato humans. The toxicity of zinc and most of zinc compounds is generally low, however,sometimes industrial and household wastes contain zinc in concentrations, which can beharmful to the environment. The zinc-accompaning impurities, such as cadmium and lead, areof much greater danger. The main source of zinc are waste waters and continuous emission fromthe production and processing of zinc, other nonferrous smelters, from coal power plants andfossil combustion.
The presented zeolites were transformed into a monocation form by treatment withvarious Na salts (Tab.2). Chemical modification considerably extends the application ofzeolites and increases their effectiveness and selectivity mainly for the sorption of multivalentand hydrated cations [1-3]. Chemical treatment of zeolite with aqueous solutions of Na-salts canto change its cation exchange capacity (CEC). Therefore, the CEC values for all mentioned
materials were determined by extracting NH4 cations from the NH4 saturated samples. The
CEC values of zeolites in mmol NH4 /g are given in Table 1.
Table 1. Values of CEC for the zeolites modified with NaOH solution
Concentrations of modifyingNaOH solution [mol/1] 0 0.5 1 2 4 6CEC [mmolNH4
+/g] 1.38 1.68 1.77 1.98 2.2 2.3
The resulting values of CEC were found to be depending on the kind of Na-salt and theconcentration of solution used for the modification of zeolite. In the case of aqueous NaOHsolution the CEC value increases with its increasing concentration. The CEC values of thezeolites modified with 1 or 4 mol/1 solutions of Na2CO3, NaHCO3 and NaCl were found to be in
the range of 1.77 -1.78 mmol NH4+/g. The treatment of zeolite with these solutions lead only to
a partial exchange of cations and the exchange ability of these zeolitic materials is even lowercompared with NaOH treated zeolite.
The static radioexchange method using model radioactive solutions was utilized for thedetermination of the sorption of Zn by the mentioned above zeolitic materials. For this purpose
XXIV DRO Demänovská dolina 27Ulili
SK02K0171

the aqueous solution of 5.10 mol/1 ZnCl2 labelled with Zn was used. The average activity of 14
ml of the labelled solution was 2x10 cpm.The static radioexchange method is as follows: to the individual vessels containing each
15 ml of the labelled zinc solution it was added 50, 100, 150, 200, 250 or 300 mg of Na-zeolites. The mixtures were slowly stirred for period of 24 hours. Then the radioactivity of a 5ml aliquot of each mixture was measured by y-ray spectroscopy with Nal(Tl) detector.
The sorption characteristics - sorption coefficient u., distribution coefficient K_ andsorption capacity F of natural and chemically treated zeolites were calculated. The distributioncoefficient KD can be used as a measure of the ability of materials to remove cations from
solutions. This value is important for the calculation of the separation efficiency of materials. Itis known that the distribution coefficient, in general, depends on the concentration of the cationsin solution as well as on the presence of other competitive cations. The distribution coefficientKD was calculated for the sorption of zinc by the zeolites from the aqueous solution, having the
zinc concentration of 3.33 mg/ml. Sorption characteristics of the zinc uptake by the investigatedzeolites are presented in Tab. 2.
Tab. 2 Sorption characteristics of natural and
chemically modified zeolites
Material
modified with
Nižný Hrabovecnatural (NH)
0.5 mol/1 NaOH
1 mol/1 NaOH2 mol/1 NaOH4 mol/1 NaOH6 mol/1 NaOH
1 mol/1 Na2CO3
1 mol/1 NaHC03
1 moUl NaCl
4 mol/1 NaCl
Ukrainenatural (U)
1 mom NaOH
4 mol/1 NaOH
[mg/g]
2,0
35,536,8
40,384,089,0
41,8
45,8
25,5
35,3
2,4
47,3
51,8
KD
[ml/g]
1,210,9
11,515,642,337,6
16,0
17,7
11,4
13,4
1,419,9
19,6
r[mmol/g]
0,06
0,490,520,68
1,491,36
0,69
0,75
0,51
0,59
0,11
0,83
0,82
The maximal exchange levels were attained as follows: 25-fold increase by usingzeolitic material from Nižný Hrabovec modified with 6 mol/1 NaOH solution, 22-fold increasefor the some zeolite modified with 4 mol/1 NaOH and 16-fold increase by using the zeolite fromUkraine modified with 4 mol/1 NaOH as compared with the unmodified zeolite. 7 - 12-foldincrease was achieved by using zeolite from Nižný Hrabovec modified with mentioned Na-saltsolutions.
It was etablished that the pH is the most important parameter affecting the adsorption.The adsorption of polyvalent metal ions (include zinc ions) from solutions on natural and
XXIV DRO Demänovská dolina 28

chemically modified zeolites is a considerably more complex process and depends in a criticalway on the pH of these solutions. Such ions easily hydrolyze to give a variety of solublecomplex species and, frequently, insoluble hydroxides at rather low pH values. Thus, an increasein pH not only affects the surface of the zeolite but also changes the entire composition of theadsorbate in solution. The zeolites chemically modified with Na-salt solutions change pH aswell. They are able to increase the pH of the solution of cations. The initial pH of ZnCl2 solution
was 4.11 and by the adding any of chemically treated zeolites was increased up 6.5.The sorption of zinc at the select pH 1,2, 3, 4, 5 continuously adjusted during sorption
experiments was studied by static radioexchange method as well (Fig. 1). Tested mixtures in thiscase, were prepared as follows: hydrochloric acid was used to adjust the pH of the model
solution of ZnCl2 labelled with Zn to 1, 2, 3, 4 or 5. The solutions were slowly stirred for 24
hours at room temperature, and the pH of each sample was maintained at its initial value. Theradioactivity of a 5 ml aliquot was measured by Nal(Tl) detector after 24 h.
The effect of the pH of ZnCl2 solution on the sorption of zinc by investigated zeolites is
showed in Fig. 1. The experimental results show that the best sorption of zinc by mentionedzeolites was in the pH range of 3 to 6.5. Chemically treated zeolites spontaneously increase pHof Zn-solutions and this fact can be very advantageous in using the modified zeolites for veryacidic waste waters. The chemically modified zeolites "adjust" the pH of solution to a valuewere the cation sorption is at its maximum.
50
30
1
20
10
NH natural ; ^
NH 4.mol/i NäOH
%H 6-mbl/ÍNäbH:
4 rhol/l Nadri'.i;
pH=1 pH=2 pH=3 pH=5 pH=6,5
Fig. I The effect of pH on the zinc uptake
The leaching of cations and radionuclides from loaded zeolites is an important processthat affects their applicability as barrier materials. The leachability (L) of zinc from the loadedzeolites into water (pH=7), basic (NaOH, pH=12.3) and acidic (HC1, pH=3.5, 2, 1) aqueoussolutions was in the following way: a sample of loaded zeolite was added into each of thesolution and kept there for a period of 7 days at the room temperature. Then the radioactivity ofa 5 ml aliquot was measured by Nal(Tl) detector. The solid material was washed with distilled
XXIV DRO Demänovská doiina 29

water, dried and then its radioactivity measured. The results of the leaching experiments arepresented in Fig. 2 and 3.
n a t u r a l0 . 5 m o l / I N a O H1 m o 1/1 N a O H2 m o l/l N a O Hi m o l/l N a O H6 m o l/l N a O H
Fig. 2 The leachability of zinc from loaded zeolites at various values of pH
E3 U n a t u r a l
U 1 m o l/l N a O H
4 m o l / I N a O H
Ľ J N H 1 m o l / l N a 2 C O 3
• N H 1 i t o l l I N l H C O !
E 5 3 N H 1 m o l / I N a C
K Í N H J m o l / l N a C I
Fig. 3 The leachability of zinc from loaded zeolites at various values of pH
The areas of application of natural zeolites have been well defined. However, their usecan become more efficient after chemical modification. The zeolites acquire new valuableproperties, while retaining their original ones. The obtained results make these materialsexcellent candidates for their potential use for waste water and radioactive waste waterdecontamination.
1. Fôldesová M., Dillinger P., Lukáč P.: Properties of NaOH-treated Slovak zeolitic tuff and itssorption ability towards some cations, In: P.Misaelides et al./eds. /, Natural MicroporousMaterials in Environmental Technology, 303-318, Kluwer Academic Publishers, 19992. Fôldesová M., Dillinger P., Lukáč P.: Sorption and desorption of Fe(III) on natural andchemically modified zeolite, J. of Radioanalytical and Nuclear Chemistry, Vol. 242, No.l, 227-230,1999
XXIV DRO Demänovská dolina 30

3. Fóldesová M., Dillinger P., Lukáč P.: Sorption and desorption of Cr(III) on natural andchemically modified Slovak zeolites, J. of Radioanalytical and Nuclear Chemistry, Vol. 245,No.2, 435-439,2000
XXIV DRO Demänovská dolina 31

THE CASES OF INTERNAL CONTAMINATION WITH 241AM
Štěpánka Foltánová, Irena Malátová, Věra Bečková and Radim FilgasNational Radiation Protection Institute, Šrobárova 48,100 00 Prague, Czech
Republic
AbstractUp to present time, 15 people with intake of 241Am are measured by direct methods and
also their excreta were analysed. Different approaches for the estimation of intake of 241Amwere used. For the direct measurement, method of counting of 241Am in the skull is the usefulone. However, the most sensitive method is excretion analysis.
Committed effective doses estimated from the measurement of skeleton and excreta arecalculated for the workers with old contamination and for the people working with 241Am up tonow. All calculations are performed according to Recommendation ICRP Publication 78.Results of committed effective dose obtained from the excreta and skeleton measurements are ina good agreement with the prediction (except for the case JH).
IntroductionHuman cases with intakes of radionuclides, which occurred long time ago, are unique
sources for the verification or an improvement of biokinetic models. There are few cases withinternal contamination of 241Am in the Czech Republic; some of the individuals are followedsince 1995.
The origin of the highest intake was probably the production of neutron Am-Be sources.However, in the same place, also sources of 241Am for smoke detectors were produced bypowder metallurgy; internal contamination occurred in a few workers, too.
In addition to the old cases that do not work any more with radionuclides, there is agroup of people working with unsealed sources of 2 4 ! Am up to now. Apart from the old internalcontamination new intakes occurred time to time. Monitoring this group is important for theestimation of their dose and improvement of work conditions.
Different approaches for the estimation of intake of 2 4 1 Am were used.For the direct measurement, method of counting of 241Am in the skull (see
Methods
fig. 1) is the sensitive one [1-3]. Retention of ^ A m in the human skeleton is measured usingtwo LEGe detectors placed over temporal region of the skull. Activity in the whole skeleton iscalculated under the assumption of homogeneous distribution of 241Am in the skeleton; skull issupposed to be 15.7 % of the skeleton. Calibration was performed using four different skullphantoms. Introduction of this method for the routine in vivo measurements of the workersmeans that more cases with ^ A m internal contamination were identified than before, whenonly simple whole body counting has been used.
The most sensitive method is excretion analysis [4] which is, of course, quite time -consuming. Alpha-spectrometry of 241Am following radiochemical separation is more sensitivethan direct gamma-spectrometry, but it requires separation of interfering alpha-emitters fromeach other and from matrix constituents in order to produce near massless deposits suitable forhigh-resolution alpha-spectrometry. As a yield monitor 243Am is used. The interpretation ofresults of excretion analysis is much more dependent on the assumed time of intake.
Evaluation of the intake from the measurement in the skeleton is less dependent on thetime of intake (see fig 2). It is not sensitive enough for monitoring of occupational exposure.This method is especially suitable for follow up of cases with old intakes.
When higher inhalation intakes occur (both continuous and single accidental),combination of both approaches - direct measurements in vivo and excretion analysis helps toestimate time of intake and enable to estimate committed effective dose in a realistic way.
XXIV DRO Demänovská dolina 32
HIHISK02K0172

Fig. 1: Measurement of retention of 24IAm in the human skeleton using two LEGe detectors(thickness 15 mm and 20 mm, active area 2000 cm2 each, carbon-epoxy window
of thickness 0.5 mm) placed over temporal region of the skull.
m•t
c0+300X0
• D
0c0c
0
Skeleton
Lungs
Urine
Faeces
1.QQE-05
1.00E-06
1.00E-O7
1.00E-08
1 10 100 1000
Time after intake, d
10000
Fig. 2: Retention and daily excretion following acute inhalation of 241Am (type M)according to ICRP Publication 78
XXIV DRO Demänovská dolina 33

Table 1: Assessment of committed effective doses for old cases241
of internal contamination with Am
Subject
JHPVFK
1
Agein
2001
666665
SŠ T 61HV """PSpp
625569~
Sex
_ M _|MMMMMF
Assumedintake in
197219761987198119801973 J1980 j
E(50) [Sv] using measurement of
skull
5.5 (17)3.0 (4)
0.23 (4)0.20 (4)0.42 (4)•1.18 (2)0.39 (4)
íurine
1.2(27;1.9(72;0.13 (9) _JÔ.Í4 (J)0.32 (7)0.47 (8)0.21 (7)
faeces
1.1 (21)
0.72 (2)0.12 (1)0.52 (3)
-0.16 (3)
These people finished their work with 24IAm many years ago. New occupational exposures areexcluded.(Number of measurement or number of samples is in parenthesis.)
Table 2: Assessment of committed effective doses for workers occupationally exposed to Am
Subject
PH
VP
AH
JV
JK
MV
RZ
BD
Agein
2001
44
48
54
64
58
53
34
58
Sex
M
F
M
M
P
F
M
M
Assumedintake in
1986and 1998
1988and 1998
1988
1988
between 1995and 2000
between 1996and 2000
1996
1998
E(50) [S
skuli
0.21 (8)0.18 (8)
0.01 (6)0.10(6)
0.02 (3)
0.10 (2)
-
0.13 (7)
0.09 (3)
v] using measu
urine
0.05 (5;
0.03 (4)
0.01 (2)
0.06 (2)
0.026 - 0.005(2)
0.003-0.001(2)
0.08 (6)
0.07 (3)
rement of
faeces
-
-
-
241These people work with Am up to now. New intakes are not excluded.(Number of measurement or number of samples is in parenthesis.)
XXIV DRO Demänovská dolina 34

Results and DiscussionThe case JH, contaminated in 1972, is followed for six years already. The intake of
Am in this case is comparable with the intake in case number 102 from The U.S.Transuranium Registry [5]. As the period of measurement covers time 8500 to 11000 days afterthe intake, no decrease of activity in the skeleton and excreta was observed up to now. It is in anagreement with biokinetic model (fig. 2). However in this case excreted fraction is lower thanthe predicted one.
Committed effective doses estimated from the measurement of skeleton and excreta arein tables 1 and 2 for the workers with old contamination and for the people working with 241Amup to now. All committed effective doses are estimated under the assumption of inhalation ofparticles with AMAD = 5 }xm, type M, according to Recommendation ICRP Publication 78.
Generally, results of committed effective dose calculated from excreta measurementsand calculated from skeleton measurements are in a good agreement, the case JH is ratherexceptional.
ConclusionsThe resulting committed effective doses from intake of 241Am are rather high. The
health status of these people will be followed, too.Standard of radiation protection in the workplace producing smoke detectors has to be
improved. There is an effort to introduce sensitive methods for the early detection of intake(measurement in lung).
References• Riihm, W., Kônig, K., Malatova, I., Doerfel, H., Foltanova, S., Sahre, P., Schiitz, R. and
Wahl, W.: Intercomparison Exercise for the Determination of241 Am in the Human Skeleton.Radiat. Prot. Dosim. 79 (1-4) (1998) 517-521.
• Malatova, I., Foltanova, S. and Novotný, T.: Estimation of the 241Am Content in the Skeletonof a Person Contaminated 25 years ago. In: Proc. 6th SRP International Symposium,Southport '99, pp.427-430 (1999).
• Malatova, I. and Foltanova, S.: Uncertainty of the Estimation of241 Am Content of the HumanBody. Radiat. Prot. Dosim. 89 (3-4) (2000) 295-299.
• Dulaiova, H., Beckova, V.: Determination of Americium by Extraction Chromatography inUrine Samples. IRPA Regional Congress on Radiation Protection in Central Europe, August22-27 1999, Budapest, Hungary, ISBN 963 8051 88 4, pp.492-495.
• The U.S. Transuranium Registry Report on the 24IAm Content of a Whole Body, HelthPhysics 49, (4), (1986), 556-676.
XXIV DRO Demänovská dolina 35

EXAMPLE OF USE OF QUANTITATIVE OPTIMIZATIONOF RADIATION PROTECTION IN OPERATION OF V-l NPP
Marek FutasVÚJE Trnava, a.s., Okružná S, 918 64 Trnava
The contemporary system of radiological protection for practices is based on the threefundamental principles: justification of practices, optimisation of protection and limitation ofindividual doses [1]. Once a practice has been justified and adopted, it is necessary to ensurethat exposure to ionising radiation is kept as low as reasonably achievable (ALARA), economicand social factors being taken into account. During past two decades the ALARA procedureshave been implemented also in the work management in Slovak nuclear facilities.
There are a number of decision-aiding techniques available for use within the ALARAprocedure. However, use of these quantitative techniques in work management of our nuclearpower plants was rather questionable due to the absence of monetary value for objective healthdetriment. This standard reference value (known variously as the alpha value or the cost ofmansievert) expresses how much should be spent to reduce or save unit collective dose. Until2001 there were no alpha values established in the Slovak republic either by the regulatoryauthorities or internally by organisations. Recommendations concerning the alpha value camewith the amendments of our radiation protection legislation [2], where a system of alpha valueswas introduced reflecting the aspect of aversion to increasing individual doses. As can be seenfrom Table 1 different alpha values are assigned to unit collective dose depending on the rangeof individual occupational doses comprising this collective dose.
Table 1: Alpha values according to Slovak radiation protection legislation [2j
Alpha value
[Sk/man.mSv]
< 2
2 000
Individual occupational dose
2 - 5
5 000
5-15
15 000
range [mSv]
15-30
20 000
30-50
25 000
NPP V-l operates two VVER 440/230 units and of numerous troubles that afflict PWRsteam generators the plant encounters also erosion damage to the feedwater distribution piping.It was decided therefore to replace the feedwater pipes gradually during regular outages. Thisprogramme has started at steam generator 26 during recent outage of Unit 2 (September -October 2001). It was clear from the very beginning of job planning process that all of theALARA trigger levels would be exceeded and the ALARA procedure was carried out. Simplequantitative tool of radiation protection optimisation (cost - benefit analysis) was used withinthe procedure in order to assess the optimum level of personnel protection. All available optionswith different levels of radiation protection were identified, namely
1. zero protection option,
2. temporary shielding (single layer of lead sheets (3 mm thick) installed inside the steamgenerator),
3. doubled temporary shielding (two layers of lead sheets installed),
4. chemical decontamination of the steam generator (with no additional shielding),
XXTV DRO Demänovská dolina 36
SK02K0173

5. chemical decontamination and temporary shielding and
6. chemical decontamination and doubled temporary shielding.
Having identified feasible radiation protection options, relevant factors whichdistinguish between these options were recognised and quantified for each option. Consideredfactors derive from two main groups - costs of protection (direct capital costs - lead shielding,decontamination fluids and operational costs - radwaste treatment and disposal) and radiationdoses (individual doses and collective doses). The cost of labour was not considered here as thetotal volume of work carried out by contractor was the same for all options and subsidiaryworks (shielding installation, decontamination) were performed by the plant maintenance. Bothcollective and individual doses were estimated from historical records of dose ratemeasurements inside the steam generators and records of achieved decontamination factorvalues.
Comparison of options and selection of optimum one was achieved by means of cost -benefit analysis. This technique defines the best or optimum solution as the option thatminimises the overall cost, i.e. the total of the financial costs and the costs of health detriment.The cost of health detriment is obtained by multiplying the monetary value of unit collectivedose (alpha value) by corresponding collective dose. Results of this analysis are illustrated ingraphic form in Figure 1.
Figure 1: Cost - benefit analysis for feedwater distribution piping replacement (assumingdose rate in steam generator 7 mSv/h)
oo5o
14 000 000
12 000 000
10 000 000
8 000 000
6 000 000
4 000 000
2 000 000
0
H Financial Equivalent ofCollective Dose
D Cost of Protection
\ '
Radiation Protection Option
It is clear from the figure that under assumed conditions the optimum radiation protectionoption is the option with the highest level of protection (chemical decontamination with doubledadditional shielding). However there is no doubt that the actual dose rate in the steam generatoris a crucial factor which can dominate the total cost and thus selection of optimum solution.Therefore it was decided to conduct sensitivity analysis in order to check the robustness of thechosen solution. Table 2 and Figure 2 show the impact of changing the dose rate value (forbetter clarity options 1 and 2 were omitted in Figure 2).
XXIV DRO Demänovská dolina 37

Table 2: Sensitivity
[mSv/h]
12345679111315
analysis 1
Deco +2 x P b
14291 4571 4861 5141 5421 57115992 2752 4232 5722 721
1475920374829263718Í6 a
171" :898a;624a
35ta; !
11111
22223
o the value
Deco -f1 xPb337 485372 828408 171443 513478 856a;:5Í4-199a-::
204 742403 999603 256802 513001 771
of dose rate in steam generatorTotal cost of option [SKK]
Deco
1 249 102rl:29:l302a:';
i"384;702a
2 085 1022 220 3022 355 5022 625 9022 896 3023 166 7023 437 102
2 x P b
; 1 248 553a
1 992 1852 735 8184 500 418
5 473 642b 'c
6446 867b>c
7 420 0 9 1 M
11535 467b;c
13 941 100b'c
> ,t',< 'A.-, >:-'
I x P b
1 402 6462 398 9314 462 1035 779 817°7 097 53 T10 446 417°
12O85 5 6 0 M
15 363 846blC
V'^í'"* '"'%
''ý,
No
14591114
\ V
ŕ
protection
657 800010 400810 400°513 000L
763 000c
013 000°yz-'% r> ľ
Optimum optionb) Not feasible option - numerous workforce requiredc) Option leading to individual doses exceeding 20 mSv(l) Not feasible option - individual doses exceeding 50 mSv
Figure 2: Results of sensitivity analysis to dose rate variation
wO
h-
4 000 000 -]
3 500 000
3 000 000 -
2 500 000 -
2 000 000 -
1 500 000 -
1 000 000 -
, /
/* 9í
' / ..4.V1 _L~~sp*—ft. ^-»
u
^ ~
s^
-•—Deco + 2 x Pb
~H~-Deco + 1 x Pb
A Deco
-o—2x Pb
4 8 12
Dose Rate in SG [mSv/h]
16
Results shown in Table 2 suggest that for dose rates of 5 mSv/h or higher solutions 1 to 3are not feasible as they lead either to cumulative individual doses exceeding dose limits(workers of contractor) or to enormous demands on workforce (over 30 workers of maintenanceassuming dose constraints raised to 2 mSv). Options leading to cumulative individual doses(workers of contractor) higher than 20 mSv are also indicated. Even more important feature isthe fact that below dose rates of 7 mSv/h the optimum option changes depending on the value ofdose rate. These changes cover almost whole range of available radiation protection options -from option with the most stringent level of protection to option with no decontamination.Conducted sensitivity analysis showed clearly that no radiation protection option should be
XXIV DRO Demänovská dolina 38

adopted before measurement of the actual dose rate. On the basis of these results the ALARAcommittee decided not to make any firm decision concerning the level of radiation protectionuntil the steam generator is opened and values of dose rate are acquired. Consequentlymeasurements inside the steam generator 26 were carried out at the beginning of outage whichlead to decision to adopt appropriate option of radiation protection.
[1] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, 1990Recommendations of the International Commission on Radiological Protection, ICRPPublication 60, Annals of the ICRP 21 (1-3), ICRP, 1991.
[2] Vyhláška MZ SR č. 12/2001 Z. z. o požiadavkách na zabezpečenie radiačnej ochrany.
XXIV DRO Demänovská dolina 39

RADIATION PROTECTION IN PET COMPLEX FORPRODUCTION, RESEARCH AND UTILIZATION OF
RADIOPHARMACEUTICALS
M. FiilôpV, A. Furiová2), J. Malysák3), J. Ďúran4), J. Krištiak5), F. Macášek6),
D. Nikodémova1*, K. Holý7)
Vstav preventívnej a klinickej medicíny, Limbová ulica, Bratislava'Onkologický ústav sv.Alžbety, Heydukova ulica, Bratislava
3>VF, a.s., Černá HoraVýskumný ústav jadrových elektrární, Trnava
5)Fyzikálny ústav SAV, Dúbravská cesta6)Prírodovedecká fakulta UK, Mlynská dolina, Bratislava
^Matematicko fyzikálna fakulta UK, Mlynská dolina, Bratislava
AbstractPET complex for production, research and utilization of radiopharmaceuticals is being built inreconstructed building I of Slovak Institute of Metrology (SMU). PET complex consists of threetechnological units. The first one is cyclotron' with beams of 18 MeV protons and 9 MeVdeuterons for production of positron emitters. In the second technological unit the positronemitters are synthesized into form of radiopharmaceuticals for positron emission tomography.The third technological part of PET complex is department of nuclear medicine with camera forpositron emission tomography.
Radiation protection and safety in the PET complex are solved on base of the law No.470/2000and the Recommendation No. 12/2001Requirements of radiation protection in PET complex can be divided into six fundamental parts:1. Specification of sources of ionizing radiation2. Technical description of connection between technological systems3. Radiation protection of working areas of PET complex4. Control and safety system5. Influence of PET complex on environment6. Evaluation of the radiological and economic consequences of decommissioning cyclotron
Radiačná ochrana a bezpečnosť sú v projekte riešené v zmysle zákona NR SRč.470/2000 Z.z., ktorým sa mení a dopĺňa zákon NR SR č.272/1994 Z.z. o ochrane zdravia ľudív znení zákona NR SR č.222/1996 Z.z., zákona NR SR č.290/1996 Z.z. a zákona č.95/2000 Z.z.Princípy radiačnej ochrany a bezpečnosti sú uplatnené tak, aby boli zohľadnené smerné hodnotya postupy na preukázanie racionálne dosiahnuteľnej úrovne radiačnej ochrany podľa §4Vyhlášky MZ SR č.12/2001. Zabezpečenie požiadaviek radiačnej ochrany a bezpečnosti jev projektovej dokumentácii rozdelené na päť základných častí:1. Špecifikácia zdrojov ionizujúceho žiarenia:- Produkcia pozitronových rádionuklidov.- Laboratória výroby PET rádioizotopov a rádiofarmák.- Pracovisko nukleárnej medicíny.- Pozitronová emisná tomografia.- Pracovisko jednofotónovej emisnej tomografie.2. Popis priestorov v PET komplexe.3. Riešenie radiačnej ochrany priestorov PET komplexu- Výpočet ochranného tienenia kobky cyklotrónu pred neutrónmi.- Výpočet ochranného tienenia kobky cyklotrónu pomocou koeficientov prechodu neutrónovéhožiarenia vrstvami betónu.- Výpočet ochranného tienenia kobky cyklotrónu Monte Carlo kódom MCNP.- Výpočet ochranného tienenia pred gama žiarením.
XXIV DRO Demänovská dolina 40
IIISK02K0174

- Popis činnosti najviac exponovaných pracovníkov podľa pobytu v jednotlivých miestnostiachnukleárnej medicíny.- Prechody technologických rozvodov cez ochranné tienenia zdrojov ionizujúceho žiarenia.
- Indukovaná rádioaktivita v kobke cyklotrónu.- Indukovaná rádioaktivita v konštrukcii cyklotrónu.- Aktivita rádionuklidov v betónovom tienení kobky cyklotrónu.- Príkon dávkového ekvivalentu v kobke cyklotrónu pri vypnutom zväzku.- Aktivácia vzduchu v kobke cyklotrónu.- Príkon úväzku efektívnej dávky vdychovaním rádionuklidov v kobke cyklotrónu po vypnutízväzku.- Optimalizácia radiačnej ochrany v kobke cyklotrónu a efektívna dávka pracovníkov obsluhy ariadenia cyklotrónu.- Optimalizácia radiačnej ochrany v kobke cyklotrónu.- Cesty zníženia ožiarenia personálu gama žiarením emitovaným 24Na.- Cena opatrení na zlepšenie radiačnej ochrany v kobke cyklotrónu.- Analýza vzťahu ceny opatrení radiačnej ochrany a úžitku.- Preukázanie racionálne dosiahnuteľnej úrovne radiačnej ochrany.- Efektívna dávka pracovníkov obsluhy a riadenia cyklotrónu po optimalizácii radiačnej ochranyv kobke cyklotrónu.- Efektívna dávka personálu pri výrobe a výskume rádionuklidov a rádiofarmák.- Efektívna dávka personálu na nukleárnej medicíne.- Úväzok efektívnej dávky z príjmu rádioaktívnych látok personálu na nukleárnej medicíne.- Počet výmen vzduchu v priestoroch s pacientmi nukleárnej medicíny.- Počet výmen vzduchu v priestoroch PET.- Počet výmen vzduchu v priestoroch SPECT.- Úväzok efektívnej dávky z príjmu rádionuklidov dýchaním pracovníkov nukleárnej medicíny.- Optimalizácia radiačnej ochrany nukleárnej medicíny.- Optimalizácia radiačnej ochrany pri práci s pacientmi.- Cesty zníženia ožiarenia personálu nukleárnej medicíny.- Cena opatrení na zlepšenie radiačnej ochrany nukleárnej medicíny.- Analýza vzťahu ceny opatrení radiačnej ochrany a úžitku.- Preukázanie racionálne dosiahnuteľnej úrovne radiačnej ochrany.- Efektívna dávka a kolektívny dávkový ekvivalent pracovníkov nukleárnej medicíny.- Zhodnotenie ožiarenia pracovníkov PET komplexu.4. Systém radiačnej kontroly:- Legislatívne požiadavky.- Zhrnutie parametrov a požiadaviek na technické prostriedky systému radiačnej kontroly.- Informačný systém radiačnej kontroly (ISRK).- Monitorovanie technologických uzlov.- Monitorovací systém radiačnej kontroly (MSRK).- Monitorovanie napájania technologických zariadení dôležitých z hľadiska radiačnej ochrany.- Monitorovanie technológie výroby RA látok.- Monitorovanie systému klimatizácie v systéme RK.- Monitorovanie pracoviska pomocou autonómnych prístrojov.- Meradlá pre bežné prevádzkové merania.- Laboratórne meradlá.- Meradlá pre havarijné účely.- RK okolia PET komplexu.- Osobné monitorovanie v PET komplexe.- Monitorovanie vstupu do priestorov v KP v systéme RK.- RK vypustí komplexu.- Archivácia skutočností dôležitých v radiačnej ochrane (ASDRO).- Dozimetrické zariadenia stacionárneho systému radiačnej kontroly.5. Vplyv prevádzky v PET komplexe na životné prostredie:
XXIV DRO Demänovská dolina 41

- Kritická skupina obyvateľstva.- Externé ožiarenie jednotlivca z kritickej skupiny obyvateľstva.- Ožiarenie jednotlivca z kritickej skupiny obyvateľstva od neutrónov a gama žiareniaprenikajúcim cez ochranné tienenie kobky cyklotrónu.- Ožiarenie obyvateľstva gama žiarením, prenikajúcim cez ochranné tienenia PET komplexuv objekte I.- Ožiarenie obyvateľstva gama žiarením rádionuklidov po aktivácii pôdy neutrónmi,prenikajúcimi cez ochranné tienenia kobky cyklotrónu.- Ožiarenie obyvateľstva gama žiarením pri prevoze rádiofarmák cez územie dotknutej oblasti.- Vnútorné ožiarenie jednotlivca z kritickej skupiny obyvateľstva.- Vnútorné ožiarenie jednotlivca kritickej skupiny obyvateľov vdychovaním rádionuklidov.- Zdroje plynných rádionuklidov.- Približný výpočet ožiarenia obyvateľa pozitronovými rádionukiidmi 1 8 F z ventilácie PETkomplexu.- Matematický model šírenia rádionuklidov ovzduším v lokalite areálu SMÚ- Vnútorné ožiarenie jednotlivca z kritickej skupiny obyvateľstva príjmom rádionukíidov ztekutých rádioaktívnych odpadov.- Aktivita rádionuklidov v spodnej vode okolo kobky cyklotrónu.- Vplyv uvoľňovaných tekutých rádioaktívnych odpadov na ožiarenie jednotlivca kritickejskupiny obyvateľov.- Vplyv pevných rádioaktívnych odpadov PET komplexu na ožiarenie jednotlivca kritickejskupiny obyvateľov.- Zhodnotenie vonkajšieho a vnútorného ožiarenia obyvateľstva počas bežnej prevádzky.- Zhodnotenie vonkajšieho a vnútorného ožiarenia obyvateľstva počas predvídateľnýchodchýlok od bežnej prevádzky (havárie).- Predvídateľné havárie pri výrobe a využití rádiofarmák.- Určenie množstva rádionuklidu prenikajúceho do životného prostredia v dôsledku havárie.- Ožiarenie obyvateľstva pri havarijnom úniku rádionukiidov ventiláciou z PET komplexu doživotného prostredia.- Preukázanie racionálne dosiahnuteľnej úrovne radiačnej ochrany obyvateľov dotknutej oblasti.- Porovnanie ožiarenia obyvateľstva v okolí PET komplexu v areáli SMU s experimentálnymimeraniami v okolí PET komplexu v Amsterdame.
Zhodnotenie ožiarenia pracovníkov PET komplexuRiešenie radiačnej ochrana v PET komplexe zaručuje neprekročenie limitov ožiarenia
pracovníkov so zdrojmi ionizujúceho žiarenia. Smerná hodnota efektívnej dávky nie jeprekročená u väčšiny pracovníkov PET komplexu.
Preukázalo sa, že v priestoroch kobky cyklotrónu a v priestoroch rádiochemickejvýroby rádiofarmák, kontrole kvality a výskumu rádiofarmák je úroveň radiačnej ochranyracionálne dosiahnutá v zmysle znenia čl.3, §4, Vyhlášky č. 12/2001.
Na oddelení nukleárnej medicíny u 13 pracovníkov so zdrojmi ionizujúceho žiareniahodnota efektívnej dávky presahuje smernú hodnotu 1 mSv v kalendárnom roku.
Optimalizačné výpočty preukázali, že úroveň radiačnej ochrany v priestorochnukleárnej medicíny je racionálne dosiahnutá v zmysle znenia čl.4, §4, Vyhlášky č. 12/2001.
Hodnoty efektívnej dávky v kalendárnom roku u najviac ožiarenej skupiny zdravotnýchsestier sú o 40% nižšie ako je priemerný ročný limit efektívnej dávky pracovníkov so zdrojmiionizujúceho žiarenia, ktorý je uvedený vo Vyhláške č. 12/2001.
Zhodnotenie ožiarenia obyvateľstva na okolí PET komplexuV žiadnej lokalite celej dotknutej oblasti, v ktorej je definovaná kritická skupina obyvateľstvaefektívna dávka jednotlivca, ani kolektívna dávka kritickej skupiny obyvateľstva neprevyšujúsmerné hodnoty podľa ods.2a a 2c §4 Vyhlášky č.12/2001 a to ani v prípade maximálnejpredvídateľnej odchýlky od normálne prevádzky.
XXIV DRO Demänovská dolina 42

Porovnanie ožiarenia obyvateľstva v okolí PET komplexu v areáli SMÚ sexperimentálnymi meraniami v okolí PET komplexu v Amsterdame
Pracovisko výroby a využitia PET rádiofarmák v Amsterdame má podobnéprevádzkové parametre (výroba 45 TBq 1 8 F za rok), je vybavené rovnakou technológiou(inštalovaný cyklotrón Cyclone 18/9) a aj jeho umiestnenie v mestskej aglomerácii (vovzdialenosti 80 m sú obytné domy) je podobné ako pri projektovanom PET komplexev Bratislave. Pri porovnaní obidvoch PET komplexov sa jednotlivé dávkové charakteristikyprepočítali na rovnakú intenzitu zväzkov protónov (pri ožarovaní terčov na produkciu 18F), bezzohľadnenia faktora pobytu T a na rovnakú ročnú produkciu rádionuklidu 1 8F. Porovnanieefektívnych dávok jednotlivca kritickej skupiny obyvateľstva v rôznych miestach okolia PETkomplexov v areáli SMÚ a v Amsterdame sú v nasledujúcej tabuľke.
Parametre porovnaniaPozemok nad kobkou cyklo-trónu prístupný obyvateľstvuEmisia rádionuklidov ventilá-ciou do životného prostredia3)
Gama1'Neutróny
Aktivita I 8 F•£•<—-Ľ'ext'^-t-'int
Priemerná efektívna dávka jednotlivcov v priestoroch,ktoré sú v tesnom susedstve PET komplexov4)
Efektívna dávka obyvateľa5'
Bratislava29 nSvtť'8 nSvh"1
25 GBqr'0,35 ^Svr1
2,7 uSvť1
0,5 uSvr1
Amsterdam67 nSvh"1
4,3-7,9 nSvh"1
1800^2,2 juSvť'11 i^Svť1
2,2 uSvr"!
Priestor nad kobkou, prístupný obyvateľstvu, tab.č.85,2) na rozdiel od Bratislavy v Amsterdame nemajú filtráciu rádioaktívnych plynov na vstupoch doventilácie v horúcich komorách a v laminárnych boxoch,3> hodnoty pre P E T komplex v Bratislave sú z tab.č.89,4) spriemerovaná efektívna dávka gama žiarenia v časti objektu I s pracoviskami S M Ú , v Amsterdame j ev tesnej blízkosti výroby P E T rádiofarmák 6 poschodová administratívna budova, ktorá sa obvodovýmmúrom dotýka objektu s P E T cyklotrónom,5) hodnoty efektívnej dávky sa vzťahujú k vzdialenosti 80m od PET komplexu, pretože v Amsterdame sahodnotila iba efektívna dávka obyvateľa pre domácnosti, ktoré sú najbližšie lokalizované k PETkomplexu (vzdialenosť 80m).
Hodnoty príkonov efektívnej dávky jednotlivcov kritickej skupiny obyvateľovožiarených rôznymi cestami zdrojmi ionizujúceho žiarenia PET komplexu v Bratislave (areálSMÚ) neprevyšujú v sledovaných parametroch ožiarenie jednotlivcov kritickej skupinyobyvateľstva na okolí PET komplexu v Amsterdame. V niektorých parametroch sú významnenižšie, napríklad pri ožiarení obyvateľstva výpusťami plynných rádioaktívnych aerosólova plynov z ventilácie. Je to tým, že v Bratislave bola v rámci optimalizácie radiačnej ochranyobyvateľstva na niektorých technológiách, u ktorých dochádza k emisii rádionuklidov, zavedenáfiltrácia rádioaktívnych plynov na vstupe do ventilácie. Týka sa to ventilácie horúcich komôr navýrobu rádiofarmák a laminárnych boxoch v laboratóriu kontroly rádiofarmák a v laboratóriuvýskumu.
XXIV DRO Demänovská dolina 43

SK02K0175ENVIRONMENTAL EFFECT OF PET COMPLEX EMISSION
TO AIR
M. Fulopl\ J. Ďúran2}, I. Gomola1}
l> Ú stav preventívnej a klinickej medicíny, Limbová ulica, Bratislava2)Výskumný ústav jadrových elektrární, Trnava
ABSTRACTRunning of cyclotron for the production of PET isotopes, production of FDG in radiochemicallaboratory and using of PET and SPECT radiopharmaceuticals for radiodiagnostics can affectthe environment. The production of moderate-en'ergetic protons and subsequent bombarding ofa target material will result in additional radiation in surroundings of cyclotron vault. Theprocess to produce FDG and diagnosis of hospital patients by using radionuclides give rise toemission of air, which can be contaminated with radioactive elements. The research to quantifythe environmental effects of emissions is described.
Plynné, kvapalné aj pevné rádioaktívne odpady sa v PET komplexe produkujú vo všetkýchhlavných prevádzkach : pri ožarovaní terčov na cyklotróne, pri výrobe rádionuklidov arádiofarmák a taktiež aj pri využití rádiofarmák na vyšetrovanie pacientov gama kamerami naPET a SPECT na oddelení nukleárnej medicíny.
Zdroje plynných rádionuklidov
• Kobka cyklotrónuV kobke cyklotrónu vznikajú rádioaktívne plyny aktiváciou vzduchu pri vyvedenom zväzku
protónov v kobke cyklotrónu. Z rádioaktívnych plynov vznikajúcich v kobke cyklotrónu je zhľadiska vplyvu na životné prostredie závažnejší iba 41Ar, ktorý má dostatočné dlhý polčaspremeny, aby difundoval do životného prostredia. Pri jednom behu výroby 1 8 F vznikne v kobkecyklotrónu 12 MBq 41Ar. Projektované sú dva behy výroby 1 8 F denne, preto denná produkciarádioaktívneho plynu 4IAr je 24 GBq.
• Rádiochemické laboratóriaPri procese výroby FDG sú dva kroky, pri ktorých je zvýšené riziko úniku 1 8F. Prvým je
okamžik po výrobe 1 8 F na terči, kedy sa kvapalina s 1 8F transportuje pomocou He cez kapilárydo kontajnera syntetizačného modulu. Pri tomto kroku transportu I 8 F môžu byť úniky ' F dopriestoru horúcej komory. Druhou operáciou výroby FDG, pri ktorej dochádza ku vznikuplynného rádioaktívneho odpadu je vákuové čerpanie modulu. Z celkovej aktivity 1 8 F vplynných rádioaktívnych odpadoch uvoľnených pri transporte a vákuovom čerpaní modulupripadá na vákuovanie modulu asi 83 %. Vákuové pumpy sú cez kompresory prepojené natienené zberné vaky, do ktorých sa čerpaný vzduch zbiera a v nich sa nechá 1 8 F premeniť nazanedbateľnú aktivitu. Priemerné úniky F pri príchode kapilárami do horúcej komory súmenšie ako 0,5%, t.j. 1,1 GBq 1 8 F pri dennej výrobe 220 GBq. Úniky 1 8 F pri príchodekapilárami do horúcej komory sú lokalizované v hermetických komorách, ktoré majú vlastnúfiltráciu. Filtrácia horúcich komôr pozostáva z dvoch stupňov. Prvý stupeň má pre rádioaktívneaerosóly zadržiavací koeficient väčší ako 99,97% a druhý filtračný stupeň pohlcuje rádioaktívneplyny s koeficientom väčším ako 99%. Po filtrácii na výstupe z horúcej komory sa do ventiláciedostáva menej ako 11 MBq 1 8F do ventilácie za deň. Pri kontrole kvality vyrobenýchrádiofarmák v laboratóriu kontroly kvality a vo výskumnom rádiochemickom laboratóriu sadenne spracováva 24 GBq v laminárnych komorách. Pri tejto práci je koeficient prestupu FDGdo vzduchu menší ako 0,001. Laminárne komory sú na vstupe do ventilácie vybavené filtromrádioaktívnych plynov so zadržiavacím koeficientom väčším ako 99%. Do ventilácie sa tak
XXIV DRO Demänovská dolina 44

denne dostáva z kontroly kvality plynný rádioaktívny odpad v množstve 0,24 MBq I 8 F. Celkovopri normálnej prevádzke výroby, kontroly kvality a výskumu radiofarmaka FDG je denne doventilácie odvádzaný plynný rádioaktívny odpad v množstve 11+0,24=11,24 MBq 1 8 F.
• Oddelenie nukleárnej medicínyPlynné rádioaktívne odpady na oddelení nukleárnej medicíny vznikajú pri príprave
injekcie, kedy sa pri odstraňovaní vzduchovej bubliny z objemu injekčnej striekačky vytlačí ajkvapka radiofarmaka, ktorá sa odstráni do vaty. Vata s kvapkou z injekčnej striekačky, sa musíokamžite uložiť do hermeticky uzavretého kontajnera. V tom prípade sa iba 0,003 aktivity 1 8 Fdostane z kvapky do vzduchu. Množstvo I 8 F, ktoré sa týmto spôsobom dostane do ventilácie je.0,011 MBq na jednu podávanú injekciu. Denne sa bude podávať 12 injekcií a predstavuje tomnožstvo 0,13 MBq 1 8F. Významným zdrojom plynných rádioaktívnych odpadov môžu byťpacienti, ktorým boli podané radiofarmaka na PET (FDG, I 5O, 13N a n C). Najväčšie množstvopodávaných rádiofarmák je vo forme FDG. FDG z tela pacienta odchádza výlučne močom akoeficient prestupu FDG z tela pacienta do vzduchu je menší ako 1%. V projektovejdokumentácii používame konzervatívny predpoklad vydychovania 2% aktivity FDG podanejpacientovi. Pri dennom počte 12 pacientov na PET sa do vzduchu uvoľní 12.0,02.370MBq=89MBq za deň a za rok to predstavuje 89.250=22GBq. Druhým významným rádiofarmakotn, zhľadiska podanej aktivity je I SO. Rádiofarmakum s 15O sa podáva pacientovi dvomi spôsobmiinjekciou do žily, alebo priamo nadýcháním. Priemerný počet pacientov vyšetrovanýchplynným, alebo vodným roztokom 15O je jeden pacient za deň. Pri vyšetrovaní pacientvydycháva vzduch do zberného vaku, v ktorom sa ponechá 15O vymrieť. Konzervatívnepredpokladáme, že pri tomto vyšetrení sa z pacienta dostane do vzduchu 50MBq 15O. Pacientmá po odchode z vyšetrenia v sebe ešte zbytky aktivity 15O, ktorú ešte dvadsať minútvydycháva. V priemere po vyšetrení pacient vydýcha priamo do vzduchu 50 MBq Teda privyšetrovaní pacienta plynným rádiofarmakom s 15O vzniká 50+50 MBq plynnéhorádioaktívneho odpadu s t5O.V priemere za rok môže z vyšetrení pomocou ! O dostať zpacientov do vzduchu 100MBqď'.250 d=25GBq. Pri vyšetrovaní pacienta rádiofarmakom s " Cje podávaná aktivita 0,37 GBq. Cesty prechodu aktivity z pacienta do vzduchu sú podobné akopri pacientovi s 15O, len hodnota aktivity " C vo vzduchu bude asi 30 krát menšia, úmernápodanej aktivite. Vyšetrenia pacientov pozitronovými rádiofarmakami s rádionuklidmi "Na Cneprispievajú významne do množstva rádionuklidov v plynných výpustiach PET komplexu,pretože ako podaná aktivita, tak aj počet pacientov sú relatívne malé v porovnaní s vyšetreniamipomocou FDG a 15O.
Využívanie rádiofarmák na SPECT. Všetky plánované radiofarmaka 201Tl, 1 2 3 I, n In,99mTc, 8 1 K r / 8 ! mRb generátor a 6 7Ga na vyšetrenie pacientov gama kamerou na SPECT budú nanukleárnu medicínu dovážané. Z týchto rádiofarmák 201Tl, n l I n a 67Ga, sú vydychovanépacientmi v množstvách menších ako 0,001 z aplikovanej aktivity. Pacienti s aplikovanýmrádiofarmakom označeným ! 2 3 I vydychujú do vzduchu 10% aplikovanej aktivity. Polovicavšetkých pacientov vyšetrovaných v časti nukleárnej medicíny na SPECT sú pacienti s T c .Časť pacientov (v priemere 1 pacient denne) inhaluje rádiofarmakum s 9 9 mTc a vydychujúvzduch do zberných vakov, ktoré sú vyprázdňované cez filter rádioaktívnych plynov sozadržiavacím koeficientom väčším ako 99%. Ostatní pacienti vydychujú do vzduchu nlTc vmnožstve 5% aplikovanej aktivity. Rádioaktívny plyn 81Kr pacient vydychuje do zberného vakua naviac má krátky polčas premeny (13s), preto nemôže mať významnejší vplyv na životnéprostredie. Denne sa tak na oddelení nukleárnej medicíny v priemere dostane do vzduchu40MBq I2: íI (denne 1 pacient s podanou aktivitou 400MBq) a 180MBq 99mTc (6 pacientov dennes podanou aktivitou 6.0,6GBq=3,6GBq). Plynné rádioaktívne odpady vznikajú pri prípraveinjekcie, kedy sa pri odstraňovaní vzduchovej bubliny z objemu injekčnej striekačky vytlačí ajkvapka radiofarmaka, ktorá sa odstráni do vaty. Kvapka na hrote injekčnej striekačky obsahujev priemere množstvo 3% aplikovanej aktivity pacientovi. Vata s kvapkou z injekčnej striekačky,sa musí okamžite uložiť do hermeticky uzavretého kontajnera. V tom prípade sa iba 0,003aktivity radiofarmaka dostane z kvapky do vzduchu. Množstvo rádionuklidu, ktoré sa týmtospôsobom dostane do ventilácie je 0,001.0,03 aplikovanej aktivity pacientovi. Denne to
XXIV DRO Demänovská dolina 45

predstavuje množstvo 0,00 i MBq 201Tl, 0,012MBq m I , 0,002MBq U 1ln, 0,04 MBq 99mTc a0,004MBq 67Ga. Aktivity plynných rádioaktívnych odpadov z priestorov PET komplexuv objekte I a konverzný faktor na hodnotenie príjmu plynných rádionuklidov pre dospeléhočloveka hjnh,a sú v nasledujúcej tabuľke.
Prekur-zoryradio-farmák
>«F1S O 4,
201 npi
l2ilm I n
y y m T cb / G a4 ! Ar
Polčaspreme-ny
110 min123s
20,3 ms72,9 h13,3 h67,3 h
6 h78,3 h1,83 h
hinh.a
[Sv Bq"1]5,9.10-"2,4.10-"2,4.10-"3,9.10-'°6,0.10""2,3.10-10
2,0.10""2,4.10-'°
S.S.IO-'fSvd-'Bq^m3]
. Vstupy
Nukleárnamedicína
0,l5>0,1
0,0040,00004
0,040,00006
0,180,00012
do ventilácie za deň[GBq ď1]Výroba rádionukli-dov a rádiofarmák
0,0111}
0,024-"
Výpuste zkomína zarok3)
[GBq r'1]25251
0,0110
0,01545
0,036
Poznámky :~ výroba J 8F a FDG2) aktivácia vzduchu v kobke PET cyklotrónu, objem 68 m3
' počíta sa 250 pracovných dní v kalendárnom roku4> konverzný faktor na hodnotenie príjmu 15O a "C pre dospelého človeka hjnh,a bol prevzatý zVyhlášky č. 12/2001 pre požitie n C5) faktor prechodu z pacienta do vzduchu podľa je menší ako 1%. V projektovej dokumentácii sapoužil konzervatívny koeficient prechodu aktivity z pacienta do vzduchu 2%
Hodnoty konverzných faktorov na prepočet príjmu rádionuklidov vdychovaním naúväzok efektívnej dávky pre obyvateľov so zdrojmi ionizujúceho žiarenia pre jednotlivérádionuklidy boli prevzaté z Vyhlášky č. 12/2001.
Matematický model šírenia rádionuklidov ovzduším v lokalite areálu SMÚPre výpočet úväzku efektívnej dávky z príjmu rádionuklidov vdychovaním pre
jednotlivca z kritickej skupiny obyvateľstva použil výpočet efektívnej dávky metódou Šíreniaplynných rádioaktívnych odpadov pomocou difúzneho modelu, kedy sa zohľadňujúmeteorologické podmienky v lokalite budúcej stavby PET komplexu.
Bratislava a jej okolie je rozložené na úpätí Malých Karpát, ktoré sú relatívne vysokouorografickou prekážkou a majú dominantný vplyv na pole vetra. Pri prúdení vzduchu častodochádza k obtekaniu Malých Karpát a smer vetra sa mení na severovýchodný. Keby sa nebralado úvahy deformácia poľa vetra pri výpočte šírenia rádionuklidov ovzduším, mohli by vzniknúťveľké chyby v určení kontaminácie životného prostredia, pretože by sa vypočítal malýpríspevok zdroja rádionuklidov práve tam, kde sa oblak rádioaktivity dostane v dôsledkudeformácie poľa vetra. Z týchto dôvodov sa pre reálny výpočet šírenia rádionuklidov využilnestacionárny, trajektorový model znečistenia ovzdušia. Vo výpočte šírenia rádionuklidov vovzduší sa použil diagnostický model poľa vetra. Diagnostický model vetra zohľadňuje vplyvorografíe na rýchlosť a smer pohybu oblaku. V Bratislave sa nachádza niekoľkometeorologických staníc s automatickou registráciou, merania ktorých je pre diagnostickýmodel výpočet poľa vetra veľmi vhodný. Zvlášť dôležité pre výpočet poľa vetra v dotknutejoblasti okolia PET komplexu sú merania meteorologickej stanice, ktorá bola v rámcipredprevádzkového monitorovania okolia PET komplexu zriadená v roku 1999 priamo v areáliSMÚ. Okrem prízemných a aerologických meraní rýchlosti větraje vstupným parametrom údajo nadmorskej výške každého uzlového bodu. Tento údaj sa získava z digitálneho reliéfuSlovenska s krokom lxl km2. Výpočet kontaminácie ovzdušia rádionuklidmi v dotknutej oblastisa robil pomocou celoštátnej metodiky pre výpočet znečistenia ovzdušia zo stacionárnychzdrojov programovým systémom RTARC 4.5 (Real Time Accident Release Consequence). Privýpočtoch sa použil koeficient S, ktorý možno hodnotiť ako krátkodobý imisný limit.
XXIV DRO Demänovská dolina 46

Krátkodobá koncentrácia bola počítaná pri najnepriaznivejších podmienkach, ktoré sa môžuvyskytnúť v Bratislave pre meteosituáciu kategórie 6, rýchlosť vetra 0.1 ms"1 a bez zrážok.Hodnotili sa nasledovné cesty ožiarenia obyvateľa : vonkajšie ožiarenie z oblaku s plynnýmirádioaktívnymi odpadmi, vonkajšie ožiarenie z povrchu zeme kontaminovaného spádmirádionukíidov z oblaku, vnútorné ožiarenie dýchaním rádionuklidov z oblaku s plynnýchrádioaktívnych odpadov a vnútorné ožiarenie dýchaním resuspendovaných rádionuklidov Naobrázku areálu SMÚ a najbližšieho okolia sú nakreslené izodózy efektívnej dávky ožiareniaobyvateľa rádionuklidmi z ventilácie PET komplexu. Izodózy sú v jednotkách nSv a bolipočítané pre územie v okruhu 250 m s krokom 50 m v kalendárnom roku.
* r 1
- " ľ V -7 ' ' '
, ' "/.'•-ir-«- "Z ' -
J
Maximálna hodnota efektívnej dávky zo všetkých ciest ožiarenia obyvateľav dôsledku plynných výpusti ventiláciou PET komplexu dosahuje hodnotu 0,7)J.Sv. Tátohodnota je viac ako 10 krát nižšia ako je smerná hodnota ožiarenia na preukazovanie racionálnedosiahnuteľnej úrovne radiačnej ochrany pri prevádzke PET komplexu podľa ods.2c §4Vyhlášky č.l2/2001.Maximálna hodnota efektívnej dávky zo všetkých ciest ožiarenia obyvateľa v dôsledkuplynných výpustí ventiláciou PET komplexu je viac ako 1000 krát nižšia ako je limit ožiareniaobyvateľstva podľa §6 Vyhlášky č. 12.
XXIV DRO Demänovská dolina 47

SK02K0176RADIOISOTOPES OF THE U, TH, PU, AM
IN THE MUSHROOMS.
D. Galanda, Ľ. MátelDepartment of Nuclear Chemistry, Faculty of Science, Comenius' University,
Mlynská dolina CH — 1, Bratislava, Slovakia
AbstractThe present work is devoted the estimation of the data about radioactive contamination indifferent species of mushrooms with the aim to analyzing the influence of soil properties.Relatively high radioactive nuclides were detected in various mushrooms produced in Europeanmany countries. Mushrooms have a high transfer factor showing a relatively high uptake ofradionuclides from wood and soil from which they grow.
The radioactive plutonium, uranium, thorium and americium was assayed in the driedmushrooms collected in areas of East and West Slovakia in 1998 - 2000, and examined theeffectiveness of this mushroom as a possible indicator of radioactive contamination ofenvironment due to nuclear contamination of biosphere.
Were determined the mushrooms of canes ".Suillus, Leccinum, Baletus, Armillariella,Xerocomus and Craterellus. The mushrooms were dried and prepared by liquide extractionwith Aliquat 336. The samples were measured by á - barrier spectrometry.
The results of specific activity of plutonium, thorium, uranium and americium in themushrooms and the layers of forest litter were summarized. The specific activity of the sampleswith nuclides of uranium content in the interval (2,71+3,07). 10"3 - (3,43±0,36) Bq.kg"1, activityof nuclides of thorium content varied (l,77±l,55).10~3 - (2,98+0,33) Bq.kg"'. Activity ofnuclides of plutonium content varied (4,7±1,67).1O"2 - (2,59±0,23) Bq.kg'1 and activity ofamericium varied (0,106±0,055) - (0,831±0,395) Bq.kg"1.
XXIV DRO Demänovská dolina 48

EXTERNAL AUDITS OF THERAPEUTIC PHOTON BEAMS INNON-REFERENCE CONDITIONS. MAILED DOSIMETRY
CHECKS WITH THE EC MULTIPURPOSE PHANTOM
Igor Gomola1'2*, Dominique Huyskens1 and Andrée Dutreix'University Hospital Gasthuisberg, Radiotherapy Department, Herestraat 49, 3000 Leuven,
Belgium
^Institute of Preventive and Clinical Medicine, Radiation Protection dept. Limbová 14, 833 01Bratislava, Slovak Republic
1. Introduction: The present accuracy required in radiotherapy, involving very often only anarrow gap between unacceptable normal tissue complications and tumour recurrence, requiresa strict quality assurance (QA) programme at the different steps in the radiotherapeutic process.Since quite some years the basic step of beam calibration in reference conditions is subject towell-codified written procedures. A major contribution to this favourable situation comes frompresent dosimetry protocols (NCS 1986, IAEA TRS-277, D?SM 1990, AAPM TG-21).Concomitantly with these protocols a number of national and international quality auditprogrammes with respect to beam calibration have been launched, part of them being based on
on-site visits (Thwaites et al1992) part on postal TLDdosimetry (Izewska et al 2000).However, several errors inradiotherapy have occurred atthe level of clinical dosimetryin spite of a correct beamcalibration in referenceconditions, because much lessclear calculation procedureswere used for the transfer ofdosimetry information from thereference conditions toclinically more relevantconditions. In a recent booklet(Dutreix et al 1997), of the
Figure 1. Schematic of the multipurpose solid phantom (EC-MPP) used in external dosimetry checks of photon beams in non-reference condition s
European Society for Therapeutic Radiology and Oncology (ESTRO), is described a reliablemethod for dosimetric calculation on the central beam axis in non-reference conditions. In orderto assess uncertainties that are more close to clinical situations, including also off-axis positions,a multipurpose solid phantom (EC-MPP) has been designed and tested in a few Europeanradiotherapy centres.
2. Material and methods: The multipurpose solid phantom (EC-MPP) has the possibility toacquire dosimetric information in different clinical conditions with respect to depth, on-axis andoff axis position, skin obliquity and tissue inhomogeneities (Bridier et al 2000, Gomola et al1999).The EC-MPP is made of polystyrene and has a cubic modular structure with a base of 20 x 20cm. It consists of six detachable pieces, the exact dimensions of which are shown in figure 2.
two homogeneous plates (A and D);two complementary plates, 20° oblique parts (B and C);one parallelepiped (E) containing a small air cavity that simulates a natural body air
cavity and a large wood inhomogeneity that simulates a lung tissue (density 0.34 g/cra3).
XXIV DRO Demänovská dolina 49
SK02K0177

Between pieces D and E it is possible tolocate: either the insert with three holes forthe TLD capsules (on the beam axis (M), 2.5cm off-axis to the left (L) and to the right (R)measurements), or the two inserts betweenwhich a film can be sandwiched.2.1. Dosimetry methods: A limited numberof TLDs are irradiated to determine theabsorbed dose on axis and in two off axispoints. The TLD capsules contain LiF powder(PTL 717 from Desmarquest-CEC, France),enriched in 7Li. The TLD powder is read-outwith a PCL3 computer controlled TLD reader(Fimel, France). For insertion into thephantom the powder is contained in opaquecylindrical polyethylene capsules identical tothose used by the IAEA.The films irradiated in the EC-MPP are usedto evaluate relative dose distributions. Kodak
' X-omat V films withdrawn from a single boxwere used to obtain all experimentallymeasured dose distributions per beam in aparticipating centre. This eliminatesdeviations due to film sensitivity variationfrom different boxes. Films were processed
with an automated Agfa Curix 260 unit, scanned using a Vidar VRX-12 densitometer andevaluated with a film densitometry software Poseidon (Precitron, Sweden) running on a PC. Forthe conversion of the optical density distributions to the dose distributions, sensitometric curveswere used to describe the non linear relationship between optical density and dose (Novotný etal 1997).2.3. Dosimetric parameters evaluated with the EC-MPP: Four different mechanical set-upsshown in figure 3. were chosen to investigate seven relevant irradiation conditions described intable 1.
A - polystyrene plate 200 x 200 x 20 mmB - polystyrene block complementary to block CC- polystyrene block tor oblique phantom0 - polystyrene plate 200 x 200 x 30 mmE - polystyrene block 200 x 200 x 100 mm with two holes F and GF - wooden block 40 x 40 x 200 mmG - air hols 20 x 20 x 200 mm
Figure 2.. Draw of the cross section of the EC-MPP. The distances are quoted in mm.
Figure.3. Four set-ups of the phantom used for investigation of seven irradiation modes
XXIV DRO Demänovská dolina 50

Table 1. Irradiation modes investigated with the EC-MPP
EC-MPPSet-upa/bba/ba/ba/b
cd
IDN
12346
57
Irradiation mode
Reference conditionsSquare fieldRectangular fieldWedgeAsymmetric field
Oblique surfaceInhomogeneities
Field size(en"10;15;9 x9 x7 x
15:15;
i x cm)xlOx 15
1515
10
Í 15
c 15
Depth(cm)5/10105/105/105/10
8.310
Off axis points(cm)±2.5, ±4±2.5, ±4, ±6.5±2.5, ±3.5±2.5, ±3.5-1.0.+2.5,+4.0
±2.5, ±4, ±6.5±2.5, ±3, ±3.5
Modification ofprimary beam
--wedgeAsymmetricjaws/blocks--
3.ResuIts: The feasibility study with the EC-MPP was performed at 17 European centres inBelgium, France, Greece, Hungary, Poland, Spain and Sweden. This resulted in a total of 8 fi0Coy-ray beams and 21 X-ray beams with quality index ranging from 0.61 to 0.79. Table 2.summarizes the combination of treatment planning systems and high energy photon beams usedat the radiotherapy departments participating in this study.
Table 2. Summary oftretment planning systems and photon beams checked with the EC-MPP
Photon beam energy
TPS/manufactu r erNominal accelerating potential (MV)60,'Co
10 15 18 20 23 25Total
Target /GE (USA)Cadplan / Varian (USA)Dosigray / Dosigray (France)TMS / Helax (Sweden)Pinnacle /ADAC (USA)Plato / Nucletron (Netherlands)ISIS / Biomed Eng. (France)Mevaplan / Siemens (Germany)Cunningham 2D / "home made"
122
111
1
1
1111
2
1 245321462
Total 7 1 I 1 29
At these centres, irradiations of 285 TLDs and 195 films in 7 different set-ups of the MSP wereperformed. The relative dose distribution measured by film was compared to the dosecalculation for 9 different TPSs in 33 off axis points per beam resulting in a total of 883 off axis
^ 5 3 ľ:d hy film/Off ails dose cutculaU-d hy TPS)
^ Ov o{ O. ^
íM3". * ?•
Mtrasui
if• a
9- £
« K
-+-
• l jl j* ~
J , '<
.03
red dose/ Staled dose
! S i S g ä £
Figure 4. Frequency distribution of the measured to stated dose values obtained at off axis ratios withfilms for all beams, irradiation modes and treatment planning systems investigated, (left picture 4a).Frequency distribution of the results obtained with TLDs parameters is shown on the right picture(4b),N is the number of the checks, m is the mean of the distribution, SD is the standard deviation Min andMax are the minimum and maximum values of the ratios between measured and stated dose.
XXIV DRO Demänovská dolina 51

points (fig4a). The measured and calculated dose values were compared in 7 differentirradiation conditions, for each of the 29 beams. For 285 TLD measurements a mean ratio ofmeasured to stated dose equal to 1.001 was observed with a standard deviation of 2.6% (1SD)for all combinations of energies, planning systems, geometries and measuring points
investigated (fig4b).5.0%
4.0%
'5 3.0
2.0%
as13a
CO
0.0%
Reference conditionsRectangular fieldOblique surface
_.J7|- — Asymmetric field— t — w edged be am
— S q u are field
The results showedlarger deviations in non-
conditionsreference
especiallypoints and
-7 -6 -5 - 3 - 2 - 1 0 1 2
Off-axis position (cm)
Figure 5. The results of the standard deviations observed from the meanof the ratios between measured and stated values of relative doses indifferent irradiation modes.
referencethan inconditions,for off axisfor wedged beams, asshown in figure 4. Thestandard deviation foreach irradiationcondition separately issmaller than 3%, exceptfor the wedged beamswhich show deviationsof 3.5% (1SD). TheKodak XV film wasused to measure therelative dose
distribution in the MSP. From 195 film measurements a total of 883 off-axis values werecompared with the dose distribution obtained from locally applied TPS. The mean value of theoff axis ratios (Film/TPS) is 1.002 with a standard deviation of 2.6% (1SD) and a maximumdeviation of 18 % in all off axis points (N=33) investigated. The results show differencesbetween the film and TPS derived profiles as a function of TPS and of irradiation geometries ofthe MSPConclusions: The present study indicates that the mailed multipurpose solid phantom is a usefultool to check the dose calculation of treatment planning systems, because a large number ofdosimetric parameters per beam can be checked. Part of this work was supported by the ECNetwork project Europe against Cancer, DG V.
References:Bridier A, Nystrom H, Ferreira I, Gomola I and Huyskens D 2000 A comparative description of threemultipurpose phantoms (MPP) for external audits of photon beams in radiotherapy: the water MPP, theUmea MPP and the EC MPP Radiother. Oncol. 55 285 -293
Dutreix A, Mijnheer B, Shaw J, Svensson H 1997 Monitor unit calculation for high energy photon beams.ESTRO (European Society for Therapeutic Radiology and Oncology), booklet no. 3 (Physics forRadiotherapy), Garant: Leuven,
Gomola I, Van Dam J, Huyskens D and Dutreix A 1999 External audits of photon beams in non-referenceconditions: Mailed dosimetry comparisons with a multipurpose solid phantom Radiother. Oncol. 51 S35
Izewska J and Andreo P 2000 The IAEA/WHO TLD postal .programme for radiotherapy hospitalsRadiother. Oncol. 00 1-8
Novotný J, Gomola I, Izewska J, Huyskens D, Dutreix A 1997 External audit of photon beams by mailedfilm dosimetry: feasibility study Phys. Med. Biol. 42 1277-1288
Thwaites D I, Wiliams J R, Aird E G, Klevenhagen S C and Wiliams P C 1992 A dosimetricintercomparison of megavoltage photon beams in UK radiotherapy centres Phys. Med. Biol. 37 445-461
XXIV DRO Demänovská dolina 52

STEP
Calibration of the beam of theSSDL in terms of air kermu fCo-60)
QUALITY CONTROL OF RADIOTHERAPY CENTRES IN THESLOVAK REPUBLIC: A DOSIMETRY INTERCOMPARISON OF
PHOTON AND ELECTRON BEAMS UNDER REFERENCECONDITIONS.
Igor Gomola1, Gabriel Králik2, Jan Van Dam3 and Viera Laginová2
Institute of Preventive and Clinical Medicine, Radiation Protection dept.,Limbová 14, 833 01 Bratislava, Slovak Republic
2 Oncological Institute of St. Elizabeth, Radiotherapy Department,Heydukova 10, 81250 Bratislava, Slovak Republic
University Hospital Gasthuisberg, department of Oncology, section RadiotherapyHerestraat 49, 3000 Leuven, Belgium
l.Introduction; The aim of radiotherapy is to eradicate tumour cells by radiation inducedlesions in their DNA structure while minimizing the radiation damage to health tissues. About50 % of all patients with cancer are treated with radiotherapy. The process of radiation therapyis complex and involves a series of procedural steps beginning with patient diagnosis anddisease staging and culminating in the treatment of a specified target volume. The accuracy ofeach step in the process has a direct impact on treatment outcome. There is increasing evidence,from a review of dose-effect curves, that a high degree of accuracy in dose delivery to tumour
cells is very important for the success ofradiotherapy. Accuracy of dose delivery is to beachieved by a precise dosimetry, which involvesa large number of steps, shown in figure 1,starting with the calibration of a dosimetrysystem through the determination of theabsorbed dose at a point of interest in a patient.According to a world wide survey performedthrough the International Atomic EnergyAgency (IAEA) and the World HealthOrganisation (WHO), about 15% of all cancerpatients treated with radiation receive anincorrect dose due to systematic uncertainties indose delivery {WHO 1988). This number isprobably higher in radiotherapy centres notimplementing Quality Assurance (QA)programmes. Even when an appropriate QAprogramme is implemented at a radiotherapydepartment, deviation between the prescribeddose and the delivered dose may occur due tovarious reasons. It is therefore recommendedand in some countries it is mandatory, that anindependent person, visiting team ororganization are asked to perform dosimetry
audit at radiotherapy departments in an independent way through an external dosimetry audit.Therefore the IAEA together with the WHO established the IAEA/WHO TL postal dosimetryaudit to verify the calibration of radiotherapy units in developing countries (Izewska et at 2000).Despite to the fact that has been established in 1969, only a few radiotherapy centres fromCentral Europe were participated in this audit. Thanks to the financial support of EuropeanCommunities and in the close co-operation with the Flemish government, a pan EuropeanRadiation Quality Assurance project (EURAQA) has been established in 1995, withparticipation of ail radiotherapy departments in the Slovak Republic. Such wide international
SSDLCalibration of the hospital dosiinctrysystem in terms of air kerma fCo-60)
Absorbed dose determination oftherapeutic beams in reference conditions
in water rCo60.X-rav. electron"!
Relative dose distributionin non-reference conditions
in water
i
Patient data
f Í
Calculation of monitor units(or irradiation time) and absorbed
dose distribution in a patient(treatment planning system)
Patient irradiation J
Fig. 1. A typical dosimetry chain applied inradiotherapy
XXIV DRO Demänovská dolina 53
SK02K0178

Dosiftieíty jnlercomparison
EURAQA structure BIPM (Bureau International dcsPoíds et Mesures), Paris, R^ancc
dosimetry audit was carried out in the Slovak radiotherapy departments for the first time. In theframework of the EURAQA project the Radiotherapy department of University HospitalGasthuisberg in Leuven, Belgium was chosen as a Reference Measuring and Co-ordinatingcentre (RMC), because of its reliability to act as the co-ordinating centre has been confirmed inprevious programmes on QA in Radiotherapy {Dutreix et al 1994).2.Material and methods: The EURAQA project started in 1995. In the framework of theproject were audited all photon and electron beams used in megavoltage external radiationtherapy in Slovak Republic.2.1. Infrastructure: The internal dosimetry infrastructure of the EURAQA project is shown infigure 2. First step of the project consisted from establishment of National Reference Centres
(NRC), which were co-ordinatingtasks between the Reference andMeasuring Centre in Leuven (RMC)in Leuven and Local Centres (LC).LCs were selected according to theirreliability and long term experiencesin the field of radiation therapy.Oncological Institute of St. Elizabethin Bratislava (OUSA), acting also asthe SSDL for the Slovak radiotherapycentres, has been established as theNRC for the Slovak Republic becausethe results achieved in theIAEA/SSDL dosimetry world-widenetwork has been proved its reliabilityin the field of radiation dosimetry. Inthe period from 1991 to 2000 at theOUSA were performed by
Reference Measuring and Co-ordinating centre (RMC),Leuven, Belgium
MEA/SSDLDosimMry \I-nboratory, Seibcrsdorf, Austria }
Co-SO J
EQUAUF.STRO InstituteGuslave-Roussy. Villejuif, France
Co-60, High Energy X-ray
RPC (Radiological PhysicsCentre) Houston, USA
High Sncrgy Electron besmi
SSDL Gcnl, BelgiumCo-«l>
Fig. 2. LURAQA dosimetry infrastructure
international bodies (IAEA, EURAQA) 28 dosimetry checks with the mean deviation betweenthe measured dose and the stated dose m = -0 .1% (1SD=1.2%, Min—2.2% Max=2.6%).2.2. Dosimetry method: For the external dosimetry audit the RMC in Leuven has chosenlithium fluoride (LiF) powder, including a proportion of 99.97 % of 7Li doped with Mg, Ti andNa). The dosimetry properties of LiF are well adapted to the conditions of mailed dosimetry, asit has been already proved in other dosimetry intercomparison programmes {Gomola et al (b)2001, Hansson et al 1991). This type of the TL material is chosen considering its effectiveatomic number (ZeffiUF - 8.2), which make it close to tissue equivalent (Zeff, tissue—7.4) and doesnot perturb too much the photon and electron fluencies in the high-energy photon beams used inradiotherapy. Its low fading (less than 5% a year) is an important characteristic for maileddosimeters as they are exposed to wide range of temperatures during travel. The method of theTLD calibration and the absorbed dose determination used at the RMC has been alreadydescribed. (Derreumaux et al. 1994)2.3. Organisation of the audit: The TLDs, instruction and data sheets are mailed to the
participant together with a TLDholder (the IAEA holder type) tobe irradiated in a water phantom ata fixed source-skin-distance (SSD)or at a fixed source-detector-distance (SDD) depending of thelocal practice (see figure 3). TheTLDs are irradiated at 2Gy. Thenumber of monitor units (linearaccelerator) or irradiation time
Fig. J. Geometry set-ups of the TLD holders. First two set-ups(from left to right) for photons, right for electrons
( C o units) required, should be
XXIV DRO Demänovská dolina54

calculated by the participant according to the procedure in use in clinical practice. The results ofexternal dosimetry audits reported in this thesis are expressed as the ratio of the measured doseby TLDs determined at the RMC to the stated dose by the local centre e.g. The results of thephoton and electron beam output checks in reference conditions are expressed as the deviationbetween the measured dose and stated dose, Dev - (DM/Ds-l)xl00%, where Dm is the absorbeddose in water measured by TLDs at the RMC and Ds is the absorbed dose in water stated by the
participant In table 1 areTable 1 Decision criteria applied for the results in the EURAQA project described criteria for the
follow up actions to beperformed by the NRC inclose co-operation with theRMC at the auditedradiotherapy departments.
3:ResuIts: A total of 75beams in 14 radiotherapy
centres in Slovak Republic have been checked including 33 photon beams (B 7Cs, 6 0Co, X-raysfrom 6MV to 18MV)
Acceptance level
Minor deviation
Major deviation
Photon beams(Co-60, X ray)
Dev <= ± 3 %
± 3 % < Dev <= ±6%
Dev > ±6%
Electron beams(4 MeV - 25MeV)
Dev <= ± 6%
± 6 % < D e v < = ± 12%
Dev>± 12%
Table 2. The results of dosiemtry checks obtained in Slovak RT centres
Beammodality
Check No: NB mean 1SD Max Min
Photon beams
1234
331371
1.8%1.3%
-1.1%-2.9%
4.3%5.7%4.1%
10.6%11.1%2.7%
-6.0%-9.9%-9.7%
Final status 33 0.0% 1.8% 2.9% -3.0%
Electronbeams
40183
0.4%1.7%2.9%
8.6%2.1%.3.3%
29.3% -14.9%5.8% -2.0%5.2% -0.9%
Final status 40 1.2% 2.4% 5.8% -3.4%
and 40 electronbeams (from 6MeVto 20MeV). The delaybetween mailing ofthe TLDs by theRMC to theparticipating centresand their evaluation ison average 54 days(min=14, max=153).The results of thephoton and electronbeam output checks
I
lsl check - EUIUOA
Priemer ^1SD =
602.2%5%
26.7%-7.3%Min =
hl check -EUJtAQA
Priamer =33
1.8%4.3%10.6%-6.0%
2 Í0 I ' JCJLt
Dev
[5 EURAQA IH Slovensko j
J3L(N <N ( S
hi check • F.URAQAN « 48
7%7.4%
-324%
Mean K
1SD-Mnx-M i n -
hi check • SlovakiaM ' 40
Prien»ir= 0.4%1SD» 8.6%
Mnx=> 29.3%M i n - -14.9%
LL iJl
fb EURAQA I[w_Slovensko |
[hŕ g g S
Dev
Figure 4 The results of the ľ' check obtained in Slovak RT centres and centres from the other pareticipatingcountries. Left picture shows the results of the photon beam output checks, right electrons
in reference conditions are reported in table 2. Comparison of the results obtained in the SlovakRT centres and RT centres of other participating countries is shown in figure 4.
4. Discussion: The results obtained in the first check shows that only about 60% of beams arewithin the acceptance limit. The reasons of discrepancies were traced, in some cases by an onsite visit of experts from the NRC, and unacceptable deviations were corrected. Analysis of theresults observed in the first and the second dosimetry checks has shown:
XXIV DRO Demänovská dolina 55

A) Significant improvement: In 11 cases the reasons ofdeviations outside the acceptance level were identifiedand the error was corrected, which was confirmed by the2nd dosimetry check.B) No improvement: In 15 cases, the deviations remainthe same or worse with the same sign of deviationsbetween measured and stated doses.C) Reverse trend: In 9 cases the LCs claimed to haveimproved the situation, but the second check revealedthat the sign deviations between measured and stateddoses were just reversed as shown in figure 5. From the Fig. S. The comparison of the results,information provided by the participants it became clear f°r ali participating countriesthat at least part of these "over corrections" were due to observed between I and 2misunderstanding, despite all efforts to inform dosimetry check of photon beamsaccurately all participants of the aim of the programme, which is to check the beam output, andnot at all to provide a new calibration factor for the local reference ionization chamber (this willalways strictly remain the responsibility of the national dosimetric standard laboratory). In orderto avoid in the future this type of difficulties, it was agreed upon to communicate to the centreinvolved neither the size nor the sign of the deviations observed.
5. Conclusions: The results clearly demonstrate the usefulness of the external dosimetry checksperformed with the mailed thermoluminescent dosimeters. Standard deviation of the distributionof the results decreased from SD=:4.3% to SD=1.8% for checked photon beams and fromSD=8.6% to SD=2.4% for electron beams, respectively, at the end of the project. The dosimetryaudits which are performed in regular intervals significantly decreasing a possibility ofmistreatment (under-dosage or over-dosage) of patients due to wrong calibration of radiationtherapy beams. In order to keep the reached level of dosimetry precision, it is necessary toestablish the external audit in radiotherapy at the national level based on postal TLD dosimetry{Gomola et al 2001 (b), Laginova et al 1998) by transferring the know-how from theinternational program on Q A in radiotherapy dosimetry'with the assistance of the IAEA. TheEURAQA project was ssupported by the EU Copernicus DGV (ERBCIPAT 94017)
6. References:Derreumaux S, Chavaudra J, Bridier A, Rosseti V and Dutreix A 1995 A European quality assurancenetwork for radiotherapy: Dose measurement procedure Phys. Med. Biol. 40 1191-1208
Dutreix A, Derreumaux S, Chavaudra J and van der Schueren E I994 Quality control of radiotherapycentres in Europe: beam calibration Radiother. Oncol. 32 256-264
Gomola I, Van Dam J, Isern-Verdum J, Verstraete J, Reymen R, Dutreix A, Davis B, Huyskens D 2001External audits of electron beams using mailed TLD dosimetry: preliminary results Radiother. Oncol. 55163-168(3.)
Gomola I, Laginová V, Cintulová A, Králik G 2001 Výsledky externého dozimetrického audituvysokoenergetíckých fotónových a elektrónových zväzkov na rádioterapeutických pracoviskách SR vrámci projektu EURAQA Slov. Radiol. in press (b)
Hansson W F, Stovall M and Kenedy P 1991 Review of dose intercomparison at a reference point IAEATECDOC-734, Vienna 121-130
Izewska J and Andreo P 2000 The IAEA/WHO TLD postal programme for radiotherapy hospitalsRadiother. Oncol. 00 1-8
Laginova V, Králik G, Cintulová A and Gomola I 1998 TLD audit for photon and electron beams inSlovak Republic. Project EURAQA. Acta Polytechnica 38 137-146
World Health Organisation 1988 Quality Assurance in Radiotherapy, WHO Report Geneva
XXIV DRO Demänovská dolina 56

THE INFORMATION SYSTEM ON OCCUPATIONAL EXPOSUREAND RELATED IAEA ACTIVITIES IN THE EUROPE REGION
Monica GustafssonInternational Atomic Energy Agency, Division of Radiation and Waste Safety
Wagramer Strasse 5, PO Box 100, A-1400 Vienna, Austria
Introduction
The International Atomic Energy Agency (hereafter referred to as the Agency or theIAEA) is unique among international organizations concerned with radiation protection issuesas having two functions, by Article III.A.6 of its Statute, to "establish or adopt ... standards ofsafety for protection of health and minimization of danger to life and property ... and to providefor the application of these standards...". The basic requirements for radiation protection againstexposure to ionizing radiation of workers, members of the public and patients are given in theInternational Basic Safety Standards for Protection against Ionizing Radiation and for theSafety of Radiation Sources (hereafter referred to as the BSS) [1],
The objectives of the Agency's Occupational Radiation Protection Programme, within theDivision of Radiation and Waste Safety, are to encourage the global harmonization andoptimization of occupational radiation protection in situations of exposures due to externalradiation and intakes of radionuclides from both artificial and natural sources of radiation; andto have in place and ensure compliance with operational health and safety measures prescribedby the Agency on its premises and in occupational activities under its supervision or control.The Information System on Occupational Exposure (ISOE) forms an integral part of thisprogramme and the purpose of this paper is to present the current status of ISOE and the IAEAactivities in the Europe region in support of the ISOE.
Information System on Occupational Exposure (ISOE)
ISOE is co-sponsored by the OECD Nuclear Energy Agency (NEA) and the IAEA,through an agreement reached in 1993, by which the IAEA is inviting those of its MemberStates with operating nuclear power plants not members of the OECD, to participate cost-freethrough the IAEA ISOE Technical Centre. Subsequently, the Agency has formed a Joint ISOESecretariat with OECD/NEA.
According to the Terms and Conditions for the operation of ISOE, the objective of theISOE Programme is to make available to participants:
Broad and regularly updated information on methods to improve the protection ofworkers and on occupational exposure in nuclear power plants;A mechanism for dissemination of information on these issues, including evaluation andanalysis of the data assembled, as a contribution to the optimization of radiationprotection.
Thus ISOE is promoting and co-ordinating international co-operative undertakings in thearea of protection of workers at nuclear power plants, at the same time providing a forum forcommunication between radiation protection experts.
The ISOE database, the world's largest available database on occupational exposure,includes information on occupational doses for 452 reactors, both operating and in cold shutdown or in some stage of decommissioning, operated by 72 utilities in 28 countries, as ofDecember 2000. National regulatory authorities from 25 countries also participate in the ISOE
XXIV DRO Demänovská dolina 57
IIISK02K0179

programme. The participation of 398 operating commercial nuclear reactors in the ISOEprogramme represents some 92% of the world's operating commercial nuclear reactors (total of433).
ISOE is organized in a decentralized form, operated through ISOE Technical Centres.The ISOE Programme is directed by a Steering Group, which is responsible for policydecisions, and the overall programme direction. The joint NEA/IAEA Secretariat facilitates thework of the ISOE Steering Group, provides and manages communication with responsible NEAand IAEA bodies and organizes transfer of information and communication between SteeringGroup, Working Groups and Technical Centres. The ISOE Bureau, appointed by the SteeringGroup, manages the ISOE Programme, through the Joint Secretariat, between Steering Groupmeetings.
A growing number of Agency Member States are participating through the IAEA. As of 1October 2001, there are eleven utilities and eight authorities from eleven countries participatingin the ISOE, i.e. utilities in Armenia, Brazil, Bulgaria, China, Lithuania, Romania, RussianFederation, Slovenia, South Africa and Ukraine (representing 44 operating reactors) and theregulatory authorities in Armenia, Bulgaria, China, Lithuania, Pakistan, Romania, Slovenia andSouth Africa. The Technical Centres are responsible for the management of the databases, serveas contact point for the transfer of information to the participants, prepare information sheetsand organize topical sessions and annual workshops. The IAEA is co-organizing the 3rd
EC/ISOE Workshop on Occupational Exposure Management at Nuclear Power Plants will beheld in Portoroz, Slovenia, in April 2002.
The ISOE communications network is an information pipeline to facilitate the real-timeexchange of experience and information among participating utilities and authorities. Thenetwork consists of all ISOE participants as well as the four Technical Centres. Any participant- utility or authority - may question the network for information on a particular problem,technique, procedure, etc. The appropriate Technical Centre will perform a survey of allparticipants, via the other Technical Centres, collect and summarize the desired information,supply the information to the requester, and - if appropriate - prepare an ISOE information sheetfor distribution to all other participants.
The ISOE database is divided into four parts including dosimetric information fromcommercial nuclear power plants in operation, such as the annual collective dose for normaloperation and outages; plant-specific information pertinent to dose reduction; radiationprotection related information for specific operations, jobs, procedures, equipment or tasks; anddosimetric information from nuclear power plants which are shut down or in the process ofdecommissioning.
All information included is supplied by participating utilities, who have full access to alldata. Participating authorities have access only to a reduced database, including data fromutilities in their own country. The ISOE database forms the basis for various types of dataanalysis and studies of occupational dose trends. Current information and trends can be found inthe 1999 Annual Report of the ISOE Programme [2]. More detailed analyses of the data can befound in the ISOE information sheets.
IAEA activities in the Europe region related to ISOE
Two very important tools for training on optimization of radiation protection have beenmade available to the ISOE participants. To introduce radiation protection optimization,especially in the nuclear industry, a software learning programme, RADIOR, has beendeveloped with the financial support of the European Commission and the IAEA. RADIOR
XXIV DRO Demänovská dolina 58

(produced by PRODIDACT with collaboration of the CEPN) is now available on diskette fromthe IAEA in six languages (English, French, German, Russian, Spanish and Swedish). TheEnglish version is also available on the IAEA Web site and this Web application shouldfacilitate translations into other languages.
The OECD document Work Management in the Nuclear Power Industry [3], which wasdeveloped by an Expert Group within the ISOE, is considered to be of great value in theoptimization process in nuclear power plants. In order to make it accessible also for persons notfamiliar with the English language, the Agency has supported its translation into Russian as wellas Chinese.
A Regional Project on Improving Occupational Radiation Protection in Nuclear PowerPlants in Central and Eastern Europe and in the Republics of the former Soviet Union waslaunched in 1997 with the general objective of implementing the optimization principle innuclear power plants in accordance with the BSS [1], As of 2001, this project is followed by aRegional Project on Enhancing Occupational Radiation Protection in Nuclear Power Plants. Thetarget countries are Armenia, Bulgaria, Czech Republic, Hungary, Lithuania, Romania, RussianFederation, Slovak Republic, Slovenia and Ukraine.
Highest priority within the project was, from the beginning, put on Workshops for HealthPhysics Groups, which have turned out to be very important occasions for informationexchange, especially on RBMK and WWER reactors, for dose and dose rate comparisons andbenchmarking. In addition, training has been the main element of the project. Two regionaltraining courses on Optimization and Radiological Protection in the Design and Operation ofNuclear Power Plants were organized in co-operation with the European Commission, one inPrague, Czech Republic, in 1997 and one in St. Petersburg, Russian Federation, in 1999. Thesetraining courses were directed at those associated directly or indirectly with designing andimplementing radiation protection programmes, including regulatory authorities, and theaudiences were composed mainly of health physicists from nuclear power plants and regulatoryauthority staff.
The primary responsibility for optimization lies with the management and thecommitment of senior management is an essential pre-requisite for successful introduction orcontinuation of an ALARA (As Low As Reasonably Achievable) programme. It was thereforeconsidered to be very important to improve the awareness of optimization in this group. For thispurpose, a Workshop on Implementation and Management of ALARA in Nuclear Power PlantOperation was held in the IAEA Headquarters in Vienna in 1998. Efforts were made to havepresentations from peers, from the target countries as well as from the rest of Europe.
Regional training events such as those mentioned above have the advantage that theparticipants enter in contact with colleagues from other countries with different experiences, butwith the disadvantage that very few persons from each country can take part. The strategy forthese projects is therefore also to promote national training, for a country as a whole or locallyin a nuclear power plant. Some nuclear power plants in the project were already organizing suchtraining events, while others felt that they needed support to achieve this. It was recognized thatthe training events held under the project provided a very good basis for national training and anexpert group, composed of experts from the target countries and the rest of Europe, wastherefore convened to prepare training material on the application of the ALARA principle innuclear power plants. The intention was to provide the material in English and Russian.
The first products from this work is available as IAEA Working Material on CD-ROM inEnglish and Russian for use in the nuclear power plants. When feedback has been collected, amore long lasting product will be produced. Also, train the trainers events will be organized incountries where the need is identified.
XXIV DRO Demänovská dolina 59

The material produced consists of two different courses. ALARA Course 1, a half daycourse, is intended for the top management of nuclear power plants and regulatory staff fromcentral regulatory offices. ALARA Course 2 is expected to last for 1Í4-2 days and will be givenfor chiefs in nuclear power plants and their deputies of operational, maintenance, radiationprotection and other departments involved in the planning and performance of work incontrolled areas, for foremen as well as local regulatory inspectors. The electronic coursematerial for both courses includes: Lecturers Help, slides in PowerPoint and full text ofreference papers (general and on examples of ALARA implementation). The Lecturers Helpincludes a description of the course (target group, aims, objectives, etc.), a list of the slidesincluded (with an indication of the keyword for the slide, its main message and a reference tothe paper it is based on), guidance for the performance of the different parts of the course (suchas indications where local material should be introduced) and lists of reference papers andreference books.
Conclusions
The ISOE programme will continue to be a very important part of the IAEA OccupationalRadiation Protection Programme as will the related activities under the Technical Co-operationprogramme. Realizing the need for information exchange and promotion of the application ofthe ALARA principle in industries other than nuclear power plants, the Agency has recentlyinitiated the creation of regional ALARA Networks. These are seen as an effective way to fostergood working practices and the development of an ALARA culture. Further information on theIAEA radiation protection programme can be found in the Web page: www.iaea.org/ns/rasanet.
References
[1] Food and Agriculture Organization of the United Nations, International Atomic EnergyAgency, International Labour Organization, OECD Nuclear Energy Agency, PanAmerican Health Organization, World Health Organization, International Basic SafetyStandards for Protection against Ionizing Radiation and for the Safety of RadiationSources, Safety Series No. 115, IAEA, Vienna (1996).
[2] Nuclear Energy Agency of the Organization for Economic Co-operation andDevelopment, International Atomic Energy Agency, Occupational Exposures at NuclearPower Plants. Ninth Annual Report of the ISOE Programme, 1999. OECD/NEA, Paris(2000).
[3] Nuclear Energy Agency of the Organization for Economic Co-operation andDevelopment, Work Management in the Nuclear Power Industry: A Manual prepared forthe NEA Committee on Radiation Protection and Public Health by the ISOE ExpertGroup on the Impact of Work Management on Occupational Exposure, OECD/NEA,Paris (1997).
XXIV DRO Demänovská dolina 60

FOUR-YEARS EXPERIENCE WITH MONITORING OF PERSONSAT THE TREATMENT OF CHIDLREN PATIENTS
WITH NEUROBLASTOMA BY 131I-MIBG COMBINATIONWITH HYPERBARIC OXYGEN THERAPY
Jindřiška Heřmanská 2'2, Jaroslav Zimák 2, Hana Křížová 2, Zuzana Pásková 3,Petr Došel4
1 Ústav lékařské biofyziky UK 2. LF Praha, 2 Klinika nukleární medicíny UK 2. LF aFN v Motole, Praha, 3 Státní úřad pro jadernou bezpečnost, 4 Ústav leteckého
zdravotnictví Praha
Treatment of children patients with neuroblastoma by 131I-MIBG in combination withhyperbaric oxygen therapy (HBO) started in the Czech Republic in 1997. Medical aspects ofthis treatment are widely discussed, e.g. [1- 4]. Rare information concerning radiation protectionis, however, at disposal. Moreover, majority of papers, e.g. [5,6], deal with the problem ofinternal irradiation. In a single work only, attention is paid to external exposures of nursing staffdelivering HBO [7].
Estimation of radiation load from external irradiation plays very important role in thetreatment scheme elaborated at the Department of Nuclear Medicine. According to this scheme,activities of 5.5 GBq and 3.7 GBq are administered at the first and repeated therapies,respectively. 3rd, 4th, 5th and 6th day after the administration patients undergo HBO in theInstitute of Aviation Medicine Prague. Activity administration and following care are realised atthe bed station of the Department of Nuclear Medicine, which is the workplace of III. categorywith unsealed radionuclide sources. During the day, instructed family members ensure anecessary non-medical care. Two-ways audio-visual circuit connects rooms of the child andfamily member. It enables mutual communication and reduces personal contacts to themaximum possible extent. In years 1997-2000, 20 therapies at 10 children (age 4-14 years at thefirst therapy) were performed.
From the description of the treatment schema it follows that two groups of populationshould by monitored:• Family members for which the special limit, equivalent dose 5 mSv during the whole
treatment time, is relevant [8].• Drivers of ambulances transporting patients to HBO and the staff maintaining the
hyperbaric chamber. In this case, the condition of non-exceeding of equivalent dose 1 mSvper year has to be fulfilled [8].
Real dose equivalents were checked during the reported four-year period. Members of bothgroups were equipped by personal digital dosemeters STEPHEN6000 for inspection.
Examples of radiation load for family members (expressed in dose equivalent H) arepresented on Figs. 1-3. Letter "C" above the column indicates that the family member waspresent together with a child in the hyperbaric chamber during the therapy. On Fig. 4, doseequivalent for all patients and family members are summarized.
The presented results and a detailed analysis published in [9] imply that H-values areindependent of:• administered activity (recall that 5.5 GBq is administered at the 1st therapy, 3.7 GBq at
further therapies)• child age and presence of a family member in the hyperbaric chamber during HBO.
Values of H 1.14 and 1.44 for the patient 2 are the consequences of enormous care requiredby the child after HBO. It indicates crucial role of child independence. The child and parentshave to be satisfied with communication by the two-ways audio-visual circuit in order to avoidhigh irradiation.
XXIV DRO Demänovská dolina 61 muSK02K0180

year
| H member 1 S3 member 2'>member"3~|
Fig. 1: H-values for family memberspatient no. 1
Fig.2: H-values for family memberspatient no. 2
1997 1998
year
2,5
2
1
0.5-
n •
j
L 11litBmemberi E3member2
number of therapies
[ilrnernberi Bmerrbar2 B member 3)
Fig. 3: H-values for family memberspatient no. 7
Fig. 4: H-values for family membersreview
Values of dose equivalent for the staff maintaining the hyperbaric chamber are demonstrated on Fig. 5.The year 2000 was selected as an illustrative example as the highest number of therapies (9) wasperformed in this year. It is obvious that dose equivalents for nurses and technicians arenegligible.
Dose equivalents for drivers of ambulances transporting patients to HBO coincidemostly with background values (see Fig. 6). Several outliers correspond to cases when thedriver helped with the transport of a child in the ambulance*
XXIV DRO Demänovská dolina 62

<0,1 0,2 0,4 0,6 0,8 1,0 1.2 1.4 1.6 1,6 2,0 2,2 2,4
H [USV]
Fig. 5: H-values for the staff maintainingthe hyperbaric chamber
Fig. 6: H-values for ambulancedrivers
From the presented results, the following conclusions can be drawn:1. Monitoring of family members has to be performed in spite of the fact that exceeding of
equivalent dose of 5 mSv is non-realistic. Unexpected situation concerning behaviour ofboth parents and children cannot be excluded. Moreover, records of H - values have to bestored and analysed in the case of possible pregnancy.
2. A question arises in connection with the special limit 5 mSv: What is the whole time of thetreatment? Is it possible to understand it, similarly as in the case of iodine therapy, as 5mSv per year or is it necessary to take into account really the whole, often very long, timeof the treatment?
3. Monitoring of the staff maintaining the hyperbaric chamber and ambulance drivers seemsto be unnecessary. Under normal condition, the staff is outside the chamber and its contactwith a patient is minimal. In unusual situation, the instructed nurse from the Department ofNuclear Medicine equipped by STEPHEN 6000 will estimate dose equivalent and contactresponsible medical physicists. An extraordinary situation during the transport will be
' solved in the similar way.
References1. Klingebiel T., Bertholf T., Treuner J. et al: Metaiodobenzylquidanine (mlBG) in treatment2. of 47 patients with neuroblastoma: results of German neuroblastoma Trial. Med. Pediatr.
Oncol., 19,1191, No. 2, 84-88.3. Lashford L.S., Lewis I.J., Fielding S. et al: Phase FII of Iodine 131
metaiodobenzylquanidine in Chemoresistant neuroblastoma: A United Kingdom Children'sCancer Group Investigation. Journal of Clinical Oncology.lO, 1995, No.2, 1889-1896.
4. Mastragelo R., Tornesselo R. Mastragelo S.: Role of 1311-metaiodobenzylquanidine in thetreatment of neutroblastoma. Med. Pediatr. Oncol. 31, 1998, No.l, 22-26.
5. Voute P.A., va der Kleij A.J., De Kraker J. et al.: Clinical experience with radiationenhancement by hyperbaric oxygen in children with reccurent neuroblastoma stage IV.Eur. J. Cancer, 331A, 1995, No.4, 569-590.
6. Fielding S.L., Flower M.A., Ackery D. et al: Dosimetry of iodine 131metaiodobenzylquanidine for treatment of resistant neuroblastoma: results of a UK study.Eur. I Nucl. Med, 18, 1991, No.5, 308-316.
7. Flower M.A., Fieding S.L. Radiation dosimetry for 13II-mIBG of neuroblastoma. Phys.Med. Bio., 41, 1996, No. 8, 1399-1370.
XXIV DRO Demänovská dolina 63

8. Melbourne G.J., Lehm P.: Quantifying the radiation exposure of nursing staff deliveringhyperbaric oxygen therapy to grade IV neuroblastoma patients post 13II-MIBG therapy.Eur. J. Nucl. Med., 27, 2000, No. 11, 1731-1733.
9. Decree of the State Office for Nuclear safety No. 184/1997 Coll.10. Heřmanská J., Zimák J., Křížová H. et al: Evaluation of radiation load of persons caring
about children with neuroblastoma treated by 131I-MIBG in combination with hyperbaricoxygen therapy. Česká radiologie, 2001, accepted. In Czech.
Acknowledgement: This research was partially supported by grants IGA MH ČR No. 3943-3and GAČR 102/99/1564.
XXIV DRO Demänovská dolina 64

SK02K0181DETECTION SYSTEM FOR CONTINUOUS 222RN MONITORING
IN WATERS
Karol Holý \ Eleonóra Patschová *, Oľga Holá 2, Ivana Bosá', Anna Polášková *Faculty of Mathematics, Physics and Informatics of Comenius University, Mlynská
dolina Fl, 842 48 Bratislava, Slovak Republic,2Faculty of Chemical and Food Technology of Slovak Technical University,
Radlinského 9, 812 37 Bratislava, Slovak Republic
Introduction
The volume activity of 222Rn in waters is the most frequently measured in order tocontrol the population exposures from the radon. During the former two decades theinvestigation of the radon in waters has been extended also for the earthquake and vulcaniceruptions' prediction, for the fault location and for requirements in hydrogeology [1, 2]. Themeasurements of the radon can be continuous or discrete, or by carrying out the grab sampling,but many applications require monitoring as continuous as possible. It is necessary because ofthe correction of experimental data from fluctuations connected with natural causes.
This contribution presents one of the high-sensitive systems of continuous radonmonitoring in waters. The device can be used for the continual control of 2 2 2Rn activityconcentration in water sources, for a study of the daily and seasonal variations of radon activityconcentration in water systems, for the determination of the infiltration time of surface waterinto the ground water and for the next untraditional applications.
Radon Monitoring Device
The working principle of the constructed device for the continual radon monitoring isbased on the removal of the radon from water and its subsequent measurement by the radondetector. The device layout is on the Fig.l. There are distinguished two circuits - water circuitand air circuit. The main part of the device is the outgassing vessel (OV) of 180 rrO volume.Water is supplied from the source (SW) to the outgassing vessel and then water outflowsthrough the hole in the sidewall of the vessel into the waste piping (WP). The water volume of120 mD in the outgassing vessel is maintained by the movable arm with a water seal (WS).Radon contained by water is released by the flow of the inactive air, which is pressed by thecompressor pump (CP) into the outgassing vessel through the frit (F). The air enriched by thereleased radon is dried and next is carried to the radon monitor (RM). The whole process runscontinuously.
The volume activity of 222Rn in input water is calculated according to the relation:
4 - A 1*.Lp* K
where: AVA- the volume activity of 2 2 2Rn in the output air from the outgassing vessel,p* - the overflow of the air through the outgassing vessel,pw - the water discharge through the outgassing vessel,kd - the outgassing coefficient defined as the ratio of the velocity of the radon
removal from the water in the outgassing vessel by air to the velocity of theradon supply by the water inflow into the outgassing vessel.
XXIV DRO Demänovská dolina 65

The value of the outgassing coefficient depends on the air overflow pa and the water
discharge pw ratio through the outgassing vessel. For the ratio—-— 10 is ká = 0,9.
Testing shows that at the present construction of the monitoring device and at the watervolume of 120 ní] in the outgassing vessel, the optimum parameters of air and water overflowsare: pA ~ (0,7 - 1,0) D.min"1 , pv ~ (0,12 - 0,20) D.min"'. At these parameters the high value ofthe outgassing coefficient is obtained (£<j ~ 0,75) and more over the device is stable from thepoint of view of air and water overflows. The detecting limit of the device for the continuousmonitoring of 222Rn in water is 0,5 Bq. IT1.
V Fl
CP
VA
-
C sk/J
FR
F2 RM
ov
A2
WS v
Fig.I. The scheme of the device for the continuous monitoring of 222Rn in water.(1 - water circuit, 2 - air circuit, SW - water source, OV - outgassing vessel, F - frit,CP - compressor pump, WS - water seal, WP - waste piping, C - cooler trap, S - silicagel, FR - filter, RM - radon monitor, Fl , F2 - flowmeters)
Results and Discussion
The long-term stability of the measuring system was tested by water supplied from thewater piping to the outgassing vessel. The overflow of the air and water through the outgassingvessel was kept on the level 0,8 D.min"1 and 0,13 D-min"1 respectively. The volume activity of222Rn in the air rising from the outgassing vessel was recorded in 10 minutes intervals.
Results of 9 days continuous monitoring of the volume activity of 222Rn in water arepresented in Fig.2. The whole system worked reliably during the testing. The volume activitiesof 222Rn in water main are not stable but there exist the daily variations of them. The minimumvalues of the volume activity of 222Rn were measured as a rule at the midday and maximumvalues at the late afternoon and night-time. During the day the volume activity of 222Rn waschanged sometimes up to 70 %. The smallest changes of the volume activity of 222Rn wereobserved on Sunday.
Till now there was not reliably explained whether these changes are connected only withprocesses in water piping or also with processes in a water source. The testing device for thecontinuous measurements of the radon in waters could be useful also to the revelation of theorigin of the radon variations in the transport water piping, respectively to its usage for the othernovel applications.
XXIV DRO Demänovská dolina 66

1/9 1/10 1/11 1/12 1/13 1/14 1/15 1/16 1/17
Day
Fig. 2. The time course of 222Rn activity concentration in water of water piping.
Acknowledgements. This study was funded by Scientific Grant Agency of Ministry ofEducation of Slovak Republic (VEGA Project).
References
[1] Monnin M.M., Seidel J.L.: Radon in soil air and in groundwater related to majorgeophysical events (a survey). Proc. of the Sec. Workshop on Radon Monitoring inRadioprotection, Environmental and/or Earth Sciences (ed. by G. Furlan and L. Tommasino),World Scientific, Singapore, pp. 274-285 (1991)[2] Friedmann H.: Selected problems in radon measurement for Earthquake prediction.Proc. of the Sec. Workshop on Radon Monitoring in Radioprotection, Environmental and/orEarth Sciences (ed. by G. Furlan and L. Tommasino), World Scientific, Singapore, pp. 307-316(1991)
XXIV DRO Demänovská dolina 67

TEMPORAL VARIABILITY OF SOME RADONCHARACTERISTICS OF THE SOIL
Karol Holýl, Anežka Ridziková *, Anna Polášková1, Tomas Stanys1, Ivana Bosá ',Oľga Holá2,
Faculty of Mathematics, Physics and Informatics of Comenius University, Mlynskádolina Fl, 842 48 Bratislava, Slovak Republic,
2Faculty of Chemical and Food Technology of Slovak Technical University, Radlinského 9, 812 37Bratislava, Slovak Republic
Introduction
The volume activity of 222Rn in the soil air is not stable. It changes with the depth aswell as with time. Radon concentrations are influenced especially by the atmospheric pressure,by the temperature and moisture of the soil, by the wind velocity and by the state of the soilsurface.
The daily and seasonal variations of the volume activity of 222Rn were observed in the soilair [1]. These variations must be taken into account for example in case that the soil's radon isused for the earthquake prediction. But mainly the seasonal variations of the radonconcentration are also the source of the uncertainties at the radon classification of the soil for thepurposes of the radiation protection. Therefore we must search such radon characteristics of thesoil, that are as little sensitive to the soil's state as possible during their determination. Furtherthe new approaches to the expression of the radon potential of soils could be developed toobecause of the more unique indication of the radon indoor levels.
Therefore the time variability of the volume activity of 222Rn in the various depth of thesoil, the variability of the diffusion radon length, of the radon exhalation's rate from the soilsurface and the radon availability of the soil are studied in our contribution. The new possibleapproach to the determination of the radon availability number of the investigated area ispresented with the aim to express the radon potential of the soil numerically and precisely.
Theoretical part
Assuming that the 222Rn is transported in the soil only by the diffusion, that theproduction rate of the radon is homogeneous and the diffusion coefficient is independent on thedepth, then the depth distribution of the radon volume activity for the steady state conditions
l-e L (1)( — — = O) is described by the relation [2]: ARn (z) = —-—^-^dt Fp-w
where ARn(z) is the volume activity of the 222Rn in the soil air at the depth of £ in (Bq.m"3), y4v,Ra
is the volume activity of the226i?ain the soil (Bq.m"3), Ke is the emanation coefficient of 222Rn,
Fv is the total porosity of the soil, w is the volumetric moisture content of the soil, L =
the diffusion length in (m), Ocf is the effective diffusion coefficient of 222Rn in the soil in ( m V ) and/tRnis the decay constant of 222Rn in (s'1).
For the depth z »L, the volume activity of radon reaches the saturated value:
A„ A.,, n„
Fp-w
XXIV DRO Demänovská dolina 68
•1SK02K0182

and for the depth z «L, the volume activity of radon is described by the linear relation:
*»&- Fp-W-L ( 3 )
If we substitute the relation (1) to the 1. Fick's law we can obtain the relation for
the surface exhalation rate of the 222Rn from the soil in the units (Bq.m2.s"!) in the
following form:
ES,Rn ~ Kn Ke A,Ra L (4)
We can write, respectively: Es Rn = ARn [Fp - w)ASRn L (5)
if we use the relation (2).In the relations (1), (2), (3) and (5) the available soil porosity (Fp-w) is presented. For its
calculation the total porosity Fp and volumetric moisture content w are determined from theanalysis of the small volume of soil. However, the equation for the difference (Fp - w) can be
derived from the relations (3) and (4): F-w = T . /;*" (6)lA{)/]AL
According to the relation (6) the representative available soil porosity can be calculated if thesurface exhalation rate and the depth concentration profile of the 222Rn are measured.
Tanner [3] suggested the next characteristics of the soil - radon availability - for theindication of the indoor radon levels. This parameter is defined as a product of the mean life ofthe radon (r = l/ARn) and its exhalation rate at steady state conditions. In the case that the radonis transported only by the diffusion in the soil, the radon availability, or more precisely - theradon availability number RAN - can be expressed by means of the relation (5) in the form:
RAN = (Fp-w)ASMn.L (7)The unit of RAN is Bq.m"2.
Sampling place and soil characteristics
The sampling place - the place where the temporal variability of the radoncharacteristics of the soil was studied - was situated in the area of Faculty of Mathematics,Physics and Informatics in Bratislava. The soil of this place is middle permeable [4]. The meanspecific activity of 226i?aup to the depth of 1,5 m is equal to 37,5 Bq.kg"1 in this soil. Theemanation coefficient of 222Rn in the surface soil is approximately 14,5% at the weight contentof the soil moisture in the range of 5 - 20 % [5].
Methods
The soil air samples were collected from different depths by using of the stainless steeltubes and the syringes [6]. For the determination of the 222Rn activity concentration the soil airwas sucked from the syringes into the pre-evacuated scintillation cells of Lucas type the volumeof which was 125 nO. The accumulation method was used for the determination of theexhalation rate of 222Rn from the soil surface. The air from the accumulation vessel circulatedcontinuously by means of the membrane pump in the closed circuit. The increase of the Rnactivity in the accumulation vessel was continuously recorded by the radon monitor [6].
XXIV DRO Demänovská dolina 69

Results and discussion
The volume activity of 222Rn in the soil air in the depth' interval of <0,15 m; 1,6 m> wasobserved from June to March. Altogether 29 depth profiles of radon were measured. The higherradon concentrations were found out during winter months than in summer months in all depths(Fig.l). The highest temporal variability of the volume activities characterized by the relativerange of the measured radon activities (ARn>maK - ARnmitl)j ARnm and by the variation
coefficient
25 -
20 -
S
I"
•
A
I
. z
i
0,3 m0,8 m1,15m
55
i
t i
' \ *
1 1
I
Z
l
J.
1
f
I .Z
•
1
10 -
5 -
05/11/00 7/10/00 9/8/00 11/7/00
Date
1/6/01 3/7/01
Fig. I Temporal courses of the radon volume activity in the soil air
SA/ARnm (SA is the standard deviation) was found out in the small soil depths. The exponential
decrease of the relative variation range and of the variation coefficient was observed with theincrease of the depth (Fig.2). Meanwhile in the depth of 0,15 m the volume activity of 222Rnoscillates round the mean value up to 150 %, the seasonal fluctuation of the volume activity of000
Rn in the depth of 0,80 m was only 30 %. The seasonal increase of the volume activity of222Rn was connected with the increase of the soil moisture. While the volume moisture of thesoil was only 5 % during dry summer days up to the depth of 0,80 m, from autumn to springmonths was this moisture in the surface layer of the soil 28 % and successively it decreased upto the depth of 1 m where reached the value of 5 %. The short-time increase of the volumeactivity of 222Rn up to the depth of 0,6 m was found out also in June after the rain when theincrease of the volume moisture of the soil was 15 % but only in the surface layer of the depthabout 0,10 m.
XXIV DRO Demänovská dolina 70

3.5
3.0
2.5
2.0 -
1.5
1.0
0.5 -
0.0
•
0
-
-
-
o
1
0
i
i r-
B
O
B
1
•o
1
B
O
1
t
(A -Amax
S /AA m
l
1 i
min in •
-
-
-
ao
i
0.0 0.2 0.4 0.6 0.8 1.0
Deptli [m]
1.2 1.4
1.0
0.9
0.8
0.7
0.6
- 0.5
0.4
0.3
0.2
0.1
0.01.6
Fig.2 The depth variability of the radon volume activity in the soil
The measured depth profiles of the volume activity of 222Rn were fitted by the function(1) and then the values of the saturated radon volume activity A^Rn and values of the diffusion
n 2.5
0.06/1/00 7/31/00 9/29/00 11/28/00 1/27/01 3/28/01
Date
Fig.3 Temporal courses of the saturated radon volume activity and radon diffusion length
length L were obtained from these fits. The determined values of As,Rn are higher in winter thanin summer months and the diffusion length has just reverse course (Fig.3). The relative variationrange is 0,26 for L and 0,6 for AsM, that is the same as for the volume activity of radon in thedepth more than 0,8 m. On the Fig. 4 there are illustrated the measured depth profiles of thevolume activity of 222Rn and their fits for the summer and winter month. The values of ASiRn
evaluated from the fits of the radon depth profiles were in a good agreement with the values ofAs%Rn calculated according to the equation (2) only under the condition that the available soilporosity (Fp - w) was determined by means of the relation (6).
XXIV DRO Demänovská dolina 71

sď
1 2 3 4 5 6Depth [m]
Fig.4 The radon depth profiles in the soil
The time variability of the measured exhalation rates was smaller than the variability ofthe other parameters. The relative variation range was only at the level of 0,21 (Fig.5).
The radon availability number (RAN) was calculated according to the relation (7). At thecalculation of RAN there were used values of As,gn and L determined from fits of the radondepth profiles and the values of (Fp - w) determined according to the relation (6) on the base ofthe measured values of ESiRn and on the base of the radon depth profiles in the soil for z « L.
6/5/00 7/25/00 9/13/00 11/2/00 12/22/00 2/10/01 4/1/01
Date
june July aug sept oct nov dec jan
Month
Fig.5 Temporal course of the radon exhalation Fig.6 Temporal course of the radonrate from the soil availability number
Conclusion
The small temporal variability of RAN and of the exhalation rate of radon were found outin contrast to the volume activity of radon in the soil air. Therefore, mainly RAN can be thesuitable characteristics of the radon soil potential because its determination is only littleinfluenced by the soil state, more over with the numerical expression applicable for the furthercalculations.
RAN of the area can be determined for example in following way:one measurement of the radon depth profile and of the radon exhalation rate from the soil isrealized at least on the investigated areathe diffusion length L and the addition ARn(z)/z for z « L is determined from the radondepth profile
XXIV DRO Demänovská dolina 72

- the volume activity of 222Rn in the depth of 0,8 m is measured in 1 5 - 2 0 checkpoints andthe mean volume activity of 222Rn is determined for this area
- the saturated volume activity of 22ZRn is calculated according to the relation (1) on the baseof the determined mean volume activity of 222Rn in the depth of 0,8 m
- the available soil porosity (Fp - w) is determined according to (6) by means of the measuredvalues of ESrRn and by the determined values of ARn(z)/z and L
- RAN of the investigated area is calculated according to the relation (7).
References
[I] Holý K., Matoš M., Bôhm R., Stanys T., Holá O., Polášková A.: Acta Phys. Univ.Com.,Vol.XL,(1999) 95-103
[2] Dôrr H., Miinnich K.O.: Tellus, 42 B (1990) 20-28[3] Tanner A.B.: Rad.Prot.Dos., Vol.24 (1988) 79-83[4] Klasifikace zemin pro zakládání staveb. CSN 73 1001[5] Holý K., PoláSková A., Baranová A., Holá O., Sýkora I.: In: Proc. Of the 21st Rad.Hyg.Days
(ed.D. Nikodémova), Jasná pod Chopkom, Slovakia (1998), 225-228[6] Holý K., Matoš JVL, Stanys T., Holá O., Polášková A.: In: Zborník prednášok 2.
banskoštiavnických dní, (2001) 124-138
XXIV DRO Demänovská dolina 73

EXPERIENCE WITH CALIBRATION OF IONISATIONCHAMBER WHICH ARE USED
FOR ABSORBED DOSE DETERMINATIONIN RADIOTHERAPEUTICAL
X-RAY BEAMS IN CZECH REPUBLIC
Ivana Horáková, Eva Jursíková, Miroslav Cvach, Helena ŽáčkovaNational Radiation Protection Institute (NRPI)Šrobárova 48,100 00 Prague, Czech Republic
INTRODUCTIONThe demand for high accuracy of the absorbed dose given to patient in radiotherapy (theuncertainty should not exceed 5 %) calls for precise determination of the dose rate to waterunder reference conditions. To reach the given demands only precise, low level energydependent and stable ionisation chamber instruments can be used for measurement inradiotherapeutical X-ray beams. To ensure that the ionisation chamber fulfils these requirementsin the long-term period it is necessary - among others - to perform regular calibration of theinstrument in the metrological laboratory. The air kerma calibration factors NK and the energydependence coefficient kE for the ionisation chamber should be regularly determined.Calibration of ionisation chamber instruments which are used for absorbed dose determinationin radiotherapeutical X-ray beams is carried out by X ray laboratory of the Radiation dosimetrydepartment of NRPI.
X-ray laboratory NRPI has a statute of the authorised metrological centre - AMS-K110. Since1988 it has been pursuing verification and calibration of instruments in the area of radiation ofX energies from 0.8 fJ up to 40 fl. Thought it serves for subjects from different fields ofradiation protection, the most demands come from the health service sector. It is given by therequirements of Atomic law which has been adopted in'1997 and which pays attention also toradiation protection of individuals in relation to medical exposure. Its demands have supportedthe requirements of other important laws - 505/1990 Sb. (metrological), its amendment119/2000 Sb. and in the regulation of Ministry of Industry and Trade no. 263/2000 Sb. In thislegislation the rules for verification of devices used for measurements of absorbed dose in thebeams of therapeutic and diagnostic sources have been adopted (among others)
Experience with the regular calibration of ionisation chambers obtained in X-ray laboratoryNRPI is presented in the paper. The attention is focused on the long term stability of energydependence coefficients kufor the most typical ionisation chambers used in the Czech Republic.
MATERIALS AND METHODSCalibration of the dosimetrical systems (ionisation chamber together with readout system)which are used as local standards at radiotherapy department in Czech Republic is performed interms of exposure and air kerma at chosen qualities in the effective X ray energy ranges from 5keV (30 kV) to 160 keV (300kV). The X-ray equipment used - an Isovolt 400, has been adaptedfor use in metrology and has two X ray tubes. One of the tubes has an inherent filtration of 3mm Be and can be supplied with HT ranging from 5 to 150kV constant tube potential, and theother has an inherent filtration of 4 mm Al and HT ranging from 60 to 400 kV.
The types and number of ionisation chamber used together with readout system type UNIDOS(the mostly used type at radiotherapeutical department in CR) - are listed in Table 1.
XXIV DRO Demänovská dolina 74 SK02K0183

Table 1 :
Producer
PTW
MINIRADNE
type
300013000230006
2336412334223344
MR 21012571A
number
61226141
number of calibrationssince 1995
21333125163
RESULTS AND DISCUSSIONSince 1995 about 70 calibrations of ionisation chamber with UNIDOS readout system havebeen carried out and energy dependence has been estimated for each calibration. As thecalibration of the local standards should be repeated each year (according to the demand ofmetrological law) we have obtained data from which the long term stability of the ionisationchambers used in CR could be evaluated. However, not all users did adhere the requirements ofthe metrological law, they haven't calibrated their local standard every year and therefore thetotal number of calibrations is less than it should be.
In Fig.l and Fig.2 energy dependence of the two representatives of the ionisation chambers ofthe types M30001 and MR 2101 (the mostly used types in CR) are presented. In two figures thedependence kE on the X-ray beam quality obtained since 1996 to 2000 for both types ofionisation chambers are pictured respectively.
Figure 1:
1.051.041.031.021.01
10.990.980.970.960.95
Ion chamber M30001 - S/N 171
50 100 150 200 250 300 350
U[kV]
XXIV DRO Demänovská dolina 75

Figure 2:
1.051.041.031.021.01
10.990.980.970.960.95
Ion chamber MR2101- S/N 109
4L '
ILL.— ut - • • •
0 50 100 150 200 250 300 350 400
U[kV]
In Fig.3 and Fig.4 the energy dependence - kE on the X-ray beam quality - as it was measured inthe year of 2000 for 7 different ionisation chambers of two main types - M30001 and MR 2101(4 and 3 ion. chambers respectively) are compared. The values kE for different energies of eachionisation chamber were normalised to kE for 200 kV to enable compare energy dependence ofdifferent ionisation chambers.
Figure 3
1,051,041,031,021,01
kE1,000,990,980,970,960,95
Ion chambers M30001 in the year 2000
-•—S/N658-H»~ S/N 171-á;--S/N 817~-«K—S/N801
50 100 150 200 250 300 350
U[kV]
XXIV DRO Demänovská dolina 76

Figure 4:
1,06
Ion chambers MR2101 in the year 2000
S/N 112S/N114S/N 109
250 300 350
U[kV]
Though the energy dependence of both main types of ionisation chambers is fairly good it isapparent that the energy dependence also the long term stability kE under 150 kV is worse forthe MR2101 type when it is compared to the same data of the M30001 type.
CONCLUSIONSWithin a given chamber type, chamber-to-chamber variations in energy response can besignificant and each individual dosimetrical system should be calibrated at a range of beamqualities suitable to allow interpolation to the clinical beam qualities.
It can be concluded that the long term energy dependence stability of the of type testedionisation chambers of "new generation" which are used in connection with readout systemUNIDOS is sufficient for the absorbed dose determination in therapeutical X-ray beam.For these systems it is possible to recommend prolongation of the term of the calibration fromone year (as it is given in present regulation) to two years term.
The work described here forms only part of the calibrations to be performed on the dosimetersused in radiation dosimetry and protection.At present time - owing to the requirements CD 97/43/Euratom (which defines demands onradiation protection of the patients and which is being adopted to Czech legislation) - increasesthe importance of the NRPI X-ray laboratory: its experience, support and metrologicalbackground is inevitable not only for calibrations of the instruments but also for the type tests,audits, and other services which ensued from new radiation protection legislation.
REFERENCES1. Doporučení SÚJB : Zavedení systému jakosti při využívání významných zdrojů ionizujícího
záření v rádioterapii: Rentgenové ozařovače, SÚJB, 20002. Doporučení SROBF ČLS J.E.P.: Doporučení pro zajištění kvality v rádioterapii, Stanovení
absorbované dávky v referenčním bodě3. Absorbed Dose Determination in External Beam Radiotherapy : An International Code of
Practice for Dosimetry Based on Standards of Absorbed Dose to Water, IAEA, 20004. HJarwinen, A.Kosunen, E.Rantanen: Stability of ionisation chambers instrument:
Experience with recalibration and constancy testing, in Measurement Assurance inDosimetry, Proceedings of a Symposium, Vienna 24—27 May 1993
XXIV DRO Demänovská dolina 77

POSSIBLE RADIATION DOSE REDUCTION BY USING DIGITALX-RAY EQUIPMENTS
Martina Horváthova1'Denisa Nikodémova2, Mariana Príkazshá3,'Faculty of Public Health and Social Care of Trnava University,
Hornopotocna 23, 918 43 Trnava, Slovakia2 Institute of Preventive and Clinical Medicine, 833 01 Bratislava, Sovakia
3General Hospital, 929 01 Dunajská Streda, Slovakia
AbstractThe radiation load of population all over the world from medical examinations clearly
demonstrates the importance of the introduction of the quality assurance and quality controlprogrammes into the activities of radiology departments.
The basic aim of quality assurance program is to ensure that the radiation dose is kept aslow as reasonably practicable while still providing an adequate image quality. As many otherfields, the rapid development of techniques brought change-over from the conventionalanalogue technique to the digital technique. In this process, the conventional X-ray film is beingabandoned and images are being viewed on either laser film or monitor. The main advantages ofusing digital equipment lay in improved image quality and diagnostic accuracy through digitalimage processing, reduction in patients exposure, cost reduction by reduction of the film usage,more efficient storage and retrieval of radiographic images through picture archiving. Severalstudies that have been conducted for comparison of various diagnostic examinations show, thatthere is potential for dose saving in the digital image intensifier technique.
The aim of this study was to compare measured values of dose-area product for coloninvestigations using different X-ray equipment types, two digital and two analogue. Ourmaterial consisted of 169 randomly selected patients, 115 of them were examined with digitalequipment and 54 patients with the analogue equipment. The obtained results have confirmedthe dose reduction and increase of diagnostic accuracy when using the digital equipment, withthe added benefit of a good image quality.
IntroductionThe basic aim of any radiology quality assurance programme is to give the required
image quality at the lowest absorbed doses. The radiologist performing an examination is ableto influence the image quality and to reduce the radiation dose delivered to the patient only inthe case that the information about the real doses is available and hence the comparison withacceptable reference dose levels is possible [ 1 ].
In recent years digital equipments are replacing the conventional X-rays units,especially for fluorography and fluoroscopy examinations. Some advantages of digital X-rayimages are : improved image quality and diagnostic accuracy, saved time, cost reduction,dose reduction, digital storage and picture archivation.The objective of our study was :- to asses the impact of digital imaging of patient doses during barium studies- to compare radiation load during the barium meal and barium enema examinations at 2 digital
and 2 conventional radiodiagnostic equipments- to discuss the conditions of dose reduction by using digital equipment- to optimize the fluoroscopic examinations, so that the required image quality is obtained at thelowest dose
SK02K0184XXIV DRO Demänovská dolina 78

Material and methodsOur investigation were carried out in four different radiodiagnostic units (two digital
and two conventional). The parameters of X-ray units used for barium meal and barium enemaexaminations are given in the Table 1.
Table 1: X-ray equipment used for our studies
Images j..;j/jjj:::jo; - : : ' V •':/•;• •.•-.' :; í , - ;
Generator->: H:: •• t f r -;; ipi : :'•;}•:•;•••;:.ie.
Itnageintéŕisifier,
Fiim.íjpé::;:M:,;;;.;':;;o
Cassette type
Gljnaägít::3:í
tmi:: W-WE
cbrivéňtíónal
tíhiräíux: i: jív
Trinlax';jj'j:.:Jv:J
.ipnýéritíoriaľ
Čhifodiiŕ 125 ;C.
Rók-T:;;::::::;::;jj:;,j:.GKÍroskop 7- :
R é t i ň a :-:ř;;:;:
K Ó d a k . > : . : J : -
Measurement of patient doses were performed using dose-area product (DAP) meterDiamentor E (PTW Freiburg) with a flat transparent ionisation chamber No. 57523(17x18,5x1,7 cm) mounted directly on the X-ray tubes. The ionisation chamber was calibratedat Slovak metrological institute. The cumulative DAP value was recorded and DAP values foreach radiograph determined. In the survey following data were collected: name, age, sex,weight and height of patient, kV, time of examination, number of radiograph and the name ofradiologist. The data of examined patients are shown in the Table 2 and in Table 3.
Table 2: Description ol'patient data inbarium meal examination
Table 3: Description of patient data inbarium enema examination
.;.,.;..;:1vV:i,:.;
•• 2::, * ; ;
•:.:,-;3. 'r:,;• • : . • : - ' A ••:,-,
J:rNQi;:OfJ!:pŠfJefiis• •'••;:22;v;jj
: •• V29..J- : j
,:'ji6jjr:j
Ráíieriís (ííiešíi^ŕangfe))Agelyear):;43 (2cŕľ6)ŕ.::36.,{2:1#1);.58(23-82)5Q:(Í8~79X:j
.66;(38-106):
J71:Í53Í97).
[ Hospita l
••••*.<;•'••-••'•:;?.}-.'••.•'••• ••••-
•••Mpfý/éifrj:|5aiienís"vh:2zm
Patle nts (rn eá n (rársge))AgôJíyQ:ar)lW/eÍgr!í ítcgy•43{ié-68)ř
:62i(34-83)i.69(45-98)71: (50-105).
The images quality in all cases was evaluated by the same senior, well experienced radiologist.
ResultsThe total DAP values recorded in barium enema and barium meai examinations, the
fliioroscopic time and the number of radiographs are summarised in Figure 1 and Figure 2.
H2.
Figure I: Dsitribution of DAP, fluoroscopic time and No. of radiographs for barium enemaexamination
1b10
b
0
I • •
"
Time ofexamination
,
No. of DAP (Gy.cm2)radiographs
XXIV DRO Demänovská dolina 79

3D -
25
20
ľ i -
10 -
5 -
0 -Time of examination No. of radiographs
-
í '
''-'/I- *"
*% "* .
DAP (Gy.cm2)
1HdigitalB conventional
Figure 2: Distribution of DAP, fluoroscopic time and No. of radiographs for barium mealexamination
From the figure 2 it can be seen that the DAP value is lower inspite of more radiographsperformed during the digital examinations.
The summary of the results for barium meal and barium enema examinations can beseen in the Table 4 and Table 5. The statistical analysis of the obtained results show thedynamic nature of this type of diagnostic examination. Therefore the significant statisticaluncertainity is observed in the given mean values.
Hospital
' • • : ! ' "
: % • -
- 3 '•'4
Table 4: Summary of the results
No. , ofpatients
32' 29
, : 1 6 - •
• -38
for barium meal examinations\ / JDose-áreá product £Gýcni2);- • , -
'roin.
•2;44 •. !
' 2,99 ',
i,72<.''1,45 '
lsťquartíle
'• 5.21-"r'é,94 '• 'Í2,t •'• "-•5,92 ••
. • m£\ •1 ;,,395;..':
30'55, - '
., median.
^•:'/ôt7i: '-"';12416'V;
9,54.
; .;• 15,93' '
" ;48ľi 8,' i%29-
max.
39.51 -26,7 ľ
.154,22' 46,47
Table 5: Summary of the results for barium enema examinations
Hospital
"i:
, : " i •
No. of patients
" •. 2232
,. _ ,, ; , ,Dose-are;a ̂ rodáci ((3ýaaz)'_ •',
. rain.-
• ' 3,75.' "•3,73"
1st quártííě
• " 8,09' •'9.21 -"
•• mean; •
- 1 4 , 1 9 •'.'
median.'
•VJ0,54'- '
'"12,17
• qijairtile.,-' "16,66V '-' 15,66 '
max. "
': 26,23" 33.38
In the Figures 3 the dependence of DAP values from the patient's weight during bariummeal examination in digital system is shown.
XXIV DRO Demänovská dolina 80

20 40 60 80
weigh of patient (kg)
100 120
Figure 3: DAP vs weight of patient for barium meal examination (digital)
ConclusionsThe preliminary results, presented in our paper for comparison of radiation load of
patients examined by digital and non digital X-ray units, have shown:• significant reduction of DAPs can be achieved using digital equipment for fluoroscopy and
fiuorography examinations;• the mean DAP value in the 3rd quartile for barium meal examination (12,8 Gy.cm2) for
digital equipment is less by a factor of two comparing with DAP value for conventional unit;• the DAP measured during our survey have shown substantial variation and it is not easy to
quantify and to standardize all parameters influencing the patient's dose• barium enema and barium meal examinations represent about 14% of all examinations in
Slovakia. Considering the radiation load connected with this examination it is worth tocontinue in its optimisation.
References
[1] Broadhead,D.A., Chapple,C.L., Faulkner.K. The impact of digital imaging on patientduring barium studies, The Br.J.of Radiol. 68 (1995) 992-996
[2] Warren-Forward,H.M., Haddaway,MJ., Temperton,D.H., McCall I.W. Dose-areaproduct readings for fluoroscopic and plain film examination, including an analysisof the source of variation for barium enema examinations, Br.J.of Radiol. 71 (1998)964-967
[3] Príkazská,M., Nikodemová,D., Horváthová,M. Morbus-crohn advantages of digitalexaminations, 32th Slovak Radiological Congress, Bratislava, April 25-28, 2001
XXIV DRO Demänovská dolina 81

Diagnostic reference levels (DRLs) for radiopharmaceuticalsadministered in nuclear medicine — four-year experience with their use
Václav Husák, Pavel Koranda, Zuzana Pásková X), Karia Petrová J),Zdeněk Prouza J )
Department of Nuclear Medicine, University Hospital and Palacký University, OlomoucState Office for Nuclear Safety (SONS) l), Prague, Czech Republic
Introduction of DRLs levels in Czech Republic (CR). DRLs were established fouryears ago using the results of the national questionnaire survey on the type and amount ofadministered radiopharmaceuticals (RP) performed during 1996. DRLs were implemented inSONS Regulation No. 184/1997 Coll. for 92 nuclear medicine (NM) procedures, e. g. for " m Tc-phosphates bone scintigraphy DRL was 800 MBq, for "mTc-HMPAO brain scintigraphy 800MBq, for "mTc-MIBI planar scintigraphy of myocardial perfusion 600 MBq, for 2OIT1 SPECTmyocardial perfusion 110 MBq, for ""Tc-DMSA kidney scintigraphy 200 MBq etc.
DRLs guidelines. In order to facilitate the implementation of DRLs into the clinicalpractice an explanatory information (guidelines) was prepared about the purpose, significanceand correct use of DRLs; the principles givert in BSS [1] and ICRP 73 [2] were taken intoaccount.
There are two inappropriate regions of administered activity of RP to patients. The upperinappropriate region is connected with a unnecessarily high radiation burden of a patientwithout improving a quality of scintillation camera images. The lower inappropriate regionresults in a poor image quality which may lead to serious diagnostic errors and/or repetition ofan examination. DRL indicates the upper boundary of the region of acceptable practice in whichthe optimal activity of RP administered to a patient is chosen according to the scintillationcamera geometry (I, 2, 3 detectors), collimators, time available for the examination etc.; optimalvalue of RP activity below DRL should assure the lowest necessary dose to achieve thediagnostic information needed.
DRLs are applied to a typical 70 kg patient and should be adjusted to account forsignificantly under-weight and over-weight patients. Activity A of RP administered to a patienthaving a weight W different from 70 kg (< 60 kg and > 85 kg) is recommended to becalculated as A = A70 x F where F = W°7/70 is the scaling factor derived from body surfacearea. Factor F for children is practically identical with that given in the known EANMrecommendation [3]. Thus, activities recommended to be administered to children and adults aredetermined consistently on a body surface area basis.
Our guidelines points out, in accordance with BBS [1] and ICRP 73 [2], that DRL is not alimit which could not be exceeded. DLR should not be exceeded in routine clinical practice;higher levels are acceptable in individual - relatively rare cases - which are justifiable by apatient's clinical condition (other diseases, complications etc.).
Check of DRLs practical use. With regard to the prepared amendment to SONSRegulation No. 184/1997 it has been necessary to check how DRLs have been respected inclinical practice. Therefore, two surveys were conducted in 1998 and 2001.
The first more detailed questionnaire circulated to 49 departments of NM in CR focussedon three major topics: an observance of DRLs in clinical practice, a method used for thedetermination of RP activity administered to patients having a weight different from 70 kg and apercentage of examinations in which DRLs had to be exceeded on clinical grounds (with theexception of examinations requiring administration of higher activities due to a patient's weightabove 70 kg). The complete response rate was 82 % (40/49).
26 departments which had no remarks on DRLs in SONS Regulation No. 184/1997 weresupposed to adhere to them without difficulties. The remaing ones complained that DRLs forsome examinations were too low: whole-body planar 67Ga scintigraphy 150 MBq, thyroid gland" m TcO 4 scintigraphy 150 MBq, whole-body scintigraphy (tumours) with 9 9 mTc labelledmonoclonal antibodies 500 MBq and others.
XXIV DRO Demänovská dolina 82 SK0PK01 ŕtó

33 departments reported the use of the known procedure recommended by EANM [3] fordetermining RP activities administered to children and of that for persons having weight higherthan 85 kg which was recommended in our DRL guidelines mentioned above. Only 5departments determined RP activity according to a patient's weight.
23 departments announced no cases of exceeding DRLs with regard to patient's conditionand other circumstances. The estimate of a percentage of these cases given by 17 departmentsranged from 0.5 % to 10 %.
The second questionnaire was distributed in 2001 several months ago before working outthe first proposal of the table containing modified values of DRL to be included into theamendment to SONS Regulation No. 184/1997 Coll. The purpose of this survey performed afteralmost three years since the first one was to find out latest comments on DRLs.
Of 49 departments only 20 ones answered; the low response rate was not a surprisebecause in our covering letter no reply was required in case that a department was satisfied withDRLs and had no comments.
Of 20 replies 5 ones contained no remarks, answers of remainig 15 departments helped usto improve the table for the proposed SONS Regulation.
DRLs in the amendment to SONS Regulation No.184/1997 Coll. Table 1 containsDRLs proposed to be included into the amendment to this regulation. Using the results ofquestionnaires and, in some cases, regarding DRLs valid abroad [4, 5, 6], too, the followingchanges were performed:
- eight new radiopharmaceuticals and examinations were included (18F-FDG, 123I iomazenil,123IIBZM, examination of sentinel nodes and others;
- DRL was increased for eight examinations: 9 9 mTc0 4 scintigraphy of thyroid gland from 150MBq to 200 MBq, "mTc-MIBI planar scintigraphy of parathyroid from 400 MBq to 750MBq, 99mTc-antibodies tumours and inflammation imaging from 600 MBq to 800 MBq etc.;DRL was decreased for seven examinations: " m TcO 4 or 99mTc-DTPA dynamic brainscintigraphy from 800 MBq to 600 MBq,, " T c - M A A , microspheres lung scintigraphyfrom 200 MBq to 150 MBq, " m Tc-DMSA kidney scintigraphy from 200 MBq to 150 MBqetc.);
- two examinations, 133Xe lungs ventilation and m I bengál rose chromextr. function of liver,were omitted;some minor modifications were carried out to improve the arrangement of the table.
The increase in DRLs for some examinations was substantiated very carefully taking pains tocounterbalance it by their decrease for other examinations where reasonable.
Conclusion. The use of DRLs, as a component of a Quality Assurance Programmesupervised in departments of NM by SONS, appears to aid in the optimisation of radiationprotection for patients undergoing N M procedures.
References[1J Safety Series No. 115: International Basic Safety Standards for Protection against IonizingRadiation and for the Safety of Radiation Sources. Vienna, IAEA 1996.[2] ICRP Publication 73: Radiological Protection and Safety in Medicine. Annals of the ICRP,26, 1996. Oxford, Elsevier Science Ltd. 1996.[3] Paediatric Task Group of the European Association of Nuclear Medicine (EANM): Aradiopharmaceutical schedule for imaging in paediatrics. Eur. J. Nucl. Med. 17, 1990, 127 -129.[4] Notes for Guidance on the Clinical Administration of Radiopharmaceuticals and Use ofSealed Radioactive Sources. Chilton, NRPB 1998.[5] Schtcha, H.: Diagnostische Referenzwerte in der Nuklearmedizin Empfehlungen derStrahlenschutzkommission verabschiedet in der 167. Sitzung der Strahlenschutzkommission am6./7. Juli 2000. Nuklearmedizin 39 (2000), N l 18 - N l 19.[6] Smart, R. C , Towson, J. E.: Diagnostic Reference Activities for Nuclear MedicineProcedures in Australia and New Zealand. Rad. Prot. In Australasia 17, 2000, No . l , 2 - 1 4 .
XXIV DRO Demänovská dolina 83

Table 1 Proposal of diagnostic reference levels in nuclear medicine to be includedin amendment to SONS Regulation No. 184/1997 Coll.
ExaminationOrgan
bone
bone marrow
brain
thyroid gland
parathyroidgland
adrenals
lungs
heart
lymphaticsystem
vessels
Kind, groupscintigraphy(whole - body, three - phases,SPECT)scintigraphy(whole - body, SPECT)scintigraphy
dynamicplanarSPECT
receptorsglucose uptake
cisternography
uptake
scintigraphy
planar
whole - body, SPECT Cin carcinoma of thyroid ~<gland [_
scintigraphyplanar
scintigraphyplanar
scintigraphyventilation
perfusion staticSPECT
myocardial imaging(SPECT)
reinjectionviability
ventriculographyfirst passradionuclidelymphographysentinel nodesfibrinogen uptakeradionuclide venography(one extremity)
radionuclide angiography
thrombus detection
Radio-nuclide
Tc-99m
Tc-99m
Tc-99mTc-99mTc-99m
1-123F-18
In-I l lYb-1691-131Tc-99m
Tc-99mTc-99m1-1231-131Tl-201Tc-99m1-131Tl-201
Tc-99m •Tc-99mTl-201
1-123
1-131
Tc-99mKr-81mTc-99mTc-99mTc-99mTl-201Tl-201F-18Tc-99mTc-99m ,.
Tc-99m
Tc-99m1-125Tc-99m
Tc-99m
Tc-99m
Substance,chemical form
phosphates
nanocolloids
TcO4, DTPATcO4, DTPATcO4, DTPA,HMPAO, ECDIomazenil, IBZMF-18-FDG
DTPAEDTAiodideTcO4
TcO4
MIBI, DMSAiodideiodidechlorideMIBI, DMSA (V)iodidechloride
TcO4
MIBIchloride
MIBGnorcholesterol,MIBG
aerosol, technegasgasMAA, microspheresMAA, microspheresMIBI, tetrofosminchloridechlorideFDGerythrocytesTcO4, HSA
nanocoloid
nanocolloid
MAA
DTPA,erythrocytes, TcO4,DTPA,HSAplatelets
DRL[MBq]
800
550
600600
800200400
4040
0.540
200400
207
80600300100
200750
80
200
20
10006000
150300
100011040
500800900
150
1003
200
300
800500
XXIV DRO Demänovská dolina 84

blood
spleen
hepatobiliarysystem
GIT
kidneys
urinarybladder
testes,scrotumtumours
inflammations
volume of blood andcomponents
survival and local destructionof blood elements
iron metabolismscintigraphy planar
SPECTscintigraphy
planarSPECTdynamic
scintigraphy of salivary glandsoesophagus motilityoesophageal refluxgastric emptyingMeckeľs diverticulum imagingGI bleedingdetermination of blood andalbumin loss in GIT
Schilling testone — probe renographyscintigraphy
planarSPECT
dynamicEPPL, GFR determination
radionuclide cystographydirectindirect
scintigraphy
scintigraphy (planar, SPECT)
scintimammography(planar, SPECT)scintigraphy (planar, SPECT)
Tc-99m
1-131Cr-51Cr-51In-111
Fe-59Tc-99mTc-99m
Tc-99mTc-99mTc-99mTc-99mTc-99mTc-99mTc-99mTc-99mTc-99mCr-511-1251-131
Co-571-131
Tc-99mTc-99mTc-99mTc-99m1-131Cr-51
Tc-99mTc-99m
Tc-99m
Tc-99mIn-Il l
Ga-67Tl-2011-1231-131F-18Tc-99m
Tc-99mTc-99mIn-IllGa-67
HSA
HSAerythrocyteserythrocytes, plateletsplatelets
Fe(III) citrátdenatured erythrocytesdenatured erythrocytes
colloidscolloidsIDA derivatesTcO4
colloidscolloidscolloidsTcO4
erythrocyteserythrocytesHSAHSA
monocyanocobal aminhippuran
DMSA (III), gluconateDMSA (III), gluconateDTPA, MAG3, ECDMAG3, DTPAhippuranEDTA
TcO4
MAG3
TcO4
MIBI, antibodiesantibodies,pentetreotideOachlorideMIBGMIBGFDGMIBI, tetrofosmin,phosphonatesleucocytes, HIGantibodiesleucocytesGa3+
80
666
10
3100200
150300250100605050
400700
466
11
150250250
200.53
50200
400
800
120300100400
20750
800600800
30200
XXIV DRO Demänovská dolina 85

COMPARISON OF VENTILATION MEASUREMENTTECHNIQUES IN REAL CONDITIONS
Kareljílek, Ladislav TomášekNational Radiation Protection Institute, Šrobárova 48,110 00 Prague, Czech
Republic
Ventilation and radon entry rate are the only two quantities that influence on indoor radonbehaviour. In order to investigate the effect of ventilation and radon entry rate on indoor radonbehaviour separately, the Institute was equiped with continuous monitor of carbon monoxide(CO). Carbon monoxide serves as a tracer gas for the determination of air exchange rate.
The use of a continuous radon monitor and the continuous monitor of CO gas at the sametime enables to measure the radon entry rate and the air exchange rate separately.
This paper summarizes results of comparison of the following three basic methods [1]performed in real living conditions:
constant decay methodconstant tracer methodsteady rate of tracer injection
to determine the air exchange rate for 22 Rn and CO gas, which were used as tracer gases.
References:
[1] Awbi.H.B : Ventilation of buildings, Chapt.3,82, 1991
SK02K0186XXIV DRO Demänovská dolina 86

Discharge radionuclides into the environment in DIAMO s.p.-o.z.GEAM Dolni Rozinka, o.z. SUL
Ing.Miroslav Jurda, Ing.Jana ŠeflováState Office for Nuclear Safety, Senovážnénáměstí9, Praha 1
DIAMO s.p.-o.z. GEAM Dolni Rozinka is last plant in the Czech republic, where mineand milling uranium ore is in an operation.
Activity MAPE Mydlovary milling plant was ceased in 1991. Decommission anddecontamination is currently under progress.
The poster summarize discharge radionuclides into the environment from workplacesand it is give it to contrast with licences of State office for nuclear safety.
1.Discharge into the environment during the release into the surface waterTwo decontamination stations mine waters are on site in GEAM o.z. an operation (DS
Rl and DS Bukov). One decontamination stations is on site in MAPE Mydlovary. All haveowned the licence of Office for discharge in accordance with Act No.18/1997 Coll. "AtomicLaw" and regulations SUJB No. 184/1997 Coll. on radiation protection requirements.Table 1. , 2. and 3. summarize average and maximal volume radionuclides in release waters
Tab.l.-DSRl
Q (m3 /year)
Vm (mg/1)2ÄRa (mBq/1)
1996
1612 835
0
0,075
56
max
0,151
120
1997
1 642 709
0
0,077
70
max
0,157
110
1998
1 406 567
0
0,054
78
max
0,116
140
1999
1 452 370
0
0,075
95
max
0,114
110
2000
1516 995
0
0,049
82
max
0,105
130
Tab.2. - DS Bukov
Q (nrVyear)
Unat (mg/1)
"6Ra (mBq/1)
1996
532 589
0
0,025
60
max
0,155
100
1997
555 590
0
0,027
69
max
0,052
150
1998
384 262
0
0,022
89
max
0,040
180
1999
358 761
0
0,015
63
max
0,027
150
2000
425 678
0
0,025
90
max
0,071
100
Tab.3. - DS MAPE
Q (nrVyear)
Unat (mg/1)
" b Ra (mBq/1)
2000
100 353
0
0,042
26
max
0,16
87
XXIV DRO Demänovská dolina 87SK02K0187

investigate level
interference level
Unat (mg/l)
DSR1
0,3
0,51
DS Bukov
0,2
0,3
DSMAPE
0,25
0,3
226Ra (mBq/1)
DSR1
500
1500
DS Bukov
350
500
DSMAPE
200
500
2. Discharge into the environment during the release into the air
The ways of the discharge into the air are:a) Air-shafts from mine (Fig.l.) and millb) Release from the drying uranium concentrate (Fig.2.)c) Deposits uranium ore (Fig.3.)d) Transport uranium oree) Sediment fields (o.z. GEAM Fig.4., o.z.SUL-MAPE Fig.5.).
The licences of Office are for the release from the drying uranium concentrate andsediment fields. Volume activity uranium is monitoring on the release from drying.(Tab.4.) Theinfluence off sources is watching with monitoring network. Dose equivalent rate, volumeactivity long-life radionuclides, radon equivalent equilibrium concentration are monitoring inmonitoring stations and content of uranium and radium are monitoring in dusty-fall.(Fig.8.- 11.)(Tab.4.)
Tab.4. Volume activity uranium in the release into air from drying uranium concentrate duringyear 2000
Av (Bq/m3)
I.
1,8
II.
0,2
IV.
2,14
V.
15,7
VI.
3,2
DC.
5,4
X.
36
XL
185,0
XII.
1.3
investigate level - 60 Bq/m3 interference level - 75 Bq/m3
Tab. 5. Average and maximal dose eqivalent rate (Hx), radon equivalent equilibriumconcentration (EOAR), volume activity long-life radionuclides (OADZ) , content of uraniumand radium in dusty-fall during year 2000
Monitoring place: o.z.GEAM Fig.6, o.z
o.z.GEAM
Hx (M-Sv/hod)
EOAR(Bq/mJ)
OADZ(Bq/mJ)
U in dusty-fall
mg/(m2.30dni)
Ra in dustyfall
Bq/(m2.30dni)
1
0
-
26
0,001
0,102
2,5
max
-
57
0,001
0,111
2,5
0
0,10
11
0,001
0,103
2,84
SUL - MAPE Mydlovary Fig.7
>
max
0,15
26
0,001
0,134
6,24
0
0,08
7
0,001
0,104
2,5
3
max
0,11
11
0,001
0,153
2,5
0
0,12
17
0,001
0.24
2,51
X
max
0,14
26
0,001
2,6
0
0,14
13
0,001
0,101
2,5
max
0,17
14
0,001
2,5
XXIV DRO Demänovská dolina 88

o.z. GEAM
Hx (jiSv/hod)
EOAR(Bq/mJ)
U in dusty-fall
mg/(m2.30dní)
Ra in dustyfall
Bq/(m2.30dní)
6
0
-
11
0,174
2,5
max
-
19
0,235
2,5
7
0
0,15
43
max
0,18
104
8
0
0,63
12
0,9
34,7
max
1,31
16
1,832
72,3
9
0
0,20
13
0,156
3,92
max
0,23
14
0,291
8,04
10
0
1,17
25
0,298
6,78
max
1,50
29
0,820
21,16
investigate level
interference level
Hx EOAR OADZ U in dusty-fall Ra in dusty-fall
(jaSv/hod) (Bq/m3) (Bq/m3) mg/(m2.30dní) Bq/(m2.30dní)
0,7 45 0,01 1 30
1,0 63 0,02 1,5 35
o.z. SUL
MAPE
Hx (uSv/hod)
EOAR(Bq/mJ)
U in dusty-fall
mg/(m2.30dni)
Ra in dustyfall
Bq/(m2.30dni)
1
0
0,22
8,8
<0,20
2,73
max
0,23
13,4
0
0,19
6,8
<0,20
3,69
I
max
0,20
7,8
0
0,16
7,6
<0,20
2,35
5
max
0,18
11,7
4
0
0,20
9,3
<0,20
1,55
max
0,22
17,3
0
0,19
7,6
<0,20
1,47
max
0,20
12,8
o.z. SUL
MAPE
Hx (juSv/hod)
EOAR(Bq/m3)
OADZ(Bq/mJ)
U in dusty-fall
mg/(m2.30dní)
Ra in dustyfall
Bq/(m2.30dní)
6
0
0,17
8,8
0,003
<0,20
5,23
max
0,18
10,1
0,009
7
0
0,21
9
0,001
<0,20
2,81
max
0,22
12,8
0,002
8
0
0,26
9,1
0,001
<0,20
2,95
max
0,27
15,1
0,001
18
0
0,13
5,8
0,001
<0,20
3,38
max
0,15
7,7
0,001
20
0
0,22
4,9
0,003
<0,20
2,63
max
0,23
6,7
0,003
XXIV DRO Demänovská dolina 89

investigate level
Hx EOAR U in dusty-fall Ra in dusty-fall
(uSv/hod) (Bq/m3) mg/(m2.30dn0 Bq/(m2.30dn0
0,3 30 0,3 8
3.ConclusionAccordance care is giving to monitoring in DIAMO s.p.. The results of monitoring
enable to determine the exposure of human population and influence into the environment.Investigate and interference levels are exceed minimally and the licence of Office for dischargeradionuclides into the environment are performed.
XXIV DRO Demänovská dolina 90

PROGRAM "SVAZEK" FOR OPTIMISATION OF RADIATIONPROTECTION AT SHIELDING BARRIERS FOR X-RAY
WORKPLACES
Martin Kadlec, Otto Kodl, Marcela ŽákovaState Office for Nuclear Safety (SÚJB), Senovážnénám.9,110 00 Praha 1
The program "Svazek" is created for Windows users as one of the tools for computation protective barrierX-ray installation. SÚJB initiated creation of such a program to evaluate submitted documentation by aninspector of radiation protection during licensing process. At this time applicant for licence must submitto SÚJB two documents concerning the shielding of X-ray sources. These are the documents required inThe Atomic Act [1]: evidence of the effectiveness of shielding protective equipment (item 4 paragraph b)appendix D) and evidence of optimisation of radiation protection at workplaces (item 4 appendix 1) [1],These documents must meet requirements in Regulation 184/1997 Sb. [2], where the guidance level ofexposure for workers and other persons is described (if it is not exceeded - optimisation is fulfilled) andrequirement for annual effective doses in the spaces adjacent to radiodiagnostic examinationroom for safety management. Program "Svazek" calculates taking into consideration theselegislation requirements, building budget, service life and value of monetary profit. There isused algorithm for the calculation of the thickness of protective barrier according to NCRP 49[3] and for optimisation calculation according to ICRP 37 [4]. The result is thickness ofprotective material such as concrete, heavy spar and heavy spar plaster. Program can be used forradiographic, fluoroscopic and therapeutic X-ray devices.
The program consists of four dialog boxes and two sheets of data results in the graphand the text form. Dialog boxes are "Calculations parameters", "Prices calculations", "Drawingparameters" and "Conversion". The user of the program must fill in all these dialog boxes andthen he can open two sheets with results. Help menu can be used during filling in all dialogboxes and offers options for setting entrance parameters.
"Calculation parameters" are records of shielding materials, information about person(working with sources or others), interval optimisation limits, characteristics of X-ray deviceexpressed by dose, voltage and by supposed extent of operation. This box can be set by twomodes: direct setting and indirect setting. Indirect mode enables the user to set only workingconditions (shielding of primary or scattering radiation, number images per year, dose, voltage)and the program uses for calculation typical values, which are set in advance. Direct modeneeds knowledge of beam characteristics such as scattering factor, angle of scattering, initialattenuation by material "z", which are found in literature. In this dialog there are threepossibilities of setting building materials, which influence the results of program: 1. Solid bricksand heavy spar plaster - the result is in thickness of heavy spar plaster, 2. Concrete - the resultis in full thickness of concrete, 3. Heavy spar - the result is in full thickness of heavy spar.
"Prices calculations" includes data of the shielding material costs, size of the area of thewall, floor or ceiling, the monetary equivalent in Kč/mSv, the option procedure of optimisationoutput according to ICRP 37 [4]or relative data processing (only increments of benefits andexpenses) and option of continuous or discrete function for processing the dependence ofmonetary equivalent on the dose.
"Conversion" - contains three parts. The first part recounts factor "z" following changesin original input material. The second part offers the option to write results in heavy spar orbrick in addition. The third part offers writes results in lead equivalent as well.
"Drawing parameters" enable the users the option of coordinating diagrams and textlocated on two results sheets. There are also two lines for specification of the document and thename of workplaces. In this sheet the user can choose the size of a character, the thickness ofgraphic lines and the contrast of the image.
Two result sheets are named "Evidence of Shielding Optimisation " and consist of thepage number 1 and 2.
XXIV DRO Demänovská dolina 91 SK02K0188

Page 1: Text part includes input data, which are entered by the user and the interval ofoptimisation. This interval is related to distance source and calculated place and its values are inthickness of shielding material for requiring limiting values of effective dose. These values aretranscribed to page 2 for displaying the diagram there. On this page there are two diagrams offunctional dependence of thickness of shielding on the distance from the source: one for lowerlimit and the other for upper limit of entered requirement of effective dose.
Page 2: On this page there is resulting optimisation diagram of functional dependence ofprice on the thickness of shielding material. Resulting optimisation value in thickness shieldingmaterial is given by local extreme of this diagram.
This is brief information about the program "Svazek", that is presented by the poster.Software of this program is further developed according to remarks of SÚJB users.
References1. Law No.18/1997 Coll., on Peaceful Utilisation of Nuclear Energy and Ionising Radiation
(the Atomic Act) and on Amendments and Additions to Related Acts, Czech Republic2. Regulation of the SÚJB No. 184/1997 Coll., on Radiation Protection Requirements, Czech
Republic3. National Council on Radiation Protection and Measurements, Structural Shielding design
and Evaluation for Medical Use of X-rays and Gamma Rays of Energies up to 10 MeV.NCRP report No. 49, Washington, DC, 1976
4. International Commission on Radiological Protection, Cost-Benefit Analysis inOptimisation of Radiation Protection. A report of Committee 4 of the InternationalCommission on Radiological Protection. ICRP Publication 37, Pergamon Press, Oxford,1982
XXIV DRO Demänovská dolina 92

CONTRIBUTION TO THE PENETRATION OF RADIONUCLIDESACROSS THE SKIN. AGE DEPENDENCE OF PROMETHIUM
THROUGH RAT SKIN IN VITRO
Zoltán Kassai1, Vasil Koprda2, Margita Harangozó2, Petra Bendová2 and KatarínaBauerová3
'Weter Research Institute, Nábr. arm. gen. L. Svobodu 5, 849 12 Bratislavadepartment of Environmental Science, Faculty of chemical and food Technology, Slovak University of
Technology, Radlinského 9, 812 37 BratislavaInstitute of Experimental Pharmacology, Slovak Academy of Science,
Dúbravská cesta 9, 842 16 Bratislava
Introduction
Regarding the actual composition of radionuclides absorbed on the surface of the skintissue two practical damages must be considered: absorbed energy of betaradiation in soft tissue, and the extent of penetrated amounts of radionuclidescaused internal contamination.Uptake of radionuclides by skin is fully different in case of intact skin, that it is in
case of damaged skin, being from tens to hundred times higher in case of skin scarified,
burned or wounded [1].
The penetration of radionuciide depends on age of the skin.In this paper:
the time dependence of permeation of l47Pm3+ from aqueous solution through animalskin model was studied,the age dependence of promethium through the skin was proved,the optimum biological model of human skin was selected, andthe relative importance of the main diffusion pathways for I47Pm3+ the diffusion acrossthe intact skin and the diffusion through the hair channels was assessed.
Experimental
The Prn3+ cation was used in the experiments. The radionuciide (I47Pm3+) was used with itshomologe nitrate carrier Nd(NO3)3.6H2O. The experimental arrangement consisted of Franz-type [2] vertical penetration cells (active area 0.8 cm2) completed with fresh skin from theabdominal region from 3- to 12-day-old rats (3DR to 12DR) of the Wistar strain (Breedeingfarm Dobrá Voda, Slovakia). The 3DR to 6DR skins are still hairless and the 7DR to 12DR arehairy.Ions that had permeated throuhg the skin from the donor solution (0.3 ml) to the receptorsolution (7.3 ml, phosphate buffered saline, 1:9; pH 7.4) were determined in aliquots (0.3 ml)sampled at 1,3,5,7,9 and 24 h after starting the experiment. The permeation cells were kept at 32°C during the experiment. The concentration of the carrier in the donor solution was 10"1 %(w/v).The activity applied in the experiment for one Franz-type cell was 790 kBq in 0.3 ml of donorsolution. The radioactivity of permeated 147Pm3+ was measured by liquid scintillationspectrometer (LSC TriCarb 2500 TR, Packard Instrument Co., Meriden, USA) in 5 ml oftoluene scintillation coctail (SLS-31, Spolana, Neratovice, Czech Republic). The permeatedfractions and fluxes were calculated by the PC program PERMEA[3].
XXIV DRO Demänovská dolina 93 SK02K0189

Results and discussion
In Fig.1. is compared the permeation of promethium across skin of different age. Theage of skin markedly influences the penetration of substances into an organism.The values of permeated fractions decrease from 3DR to 7DR and furtherincrease til! 12DR. This proces can be explained with:
with accelerated thickness of the skin before maturation of the skinrising of surface density of folicules, which contribute to the transfolicular
penetration.
147
c0
'•O
u
ted
TO<J>
a>O-
0,001 -0,0009 -0,0008 -0,0007 -0,0006 -
0,0005 -0,0004 -
0,0003 -0,0002 -0,0001 -
0 -
Pm
£11 13D5 S7
3DP 4DP 5DP 6DP 7DP 8DP 9DP 11 DP 12DP
Age of the skin
Fig. 1. Age profiles of permeated fraction of i47Pm across the intact skin from 3DR to 12DR atdonor carrier concentration 0.1 %.
147,
0,0003 -i
0,00025 -
0,0002 -
0,00015
0,0001
0,00005 -
0
Pm
H3DP ®4DP D5DP D6DP H7DP
24
Fig. 2. Time profiles of permeated fraction of 147Pm across the intact skin from 3DR to 7DR atdonor carrirer concentration 0.1 %.
XXIV DRO Demänovská dolina 94

The increasing density of hairs at the oldest rat skins prevent the access of donorsolution to the surface of the skin and is directly proportional to the density offolficules.The results in Fig. 2 and 3 document the discussed facts.
In the Fig. 2 are given the permeated fractions of 3DR to 7DR skin. The permeated fractionthrough the 3DR skin is caused by low thickness of the skin, yet not quite proper forexperimental use as animal model from mechanical point of view. The skin of 4DR and 5DR ismore thick and resistant as documented by decreasing speed of permeation.5DR represents the optimal animal model of human skin as certified in our work as well
as by other authors[4-6].
0,001 -j
0,0009 -
0,0008 -
0,0007 -
0,0006 -
0,0005 •
0,0004 -
0,0003 -
0,0002 -
0,0001 -
0-
147, Pm
H9DP 011DP E12DP
3 5 7
Time (h)
Fig. 3. Time profiles of permeated fraction of I47Pm across the intact skin of 8DR to 12DR atdonor carrirer concentration 0.1 %.
In Fig. 3 are given the permeated fractions through 8DR to 12DR. The higher permetioncomparing to case of 5DR was caused with higher density of follicules. It was applied thetranepidermaly passage of ions of donor solution. In the case of 12DR the more grown hairsprevent the direct contact of the skin with donor solution and consequently the value ofpermeated fraction is lower. This transfolicular permeation contribute to transepidermalpermeation as is with 5DR.
Conclusion
Concluding it can be said, that:- it was proved, that the 5DR represents the optimum animal model to the human skin,- in the case of 8DR to 11DR the dominant route of I47Pm3+ penetration is along the
follicles,- the permeation resistance of the skin depends on the thickness and mechanical
properties of the skin.
Comparing amounts of penetrated ions of promethium through the skin withouth hairs(3DR to 6DR) and through the skin with hairs, it was showed that the additionaldiffusion along hair's follicles pronaunced with animal skin can be important also incase of human skin where hair density is many times lower than in used animal models.
XXIV DRO Demänovská dolina 95

Acknowledgements
This work was partially supported by VEGA grant No. 2/6027/99.
References
[1] Kassai Z., Koprda V., Harangozó M.: Contribution to the penetration of radionuclides acrossthe skin. Concentration dependence of 6 0Co permeation. Journal of radioanalytical andnuclear chemistry, Vol. 242, No. 2, 1999, p. 561-563.
[2] Franz TJ.:Percutaneous absorption on the relevance of in vitro data. J. Invest. Dermatol. 64,1975, p. 190-195.
[3] Boháčik, Ľ.: Vply chemických urýchľovačov permeácie a chemických foriem liečiv natransdermálnu permeáciu, dizertačná práca PGS, Farm. fak. UK v Bratislave, Kat.analyt.chémie, 1996, s. 6-19.
[4] Hadgraft J.: Recent developments in topical and transdermal delivery. Eur. J. Drug Metab.Pharmacokinet. 2, 1996, p. 165-173.
[5] Koprda V., Harangozó, M., Boháčik Ľ.: Permeation of Cs+ ions across skin barriers. J.Radioan. Nucl. Ch. Ar. 229, 1998, p. 91-93.
[6] Bauerová K., Kassai Z., Koprda V., Harangozó M.: Contribution to the penetration ofradionuclides across the skin. Concentration dependence of strontium through the skin invitro. Journal of applied toxicology, 21, 2001, p. 241-243.
XXIV DRO Demänovská doli na 96

SIMULATION OF THE PHOTON FIELDS AND DOSEDISTRIBUTIONS FOR BRACHYTHERAPY SOURCES
7. Klusoň1], P. Švihla, T. Čechákl)
} ČVUT v Praze, Fakulta jaderná a fyzikálně inženýrská, Břehová 7, 115 19 Praha 1
Introduction
Brachytherapy represents one of important methods of cancer treatment. About 10radioisotopes have applications in clinical brachytherapy according to the some specificrequirements for the physical properties of radionuclides proper for clinical practice [1]. Inaddition to widely used sources for brachytherapy (226Ra, 137Cs, 198Au, 192Ir, I) some newsources were developed during the last years (103Pd, 145Sm, 241Am, 169Yb) that exhibitcharacteristics more approaching ideal requirements [1, 2]. For brachytherapy treatmentplanning and optimisation, some source characteristics are necessary. Very importantparameters as dose rate depth distribution and dose distribution isotropy can be calculated usingMonte Carlo photon transport simulation. The model of the 145Sm source in air and water andtissue spherical phantoms described in MCNP4B code is refereed and examples of calculatedresults are presented.
Model and calculations
Three arrangements were described by MC model (using MCNP4B code): I45Sm sourcea) in the free air, b) in the spherical water phantom with diameters 15 and 20 cm and c) in thespherical tissue phantom with diameters 15 and 20 cm. Source description was based on the NPIASCR Řež prototype construction (cylindrical source <j)0.6x3 mm in chemical form Sm2O3, inTi encapsulation [3]). Emission spectrum of 145Sm was taken from [2]. Average photon fluxesenergy distributions at distances 0.35, 0.5, 0.7, 1, 1.5, 2, 3, 5, 10, 15 and 20 cm for all threearrangements were calculated (thereby also photon spectra are available) and desired dosimetryquantity (dose rate) was recalculated from the spectra. To calculate the dose rate spatialdistributions, the sets of point/ring detector tallies were defined for the same individualdistances from source centre (see above). Ring detectors use expected photon field symmetrywith respect to source longitudinal axis.
Results
Calculated average dose rates per unit source activity as function of distance from thesource are shown in the Fig. 1 (presented data are for the 20 cm diameter phantoms, shape ofcurves for 15 cm water and tissue phantoms are the same up to distance 10 cm and thendecrease slightly more quickly).
For calculation of the irradiation plans, the fit of tissue attenuation function was proposedby Meisberger et all. [4]. The ratio of the dose rate depth distributions in water and air is fittedby the 3rd order polynomial. This ratio was derived from the calculated data and fitted bycorresponding polynomial. Results are shown in the Fig. 2. Fit by 4th order polynomial isproposed as better namely for the shorter distances from the source. Calculated polynomialcoefficients are presented in the Fig. 2 legend. Data can not be reasonably fitted by functionproposed by Van Kleffens [5].
Calculated photon flux spatial distributions (symmetrical with respect to the longitudinalaxis) are in the Fig. 3. Data are normalised to value on longitudinal axis normal in the sourcecentre. Small asymmetry (apparent namely for angles up ±70 deg) corresponds to fact, thatsource encapsulation is not fully symmetrical with respect to transverse axis. Data calculated for
XXIV DRO Demänovská dolina 97 SK02K0190

m
>,(3a.
c
t_O)Q.
CO
0 . 1 -•••
Ä 0.01 -—
g 0.001 —TJ
g"10)S 0.0001 -ľ3
(DO
1e-05
1
L
1i;
ísSšj—-
j 145-Smair — a — •
tissue (sphere r=20cm) — e —water (sphere r=20cm) —-n—
ii!"" """ "~"
:
"
;
~ a
6 8 10Distance from source centre [cm]
]45r
12 14 16
Fig. 1 Calculated average dose rates depth distributions for Sm source
1.4
1.2 - •
-I __
3 0.6 —
0.4 -
0.2 -
1
X -r
145-Sm• wate
P4(9
r (sphere r=20
.04883, 2.0386
.954416-1,3.0
cm) to air (calculated data)
8e-1, -3.76040e-2,1.39523e-3) - Meisberger
3886e-1, -7.409866-2, 5.608386-3, -1.46434e-4), , : , ( 1
12 14 164 6 8 10
Distance from source centre [cm]
Fig. 2 Calculated ratio of dose rate in water (water phantom diameter 20 cm) to dose rate in air5Sm source and polynomial fits of this dependencevs. distance from 1 4 5 c
XXIV DRO Demänovská dolina 98

the distance 60 cm are in very good agreement with directional emission characteristicpreliminary experimental results.
110
100 -
z
-90 -80 -70 -60 -50 -40 -30 -20-10 0 10 20 30 40 50 60 70 80 90angle to longitudinal axis normal in source centre [deg]
Fig. 3 Relative photon flux angular distributions for distances r from source centre (source in air, normalised to value on longitudinal axis normal in source centre)
145,Sm
Conclusion
I45rThis work was done as supporting study oriented to ""Sm brachytherapy sourcesproduction and application. Results show that computational methods can bee effectively usedfor simulation, calculation and analysis of brachytherapy sources characteristics and dosimetricproperties. In the next step study should bee supplemented with more experimental verificationand with updated calculations, taking into account possible radioactive contaminants in the145,'Sm source.
References
[1] Mould, R. F., Battermann, J. J., Martinez, A. A., Speiser, B. L.: Brachytherapy fromRadium to Optimization, Nucletron International B. V., ISBN 90-5353-035-5, 1994.
[2] Fairchild, R. G., et al: Phys. Med. BioL, Vol. 32, No 7, 847 - 858,1987.[3] NRI ASCRŘež, Report No. CH10777, 1996.[4] Meisberger, L. L., Keller, R. J., Shalek, R. J.: Radiology 90, 953 - 957, 1968.[5] Van Kleffens, H. J., Star, W. M.: Int. J. Rad. Oncol. Biol. Phys., Vol. 5, 557 - 563, 1979.
XXIV DRO Demänovská dolina 99

ALARA PRINCIPLE IMPLEMENTATIONON THE TEMELÍN NPP
Petr Koláček, Jaroslav Hak, Mí VokálekČEZa.s. - Human Resources Training and Development Section
Temelín NPP - Department of Health Physics
Introduction
A new original procedure on the reasonably achievable norm of radiation protection wasimplemented in the Temelin NPP. The procedure is fully in line with the requirements of act18/97 Coll. (so called „atom act" of the Czech Republic). This procedure is called the ALARAsystem (as low as reasonably achievable). It comprises five components:
• personnel preparation and education," input data,• ALARA tool,« results and• assessment.
The ALARA system was implemented in December 2000 and it proves the optimization ofradiation protection for activities performed within the controlled area of the Temelin NPP.Next step in the process implementation was the establishment of an ALARA committee inMay 2001. This committee serves as an advisor to the director of production concerning theapplication of the ALARA principle to all activities that can affect the optimization of radiationload of NPP personnel, population, or environment.
Personnel preparation and education
The ALARA system concerns all workers who enter the Temelin NPP controlled area. That iswhy it is a part of training needed for working in the controlled area. There exists a specialcourse for ALARA experts in length of 160 hours managed by the human resources training anddevelopment section
Input data
The ALARA committee provides underlying data for calculation of the CDE, information onfinancial costs and radiation waste production.The ALARA system evaluates selected activities performed within the controlled area. The aimis to monitor the CDE and the financial costs of radiation protection of these selected activities.The expected values of the CDE for the following time period are loaded to the ALARA systemdatabase.The activities are selected from two standard points of view:1. All activities where participating workers who are exposed to IDE > 80 fiSv per month.
This selection provides optimization of all activities where participating workers whoare exposed to IDE > 1 rnSv per year. The value of the IDE standard is temporarilyreduced to 40 uSv.
2. All activities performed in the containment during an outage.There were 71 activities monitored by this way up to 1 June 2001. ČEZ in cooperation with itssuppliers has been the authors in cooperation with representatives of ČEZ and its contractorssuggested performance alternatives for these 71 activities. An alternative is characterised by achange of procedure, that represents a different CDE and / or different costs of radiation
XXIV DRO Demänovská dolina 100 SK02K0191

protection. The aim of the ALARA system is to collect appropriate information on everyalternative of the procedure and to prepare the way of its selection and evaluation.
ALARA tool
The information in the database of activities and their alternatives is evaluated by the originalcomputer program OptimCOD, that was developed by Human Resources Training andDevelopment Section, ČEZ a.s. The OptimCOD generates combinations of the activities andtheir variations for arbitrary selected time period. The aim is to find such a combination thatmeets the following:1. The same or lower value of the year by CDE reached by presently used performance of
activities2. The minimum of the overall cost, i.e. the total of the radiation protection costs and of the
health detriment costs (CDE).The combination that meets the requirements above, is taken as optimum and guaranteesreasonably achievable radiation protection level in the Temelin NPP. The optimum solution waschosen from 48 combinations that were prepared for 71 selected activities. To put this optimumsolution into praxis and to supervise its function is the responsibility of the ALARA committee.
Results
The selected optimum solution is realised during the activities performed in the controlled area.Continuous of evaluation combinations, adding of further activities, updating of the appropriateIDEs and costs of radiation protection means further application of OptimCOD program. Theoutput of the OptimCOD provides a possible new optimum solution. This process is a proof ofreasonably achievable level of radiation protection in NPP Temelin.
Assessment
The Temelin NPP is in the stage of an active testing at present. That stage is characterized bylow power of reactor, which means low IEDs. In spite of that, the realization of the selectedoptimal solution reduced the month by CDE by 260 |JSV, which means approximately 25 % ofthe month by CDE. The aim of the ALARA system is to meet the essential requirement of theact 18/97 Coll. § 4 („atom act" of the Czech Republic), as quoted: „The level of the radiationprotection must be such that the risk of endanger of human life, health and environment wouldbe so low that it is reasonable achievable considering economical and social points of view."
Abbreviations
ALARA - as low as reasonably achievableCDE - collective dose equivalentIDE - individual dose equivalentNPP - nuclear power plant
XXIV DRO Demänovská dolina 101

AppendixTable of month by CDE and number of people who entered the controlled area in theTemeiin NPP from October 2000 to May 2001
' CDE and number of people who entered to controlled, areaMonthNumber of people intheCA ;{ }CDE [mSv]
X.001043 \
0,879
XI.00; 988
1,147
XII.00783\,
0,596
1.011088
0,785
11.011.115,
1,144
111.01823
0,894
IV.01725
0,731
V.01855
1,202
n, 1200O £€ ra 1000
•Q. "5o t.
& 11800
600 -f~
400
§ o 200c c
10 0
tuQO
1,400
1,200
1,000
0,800 -
0,600 -
0,400
0,200 -)-
0,000
+• v
month
o p o o o oR = ~ = = >
month
XXIV DRO Demänovská dolina 102

ANALYSIS OF THE MORTALITY DEVELOPMENTOF THE POPULATION IN THE SURROUNDINGS
OF BOHUNICE NPP USING THE FUZZY LOGIC METHODS
Mária Letkovičová, 2Beáta Stehlíková, * Martin Ďurov1 Environment,a.s., Centrum bioštatistiky a environmentalistiky, Nitra
2SPUNitra
Úvod
Sledujeme okolie Atomových elektrární Bohunice (ďalej EBO). Okolie má tvar kruhus polomerom 30km, čo predstavuje rozlohu cca 2800 km2. Tento rozmer sledovaného okolia jepredpísaný bezpečnostnou správou EBO. K predkladaným výpočtom sme použili kompletnédatabázy Registra úmrtí, Registra obcí a Vekového zloženia obyvateľstva SR v rokoch 1993 až1999, vypracované v Štatistickom úrade SR. Pracujeme s databázami, ktoré neobsahujú osobnéidentifikácie.Vývoj úmrtnosti sledujeme pomocou indikátorov úmrtnosti, vypočítaných podľa WHO.Podľa literárnych prameňov a aj podľa našich skúseností je potrebný súčet najmenej troch rokovna výpočet stabilných demografických a epidemiologických parametrov. Preto pracujememetódou krátkych časových radov. Základná pozorovaná jednotka, ktorú predstavuje jednahodnota indikátora je jedna obec. Všetky naše hodnotiace analýzy sú vypočítané z trojročnýchsúčtov všetkých ukazovateľov, čiže pracujeme s tzv. osoborokmi.Predkladaná práca je upraveným výňatkom z Komplexnej správy o stave životného prostredia azdravotnom stave obyvateľstva v okolí atómových elektrární Bohunice za rok 1999, ktorúv marci tohto roka predkladala naša spoločnosť.
Cieľ práce
• Zistiť momentálny stav úmrtnosti v sledovanej oblasti EBO• Zistiť časový vývoj úmrtnosti• Porovnať výsledky so stavom v Slovenskej republike
Dáta
Všetky indikátory sú vypočítané z presných údajov za jednotlivé obce. Trojročné súčty za každúobec sú konštruované tak, že sa navzájom čiastočne prekrývajú. Tak je možné s určitýmoneskorením, ale pomerne presne a čo najviac zbavené chýb, odhadnúť vplyv konkrétneho rokana hodnotu sledovaného indikátora, pričom sa neeliminujú extrémy.V dostatočnom počte takýchto radov dostaneme každý rok dvakrát samostatný, čím je jasnýjeho vplyv v trojici rokov.
Na podrobný rozbor pre účely tejto práce sme vybrali nasledovné zdravotné indikátory:
• Hrubá úmrtnosť• Predčasná úmrtnosť• Potenciálne roky strateného života (PYLL)• Úmrtnosť na vybrané príčiny
MetódyZákladná analytická metóda je Fuzzy zhluková analýza založená na relácii fuzzy podobnostiZhluková analýza patrí k známym a rozpracovaným mnohorozmerným štatistickým metódam.Umožňuje rozdeliť danú množinu objektov do niekoľkých podmnožin v istom zmyslepodobných objektov.
XXIV DRO Demänovská dolina 103 SK02K0192

V súčasnosti existuje takmer pre každú oblasť matematiky jeho "fuzzy analógia". Teória fuzzymnožín významne prispela aj k riešeniu úlohy zhlukovej analýzy.Nech Uje množina, L — (L, A , V, 1, 0) je zväz- Funkciu A definovaná na univerzu UA:U-+Lnazývame fuzzy množinou, presnejšie funkciou príslušnosti fuzzy množiny A. V našom prípadebude L = (0, 1).Vyjadrovanie v prirodzenom jazyku je do istej miery nepresné, neurčité, vágne. Chápanievýznamu slov je doménou človeka a teda je do istej miery subjektívne. Prirodzený jazyk je všaknositeľom informácií a preto chápanie slov musí byť viac-menej rovnaké pre všetkých ľudí.Preto je prirodzené a má zmysel vyjadriť význam modelovaného pojmu pomocou funkciepríslušnosti fuzzy množiny. Neurčitosť je v teórii fuzzy množín určitým spôsobom exaktnekvantifikovaná.Nech T je množina slov prirodzeného jazyka, význam slov budeme stotožňovať s nepresne vymedzenoutriedou prvkov univerza U. Nech AeT je slovo. Potom M(A) - význam slova A - je ŕuzzy množina A cU. Hodnotu stupňa príslušnosti Ax prvku x e U do významu M(A) = A slova A e T môžeme chápať doakej miery daný prvok x odpovedá významu slova A. Je prirodzené zvoliť e > 0 vyjadrujúcu mierutolerancie pre výber prvkov x, ktoré v obvyklom chápaní zmyslu slova patria do A.V prirodzenom jazyku sú často používané jazykové operátory, t.j. příslovky veľmi, málo,značne, skôr, viac-menej, atď .. Pri modelovaní .sémantiky prirodzeného jazyka pomocou fuzzymnožín sú jazykové operátory modelované prostredníctvom vhodných operácií nad funkciamipríslušnosti významu slov pri ktorých stoja.Nech A je slovo, ktorého význam je M(A) = A c U, m eT je jazykový operátor s asociovanoufunkciou fm : L —>L. Potom význam výrazu mA je M(mA) = fm ° A, kde ° označuje skladaniefunkcií. V našom prípade sme využili jazykový operátor "veľmi" (very) s asociovanou funkcioufv(a) - o?, operátor „približne" (more or less) ) s asociovanou funkciou fp(a) = 2a - o?a operátor „zhruba" (roughly) s asociovanou funkciou fz(a) = -a4 + 4a3- 6a2 + 4a.V ďalšom budeme modelovať pojem A = "podobná obec z hľadiska určitého indikátora".
Výsledky
Ako súčasť výsledkov ukážeme na jednom indikátoři výstup z fuzzy c analýzy.Analyzujeme indikátor HRUBÁ ÚMRTNOSŤ OBYVATEĽSTVA (počet úmrtí na 1000obyvateľov).
Výsledok je komentovaný niekoľkými spôsobmi, pričom pre existenciu interpretácie musia byťprítomné všetky jeho zložky:
a. tabuľka typických predstaviteľov jednotlivých zhlukovb. mapa zhlukovc. graf priebehu zhlukovd. tabuľka hodnôt funkcie príslušnosti k jednotlivým zhlukom pre jednotlivé obce
a znaky
XXIV DRO Demänovská dolina 104

Fuzzy C zhluková analýzy časových radov demograficko zdravotnických indikátorov
Počet úmrtí na 1000 obyvateľov
Ca
12345
5ový rad
1993-1994-1995-1996-1997-
19951996199719981899
Hodnota funkcie pri slušnosti{* , j 0-0.2| 0.2001 -0.4999f ^ * 0.5-0.7999f " " 0.8-0.9999
HUS
-1.zhluk
-2.zhluk
os x označuje poradové číslo časového raduos y označuje počet úmrtí na 1.000 obyvateľov (hrubá úmrtnosť obyvateľstva)1.zhluk: vyhranené (tmavomodré) obce, nevyhranené (bledomodré) obce, modrá čiara na grafe2.zhluk: vyhranené (tmavozelené) obce, nevyhranené (bledozelené) obce, červená čiarana grafe
Komentár:
Obce v rôznych zhlukoch majú rôznu počiatočnú výšku ale rovnakú dynamiku vývojaindikátora.Existujú stabilné lokality s trvalým vysokým výskytom úmrtí (1.zhluk). Druhý zhluk má asi o30% priaznivejšie hodnoty. Indikátor vykazuje miernu zbližovaciu dynamiku a naznačujepomalé vyrovnávanie oblasti.
Súhrn niektorých záverov analýz vývoja úmrtnosti z pohľadu oblasť EBO vs. Slovensko
J Hrubá úmrtnosť obyvateľstva je na stabilnej úrovni a počas rokov sa v okolí EBOv podstate nemení, zaznamenali sme nárast o dve desatiny percenta.
S V porovnaní s priemerom SR má okolie EBO sústavne o 0,4 až 0,6 promile vyššiu hrubúúmrtnosť, dynamika je rovnaká.
S Rovnaké závery platia aj pre hrubú úmrtnosť vyčíslenú podľa pohlavia.
XXIV DRO Demänovská dolina 105

S Vo všetkých prípadoch sme zaznamenali pomerne vysoký percentuálny nárast hrubejúmrtnosti v smere - severo -severo-východ od EBO, čím sa tento segment dorovnal nahodnoty ostatných.
S Počas všetkých rokov zaznamenávame najvyššiu hrubú úmrtnosť západným smerom odEBO, ktoré majú aj najvyšší počet starého obyvateľstva, čím sa toto zvýšenie bezo zvyškuvysvetľuje.
•S Percento predčasných úmrtí je v okolí EBO stabilne nižšie, ako u celej SR, čo sa týka ajprepočtu podľa pohlavia.
S Po celý čas nezaznamenávame nárast predčasných úmrtí, čo interpretujeme, že sanezhoršuje zdravotný stav
•S Podľa PYLL - počtu stratených potenciálnych rokov života môžeme vysloviť predpoklad,že plošne predčasnosť úmrtí narastá v celej SR,
S v okolí EBO narastá s vyššou dynamikou ako je slovenská, ale ani na konci sledovanéhoobdobia nedosahuje ani počiatočnú výšku S R - j e celkove nižšia
•f rovnaký záver platí o prepočítaní PYLL najedno predčasné úmrtieS Najčastejšia príčina úmrtia v SR je kardiovaskulárne ochorenie. V rámci SR
zaznamenávame v rámci sledovaného obdobia sústavný mierny relatívny nárast. Rovnakýtrend je aj v okolí EBO, aj keď celkove je po celý čas tento ukazovateľ vyšší, ako v celej SR- v okolí EBO je táto príčina častejšia
S Úmrtia na zhubné nádory narastajú počas rokov v SR aj v okolí EBO. Dynamika jerovnaká, rozdielny je stav - v okolí EBO je sústavne mierne vyšší počet.
S Počet úmrtí na zhubné nádory tráviaceho traktu mierne narastá v celoslovenskom merítku ajv okolí EBO ako celku.
S Úmrtnosť na rakovinu pľúc je takmer stabilná v rámci SR, v rámci EBO mierne narástla a jepo celý čas nad hodnotami SR.
•f Počet úmrtí na leukémie je ťažko hodnotiteľný aj tomto časovom merítku pre svoj malývýskyt. Jednotlivé prípady spôsobujú ešte stále značnú nestabilitu výpočtu. Môžemekonštatovať, že relatívne počty aj dynamika výskytu v čase sú v okolí EBO totožné ako nacelom Slovensku.
Súhrn niektorých záverov analýz vývoja úmrtnosti ibä v oblasti EBO
S Úmrtnosť na zhubné nádory sa v rámci celej oblasti vyrovnáva na hodnotu cca 300prípadov ročne na 100.000 obyvateľov
S Úmrtnosť na zhubné nádory tráviaceho traktu kopíruje vo vývoji celkovú úmrtnosť nazhubné nádory, prichádza k vyrovnávaniu oblasti na hodnotu cca 100 prípadov ročne na100.000 obyvateľov
•f Počet potenciálne stratených rokov života na 1 predčasné úmrtie celkove narastá, pričomexistujú veľmi rozdielne oblasti, ktoré si svoj rozdiel udržujú (klesá vek, pri ktoromprichádza k predčasnému úmrtiu, napr. na infarkty sa zomiera v mladšom veku)
S Počet potenciálnych rokov strateného života na 100.000 obyvateľov sa pomaly vyrovnávav oblasti, aj keď existujú veľmi rozdielne skupiny obcí. Skupiny obcí s veľkým počtompredčasných úmrtí sa trošku zlepšujú.
S Hrubá úmrtnosť obyvateľstva zostáva takmer na rovnakej úrovni, prichádza k pomalémuvyrovnávaniu oblasti
V Percento predčasných úmrtí mužov aj žien zostáva stabilné, neprichádza k vyrovnávaniu,existujú trvalé oblasti s vysokým počtom predčasných úmrtí.
S Prichádza k vyrovnávaniu celej oblasti v počtoch úmrtí na rakovinu pľúc, zjednocuje sa nahladine cca 50 prípadov ročne na 100.000 obyvateľov
S Prichádza k vyrovnávaniu oblasti v počtoch úmrtí na leukémie spôsobom, že sa celoplošneznižuje ich počet, hlboko pod slovenský priemer
S Úmrtnosť na kardiovaskulárne ochorenia je stabilná a vysoká. Existuje skupina obcís rovnakým vysokým počtom a rovnakým veľmi vysokým počtom prípadov na 100.000obyvateľov (na úrovni cca 600 a 900 prípadov ročne na 100.000 obyvateľov)
XXIV DRO Demänovská dolina 106

S Významný korelačný koeficient nachádzame iba medzi hrubou úmrtnosťou obyvateľstva aúmrtiami na kardiovaskulárne choroby, čo je interpretovateľné ako fakt, že väčšinaobyvateľstva v tejto lokalite zomiera práve na túto príčinu
Celkový záver
Prichádza k vyrovnávaniu celej oblasti EBO z pohľadu niekoľkých indikátorov:S úmrtnosti na zhubné nádory celkovej aj podľa najzastúpenejších druhovS hrubej úmrtnosti obyvateľstva spolu, ako aj mužov a žien samostatneS počte potenciálne strateného života v prepočte na 100.000 obyvateľov
Existujú stabilné indikátory, kde sú rozdielne lokality, nieje žiadna medziročná dynamika užiadnej z nich a svoj rozdiel si zachovávajú:
S úmrtnosť na kardiovaskulárne ochoreniaS percento predčasných úmrtíS percento spontánnych potratov
Existujú indikátory, kde sa zvyšuje rozdiel medzi lokalitami:S percento nedonosených detí
Vzhľadom k tomu, že vo väčšine nepriaznivých javov prichádza v dlhodobom pohľadek zjednocovaniu alebo aspoň k približovaniu hodnôt jednotlivých obcí v rámci celej oblastiEBO konštatujeme, že ani veľmi podrobným rozborom sme nezistili žiadne smerové rozdiely,čiže smerové pôsobenie prevádzky EBO na zdravotný stav obyvateľstva v jeho 30 km okolí.
XXIV DRO Demänovská dolina 107

STATISTICAL SURVEY OF THE CONSUMPTIONOF THE PRODUCTS FROM SEMINATURAL ENVIRONMENT
IN THE CZECH REPUBLIC
Irena Malátová, Josef TedStátní ústav radiační ochrany, Šrobárova 48,100 00 Praha 10
The central aspect of the work in international project SAVEC (Spatial Analysis ofVulnerable Ecosystems in Central Europe) is the identification of vulnerable areas. These areareas which, by virtue of the processes governing the transfer of radionuclides through food-chains, deliver high radionuclide fluxes to man. Identification of vulnerable areas is essential inestablishing where intervention levels are likely to be exceeded in the event of a nuclearaccident. Vulnerable areas could be identified using many criteria, a.o. high production rates ofcertain foodstuffs which substantially accumulate specific radionuclide. In addition toenvironmental factors, social factors will also contribute to vulnerability, in particular, dietarypreferences can lead to the ingestion of more contaminated foodstuffs.
Since Chernobyl accident, it is well known fact that in the Czech Republic, the mostcontaminated foodstuff is coming from seminatural ecosystem (mushroom, forest berries andgame). However, critical group as to the size and composition was not quantitatively evaluatedup to now.
Therefore, in the frame of SAVEC project, a statistical survey with the aim of findingcritical group of inhabitants in the Czech Republic was performed. The survey was performedby a specialised marketing agency AMASIA [1]. It was aimed at the consumption of productsfrom seminatural environment - mushrooms, forest berries and game. Two independent sub -surveys were performed.
The first one, aimed at randomly selected households from phone directory, had a goalto obtain 1500 interviews among the whole population. In individual regions, number ofrespondent was selected according to the number of inhabitants of the region.
The second survey was aimed at the hunters and their households. Mostly members ofthe hunting association were included into survey as there is only small number ofprofessional hunters in the Czech Republic. The criterion was chosen that the respondent has tobe hunter, gamekeeper or similar profession who consumed game at least ten times during thelast year. The aim was to obtain at least 400 interviews. This survey was performed throughinterviewers.
People were asked if they consumed game, mushroom or berries last year andafterwards, if they asked "yes", they were asked to quantify it. People were asked also someadditional questions about their age, sex, profession, education, number of household'smembers, place of residence and the size of it. These additional questions enabled to estimatehow representative from the statistical point of view the group is.
Also the size of the critical group was estimated - under the assumption that through theconsummation of game the highest intake of 137Cs could occur. During the survey of the criticalgroup (hunting association) people were asked to estimate how many of their colleagues -members of the hunting association consume more than 5 kg of game per year. Averageestimation was that 36% of colleagues consume more than 5 kg per year. There is altogether 98836 members of hunting association and 36% of it is about 35 600 people.
From the survey among households 21,6% answered that they consume game. Fromthis amount, 1,2 % answered that they consume more than 5 kg per year. It means that 0,25% ofinhabitants consume more than 5 kg of game per year. The number of the inhabitants of theCzech Republic is about 10 000 000 people, so the critical group is about 25 000 people . Thisestimate is very close to the estimate from hunting association.
SK02K0193XXIV DRO Demänovská dolina 108

As a result, we suppose that about 30 000 people in the Czech Republic consume morethan 5 kg of game per year and this group is a critical group.
Table 1 Example of quantification of product consumed by an individual and numberwhich was used in statistical evaluation
Question from interview
more than 5 kg
about 3 -ŕ 5 kg
about 2 kg
about 1 kg
less than 1 kg
less than 0.5 kg
Estimated mid-interval
for use in calculation
7
4
2
1
0.75
<0.5
Normal distribution and logarithmic normal distribution were used for the calculationof medians and geometric and arithmetic means and statistical errors. There were no very bigdifferences among the calculated averages in the most cases. The results from logarithmicnormal distribution were used as the logarithmic normal distribution probably describes thereality in the best way. Formulation of the questions in questionnaires are given in the firstcolumn of the table 1. The number substituted for the given interval is in the second column.Calculated average from the distribution was afterwards corrected for the number of positiveanswers.
When members of the assumed critical group (hunters) were asked on consumption ofgame and if they answered that they consume more than 5 kg, they were asked to quantify it. Inthis case, all these numbers were used for the logarithmic normal distribution.
Table 2 The results of two dietary surveys in the Czech Republic.
Average consumption of the products from seminatural environment by the Czechpopulation and by selected critical group
( arithmetic averages calculated from logarithmic - normal distribution)
Item
MushroomForestberriesGame
Average consumption bypopulation (kg/y)
2,4
1,5
0,28
Average consumption by criticalgroup (kg/y)
3,4
2,85
6.23 (14.7) *)
*) Calculated for selected group with consumption more than 5 kg game per year.
Surveys among assumed critical group in smaller scale were performed in Poland andHungary. In Poland 25 people were interviewed, in Hungary, altogether 79 people wereincluded into study, The settlements in which people were interviewed in Hungary are inmountains, covered by forest. The people interviewed in Hungary and Poland were hunters,forest engineers and amateur hunters.
XXIV DRO Demänovská dolina 109

Results from surveys were compared with the similar survey from EU countries.
Table 3 Comparison with other countries [2]
Austria
Belgium
+Luxembourg
Denmark
Finland
France
Germany
Greece
Ireland
Italy
Netherlands
Norway
Portugal
Spain
Sweden
UK
Czech Rep
Poland
Hungary
Estimated average consumption
(kgfw/person/year)
Game
1,0
0,02
0,7
1,9
0,5
0,5
0,11
2,6
0,4
3,5
0,1
0,28
Mushroom
0,4
1,5
0,03
0,01
0,03
0,2
0,1
0,9
2,4
Berries
0,6
8,4.
2,5
5,1
1,5
Summary of national hypothetical wild
food consumption (kgfw/person/year)
Game
15
15
15
16,6
15
20
15
15
15
15
17,8
15
15
16,7
9
6,2(14,7)
23,3
6,9
Mushroom
6
6
2
2,3
6
9,9
6
6
6
6
0,9
6
6
2,1
1,8
3,4
2,4
3,6
Berries
4
4
4
13
4
4
4
4
4
4
6,6
4
4
7
4
2,8
1,3
2,1
Consumption of game, mushrooms and forest berries by the Czech population and bycritical group resulting from statistical survey was compared with expert judgment, used by usin previous SAVEC report [3]. *•
Consumption of game is in good agreement with previous estimation for bothpopulation and critical group. Also, in comparison with other countries our results are in quitegood agreement.
Consumption of forest berries is rather high, however, again, it is in good agreementwith other countries.
Consumption of mushroom is very high for the Czech population. For the criticalgroup, it seems again to be in quite good agreement with other countries, however, for the
XXIV DRO Demänovská dolina 110

population it is the highest from all countries given in table 2, 3. It is lower than e.g.consumption of mushroom in village Veprin in Russia (Briansk Region) [4].
To estimate how realistic the conclusions of the statistical study were, ad hoc smallsurvey was performed among the employee of the NRPI in Prague and NRPI dependence inHradec Králové. Altogether 40 people answered within 4 days; surprisingly, average amount ofmushrooms consumed was even higher than the one from nation - wide survey.
Table 4 Calculated yearly intake of Cs by the Czech population and by the criticalgroup.
Mushroom
Forest
berries
Game
Sum
Factor of
losses by
culinary
preparation
0,5
0,5
0,3
Average
activity
(Bq/kg)
700
10
150
Consumption -
population
(kg/y)
2,4
1,5
0,28
Consumption -
critical group
(kg/y)
3,44
2,85
6,23
Intake of137Cs-
population
(Bq/y)
840
7,5
12,6
860
Intake of137Cs-
critical
group
(Bq/y)
1204
14.25
280
1498
Yearly intake of 137Cs, calculated from products coming from seminaturalenvironment is much higher than yearly intake calculated from yearly survey of internalcontamination through whole body counting and urine measurements. The reason ofdisagreement are further investigated - it is possible that the yearly survey do not coverrepresentative sample of inhabitants. Possible overestimation of 137Cs activity in mushroomswas, up to now excluded.
The work was performed in the frame of the EU project SAVEC - Spatial Analysis ofVulnerable Ecosystems in Central Europe (contract number: ERB IC15-CT9 8-0206).
References
[1] Consumption of game and forest berries, Amasia, March - April 2001 (in Czech)
[2] Spatial Analysis of Vulnerable Ecosystem in Europe: Spatial and dynamicprediction of radiocesium fluxes into European food (SAVE). Summary andFinal report, Contract F14PCT950015. August 1999
[3] Critical groups due to dietary habits in Poland, Hungary and the Czech Republic.Deliverable for the EU project SAVEC. November 2000
[4] Travnikova et al. Contribution of different foodstuffs to the internalexposure of rural inhabitants in Russia after the Chernobyl accident,Radiation Protection Dosimetry, Vol. 93,4, pp.331 - 339, 2001
XXIV DRO Demänovská dolina 111

ADVANCED SEPARATION TECHNIQUES IN RADIOCHEMICALANALYSIS OF ENVIRONMENTAL SAMPLES
Ľ.Mátel, P.Rajec, O.Rosskopfová,Department of Nuclear Chemistry, Comenius University, Bratislava, Slovakia
Radiological monitoring of environment enables to get a direct information on radiationdoses of individuals living there and in the case of unbalance relationship between radiationsource and local population enables to correct them. Monitoring programs for environmentenables measure and check long term changes and trends in radioactive contamination andbehaviour of radionuclides in environmental including their ecological, hydrological, geologicaland meteorological aspects of such behaviour.
A strategy of separation techniques in radiochemical analysis of environmental sampleswill be presented. A comparison of different methods of alpha radionuclides based onextraction, ion exchange and extraction chromatography techniques will be presented and someadvantages and disadvantages of methods used in our laboratory will be demonstrated.
The actual geographic distribution of the ^K, 2 3 2Th, 2 3 8U, 137Cs, 90Sr, 2 3 9 '2 4 0Pu, 24IAmwas measured in the lake sediment of North Slovakia is presented. The activity of ^Sr, 239l24i>Pu,2 4 1 Am was measured and the activity of "°K, 232Th, 2 3 8U, 137Cs was measured from 150 locationsfrom different regions of Slovakia.
The sediments were analysed using gamma spectrometry - ( HPGe detector with relativeefficiencies 28 %, Ortec). Analytical procedures involve total dissolution of the samples,followed by radiochemical separation and purification using solvent extraction ( Aliquat-336 -239>24<>Pu, TBF - 9 0 Sr), calcium oxalate precipitation and extraction chromatography an EichromTRU Resin - 2 4 t Am.
SK02K0194XXIV DRO Demänovská dolina 112

ACTUAL TRENDS IN PATIENT DOSE REDUCTIONIN RADIODIAGNOSTIC
Denisa Nikodémova,^ Igor Gomola,1} Martina Horváthova,2*Institute of Preventive and Clinical Medicine,, Bratislava
2 Faculty of Public Health and Social Care of Trnava University, Trnava
IntroductionIonizing radiation is firmly established as an essential tool for diagnosis in medicine.
Diagnostic examinations involve imaging with X-rays which constitutes over 90% of allexaminations and is the major contributor to the collective dose. Many technical advances havemade it possible to achieve considerable dose reduction.
The factors responsible for managing patient dose are:. developments in equipment and accessories,. techniques,. education and training,. dosimetry,. quality criteria and reference dose levels.The technical development responsible for the most significant contribution to patient
dose reduction has been the intensifying screen. Modern rare earth phosphors made possible adose reduction of a factor from 15-500. Appropriate filters play also a very important role incutting done the low energy X-rays. Change over from the conventional analogue technique tothe digital improves the image quality and the diagnostic accuracy through digital imageprocessing, reduces film usage and although the patient exposure by saving the exposure time.The radiological technique should be selected according to the principle of ALARA, so that bestexposure parameters are chosen (kV, mAs, FFD, etc.).
EU Directive 97/43 [1] requires from Member States to ensure that appropriate qualityassurance programmes are included together with quality control measures in the nationallegislation. On the basis of this Directive, as well as of the Basic Safety Standards [2] althoughthe New Act of Slovak National Council No.470/2000 Coll. improved the national system ofacceptability of radiological examinations by implementation of Guidance Levels, system ofeducation and necessity of introduction of Quality Assurance (QA) and Quality Control (QC)programmes in radiodiagnostic departments.
One of the primary aims of QA in diagnostic radiology is to produce diagnostic imagesof adequate quality at the lowest radiation dose to the patient. In essence this implies that thetwo key parameters to be assessed are image quality and radiation dose, so allowing to find theoptimal balance between the two. Consequently collecting information on radiation dosereceived by patients should be a vital part of any QA programme fo diagnostic radiology.Knowledge of doses under practical conditions used for variety of diagnostic examinations,serves not only for verification of compliance with recommended guidance levels but also forstimulation of the awareness of medical staff to aspects of radiation protection of the patient, i.e.of variations in doses delivered to patients due to variations in technical conditions of theequipment used and the diagnostic procedures applied. Risks to paediatric patients areacknowledged to be greater than for adults. It is therefore essential to developed appropriateradiation protection measures also in the field of paediatric patient.
In our contribution we tried to survey the entrance surface doses, as well as dose areaproduct measurements by studying 3 types of radiodiagnostic examinations (mammography,chest examination of children and fluoroscopy). The analysis of the obtained data and theircomparison with reference values of EU has demonstrated the significant role of radiationprotection dosimetry as an integral part of quality assurance strategy in radiology.
XXIV DRO Demänovská dolina 113 SK02K0195

Paediatric radiologyIn 1996 European Communities (EC) adopted Guidelines on Quality Criteria for
radiodiagnostic images in paediatric.[3] This guidelines contain reference entrance surfacedoses for various diagnostic examinations and for 5 years old children. In our survey we havecollected detailed information on radiographic examinations of children aged to 15 years. Thequestionnaire fulfilled at 9 paediatric radiodiagnostic departments in the county of Trnavaallowed us to select the chest PA projection as a most frequent radiodiagnostic examination. Toprovide information on paediatric dose levels during chest examination a combination of directmeasurements using LiF -700 Harshaw thermoluminiscent dosimeters and indirectmeasurements using dose area product meter was used.
The table 1. shows technical parameters, as well as the adequate ESD for chestexamination. Comparison of our data for 149 patients, divided in 5 age categories, withreference values published in EC document, indicate that our results of ESD were several timehigher than reference value of 0,1 mGy recommended by EC.
Tab. 1.Technical parameters and entrance surface doses for X-ray examinations of chest(children 5-9 years)
Hospital
123456789
Usedequipment
chiralux 2chiralux 2
MP 15-chiranachiralux 2chiralux 2
duroluxchiralux 2
chirodur 125 Cchiralux 2
Technical parameters FSD
kV
38-4650-5355-60
5050
71-7340-4445-4742-46
mA.s
24-4218
4-618
13-185-1224
8-1318
cm
100-150100-150
150150-200
150150-200
150150
110-150
HVL
mmAl
31,0
2,82,22,852,6Z,8Z,oZ,O
ESD
nGy586562403431443432305488326
Total filtration 3 mm A!
In the table 2. one can see the great spread of the obtained results with the conclusionthat due to "low kV technique" only 10% examinations fulfilled the EC requirements.
Tab.2 Entrance surface dose of 5-9 year old children for the chest PA/AP examination
ESD [uGy]
departments ofTrnava county
European hospitals
min
253
19
max
708
1347
median
414
67
ratio of min:max
1:3
1:71
XXIV DRO Demänovská dolina 114

MammographyMammography is a highly specialised form of radiographic imaging using low energy
X-ray from 25-28 kV. This low energy radiation is absorbed by breast tissue, resulting inrelatively high radiation doses. The average thickness of compressed breasts during themammography examinations is about 4,5 cm. According to the alarming increase of the numberof mammography examinations it is absolutely necessary to work out criteria and principles forQuality Control at mammographic workplaces in our country and make it obligatory for thestaff of all mammographic units.
At the Institute of Preventive and Clinical Medicine was established in 1991 a survey ofmean glandular doses at 15 existing mammography units in the country. In the following yearsthe claim to the modern mammographic units kept growing and in the year 1999 the totalnumber of 63 mammographic units were operating in Slovakia providing about 101 471mammographic examinations (fig.l).
120000
•S 100000ú-rax
oH
80000 f !
60000 K íI Á
40000 J/ í
20000
1999
Figure L Number of mammographic examinations at Slovak radiodiagnostic departments
With regards to mammography it has been recognised that the reduction of the mean glandulardoses is possible only when internationally recognised Quality Criteria shall be introduced.Two series of measurements of entrance surface doses and mean glandular doses were
performed at all mammographyunits in Slovak Republic. In theframework of our participation inResearch Project co-ordinated bythe IAEA it is foreseen animprovement of image quality andreduction of patient doses inmammography in a selectedsample of 3 mammographicinstallations.
It is important toremember that for mammographicmeasurements is substantial tohave a good calibration of dosemeasuring system. Overalluncertainty at the 95% confidencelevel should be less or equal to±10%. The obtained values of
Figure 2. Dosimetry intercomparison expressed as the ratio of the air calibration performed at IAEA arekerma measured by the participants to the air kerma staled by the given in the figure 2IAEA
VUr3S3Of
1.40
1.30
1.20
i i n1. (U
1.00
0.90
0.80
0.70
0.60
0.50
0.40
0.30
r
•O
f
r
SlovakRepublic
•Q • o~ B ¥"
O
M
So o
Ao
Czech Hungary Romania PolandRepublic
Spain
XXIV DRO Demänovská dolina 115

FluoroscopyAbout 14% off all radiological investigations undertaken in SR involve fluoroscopy.
Because of the exposure factors used in these examinations, particularly the screening time, theycontribute a substantial proportion of the overall population dose from medical examinations. Inour work we have compared the values of dose area product for colon investigations using 2digital and 2 analogue equipments. As it can be seen from the table 4 the mean DAP value inthe 3rd quartile for barium meal examination for digital equipment (column 1,2) is less by afactor of two comparing with the DAP value for conventional unit.
Table 4. Summary of the results for barium meal examinations
Hospital
1
2
3
4
No.ofpatients
32
29
16
38
Dose-area product (Gycm2)
min.
2.44
2.99
1.72
1.45
1stquartile
5.21
8.94
12.1
5.92
mean
9.71
13.3
39.5
10.55
median
6.71
12.16
26.26
8.61
3rdquartile
9.54
15.93
48.18
12.29
max.
39.51
26.71
154.22
46.47
ConclusionOptimisation in radiodiagnostic requires fulfilling the following criteria:• patient doses to be in accordance with accepted diagnostic practice• patient doses to be as low as reasonably practicable in order to achieve the required
diagnostic results• professionals clinically and physically directing medical exposures to be familiar
with typical doses, methods of measurements and means of dose reductionOne of the basic requirements for continuous quality improvement is the repeating cycle
of patient dose measurements for determining the level of risk associated with particularradiological examination at given radiodiagnostic department. Beside the undeniable positiveinfluence of QA procedures possible negative effects should be avoided. The danger exist thatthe development of new techniques is slowed down by standardising all procedures and wideagreement in implementing of required modifications. Reaching of a consensus of a certainprocedure became therefore a labour intensive and time-consuming process.
References
[1] European Union, Council Directive 97/43/Euratom 1997, Health Protection ofIndividuals against the Danger of Ionizing Radiation in Relation to Medical Exposure.Luxemburg 1997,
[2] Basic Safety Standards, Safety series No. 115: Guidance Levels of Dose, Dose Rate andActivity for Medical Exposure; IAEA, Vienna 1996,
[3] EUR 16261 - European guidelines on quality criteria for diagnostic radiographic imagesin paediatric; edited by M.M Kohn, B.M.Moores, K.Schneider; Luxemburg: Office forofficial communities 1996 - IX,
XXIV DRO Demänovská dolina 116

POSTAL AUDIT IN DENTAL RADIODIAGNOSTICS
Leoš Novák, Daniela KroutilíkováNational Radiation Protection Institute, Šrobárova 48,100 00 Prague 10, Czech
Republic
Introduction
According to Czech laws dental intraoral X-ray machines are classified as "simple sourcesof ionizing radiation". Consequently, their use is licensed on condition that an adequate qualityassurance program is realized. In general, the programme is based on acceptance tests, statustests and constancy tests. The particular methods are specified in the recommendation [1]published by State Office for Nuclear Safety. Both the acceptance and status tests involve in situmeasurements to control parameters of the X-ray machine and the developing process. Onlypersons who were licensed for such handling can do these measurements. The yearly status testsare very detailed and several years' experience showed it might be advantageous to have asimpler method additionally available for purposes of the state supervision. Such a method issupposed as a postal audit. It should be simple enough to make the operation of the statesupervision more effective but it also should provide sufficient information on radiationprotection of the patients. Besides it should enable to prolong the period for the status testsultimately. As for the postal audit, a small package containing a proper dosimetric set would besent directly to the dentist who would treat it according to instructions. This paper describessuch method that was developed in the National Radiation Protection Institute (NRPI) andresults of pilot study that was carried out to test the method.
Material and methods
The method is supposed to control a few important parameters of the X-ray unit that aresignificant as concerns the radiation safety of the patient. It involves control of both dosimetricand sensitometric parameters. The dosimetric part covers measurements of air kerma Ka at thetop of the X-ray tube, radiation area diameter and exposure reproducibility. As for thesensitometric part, basic fog, sensitivity index and contrast index are measured.
Fig. 1: The irradiation geometry
For this purpose the dentist receives a small package with the dosimetric set andinstructions. The set is formed by radiographic film FOMA MEDIX 90 NEW (format18x24 cm) inserted in a plastic opaque cassette. On the cassette two areas to be irradiated are
XXIV DRO Demänovská dolina 117SK02K0196

marked. TL - dosemeter is attached to the plastic cassette just within one of the areas to beirradiated. Another particular part of the set is one preexposed intraoral filmAGFA DENTUS M2. The dentist is asked to irradiate the two marked areas on the cassetteusing the usual upper molar exposure (see Fig. 1). His next task is to develop the preexposedintraoral film using a usual way. Finally he is asked to provide own dental film and to irradiateit through a special phantom using the usual upper molar exposure. This film is supposed to beprocessed later in NRPI where it is measured and evaluated.
TL measurement
The TL measurement provides the value of the applied Ka. Since the TL pellets ofLiF:Mg,Ti are covered with the plastic layer forming a standard badge, the dosemeter shows flatenergy response in the region of interest corresponding to 50-70 kV. The TL dosemeters areread by Dosacus - Rados reader. The TLD system is calibrated by means of a reference X-rayunit (Prostyle Intra). The air kerma, Ka, is calculated from the TL reading, R, using thefollowing equation
Ka = R fcaľ ffad
where:- fcai ... calibration factor determined from measurement of calibration TL
dosemeters- ffad... fading correction factor
There usually is no need to correct the fading because the dentist is asked to irradiate thedosimetric set during a given time period when the calibration dosemeters are irradiated in theNRPI laboratory. The measured value of Ka should not exceed the guidance level that is 5 mGy.
Radiographic film measurement
The developed radiographic film enables to verify the dimension of the radiation area. Itsdiameter should be in range from 5.4 to 6 cm. The comparison of densities measured within thetwo irradiated areas makes possible to evaluate the irradiation reproducibility. The differencebetween the optical densities should not exceed 6% since it would entail the difference about10% in terms of Ka. The value of 6% is proximate and depends on a current calibration.Homogeneity of the radiation areas can be easily evaluated visually because the densitiesusually range from 0.8 to 1.8.
Dental films evaluation
The developing process quality is verified by means of the couple of the dental intraoralfilms. The film forwarded with the whole set to the dentist is preexposed in NRPI lab. The filmirradiation is made with the reference Prostyle Intra X-ray machine. The distance from the X-ray tube bottom to the film is set to be 2 cm. Applied exposure parameters correspond to theoptimal upper molar exposure, which gives kerma value about 250 u.Gy under 6 mm thick layerof aluminium. These exposure parameters ensure the maximal quality of the X-ray imageprovided that the correct developing conditions are observed. The film is covered by a specialdental phantom during the irradiation. The phantom is formed as a wedge step from aluminium(declared purity 99.5%) and involves a few ancillary spots (a blank field, a small lead seal toassess the basic fog and a fine grid to assess the resolution). The thicknesses of the steps arechosen to cover the whole spectrum of contrasts in the dental radiography. There are two typesof the phantom used in the Czech Republic (VMK and Radex) that partly differ in the stepthicknesses, the VMK phantom contains also a significant admixture of copper (the declaredpurity is not observed though). The preexposed film is to be developed by the dentist who
XXIV DRO Demänovská dolina 118

should apply the usual developing procedure. Vice versa the second dental film is appointed tobe exposed by the dentist using his/her own setting of the X-ray machine corresponding theupper molar exposure for an adult. The film is also covered by the phantom with the setting ofthe distance of 2 cm between the top of the X-ray tube and the film. This film is to be developedby NRPI, not by the dentist. The processed films are inspected visually first. Each step must bedistinguishable from the adjacent one and the thinnest step must be visible compared with theblank field. After this visual control the films are compared with reference films correctlyexposed and processed. Both the audit films should look like these reference films.
The next step of the dental films evaluation is the measurement of the sensitometricparameters, specifically basic fog (BF), sensitivity index (SI) and contrast index (CI). The basicfog corresponds to the optical density measured under the lead seal. The sensitivity index isdefined as the density measured under one given step of the wedge (for the VMK phantom it isthe 8.3 mm step, for the Radex phantom it is the 7.4 mm step). The contrast index is thedifference between densities under two given steps (for VMK phantom it means steps of 4.26and 12.3 mm, for the Radex phantom 3.5 and 11 mm).
The acceptable values of the measured BF, SI and CI values that ensure a high qualityradiograph were derived from reference measurements and experiences from the everydaydentist practice (Tab.l).
VMKRADEX
BF
<0.35<0.33
Tab. 1. The acceptance intervals for BF,SI
Rec. Accept.0.8-1 0.7-1.31.1-1.3 1.1-1.6
50 kV^ 1
>0.9
SI and CI
60 kV
IV
IVp
o
bo
\o
CI70 kV>0.8>0.75
80 kV>0.75>0.7
Results and Discussion
After the method had been developed, 49 dosimetric sets were sent to the dentists forpurposes of the pilot study. Unfortunately 5 of these sets were not returned to the NRPIthereafter. Besides there were a few cases when some of the tests were not performed properlybecause the dentists did not fully observed the instruction sheet. The TLDs were not exposed in2 cases, the plastic cassette with the large film was open in 9 cases, some problems with thedental films occurred in 10 cases. To avoid such mistakes in future, the instructions will bewritten at each part of the set additionally, not only in the instruction sheet.
As regards the dosimetric matter, the method seems to be suitable for the purpose thatwas intended. It is able to provide the required information on the standard of radiationprotection in the dental surgery. The obtained results confirmed the expected fact that the mainproblem in the dental radiodiagnostics is just the way of the film processing. Besides, manyoutdated X-ray machines are in operation that makes the situation even worse.
Results of the pilot study show the following facts. Ka values lower than -3.5 mGy (thatis the maximal value of Ka that still gives good quality of the image for the speed of the usedAGFA DENTUS M2 films provided that its processing is performed correctly) was achieved in25 cases (60%), Ka exceeding 5 mGy (guidance level) was found in 6 cases (14%). In 6 casesthe radiation area diameter exceeded the upper limit of 6 cm. Some of the fields also showedfuzzy shapes and so they were not demarcated properly. These problems occurred mainly forthe outdated X-ray units. In 10 cases the limit of 6% for the difference between the densities ofthe couple of the fields was exceeded. Obviously the lower density always occurred for the fieldwith the TLD and not for the field without TLD. In this way, there were found 3 cases when thedifference even was more than 30% that indicates a possible attempt to affect the Ka valuepurposely. As for the dental films evaluation, there can be seen obvious differences in values ofthe sensitometric parameters for referentially exposed films processed by the dentists (RE films)and referentially processed films exposed by the dentists (RP films). The higher basic fog valuesof RP films indicate wrong storage of the films at the place. The sensitivity index of RP films is
XXIV DRO Demänovská dolina 119

greater owing to unnecessarily high exposures that were applied by dentists. Conversely, the.lower values of sensitivity index of the RE films are connected with the too short developingprocess at the dentists. The same conclusion counts for the contrast index as well. Some of theRP films were exposed so much by dentists that it was impossible to assess the SI and CI due tothe density that was beyond the usable range.
Conclusions
The described method will be a helpful tool for the operation of the state supervision inthe dental radiodiagnostics. The method will be implemented into the existing system ofcontrols from 2002. Due to its simplicity and a quite rich content of information allows to checka big amount of the dental workplaces at once. It is supposed that one half of all Czech X-rayunits will be checked in this way every year performed on state costs. It means 175 audits permonth approximately. In this way, the operation of the quality assurance programme will besimplified due to the partial substitution the postal audits for the in situ measurements as well.The medical workplaces with good results of the audit will not be required to undergo statustests for a period of one year then. The status tests will be less frequent then. Moreover, theresults of the postal audit can be compared with the in situ control results. This indicates anotherpossible application of the method, namely independent inspection of the private companies thatperform the acceptance test and status tests.
References1. State office for Nuclear Safety. Recommendation ~ Quality control for X-ray exams in
dental surgery. Radiation Protection (1998)2. Regulation No. 184/1997 Coll. Of the State Office for Nuclear Safety on Radiation
Protection Requirements
XXIV DRO Demänovská dolina 120

DETERMINATION OF ABSORBED DOSEIN THE EXPERIMENTAL ANIMAL IRRADIATED
ON THE LEKSELL GAMMA KNIFE
1 Josef Novotný Jr., * Josef Novotný, 2 Václav Spěváček, 2Pavel Dvořák,2 Tomáš Čechák, * Roman Liščák,3 Gustav Brožek, Jaroslav Tintěra, * Josef Vymazal
Hospital Na Homolce, Department of Stereotactic and Radiation Neurosurgery,Roentgenova 2, Prague 5 151 30, Czech Republic
CTU Faculty of Nuclear Science and Physical Engineering, Department of Dosimetryand Application of Ionizing Radiation, Břehová 7, Prague 1 110 00, Czech Republic
Charles University Faculty of Medicine, Department of physiology,V Úvalu 84, Prague 5 150 06, Czech Republic
IntroductionStereotactic irradiation with the Leksell gamma knife (ELEKTA Instrument AB,
Stockholm Sweden) is one of the primary methods used for the stereotactic radiosurgerytreatment of intracranial lesions [1]. This technique is the well established alternative forsurgical treatment of arteriovenous malformations, benign tumors, malignant tumors andfunctional disorders [1], However, clinical observations and experimental data suggest that thescope of the Leksell gamma knife radiosurgery may ultimately be far broader [2].
A potential role of radiosurgery for the treatment of epilepsy has been evaluated insmall clinical series of patients suffering from this disease [3, 4]. However, several major issuesregarding the implementation and potential value of radiosurgery in the treatment of epilepsyhave not been yet addressed. Therefore it remains important to conduct experimental studies toevaluate the anticonvulsant action of radiosurgery and to identify key parametric features thataffect the efficiency of this therapy. Among the important questions that need to be addressedare these: 1) what is the most effective absorbed dose for seizure suppression with acceptedcomplication rate, 2) what is the effective target site, and 3) what is the time course ofbehavioral changes that occur in response to the therapeutic irradiation? One of the importantway for such a research is utilization of experimental animals.
The project focused on the evaluation of the changes after radiosurgery inducedhypocampal lesion in rat brain is being solved in Na Homolce Hospital since 1999. The changesafter irradiation are evaluated as a function of applied dose by following methods: 1) testing ofrat memory deficit in a water labyrinth, 2) evaluation of changes in a rat brain by magneticresonance spectroscopy, and 3) evaluation of histopathological changes in a rat brain. This studyshould provide basic experimental data for the treatment of temporal epilepsy by radiosurgerywith the Leksell gamma knife. Results of this study will be published elsewhere.
Irradiation of experimental animals on the Leksell gamma knife for research purposes isconnected in principal with two major problems: 1) suitable stereotactic fixation that allows toperform necessary stereotactic investigation and subsequent irradiation is needed, and 2)treatment planning and determination of absorbed dose in the experimental animal must beperformed.
Stereotactic fixation device that can be used for stereotactic magnetic resonanceimaging (MRI) or computed tomography (CT) and irradiation of experimental animals has beendescribed elsewhere [5]. Similar device has been designed and constructed also in ourdepartment and used for fixation of rats during MRI and subsequent irradiation on the Leksellgamma knife. Detailed description of this device will be published elsewhere.
Treatment planning and dosimetry for experimental animals irradiated on the Leksellgamma knife is rather complicated task [6, 7]. As a first approach for the determination of thedose that should be delivered to an experimental animal Leksell GammaPlan (ELEKTA
XXIV DRO Demänovská dolina 121 QKDPkTíi Q7

Instrument AB, Stockholm Sweden) treatment planning system can be used. This system isdesigned for precise [8] calculations of the treatment plans for patients treated on the Leksellgamma knife. In the case of experimental animals these calculations are associated with somelimitations which must be taken into account: 1) definition of the experimental animal outerbody contours is not accurate, 2) calculating algorithms in the treatment planning system forsuch an irradiation geometry are not accurate, 3) absorption in a special fixation device (wherethe experimental animal is fixed during irradiation) is not included into these calculations.
The purpose of this study was to evaluate and quantify inaccuracy of LeksellGammaPlan relative and absolute dose calculations for the experimental animal and todetermine necessary corrections that must be applied.
Methods and MaterialsDetermination of absolute dose
Altogether three different types of dosimeters were used for evaluation of absolute dosedelivered in the rat brain: ion chamber, thermoluminescent dosimeter (TLD) and semiconductordetector.
A spherical plastic phantom (160 mm in diameter, produced by ELEKTA InstrumentAB, Stockholm) and 18 mm collimator helmet were used for the calibration. The phantomconsists of two hemispheres and a special insert plate that allows fixing different detectorsexactly into the center of the spherical phantom. Three different insert plates were made. Thefirst one contains axial hole for the ion chamber, the second one small groove forthermoluminescent dosimeter and the third one slot for semiconductor detector. The correctposition of all three detectors in the center of the spherical phantom was subsequently checkedby X-ray examination. This phantom can be fixed in the Leksell gamma knife collimator helmetwith detector positioned exactly in the izocenter of the helmet.
Ion chamber PTW M 233 331 connected to PTW UNIDOS electrometer (PTW,Freiburg Germany) was used as a primary reference detector for Leksell gamma knifecalibration.
Thermoluminescent dosimeters (LiF chips, 3 mm x 3 mm x 1 mm) (Harshaw Bicron,Solon USA) were used. Large number of TLD chips was carefully sorted to have maximalresponse deviation ± 1.5 %. The Harshaw 3500 TLD reader was used for the evaluation ofdosimeters. The TLDs were calibrated in the spherical plastic phantom with the insert platedescribed above and 18 mm collimator helmet on the Leksell gamma knife by doses in therange of 2-6 Gy. The TLD was fixed in the spherical phantom and then moved into thetreatment position and after irradiation moved out of the treatment position. Consequently thecalibration includes also small dose that is delivered to TLD during the phantom transportationin and out of the treatment position (so called transportation dose). Annealing of the TLD chipswas carried out in Harshaw annealing computer controlled oven.
Semiconductor detector type Scanditronix EDD-2 (0.5 mm thickness, 1.5 mm diameter)(Scanditronix Medical AB, Uppsala Sweden) connected to PTW Freiburg UNIDOSelectrometer was used. The semiconductor detector was calibrated in the spherical plasticphantom with the insert plate described above and 18 mm collimator helmet on the Leksellgamma knife by doses in the range of 2-6 Gy. The electrometer timer was used for measurementof time during the calibration procedure. Dose that is obtained during the transportation into andout of the treatment position was studied as well and correction coefficient evaluated.
A cadaver of male rat (about 300 grams) was used for the simulation of real irradiationconditions during in vivo dosimetry. The rat cadaver was fixed in the special fixation devicedeveloped in our department (Fig.lA). Semiconductor detector or TLD chip covered in a plasticcoat was implanted into the rat brain in the region of planned radiation intervention. To localizeexactly the position of dosimeter stereotactic MRI (SIEMENS IT EXPERT, ErlangenGermany) in the case of TLD and stereotactic CT (SIEMENS SOMATOM PLUS 4, ErlangenGermany) in the case of semiconductor detector were performed. Treatment planning and theirradiation was carried out exactly in the same geometry as normally for live rat.
XXIV DRO Demänovská dolina i 22

Determination of relative dose distributionTo evaluate relative dose distribution delivered into the rat brain the polymer gel
dosimeter was used [8]. Composition and the process of polymer gel dosimeter preparation havebeen described elsewhere [8]. Calibration of the polymer gel dosimeter was done on the Leksellgamma knife with the use of a special head phantom. Altogether six dosimeter samples fixed inthe head phantom were subsequently irradiated by the doses in the range of 1-9 Gy. Twononirradiated dosimeters were used for background reading. Detailed description of thecalibration procedure has been described elsewhere [8]. To evaluate dose distribution in the ratbrain a special glass phantom was made. This phantom mimicked exactly the shape of the ratbody and could be filled by the gel dosimeter. Filled phantom was fixed into the special fixationdevice and then underwent stereotactic MRI, treatment planning and irradiation exactly thesame way as during the experiment with living animal (Fig. IB). Irradiated polymer gel phantomwas then evaluated on MRI by the procedure described elsewhere [8].
Fig.l Experimental arrangements for measurement of absorbed dose in the rat. A) In vivomeasurement with the implanted semiconductor detector in the rat brain. B) Measurement withthe special glass phantom of the rat body filled by polymer gel dosimeter.
Irradiation of the rat cadaver and polymer gel phantomA typical irradiation of the rat brain consisted of four 4 mm collimator isocenters
arranged to create horse shoe shape dose distribution covering hypocampus of the rat brain by70 % isodose. Knowledge of mean dose to the volume defined by 70 % isodose curve wasrequested, since this dose was used as a reference dose for reporting effects after rat irradiation.The TLD chips were always inside the volume of 70 % isodose, but semiconductor detector wasdue to very small dimensions situated inside 90 % isodose.
The irradiation geometry of both detectors exactly simulated real irradiation of livingexperimental animal. For TLD and semiconductor detector doses of 5.5 Gy to the maximumwere applied. Altogether twenty subsequent measurements were carried out with TLDs and tenmeasurements with semiconductor detector. The signal from both detectors represents meandose. The measured mean dose and calculated one by the Leksell GammaPlan treatmentplanning system were finally compared.
Glass rat phantom filled by polymer gel dosimeter was irradiated by maxima! dose 8Gy. Irradiation was performed in the same geometry as described above. To compare relativedose distribution calculated by the treatment planning system and real measured one in the glassrat phantom profiles in three axis were evaluated and compared.
XXIV DRO Demänovská dolina 123

ResultsMeasurements with TLDs and semiconductor detector evaluated mean dose delivered to
these detectors. This average dose was compared with calculations. Results are presented inTab.l.
Detector
TLDSemiconductor
Mean dosecalculated bythe TPS [Gy]
4.85.1
Mean dosemeasured[Gy]
5.185.49
STD [%]
5.410.95
Deviation
7.927.65
Tab.l Results of in vivo measurements with TLD and semiconductor detector in the rat brain.Average observed deviation between the mean" dose calculated by the Leksell GammaPlantreatment planning system (TPS) and measured one is 7.79 %.
Profiles calculated in X, Y and Z axis by the treatment planning system showedacceptable agreement with measured ones by polymer gel dosimeter.Conclusions
Both TLD and semiconductor detectors appeared to be suitable for measurement ofabsorbed dose in the rat brain irradiated on the Leksell gamma knife. Both detectors, due to theirsize, measured mean doses, nay doses to maximum. The Leksell GammaPlan treatmentplanning system can be employed for the calculation of absorbed doses even in such an extremecondition like irradiation of experimental animals. However, in our concrete case, it wasnecessary to apply correction factor of 1.0779 for the absolute absorbed dose to obtain reliableresults. Comparison of dose profiles in all three axis calculated by the treatment planning.system and measured ones by polymer gel dosimeter showed acceptable agreement. Resultspresented in this study are strictly related to the Leksell GammaPlan treatment planning systemand the special fixation device developed in Na Homolce Hospital.References
1. Lunsford L.D., Kondziolka D., Flickinger J. Progress in Neurological Surgery. GammaKnife Brain Surgery. Karger, 1998
2. Lindquist C , Kihlstrom L., Hellstrand E.. Functional neurosurgery- a future for the gammaknife? Stereotact. Funct.Neurosurg. 57, 72, 1991
3. Barcia S.J.L., Roldam P., Hernander G., Lopez-Gomez L. Radiosurgical treatment ofepilepsy. Appl. Neurophysiol. 48, 400, 1985
4. Barcia S.J.L., Roldam P., Hernander G., Lopez-Gomey L. Radiosurgery of Epilepsy. Long-term results. Acta Neurochir.fSuppI.] 62, 111, 1994
5. Kamiryo T., Berr S.S., Berk H.W., Lee K.S., Kassell N.F., Steiner L. Accuracy of anexperimental stereotactic system for MRI/based Gamma Knife irradiation in the rat. Actaneurochir. 13 8,1103,1996
6. Duftschmid K.E., Kindl P., Obenaus B., Strachotinsky Ch., Winker N. Precision dosimetryin narrow collimated radiation beams of the Leksell Gamma Knife. Rad. Prot. Dostm. 66,295, 1996
7. Niyin P.S. An absorbed dose in narrow Co-60 gamma-ray beams and dosimetry of theGamma Knife. Med. Phys. 25, 2347, 1998
8. Novotný Jr. J, Dvořák P., Spěváček V., Tintěra J., Novotný J., Čechák T., Liščák R. Qualitycontrol of the stereotactic radiosurgery procedure with the polymer-gel. Sent for publicationin Radiotherapy and Oncology
XXIV DRO Demänovská dolina 124

DETERMINATION OF ALPHA RADIONUCLIDES IN FISH
Pernická L., Mátel R, Rosskopfová O.Department of Nuclear Chemistry, Faculty of Science, Comenius University
Mlynská dolina CH-1, 842 15 Bratislava, Slovakia
Abstract:In atmospheric water, external water and undercurrent the occurrence of radionuclides is
usual. It is an important factor of quality of the environment. Plants ingest radionuclides fromwater and with they everyone. And it arises radioactivity infest food - chain.
Radiotocity of this radionuclides is very deer sometimes. The sensitive radiochemicalprocedures for their determination are necessarily important.
The poster presents the combined procedure used at our laboratory for determination ofalpha radionuclides in biological samples.
The specific activity of alpha radionuclides was determined in biological samples.The biological samples were chosen kinds offish, concretely macrels, herrings and haddocks.
Analytical procedures were involved total dissolution of the samples, then wasfollowed extraction of uranium and thorium with Aliquat - 336 from aqueous (HNO3 or HC1)media and they were separated from Pu, Am and Sr. Final purification of the dissolved samplesemployed an extraction chromatographic column. The column was packed with achromatographic resin U/TEVA Spec. . (The organic extractant is diamyl amyl phosphineoxide, which is coated onto the surface of an inert polymeric support - Amberline XAD-7).Uranium and thorium were separated by Eichrom U/TEVA resin prior to measurement. Thinsources for uranium and thorium determination were prepared by micro-co—precipitation withNdF3 and their activities were determined by alpha spectrometry, using low - backgroundcounter ORTEC (600-mm2 silicon-surface barrier detector). The alpha spectrums of uraniumand thorium fractions in the observed kinds of fish were showed dee* radionuclide purity.
ia
SK02K0198XXIV DRO Demänovská dolina 125

THE SYSTEM OF REGISTRATION AND EVALUATIONOF HIGHER OCCUPATIONAL DOSES IN THE CZECH
REPUBLICTHE ANALYSIS AND RESULTS
Ing.Karla PetrováStátní úřad pro jadernou bezpečnost, Senovážné nám. 9, Praha
The evaluation and registration of occupational exposure is, in accordance with recentCzech legislation, issued by State Office for Nuclear Safety (SONS). The purpose of this centralevidence is not only to create and evaluate the statistics and time trends (see poster Petrová), butalso the monitoring and control of individual exposure of workers in relation to establishedbasic limits for occupational exposure. In accordance with legislation, the licensee is obliged toreport SONS immediately each personal dose exceeding 20 mSv in given monitoring period orafter the evaluation of annual dose. The same duty is also on the side of personal dosimetricservice. Licensee is obliged to report also the results of investigation of such event and themeasures accepted.
As the first result of investigation we can see the determination if evaluated dose is reallypersonal. The conclusion of investigation has to be confirmed by the radiation protection officerand by the radiation worker concerned.
In case, that measured dose was evaluated as non-personal, the value is not included inoccupational exposure of worker. However frequently repeated cases, when only dosemeter isirradiated from the reason of its irregular use, could be an initiation for the control from the sideof SONS. Namely if these cases are repeated for one worker, for one workplace or for moreworkers on one workplace. Each such situation can indicate the break or systematic break ofradiation protection principles on the workplace or during certain practice.
In case, that dose is evaluated as personal, it is necessary, first of all, to ensure that thecorrection for the attenuation effect of shielding apron was done, where is appropriate. Thepersonal dosemeter is wears in accordance with Czech legislation over the shielding apron. Therecalculation is not execute automatically for all values measured. The proposal of new Decreefor radiation protection established, that the correction is carried out in accordance with theapproved monitoring program in relation with equivalent of Pb of apron used and energy ofradiation. SONS initiated the elaboration of the procedure for recalculation for current usedshielding apron in our country (Trousil, kol.). As the reasonable value, from which thecorrection is carried out, seems to be the value of 10 mSv, which after correction (0.5 mmPb,60-80 keV) corresponds to 1 mSv of effective dose approximately. In the frame of theevaluation of annual doses, the licensee should to correct all values exceed the defined referencelevel and corrected values report to SONS. Based on this report the value is corrected also in theCentral Register of Occupational Exposure (CROE). It is necessary to secure that correction isnot doubled for one value. It could sometimes happen that during the year one measured valueexceed 20 mSv and it is corrected, after the evaluation of annual dose is the value again higherthan 20 mSv. Than it is necessary to correct only this part of the value which was still notcorrected.
The dose evaluated as personal and which occurred as the consequence of the exceptionalevent is registered separately and it is not included in the occupational exposure of worker.
Principally said, all doses exceeding the basic limits established for occupationaiexposure should be a consequence of exceptional events. In case, that the overexposure occurs
XXIV DRO Demänovská dolina 126SK02K0199

in course of approved practice and worker follows all determined radiation protection rules, thanthe question of justification and optimisation arises. This problem is recently very actualconcerning two professions - intervention radiology and industrial radiography. There we canfind certain group of workers with evaluated doses approaching often the limit valid till the endof year 2000 - 50mSv. There could be a problem for some of these workers to keep the newlimit 100mSv/5years. Within the framework of investigation of all these cases exceeding theestablished value 20mSv, the measures preventing or decreasing the probability of repetition ofsuch exposure should be set up. If there is not, from the side of relevant licensee, the answer tothe reported higher dose, the regional centre of SONS is pointed out and they should decide thenext steps. In case that for one licensee there are often repeated events connected with higherexposure, it is appropriate to manage investigation directly on the place, organising inspectionif necessary.In case that evaluated dose exceeds significantly the basic limit, the circumstances areimmediately investigated and after discussion with physicians, the measures are adopted whenthe non-personal dose is not confirmed unambiguously. These cases happen once or two timesper year.
Based on the data registered in the Central Register on Occupational Exposure there hasbeen investigated 13 values exceeding 20 mSv during the year 2000. 8 cases have beenconcluded as non-personal after evaluation, 3 cases corrected for shielding apron, 2 confirmedas personal doses. In addition to these cases, the licensee have announced directly to dosimetricservice that the values evaluated on dosemeters are not personal, but the dosemeters wereirradiated from the reason of the irregular handling.
The evaluation of annual doses shows 79 cases in year 2000, when the personal dosesexceeded 20 mSv. 43 cases from this amount have been the doses of uranium miners. Thecontrol and regulation of their doses is ensured during the year and these doses are not of courseinvestigated again. 26 cases have fell into the health care branch - 24 cases of them have beencorrected for the shielding apron and 2 cases have been investigated additionally as non-personal. 10 cases of all arise in industrial radiography. 1 value has been evaluated as non-personal caused by systematic irregular deposition of film dosemeters close to the source. Restof 9 values are confirmed as personal doses due to the regular activity of workers and they aremostly exceeding 40 mSv. The exceptional dose of one worker around 250 mSv has beenconcluded by inspection of SONS as personal without clarification of circumstances of thisevent. The worker's activity has been temporary changed to the work without source ofionizing radiation.The industrial radiography is generally the profession with higher exposure of workers. Theiraverage dose is relatively high around 2 mSv per year, but using the technical equipmentavailable and optimisation process, there is necessary to ensure that the personal doses of theseworkers will not be permanently on the level of basic limits for occupational exposure.During the year 2000 there have been found also 413 cases (without uranium miners) ofpersonal dose exceeding the investigation level for annual dose 6 mSv. These cases haveconcerned to 102 licensee - 48 health care organisations (mostly large hospitals), 24 industrialradiography companies, 30 research, service or inspection organisations and nuclear powerplants.
Finally we can conclude, based on the analysis of results of higher doses investigation,that critical profession groups are as usual the physicians practise the interventional radiologicalprocedures and industrial radiographers. There is not observed the increase of investigated casesduring last years. As the negative phenomenon we can observe increased number of irregularhandling with personal dosemeters - insecure deposition, irregular deposition on exposedplaces, wrong position on the body, intentional exposure, etc. Also the cases appears when thereason of higher exposure is difficult or impossible to find and due to the conservative approachthe dose is registered as personal. However, treatment of these cases as the consequences ofexceptional events could be very speculative and debatable.
XXIV DRO Demänovská dolina 127

The dose distribution of occupational exposure during the years1997 - 2000 in the Czech Republic
(uranium miners excluded)
100000
mSv
XXrV DRO Demänovská dolina 128

THE USE OF GEL DOSIMETER OF FRICKE TYPEIN THREE-DIMENSIONAL DOSIMETRY
Spěváček V. a, Dvořák P. a'b, Novotný J. h ml,Čechák T. a,MarekM.c
a Faculty of Nuclear Sciences and Physical Engineering, CTU in PragueBrehová 7,1 J 5 19 Praha 1
Department of Stereotactic and Neurosurgery, Hospital Na HomolceRoentgenova 2, 150 30 Praha 5
c Nuclear Research Institute, 250 68 Řež u Prahy
Introduction
Several recently developed techniques in radiotherapy, including 3-dimensional dosecalculation algorithms, inverse therapy planning, multileaf collimators, stereotactic radiotherapyand radiosurgery are applications which demand certain special properties of radiationdosimeters. While the modern techniques of conformal radiotherapy can create rathercomplicated 3-dimensional dose distributions there are no available dosimeters which cancontinuously measure 3-dimensional absorbed dose distributions in phantoms of arbitrarygeometry which are also capable of integrating the dose.
The gel dosimeter is a new and promising tool which attempts to satisfy the requirementsof the ideal dosimetry system. Unlike every other dosimetry method, gel dosimetry is totallynon-invasive. There is no need to introduce a probe into the phantom, nor is it necessary toremove part of the irradiated material for testing because the phantom itself forms the detector.The atomic composition and electron density of the gel are almost water equivalent. The site ofmeasurement is determined entirely by the measuring system, which can be programmed toscan the complete 3-dimensional dose distribution.
Gel dosimeters, in accord with the composition of the gel, were originally divided intotwo groups: Fricke-infused gel dosimeters [ 1 ] (formed by Fricke solution which is fixed in agel) and polymer-gel dosimeters [ 2-4 ] (formed by acrylic monomers which are uniformlydispersed in a gel). While the Fricke-infused gel dosimeter is based on radiation-inducedoxidation of ferrous ions which modifies NMR relaxation rates or reacts whith metal indicatorday, the polymer-gel dosimeter is based on radiation-induced polymerization and cross-linkingof acrylic monomers. The formation of cross-linked polymers in the irradiated regions of the gelincreases the NMR relaxation rates of neighbouring water protons.
The use of both types dosimeters has been associated with certain problems. In theFricke-infused gel the main problem is ferric ion diffusion which leads to significant blurring ofthe images of radiation fields within short time after irradiation. In the polymer-gel dosimeterthe most important is an inhibition of polymerization by oxygen. Radiation-inducedpolymerization is ineffective in those parts of the dosimeter contaminated by air. This effect canprobably be explained by the inhibiting effects that oxygen has on the free-radicalpolymerization. To avoid this effect the containing vessel should be made from material whichis not permeable to atmospheric oxygen (e.g. glass) and the container should be bubbled byultra-high-purity nitrogen gas before the dosimeter is filled into it.
Futher disavantage of the polymer-gel dosimeters is the evaluation of the response by theway of imaging NMR (measurement of the transversal relaxation time T2), which price is about1,5 millions US$ (cca 60 millions Kč) and therefore its use is very expensive.
The response of the Fricke-gel dosimeters was in the past evaluated also by the NMR [1](measurement of the longitudial relaxation time TO, but in the begining of the 90' of the XX.century, Appleby and Lenghrouz [6] and Bero and others [7] have used a modified system
XXIV DRO Demänovská dolina 129 Qi<n?Kn?nn

published by Gupta and Narayan [5]. They added xylenol orange (XO) into the dosimeter. XOforms a violet complex with Fe3+ ions which has the maximum of absorbance (A) at 585 nm.Because the Fe3+ ions are formed by the radiation oxidation of the Fe2+ ions of the dosimeter, itis possible to evaluate the dose by the absorbänce measurement at 585 nm which corresponds tothe concentration of Fe3+ ions. Therefore it is possible to evaluate the 3-D dose distribution bythe way of optic tomography, i.e. by the device of about 3 orders cheaper than NMR scanners.
Experimental
The composition of the gel-dosimeter used in our work is shown in the table 1
Table 1
CompoundGelatine
Xylenol orangeFe(NH4)2(SO4)2.6H2O
H2SO4(93%)
mol.w.402.47760.58392.4798.07
mM/1 j124.38
0.10.525
£/l50
0.07610.1962.64
a) the dose dependence of the gamma radiationThe basic characteristic of the dosimeter is the dependence of its response on the dose.
With an increasing dose the absorbance at 585 nm increases (formation "of the complexXO:Fe3+) whereas absorbance at 440 nm decreases (lost of the free XO). The dependence of theabsorbance on the dose is shown on the Figure 1.
3,5-i
• 585 nm
O 440 nm
©©.
a
'Q
30
" Q
40
o
• %
50
O
1
60-0,5
-1,5
Dose (Gy)
Fig. 1: Dependence of absorbance on dose
From this figure it follows that to the value of 30 Gy the dependence is linear and the useof the wavelenght 585 nm is 3x more sensitive than the use of 440 nm. At the line 585 nm, limitof dose determination is 0.4 Gy (at the 95% level).
XXIV DRO Demänovská dolina 130

b) the dose determination in the boron neutron capture therapyThe neutron capture therapy is a perspective method for the treatment of some types of
tumour diseases. The princip of this method is following: into the blood stream of the patient isinjected the chemical compound, containing isotope 10B. Due to its structure, the compound isselectively concentrated in the cancer cells. Than, the tumour area is irradiated by the beam ofepithermal neutrons (which are thermalized passing the tissue) and the following nuclearreaction occurs:
"fc + 'n -> 7Li + 4He + 2,792 MeV (6,31%)!0B + 'n -> 7Li + 4He + 2,314 MeV -> 7Li + y + 0,478 MeV (93,69%)
with the neutron cross-section of 3838 barns. Products of the reaction, due to its largeLET, transfer its energy directly to the cell and therefore the high efficiency of the tumourirradiation is assured. Simillary, the healthy tissue is maximally protected.
The main problem of this method is the estimation of the real dose in a tissue in situ, i.e.in the area where the nuclear reaction occurs. To solve this problem, we have proposed to usethe above mentined gel dosimeter of Fricke type which properties are very advantageous forthis purposes. To the dosimeter, we added boric acid as a source of the 10B, and the dosimeterwas exposed to the epithermal neutron beam from the neutron source, developped in theNuclear Research Institute [8], The concentration of the isotope 10B was 440 ppm.
The relative dose was measured (as the absorbance at 585 nm) as dependence on thedepth in water-phantom.The dosimeter had the form of glass tube of the diameter of 24 mm andthe longitude of 15 cm. The measurement was provided for gels with addition of the boron andwithout boron resp. The dependence of the dose on the depth in the phantom measured in thedirection of the beam of epithermal neutrons for gel with and without boron and their differenceare on the fig. 2. The difference corresponds to the reactions on nucleus IOB, where the dose inthe dosimeter without boron is done mainly by tha gamma radiation of the nuclear reactor.
-0,2 J
Depth (cm)
Fig.2: Dependence of dose on depth in the water phantom
XXIV DRO Demänovská dolina 131

ConclusionsIn our work two examples of the use of Fricke-gel dosimeter with XO and photometric
determination of a dose are described.The advatage of gel dosimeters generally are:• the possibility of the experimental determination of the 3-D distribution of integral
dose in various complicated volumes• tissue equivalence of a gel dosimeter (dosimeter is in the same time also phantom)
Further advantages specific for the described dosimeter are:• the possibility of the optical determination of a dose (significantly low price comparing
to to NMR)• very easy preparation of dosimeter and its low price
Comparing to the polymer gel dosimeters, the described system has two disavatages:• low time stability of dosimeter due to the spontaneous oxidation of Fe2 + to the
Fe3 +
• low time stability of the information about 3-D distribution of a dose done by thediffusion of Fe3 + ions due to their concentration gradient.
Our further work is oriented to the supression of these undesirable properties.
References
[3] Olsson L.E., Petersson S., Ahlgren L., Mattsson S., Phys. Med. Biol. 34(1989)43-52[2] Appleby A., Christman E.A., Leghrouz A., Med. Phys. 14(1987)382-384[3] Gore J.C., Kang Y.S., Schulz RJ Phys. Med. Biol. 29(1984) 1189 - 1197[4] Maryanski M.J., Gore J.C., Kennan R.P., Schulz R.J., Magnetic Resonance Imaging
11(1993)253-258[5] Gupta B.L., Narayan G.R., Phys.Med. Biol. 30(1985)337[6] Appleby A., Leghrouz A., Med.Phys. 18( 1991 )309 .[7] Bero M.A., Gilboy W.B., Glover P.M., Keddie J.L., Nucl.Inst. and Meth. in Phys. Res.
A422 (1999)617[8] Burian J., Marek M., Polák J., Prokeš K., Rataj J., Čsl.čas. pro fyziku 47(1997)231
XXIV DRO Demänovská dolina 132

AIRCREW RADIATION DOSIMETRY - LAST DEVELOPMENT^
Spurný FrantišekNuclear Physics Institute - Department of Radiation Dosimetry, Czech Academy of
Sciences, Na Truhlářce 39/64,18086 Prague 8, Czech Republic
IntroductionExposure to cosmic radiation increases rapidly with the altitude. At the flight levels of
commercial aircraft it is of the order of several jxSv per hour. The most of aircrew are exposedregularly to the effective dose exceeding 1 mSv per year, the limit of exposure of non-professionals defined in ICRP 60 recommendation [1]. That is why this problem has beenintensively studied from many aspects since the beginning of 90's [2]. This contributionsummarises new developments in the field during last two years. First, new internationalactivities are presented, further, new achievement obtained mainly in the author's laboratory arepresented and discussed.
International activitiesEuropean Council Directive 96/29/EURATOM implemented ICRP 60 to basic safety
standards for the protection of the health of workers and the general public against the dangersarising from ionising radiation. It was issued at the 13lh May 1996 and followed byrecommendations concerning significant increase in exposure due to natural radiation sources,cosmic radiation on aircraft board included [3,4]. It was supposed that the member states realiseall necessary to comply with the Directive before 13 May 2000. Actually, it is not a generalcase. It was found that some additional studies and administrative measures are necessary beforefull implementation. When only technical aspects of the topic are taken into account, two mainactivities are now in course.
A new research project was accepted, DOSMAX [5]. The main objective of the project isto extend the measurements and the estimation of the aircrew exposure during the period ofsolar maximum which occurs between 2000-2003 and to compare the results obtained withthese obtained between 1992-1999, i.e. during low solar activity. The project is co-ordinated byprof. Denis O'Sullivan (Dublin Institute for Advanced Studies), there are 14 participants in,among them also the author's institution. The main objectives of the project are:• Calibration and detector's characterisation in high energy radiation fields;• In-flight measurements with passive detectors and their sets;• In-flight measurements with active devices;• Simulation and calculation of doses due to galactic cosmic radiation and solar particles;• Improvement in the dose assessment; and• Dissemination of information in view to update previous document [2].
Particular attention would be devoted to cover as large periods of measurements as possiblewith the goal to try to perform onboard measurements during an intense solar eruption. It isknown, that their probability increases at the end of solar maximum period.
The creation of new working group of EURADOS on aircrew exposure was initiated inspring 2000. Its main task would be, in view of the Article 31 of the EURATOM Treaty, toharmonise the procedure used to perform individual dosimetry of aircrew in the EC memberstates. The first meeting of the group was held at Braunschweig, January 2001. It was decided tocreate four working subgroups. Their main goals will be to collect both integral and differentialexperimental data accumulated since 1991and perform a critical analysis of them; and to use^ The studies were partially supported through EC Project FI5P-CT00-0068 and the Projectsof the Grant Agency of Czech Republic Nos. 202/99/0151 and 202/01/0710
SK02K0201XXIV DRO Demänovská dolina 133

these data to compare available codes for the transport of galactic cosmic radiation through theEarth's atmosphere (CARI, EPCARD, PC-AIRE, and FREE/LUIN).
The data are now collected, some part of integral data was already confronted with theresults of calculation by means of the code EPCARD, developed under the support of DGXI ofthe EC. The author of this contribution participates in the subgroup, which collect thedifferential experimental data. He also submitted the integral dose data on 86 flights performedbetween 1991and 1999. These data were also treated by both EPCARD and CARI6 codes. Itwas found that:• the average ratio of our measured integral values of H*(10) and the values E calculated by
CARKis 1.12+0.20;• the average ratio of H*(IO) values calculated by CARI6 and EPCARD is 0.88+0.11; and• the average ratio of E values calculated by CARI6 and the H*(10) values calculated by
EPCARD is 1.04+0.12.The agreement of all these sets of data can be from the point of view of requirementsconcerning the precision of individual dosimetry data [6] taken as very satisfactory.
Review of last results obtained in the author's laboratoryIndividual dosimetry of Czech air companies aircrew
All activities realised in the author's laboratory since 1991 have been recently describedin review article [7]. As far as the individual aircrew dosimetry is concerned, ICRP 60recommendations were incorporated to the Czech regulation already at 1997. Since the end ofthat year, a preliminary analysis of the exposure of Czech air company's aircrew members wasstarted with the goal to develop an „optimal" procedure of aircrew exposure level estimation.The analysis was based on the CARI code [2]. The main principle of the modelisation, agreedwith air companies, were the choice of an optimum flight altitude for each aircraft, and that of aconstant times of taking off and landing. The procedure was further developed, the code CARIhas been regularly changed to later versions (now 6), which calculate already the exposure levelin the effective dose E, the quantity used for the limitation. It was finally proposed to the Czechauthorities to be used for companies concerned. It has been accepted and used since 1998.Figure 1 shows E-rate distributions in the case of CSA company and 1998 year, figure 2 theaircrew effective dose distributions for all air companies concerned for the years 1998-2000.
0,4
:0,3
: 0,2
' 0,1
0,0
CSA- E-rate distribution 1998
ír1
1
0.0- 0.5-0.5 1.0
1.0-1.5
1.5.2.0
2.0- 2.5-15 3,0
Erato,
3.0-3.5
3.5-4.0
40- 45-4.5 5.0
5.O-5.5
0,60
0,45|
a
o 0,30
Distribution of E
0,15
• OS/tawSITS
^
m
i.' I
r?
!
;
j
o.o- 0,2- oA o,e- o,8- 1,0- - u - 1A~ i,e- 1,8- 2,0- 2,2- 2,4-0,2 0,4 0,6 0,8 1,0 1,2 1,4 1,6 1,8 2,0 2,2 2,4 2,6
Annual effective tJosa, mSv
Fig.l: E-rate distributions of CSA aircrew in 1998 Fig.2: Annual E distributions of aircrewof Czech companies
Following main characteristics can be deduced from these figures:• E-rate distribution is large, one can not envisage to obtain correct estimation of the exposure
from simple flight time;• annual average E - value for all companies were in the period 1998-2000 a little lower than
2 mSv, higher than for many other groups of occupationally exposed persons [8];
XXIV DRO Demänovská dolina 134

• for two companies flying only short haul routes in the Europe and to its holiday's regionthere is a one rather narrow maximum, while the distribution for the third one, flying alsolong haul flights to the North America and the Far Orient is more large and characterised bytwo maxims; the second one corresponding to North-Atlantic flights.
Results of recent experimental studiesFirst experimental studies of the aircrew exposure were in Czech Republic realised in
1991-1995 years. Another large series was realised during 1999 year, in collaboration with CSAcompany [8]. For each flight, all necessary parameters have been received and the exposure fora flight has been also calculated by means of CARI code. The results of calculation werecompared with the measured data, obtained by means of all available instruments and methodscalibrated in CERN high-energy reference field (concrete shielding) [2]. The tendenciesexpected were confirmed by our experimental results (see Table 1), i.e. the relative importanceof both component of radiation field at northern parts is close to be the same, the importance ofhigh LET component diminishes when going to the south. The experimental values of H*(30)were a little higher, in average by (9±6) %, than theoretical E-values.
Table 1: Relative contributions of low and high LET components to the total dose equivalent.
Destination from Prague
Northern AmericaNorthern EuropeSouthern Europe
Abu DhabiAbu Dhabi - Bangkok
Ratio of values high to low LETcomponent
1.15 "1.090.860.5140.439
Contribution of high LETcomponent to the total
0.535 !)
0.5210.4620.3380.291
i} Uncertainty of values is estimated to about ± 15 % ( la)
At the spring of 2000 we have acquired a new measuring instrument, MDU-LIULIN, anenergy deposition spectrometer base on a Si-detector. It is in more details described in anothercontribution to this conference [9], the results of calibration in CERN high-energy referencefields included. We have used three modules available for onboard measurements during morethan 10 individual flights. The directly experimentally measured data, i.e. event rate and thedose in Si were transformed on the base of CERN calibration to the H*(10) of reference CERNvalues [10]. They were compared with the values of E calculated by means of the CARI code.Some of results obtained are presented in Figures 3 and 4.
Flight Profiles JFK-PRG15-16/04/01
Tlmt ofnight,hour»
Flight profiles SOF- PRG 21 -08
MOOOg"
17:51 18:00 1«:2J 18:57Flight Bme, UTC*4
Fig.3: Flight profiles - flight New York -Prague Fig.4: Flight profiles - flight Sofia -Prague
One can see there that the agreement of calculated data and the results of measurementstransformed on the base of CERN calibration is satisfactory. The differences in integral values
XXIV DRO Demänovská dolina 135

do not exceed about 15 %. Differential data vary more when the acquisition time (AT) is short.One can see on the figures, that these variations are more important for the flight from Sofia toPrague (AT 5 min) than for the flight from New York to Prague (AT 10 min). One can see alsoin the figures that these variations are due to statistical reasons (much less of impulsions) muchhigher for higher energy depositions, i.e. for high LET component of the radiation field.
One of the modules MDU-LIULIN permits to be powered with Li-batteries giving himthe autonomy about 1400 hours. The module can be now placed, thanks to the understanding ofCSA, onboard of one of A310-300 aircraft for long term exposure. The first such exposure wasrealised between 22nd March and 7th May 2001, the aircraft was flying very intensely (about 660hours on the altitude). The experiment was very successful, just during the flight from Prague toNew York on the 15th April, an important solar flare occurred (ground level event-GLE 60). Theresults of our measurements together with CARI calculations (corresponding only to thegalactic component of cosmic radiation) and flight altitude are presented in the Figure 5. Onecan see there that the excess above galactic component level is about 80 % for the event rate,more than twice for dose values. It means also, that the spectrum of events in Si is different forgalactic and solar components. The results are now analysed, two other long-term exposureshave been already, realised before the autumn 2001.
PRG-JFK 15/04/01 GLE 60 influence12
10:48 12:00 13:12 14:24 15:36 16:48 18:00 19:12Time, UTC
Fig.5: Dose and flight profiles during the flight at the time of intense solar flare
REFERENCES1. 1990 Recommendations of the International Commission on Radiological Protection. ICRP Publication 60,
Annals ofthelCRP 21,1991, No. 1.2. Exposure of Air Crew to Cosmic Radiation. In: McAulay IR et al. (eds.) EURADOS Report 1996-01, ISBN 92-
827-7994-7, Luxembourg 1996.3. Council Directive 96/29/EURATOM of 13 May 1996, Official Journal of the EC, No. L. 159/14. Recommendations for the Implementation of the Title VIII of the European Basic Safety Standards Directive
Concerning Significant Increase in Exposure due to Natural Radiation Sources. EC, DG XI, ISBN 92-827-5336-0, EC 1997.
5. EC Contract No.FIGM-CTOO-00068: "DOSMAX", Co-ordinator O'Sullivan D (DlAS Dublin), 2000-2003.6. International Commission on Radiological Protection 75: General Principles for the Radiation Protection of
Workers. Pergamon Press, Oxford 1997.7. Spurný F.: „Exposure of Air Crew to Cosmic Radiation. Calculation and Experimental Approach"; will be
published in: High Levels of Natural Radiation and Radon Areas: Radiation Dose and Health Effects, : A.Bayer, Elsevier Science 2001
8. Prouza Z., Spurný F., Klener V., Fojtíková I., Fojtík P., Podškubková J. Occupational Radiation Exposures inthe Czech and Slovak Republic. Radiat Prot. Dosim. 1994; 54: 333-336.
9. Spumý F., Dačev C : "Semiconductor Spectrometer for Radiation Protection Application", this Proceedings10. Mitaroff A., Silari M.: "The CERN-EU high-energy Reference Field (CERF) facility for dosimetry at
commercial flight altitudes and in space", CERN-TIS-2001-006-RP-PP
XXIV DRO Demänovská dolina 136

SEMICONDUCTOR SPECTROMETER FOR RADIATIONPROTECTION •>
Spurný František**, Dačev Cvetan***'Nuclear Physics Institute - Department of Radiation Dosimetry, Czech Academy of
Sciences, Na Truhlářce 39/64, 18086 Prague 8, Czech RepublicSolar Terrestrial Influence Laboratory, Bulgarian Academy of Sciences, Sofia
IntroductionThe radiation fields on aircraft board and for other radiation protection application are
complexes they contain the particles with energies up to few hundreds MeV [1]. Obviously, onedistinguishes the components with low resp. high linear energy transfer (LET). Recently, wehave acquired a new measuring instrument, MDU-LIULIN, an energy deposition spectrometerbase on a Si-detector [2,3]. The spectrometer was originally developed and largely testedonboard of cosmic vehicles, its sensitive element is a Si-diode. The spectrometer has beencalibrated in photon, neutron and high-energy radiation reference fields (CERN [4]), The energydeposited in the detector by a particle is analysed by a 256-channel spectrum analyser, it permitsto distinguish the contribution of different types of radiation to integral dosimetry quantities.The spectrometer has been, since April 2000 used for some radiation protection applications,mostly on aircraft board. Results obtained are presented, discussed and analysed.
Materials and methodsSemiconductor spectrometer MDU [2,3]
The Mobile Dosimetry Unit (MDU) can monitor simultaneously the doses and numbersof energy deposition events in a semiconductor detector. It consists of the detector itself, acharge-sensitive preamplifier, 2 micro-controllers, a flash memory and Li-ion cells. Pulseanalysis technique is used to measure the deposited energy in the detector. The unit is managedthrough specially developed firmware. Plug-in links provide the transmission of the data storedin the flash memory through the control and interface unit toward the standard PC. Same plug-in link is used to recharge the Li-ion cells in the MDU's. The MDU is designed as handyequipment. After switching on, it starts to measure the spectrum of energy deposition events.The acquisition time is variable in the interval 10 - 3539 sec with 10-sec step. After finishing,the data are stored in different places of the memory, which later is used to recalculate the timeof the measurement. The amplitude of the pulses is proportional to the energy loss in thedetector. Final adjustment of the energy scale is made through the 60 keV photons of 241Am.The amplitudes are digitised and organised in a 256-channel spectrum.The dose D [Gy] is calculated from the spectrum as:
D = K.*$Ei*AtfMD,
where MD is the mass of the detector in [kg]; E; is the energy loss in the channel i; Ai is thenumber of events in it; and K is a coefficient.
In the working mode the instrument is operating under the software of the micro-controllers. The operational time of the instrument depends on the lifetime of the accumulatorsand on the rate of the memory fills up. In the case of continuous operation the lifetime is about120 hours with the standard 1350 mAh Li-Ion accumulators. In the mode of data transfer theinstrument is switched on by special command when it is connected to the PC. In this mode the
^ The studies were partially supported through EC Project FI5P-CT00-0068 and the Projectsof the Grant Agency of Czech Republic Nos. 202/99/0151 and 202/01/0710
XXIV DRO Demänovská doli na 137SK02K0202

connection of the data with real time and the calculation of the physical values is performedthrough a special program in the PC.
Results and discussionEvent spectra in reference fields
First, MDU units available were exposed in reference radiation fields. The resultsobtained at some photon and neutron sources are presented in Fig. 1 and 2.
0,00001
0,000001
- » - Cs-137 experiment* Co-60 experiment
-{J-Cs-137 calculation—A— Co60 calculation
500 1500 2000
Neutron sources event spectra
I 0,01cI 0,001
~ 0,0001at
0,000001
hAm A.
a
< AmBe•O—Cf 252-A—AmF
ill) II rj
I• i f f *
4 6Edep.MeV
10
Fig. 1: Event spectra in some photon beams Fig. 2: Event spectra at some neutron sources
Not only experimental but also theoretical event spectra in the semiconductor arepresented in Fig. 1 for I37Cs and 6 0Co photons. They were calculated by means of EGS 4-transport code and one can see that the agreement of both spectra is rather satisfactory. Figure 2presents the event spectra at some radionuclide neutron source. What should be stressed is largedifference in the event spectra for neutrons as compared to photons. It could permit todistinguish photon and neutron induced events in other radiation fields.
MDU units have been tested since the spring 2000 during three calibrations runs in theCEC-EC high-energy reference field behind the concrete shield [4]. The examples of eventspectra in this field are presented in Figs. 3 and 4 as a function of the reference field intensity.
1,06*06
i,oe*«s
1,06KWí•1,06+03
i.j I.OEMtt>
1,06HH
1,0E*00
1,0601
Inte
EU8ŕ^ ...
TIS
i ^
gg
S
i
tyinfluen
- o - W O T-•-1200T-O-28WT
- * - « 0 0 s |
ce on even
ÍSHPF
it spectra
-.TJiŤ''Tr^'ŕ1'"S'M'—^r
v * • '̂•"•T-
1 i
A—»É -
10 15Edep,MeV
140000 •
120000
o 10O000JEi!=• aoooo
2
o 60000
40000-
20000
Ol
Intensity Influenca on event spectra, kwE dep
kzM:
ftrt
I—0—BOOT
-O-JSCOT
—
0,2 0,4 o,sE dep, MaV
1.2
Fig.3: Intensity influence on event spectraall Ed e p
Fig.4: Intensity influence on event spectralow Edep
First. It should be stressed, that in this case the spectrum is still much larger than in the case ofradionuclide neutron sources, reaching the highest values of the energy deposition above
XXIV DRO Demänovská dolina 138

20 MeV. As far as spectra form is concerned, one can see in Fig.3 that the spectra becomeharder with the increasing beam intensity. It is the consequence of decreasing importance of themuon background [4]. This influence is more visible in Fig.4, where the absence of muons atside (S) position is clearly manifested for the lowest values of energy deposition. The responseof MDU modules in CERN reference field increases linearly with the intensity, the behaviour ishowever quite different for low and high values (threshold about 1 MeV) of the energydeposition, see Figs 5 and 6.
Intensity influence on D(Si)-rate
—»-MDU05!owEifcp
~*-MDU01MgdE*|>
-•-MDUHhighBfcp
- * — MOUWhlghEdep
2000 3000
PIC counts per burst
Intensity influence on D(Sf) per PIC count
o
í-ľ=•200tnS
100
V"1~
-Ä-MX)01low
-D-NDXaltm
- 0 — Mxnsicw
-«-M3U02hlgh
-•-MDUOSWsh
*
340 *
w
Ď
20
2000 3000
PIC courts per bust
Fig.5: Intensity influence on D(Si) per hour Fig.6: Intensity influence on D(Si) per 1 countof monitor
Muon background contributes only to signal in low Edep region. Due to that there is anon-zero response in this region when extrapolated to the zero beam intensity. It is not the casefor high E d e p , there the increase of signal is proportional to the beam intensity, i.e. independenton the number of monitor counts (see Fig.6). It is very important for the interpretation of thedata measured in reference and similar fields.
Doses in reference fieldsAs far as the absolute values of dose calculated from the spectra is concerned, they were
in very good agreement for 60Co photons, the value obtained for 137Cs photons was about 8 %lower than the reference one. In CERN reference field, the dose calculated for low Ed e p regionwere about 40 % lower than values measured with other standard low LET measuringinstruments (RSS 112 chamber, TLD's, etc.). We have observed the same behaviour also forindividual electronic dosemeters based on Si-diode and taken it into account for theinterpretation of these detector's readings [5].
The dose absorbed from neutrons in Si calculated from the event spectra in the case ofneutron sources and in CERN reference field are, as expected, lower than the dose absorbed in asmall volume of human tissue. The values of relative response are given in Table 1.
Table 1: Relative responses of MDU to neutrons in some reference fields
^Neutron source *„**&/AmF
AmBeCERN - concrete shielding
Av^rag^rieutrbn. •e.ttfergy, MeV1.52.14.4
49.5* 11 * l
Reíatívéiteápoňse"?''.;0.260.480.600.76
It should be stated that their values are, nevertheless, for higher neutron energies relatively high.
XXIV DRO Demänovská dolina 139

Examples of semiconductor spectrometer use for radiation protectionFirst we tried to appiy MDU modules to estimate natural radiation background and to
estimate the range of its use as a function of dose rate level. One of modules was exposed in thePb-shield used to minimise TLD's background for natural radiation. The kerma-air ratemeasured in it by means of TLD's was (35±2) nGy per hour, the D(Si) rate measured by MDUwas 39 nGy per hour. One can therefore use the MDU modules for the measurements of naturalradiation background, we proved it through direct comparison with RSS 112 ionisationchamber. The linearity and maximum dose rate measurable were tested in etalon photon beamsof author's laboratory. It was found that the linearity is kept up to the kerma-air rate valuesabout 5 mGy per hour.
Main effort was given to the measurements on aircraft board. It was actually observedthat the spectra registered at CERN reference field are very similar to the spectra registered onthe aircraft and/or balloon (see Fig.7). To interpret the data measured on aircraft board (D(Si)),we decided to use CERN reference field results. The dose in Si measured below 1 MeV wassupposed to represent the contribution of low LET radiation, the dose above 1 MeV that of highLET component (neutrons). In this way, D(Si) measured on board was recalculated to obtainapparent H*(10) values. As an example, the results obtained in the case of CSA flight fromOsaka to Zurich (May 2000) are presented in Fig. 8. One can see there that corrected values area little (less than 10%) higher than E-values calculated by means of CARI6 code, very close forboth modules used. It seems therefore that the use of MDU modules for different applications inradiation protection is promising.
1
0,1
• 0,01S
•D
S 0,001
0,0001
0.00001
f—Dose distribution comparison
—•—cewTc—EJ—balloon
—*— Osaka-Zurich
—O—gamma
T S H ^ H knra
—
m
í t-Fi 1
U Q
f*1
' • • • •
i§tí
"í —̂
tO 12 14 18 1B 20 22E dep. MeV
Flfght profiles Osaka-Zurich 20/05/00
4 6 8Fígihttime, hours
Fig.7: Comparison of dose spectral distributions Fig.8: Flight profiles obtained by MDU's andCARI
References1. EUR ADOS, Exposure of air crew to cosmic radiation EURADOS Report 1996-01, eds.:
McAulay I. et al., Luxembourg, (1996), 1-77.2. Dachev, Ts.P. et al.: "Detailed Study of the SPE and their Effects on the Dose Rate and
Flux Distribution Observed by LIULIN Instrument on MIR Space Station." RadiationMeasurements, 30 (3) (1999), 317-325.
3. Dachev, Ts.P., Spurný, F. et al.: „Calibration Results Obtained with LIULIN-4 TypeDosemeter." Paper F2.2-0025 presented at 33rd General Assembly of COSPAR, Warsaw,Poland, July 2000.
4. Mitaroff A., Silari M.: "The CERN-EU high-energy Reference Field (CERF) facility fordosimetry at commercial flight altitudes and in space", CERN-TIS-2001-006-RP-PP.
5. Spurný F.: „Experimental Approach to the Exposure of Aircrew to Cosmic Radiation."Radiat. Prot. Dosim. 70 (1997), 409-412.
XXIV DRO Demänovská dolina 140

MONITORING OF CARBON 14 IN ATMOSPHERIC CARBONDIOXIDE
/. Světlíkl, V. Michálek 2, P. Rulík 2, L. Tomášková *1 Nuclear Physics Institute of the AS CR, Department of Radiation Dosimetry, Na
Truhlářce 39, 180 86 Prague, Czech Republic2 National Radiation Protection Institute, Šrobárova 48, 100 00 Prague, Czech
Republic
A purpose of this article is to present the first data of the atmospheric C-14 monitoring in CO2
form. In the Prague-Bulovka locality atmospheric CO2 have been continuously collected by absorption in0,7M NaOH solution. The samples were one month cumulated. Afterwards, the CO2 was extracted fromthe NaOH solution and benzene was synthesised. The benzene was measured by liquid scintillationcounting (LSC). The monitoring results from January to July 2001 period are discussed and comparedwith the results from other countries.
Carbon 14 with a half-life of 5730 years is a significant radionuclide with globaloccurrence and with particularly anthropogenic origin. This radionuclide is a clear beta emitterwith E™^ 156.5 keV[l].
Carbon 14 with natural origin is produced by nuclear reactions induced by cosmicradiation in higher atmospheric layers. The biggest part of the anthropogenic C-14 wasproduced by nuclear bomb tests during 1960's [2, 3]. Actual production of the anthropogenic C-14 is mostly results from the operation of nuclear energy facilities. Nevertheless, thebackground level of the activity of atmospheric C-14 has decreasing trend over the last decadescaused by deposition in environmental components (esp. oceans and sediments) and diluting byfossil carbon.
Considering biological importance of this radionuclide in livings and given its long half-life considerable attention has to be paid to C-14 concentration in the environment, especially inthe NPP's vicinity [4-5]. In the case of NPP normal operation the effluents of otherradionuclides are only fraction of allowed limits and C-14 is significant part of anthropogenicradionuclides supply to the effective individual dose from these sources.
Worldwide the largest number of C-14 determination is performed for a purpose ofradiocarbon dating of carbon containing samples. A range of the method, depending oninstrumentation, quantity, and type of samples, approaches to 100 000 years BP. Radiocarbondating has applications in geology, archaeology, hydrogeology, climatology, oceanology,paleontology, etc.
Methods of C-14 determinationThe most frequented conventional method (counting) of C-14 determination is the liquid
scintillation counting (LSC). Benzene from the carbon containing samples is usuallysynthesised and then counted by low background LSC counters, benzene counting enablesmaximum amount of sample carbon in measuring vial. The benzene is also a solvent in thescintillation cocktail and only small quantity of scintillator needs to be added (0.15 g ofscintillator per 10 g of benzene). If the benzene with low amount of other hydrocarbons isprepared, the quantity of sample carbon can be calculated from weight of the benzene in acounting vial. Counting of benzene is relative robustness and characterised by a high countingefficiency [6].
Determination of C-14 by Accelerator Mass Spectrometry (AMS) enables to analyseextremely small quantities of sample. Radiocarbon dating of nearly 100 000 years old samplesby AMS is possible. Considering the expensiveness this instrumentation is not accessible in ourcountry.
SK02K0203XXIV DRO Demänovská dolina 141

In some radiocarbon laboratories is also measured C-14, in CO2 or CH4 form, by gasproportional counters.
LSC measurement of C-14 in carbonate form in water solution, carbonate precipitation,or carbon dioxide in basic organic sorbents (CarboSorb, triethanolamin) with liquid scintillationcocktails does not need long time for benzene synthesis. Principally, the method has thefollowing disadvantages: small possible amount of sample carbon in counting vial, complicateddetermination of sample carbon loaded with bigger uncertainty, and also interference of otherradionuclides in the sample is more possible. The method is applicable for measurement ofhigher C-14 activities.
Collection and treatment of atmospheric C-14 samplesIn the beginning of 2001, the monitoring of atmospheric C-14, in CO2 form, was
experimentally launched in the Prague-Bulovka locality. Carbon dioxide sample was collectedcontinually and cumulated in the one-month period.
Apparatus for atmospheric carbon dioxide collection
-0—•*•
•
A I í 8
1 - aerosol filter, 2 - air pump, 3 - gas meter, 4 - flow meter, 5 - humidifier, 6 - ampoule withNaOH solution I, 7 - ampoule with NaOH solution II, 8 - water gauge
Air was sampled about 8 m above surface, filtered from aerosols and humidified by 1%H3PO4. Carbon dioxide was sorbed in two serial engaged ampoules containing 0.7 M solution ofNaOH with a low and controlled initial amount of carbonates. Both carbonates containingsolutions were in two-week period replaced and processed.
Concentration of carbonates was volumetrically determined in solutions. Quantity ofsorbed CO2 and yield of sorption was then calculated (this yield fluctuated between 98.2 - 99.0%). The total amount of carbon dioxide in a normalised volume of sampled air was thencalculated with correction of the sorption yield.
Carbonates in NaOH solutions were precipitated by an addition of carbonates-free CaCl2
and the precipitate was cumulated for one month.After one-month period the precipitate was hydrolysed by 10% hydrochloric acid and
carbon dioxide was collected in two liquid nitrogen cooled traps. Carbon dioxide was then driedby slow sublimation through column filled by silikagel. A carbide synthesis reactor withmetallic lithium was evacuated and heated to temperature.,900 °C. The pressure of the carbondioxide inputting to the reactor did not exceed 2 kPa. When CO2 was admitted into the reactorand the pressure decreased below 200 Pa the reactor vessel was evacuated. To complete lithiumcarbide synthesis the reactor is subsequently heated for 30 minutes at 900 °C under dynamicvacuum. The formation of acetylene gas was accomplished by hydrolysing LÍ2C2 at roomtemperature by adding demineralised water. Acetylene was collected in two LN2 cooled trapsand hydrogen produced by reaction of excess Li with water was pumped out. Residuum ofwater vapours was removed by sublimation through column filled by silikagel. Acetylene wasslowly sublimed onto the catalyst containing V2O5 and pressure of C2H2 did not exceed 3 kPa.
XXIV DRO Demänovská dolina 142

Benzene was removed from catalyst after expiring approximately 12 hours and collected in LN2
cooled trap.
Samples measurement by liquid scintillation spectrometryBenzene samples were weighted into 0.8 ml teflon vials and scintillator (b-PBD) was
added. The samples were counted by TriCarb 1050 TR/SL for 2800 minutes. Calibration wasperformed with NBS oxalic acid HOX II [7]. Measured activities were calculated and resultswere reported as 514C following generally accepted Stuiver-Polach notation [8].
Results and discussionThe activities of C-14, in CO2 form, measured in period January - July 2001 in the
Prague-Bulovka locality are reported in the figure. The table also reports activity concentrationsof carbon 14, which were calculated from CO2 concentration. The results of activityconcentration are burden by higher uncertainty caused by volumetric determination ofatmospheric CO2 concentration.
January
February
March
April
Mai
June
July
Average value
514C
17 ±15
55 + 16
58 ±19
-5 + 17
29 ± 1 6
-29 ± 44
22 + 11
21 + 12
a (mBq.m"3)
52.6 ± 5.3
46.9 ± 3.4
43.6 ± 3.2
44.0 ± 2.7
46.9 ± 2.9
46.9 ± 2.9
46.9 + 2.9
46.4 ±1.2
100
C-14 monitoring in atmospheric carbondioxide
1-01 11-01 111-01 IVW1 V-01 VI 01 Vll-01
Uncertainties reported in the diagram and in the table are combined standard uncertainties.
The observed average value of 814C 21 ± 12 %o is lower than background valuesestimated for 2001 on the basis of long term monitoring in surrounding countries [9-11]. Also,the reference value of 814C for the year of 2000 in the locality Buchenblättern, Switzerland is 94± 3 %o [12]. The difference between the value in our locality and probable background values inthe Czech Republic is caused primarily by local influences of carbon dioxide released by fossilfuel combusting.
XXIV DRO Demänovská dolina 143

R e f e r e n c e s1. CM. Lederer - V.S. Shirley-ed.: „Table of Isotopes" IVSRDS 7th edition, 1978.2. H. A. J. Meijer, J. Plicht: "Comparing Long-Term Atmospheric 14C and 3H Records near
Groningen, the Netherlands with Fruholmen, Norway and Izaňa, Canary Islands I4CStations". Radiocarbon, 37(1), 1995
3. R. Berger, W. F. Libby, G. V. Alexander, J. F. Mead, J. F. Ross: „Atmospheric BombRadiocarbon as a Tracer in Human Beings,,. Advances in Tracer Methodology 3, (1966),321-329
4. N. McNamara, M. McCartney: "A review of 14C Waste Arising from the Nuclear Industryin the United Kingdom". Radiocarbon, 40(1), 1998
5. K. Stenstrom, G. Skog, C. Thornberg, B. Erlandsson, R. Hellborg, S. Mattson, P. Person:" l 4 C Levels in the Vicinity of Two Swedish Nuclear Power Plants and at Two "Clear-Air"Sites in Southernmost Sweden". Radiocarbon, 40(1), 1998
6. S.K. Gupta, H.A. Polach: Radiocarbon Datirig Practices at ANU. Radiocarbon Laboratory,Research School of Pacific Studies, ANU, Canberra, 1985.
7. R. J. Schneider, A. P. McNihol, M. J. Nadeau, K. F. Reden: "Measurements of the OxalicAcid II/Oxalic Acid I Ratio as a Quality Control Parameter at NOSAMS". Radiocarbon,37(2), 1995
8. M. Struiver, H.A.Polach: "Discussion: Reporting of C-14 Data". Radiocarbon, 19(3), 19779. Levin, B.Kroner: "1997. DI4CC>2 Records from Schauisland. In Trends: A Compendium of
Data on Global Change." Carbon Dioxide Information Analysis Center, Oak RidgeNational Laboratory, U.S. Department of Energy, Oak Ridge, Tenn., U.S.A.
10. T. Kuc, M. Zimnoch: "Changes of the CO2 Sources and Sinks in Polluted Urban Area(Southern Poland) over the Last Decade, Derived from the Carbon Isotope Composition".Radiocarbon, 40(1), 1998
11. Krajnar-Novič, N. Horvatinčič, B. Obelič: "Two Decades of Environmental IsotopeRecords in Croatia: Reconstruction of the Past and Prediction of Future Levels".Radiocarbon, 40(1), 1998
12. H. Loosli, U. Schoetter, H. Burki, H. Fisher, M. Moll, F. Cartier, J. Lôhle, W. Weiss, H.Sartorius: "Tritium, Kohlenstoff-14 und Krypton-85" in Environmental Radioactivity andRadiation Exposure in Switzerland. OFSP, Division of Radiation Protection, 2000
XXIV DRO Demänovská dolina 144

AEROSOLS RADIOACTIVITY IN THE BRATISLAVAATMOSPHERE
/. Sýkora, M. Chudý, L. Ďurana, K. Holý, J. MerešováDepartment of Nuclear Physics, Comenius University, Mlynská dolina Fl,
842 48 Bratislava, Slovakia
1. Introduction
Radionuclides in the atmosphere come from various sources. Long-term monitoring ofradioactivity of atmosphere allows to obtain useful information about radiation in theenviroment due to natural and man-made radionuclides and enables evaluation of their impacton peoples. Cosmogenic radionuclides present in ground level air enabled also study ofdynamics of exchange and transport processes between various layers of atmosphere.Cosmogenic 7Be is very suitable radionuclide to such investigation. It is produced by theinteractions of cosmic radiation with the high levels of atmosphere by spallation of oxygen andnitrogen. This reaction produced BeO and Be(OH>2 which diffuse through atmosphere untilthey attach to an atmospheric aerosols. There are transported from stratosphere and uppertroposphere to the ground-level air by exchange processes between air masses. Activityproduced in stratosphere has residence time about a year and is transferred in troposphere,where the residence time is about sixt weeks. Transfer to eartlťs surface is largely accomplishedby gravitational settling and precipitation processes. Concentration of cosmogenic 7Be maysignificantly vary with altitude, also with latitude not only because of location of production,but because of atmospheric mixing process and half-life. 7Be is relatively short-lived (Ti/2 =53.3 d) and emits 477.6 keV gamma rays with relative intensity 10.3 %. Variation in annualmean 7Be concentration in long term monitoring is attributed mainly to changes in theatmospheric production rate, while seasonal summer incrasing 7Be concentration is consideredto be due to strong stratosphere to troposphere exchanges. The flux of primary galactic cosmicrays that attact on the Earth's atmosphere is affected by the solar activity. Because 7Be ispurely outdoor origin, it is also suitable as a tracer in experiments examinig the ingress ofaerosols into buildings.
From natural radionuclides is interesting long lived 2 1 0Pb (Tm = 22.3 y) - progeny of theprimordial 238U-226Ra-decay chain, which emits 46.5 keV gamma rays with relative intensity 4%. In opposite to 7Be , it is mainly produced in the atmosphere near ground level by the decayof rare gas 2 2 2Rn, which emanate from soil. After decay of radon, the 2 1 0Pb attach on theaerosols and their fate will become fate of the carrier aerosols. Also 2 1 0Pb as well as 7Be is verysuitable for studying of the environmental processes such a aerosols transport and residencetimes in the troposphere, aerosols deposition velocities, and aerosols trapping above the groundvegetation. Informations about 2 1 0Pb concentration is also important from radiohygienical pointof view, because of its long half-life can contribute to radiation dose to man.
2. Experimental
2.1 SamplingRadioactivity of atmospheric aerosols was typicaly monitored two times weekly in
locality Mlynská dolina in Bratislava. Collection period was obviosly about 3-4 days at air flowrate about 70 m3h"]. Aerosols were collected on nitrocellulose membrane filters (PRAGOPOR4) with area 255 cm2 and pore size 0.85 Dm. __.
XXIV DRO Demänovská dolina 145 SK02K0204

2.2 MeasurementThe aerosols filters were masured in low-level background shield [1] using the Ortec
HPGe detector with Be window (FWHM at 122 keV 1 keV, peak efficiency at 46.5 keV about15 %).
Results and discusion
In our laboratory we measured temporal variation of 7Be concentration in theatmosphere in period 1977 -1994 years [2] (Fig.l). The aerosols were collected through everymonth at Hydrometeorological Institute in Bratislava - Koliba, latitude 48° 10' and altitude 286m above sea level.
1977 1980 1983 1986 1989 1992
Fig. f. Quarterly mean 7 B e concentration during the investigated period
Since end of year 2000 we have started to continue monitoring radioactivity ofatmosphere aerosols in new locality in Bratislava -Mlynská dolina. Beside 7Be we measuredalso 2 I T b radionuclide aerosols concentration. Results until September 15. are on Fig. 2 and 3.
crCD
E,_o
I0)oĽoo
.QD. 0.2-
0.0
01/11/00 01/01/01 01/03/01 01/05/01 01/07/01 01/09/01
Date
Fig 2. Temporal variation of 2 ! 0Pb concentration in aerosols
XXIV DRO Demänovská dolina 146

For measured values 7Be concentrations are considered corrections for decayradionuclide during the time of filters collection, time between end of collection andmeasurement and decay during the time of measurement.
co
CDO
8Q)
m
OT -. , . r
01/11/00 01/01/01 01/03/01 01/05/01 01/07/01
Date
01/09/01
Fig. 3 Temporal variation of 7Be concentration in the aerosols
Obtained results for 7Be concentrations in aerosols shows seasonal summer maximum,but for 2 I 0Pb concentration in aerosols the seasonal variations are not evident. The temporalvariations of this radionuclide which is originated in ground-level atmosphere are moresensitive on meteorological factors and can be also influenced by the industrial activity. Forbetter understanding is needed long term monitoring.
References
[1] I. Zvara, P. Povinec, I. Sýkora, M. Sakanoue, Pure and Applied Chemistry 66 (1994) 2537--2586
[2] L. Ďurana, M. Chudý, J. Masarik, J. Radioanal. Nucl. Chem. 207 (1996) 345-356
XXIV DRO Demänovská dolina 147

TGF-BETA AND APOPTOSIS - RAT MODEL OF RADIATION
PNEUMONITIS.
J. Škopek1, J. Ôsterreicher2, L. Navrátil1, M. Králik2, J. Vávrová2, J. Knížek2, A.Macela2.
1 Department of Biophysics, 1st Medical Faculty of Charles University,Prague 130 00, The Czech Republic.
2 Department of Radiobiology and Immunology, Purkyně Military Medical Academy,Hradec Králové, 500 01, The Czech Republic.
Purpose: To measure the involvement of bcl-2, apoptosis, TGF-P, number ofneutrophils and other markers in the rat model of induced radiation pneumonitis (RP). Todescribe sub-sequential changes in irradiated lung tissue.
Materials and methods: Wistar male rats were irradiated with 15 Gy (0,96 Gy/min.).Six groups of irradiated animals were studied in 1,2, 3, 4, 5, and 8 weeks following radiation.Non-irradiated animals were used as a control. Amount of sub-population of TGF-P (|31, 2, and3), bcl-2 positive cells and neutrophil number were measured within the tissueirnmunohistochemically, alveolar šeptal thickness was also determined.
Results: Bcl-2 production was inhibited during the whole experiment (1/3 to 1/2 of thecontrol values) in the irradiated tissue. Significantly higher number of neutrophils were found 3,5, and 8 weeks after irradiation. TGF-(31 positive cells were found from the beginning with themaximum 4 weeks after irradiation. Higher amount of TGF-beta 2 positive cells were measuredin all intervals after irradiation with the maximum 1st week following radiation. Significantlyhigher TGF-beta 3 positive cell number in irradiated rats were seen, except 2 weeks afterirradiation, in all other periods. The maximum amount of TGF-beta 3 was found 8 weeks afterirradiation. Correlation coefficient between neutrophil number and TGF-J33 immunoreactivecells was 0.621.
Conclusions: We proved TGF P 1 to be important marker of post-irradiation reaction.Besides, we suggest that TGF-p 3 expression might be closely related to the activity ofneutrophils and activity of the process in irradiated lung tissue. We proved our recent findingsof suppression of the anti-apoptotic activity after lung irradiation.
Acknowledgements: Grant of the CR Defence Secretary, MO 66 02 03 98 127, theCzech Ministry of Education grant, MSM 111100005, Pharmacon Research, Prague.
SK02K0205
XXIV DRO Demänovská dolina 148

)IL-TQ-MEAS
TRANSFER FACTORS FOR RADIO CAESIUMIN DIFFERENT SOIL TYPES IN THE CZECH
Josef Ted, Reza Mirchi, Irena Malátová, Vlasta Pešková, Eva SchlesingerováNational Radiation Protection Institute, Šrobárova 48, 100 00 Prague 10, Czech
Republic
This study was perform in frame of the SAVEC project (SAVEC = Spatial Analysis ofVulnerable Ecosystems in Central Europe; Európa Union project). The aim of the SAVECproject was to develop a user-friendly software package that will allow the identification ofareas vulnerable or resilient to radiocesium deposition in the Central European countries:Poland, Hungary and the Czech Republic. The software package will incorporate a semi-mechanistic soil-to-plant transfer model which uses commonly measured soil properties toestimate the dynamic behaviour of deposited radiocesium. This model was developed for theEuropean Commision IVth Framework programme Spatial Analysis of Vulnerable Ecosystems(SAVE) project. In the SAVEC software package, spatially variable data (including 137Csdeposition, soil property, agricultural production and dietary data) can be used to assess theconsequences of the deposition in the three Central European countries following nuclearaccidents.
The SAVEC project collates data of sufficient resolution specific to Poland, Hungaryand the Czech Republic for integration within the SAVE-IT software package to allow theidentification of areas and population groups that may be vulnerable to radiocesium deposition.From this viewpoint the samples of soil and vegetation were collected (1999 and 2000; thelocations of the sampling places are in Fig. 1.) in which the content of 137Cs by semiconductorgamma spectrometry were determined. The mass activity of 137Cs were used for' calculation ofsoil-to-plant transfer factors.
Fig.l: Location of vegetation aisd soil samples collection in the Czech Republic
ar1999
ir 2000
XXIV DRO Demänovská dolina 149SK02K0206

The calculation of soil-to-plant transfer factors was made for two soil layers (0 4- 5 cmand 0 -r 20 cm); the transfer factors were calculated as a ratio of mass activity of 137Cs in dryvegetation (Bq.kg"1) and of mass activity of 137Cs in dry soil (Bq.kg"1).
The soil-to-plant transfer factors were calculated for two soil groups: cultivated oruncultivated soil; in case of cultivated soils samples with grass were used only (the sampleswith straw were not used due to unknown ratio of activity in ear with grain and in the straw).The results are in the tables 1 and 2.
Table 1: The soil-to-plant transfer factors for soil layer 0 -ŕ 5 cm
Vegetation / Soil 0-̂ 5 cm
Uncultivated soilCultivated soil - grass
Number ofvalues
779
Arithmeticmean0,330,24
95% confidence interval
0,010,05
2,40,99
Table 2: The soil-to-plant transfer factors for soil layer 0 -f 20 cm
Vegetation / Soil 0-=-20 cm
Uncultivated soilCultivated soil - grass
Number ofvalues
809
Arithmeticmean0,690,24
95% confidence interval
0,010,05
6,10,95
The software package SAVE-IT incorporate a soil-to-plant transfer model which usesmeasured soil properties to estimate the dynamic behavior of deposited Cs. From this reasonfollowing chemical properties of the soil were determined (soil samples from the year 1999only): pHH2o> pHcaci2, exchangeable tt, cation exchange .capacity (CEC), exchangeable K+,exchangeable Ca2+, exchangeable Mg2+ and content of oxidizable carbon (Cox). Thedetermination was performed by Research Institute of Reclaiming and Protection of the Land,Prague, Prague - Zbraslav.
An attempt was made to find difference among soil-to-plant transfer factors by pHH20.cation exchange capacity (CEC) and content of oxidizable carbon (Cox)- The results are in tables3 and 4.
Table 3: The soil-to-plant transfer factors by chemical properties for soil layer 0 ~ 5 cm
Vegetation / Uncult. soil O-i-5 cm
Altogether
pHn2O
CEC (mmol/lOOg)
Cox (%)
5 * 66^-7
7-5-7,58-ŕ 1515^-2020-ŕ 421,8 -ŕ 2,32,3 -f 3,33,3 -s- 7,2
Number ofvalues
23106741094910
Arithmeticmean0,140,120,120,180,100,150,150,200,120,13
95% confidenceinterval
0,010,0060,0060,0030,0020,0070,0050,01
0,0070,004
0,91,31,74,73,31,62,22,81,11,7
XXIV DRO Demänovská dolina 150

Table 4: The soil-to-plant transfer factors by chemical properties for soil layer 0 -f 20 cm
Vegetation / Uncult. soil 04-20 cm
Altogether
PH„„
(mmoI/lOOg)
v-ox V i°)
5-f664-7
7^-7,58 4-1515 4-2020 4-421,8 4-2,32,3 4- 3,33,3 4- 7,2
Number ofvalues
23105861071076
Arithmeticmean0,180,170,160,200,120,180,220,240,080,18
95% confidenceinterval
0,020,0050,0050,01
0,0070,0050,020,03
0,0050,005
1,12,33,62,41,62,91,91,40,83,7
The soil-to-plant transfer factor calculated for uncultivated soil is highher than forcultivated soil. In case of cultivated soil there is no difference between transfer factor for soillayer 0 -f 5 cm and transfer factor for soil layer 0 -ŕ 20 cm (the soil is mixed for example bytillage). In case of uncultivated soil the difference between transfer factor for soil layers existsbecause the activity of 137Cs in top layer (0 -ŕ 5 cm) is higher.
Differences in soil-to-plant transfer factors by chemical properties of soil were not found(always in 95% confidence interval).
The values of soil-to-plant transfer factors for 137Cs are in a good agreement withprevious publications [1] for example the transfer factor for grass and soil (upper 10 cm, pH =6) the value 0,11 is given with 95% confidence interval 0,011 -r 1,1.
The work was performed in the frame of the EU project SAVEC - Spatial Analysis ofVulnerable Ecosystems in Central Europe (contract number: ERB IC15-CT98-0206).
[1] Handbook of Parameter Values for the Prediction of Radionuclide Transfer in TemperateEnvironments, IAEA, Vienna, 1984.
XXIV DRO Demänovská dolina 151

EFFECTIVE DOSE ESTIMATION FROM THE HP(10) VALUEMEASURED BY FILM OR TL DOSEMETER LOCATED
ABOVE THE LEAD APRON IN MEDICAL DIAGNOSTICAND INTERVENTION RADIOLOGY.
Trousil Jaroslav 1\ Plichta Jiří1*, Petrová Karla 2)
^National Personal Dosimetry Service Ltd., Prague2>State Office for Radiation Safety
In medical institutions where the diagnostic and intervention radiology is examined the staffpersonnel doses reach for a long time the annual limit.
State Ofice for Radiation Safety ordered the research task with a view to:a) the influence of the dosemeter location on different parts of the body on the reliability
of E value estimation by means of the value which is measured on the standard bodylocation - left part of the chest above the lead apron.
b) the influence of the protective lead apron (neck, spectacles) with known lead equivalenton the E and HT value determination.
In this contribution we present the results of this experimental study including therecommendation for the number and location on the body of dosemeters which are needed forthe reliable estimation of E value. In the conclusion the comparison of our results and resultspublished in Radiation Protection Journal is presented.
SK02K0207XXIV DRO Demänovská doli na 152

NEW DEVELOPMENTS OF CZECH PERSONNEL NEUTRONDOSEMETER AND ITS APPLICATION
Trousil Jaroslav^, Spurný František, Králík Miloslav3\
Zelenka Zdeněk4),^National Service of Personal Dosimetry Ltd., Prague; 2)Nuclear Physics Institute,
Czech Academy of Sciences, Prague; 3* Czech Metrological Institute, Prague;Dukovany Nuclear Power Station
IntroductionThere are two systems for neutron personal dosimetry used at practice in the Czech
Republic:• Solid state nuclear track detectors in contact with fissionable materials (intermetalic
enriched U+Al alloy, and 232Th) in Cd shield badge [1], and• Albedo dosimeter based on 6LiF and 7LiF thermoluminescent detectors in a plastic badge
covered from the front side by Cd to screen it from directly coming thermalised neutrons[2].
The first system is used in National Personal Dosimetry Service (CSOD); its performance iscontinuously checked and improved. In this contribution we would like to present some ofresults of this development, the contribution to the calibration of the second system included.
Results and DiscussionBasic Principle of the CSOD Neutron Dosimeter [1]
The dosimeter is composed of the Mylar solid state nuclear track detector, 8u.m thick,placed between two fissionable materials: intermetallic U-Al alloy with U (20 wt %) enriched to90 % in 2 3 5U, and metallic 2 3 2Th. These two radiators are afixed to a 0.5 mm thick Cd filter andthe complete set, i.e. two couples of radiators with the track detector in between them, isinserted in a dosimetric badge. Cd filter serve to absorb thermal neutrons coming or directly oras albedo. After the use, the track detector is chemically etched and evaluated using a sparkcounter. The value of Hp(10) is derived from the apparent value of dose equivalent establishedunder uranium, H(app)uAi, as equal to 0.0687pUai. The value obtained is corrected using a factork which can be found on the base of the ratio of track densities puai /p™ • This ratio is anindicator of the neutron energy. When primary neutron source is known, the value of Hp(10) iscalculated as: Hp(10) = H(app)uAi.-n.k. The value of n depends on the primary source and it isequal to 1.0 for Cf, 0.57 for AmBe, and 0.37 for 14 MeV neutrons. When the primary neutronsource is not known, only the factor k, based on the track densities ratio mentioned is used. Theuncertainty of Hp(10) determination in this case deteriorates, of course. The dependence of k onthe track densities ratio was established experimentally through the evaluation of dosimetersirradiated in more than 50 neutron fields with known spectra determined by means of Bonnerspectrometer. The spectra were chosen in the way to have as large variety of shielding aspossible. When the primary neutron spectrum is known, the uncertainty of the Hp(10) value isestimated to not less than ± 30% ( la) for Hp(10) > 1.25 mSv (declared minimum detectabledose equivalent).
This basic interpretation procedure can not be used when track densities ratio is toohigh, above 260. It occurs in very heavily moderated spectra. In such case only track densityunder U-Al radiator is used. In WWR energetic reactor environment it was found, that theaverage factor is equal to 535 tracks under U-Al corresponds to 1 mSv of Hp(10).
The numbers of tracks evaluated are stored, even when the value of Hp(10) is lower than1.25 mSv. It permits to estimate, at the end of each year, an annual value of Hp(10) based on thetotal numbers of tracks during the whole year.
XXIV DRO Demänovská dolina 153 SK02K020

Performance testingPerformance testing is performed by the calibration realised through the cooperatin with
the Inspectorate for Ionising Radiation of the Czech Metrological Institute (CMI-IIZ). Thisinstitution is authorised to verify the quality assurance of all personal dosimeters in the CzechRepublic. The testing is realised through the irradiation of neutron personal dosimeters todifferent values of Hp(10) by means of 252Cf neutrons. The procedure of testing woulddemonstrate that the essential performance specifications are maintained in the routineindividual dosimetry. The tests are performed with the regular interval of two years.
The last tests have been realised at the beginning of the 2001-year, CSOD neutronpersonal dosimeters were irradiated on the PMMA phantom 30x30x15 cm. The averagedifference of the value of Hp(10) established by means of the CSOD routine procedure was+13% in one case, +15% in other one, when compared to the value determined by CMI-IIZfrom the known neutron emission rate and ICRP 74 conversion factor for 252Cf neutrons, 400pSv.cm2.
We suppose that the difference obtained is related to the fact, that the routine calibrationof CSOD personal dosimeters was related to previous ICRP recommendations not directlyconnected with Hp(10) quantity. We estimated the uncertainty of recalculation of the constant topass from H(app)uAi to Hp(10) to about 10%. We decided therefore to lower the value 0.0687used to calculate Hp(10) from H(app)uAb in 10% (see above). In such way, the differencescomparing to the CMI-IIZ estimation will not exceed 5%.
Using CSOD dosimeter to test an albedo dosimeter applied in Dukovany nuclear power plantThe dosimetry service of Dukovany nuclear power plant (NPP) used for the individual
neutron dosimetry an albedo system based on 6LiF and 7LiF thermoluminescent detectors [3].Recently, it was decided to modify this dosimeter slightly. First, a plastic hemisphere simulating10 mm of the tissue was removed from the badge. Furthermore, 0,8 mm thick Cd-shield wasadded to protect the dosimeter against directly falling thermal neutrons. To verify the behaviorof this modified albedo-dosimeter, we compared them in real neutron fields in-reactor buildingwith CSOD neutron personal dosimeter. Two extreme fields were chosen for such tests:• The board of main circulation pumps, where the spectrum is extremely moderated as found
through the measurements with Bonner spectrometer [4]; and• The room of "bor-meters", where the spectrum of neutrons corresponds to only slightly
moderated AmBe neutrons.Both types of neutron dosimeters were irradiated on a phantom, 4 dosimeters of each type wereirradiated together. Some gamma dosimeters were also irradiated at the same time, the results oftheir evaluation were recently published [2] and will not be discussed in this work.
In both fields mentioned the dosimeters were irradiated 333 hours. First it should bereminded that the signal of TLD's in the albedo system is primarily expressed in terms ofkerma-air of reference photons of 137Cs. The results of evaluation of both neutron personaldosimeters are given in Table 1.
Table 1: The results of evaluation of neutron personal dosimeters irradiated inside NPPDukovany
, >|ettíojj dosimeterCSOD
Albedo, NPP
Hp(10), mSvKair-6LiF = A, mGyKair-'LiF = B, mGy
A-B, mGy
44.7±3.8
16.4±1.91.41 ±0.0615.0+1.9
Kfn^^uláiíÄpíimps14.8±1.2
45.0±1.22.53+0.0542.5±1.2
It has to be mentioned that the evaluation of CSOD-dosimeter proved again thedifference in the hardness of neutron spectra in both fields. While the ratio of track densities puai
XXIV DRO Demänovská dolina 154

/pih in the room of „bor-meters" was about 5.5, close to the main circulation pumps about 260.The values of Hp(10) were therefore in the first case determined by standard procedure withAmBe as primary source, in the second the factor 535 tracks per 1 mSv was used. It should be,however mentioned that the value obtained in the second case through the standard procedure,11.3 mSv, was close to the value given in the Table 1. Supposing that the values obtained withCSOD dosimeter are correct, a conversion factor permitting to interpret the difference of TLDsignals to Hp(10) can be determined. It is equal to (3.0±0.4) in the case of bor-meter room,(0.35+0.03) at the main circulation pump. It means that the conversion factor inside of a NPPcan differ for an albedo system up to one order of magnitude. It should be mentioned in thisconnection that corresponding conversion factor for neutrons of 252Cf source is equal to(4.5±0.5), not too far from the value established in "bor-meters" room.
As mentioned, the determination of Hp(10) by means of CSOD dosimeter is, even in sospectrally different fields as tested, sufficiently correct, the requirement to be inside (-33 to+50%) [5] would be fulfilled. The use of an albedo dosimeter represents more complicated task.Two solutions are possible:1. Dosimetry service ensures the information in what area the person worked during the period
of dosimeter use, or2. The interpretation starts with more safe hypothesis, i.e. the difference of TLD signals is
multiplied by the highest conversion factor possible. If the value obtained is higher thansome properly chosen limit, the information mentioned in the item 1) has to be ensured.
Technical improvementsAs mentioned in the first chapter, CSOD dosimeter is after the etching evaluated by
means of a spark counter. At usual conditions, the maximum number of tracks countable on theevaluated area 2.5 cm2 was estimated to be about 3000 [1]. It limits of its use to mostlyoccupational type of exposure (Hp(10) below few 100 mSv), occasional accidental exposureswould be difficult to evaluate properly. Recently, the spark counter has been modified from thisreason to extend the linearity of the response to 10000 and/or more numbers of tracks per 2.5cm area of the electrode. We decide to verify to what extent the linearity of the response wasenlarged.
Routine neutron personal dosimeters were irradiated by means of a 239PuBeneutron source available at the Nuclear Research Center of Fontenay-aux-Roses, France. Itsemission rate is 2.12xlO7 s ' \ diameter 3.95 cm and the height 8.6 cm. The source waspositioned at the center of a room 5x5x3.5 m3, at the height of 1.35 m.
The dosimeters were irradiated at the distances from 15 to 40 cm. Due to rather largesource dimensions, the corrections for non-punctuality were estimated following the proceduredescribed in [6]. They were equal to - 8 % at the distance of 15 cm, -4% at the distance of 25 cm,less than 0.5% at the distance of 40cm.
A set of three routine neutron personal dosimeters was irradiated at each distancementioned, with the values of Hp(10) from about 100 up to 600 mSv. The dosimeters weretreated in such a way that the corrections for spontaneous fission were negligible. The results oftheir evaluation by means of the modified spark counter are presented in the Table 2. Theroutine spark counting includes pre-sparking at 1000 V and repeated sparking at 600 V.
Table 2: Results of the evaluation of dosimeters exposed at a 239PuBe neutron source
Exposure
No.1 (40 cm)2 (25 cm)3 (15 cm)
Number of tracks per electrode area of2.5 cm2 under
Th-NTh
1557 ± 63*>3902 ± 3809944 ± 553
UA1 alloy-Nu2045 ± 783610 ±38
7401 ±213
NTh/H
16.2 ± 0.716.9 ±1.616.5 ±0.9
Nu/H
mSv'1
21.3 ±0.815.6 ±0.212.3 ±0.4
XXIV DRO Demänovská dolina 155

The detectors were irradiated in the free-in-air irradiation geometry. In spite of that, lowenergy neutrons scattered from the room walls influence the reading of detectors with UAl-alloyradiator. The larger is distance from the source, the higher is contribution of these neutrons tothe number of tracks under UAl-alloy and the higher is therefore number of tracks per 1 mSv.One can see in the Table 2 that this is actually the case.
Largely more important is therefore the analysis of data obtained for the number oftracks behind Th-radiator. One can see in the Table 2 that an excellent linearity is observed fortrack numbers between 1500 and 10000. Besides, also absolute values are in quite goodagreement with expectation. Actually, the number of tracks counted behind Th per 1 mSvduring regular calibration by means of 252Cf neutrons is about 8.5 mSv"1 [1]. When the ratio offission cross sections is taken into account [7] it should be between 14 and 20 mSv"1, dependingon the spectra taken into account. Some preliminary tests with an AmBe neutron source in theCSOD irradiation hall have given the value (13.9 ± 0.7) mSv"1.
The tests performed confirmed therefore that the modifications realised would permit toextend substantially the range of the linearity of counting up to, at least, 10000 tracks perelectrode area of 2.5 cm2. The limit of dose equivalent measurable would be therefore at least600 mSv for a Pu(Am)Be neutrons, about 1.4 Sv for 252Cf neutrons, up to 5-10 Sv atexperimental reactors, and up to ten times more than the last figures inside nuclear powerstations with a PWR reactor.
When an average quality factor about 10 would be supposed, the absorbed dose up toabout 1 Gy could be measurable with detectors exposed at experimental reactors. It is close tothe accidental conditions, such possibility should and will be tested during an intercomparisonof such types of dosimeters. Nevertheless, it should be recommended first to repeat the tests ofthe type described in this report for still larger extent of expected numbers of tracks, up to, atleast, 20-30000.
REFERENCES1. J. Trousil, et al.: "Basic Dosimetric Characteristics of the Czechoslovak
Thermoluminescent and Neutron Dosemeter". Kernenergie 27, (1984), p. 246-254.2. J. Trousil et al.:"K využití albedo dozimetrů v JE Dukovany", Bezpečnost Jaderné Energie
9(47), (2001), 247-250.3. P. Čárný a kol.: „Zdokonalenie osobnej dozimetrie na JE časť II - neutronová dozimetria."
Zpráva VUJE č. 227/92.4. P. Šujak, P. Čárný, Z. Prouza, J. Heřmanská: „Energy spectra of Stray Neutron Fields at
PWR Nuclear Power Plants." Radiat. Prot. Dosim. JJL_(1987), No. 3.5. „General Principles for the Radiation Protection of Workers. ICRP Publication 75,
Pergamon Press, 1997.6. N.T. Gusev, J.E. Kovalev, D.P. Osanov, V.I. Popov: "Zashchita ot izlucheniya
protjazhennych istochnikov". Gosatomizdat, Moscow 1961, p. 51.7. "Compendium of Neutron Spectra and Detector Responses for radiation protection
Purposes." eds.: R. V. Griffith, J. Pálfalvi, U. Madhvanath; IAEA Techn. Rep. Series No.318, IAEA, Vienna 1990.
XXIV DRO Demänovská dolina 156

STATE METROLOGICAL CENTRE
Magdaléna VičanováInstitute of Preventive and Clinical Medicine
Limbová 14, 833 01 Bratislava, Slovakia
Introduction
The Slovak radon program started in 1990 and was organised by the Institute ofPreventive and Clinical Medicine. The uniform calibration and comparison of differentmeasurements were necessary to indemnify for measurements of radon and its daughterproducts. The calibration methods were taken over and developed, and radon calibrationchamber were built too. This system is the basis of secondary radon standard, which wasauthorised in 1992 and consist of two measuring systems:
- radon chamber for measurement of radon and its daughter products.- system IIC for measurement of radon (222Rn) and thoron ( 2 0 Rn).Both calibration systems, together with the estimate of the relative combined standard
uncertainties for estimation of radon and its daughter products concentrations and internationalcomparison of our measuring systems are presented in this paper.
Description ofI PCM Radon Standard Facilities
Radon ChamberThe radon chamber is used for calibration and verification of the radon meters and the
radon daughters meters, for measurement of diffusion coefficient of the materials, exposure ofanimals and consist of the following main components (see figure l) i l ] :- steel chamber with volume of 1.26 m3;- radon and daughters monitoring devices;- radon sources with activities of 226Ra from 2 to 400 kBq in solution or in dry sources;- aerosol system is not completed yet and for aerosol conditions there are used manual injection
of cigarette smoke into the chamber, the range of equilibrium factor is from 0.2 to 0.85;- ventilation and climatisation manual control system with temperature about 22 °C,
atmospheric pressure, relative humidity ranges from 20 to 95 % and ventilation rate up to0.007 s"1;
- climatic parameters monitoring and data acquisition systems.
System IICThe standard system IIC is used for calibration and verification of radon and thoron
meters and measuring techniques. The system consists of three basic parts (see figure 2)m:- filling part consists of radon and thoron generators, radon tank with volume of 40 L and
working gas supply (argon or nitrogen), working pressure ranges from 500 to 2000 hPa;- measuring part is cylindrical ionisation chamber with volume of 4 L. The ionisation chamber
works in stationary and in flow modes. The resolution for radon alpha particles (5.5 MeV) is180 keV and efficiency for stationary mode for radon gas is 63 %;
- sampling part consists of sampling station for filling external detectors and of experimentalcylindrical stainless steel chamber with volume of 10 L for exposure of passive detectors.
SK02K0209
XXIV DRO Demänovská dolina 157

sampling part consists of sampling station for filling external detectors and of experimentalcylindrical stainless steel chamber with volume of 10 L for exposure of passive detectors.
Humidify Radon
Generator Source
Ventilation
System Aerosol
Generator
Radon andRn DaughtersMeters
Spectrometer
Fig. 1 Schematic diagram of the radon chamber
-i SamplingStation
PressureGauge
Fig. 2 Schematic diagram of the IIC radon standard system
XXIV DRO Demänovská dolina 158

Radon and Radon Daughters Measuring Methods
The radon gas concentration measurement system in the radon chamber is based onsampling and cauting of scintillation cells with volume of 160 and 1000 ml. Radonconcentrations during the long-term exposure in the chamber are observed by continuous radonmonitor with a scintillation cell of 1000 ml. The efficiency of 160 and 1000 ml scintillation cellsis 65 % and 55% respectively11-1.
The radon daughter and equilibrium equivalent radon concentrations (EER) in the radonchamber are determined by spectrometric monitor Silená 4S placed outside of the chamber andsampling through a tube with flow rate of 3.5 L/min and counter efficiency of 28 %. Secondmethod for determination of EER and radon daughters concentrations in chamber air issampling a filter with flow rate of 13 L/min, with counter efficiency of 25.6 % and counted andcalculated by Thomas method'31. In the both methods are used membrane filter Millipore typeA A with 0.8 jim pore diameter.
The relative uncertainty for determination of radon and its daughters concentrations are inthe table 1.
Table 1 Assessed uncertainty in the measurement of radon concentrations and forEER concentrations of 100 Bq.m'1
Relative uncertainty
Type A (uA)-(standard error)for repeated measurement
Type B (uB):Counting statisticsCalibration coefficientVolume of detectorVolume of flow airTotal type B
Combined standard uncertainty for68% confidence interval(uc
2 = uA2+uB
2)
Radon
Scintillation Ionisationcells chamberUx[%] ux[%]
1.5
32.12
4.2
4.5
-
121
2.5
2.5
EER
Silená 4Sux [%]
-
102
411.0
11.0
Thomasmethodux[%]
-
125
213.2
13.2
Intercomparison Measurements
The results from three intercomparison and calibration measurements of the IPCMsecondary radon and radon daughter measuring system in National Radiation Protection Board(NRPB) in England and one intercomparison of radon daughter meter in VNIIFTRI in Moscoware summarised in the table 2.
XXIV DRO Demänovská dolina 159

Table 2 Intercomparison results
Year (Place)
1992(VNIIFTRI)1994 (NRPB)1995 (NRPB)1995 (UHP)1996 (NRPB)1997 (EMI Praha)
1997 (UHP)
Monitor
1.02 ±1.13 ±1.04 ±
1.02 ±-
Silená
0.200.090.07
0.08
Ratio LABS/IPCM
EER
Thomas method
_-
0.98 ±0.09
1.02 ±0.08-
1.05 ±0.02
Radon
Scintillation celts
_0.96 ± 0.030.98 ± 0.021.01 ±0.071.01 ±0.020.95 ±0.06
0.97 ±0.03*0.91 ±0.03
*for Ionisation chamber
Fig. 3 Photo of the radon chamber
[1] F. Havlík, M. Ďurčík and D. Nikodémova: The Safety of Nuclear Energy, 1993, 1(39),No. 3, pp. 107-111.
[2] M. Ďurčík, F. Havlik and D. Nikodémova: The Safety of NuclearEnergy, 1993, 1(39), No. 4, pp. 133-136.
[3] J.W. Thomas: Health Physics, 1972, Vol. 23, pp.783-789.
XXIV DRO Demänovská dolina 160

DETERMINATION OF 210PB IN WATER SAMPLES BY LIQUIDSCINTILATION SPECTROMETRY
Marta Vršková, Katarína SedláčkováWater Research Institute, Department of Radiochemistry, Nábr. L. Svobodu 5, 812 49 Bratislava
AbstractIn this study the method for determination of naturally occurring radionuclide Pb2 + in watersamples is proposed. The method has been developed taking into account the main requirementsof the environmental monitoring activities. The separation of Pb2 + radionuclide from the complexsample matrices was performed using different types of ion exchangers to compare their abilityto remove Pb2 + ions from water solution. Moreover, Pb2 + uptake was found to be markedlyinfluenced by solution pH. The samples were counted after pre-concentration on liquidscintillation spectrometer Tri-Carb® 2900TR fa Packard. The comparison of three types ofscintillators was performed.
Introduction
The toxic nature of many metals, even at trace level, has been a public health problemfor many years. Their presence in aqueous solution has been of great concern in termsof environmental protection. From the ecotoxicological viewpoint the most dangerousmetals are mercury, cadmium and lead.210Pb is one of the most toxic natural radioisotopes. According to the ICRP recommendationsthe annual limit of intake (ALI) of 2 I 0Pb is 2.104 Bq, while ALI for 2 2 6Ra is 3,5 times higher -7.10 4Bq[l].210Pb is a member of 2 3 8 U series - a daughter product of the last isotope of so-called short livingradon daughters - 2 1 4Po (T1/2 = 1.64.10"4 s). 2 1 0Pb emits Pand y-radiation, a decay scheme of2 l 0Pb is shown in Tab. 1 [1, 2]. The immediate 2 I 0Pb decay product 210Bi is also a beta emitter,however it emits beta particles of much higher energy (EP m a x =1160 keV). The followingdaughter isotope 2 1 0Po emits alpha particles with the energy E a = 5,503 MeV.
Tab. 1 Decay scheme of 2 1 0Pb.
Radionuclide
2 1 0 P b
2 1 0 B i2 1 0 P o
Half time Tm
22,3 y
5,0 d
138,4 d
Type of radiation
P
y
Pa
Energy
E p m a x =17keV(85%)
E p m a x =61keV(15%)
E r =46,5keV(5%)
E p m a x =1160keV(100%)
E a = 5,503 MeV (100%)
The main source of 2 1 0Pb in the environment is the gaseous 222Rn, which escapes from the earthcrust into the atmosphere and the daughter products of 2 2 2Rn decay which fall out with aerosolparticles.
I0Pb enriched in the human body through the food chain remains in the skeleton long enough toproduce the highest skeletal dose of any natural radionuclide under conditions of averagebackground exposure. On the other hand, the short life of 2 1 0Po relative to that of 2 ! 0Pb, as wellas its short biological half-life of 50 days [1], makes 2 1 0Pb in the body the most important sourceof high energetic 2 1 0Po under normal conditions.
SK02K0210XXIV DRO Demänovská dolina 161

The total 2 1 0Pb activity can be determined by direct gamma radiation counting (46.5 keV), bybeta counting of daughter 210Bi or by measuring the alpha emission of its granddaughter 2 1 0Po[2J.Liquid scintillation technique is rarely used for determination of environmental 2 1 0Pb because oflow environmental 2 1 0Pb activities. This problem can be solved by means of low-backgroundliquid scintilation spectrometer and appropriate radiochemical sample preparation (pre-concentration, suitable scintillation cocktail, etc.).
ExperimentalSample preparationConsidering the determination level of the method, an appropriate initial volume of sample mustbe chosen depending on the expected 2 I 0Pb concentration in the analysed water sample.According to the NCRP 77 [1] the ranges of 2 1 0Pb concentration in different types of waterswith not elevated 2 1 0Pb content are given in Tab. 2.
Tab. 2 210Pb content in different types of water.
Water
Precipitationtapraw(drinking water supplies)
Activity
0,11 Bq/10,0007 Bq/10,005 Bq/1
Required sample(minimum)
0,18128,01
4,01
The upper limits for 2 1 0Pb and 2 1 0Po concentrations in water supplies are specified in „VyhláškaMZ SR č. 12/2001 Zb.z. O požiadavkách na zabezpečenie radiačnej ochrany" (Tab. 3). Thecommon concentrations are, however, mostly much lower.
Tab. 3 The upper limits for radionuclides content in water supplies.
Radionuclide
210pb
210po
Concentration in babywater
[Bq.l1]
0,10,1
Concentration innatural mineral tablewater and other table
water[Bq.ť]
0,80,5
Concentration indrinking and tap water
[Bq.ť]
0,30,2
In our laboratory, the distilled water of 2 1 of volume with addition of following solutions waspocessed:
• 0.5 ml of standard 210Pb solution (of 2 1 0Pb activity of 6.67 Bq/0.5 ml)• 0.2 ml of carrier Pb(NO3)2 (Pb concentration 4 mg/21)• 40 ml of HNO3 (1:1) (to adjust the pH to 2), respectively 40 ml of acetate puffer (pH =
5.5)The separation of Pb was carried out on different types of ion-exchangers (Tab. 4) to comparetheir ability to remove Pb2+ ions from the complex sample matrices. Prepared solutions werepassed through an ion-exchanger loaded column. Lead was eluted after washing the columnwith25mlof3MHNO 3 .
XXIV DRO Demänovská dolina 162

Measurement
The samples were counted after pre-concentration on liquid scintillation spectrometer PackardTri-Carb 2900TR. The comparison of three types of scintillators was performed.Tab. 4 Investigated ion exchangers.
Trade name
AmberIitIR-122
Dowex 50X1-100
OXIN
SAL
THIOL
CEL DETA
Description
Strongly acidic cation exchanger onpolystyrene, ionic form Na+
Strongly acidic cation exchange resin onpolystyrene, ionic form ITOrganic sorbent based onhydroxyetylmetacrylate HEM A, SPHERONgel + 8-hydrochinoline, ion-selectiveexchanger for heavy metalsOrganic sorbent based on HEMA,SPHERON gel + salicylic acidOrganic sorbent based on HEMA,SPHERON gel + thiol -SHOrganic sorbent based on polystyreneand spherical cellulose,OSTSORB gel + dietylentriamine,selective sorbent for heavy metal ions
Exchangecapacity
2,1 meq/ml
1,8 meq/ml
0,3 mmol/g
0,3 mmol/g
0.5 mmol/g
1,0 mmol/g
Results
Following types of scintillator were compared:1. Instagel
Multipurpose, holds up to 50% water, homogenous redistribution of countedmedium thanks to the gel phase, high efficiency, low background
2. Ultima Gold LLTFor environmental sample counting, accepts up to 54% water, high counting
efficiency, very low background levels3. Optifluor
For safety and simplicity, universal, multipurpose
The comparison of the scintillators used is depicted in Fig. 2.
2000
1600
Calibration curve
1200 -
DLO
800 -
400 -
«Instage!
H Ultima Gold
AOeiiftuor * , - ,4 -,
10 15 20 25
concentration [Bq/IOml]
Fig. 2 Comparison of different scintillation cocktails.
XXIV DRO Demänovská dolina 163

From Fig. 2 it is evident that scintillation cocktail Instagel shows the best properties in 210Pbdetermination. Based on this result, for further investigation Instagel was used.
• 'Áfeha - ; JÔÔ i:{1000 0 , f{4 ,5 • -.;,
.J?rft.i,
••• ' • .4Ó' ,80 „.-,80. • .lO'O" ..120": V140'-" :160, .180; - .200
Fig. 3 Typical spectrum of Pb standard solution.
Tab. 5 compares the yields reached for investigated ion-exchangers. It is evident, that the Pb +
uptake was found to be strongly dependent on the type of ion exchanger and markedlyinfluenced by the sample pH and exchanger volume/weight either.
Tab . 5 Yields reached for used ion-exchangers.
Ion-exchanger
Amberlit
Dowex
DetaOxin
ThiolSal
Weight/Volume
3 ml3 ml3ml3ml1 ml
500 mg500 mg250 mg500 mg250 mg
pH
25.52
5.522
5.55.52
5.5
Yield [%]
51.924.913.398.54.1< !)
100.435.4<97.1
under detection limit
Conclusion
The preliminary results provide relevant information and highlight the necessity for furtherinvestigation into this problem. To analyse the environmental samples and thus verify theproposed method will be of our interest.
XXIV DRO Demänovská dolina 164

References[1] Lebečka, J. - Chalupnik, S.: Method of Determination on 2 I 0Pb by Liquid ScintillationTechnique, Rare Nuclear Processes, 14th Europhysics Conference on Nuclear Physics,Bratislava, 1990[2] The Investigation and the Developments of Methods for the Determination 2 1 0Pb in Water,unpublished
XXIV DRO Demänovská dolina 165

COLLECTIVE AND INDIVIDUAL EFFECTIVE DOSES INDUKOVANY NPP DURING 1996-2000
Zdeněk ZelenkaČEZ a.s. - Jaderná elektrárna Dukovany
Cílem příspěvku je analýza kolektivních a individuálních effektivních dávek KED v Jadernéelektrárně Dukovany za období 1996 - 2000.
Příspěvek ukazuje:• podíl čerpané KED při odstávkách na celkové roční KED (80 - 90 %)• vliv délky odstávky a plánovaných činností na KED při odstávce• podíl čerpané KED pro vybraná zařízení a činnosti• distribuce individuálních osobních dávek
Od roku 1993 se daří snižovat roční kolektivní efektivní dávku KED na lokalitě JE Dukovany (vr. 1993 KED = 1,44 Sv, v r. 2000 KED = 0,99 Sv). K tomu zejména přispívá:
• postupné snižování počtu sledovaných pracovníků v kontrolovaném pásmu (v r. 1993 -2574 pracovníků, v r. 2000 - 2161 pracovníků)
• zkracování doby trvání odstávky (o cca 10 dní na odstávku)• mnohaleté zkušenosti pracovníků, provádějících práce v KP• neustálé zdokonalování řízení prací vKP včetně využití plánování čerpání KED po
měsících• zavedení systému elektronické osobní dozimetrie pro operativní osobní dozimetrii (od r.
1997 pro vybrané radiačně exponované pracovníky, od r. 2000 pro všechny)
Distribuce BED potvrzuje, že i při zvyšování objemu prací při odstávkách v důsledku obnovy amodernizace zařízení a zároveň při nižším počtu sledovaných pracovníků zůstává procentopracovníků, čerpajících dávky v jednotlivých intervalech'na stejné úrovni:0 -1 mSv 87 % pracovníků1 - 5 mSv 11 % pracovníků5 a více mSv 2 % pracovníků
SK02K0211
XXIV DRO Demänovská dolina 166

QUALITY AUDITS OF THE REMOTE-CONTROLLEDAUTOMATICALLY-DRIVEN GAMMA RAY AFTERLOADING
EQUIPMENT USED IN BRACHYTHERAPY IN THE CZECHREPUBLIC
Helena Žáčkova, Ivana HorákováNational Radiation Protection Institute (NRPI)Šrobárova 48, 100 00 Prague, Czech Republic
INRODUCTIONTo reach safety and precise application of ionisation radiation to patients Atomic act
declares, in its Article no.7, requirements for medical exposure. There are also given - amongothers - the demands to "install the quality assurance programmes (QA) for medical actions andfunctions".
Since 1997, when the act has been adopted, a set of five Recommendations of StateOffice for Nuclear Safety (SONS ) for radiotherapy has been prepared to instruct users how toprepare quality control system (i.e. system of tests required by of the regulation no. 184/1997 Sb.- acceptance, status and constancy tests) for main types of sources used in radiotherapy fortreatment of the patients. Among them also the Recommendation on QA in brachytherapy hasbeen issued by SONS in 1998.
National Radiation Protection Institute (NRPI) has been performing the regular in situquality audits in which the chosen parameters (which could seriously influence the dose to thepatients - i.e. absorbed dose, main geometrical and radiation parameters etc ) are independentlychecked by the NRPI experts. System of Quality Audits on the sources used in teletherapy hasbeen introduced in 1997 and at present time they are smoothly carried out according theSONS's demands. This work describes the process of installing of the Quality Audit system onbrachytherapy.
MATERIALS AND METHODSThere are 32 radiotherapeutical departments in the Czech Republic and in 19 of them
brachytherapy treatment is carried out (besides teletherapy). Only in two departments oldfashion type of source application - manual afterloading - is used. The rest of RT departments(17) use the remote controlled afterloading equipment. There are two main types of the remotecontrolled automatically driven afterloading (AFL) equipment used in CR: the types for highdose rate (HDR) treatment (using usually Ir-192) and the types for low dose rate (LDR)treatment (with Cs-137). Up to now there are 11 HDR and 6 LDR installations in CR.
The type, acceptance and status tests can be performed - according Atomic actrequirements - only by persons who are licensed by SONS. Up to now there are five personslicensed by SONS to perform acceptance or status tests for some of the types of these AFLinstallations.
The list of tests, for which the methods should be worked out in the documentation bythe person, who applies for license to perform authorised tests of AFL equipment are presentedin Table 1. There is indicated by T - the type test, by P- acceptance test and by D - status test.There is also given, for each parameter, the reference on the relevant document, which requiresthe check or verification of the parameter (number of the article in standards ČSN EN andnumber of chapter in Recommendation of SONS). At the third column there is also indicatedthe reference number of the chapter in the Method NRPI 43-01.30 (which is a part of QAprogram of NRPI). There - in the Method NRPI - could be found the detailed information on themethods of single checks and verifications together with tolerances, evaluation anddocumentation.
SK02K0212XXIV DRO Demänovská dolina 167

The documentation which was completed only on September of this year is rather hugebecause it adapts and elaborates all relevant requirements of the standards ČSN EN (they havebeen adapting from European standards since 1997) as well as requirements given by theRecommendation on QA in brachytherapy issued by SONS. For absorbed dose estimation theguideline of IAEA-TECDOC-1079 : Calibration of brachytherapy sources has been adopted.Contrary to other persons who are authorised by.SONS to perform acceptance and /or statustests required by legislation (and who are usually focused only on one or a few types of sources)NRPI should be able to perform test of all the types of sources used in Czech Republic.
Table 1:
CHECK / VERIFICATIONType ofthe test
Chapter,inMethodsof NRPI
Article oftheČSN EN601-2-17
Chapterin Recom.of SONS
Safety parameters :
Verification of the marking outside ofequipmentVerification of the marking of the controlsVerification of the indicator lights and pushbuttonsVerification of the accompanyingdocumentsCheck of the leakage of radiation fromstorage containersCheck of the position of SRS in the selectedpositionCheck of the possibility of the key control topre-set the controlling timer and movementof SRSCheck of the treatment timeCheck of the indications by controlling timerand of treatment timeCheck of selection and confirmation ofchannels, SRS, and positions andmovements of SRSCheck of the initiation, continuation,interruption and termination of irradiationCheck of the distant interruptionCheck of the rendering of inoperative of thetreatment control panelCheck of the protection of SRSCheck of the protection against failure of thesupply mainsCheck of the protection against failure ofcontrolling timerCheck of the protection against failure ofpositional accuracy and movement of theSRS and of source drive mechanismCheck of the protection against failure of thecouplings of channels and source applicators
T,P
T,PT,P
T,P
T,P,D
T,P,D
T,P,D
T,P,D,AT,P,D
T.P.D
T,P,D
T,P,DT,P,D
T,P,DT,P,D
T,P,D
T,P,D
T.P.D,
2.1.1.
2.1.2.2.1.3.
2.1.4.
2.2.1
2.2.2
2.2.3
2.2.42.2.5
2.2.6.
2.2.7.
2.2.8.2.3.1.
2.3.2.2.4.1.
2.4.2.
2.4.3.
2.4.4.
6.1.
6.3. ľ*6.7.
6.8.
30.1.1.
30.1.2.
30.1.3
30.1-.4.30.1.5
30.1.6.
30.1.7
30.1.830.2.1
30.2.2.30.3.1.
30.3.2
30.3.3.
30.3.4.
~
3.8.3—
2.1,2.2,3.1,3.23.2.1
3.8.3.
3.8.6.3.8.6.
—
3.9.—
—3.8.3.
3.8.6.
3.5., 3.8.3
XXIV DRO Demänovská dolina 168

Check of the protection against failure ofconnections to the SRSCheck of the protection against failure ofinterlocksCheck of the indication of single faultconditionsCheck of the information on gammairradiationCheck of the scales and unitsCheck of the indication of selection ofchannels, SRS, and positions andmovements of SRSCheck of the information required forlimiting the irradiation during transit ofthe SRSCheck of the position of SRS withinsource applicatorCheck of the controlling timers
T,P,D
T.P.D
T.P.D,
T.P.D
T,P,T,P,D
T,P,D,A
T,P,D,A
T,P,D
2.4.5.
2.4.6.
2.4.7.
2.5.1
2.5.22.5.3
2.5.4.
2.5.5.
2.5.6.
30.3.5.
30.3.6
30.3..7
50.1.1.
50.1.2.50.1.3
50.1.4,
50.2:1.
50.2.2.
~
3.9.
3.8.3.
—
__
3.1,3.6.
3.8.6
Treatment planning system
Check of the hardware and software
supplied
Check of the mathematical models
Check of the treatment plan
T,P
T.P.D
T,P,D
2.6.1.
2.6.2.
2.6.3.
4. /**
7., 8., 9./#*
10. /**
5.
5.1., 5.2,5.3., 5.4,—
Functional characteristics
Check of SRS identificationCheck of SRS certification
Check of SRS documentation, monitoring ofthe movement of SRS and of the disposal ofthe SRSCheck of accompanying documentsCheck of the applicators
Check of the containers
Check of the coupling and transit channels
Check of the connection of SRSCheck of the coupling connectorsCheck of the dummy sources
Check of the source drive mechanismCheck of the treatment control panel
Check of the safety interlocks
P,DP,D
P,D
P,DP,D
P,D
P,D
P,DP,DP,D
P,DP,D
P,D
3.1.13.1.2
3.1.6
3.2.13.2.2
3.2.3
3.2.4
3.2.53.2.63.2.7
3.2.8.3.2.9.
3.2.10
—
2.1.430.3.3.50.2.1.6.8.3.a), b)30.1.1.,30.1.2.a)30.3.3.,30.3.4.30.3.5.30.3.4.—
30.3.3.in 30.1.,30.2. ,30.3.30.3.6.30.3.7.
2.12.2
2.6
3.3.1., 2.5
3.2.,3.2.1,2.5
3.3, 2.5
3.4, 2.53.53.6
3.73.8
3.9
XXIV DRO Demänovská dolina 169

Check of the localisation jig
Check of the localisation chainCheck of the localisation X-ray devices
Check of the mathematical models
Check of the databases used in the treatmentplanning in brachytherapyCheck of the reconstruction model
Check of the dose calculation
Dosimetrical parameters
oshnetry verification of air kerma rate ofSRS
Verification of active length and uniformityof SRSCheck of the unwanted radiationCheck of the containers
P A
PAP,D
PAAP,D
PAA
P,D
PAA
P,D
P,DP,D
3.3.1
3.3.23.3.3
3.4.1
3.4.2.
3.4.3
3.4.4
3.1.3
3.1.4
3.1.53.2.3
——
4. /** •
7., 8., 9./##7., 8., 9. •/**
7.,8.,9.,10/**
IAEA-TECDOC1079—
—--
4.1
4.24.3
5.1
5.2
5.3
5.4
2.3
2.4
2.53.2.
Notes: SRS - sealed radioactive source* in the standard ČSN EN 60601-1** in the standard ČSN EN 62083
In the Table 1. there have been marked the parameters appointed as the most importantfor influence of the absorbed dose to patient during the brachytherapy and therefore they shouldbe audited by independent person. For measurement of the chosen parameters the Method NRPI43-01.30 (authorised by SONS as a part of QA program of NRPI - 43-01-0 with registrationnumber SONS 11273/4.1/ 2000/Ky) will be used. At present time the measuring equipment hasbeen completed at NRPI and the described methods have been tested in the frame work ofinstitutional investigation. The first audits will be carried out in near future with the aim toperform audits of all AFL installation in the Czech Republic.
CONCLUSIONS:
The work described here forms the only part of the activities, which have been carryingout by the department of dosimetry gamma and X-rays of NRPI to support supervisions ofSONS in the field of radiation protection in radiotherapy. Quality audits in brachytherapy willextend the possibilities of NRPI. The Methods NRPI 43-01.30 prepared by NRPI could be usedas documentation for all types of test which are at present time required by Czech legislation forthe remote-controlled automatically-driven gamma-ray afterloading equipment's used inbrachytherapy.
REFFERENCES:1. ČSN EN 60601-1 : Zdravotnické elektrické přístroje Část 1: Všeobecné požadavky a
bezpečnost *(Cor.l) 8.97, *(A1,A11,A12/Cor.l) 8.97, *(A1,A11,A12/Cor.2) 8.97tiskové opravy *(A1+A11+A12) 12.94, *(A13) 7.97, *(A2) 8.97 tiskové změny
2. ČSN EN 60601-1-1 + změna 1 : Zdravotnické elektrické přístroje Část 1: Všeobecnépožadavky na bezpečnost 1.skupinová norma: Požadavky na bezpečnost zdravotnickýchelektrických systémů +(A1 7.97) tisková změna
XXIV DRO Demänovská dolina 170

3. ČSN EN 60601-2-17+Al : Zdravotnické elektrické přístroje Část 2: Zvláštní požadavkyna bezpečnost dálkově řízených automatických přístrojů pro afterloading se zařízenímgama
4. CSN EN 62083: Zdravotnické elektrické přístroje - Požadavky na bezpečnost systémůpro plánování rádioterapeutické léčby
5. Doporučení SÚJB - Zavedení systému jakosti při využívání významných zdrojůionizujícího záření v rádioterapii: Uzavřené radionuklidové zářiče v brachyterapii, 1998
6. IAEA-TECDOC-1079: „Calibration Of Brachytherapy Source", ffiAE, VIENNA, 19997. AAPM (American Association of Physicists in Medicine): Code of practice for
brachytherapy physics: Report of the AAPM Radiation Therapy Committee TaskGroup No. 56. Med. Phys. 24, 1157-1598, October 1997
XXIV DRO Demänovská dolina 171









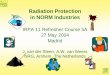

![IRPA guidance on implementation of eye dose …33FC6658-43C3-4DB4-B062...01 mai 2016 [Édition 1, volume 1] INTERNATIONAL RADIATION PROTECTION ASSOCIATION 4 IRPA GUIDANCE ON IMPLEMENTATION](https://img.pdfslide.us/doc/110x75/5ecd80276feee40e4273d82d/irpa-guidance-on-implementation-of-eye-dose-33fc6658-43c3-4db4-b062-01-mai-2016.jpg)