Embed Size (px)
DESCRIPTION
aa
Citation preview

C H A P T E R
99Inherited Porphyrias
R J Desnick and Manisha Balwani
Department of Genetics and Genomic Sciences, Mount Sinai School of Medicine of New York University, New York, NY, USA
Karl E Anderson
Departments of Preventive Medicine and Community Health (Division of Human Nutrition), Internal Medicine (Division of Gastroenterology) and Pharmacology and Toxicology,
University of Texas Medical Branch/UTMB HealthGalveston, TX, USA
This article is a revision of the previous edition article by Robert J Desnick, Kenneth H Astrin and Karl E Anderson, volume 3, pp 2331–2358, © 2007, Elsevier Ltd.
© 2013, Elsevier Ltd
99.1 INTRODUCTION
The inherited porphyrias are a diverse group of inborn errors of metabolism, with each resulting from the defi-cient activity of a specific enzyme in the heme biosynthetic pathway (Tables 99-1 and 99-2). The resultant accumu-lation of porphyrin precursors and/or porphyrins causes the major clinical manifestations, neurologic symptoms, and/or cutaneous photosensitivity. These seven disorders are classified metabolically as hepatic or erythropoietic, depending on the primary source of their accumulated heme biosynthetic intermediates. They also are classi-fied clinically as acute or cutaneous. Of the five hepatic porphyrias, four are characterized by life-threatening acute attacks of neurologic manifestations that occur in association with excess amounts of the porphyrin pre-cursors, 5-aminolevulinic acid (ALA), and porphobilino-gen (PBG), and they are classified as acute porphyrias. Three porphyrias have primarily cutaneous manifesta-tions, including the two erythropoietic porphyrias and porphyria cutanea tarda (PCT). Two other hepatic por-phyrias, hereditary coproporphyria (HCP) and variegate porphyria (VP), may cause acute neurologic attacks and cutaneous manifestations. The skin damage results from photoactivation of the accumulated porphyrins by long-wave ultraviolet (UV) light.
From a genetic point of view, the porphyrias are unique as five of the seven disorders are autosomal domi-nant enzymopathies. Of note, only a minority of hetero-zygotes becomes symptomatic. The onset and severity of the hepatic porphyrias are greatly influenced by environ-mental and metabolic factors, such as hormones, drugs, and nutrition. In addition, modifying genes presumably play an important role in the clinical expression of these disorders.
. All rights reserved. 1
Here, we describe the clinical, metabolic, and genetic features of the seven porphyrias; mutations in the first enzyme in the heme biosynthetic pathway cause X-linked sideroblastic anemia (1). Optimal methods for their diag-nosis and treatment are presented, and the current under-standing of the genetic basis and disease pathogenesis in these acute and cutaneous disorders are discussed. Recent reviews on the inherited porphyrias are available (1–5). For lists of mutations causing each porphyria, please see the Human Gene Mutation Database (www.hgmd.org) (6). Informative and up-to-date Web sites are sponsored by the American Porphyria Foundation (www.porphyri-afoundation.com) and the European Porphyria Initiative (www.porphyria-europe.org).
99.2 THE HEME BIOSYNTHETIC PATHWAY
99.2.1 The Heme Biosynthetic Enzymes
The heme biosynthetic pathway is shown in Figure 99-1 and Table 99-1. Nine nuclear heme biosynthetic genes, including separate genes for the housekeeping and erythroid-specific isozymes of ALA-synthase, encode the enzymes that catalyze the eight steps in the conversion of glycine and succinyl-CoA to heme (1). The first and the last three enzymes are in the mitochondrion, and the other four function in the cytosol. The characteristics of the genes, their respective enzymes, and their chro-mosomal locations are summarized in Table 99-1. The heme biosynthetic pathway is responsible for the pro-duction of heme for hemoproteins, including the super-family of cytochrome P450 enzymes, which are most abundant in the liver, and hemoglobin in erythrocytes.

2 CHAPTER 99 Inherited Porphyrias
TABLE 99-1 Human Heme Biosynthesis Enzymes and Genesa
Enzyme Gene SymbolChromosomal Location cDNA (bp) Protein (aa)
Gene
Size (kb) Exonsb
5-Aminolevulinate synthase: (ALA-synthase)Housekeeping ALAS1 3p21.1 2,199 640 17 11Erythroid-specific ALAS2 Xp11.2 1,937 587 22 115-Aminolevulinate dehydratase: (ALA-dehydratase)Housekeeping ALAD 9q32 1,149 330 15.9 12 (1A + 2–12)Erythroid-specific ALAD 9q32 1,154 330 15.9 12 (1B + 2–12)Hydroxymethylbilane synthase: (HMB-synthase)Housekeeping HMBS 11q23.3 1,086 361 11 15 (1 + 3–15)Erythroid-specific HMBS 11q23.3 1,035 344 11 15 (2–15)Uroporphyrinogen III synthase: (URO-synthase)Housekeeping UROS 10q26.2 1,296 265 34 10 (1 + 2B-10)Erythroid-specific UROS 10q26.2 1,216 265 34 (2A + 2B-10)Uroporphyrinogen
decarboxylaseUROD 1p34.1 1,104 367 3 10(URO-
decarboxylase)Coproporphyrinogen
oxidaseCPO 3q12.1 1,062 354 14 7(COPRO-oxidase)
Protoporphyrinogen oxidase
PPOX 1q23.3 1,431 477 5.5 13(PROTO-oxidase)
Ferrochelatase FECH 18q21.31 1,269 423 45 11
aReferences in Anderson KE, Sassa S, Bishop DF, et al. (2001) Disorders of heme biosynthesis: X-linked sideroblastic anemias and the porphyrias. In Scriver CR, Beaudet AL, Sly WS, Valle D (eds): The Metabolic and Molecular Basis of Inherited Disease, 8th ed. McGraw-Hill, New York, p 2991.
f(hcrrcognmhrtmca
bNumber of exons and (in parentheses) those encoding separate housekeeping and erythroid-specific forms.
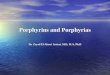
Different regulatory controls have evolved for hepatic and erythroid-specific heme synthesis, including negative feedback repression by heme in the liver, and separate erythroid-specific genes or promoters in the first four genes in the pathway (Figure 99-2). Each of the enzy-matic steps in the pathway is briefly described in this chapter.99.2.1.1 5-Aminolevulinate Synthase. The first enzyme in the pathway, 5-aminolevulinate synthase (ALA-synthase; also known as d-aminolevulinate syn-thase; E.C. 2.3.1.37), catalyzes the condensation of gly-cine (activated by pyridoxal phosphate) and succinyl coenzyme A to form ALA. Distinct human housekeep-ing and erythroid-specific ALA-synthase isozymes are encoded by separate genes: the ~17-kb housekeeping gene (ALAS1), located at chromosome 3p21.1, is expressed in all tissues, while the ~22-kb erythroid-specific gene (ALAS2), located at chromosome Xp11.21, is expressed only in erythroid cells to supply the large amounts of heme required for hemoglobin (see Figure 99-2). These findings provide a basis for the tissue-specific regulation of this pathway (for a review see Reference (1)). Of note, expression of the housekeeping gene ALAS1 in the liver is under negative feedback repression by the cellular heme concentration and functions to modulate the sup-ply of heme for the hepatic cytochrome P450 enzymes and other hepatic hemoproteins (7). In acute porphyr-ias, the depletion of hepatic heme by various drugs, hor-mones, and glucose restriction, the increased synthesis of the housekeeping ALAS1 isozyme, and the generation of
the large amount of the porphyrin precursors, ALA and PBG, are the biochemical hallmarks of acute neurologic attacks (2).
Mutations in the X-linked ALAS2 gene and the resul-tant deficient activity of the erythroid-specific isozyme cause X-linked sideroblastic anemia (1,8). Over 35 muta-tions in the erythroid-specific ALA-synthase gene causing X-linked sideroblastic anemia are listed in the Human Gene Mutation Database (www.hgmd.org) (6). Except or a mutation in the promoter region of the ALAS2 gene 9) and one nonsense mutation, all of the reported lesions ave been missense mutations in the ALAS2 catalytic ore encoded by exons 5 to 11, with the majority occur-ing in exons 5 and 9. Most mutations were pyridoxine esponsive in vivo and when expressed in Escherichia oli. Molecular modeling of the ALAS2 isozyme, based n the crystal structure of a bacterial ALA-synthase, sug-ested the molecular basis for the pyridoxine responsive-ess of certain mutations (10). Recently, gain of function utations in exon 11 of ALAS2 that increase its activity ave been shown to cause an X-linked form of eryth-opoetic protoporphyria (EPP), known as X-linked pro-oporphyria (XLP). To date, only two gain of function utations in ALAS2 have been described. No deficien-
ies of the ALAS1 isozyme have been described; presum-bly, the enzymatic deficiency would be lethal.
99.2.1.2 5-Aminolevulinic Acid Dehydratase. The second enzyme in the pathway is 5-aminolevulinic acid dehydratase (ALA-dehydratase; also known as PBG synthase; E.C. 4.2.1.24). This enzyme catalyzes the

CH
APTER
99 Inherited Porphyrias
3
TABLE 99-2 cal Features
Biochemical Findingsa
or CP Classification Erythrocytes Urine Stool5-ALA dehydratas
(ADP)in ALA, Coproporphyrin III — deficient
Acute intermittent ALA, PBG, Uroporphyrin — porphyriaCongenital erythro
porphyria (CEP rin IUroporphyrin I
Coproporphyrin ICoproporphyrin I
Porphyria cutanea Uroporphyrin, 7-carboxylate porphyrin
Isocoproporphyrin
Hepatoerythropoiephyria (HEP)
in Uroporphyrin, 7-carboxylate porphyrin
Isocoproporphyrin
Hereditary coprop(HCP)
ALA, PBG, Coproporphyrin III Coproporphyrin III
Variegate porphyr ALA, PBG, Coproporphyrin III Coproporphyrin III Protoporphyrin
Erythropoietic pro(EPP)
— Protoporphyrin
H, hepatic; E, erythrop hyrinogen; NV, neurovisceral; CP, cutaneous photosensitivity.aIncreases that may bbThese porphyrias alscInherited deficiency dPolymorphism in intr
Classification of the Human Porphyrias including Major Clinical and Biochemi
Symptomatology Porphyria Enzyme H or E
Principal Inheritance Deficient NV
e-porphyria 5-ALA-dehydratase Hb AR NV Zn-Protoporphyr
(AIP) HMB-synthase H AD NV —poietic )
URO-synthase E AR CP Uroporphyrin I Coproporphy
tarda (PCT) URO-decarboxylase H ADc CP —
tic por- URO- decarboxylase H AR CP Zn-Protoporphyr
orphyria COPRO-oxidase H AD NV & CP (uncommon)
—
ia (VP) PROTO-oxidase H AD NV & CP —
toporphyria Ferrochelatase E ADd CP Protoporphyrin
oietic; AR, autosomal recessive; AD, autosomal dominant; Type I isomers: ALA = 5-aminolevulinic acid; PBG = porpe important for diagnosis.o have erythropoietic features including increased erythrocyte porphyrins.of UROD is partially responsible for familial (Type II) PCT.on 3 of wild-type allele affects level of enzyme activity and clinical expression.

4 CHAPTER 99 Inherited Porphyrias
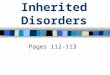
FIGURE 99-1 The human heme biosynthetic pathway. Ac, acetyl; Pr, proponyl.
condensation of two molecules of ALA to form the cyclic pyrrole, PBG (see Figure 99-1). Human ALA-dehydra-tase is composed of eight identical 31-kDa subunits and eight atoms of zinc, which are required for both enzyme stability and catalytic activity. The zinc atoms are bound to each subunit by a typical zinc finger domain consisting of four cysteine and two histidine residues (1). The zinc atoms protect essential sulfhydryl groups in the enzyme and can be displaced by lead or other heavy metals. In fact, the measurement of erythrocyte ALA-dehydratase activity is a highly sensitive index of lead exposure.
The 16-kb human ALA-dehydratase gene encodes housekeeping and erythroid-specific transcripts by alter-native splicing (11); see Figure 99-2. Both transcripts encode the same amino acid sequence, as translation begins in exon 2. The housekeeping promoter region is upstream of exon 1A, while the erythroid-specific promoter is upstream of exon 1B. Mutations in the ALA-dehydratase gene result in the deficiency of ALA-dehydratase, causing a rare, recessively inherited acute hepatic porphyria, ALA- dehydratase-deficient porphyria (ADP) (6,12,13). Only six cases of ADP with 13 different ALA-dehydratase mutations have been reported (www.hgmd.org) (6,14).
Of note, there are two common alleles at the ALA-dehydratase locus, ALAD1 and ALAD2, which are responsible for three electrophoretically distinguish-able enzyme forms designated 1–1, 1–2, and 2–2. The frequencies of the corresponding phenotypes in white populations are about 80%, 18%, and 1%, respectively,
giving gene frequencies of 0.9 and 0.1 for the ALAD1 and ALAD2 alleles, respectively. Gene frequency of the ALAD2 allele is lower in Hispanics, Asians, and African-Americans (15), and in a Liberian population, the ALAD2 allele was not detected. The ALAD2 allele has normal ALA-dehydratase activity but may bind zinc more effectively. Several epidemiologic studies have demonstrated an association between the ALAD2 allele and high lead levels (16–20). Although blood and serum lead levels were 5%–10% greater in individuals with the ALAD2 allele than in individuals with the other alleles, bone lead was not increased (17).99.2.1.3 Hydroxymethylbilane Synthase. Hydroxy-methylbilane synthase (HMB-synthase; formerly known as PBG-deaminase or uroporphyrinogen I synthase; E.C. 4.3.1.8), the third enzyme in the pathway, cata-lyzes the head-to-tail condensation of four molecules of PBG by a series of deaminations to form the linear tetrapyrrole, hydroxymethylbilane (HMB) (see Figure 99-1). HMB can cyclize nonenzymatically to form uro-porphyrinogen I, a nonphysiological and phototoxic compound. Because HMB-synthase activity is almost as low as ALA-synthase activity in the liver, it may become rate-limiting when the enzyme is partially defi-cient. The ~10-kb human HMB-synthase gene encodes erythroid-specific and housekeeping isozymes by alter-native splicing (see Figure 99-2). The housekeeping and erythroid isozymes are monomeric proteins of 361 and 344 amino acid residues, respectively. The housekeep-ing promoter functions in all cell types, whereas the

CHAPTER 99 Inherited Porphyrias 5
Mitochondria Cytoplasm
SUCCINYL COA
GLYCINE 5-AMINOLEVULINICACID
ALA -
Synthase
Ferrochelatase
PROTO - Oxidase
HMB-
Synthase
5-ALA -
Dehydratase
URO-
Synthase
COPRO - Oxidase
COO
COO
C=O
COOCHCH2
CO2B6
CH2
NH2
CH3
CH3
CH3
2H+
Fe++
CH3
CH2C
C
C NHHH
HH
N N
N
ViVi
N
PrHEME
Pr
Fe
CoAS
CoASH
O
CH3
CH3
CH3 CH
NH
HN
N
ViVi
N
PrPROTOPORPHYRIN IX
Pr
PROTOPORPHYRINOGEN IX
CH
CH3
CH3 CH
NH
HH
HN
N
ViVi
N
Pr Pr
6H
2CO2 2H
URO -
Decarboxylase
Ac
Ac
Ac
AcHO
H2O
4 NH3
NH2
CH2 CH2
CH2
CH2
H2O
NH H
HHN
NN
Pr
Pr
Pr
Pr
HYDROXYMETHYLBILANE
PORPHOBILINOGEN
UROPORPHYRINOGEN III
COPROPORPHYRINOGEN III
Ac
Ac
Pr
Ac
NH H
HHN
NN
Pr
Pr
Ac
Pr
CH3
CH3
Pr
CH3
NH H
HHN
NN
Pr
Pr
CH3
Pr
4H
4CO2
N HH
COOCOO
Feedback Repression
FIGURE 99-2 The first four genes in the human heme biosynthetic pathway have housekeeping (PH) and erythroid-specific (PE) promoters and transcripts. The dotted lines indicate the exons transcribed by each promoter.
erythroid promoter functions only in erythroid cells. Human HMB-synthase has been purified from eryth-rocytes and its properties are characterized. Of note, the enzyme forms stable covalent enzyme–substrate complexes with PBG (21), and a unique dipyrrometh-ane cofactor binds the di- and tri-pyrrole intermedi-ates at the active site until the formation of HMB is complete (22).
Mutations in the HMB-synthase gene result in the deficient activity of HMB-synthase, causing acute intermittent porphyria (AIP), an autosomal dominant acute hepatic porphyria (23). Over 300 HMB-synthase mutations are listed in the Human Gene Mutation Database (www.hgmd.org) (6). Studies on crystallized HMB-synthase from E. coli showed that the protein is folded into three domains, each comprising b-strands and

6 CHAPTER 99 Inherited Porphyrias
a-helices and a discrete hydrophobic core. Because the human and E. coli HMB-synthase amino acid sequences have about 35% homology and greater than 70% simi-larity, it was possible to infer the structure–function rela-tionships for certain human HMB-synthase mutations from the bacterial enzyme (24,25).99.2.1.4 Uroporphyrinogen III Synthase. Uropor-phyrinogen III synthase (URO-synthase; E.C. 4.2.1.75) catalyzes the rearrangement of HMB by inversion of the pyrrole D ring and ring closure to form the asymmetric uroporphyrinogen type III isomer (see Figure 99-1). In the absence of URO-synthase, HMB nonenzymatically cyclizes to form the uroporphyrinogen I isomer. This nonphysiologic compound can be metabolized to copro-porphyrinogen I, but further metabolism cannot proceed as the next enzyme, coproporphyrinogen oxidase, is ste-reospecific for the III isomer.
The ~34-kb human URO-synthase gene has alter-native promoters that generate housekeeping and erythroid-specific transcripts, which encode the same 265 amino acid polypeptide (see Figure 99-2) (26). The enzyme is active as a 29.5-kDa monomer. The human enzyme has been crystallized at a resolution of 1.85 Å (27). The protein folds into two alpha/beta domains connected by a beta-ladder, with the active site between the domains.
Mutations in the URO-synthase gene results in defi-cient but not absent, URO-synthase enzyme activity, causing congenital erythropoietic porphyria (CEP), an autosomal recessive erythropoietic porphyria (6,28). Over 35 URO-synthase mutations are listed in the Human Gene Mutation Database (www.hgmd.org) (6).99.2.1.5 Uroporphyrinogen Decarboxylase. Uro-porphyrinogen-decarboxylase (E.C. 4.1.1.37), the fifth enzyme in the pathway, catalyzes the sequential removal of the four carboxyl groups from the acetic-acid side chains of uroporphyrinogen III (clockwise, starting with ring D) to form the four methyl groups of coproporphy-rinogen III, a tetracarboxyl porphyrinogen (see Figure 99-1). The enzyme has no coenzyme or metal require-ments, and iron does not appear to directly affect URO-decarboxylase activity in vitro.
The ~3-kb human URO-decarboxylase gene has a single-mRNA species, which expresses a 367-residue polypeptide in all tissues, where it is active as a homodi-mer (29,30). Recombinant human URO-decarboxylase has been crystallized at 1.60-Å resolution, and its reac-tion mechanism has been studied (30–33).
This enzyme is deficient in the liver in PCT, the most common porphyria. The majority (~80%) of PCT patients have no URO-decarboxylase mutations and are termed type I if the disease is sporadic or type III, if (rarely) more than one family member is affected. Het-erozygous mutations and half-normal enzyme activities are found in all tissues (e.g. erythrocytes) in familial (type II) PCT (~20% of all PCT patients). In overt PCT of all types, hepatic URO-decarboxylase activity is always
reduced by additional factors to well below 50% of nor-mal, which is consistent with an acquired tissue-specific inhibition of hepatic URO-decarboxylase. Hepatoeryth-ropoietic porphyria (HEP) is the homozygous form of familial (type II) PCT and, generally, has a more severe phenotype (1,34). Over 100 URO-decarboxylase muta-tions identified in PCT and HEP are listed in the Human Gene Mutation Database (www.hgmd.org) (6).99.2.1.6 Coproporphyrinogen Oxidase. The sixth enzyme in the pathway, coproporphyrinogen oxidase (COPRO-oxidase; E.C. 1.3.3.3), catalyzes the decar-boxylation of two of the four propionic acid groups of coproporphyrinogen III (on rings A and B) to form the two vinyl groups of protoporphyrinogen IX, a dicar-boxyl porphyrinogen (see Figure 99-1). COPRO-oxidase is located between the mitochondrial inner and outer membranes, requires molecular oxygen for its activity, and contains no metals (1,35). An intermediate in the two-step decarboxylation is a 3-carboxyl porphyrinogen (termed harderoporphyrinogen, because this porphyrin in its oxidized form (harderoporphyrin) was first isolated from the rodent harderian gland). Coproporphyrinogen I, which is formed by decarboxylation of uroporphyrino-gen I, is not a substrate for this enzyme and therefore is not metabolized to heme.
The ~14-kb human COPRO-oxidase gene encodes a single transcript, which expresses a 474-residue polypeptide including an N-terminal mitochondrial, targeting signal peptide of 120 residues (36–38). Human COPRO-oxidase has been crystallized to a resolution of 1.58 Å (39). Studies of the crystal structure confirmed that COPRO-oxidase functions as a dimer and identified the residues in the enzyme’s active site (39).
Mutations in the COPRO-oxidase gene result in defi-cient enzymatic activity, causing HCP, an autosomal dominant disorder (40). Over 40 COPRO-oxidase muta-tions are listed in the Human Gene Mutation Database (www.hgmd.org) (6). Mutation K404E in the COPRO-oxidase gene, when present in either the homozygous or compound heterozygous states, causes a biochemi-cal variant, termed harderoporphyria (39,41). Cases of homozygous dominant HCP have also been described (6,42,43).99.2.1.7 Protoporphyrinogen Oxidase. The seventh enzyme in the pathway, protoporphyrinogen oxidase (PROTO-oxidase; E.C. 1.3.3.4), catalyzes the oxidation of protoporphyrinogen IX to protoporphyrin IX by the removal of six hydrogen atoms (see Figure 99-1). The product of the reaction is a porphyrin (oxidized form), in contrast to the preceding several products, which are porphyrinogens (reduced forms). This oxidation occurs readily in vitro under aerobic conditions in the absence of the enzyme. PROTO-oxidase is an integral protein of the mitochondrial inner membrane spacing and appears to be active as a dimer. PROTO-oxidase is inhibited by bilirubin, perhaps accounting for the decreased levels of the enzyme activity in Gilbert disease.

CHAPTER 99 Inherited Porphyrias 7
The ~5.5-kb human PROTO-oxidase gene encodes a single ~1.8-kb mRNA in all tissues, which expresses a mitochondrial-targeted polypeptide of 477 amino acids (~51 kDa) (44–46). PROTO-oxidase lacks a typical mitochondrial targeting leader sequence but is effectively targeted by its 17 N-terminal residues (36).
Mutations in the PROTO-oxidase gene result in 50% of normal enzymatic activity, causing VP, a domi-nantly inherited hepatic porphyria (47). Over 150 PROTO-oxidase mutations are listed in the Human Gene Mutation Database (www.hgmd.org) (6). Several cases of homozygous VP have also been described (48,49).99.2.1.8 Ferrochelatase. The final step in heme bio-synthesis is the insertion of ferrous iron into protopor-phyrin IX to form heme. This reaction is catalyzed by ferrochelatase (heme synthetase or protoheme ferrolyase; E.C. 4.99.1.1), which is associated with the inner side of the inner mitochondrial membrane. The enzyme is spe-cific for the reduced form of iron (Fe2+) but can use other metals (e.g. Zn2+ and Co2+) and other 2-carboxyl por-phyrins. The enzyme appears to function as a dimer in mitochondria (50), and there is suggestive evidence that the membrane domains of PROTO-oxidase dock onto the dimeric structure of ferrochelatase (51).
The ~45-kb human ferrochelatase gene encodes a 423-amino acid polypeptide including a 54-residue leader sequence (36). An iron–sulfur cluster [2Fe-2S] has been identified in recombinant human and mouse ferrochelatase (52,53) and is thought to be essential for enzyme activity (54). The putative iron–sulfur binding site is at the C-terminus in a 30-amino acid region that contains four cysteines. Recombinant human ferroche-latase has been crystallized and diffracted to about 2 Å (55,56).
Coding region mutations in the ferrochelatase gene result in a decreased enzymatic activity, causing erythro-poietic protoporphyria (EPP) (57). Over 100 ferrochela-tase mutations are listed in the Human Gene Mutation Database (www.hgmd.org) (6). Clinical expression of this porphyria occurs when a disabling ferrochelatase muta-tion is heteroallelic with a polymorphism in intron 3 of the wild-type ferrochelatase gene that reduces expression of normal enzyme (58) or, less commonly, in individuals who inherit two mutations that impair enzyme function (e.g. coding region or splice-site mutations).
99.3 REGULATION OF HEME BIOSYNTHESIS
In humans, about 85% of heme is synthesized in ery-throid cells to provide heme for hemoglobin, while most of the remaining heme is produced in the liver, where it is used primarily as the prosthetic group in cytochrome P450 enzymes and other hemoproteins. In the liver, the heme biosynthetic pathway is under a negative feedback control at the level of the first enzyme in the pathway, ALAS1 (the housekeeping form), by the concentration
of “free” heme (7). Heme represses the transcription and translation of liver ALAS1 mRNA, reduces ALAS1 mRNA stability (7), and interferes with the transport of the enzyme into mitochondria. High concentrations of free heme can also induce heme oxygenase and there-fore stimulate heme catabolism (59). ALAS1 is inducible by many of the same chemicals that induce the hepatic cytochrome P450 enzymes. Because most of the heme synthesized in the liver is used for the synthesis of the cytochrome P450 enzymes, the induction of hepatic ALA-synthase and the cytochrome P450s occurs in a coordinated fashion. Recently, two sequence elements in the distal 5¢-flanking region of the human ALAS1 gene were identified, which mediate direct transcrip-tional activation in response to drugs metabolized by the cytochrome P450s (60). When the regulatory “free” heme pool becomes depleted (which may occur, for example, when more heme is required for the synthesis of hemoproteins), the synthesis of ALAS1 is increased. Conversely, repression of ALAS1 synthesis results from augmentation of the regulatory heme pool. The evidence that ALA-synthase1 functions as a rate-controlling enzyme, at least in the liver, includes its relatively low Vmax value (compared with most other enzymes in the pathway), its inducibility and short half-life, and its great sensitivity to repression by cellular heme (at con-centrations below 10−6M). In addition, ALAS1 mRNA is markedly increased under conditions when more heme is required by cells while expression of the other enzymes in the pathway do not change significantly (7). The low affinity of the enzyme for glycine suggests that the intra-cellular glycine concentration also determines the rate of ALA formation.
In erythroid cells, there are novel regulatory mech-anisms for the production of the very large amounts of heme needed for hemoglobin synthesis. As noted previously, there is a separate erythroid-specific ALA-synthase gene (ALAS2) (1) and unique erythroid-specific promoters in ALA-dehydratase (11), HMB-synthase (23), and URO-synthase (61), the first four enzymes in the heme biosynthetic pathway (see Figure 99-2). The erythroid-specific gene ALAS2 on the X chromosome is expressed at high levels during erythroid differentiation. Synthesis of ALAS2, unlike ALAS1, is not repressed by hemin treatment and therefore is not regulated by the heme feedback repression. Transcriptional control of ALAS2 is exerted by erythroid-specific promoter ele-ments in the 5¢-flanking region of the gene. Transla-tional control results from an iron-responsive element in the 5¢-untranslated region of the mRNA. Transcription of the housekeeping ALAS1 gene may be downregu-lated during erythroid differentiation. In addition, heme regulates the rate of its synthesis in erythroid cells by controlling the transport of iron (required for ferrochela-tase) into reticulocytes. Thus, the rate of iron acquisition from transferrin may be an important regulator of the erythroid heme biosynthesis (62).

8 CHAPTER 99 Inherited Porphyrias
These enzymes function in all cells to make heme for cytochromes and other hemoproteins. However, regula-tion of the heme biosynthesis in many tissues has not been the subject of intensive investigation, and some studies suggest that it may be different in tissues other than the liver and bone marrow (1).
99.4 CLASSIFICATION AND DIAGNOSIS OF THE PORPHYRIAS
As mentioned previously, the porphyrias can be classi-fied as either hepatic or erythropoietic, depending on whether the heme biosynthetic intermediates that accu-mulate arise initially from the liver or developing eryth-rocytes, or as acute or cutaneous, based on their clinical manifestations. Table 99-2 lists the porphyrias, their symptoms, major biochemical abnormalities, and inheri-tance patterns. Further details on the deficient enzymes are given in Table 99-3. Of the five hepatic porphyrias, four of them, acute intermittent porphyria (AIP), HCP, VP, and ALA-dehydratase porphyria (ADP), are pres-ent with acute attacks of neurologic manifestations and elevated levels of one or both of the porphyrin precur-sors, ALA and PBG, and are thus classified as acute porphyrias. Symptoms of neuropathic abdominal pain, peripheral neuropathy, and mental disturbances develop during adult life and are more common in women than in men (1,2,4). By contrast, PCT, while classified as a hepatic porphyria, presents with blistering skin lesions and not acute attacks. HCP and VP may cause cutane-ous manifestations similar to PCT, in addition to acute neurological symptoms. The erythropoietic porphyrias, CEP, and EPP, are characterized by elevations of porphy-rins in bone marrow and erythrocytes and present with
cutaneous photosensitivity. X-linked protoporphyria, a variant form of EPP, has a clinical presentation identi-cal to classic EPP. Lesions in CEP resemble PCT but are usually much more severe, whereas EPP causes a more immediate, painful, and nonblistering type of photosen-sitivity. Homozygous dominant forms of AIP, HCP, VP, and familial (type II) PCT (known as HEP) and the auto-somal recessive ADP also have erythropoietic features (e.g. increased erythrocyte porphyrins). Rare patients who have mutations in two different heme biosynthetic genes have also been described (see “Dual Porphyrias” section).
99.4.1 Diagnosis
When porphyria is suspected clinically, proper labora-tory testing is important to confirm or exclude the diag-nosis for appropriate medical management and genetic counseling (2). Accuracy and speed are especially impor-tant in the diagnosis of an acute porphyric attack, so treatment can begin to prevent neurologic damage and even death. Tests for porphyria may be difficult to inter-pret because some abnormal results are seen in disorders other than the porphyrias; in particular, minimally ele-vated levels of urinary porphyrins may have little or no diagnostic significance.
Table 99-3 summarizes the major metabolites that accumulate in each porphyria. However, for initial diag-nosis of porphyrias, it is unwise to measure all of these intermediates routinely or attempt to identify a diagnos-tic profile. For initial screening, we recommend relying on a limited number of tests that are sensitive, specific, and cost effective; additional testing should be done only if a screening test is positive. Testing for elevated urinary
TABLE 99-3 Human Porphyrias Associated with Deficiencies of Specific Enzymes of the Heme Biosynthetic Pathway
InheritanceDeficient Enzyme
Subcellular Localization
Enzyme Activity % of Normal
Known Mutations nd
Porphyria OMIM Numbera
5-ALA dehydratase-deficient 125270 AR ALA-dehydratase C ~5 9 porphyria (ADP)Acute intermittent 176000 AD HMB-synthase C ~50244 porphyria
(AIP)Congenital erythropoietic 263700 AR URO-synthase C 1–5 36 porphyria
(CEP)Porphyria cutanea tarda 176100 AD URO-decarboxylase C ~50b 55 (PCT, type II)Hepatoerythropoietic 176100 AR URO-decarboxylase C 1–5 10 porphyria
(HEP)Hereditary coproporphyria 121300 AD COPRO-oxidase M ~50 37 (HCP)Variegate porphyria (VP) 176200 AD PROTO-oxidase M ~50 129Erythropoietic 177000 ADc Ferrochelatase M ~20–3088 protopor-
phyria (EPP)
AR, autosomal recessive; AD, autosomal dominant; C, cytosolic; M, mitochondrial.aOMIM, Online Mendelian Inheritance in Man (www.ncbi.nlm.nih.gov/entrez/query.fcgi?=OMIM).bClinical expression occurs when an iron-mediated inhibitor of URO-decarboxylase is generated and enzyme activity is further reduced (see text for details).cPolymorphism in intron 3 of wild-type allele affects level of enzyme activity and clinical expression.dNumber of known mutations from Human Gene Mutation Database (www.hgmd.org) as of March 29, 2006.

CHAPTER 99 Inherited Porphyrias 9
PBG is especially important in screening for acute por-phyrias. Active cutaneous porphyrias are readily detected by measuring total plasma porphyrin levels, although, if EPP is suspected, measurement of erythrocyte pro-toporphyrin is more sensitive. If a screening test result is abnormal, additional measurements are essential for establishing the specific type of porphyria (2). Urinary ALA and PBG are easily quantified by chemical methods (63), and the individual porphyrins in urine and feces can be separated and quantified by high-performance liquid chromatography. Assays are described in the literature for each of the eight heme biosynthetic enzymes, using erythrocytes, lymphocytes, cultured lymphoblasts, or cultured fibroblasts, although most are not widely avail-able for diagnostic purposes (63). However, erythrocyte HMB-synthase activity is commonly measured to con-firm the diagnosis of AIP and detect asymptomatic gene carriers.
Establishing the definitive diagnosis of a particular porphyria should include identification of the causative gene mutation(s). This is the preferred method for detect-ing asymptomatic relatives who carry the mutation iden-tified in an index case (2).
99.4.2 5-Aminolevulinic Acid Dehydratase-Deficient Porphyria (ADP)
ALA-dehydratase-deficient porphyria (ADP) is a rare autosomal recessive acute hepatic porphyria caused by the severe deficiency of ALA-dehydratase activity (1,2). To date, only six cases have been reported with documentation by molecular methods (1,12–14). These affected homozygotes had less than 10% of normal ALA-dehydratase activity in erythrocytes, but their clini-cally asymptomatic parents and other heterozygous rela-tives had about half-normal levels of activity and did not excrete increased levels of ALA. The frequency of ADP is unknown, but the frequency of heterozygous individuals with less than 50% of normal ALA-dehydratase activity was ~2% in a screening study, in Sweden. Because there are multiple causes for deficient ALA-dehydratase activ-ity, it is important to confirm the diagnosis of ADP by mutation analysis.99.4.2.1 Biochemical Aspects. ALA-dehydratase-deficient porphyria is characterized by the markedly increased urinary excretion of ALA and coproporphy-rin III and increased erythrocyte protoporphyrin (com-plexed with zinc). The markedly reduced erythrocyte ALA-dehydratase activity in these patients is not restored to normal by the in vitro addition of sulfhydryl reagents such as dithiothreitol. Immunologic studies in several cases revealed the presence of nonfunctional enzyme protein, which crossreacted with anti-ALA-dehydratase antibody.99.4.2.2 Molecular Aspects. Molecular studies of ADP patients have identified nine-point mutations, two splice-site mutations, a two-base deletion, and
two different base changes at position -11 bp upstream of the exon 3 start site in the ALA-dehydratase gene (Human Gene Mutation Database; www.hgmd.org) (6,12,14,64). The parents in each case were not con-sanguineous, and the index cases had inherited a dif-ferent ALA-dehydratase mutation from each parent. In addition, a point mutation, F12L, was identified in an asymptomatic Swedish girl who had 12% of normal erythrocyte ALA-dehydratase activity (64,65).
The molecular basis of the ALAD2 polymorphism is a substitution of a lysine by an asparagine at residue 95 (K95N). To date, ADP has not been diagnosed prena-tally, but this should be possible by determination of the ALA-dehydratase specific molecular lesions in cultured chorionic villi or amniocytes.99.4.2.3 Clinical Manifestations. The onset, sever-ity, and clinical presentations of ADP are variable, presumably depending on the amount of residual ALA-dehydratase activity. All patients had significantly elevated levels of plasma and urinary ALA, with little increase in PBG concentrations and ALA-dehydratase activities of 10% or less of normal. Four reported patients were male adolescents with symptoms resem-bling those of AIP, including abdominal pain and neu-ropathy (12–14). The third patient was an infant with more severe disease, including failure to thrive begin-ning at birth. The earlier age of onset and more severe manifestations in this patient reflect a more significant deficiency of ALA-dehydratase activity (64). Another patient was essentially normal until age 63, when he developed an acute motor polyneuropathy that was associated with a myeloproliferative disorder. This patient was heterozygous for an ALA-dehydratase mutation that presumably was present in erythroblasts that underwent clonal expansion due to the bone mar-row malignancy (66).99.4.2.4 Differential Diagnosis. Lead, styrene, and succinylacetone (which is structurally similar to ALA and accumulates in hereditary tyrosinemia type 1 due to fumarylacetoacetase deficiency) inhibit ALA-dehydratase, causing increased urinary excretion of ALA and coproporphyrin, and clinical manifestations that resemble those of the acute porphyrias. Idio-pathic acquired ALA-dehydratase deficiency has also been reported. Therefore, these known causes of ALA-dehydratase deficiency should be considered in the differential diagnosis of ADP and the diagnosis of ADP confirmed by demonstrating the underlying ALA-dehydratase mutations.99.4.2.5 Treatment. Because of the small number of ADP patients, there is a limited experience in treatment. Glucose has shown little benefit. Hemin therapy has helped the clinical symptoms in patients with adolescent-onset ADP (12,14,67) and was beneficial for preventing symptoms in one patient (12). A severely affected ADP child did not improve significantly with glucose, hemin, or liver transplant (13,64).

10 CHAPTER 99 Inherited Porphyrias
99.4.3 Acute Intermittent Porphyria
Acute intermittent porphyria (AIP) is an autosomal dom-inant acute hepatic porphyria resulting from half-normal levels of HMB-synthase activity. The disease occurs in all ethnic groups with an estimated frequency of individuals with acute attacks of 1 to 2 per 100,000 in most European countries, making it the most common acute porphyria (3,23). It is estimated that less than 10% of individuals with an HMB-synthase mutation have acute attacks (3). A survey of 3350 healthy French blood donors identified two with HMB-synthase gene mutations for a frequency of 1 in 1750, indicating that clinical expression is low (3). The highly variable symptoms and signs include vis-ceral, autonomic, peripheral, and central nervous system manifestations. Activation of the disease is clearly related to ecogenic factors, as its expression is usually triggered by hormonal, metabolic, dietary, or environmental fac-tors, which can precipitate acute attacks. Symptomatic patients always have increased urinary excretion of the porphyrin precursors ALA and PBG. However, the great majority of heterozygotes with HMB-synthase deficiency remains clinically asymptomatic (“latent” or presymp-tomatic) and may never have increased urinary ALA and PBG excretions.99.4.3.1 Biochemical Aspects. The metabolic defect in AIP is the half-normal activity of HMB-synthase. For most HMB-synthase mutations, the enzyme activ-ity is half-normal in all tissues. However, about 5% of patients have normal HMB-synthase activity in their erythrocytes (23) because they have mutations in or near exon 1 (see “Molecular Aspects” section). Moreover, the range of erythrocyte HMB-synthase activities in patients with classic AIP overlaps the range for normal individu-als, as discussed later. Hepatic HMB-synthase activ-ity in patients with active and latent AIP has not been compared.99.4.3.2 Molecular Aspects. To date, over 300 mutations have been identified, most being either point or splice-site mutations (Human Gene Mutation Data-base (www.hgmd.org) (6). Most are private, occurring in only one or a few unrelated families. Exceptions include W198X and R116W, which are common in the Swedish and Dutch populations, respectively and G111R, which was found in Argentinean AIP patients (68). A study of 143 Russian and Finnish AIP patients identified genotype-phenotype correlations (69). Based on the crystal structure of E. coli HMB-synthase, effects of specific AIP mutations on the human enzyme structure and function have been predicted (24,25).
In a variant form of AIP, molecular studies have identified mutations that impair splicing of exon 1 to exon 3, thereby preventing the formation of the house-keeping but not the erythroid-specific transcript (1,6,23). Other exon 1 mutations alter the initiation of the trans-lation codon, thereby precluding the translation of the housekeeping transcript (70). These tissue-specific
splicing and initiation of translation mutations provide an explanation for the deficient activity in the liver and other nonerythroid tissues in these cases, while the levels of HMB-synthase activity in erythrocytes remain normal. This variant form of AIP can be suspected in a patient with increased PBG, normal erythrocyte HMB-synthase, and laboratory findings that exclude HCP and VP, and mutation analysis is required for confirmation.
Homozygous dominant AIP is a rare form of AIP in which patients have mutations in both of their HMB-synthase alleles and, therefore, very low (<2%) enzyme activity. The disease has been described in a Dutch girl, two young British siblings, and a Spanish boy (71,72). In these homozygous-affected patients, the disease pre-sented in infancy with failure to thrive, developmental delay, bilateral cataracts, and/or hepatosplenomegaly. Interestingly, all these patients’ mutations (R167W, R167Q, and R172Q) were in exon 10 within 5 bases of each other.99.4.3.3 Clinical Manifestations. Acute intermittent porphyria is characterized by neurovisceral disturbances that develop after puberty in a minority of heterozygotes with HMB-synthase deficiency. Symptoms and signs are nonspecific and require a high index of suspicion to sug-gest the proper diagnosis (2). Abdominal pain, which is the most common symptom, is usually steady and poorly localized, but may be cramping, and is accom-panied by nausea and vomiting. Constipation and signs of ileus, including abdominal distension and decreased bowel sounds, are common. However, increased bowel sounds and diarrhea may also occur. These abdominal manifestations are neurologic rather than inflamma-tory, and therefore tenderness, fever, and leukocytosis are generally absent or mild. Tachycardia, hyperten-sion, restlessness, fine tremors, and excess sweating may be explained by sympathetic overactivity. Dysuria and bladder dysfunction are common, and urinary retention may require catheterization. Chronic hypertension and impaired renal function may develop over a long term. AIP is also commonly associated with mild abnormali-ties in liver function and the risk of more advanced liver disease and hepatocellular carcinoma is increased.
Peripheral neuropathy in AIP is primarily motor and appears to result from axonal degeneration rather than demyelinization. However, paresis does not develop in all patients who suffer from acute attacks, even when abdominal symptoms are severe. Muscle weakness most commonly begins proximally, more often in the arms than in the legs. Tendon reflexes may be normal or hyper-active in early disease stages but are usually decreased or absent with advanced neuropathy. Paresis can be asymmetric and focal. Cranial nerves, most commonly the tenth and seventh, can be affected. Rarely, involve-ment of the optic nerves or occipital lobes may produce blindness. Extremity pain and paresthesia and areas of loss of sensation are indications of sensory involvement. Muscle weakness can progress to respiratory and bulbar

CHAPTER 99 Inherited Porphyrias 11
paralysis and death, but this seldom occurs unless the porphyria is not recognized, harmful drugs are not dis-continued, or appropriate treatment is not instituted. Sudden death, presumably due to cardiac arrhythmia, also may occur. Complete recovery even from severe neuropathy over a period of a year or longer is possible.
Central nervous system involvement during acute attacks may be manifested as anxiety, insomnia, depres-sion, disorientation, hallucinations, and paranoia and may suggest a primary mental disorder. Some patients have been mistakenly regarded as hysterical. Depres-sion and other mental symptoms may be chronic in AIP patients. However, it has not been proved that the preva-lence of AIP is higher in psychiatric patients than in the general population. Seizures may occur as part of the acute neurologic manifestations of AIP or as a result of hyponatremia, which have been observed and may result from a variety of causes, including inappropriate antidi-uretic hormone (ADH) secretion, gastrointestinal losses secondary to vomiting and diarrhea, poor intake, or excess renal sodium loss. Antiseizure drugs are problem-atic because almost all have at least some potential for exacerbating AIP, with clonazepam being less likely to do so than phenytoin or barbiturates. Improved overall morbidity and mortality in acute porphyrias in the past 20 to 30 years is attributable to earlier detection, less use of barbiturates and sulfonamides in clinical practice, and better treatment of acute attacks (4).99.4.3.4 Etiology and Pathogenesis. Most of the factors known to precipitate acute porphyric attacks have the potential to induce the synthesis of ALAS1 in the liver, thereby increasing the accumulation of ALA, PBG, and other heme pathway intermediates. Normally, a half-normal amount of hepatic HMB-synthase activity is sufficient to avoid any accumulation of PBG. However, when certain environmental, metabolic, and hormonal factors increase the flux of ALA, PBG, and porphyrino-gens through the pathway, the partially deficient activity of HMB-synthase may be insufficient to metabolize the increased amounts of PBG.
The etiology of the neurologic manifestations in AIP is not established (73). The possibility that ALA or PBG might be neurotoxic is favored by the increased production of porphyrin precursors during acute por-phyric attacks. ALA is taken up by most tissues more readily than PBG, which appears to more readily cross the blood–brain barrier. These intermediates may be converted in vivo to other substances, including por-phyrins, which may have neurotoxic potential. The fact that AIP, HCP, VP, ADP, plumbism, and hereditary tyrosinemia are all associated with increased ALA and similar neurologic manifestations favors a neuropathic role for ALA. Moreover, ALA is structurally analogous to g-aminobutyric acid (GABA) and can interact with GABA receptors (73).
Alternatively, deficient HMB-synthase activity could lead to a functional heme deficiency in the nervous
system, or predispose to unsaturation of hepatic tryp-tophan pyrrolase, thus leading to altered tryptophan delivery to nervous tissue. Experimental observations regarding these and other possible mechanisms for neu-rologic dysfunction in the acute porphyrias are reviewed in more detail, elsewhere (2,72,73).
A mouse model in which HMB-synthase deficiency was introduced by gene targeting has been developed (74,75). These animals, when treated with a barbiturate, have impaired motor function, ataxia, increased levels of ALA in brain and plasma, and decreased heme satu-ration of liver tryptophan pyrrolase. Motor neuropathy can develop in these mice with normal or only slightly increased plasma or urinary ALA, suggesting a role for heme deficiency in nervous tissue (73,74). Studies of the brain MRIs of children with homozygous AIP have sug-gested damage primarily in white matter that was myelin-ated postnatally, while tracks that myelinated prenatally were normal (72). These findings suggest that a postnatal toxin such as elevated ALA or PBG rather than heme deficiency caused nervous tissue damage since prenatally elevated ALA and PBG would cross the placenta and be excreted in the mother’s urine. Also, the recent finding that a hepatic transplant cured a woman with AIP who had 37 acute attacks in 29 months pre-transplant sup-ports the notion that the acute attacks result from the excess porphyrin precursors produced in the liver (76).99.4.3.5 Precipitating Factors. Certain clinical fea-tures of AIP suggest that endogenous steroid hormones are important precipitating factors (1). These include (i) the rarity of symptoms and excess porphyrin precur-sor excretion before puberty; (ii) more frequent clinical expression in women than in men; (iii) premenstrual attacks of the disease in some women and their pre-vention by gonadotropin-releasing hormone (GnRH) analogues; (iv) exacerbation of AIP due to exogenous steroids, such as oral contraceptive preparations; and (v) the presence of more subtle abnormalities in steroid hor-mone metabolism, such as a deficiency of hepatic steroid 5a-reductase activity. The latter can predispose to the excess production of steroid hormone metabolites that are inducers of hepatic ALAS1.
99.4.3.5.1 Pregnancy Is Usually Well Tolerated. However, some women with AIP do experience an increased frequency of attacks during pregnancy. Ear-lier reports that worsening symptoms during pregnancy are more common may have been due in part to the use of barbiturates and perhaps to reduced caloric intake. Thus, pregnancy is not contraindicated in most women with AIP if harmful drugs are avoided and attention is given to proper nutrition.
Drugs are an important cause of AIP attacks, and the avoidance of harmful drugs can favorably impact the disease course. The major drugs known or strongly sus-pected by most observers to be harmful in the acute por-phyrias, as well as drugs that are known to be safe, are listed in Table 99-4 and include most anticonvulsants,

12 CHAPTER 99 Inherited Porphyrias
barbiturates, sulfonamide antibiotics, and metoclo-pramide. Other reviews and more extensive lists of drugs that are harmful or safe are published (1,2) or available through the American Porphyria Foundation Web site (www.porphyriafoundation.com) and the European Porphyria Initiative Web site (www.porphyria-europe.org). Most porphyrogenic drugs (e.g. barbiturates) exert their action by induction of hepatic ALAS1, cyto-chromes P450, and heme synthesis in the liver. Smoking
TABLE 99-4 Some Major Drugs Considered Unsafe and Safe in Acute Porphyriasa
Unsafe Safe
Alcohol AcetaminophenBarbituratesb AspirinCarbamazepineb AtropineCarisoprodolb BromidesClonazepam (high doses)Danazolb Erythropoietinb,c
Diclofenac and possibly other Gabapentin NSAIDsb
Ergots GlucocorticoidsEstrogensb,d InsulinEthchlorvynolb Narcotic analgesicsGlutethimideb Penicillin and derivativesGriseofulvinb
Mephenytoin Ranitidineb,c
Meprobamateb (also mebutamateb, Streptomycin tybutamateb)MethyprylonMetoclopramideb
Phenytoinb
Primidoneb
Progesterone and synthetic progestinsb
Pyrazinamideb
Pyrazolones (aminopyrine, antipyrine)
Rifampinb
Succinimides (ethosuximide, methsuximide)
Sulfonamide antibioticsb
Valproic acidb
NSAIDs, nonsteroidal anti-inflammatory drugs.aMore extensive list of drugs and their status are available in Anderson KE, Sassa S, Bishop DF, et al. (2001) Disorders of heme biosynthesis: X-linked sideroblastic anemias and the porphyrias. In Scriver CR, Beaudet AL, Sly WS, Valle D (eds): The Metabolic and Molecular Basis of Inherited Disease, 8th ed. McGraw-Hill, New York, p 2991; also see Web sites (www.porphyriafounda-tion.com; www.porphyria-europe.com).bPorphyria is listed as a contraindication, warning, precaution, or adverse effect in the U.S. labeling for these drugs. For drugs listed as unsafe, absence of such cautionary statements in the U.S. labeling does not imply lower risk.cAlthough porphyria is listed as a precaution in the U.S. labeling, these drugs are regarded as safe by other sources.dEstrogens have been regarded as harmful, mostly from experience with estrogen–progestin combinations and because they can exacerbate por-phyria cutanea tarda (PCT). Although the evidence that they exacerbate acute porphyrias is weak, they should used with caution. Low doses of estro-gen (e.g. transdermal) have been used safely to prevent side effects of GnRH analogues in women with cyclic attacks.
results in exposure to chemicals that induce cytochrome P450 enzymes and heme synthesis in the liver, and may increase the risk of attacks.
A large retrospective study of risk from anesthetic use in AIP concluded that barbiturates or other induc-ing drugs are quite frequently detrimental in patients who have already displayed porphyric symptoms, but that they seldom exacerbate latent disease (77). Drugs are only rarely reported to cause acute symptoms in children, who have naturally low levels of endogenous hormones. Such observations indicate that attacks are likely to be due to the additive effects of more than one precipitating factor.
Attacks can also be provoked by intercurrent infec-tions and other illnesses and by major surgery. The mech-anisms are not understood but may involve metabolic stress, impaired nutrition, and the increased production of steroid hormones and their ALA-synthase-inducing metabolities. A low caloric intake, usually instituted in an effort to lose weight, is a common contribut-ing cause of acute attacks. Caloric or carbohydrate restriction can precipitate acute symptoms of AIP and increase porphyrin precursor excretion. Recent findings indicate that hepatic ALAS1 is regulated by the per-oxisome proliferator-activated receptor g coactivator 1a (PGC-1a), which may represent an important link between nutritional status and acute porphyrias (78).99.4.3.6 Laboratory Evaluations. Urinary excretion of porphyrin precursors is markedly increased during acute attacks of AIP. Fecal porphyrins are usually nor-mal or minimally increased in AIP, which helps to dis-tinguish this disorder from HCP and VP. Because ALA and PBG are colorless, the reddish urine observed in AIP is due to increased porphyrins, which can form nonen-zymatically from PBG. Brownish discoloration may be due to porphobilin, a degradation product of PBG, or dipyrrylmethenes. A normal result of a quantitative test for urinary PBG during a symptomatic period virtually excludes acute porphyria as a cause for concurrent symp-toms. An exception is ADP, in which there is an increase in ALA, but not PBG (2).
It is useful to follow ALA and PBG excretion in a symp-tomatic patient because the concentrations of these com-pounds generally decrease with clinical improvement. Such decreases are particularly dramatic after heme infu-sions. But, it is unusual for excretion of ALA and PBG to decrease to normal levels and remain normal unless the disease becomes clinically latent for a prolonged period. In contrast, ALA and PBG levels are often less elevated and may decrease to normal soon after acute attacks of HCP and VP.
The diagnosis of AIP heterozygotes can be confirmed by the finding of half-normal levels of erythrocyte HMB-synthase. However, normal erythrocyte HMB-synthase activity does not exclude AIP, as some mutations in the HMB-synthase gene lead to a deficiency of the enzyme in the liver and other organs, but not in erythrocytes

CHAPTER 99 Inherited Porphyrias 13
(1,78,79). A definitive diagnosis may also be precluded because of the following: (i) the normal range for eryth-rocyte HMB-synthase activity is wide (up to threefold) and low normal and high carrier values overlap; (ii) the enzyme activity is much higher in younger than older erythrocytes and therefore increases when erythropoiesis is stimulated; and (iii) improper processing, storing, and shipping of blood samples can decrease enzyme activity (2). The specific molecular defect in the HMB-synthase gene should be identified in each family in order to provide accurate diagnosis of presymptomatic AIP heterozygotes (2). Most HMB-synthase mutations are family-specific, with a few notable exceptions, where particular muta-tions have been transmitted over generations from sin-gle founders (1). Patients with AIP should have genetic counseling and be encouraged to inform family members about the disease and its genetics. Knowledge of genetic status enables family members to make informed deci-sions about lifestyle and to know the potential risks of certain drugs, preferably before the development of an acute illness. However, latent porphyria should not be construed as a health risk that limits health or life insur-ance. Prenatal diagnosis of AIP has been performed by enzymatic assay but is seldom indicated because the out-look for most carriers is favorable.99.4.3.7 Treatment.
99.4.3.7.1 Supportive and Symptomatic Treat-ment. Hospitalization may be required: for evaluation and treatment of severe pain, nausea, and vomiting; for administration of intravenous fluids, electrolytes, glu-cose, and hemin; and for close observation for electrolyte derangements and neurologic complications. Medica-tions taken by the patient should be reviewed immedi-ately and those identified as harmful stopped, if at all possible. Narcotic analgesics are usually required for abdominal pain, and small to moderate doses of a phe-nothiazine are indicated for nausea, vomiting, anxiety, and restlessness.
Carbohydrate loading provides nutritional replace-ment, has some repressive effect on hepatic ALA syn-thase, but is less effective than hemin. It may suffice for mild attacks in patients with low narcotic requirements and without hyponatremia or paresis. Sucrose, glucose polymers, or carbohydrate-rich foods may be given to patients without abdominal distention and/or ileus and who can tolerate oral treatment. The standard intra-venous regimen is 10% glucose for a total of at least 300–500 g daily. However, large volumes of 10% glu-cose may increase the risk of hyponatremia. Severe or prolonged attacks should be treated with hemin and may also require more nearly complete nutritional support.
Tachycardia and systemic arterial hypertension may be treated cautiously with b-adrenergic blocking agents, but they may be hazardous in patients with hypovole-mia, in whom increased catecholamine secretion may be an important compensatory mechanism (2). Seizures
are difficult to treat because almost all antiseizure drugs can exacerbate an attack. Gabapentin, and probably vigabatrin, can be given safely and benzodiazepines are relatively safe. Careful correction of hyponatremia and hypomagnesemia is important, particularly when associ-ated with seizures.
99.4.3.7.2 Hemin Therapy. Intravenous hemin addresses the underlying pathophysiology by repressing hepatic ALAS1, hence decreasing the overproduction of ALA and PBG. Hemin given intravenously at moderate dose (3–4 mg/kg day for 4 days) is mostly taken up in the liver, and can at least transiently replenish the depleted heme pool that regulates the synthesis of ALAS1. It can-not be given orally because it is catabolized by heme oxy-genase during intestinal absorption.
Hemin therapy should be started early (2). Although product labeling recommends an initial trial of intrave-nous glucose, hemin is the preferred therapy (80–82). The standard regimen is 3–4 mg of hemin per kilogram of body weight, infused intravenously once daily for 4 days. Hemin (Panhematin®), Lundbeck Pharmaceu-ticals, is available in the United States as lyophilized hydroxyheme (hematin) for reconstitution with sterile water just before infusion, and it is approved by the FDA for amelioration of acute porphyric attacks. Degra-dation products form rapidly in vitro when this product is reconstituted with sterile water, as recommended in product labeling, and these adhere to endothelial cells, platelets, and coagulation factors and cause a transient anticoagulant effect and often a phlebitis at the site of infusion. With repeated administration, phlebitis can compromise venous access. It is recommended that lyophilized hemin be reconstituted with human albumin to enhance stability (2). Another hemin preparation, heme arginate, is more stable in solution but is not avail-able in the United States.
Reconstitution of lyophilized hydroxyheme with albu-min enhances stability of lyophilized hemin, decreases the incidence of phlebitis, and may enhance efficacy. Other uncommon reported side effects of hemin include fever, aching, malaise, hemolysis, a case of circulatory collapse that resulted in full recovery after subsequent hemin infusions, and one case of transitory renal fail-ure after a dosage of 1000 mg. Experience indicates that hemin can be administered safely during pregnancy.
Patients should be monitored closely during manage-ment of acute attacks for complications and signs of progression of acute porphyria such as electrolyte imbal-ance, acute psychiatric manifestations, muscle weakness, bladder retention, and ileus (2). Spirometry is sometimes indicated daily to detect respiratory impairment at least until the attack begins to resolve. Since patients with respiratory impairment can deteriorate rapidly, it is rec-ommended they be placed in intensive care. ALA and PBG usually fall to normal whether therapy is started early or late, but this does not necessarily predict a clini-cal response.

14 CHAPTER 99 Inherited Porphyrias
Clinical improvement may occur within 1 to 2 days if hemin is started early in an attack. Patients can some-times be discharged from the hospital within several days, although we recommend completion of the stan-dard 4-day treatment course in the outpatient clinic. If initiated late, efficacy of hemin may not be immedi-ately apparent because neuronal damage may already be advanced and slow to recover. In such cases, treatment for longer than 4 days should be considered, although the evidence that this improves the outcome is lack-ing. Hemin is seldom effective for chronic symptoms. Hemin therapy can be given in outpatient settings or in the home, if this facilitates prompt therapy and reduces medical care costs in patients with frequent attacks.
Chronic renal failure has developed in some AIP patients and required renal transplantation. This may be caused by the development of chronic hypertension and prevented by control of blood pressure. AIP also increases the risk of chronic liver disease and especially hepatocellular carcinoma. These tumors seldom increase serum a-fetoprotein levels. Therefore, periodic screening by ultrasound or another hepatic imaging technique is recommended.
99.4.3.7.3 Transplantation. An allogeneic liver transplant was performed on a 19-year-old female AIP heterozygote who had 37 acute attacks in the 29 months prior to transplantation. Posttransplantation, her elevated urinary ALA and BPG levels returned to normal in 24 hours, and she did not experience acute neurologic attacks for more than 18 months posttrans-plant (76). Two AIP patients had combined liver and kidney transplants secondary to uncontrolled acute por-phyria attacks, chronic peripheral neuropathy, and renal failure, requiring dialysis. Both patients had marked improvement with no attacks and normal urinary PBG levels posttransplantation, as well as improvement of their neuropathic manifestations (83). It should be noted that liver transplantation is a high-risk procedure and should not be considered as an established treat-ment for acute porphyrias. Recently, liver-directed gene therapy has been proven successful in the prevention of drug-induced biochemical attacks in a murine model of human AIP (84).99.4.3.8 Prevention of Acute Attacks and Later Complications. Prevention of future attacks requires identifying precipitating factors. Educating the patient to avoid alcohol, smoking, and drugs that can induce exac-erbations (see Table 99–4) is important, as in maintain-ing adequate nutrition. Lists of safe and harmful drugs are available (see previous discussion for references) but these are not infallible. Medical alert bracelets and wal-let cards can help notify emergency medical personnel and ensure that unsafe drugs are not given to patients in emergencies. Some patients have frequent attacks even after exacerbating factors are removed, possibly because of unidentified modifier genes or environmental or endogenous precipitating factors. These patients should
be evaluated by a nutritionist and follow a well-balanced diet with sufficient calories to maintain weight.
Gonadotropin-releasing hormone (GnRH) analogues can be highly effective for women with frequent cyclic attacks when symptoms are confined to the luteal phase of the menstrual cycle (1). The low-dose estrogen patch has been successful in reducing side effects when treat-ment beyond six months is contemplated. Gynecologi-cal examinations and bone density determinations are advised every 6 months during treatment. Continued need can be assessed every 1 to 2 years by stopping the treatment.
Pregnancy increases levels of progesterone, a potent inducer of heme biosynthesis in the liver but nevertheless is well tolerated in most women with acute porphyria. For example, in a large series of women with AIP or VP who had 176 deliveries, porphyric symptoms were absent in 92% of their pregnancies (85). Because some women experience more frequent attacks during preg-nancy, counseling women who wish to become pregnant must be individualized.
Recurrent noncyclic attacks are sometimes prevented by weekly or biweekly infusions of single doses of hemin (3–4 mg/kg). Frequent treatment with hemin has a the-oretic risk of iron overload (100 mg of hemin contains 8 mg of iron); therefore, serum ferritin levels should be monitored. In selected rare instances of severe, unremit-ting symptomatic disease, consideration might be given to orthotopic liver transplantation (76). Transplantation of hepatocytes or specific gene replacement therapy is a possible future therapeutic strategy.
99.4.4 Congenital Erythropoietic Porphyria
Congenital erythropoietic porphyria (CEP), also known as Günther disease, is an autosomal recessive disorder due to the markedly deficient activity of URO-synthase, the forth enzyme in the heme biosynthetic pathway. CEP is panethnic, and as of 2000, about 160 cases were reported (28,86).99.4.4.1 Biochemical Aspects. The deficient activity of URO-synthase is the enzymatic defect in CEP. Affected homozygotes have markedly deficient, but not absent, URO-synthase activity, as sufficient enzyme is required to produce uroporphyrinogen III for normal (or even increased) rates of heme production. Most CEP patients have less than 10% of normal erythrocyte URO-synthase activity. The deficient URO-synthase activity leads to the accumulation of the substrate, hydroxymethylbilane (HMB), most of which is converted nonenzymatically to uroporphyrinogen I. Although uroporphyrinogen I can undergo decarboxylation by URO-decarboxylase to form hepta-, hexa- and pentacarboxyl porphyrinogen I and finally coproporphyrinogen I, further metabolism cannot proceed because the next enzyme in the pathway, COPRO-oxidase, is stereospecific for the III isomer.

CHAPTER 99 Inherited Porphyrias 15
Therefore, the isomer I porphyrins are nonphysiologic, in that they cannot be metabolized to heme, and are pathogenic when they accumulate in large amounts and undergo auto-oxidizidation to their corresponding por-phyrins. In patients with CEP, the large amounts of iso-mer I porphyrinogens that accumulate in bone marrow erythroid precursors (especially normoblasts and reticu-locytes) and erythrocytes undergo auto-oxidation to the corresponding porphyrins, which damage erythrocytes, cause cutaneous photosensitivity, are deposited in tissues and bones, and are excreted in large amounts in the urine and feces.99.4.4.2 Molecular Aspects. The isolation and char-acterization of the URO-synthase cDNA and genomic sequences have permitted the identification of muta-tions in CEP patients (26,28,87). Over 39 mutations have been detected in unrelated CEP families including missense and nonsense mutations, large and small dele-tions and insertions, splicing defects, intronic branch point mutations, and erythroid-specific promoter muta-tions (6). Most mutations have been detected in only one or a few unrelated families, except for C73R, which has been found in about 33% of the alleles studied, L4F in 7%, and T228M in 6% (28). The recent discovery of alternative housekeeping and erythroid-specific pro-moters in the human URO-synthase gene facilitated the identification of four-point mutations within a 20-bp region of the erythroid-specific promoter in six unre-lated CEP probands (26,88). These mutations included a −70T to C transition altering a GATA-1 binding ele-ment, a −76 G to A transition, a −86C to A transversion in three unrelated patients, and a −90C to A trans-version that altered a putative CP2 binding element. These four pathogenic erythroid promoter mutations impaired erythroid-specific transcription, caused CEP, and identified functionally important GATA1 and CP2 transcriptional binding elements for erythroid-specific heme biosynthesis. To date, these are the only known promoter mutations in the erythropoietic porphyrias. For a review of URO-synthase mutations causing CEP, see (6,28).
Genotype–phenotype correlations are possible in CEP once a patient’s mutations are known. Prokaryotic expression and gene promoter-reporter systems have been used to determine the in vitro levels of enzymatic activity expressed by the missense mutations and the promoter function of mutations in the erythroid-specific promoter. The prokaryotic expression of URO-synthase constructs containing missense mutations resulted in levels of enzymatic activity that ranged from essen-tially nondetectable to about 35% of the mean activity expressed by the wild-type allele in E. coli. The effect of the four promoter mutations on transcription also was assessed in vitro by determining the luciferase activity of each lesion using promoter-reporter gene constructs in uninduced and induced (with hemin) K562 erythroleu-kemia cells (88).
For genotype–phenotype correlations, a series of CEP patients were classified as very mild to severely affected, based on age, degree of hemolytic anemia, organomegaly, osteopenia, and cutaneous involvement (28). Homoallel-ism for the most common allele, C73R, was correlated with the most severe phenotype, nonimmune hydrops fetalis and/or transfusion dependency from birth. Con-sistent with the severe phenotype of C73R/C73R homo-zygotes, expression of the C73R allele in E. coli resulted in the detection of less than 1% of the activity expressed by the wild-type allele. The fact that the C73R/C73R homozygotes are viable and do not die early in fetal life indicates that the mutant enzyme retains a very small amount of residual activity that is sufficient to produce enough heme for the biosynthesis of hemoglobin and other essential hemoproteins. Alternatively, if the C73R mutation produced only nonfunctional or barely func-tional enzyme, then the fact that affected fetuses survive suggests the possibility of another gene that is respon-sible for URO-synthase activity during development. However, knockout mice homozygous for a null muta-tion in the URO-synthase gene died early in embryogen-esis, indicating that the total deficiency of URO-synthase activity was an embryonic lethal (89).
Patients heteroallelic for C73R and another muta-tion that expressed little residual activity, such as P53L, also resulted in a severe or moderately severe phenotype. Patients heteroallelic for mutations that expressed more residual activity such as A104V (7.7% of normal activ-ity), A66V (14.5% of normal activity), and V82F (35% of normal activity) had milder forms of CEP, even if the other allele was C73R or another mutation that did not express detectable activity (e.g. nonsense and frameshift mutations). For example, a teenage boy whose genotype was C73R/A66V had only mild cutaneous involvement. Genotype–phenotype correlations for CEP probands with erythroid promoter mutations also have been made (88). For example, a proband heterozygous for a pro-moter mutation with low activity (–70C) and for C73R had the severe nonimmune hydrops fetalis phenotype, while a proband with the C73R mutation in one allele but with a promoter mutation with more activity (–76A) in the other allele had a mild cutaneous disease pheno-type (88). As additional mutations are identified and expressed, more information will become available to evaluate genotype/phenotype correlations.
Affected fetuses can be detected in utero by deter-mining the uroporphyrin I levels in amniotic fluid, the URO-synthase activity in cultured amniotic fluid cells or chorionic villi, and/or by molecular analysis in families where the URO-synthase mutation(s) has been identified (90), or by a combination of these methods (91).99.4.4.3 Clinical Manifestations. The age at onset and clinical severity of CEP are highly variable, ranging from nonimmune hydrops fetalis due to severe hemolytic anemia in utero to milder, later-onset forms that have only cutaneous lesions in adult life (28,87). At least some

16 CHAPTER 99 Inherited Porphyrias
of the late onset cases have been associated with myelo-proliferative disorders, in which a clone of erythroid cells caries expresses URO-synthase deficiency (66). A num-ber of factors are responsible for the phenotypic variabil-ity including (i) the amount of residual URO-synthase activity, (ii) the degree of hemolysis and consequent stimulation of erythropoiesis, and (iii) exposure to UV light. Therefore, as in other porphyrias, an interplay of environmental factors with the deficient enzyme activ-ity determines the clinical expression of disease. Life expectancy may be diminished in more severely affected patients owing to the hematologic complications and the increased risk of infection (28).
The major debilitating clinical features of CEP are photosensitivity and anemia. Severe cutaneous photo-sensitivity begins in early infancy and is manifested by increased friability and blistering of the epidermis on the hands and face and other sun-exposed areas. Skin mani-festations resemble those of PCT, but with the much higher levels of porphyrins in plasma are usually much more severe. Bullae and vesicles contain serous fluid and are prone to rupture and infection. The skin may be thickened, with areas of hypo- and hyperpigmenta-tion. Hypertrichosis of the face and extremities is often prominent. Recurrent vesicles and secondary infection can lead to cutaneous scarring and deformities, as well as to loss of digits and facial features such as eyelids, nose, and ears. Corneal scarring can lead to blindness. Porphyrins deposited in the teeth produce red fluores-cence on exposure to long-wavelength UV light and a reddish-brown color in natural light, termed erythrodon-tia. Bone demineralization may result from expansion of the hyperplastic bone marrow and associated porphyrin deposition in bone (1,92).
Hemolysis is accompanied by anisocytosis, poikilo-cytosis, polychromasia, basophilic stippling, reticulo-cytosis, increased nucleated red cells, decreased serum haptoglobin, increased unconjugated bilirubin, increased fecal urobilinogen, and increased plasma iron turnover, and probably results from the accumulated porphyrins in erythrocytes. Development of secondary splenomegaly may contribute further to the anemia and may also result in leukopenia and thrombocytopenia. The latter is some-times associated with significant bleeding, and in such cases, splenectomy may be beneficial. Hemolytic anemia is especially severe if the bone marrow does not compen-sate, and some patients are transfusion dependent. For example, CEP-genotype C73R/C73R usually presents in utero with hemolysis and nonimmune hydrops, which if recognized can be treated by intrauterine transfusions.
To better understand the pathophysiology and for studying treatment modalities, mouse models of CEP using knock-in techniques have been developed in which the mice have low URO-synthase activity and clinical symptoms, including erythrodontia, characteristic light-induced cutaneous involvement, hepatosplenomegaly, and hemolytic anemia (93,94).
99.4.4.4 Laboratory Evaluation. CEP should be sus-pected as a cause of nonimmune hydrops and in infants or young children with severe photosensitivity and mark-edly increased urinary and plasma porphyrins. Reddish urine in the diaper shortly after birth is often the first sug-gestion of this disease. Milder cases of CEP may be devel-oped later in life in the presence of a myeloproliferative disorder and resemble PCT. Accumulation of isomer I porphyrins, especially uroporphyrin I and coproporphy-rin I in bone marrow, erythrocytes, plasma, and urine is the biochemical hallmark of the disease. Urinary por-phyrins are primarily uroporphyrin I and coproporphy-rin I, the intermediate 7–, 6–, and 5–carboxyl porphyrins being excreted in excess as well. Although there is a great predominance of type I isomers, type III isomers are also increased. Protoporphyrin IX is sometimes the predomi-nant porphyrin in erythrocytes in CEP, as in other auto-somal recessive porphyrias. Urinary ALA and PBG are not increased. Fecal porphyrins are markedly increased, with a predominance of coproporphyrin I.
URO-synthase activity can be measured in erythro-cytes and cultured cells using either direct or coupled enzyme assays (95). CEP should be differentiated from other porphyrias with cutaneous photosensitivity. For example, HEP often mimics CEP clinically but is the homozygous dominant form of URO-decarboxylase deficiency. HEP is distinguishable from CEP by por-phyrin patterns resembling PCT, including high levels of isocoproporphyrin in feces and urine and markedly decreased URO-decarboxylase activity in erythrocytes. Very rare homozygous forms of VP and HCP also may be characterized by photosensitivity in childhood and increased erythrocyte porphyrins.99.4.4.5 Treatment. Skin Protection. Protection of the skin from sunlight and minor trauma is essential. Sun-screen lotions and b-carotene are sometimes beneficial. Bacterial infections that complicate cutaneous blisters require timely treatment in an effort to prevent scarring and mutilation. Severe infections such as cellulitis and bacteremia may require intravenous antibiotics.
99.4.4.5.1 Marrow Suppression. Frequent blood transfusions are sometimes essential for severe anemia. Transfusions repeated frequently enough to suppress erythropoiesis, and thereby decrease porphyrin pro-duction, can greatly reduce porphyrin levels and pho-tosensitivity. Such therapy is likely to be successful if the hematocrit remains above 35% and deferoxamine is administered to reduce the resulting iron overload. Treatment with hydroxyurea to reduce the bone mar-row porphyrin synthesis may be considered, especially after puberty when porphyrin production may increase (96). Splenectomy has substantially reduced transfu-sion requirements in some patients. Oral charcoal has increased fecal loss of porphyrins with milder disease, but seems less successful in more severe cases (97). Hemin therapy, which is effective for the treatment of the acute hepatic porphyrias, may be somewhat effective in CEP

CHAPTER 99 Inherited Porphyrias 17
but has not been extensively studied. Chloroquine has not been beneficial.
99.4.4.5.2 Bone Marrow Transplantation. Bone marrow transplantation (BMT) has proved curative for patients with CEP. To date, nine transplanted patients have been reported, and when successful, BMT has resulted in marked reduction in porphyrin levels and photosensitivity (for reviews, see (98,99)). The source of the hematopoietic stem cells has included bone marrow or umbilical cord blood from histocompatible sibs as well as from unrelated HLA-matched marrow.
99.4.4.5.3 Experimental Gene Therapy. The suc-cess of BMT provides the rationale for hematopoietic stem cell gene therapy. The stable transduction of the patient’s own stem cells with vectors containing the URO-synthase cDNA would abrogate the need for HLA-identical donors and the risk of rejection. Various retroviral and lentiviral vectors expressing human URO-synthase have been used to transduce a variety of cell types including mononuclear cells derived from the bone marrow of normal and CEP subjects (100–106). Better transduction efficiencies were obtained with the lentivi-ral vectors than the retroviral vectors and all transduced cell types had increased URO-synthase activity and sup-pression of porphyrin accumulation. These studies are encouraging; however, in vivo efficacy of individual vec-tor constructs may not be predictable from these in vitro experiments, and animal studies are needed. Such in vivo experiments could determine whether transduction of hematopoietic stem cells can be efficient enough to minimize the proportion of nontransduced progenitors capable of producing toxic quantities of porphyrins in their descendants.
99.4.5 Porphyria Cutanea Tarda
Porphyria cutanea tarda (PCT) is caused by reduced activity of URO-decarboxylase, the fifth enzyme in the heme biosynthetic pathway. PCT is unique among the porphyrias as this cutaneous and biochemical phenotype results from an acquired, liver-specific enzyme inhibition in both sporadic (type I) and familial (types II and III) forms (1,34,107). PCT is the most common porphyria and has an estimated frequency of 1 per 25,000, of which ~80% have type I disease (34,107). This porphyria can also result from exposure to certain polyhalogenated aromatic hydrocarbons. The most notable occurrence of environmentally induced PCT was an outbreak in Turkey in the 1950s, caused by the ingestion of wheat treated with the fungicide hexachlorobenzene (HCB).99.4.5.1 Biochemical Aspects.
99.4.5.1.1 Types I–III PCT Are Clinically Very Similar. The enzymatic activity of hepatic URO- decarboxylase must be decreased by ~75% before porphyrins accumulate and clinical symptoms occur (34,107). However, the amount of hepatic URO-decarboxylase enzyme protein is not decreased below
its genetically determined level but is inhibited by a substance, not yet characterized, derived from a heme pathway intermediate (107). Production of the URO-decarboxylase inhibitor is iron-dependent. The multiple factors that can precipitate types I–III PCT act mostly be increasing hepatic iron content or oxidative stress (see later discussion). The genetically determined level of URO-decarboxylase in type II PCT is half-normal in all tissues, and the disease becomes manifested only when the hepatic enzyme becomes further reduced.
99.4.5.1.2 Type I Porphyria Cutanea Tarda. In type I PCT, URO-decarboxylase activity is deficient in the liver and is normal in all other tissues such as eryth-rocytes. No URO-decarboxylase mutations have been identified in type I PCT. Moreover, there are no tissue-specific isoenzymes of URO-decarboxylase, and there-fore, a mutation of the gene for this enzyme is unlikely to lead to a tissue-specific enzymatic deficiency. The tissue-specific enzymatic deficiency in type I PCT appears to be acquired because the amount of hepatic URO-decarbox-ylase protein, as measured immunochemically, is normal, suggesting that the enzyme has been inhibited, and with phlebotomy the enzyme activity gradually increases and both catalytic and specific activity may return to normal (108). URO-decarboxylase activity is not directly inhib-ited by iron. Considerable evidence suggests that type I PCT is caused by inhibition or inactivation of struc-turally normal URO-decarboxylase by a liver-specific, iron-dependent process that promotes the oxidation of uroporphyrinogen to uroporphyrin and a product that inhibits URO-decarboxylase. Efforts to isolate and char-acterize this inhibitor are currently in progress using lab-oratory models (107).
99.4.5.1.3 Type II Porphyria Cutanea Tarda. In type II or familial PCT, the genetically determined level of URO-decarboxylase activity in all tissues is half-normal due to the autosomal dominant inheritance of a URO-decarboxylase mutation. The half-normal amount of enzymatic activity is the product of the normal URO-decarboxylase allele. Half-normal enzyme protein and activity is demonstrated in nonhepatic tissues such as erythrocytes and cultured skin fibroblasts in clinically affected individuals and in family members with latent disease. However, manifest type II PCT develops only when hepatic URO-decarboxylase becomes reduced con-siderably below the inherited enzyme level, and to lev-els of activity corresponding to type I PCT (107). The amount of hepatic enzyme protein remains half-normal in type II PCT.
URO-decarboxylase is not a rate-limiting enzyme for heme biosynthesis, and therefore most type II heterozy-gotes do not develop PCT unless precipitating factors are present (see later discussion) (107,109).
99.4.5.1.4 Type III Porphyria Cutanea Tarda. Type III PCT is rare and is presumed to be inherited because more than one family member is affected. How-ever, it resembles type I in that URO-decarboxylase

18 CHAPTER 99 Inherited Porphyrias
activity is normal in extrahepatic tissues such as erythro-cytes and URO-decarboxylase mutations have not been identified (108). Therefore, the genetic basis for this type of PCT is not yet understood, and it is not readily dif-ferentiated from type I.
99.4.5.1.5 Hepatoerythropoietic Porphyria. Hepatoerythropoietic porphyria (HEP) is the homo-zygous dominant form of type II PCT. This disease is rare, as only about 30 cases from 24 families have been reported (110). The URO-decarboxylase mutations causing HEP often do not lead to complete loss of the enzyme activity, and some are CRIM-positive (29,111). The URO-decaboxylase activity in HEP patients has ranged from 3% to 28% of normal (29).99.4.5.2 Genetic and Molecular Aspects. URO-decarboxylase gene mutations are found only in type II PCT, as well as HEP. However, in types I and III PCT, other genetic as well as environmental factors (see later discussion) appear to contribute to the reduction of hepatic URO-decarboxylase in liver that is necessary for development of the clinically manifested disease.
The half-normal activity of URO-decarboxylase in type II PCT is clearly inherited as an autosomal dominant trait. Over 100 mutations in the URO-decarboxylase gene have been identified, including over 50 mutations underlying type II PCT, and ten different missense muta-tions causing HEP (Human Gene Mutation Database; www.hgmd.org) (6). The ten mutations in the URO-decarboxylase gene identified in HEP include five such as G281E (112) that also have been found in type II PCT (29,31,110,113–116). HEP patients are either homoal-lelelic or heteroallelic for the URO-decarboxylase mutations.
Of the URO-decarboxylase mutations listed in the Human Gene Mutation Database (6), 57.4% are mis-sense, 0.7% nonsense, and 13.1% are splice-site muta-tions. Most URO-decarboxylase mutations have been identified in only one or two families. Exceptions include mutations g10insA (found in six Argentinean families) (111), G281E (found in 14 unrelated Spanish families) (112), and IVS6+1 (found in 6 unrelated families).
Type III PCT has been studied in four Spanish fami-lies, in which at least two relatives had clinical manifesta-tions of PCT with decreased URO-decarboxylase activity in liver but normal levels in erythrocytes and other tis-sues. To date, no mutations of the URO-decarboxylase locus have been detected in type III PCT.99.4.5.3 Precipitating Factors. A number of inherited and environmental factors contribute to the profound inhibition of hepatic URO-decarboxylase activity and the development of clinically manifested PCT. In type II PCT, the inheritance of a heterozygous URO- decarboxylase mutation predisposes to the disease because the amount of enzyme is half-normal initially, and less inhibitor is required to develop overt PCT (107). Other inherited susceptibility factors include HFE mutations (C282Y and H63D) that increase iron retention, and possibly
polymorphisms of cytochrome P450 enzymes (117). Environmental and infectious factors include excess alcohol consumption, hepatitis C virus infection, HIV infection, estrogen use, smoking, decreased levels of antioxidants such as vitamins E and C, and carot-enoids (3,107,108,118). These appear to contribute to development of PCT by increasing oxidative stress in hepatocytes and the production of an inhibitor of URO- decarboxylase. Multiple factors are present and may act in an additive fashion in the individual PCT patient (119). A study of 84 Swedish patients with PCT found that 23% of the patients had Type II PCT and 57% had hemochro-matosis mutations, 14% of whom were homozygous for the C282Y mutation. Other risk factors included alco-hol abuse (38% of males), estrogen treatment (55% of females), and antihepatitis C virus (29% of males) (120).
Mutations in the hemochromatosis (HFE) gene may result in elevated tissue iron levels and therefore predis-pose to PCT. There are two common mutations causing hemochromatosis: the C282Y mutation causes hemo-chromatosis in homozygotes in northern Europeans and their descendents, and the H63D mutation, which is more common in southern Europe. One in ten normal individuals is a carrier of a HFE gene mutation and an increased frequency occurs in both sporatic and familial PCT patients (107,108,121). In American PCT patients, 63% to 73% had HFE mutations (119,122,123); in one series, 17 of 87 (19%) PCT patients were homozy-gous for C282Y compared with zero for the 56 controls (123). Among English PCT patients, 17% were found to be homozygous for the C282Y mutation and 20% were heterozygous (124). A review of eight studies (121) found a mutant hemachromatosis allele in 17% to 47% of patients with sporadic or familial PCT suggesting that the HFE gene is an important predispositional modifier gene for the clinical expression of PCT (121).99.4.5.4 Porphyria Cutanea Tarda due to Haloge-nated Hydrocarbons. In 1955 to 1958, an extensive outbreak of PCT occurred in eastern Turkey as a result of the ingestion of wheat treated with the fungicide HCB (1,108). Feeding of HCB to animals was subsequently shown to decrease hepatic URO-decarboxylase activity and to produce a porphyria biochemically similar to human PCT. Smaller case clusters have also been reported after exposure to other chemicals, including di- and trichlorophenols and 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD, dioxin) (108).99.4.5.5 Clinical Manifestations. Skin lesions consist of fluid-filled vesicles and bullae on sun-exposed areas such as the dorsa of the hands and feet, the face, fore-arms, and legs. These may rupture, form crusted lesions, and heal slowly with residual scarring. Secondary infec-tion may occur. Sun-exposed skin becomes friable, and minor trauma may precede the formation of bullae or may cause denudation of the skin. Small white plaques, termed milia, may precede or follow vesicle formation. Other cutaneous manifestations include hypertrichosis

and hyperpigmentation, especially of the face, which can present in the absence of vesicles. Thickening, scarring, and calcification of affected areas of skin are sometimes striking and has been termed pseudoscleroderma because it resembles the cutaneous changes of systemic sclerosis. The skin lesions in PCT are generally indistinguishable from those in VP and HCP.
PCT is commonly associated with evidence of chronic liver disease and sometimes with cirrhosis. Patients with PCT are also at risk to develop hepatocellular carcinoma; in several series, the incidence has ranged from 4% to 47%. These tumors appear as a complication of PCT and do not themselves contain or produce porphyrins in large amounts. They may result from longstanding liver damage in PCT, hemosiderosis, coexistent chronic hepa-titis C infection, exposure to halogenated chemicals that are also carcinogenic, or to the effects of porphyrin depo-sition in the liver. PCT associated with advanced renal disease is often more severe and intractable than PCT occurring in its absence (1).
HEP resembles CEP clinically and usually presents in infancy or childhood with onset of blistering skin lesions, hypertrichosis, scarring, and red urine. HEP is genetically heterogeneous, and unusually mild cases have been described (125). Two mild cases of HEP with only minor scarring have recently been described in two unre-lated patients, one in a 5-year-old boy and the other in a 38-year-old man (110,126). Interestingly, both patients were homoallelic for the same mutation F46L, which resulted in less than 10% of normal URO-decarboxylase activity in these patients.99.4.5.6 Laboratory Evaluation. PCT is strongly sug-gested by the characteristic skin lesions in sun-exposed areas, especially on the backs of the hands. However, similar skin blistering is seen with other cutaneous por-phyrias, with the exception of EPP. The most useful initial diagnostic test is a total plasma porphyrin deter-mination. A normal plasma porphyrin level excludes PCT, whereas a high level with a fluorescence emission maximum at neutral pH near 619 nm excludes VP and is highly suggestive of PCT (108). Measurements of urinary and fecal porphyrins provide confirmation of PCT. URO-decarboxylase activity can be measured in erythrocytes and lymphoblasts (89) and can be used to distinguish Types I and II since Type 1 PCT patients will have normal levels of erythrocyte URO-decarboxylase, while Type II PCT patients will have ~50% of normal levels (15). Molecular analysis more reliably diagno-ses type II patients by identifying the underlying URO-decarboxylase gene mutations (127).
Porphyrins are increased in the liver, plasma, urine, and stool in PCT (63). A slight increase in ALA is noted in some patients, but PBG excretion is nor-mal. Urinary porphyrins consist mostly of uroporphy-rin and 7-carboxyl porphyrin, with lesser amounts of coproporphyrin and 5- and 6-carboxyl porphyrins. The excess urinary uroporphyrin in PCT is predominantly
CHAPTER 99 Inherited Porphyrias 19
isomer I; 7- and 6-carboxyl porphyrins are mostly iso-mer III; and 5-carboxyl porphyrin and coproporphyrin are approximately equal mixtures of isomers I and III.
The finding of increased isocoproporphyrins, most readily demonstrated in feces, is diagnostic for a defi-ciency of URO-decarboxylase (34). These unusual 4-carboxyl porphyrins are produced when hepatic URO-decarboxylase is deficient, because 5-carboxyl porphyrin-ogen III, which accumulates in PCT, can be metabolized by COPRO-oxidase to yield dehydroisocoproporphy-rinogen. This porphyrinogen is excreted in bile and undergoes auto-oxidation and side-chain modification by bacterial enzymes in the intestine to give isocopropor-phyrin and deethylisocoproporphyrin, the major repre-sentatives of the isocoproporphyrin series in the feces of PCT patients. Increased liver porphyrins are composed mostly of uroporphyrin and 7-carboxyl porphyrin.
The biochemical findings in HEP are similar to those in other forms of PCT. In addition, the concentration of protoporphyrin in erythrocytes is increased and is pre-dominantly zinc protoporphyrin.99.4.5.7 Therapy. The diagnosis of PCT should be firmly established by biochemical investigations before treatment is initiated, because VP and HCP can produce similar cutaneous lesions but are unresponsive to mea-sures that are highly effective in PCT. Imaging studies are advisable to exclude complicating hepatocellular car-cinoma and to serve as a baseline for follow-up. Test-ing for known precipitating factors is recommended to include hepatitis C and HIV infections. Patients should abstain from alcohol, estrogens, iron supplements, or other exogenous agents that may exacerbate the disease. Drugs such as barbiturates, phenytoin, and sulfonamides that are harmful to patients with acute porphyrias are seldom reported to contribute to the clinical expression of PCT, but should be avoided as a precaution.
Standard therapy consists of repeated phlebotomy, which can produce remission in almost all patients (1). The aim is to gradually reduce excess hepatic iron by removing about 450 mL of blood at intervals of 1 to 2 weeks until the serum ferritin reaches the lower limits of normal (108). Plasma (or serum) porphyrin levels decrease in parallel and become normal within 1 to 2 months after the target ferritin concentration is achieved. Hemoglobin or hematocrit levels should be followed closely to prevent the development of symptomatic ane-mia. Continued phlebotomies are seldom needed even if ferritin levels later return to normal. However, it is advisable to follow porphyrin levels and reinstitute phle-botomies if porphyrin levels begin to rise. Even cutane-ous scarring and pseudoscleroderma can improve with phlebotomy and serum markers for the liver cell function to normalize (108). Recombinant erythropoietin is an effective treatment and can support phlebotomy therapy when PCT is associated with end-stage renal disease (1).
Small doses of chloroquine (125 mg twice weekly) or hydroxychloroquine (100 mg twice weekly) are also

20 CHAPTER 99 Inherited Porphyrias
effective in producing remissions of PCT (127). These drugs promote excretion of accumulated porphyrins in the liver in PCT, possibly by complexing with porphy-rins. However, the standard antimalarial doses of these drugs may induce acute hepatic damage, nausea, vomit-ing and fever, and elevated urinary and plasma porphy-rin levels due to the release of large amounts of stored porphyrins from the liver (1). There may be a transient increase in photosensitivity. Such side effects are mini-mal or absent with much lower doses. This treatment is sometimes combined with repeated phlebotomy (108). Prospective study comparing these two forms of therapy is lacking.
99.4.6 Hereditary Coproporphyria
Hereditary coproporphyria (HCP) is an acute hepatic porphyria and results from the deficient activity of COPRO-oxidase, the sixth enzyme in the heme biosyn-thetic pathway. HCP is inherited as an autosomal domi-nant trait due to COPRO-oxidase mutations, whose clinical expression is influenced by ecogenic and meta-bolic factors. This condition is less frequent than AIP or VP (40). Clinical symptoms rarely occur before puberty and are very similar to AIP with the exception of photo-sensitivity, which can develop in HCP patients but much more rarely than in VP (1). Certain mutations in the COPRO-oxidase gene, such as K404E, when present in either the homozygous or compound heterozygous states produce a biochemical variant called harderoporphyria, characterized by increased fecal levels of a tricarboxylic porphyrin, harderoporphyrin (41,129). Cases of homo-zygous HCP have also been reported (42,43).99.4.6.1 Biochemical Aspects. The activity of the mitochondrial enzyme COPRO-oxidase is about 50% of normal in cultured fibroblasts, circulating lympho-cytes, and leukocytes from HCP heterozygotes. In one case of homozygous HCP, the residual COPRO-oxidase activity (approximately 2% of normal) had a normal Km value. By contrast, in three cases in a family with har-deroporphyria, the mutant enzyme exhibited increased thermostability and reduced affinity for both hardero-porphyrinogen and coproporphyrinogen III, which is consistent with a structurally altered enzyme.99.4.6.2 Molecular Aspects. Over 40 mutations in the COPRO-oxidase gene are listed in the Human Gene Mutation Database, including missense, nonsense, splice-site, and small insertion or deletion mutations (Human Gene Mutation Database; www.hgmd.org) (6,130). Most have been identified in only one family (40). In a study of 17 unrelated British HCP patients, only one mutation, 1277GÆA, which causes exon 6 skipping was found in more than one patient (131). No genotype–phenotype correlations have been observed in HCP (131). Five single nucleotide polymorphisms were identified in the COPRO-oxidase gene, but none appear to play a major role in clinical expression of HCP (132).
Studies of the human COPRO-oxidase crystal structure and a hydrophobic cluster analysis method indicated that only missense mutations in amino acids positions 400–404 in exon 6 resulted in harderoporphyria. In fact, mutation K404E is found either homoallelic or heteroallelic in all patients with harderoporphyria stud-ied, to date. The amino acids in this region appear to be involved in retaining harderoporphyrinogen for the second decarboxylation step whereas mutations in these amino acids lead to the release of the porphyrinogen intermediate (39,41).99.4.6.3 Clinical Manifestations. The neurovisceral symptoms of HCP are identical to those of AIP; however, the disease is probably less severe than AIP, and only a few patients have been reported to die from respiratory paralysis. Photosensitivity similar to that in PCT and VP sometimes occurs. In one series of 50 patients, the most common clinical manifestations were abdominal pain (80%), vomiting (34%), skin lesions (29%), neuro-pathic involvement (23%), psychiatric symptoms (23%), and constipation (20%) (40). In a study of 53 German HCP patients during acute manifestations, 89% had abdominal pain, 33% had neurologic symptoms, 28% had psychiatric symptoms, and 25% had cardiovascular symptoms, while only skin photosensitivity was observed in only 5% (114). In 69% of these patients, the abdomi-nal pain occurred without other neurologic manifesta-tions, while 27% of the patients had both abdominal and other neurologic symptoms; 4% had only neuro-logic symptoms (114). HCP can be exacerbated by many of the same factors that cause attacks in AIP, including drugs such as barbiturates and endogenous or exogenous steroid hormones. The disease is latent before puberty, and symptoms are more common in adult women than in men. Hepatitis and other superimposed liver diseases in an HCP patient can increase porphyrin retention and photosensitivity.
Patients with homozygous HCP, including some with harderoporphyria, developed symptoms in early child-hood. Manifestations have included jaundice, severe hemolytic anemia with splenomegaly, and compensatory hyperactive bone marrow (43,133).99.4.6.4 Laboratory Evaluation. A common and characteristic biochemical change in HCP is a large, iso-lated increase in fecal coproporphyrin, predominantly isomer III (40). Feces of symptomatic heterozygotes have a 10-fold to 200-fold increase in coproporphyrins and little or no increase in protoporphyrin. An increase in the ratio of coproporphyrin III to coproporphyrin I in feces is useful for diagnosis of both active and latent HCP. Increased urinary excretion of ALA, PBG, and total por-phyrins (mostly uroporphyrin III and coproporphyrin III) is observed during acute attacks (114).
With resolution of symptoms, ALA and PBG levels revert to normal more readily in HCP (and VP) than in AIP, and HCP patients in nonacute stages may show only increases of urinary and fecal porphyrins. For

CHAPTER 99 Inherited Porphyrias 21
example, in a series of 53 German HCP patients, the average total urinary porphyrins during acute phases was 29,905 nmol/24 hr (6 patients) and around 1100 nmol/24 hr during subclinical and latent phases (aver-age of 47 patients); normal levels were <224 nmol/24 hr (113). Total fecal porphyrins were 5508 nmol/g dry weight at active stages of HCP, compared with 1730 and 694 nmol/g dry weight (normal <224 nmol/g dry weight) in subclinical and latent phases, respectively. However, the percentage of the fecal coproporphyrin III isomer was still elevated in the patients in the subclinical and latent phases (114).
Porphyrin excretion patterns in homozygous HCP resemble those observed in heterozygotes but reflect a more profound enzymatic deficiency. Harderoporphyria is characterized by a marked increase in fecal excretion of harderoporphyrin as well as coproporphyrin. In one patient with harderoporphyria, 90% of the porphyrins in his feces were in the form of harderoporphyrin (129).
COPRO-oxidase activity can be measured in mono-nuclear cells (134). Individuals with a mutation in one of their COPRO-oxidase alleles have about 50% of nor-mal activity in mononuclear cells. For screening family members, measurement of fecal porphyrins may be use-ful, especially if the ratio of coproporphyrin isomers I and III is determined; however, asymptomatic adults and children with the enzymatic deficiency may not excrete excess porphyrins.99.4.6.5 Therapy. Acute attacks of HCP are treated in the same manner as in AIP (2). Hemin (lyophilized hydroxyheme or heme arginate) therapy is helpful in treating acute attacks of HCP (40). Cholestyramine may be of some value for photosensitivity occurring with liver dysfunction, but phlebotomy and chloroquine are not effective.
99.4.7 Variegate Porphyria
VP is an autosomal dominant hepatic porphyria result-ing from the deficient activity of PROTO-oxidase, the seventh enzyme in the heme biosynthetic pathway. The disorder is described as variegate because it can pres-ent with neurologic manifestations, photosensitivity, or both. The clinical penetrance of VP in adults is esti-mated at ~40% (135–137). In most countries, VP is less common than AIP, with the notable exception of South Africa, where 3 of every 1000 white persons have inher-ited VP. This high prevalence is due to a founder effect from a Dutch couple who immigrated to South Africa in 1688, one of whom carried a specific PROTO-oxidase mutation (133). A number of cases of homozygous dom-inant VP have also been described (49,50,138–141).99.4.7.1 Biochemical Aspects. PROTO-oxidase activity is approximately half-normal in cultured skin fibroblasts and lymphocytes from VP patients. Because PROTO-oxidase is a mitochrondrial enzyme, it is not present in mature erythrocytes. Assays for
PROTO-oxidase in lymphocytes or cultured cells are dif-ficult and are not widely available for diagnosis and fam-ily screening (136).
Protoporphyrinogen IX, the substrate for PROTO-oxidase, accumulates in patients with VP and undergoes auto-oxidation to protoporphyrin IX, which is charac-teristically increased in VP. A close functional associa-tion between PROTO-oxidase in the inner mitochondrial membrane and COPRO-oxidase in the intermembrane space may relate to the excess excretion of both proto-porphyrin IX and coproporphyrin III in this disease.99.4.7.2 Molecular Aspects. Around 150 muta-tions in the PROTO-oxidase gene have been identified in patients with VP including missense, nonsense, splice site, and small deletions and insertions (Human Gene Mutation Database; www.hgmd.org) (6,136). The mis-sense mutation, R59W, is the common mutation in most South Africans with VP of Dutch descent (133). In 108 unrelated English and French VP patients, 66 mutations were identified; most were found in only one or two unre-lated families, but five (L15F, E198X, L295P, 1082insC, and Q435X) had frequencies of 7% to 12% (142). No genotype/phenotype correlations were identified. In 21 Finnish VP families, the common missense mutation R152C was identified in 11 (52%), while the missense mutation I12T was found in two large families (9.5%) (137). Of interest, none of the patients with the I12T muta-tion had photosensitivity, only one had an acute attack, and all had lower levels of porphyrins than patients with mutation R152C (137). Mutations have also been iden-tified in patients with the rarer homozygous dominant form of VP (48,49,138–141). Most have some residual enzymatic activity, allowing for synthesis of heme in amounts sufficient for many essential hemoproteins.99.4.7.3 Clinical Manifestations. Clinical expression of VP before puberty is rare; the disease may even pres-ent late in life (143). VP can present with skin photo-sensitivity, acute neurovisceral crises, or both (47). In two large studies of VP patients from Europe and South Africa, 59% had only skin lesions, 20% had only acute attacks, and 22% had both (142). Among Finnish VP patients, the frequency of skin symptoms was 40% and acute attacks 27% (137). Interestingly, the proportion of Finnish patients with acute attacks decreased from 38% to 14% among patients diagnosed before and after 1980, while the proportion with skin symptoms remained simi-lar. The reasons for the decline in symptoms are unclear (137). A similar decline in the frequency of acute attacks, from 38% before 1980 to 4% in 2004, was observed among South African VP patients, presumably due to increased detection and counseling of heterozygotes to avoid use of acute attack-inducing drugs, steroids, and dieting (135).
The neurovisceral manifestations of abdominal pain, vomiting, constipation, hypertension and tachycardia, and peripheral neuropathy are indistinguishable from those of AIP and HCP. Skin manifestations are very

22 CHAPTER 99 Inherited Porphyrias
similar to those of PCT and HCP, are usually of lon-ger duration, and may occur apart from the neurovis-ceral symptoms. Photosensitivity is more common than in HCP. Drugs, steroids, and nutritional factors that are detrimental in AIP can also provoke exacerbations of VP (1,2). Photosensitivity may be less commonly associated with VP in more northern countries, where sunlight is less intense (136).
Patients with homozygous dominant VP have the early onset of symptoms, severe photosensitivity, absence of acute attacks, and elevated erythrocyte zinc protopor-phyrin levels (49). In some cases, neurologic symptoms and developmental disturbances, including growth retar-dation, were noted in infancy or childhood. One homo-zygous VP patient had severe photosensitivity and mild sensory neuropathy and over a 20-year period developed IgA nephropathy (48). The heterozygous parents of these patients had approximately half-normal enzyme activity as expected.99.4.7.4 Laboratory Evaluation. Fecal protoporphy-rin and coproporphyrin and urinary coproporphyrin are markedly increased in clinically expressed VP. Urinary and fecal coproporphyrin is mostly type III. Urinary ALA, PBG, and uroporphyrins are increased during acute attacks but may be normal or only slightly increased dur-ing remission. ALA and PBG may be less elevated and return to normal more rapidly in VP and HCP than in AIP. Plasma porphyrins, consisting in part of a dicar-boxylate porphyrin tightly bound to plasma proteins, are increased in VP particularly when photosensitivity or other symptoms are present. The fluorescence emission spectrum of plasma porphyrins at neutral pH in VP is characteristic and can distinguish this disease from other types of porphyria, especially PCT: the emission maxima occurs at 626 nm in VP; 619 nm in PCT, CEP, HCP, and AIP; and 634 nm in EPP (63). This method of measuring plasma porphyrins is perhaps the most sensitive method of detecting latent cases of VP, other than measuring PROTO-oxidase in lymphocytes or detecting a specific mutation by molecular methods. VP can be distinguished from HCP by fecal and plasma porphyrin analyses.
Assays for PROTO-oxidase are difficult, since the enzyme is not present in erythrocytes and are not widely available for diagnostic and family screening (63). Muta-tion analysis is preferred for confirming the diagnosis and detecting heterozygous relatives.99.4.7.5 Therapy. Glucose, hemin, and other mea-sures employed in AIP are recommended for the treat-ment of acute attacks of VP (2,47,136). Other therapies such as propranolol, d-penicillamine, hemodialysis, alkalization of urine, and b-carotene are of little or no benefit. Repeated venesections and chloroquine are not effective for skin manifestations in VP, even though these appear identical to those of PCT. Measures to protect the skin from sunlight with appropriate clothing and opaque sunscreen preparations are useful. Exposure to short-wavelength UV light, which does not excite
porphyrins, may provide some protection by increasing skin pigmentation.
99.4.8 Erythropoietic Protoporphyria
Erythropoietic protoporphyria (EPP) is due to the par-tially deficient activity of ferrochelatase, the last enzyme in the heme biosynthetic pathway (1,57). EPP also has been termed erythrohepatic protoporphyria and proto-porphyria. EPP is the most common erythropoietic por-phyria and, after PCT and AIP, is the third most common porphyria. EPP is an autosomal dominant disease in most affected families. However, many EPP patients had only 10% to 30% of normal ferrochelatase activity instead of the expected 50% of normal activity. Recently, it was shown that an intronic polymorphism in the wild-type allele reduces its expression, accounting for the lower level of enzymatic activity. EPP is therefore an autoso-mal dominant porphyria in which a low-expression poly-morphism predisposes to clinical expression (penetrance) (134). The presence of the intronic polymorphism and the nature of the other mutation (e.g. null vs. missense) may be responsible in part for the penetrance and vari-able expressivity of this disease. In some families, the pat-tern of inheritance is autosomal recessive, with affected individuals inheriting a coding region mutation from each parent (144). Although the disease is most common in whites, it does occur in persons of other races, includ-ing blacks. The low expression polymorphism is found in ~10% of the normal white population and is also com-mon in Asians but is rare in Africans (58). Recently, dele-tions in exon 11 of the ALAS2 gene have been described, which cause an X-linked protoporphyria (XLP) which is clinically indistinguishable from EPP. The deletion of the c-terminal amino acids of ALSA2 results in increased ALAS2 activity and the accumalation of protoporphyrin (145). XLP accounts for approximately 2% of cases with the EPP phenotype (146).99.4.8.1 Biochemical Aspects. Partially deficient ferrochelatase has been documented in bone marrow, reticulocytes, liver, cultured fibroblasts, and blood or leukocytes from patients with EPP (1). The deficient enzyme activity becomes rate-limiting for protoporphy-rin conversion to heme primarily in bone marrow reticu-locytes. Ferrochelatase activity in tissue lysates of EPP patients has been reported to be as low as 10% to 30% of normal, which is much less than the 50% of normal activity that would be expected if EPP were inherited as an autosomal dominant enzymopathy. In a study of French and Swiss EPP patients, ferrochelatase activity ranged from 15% to 50% of normal (147). In a recently described variant form of EPP, ferrochelatase activity was normal, and an abnormality in iron delivery to the normal enzyme was postulated (148).99.4.8.2 Molecular Aspects. To date, over 100 mutations in the ferrochelatase gene have been identi-fied that cause EPP (Human Gene Mutation Database;

CHAPTER 99 Inherited Porphyrias 23
www.hgmd.org) (6,147) including nonsense, missense, splice-site mutations, nonsense, and insertions/deletions or rearrangement mutations. Based on the type of muta-tion, about 75% of lesions result in an unstable or absent protein (null alleles). It has been suggested that there are genotype–phenotype correlations between mutations that result in unstable proteins (null) and liver compli-cations in EPP patients. A study of 112 EPP patients with known ferrochelatase mutations found that all 18 EPP patients with severe liver complications had “null” alleles, while none of the 20 patients who had missense mutations developed liver complications (149). Another study of 31 EPP patients found that all 15 EPP patients with liver disease had null mutations (splicing, nonsense, or frameshift mutations), while 50% of the 16 patients who had only photosensitivity had missense mutations (150,151).
Mutation analysis of 105 English EPP patients iden-tified three typical EPP patients with homozygous EPP, having two different mutations and one who was homoal-lelic for a missense mutation (152). The phenotypes of these homozygous EPP patients were very similar to EPP patients with one disabling mutation and the low expres-sion intron 3 polymorphism, but their low ferrochela-tase activity increased their risk for liver disease (152). In XLP, the erythrocyte protoporphyrin levels appear to be higher than other forms of EPP, and the proportions of free and zinc protoporphyrins are approximately equal.99.4.8.3 Genetic Aspects. As noted previously, many EPP patients have about 20% to 30% of normal ferro-chelatase activity rather than the 50% expected if the EPP was inherited as a simple autosomal dominant trait. Recent studies have shown that the presence of a poly-morphism in intron 3 of the normal ferrochelatase allele affects the level of ferrochelatase activity and the sever-ity of EPP. When the normal allele has a C at position -48 of intron 3, a cryptic acceptor splice site is activated, resulting in the insertion of 63 bp of the intron into the coding sequence (134). The IVS3-48C mRNA transcript contains a new stop codon and is rapidly degraded. The IVS3-48C polymorphism was present in ~10% of nor-mal European individuals, 43% of normal Japanese, 31% of normal southeast Asians, and <1% of normal black West Africans (58,134,152). Transfection studies showed that the IVS3-48C construct produced ~40% aberrantly spliced mRNAs, while the common IVS3-48T construct produced only 20% aberrantly spliced mRNAs (134).
In studies of 40 unrelated European and 31 American symptomatic EPP patients, 95% (38 of 40) and 94% (29 of 31), respectively, had the IVS3-48C allele (132,150). Of note, none of 12 asymptomatic individuals with fer-rochelatase mutations had the IVS3-48C allele (151). Additional studies of 113 overt French EPP patients and 61 asymptomatic carriers showed that none of the asymptomatic carriers had the IVS3-48C allele while 93 of 95 overt patients did (58). The EPP patients with the
IVS3-48C allele had lower levels of ferrochelatase activ-ity than individuals with the IVS3-48T allele. These stud-ies and others (150,153–155) indicate that symptomatic disease in most EPP patients is the result of a mutation in one ferrochelatase allele that alters markedly the struc-ture, stability, and activity of the enzyme protein and a low expressing normal ferrochelatase allele, which is caused by the presence of the IVS3-48C polymorphism. Therefore, it appears that in most families the presence or absence of the IVS3-48C allele determines which indi-viduals will be symptomatic.
In patients who do not have the IVS-48C polymor-phism, it is possible that their reduced ferrochela-tase activities result from the fact that the enzyme is a homodimer, and the dimerization of mutant and wild-type polypeptides may reduce the total activity. Recent studies of recombinant human wild-type and mutant ferrochelatase, expressed in E. coli, confirmed that fer-rochelatase functions as a dimer and indicated that, for some mutations, the dimeric enzymes containing only mutant or mutant and wild-type heterodimers may be unstable or have markedly reduced activity (50,156).
Mouse models of EPP (157,158) may help further clarify the lower than expected ferrochelatase activity in EPP patients. In these models, the different genetic backgrounds or the absence of the heme-regulated eIF2a kinase (HRI) can effect the clinical severity of EPP (157,159). In XLP, to date, only two ALAS2 mutations, all deletions of 1 to 4 bases, have been described, which markedly increase ALAS2 activity (145).99.4.8.4 Etiology and Pathogenesis. Porphyrins absorb light maximally at wavelengths near 400 nm (the Soret band) and enter an excited energy state that is man-ifested by fluorescence and, in the presence of molecular oxygen, by the formation of singlet oxygen and other oxygen species that can produce tissue damage. As might be expected, the skin is maximally sensitive to 400-nm light in EPP. Light-induced tissue damage may be accom-panied by lipid peroxidation, oxidation of amino acids, and crosslinking of proteins in cell membranes. Histo-logic changes, predominantly in the upper dermis, may include amorphous material deposited around blood ves-sels and may resemble the findings in PCT. Immediate light-induced damage to capillary endothelial cells in the upper dermis has been described in EPP.
Circulating erythrocytes are an insufficient source for the excess protoporphyrin produced and excreted in EPP, and the presence of brightly fluorescent imma-ture erythroid cells in the bone marrow of EPP patients presumably is a major source of the excess protopor-phyrin (57). The liver also may be a source for some of the accumulated protoporphyrin (108); however, the relative contribution of hepatic and erythroid sources of the excess protoporphyrins is unclear. Studies in an EPP mouse model showed that bone marrow cells from a wild-type animal when transplanted into an irradiated EPP animal corrected the photosensitivity and fatal liver

24 CHAPTER 99 Inherited Porphyrias
disease, suggesting that the bone marrow was the major site for the excess protoporphyrins (160). In the reverse experiment, transplanting EPP bone marrow cells into irradiated normal mice resulted in protoporphyria (38% of erythrocytes contained flurorescent protoporphyrins), but not in liver disease, suggesting that the absence of ferrochelatase activity in the liver is a necessary com-ponent for development of EPP-associated liver disease (161). The normal recipients of EPP bone marrow cells also showed minimal skin photosensitivity despite high levels of plasma and erythrocyte protoporphyrins, sug-gesting that normal ferrochelatase activity in skin pre-vented photosensitivity (161).
Free protoporphyrin in EPP binds less readily to hemo-globin than does zinc protoporphyrin and diffuses more rapidly into the plasma. Moreover, UV light may cause free protoporphyrin to photodamage its hemoglobin-binding site and thus be released from the erythrocytes, even without disruption of the cell membrane. Protoporphy-rin may then diffuse into the plasma, where it is bound to albumin. This light-mediated mechanism for the release of free protoporphyrin from hemoglobin in EPP may be important because binding of excess free protoporphyrin to hemoglobin is usually greater than binding to plasma proteins. Most of the protoporphyrin in erythrocytes is found in a small percentage of cells, and the rate of pro-toporphyrin leakage from these cells is proportional to their protoporphyrin concentration. The capacity of the liver to take up and excrete protoporphyrin into bile may also influence the flux of protoporphyrin from erythroid cells to the plasma.
In uncomplicated cases, hemolysis is uncommon or very mild. However, mild anemia with hypochromia and microcytosis or mild anemia with reticulocytosis is sometimes noted (144). Depletion of iron stores may be relatively common even in the absence of iron-deficiency anemia in EPP. Iron accumulation in erythroblasts and ring sideroblasts occur in some EPP patients.
Patients with EPP have high concentrations of pro-toporphyrin in bile and seem predisposed to develop gallstones that are fluorescent and composed at least in part of protoporphyrin. Protoporphyrin is cholestatic when infused intravenously in rodents. The potentially life-threatening hepatic complications of EPP are often preceded by increasing levels of erythrocyte and plasma protoporphyrin, abnormal liver function tests, and marked deposition of protoporphyrin in liver cells and bile canaliculi.99.4.8.5 Clinical Manifestations. A major clinical feature of EPP is cutaneous photosensitivity, which usu-ally begins in childhood. Photosensitivity is associated with substantial elevations in erythrocyte protoporphy-rin and occurs only in patients with a genotype that results in ferrochelatase activity below ~35% of normal (3,108). Protoporphyrin levels remain quite constant over time, although cutaneous symptoms are gener-ally more troublesome in the spring and summer when
sunlight exposure is greatest. Burning, itching, erythema, and swelling are the most common symptoms and can occur within minutes of sun exposure. Even brief expo-sure to the sun may result in intense skin pain lasting for hours, which has been described like “having a lighted match held against the skin or hot needles stuck into it” (108). Edema of the skin may be diffuse and resem-ble angioneurotic edema. Burning, itching, and intense pain can occur without obvious skin damage. Vesicles and bullae are absent or sparse. Epidermal intracellular vacuoles and interstitial edema are seen in fresh lesions, accompanied by acute inflammatory changes and extrav-asated red cells (57). Some residual scarring from vesicles or severe swelling may occur, but this is rarely severe or deforming. Pigment changes, friability, and hirsutism also are not characteristic of EPP. Thus, the cutaneous features of this disease are distinct from those of other cutaneous porphyrias. Also, in contrast to CEP, there is no discoloration or fluorescence of the teeth. It is also notable that neuropathic manifestations are not found in EPP, except rarely with advanced liver failure.
Although this is an erythropoietic porphyria, the hepatic complications that develop in a small percent-age of patients (probably less than 5%) are most life threatening. Liver function is usually normal in this disease, but up to 20% of patients may have minor abnormalities of liver function. In XLP, about 17% of patients had overt liver disease, suggesting that the risk of liver disease may be higher with XLP than classic EPP (145). Rapidly progressive liver disease appears to be related to the cholestatic effects of protoporphyrin and is associated with increasing protoporphyrin levels due to impaired hepatobiliary excretion and increased photosensitivity (144). Splenic enlargement and hemo-lysis may be accompanying features. Upper abdominal pain may suggest biliary obstruction (57). Concurrent factors impairing liver function or the metabolism of protoporphyrin to heme, such as viral hepatitis, alco-hol, iron deficiency, and fasting or oral contracep-tive steroids, have played a role in some patients. An enterohepatic circulation of protoporphyrin may favor its retention in the liver, especially when liver function is impaired. Liver biopsies of EPP patients with severe liver disease contain dark brown pigment with a typical birefringence under polarized light. This pigment is pro-toporphyrin, which has been deposited in hepatocytes, macrophages, bile canaliculi, and small bile ducts. For a detailed discussion of the hepatic complications of EPP, see Cox (144) and Thunell and coworkers (162).99.4.8.6 Clinical and Laboratory Evaluation. EPP should be suspected in individuals with intense skin pain after short exposure to the sun without blistering skin lesions (144). A lack of severe cutaneous signs distin-guishes this disease from all other cutaneous porphyrias. Protoporphyrin concentrations are increased in the bone marrow, circulating erythrocytes, plasma, bile, and feces of EPP patients.

CHAPTER 99 Inherited Porphyrias 25
A substantial increase in erythrocyte protoporphy-rin concentration, which is a readily obtained measure-ment, is essential for diagnosis of EPP. Erythrocytes also exhibit red fluorescence when studied by fluorescence microscopy at 620 nm (163). However, an increased erythrocyte protoporphyrin concentration is not specific to EPP. Erythrocyte protoporphyrin concentrations are increased in other conditions such as lead poisoning, iron deficiency, anemia of chronic disease, and various hemolytic disorders, and also in all homozygous forms of porphyria and sometimes in acute porphyrias. How-ever, the increased protoporphyrin in conditions other than EPP is in the form of zinc protoporphyrin, whereas in EPP it is free protoporphyrin (not complexed with zinc). Many assays for erythrocyte protoporphyrin or “free erythrocyte protoporphyrin” measure both the zinc-chelated and the free protoporphyrin. Free proto-porphyrin is distinguished from zinc protoporphyrin by ethanol extraction or HPLC (144). In XLP, both free and zinc protoporphyrins are increased in equal proportions.
Plasma porphyrins may be less increased in EPP than in other porphyrias with cutaneous manifestations (1). Other heme pathway intermediates do not accumulate in EPP. Thus, urinary porphyrin and porphyrin pre-cursor concentrations are generally normal. Fecal total porphyrins may be normal or somewhat elevated. Life-threatening hepatic complications of EPP are commonly preceded by increased photosensitivity and by increasing erythrocyte and plasma protoporphyrin levels. The ratio of erythrocyte to fecal protoporphyrin and the ratio of biliary protoporphyrin to biliary bile acids may also be observed to increase as liver failure develops. Ferroche-latase is a mitochondrial enzyme and can be measured in lymphocytes isolated from peripheral blood. As men-tioned previously, EPP patients may have only around 20% to 30% of normal activity. Mutation analysis can be used to identify mutations and polymorphisms in the ferrochelatase gene.
A high prevalence of Vitamin D deficiency has been observed in EPP patients (164) and measurement of Vita-min D 25 OH levels would be recommended for moni-toring these patients.99.4.8.7 Treatment. Photosensitivity is managed by avoiding excessive sunlight and long-wave UV light. b-carotene was developed as a drug for treating EPP (162) and may improve tolerance to sunlight. Doses of 120 to 180 mg daily in adults are usually required to maintain serum carotene levels in the recommended range of 600–800 mg/dL. Improvement is noted 1–3 months after the initiation of treatment. With pure preparations of b-carotene, no side effects other than a mild and dose-related skin discoloration due to caro-tenemia have been noted. The mechanism of action may involve quenching of singlet oxygen or free radicals. The drug appears less effective in other forms of porphyria associated with photosensitivity, such as CEP and PCT. Dihydroxyacetone and lawsone (naphthoquinone),
which darken the skin when applied topically, partially block exposure of the dermis to light and are of some benefit in EPP. Cholestyramine, which may interrupt the enterohepatic circulation of protoporphyrin and promote its fecal excretion, has been reported to reduce liver protoporphyrin and improve cutaneous symptoms in some EPP patients. Increasing skin pigmentation by exposure to short-wave UV light may also offer some protection. Caloric restriction, drugs and hormone preparations that exacerbate acute porphyrias are often avoided in EPP, and iron deficiency should be corrected if present. Vitamin D should be supplemented if deficient.
Treatment of hepatic complications is difficult and must be individualized. Cholestyramine and other por-phyrin absorbents, such as activated charcoal, should be considered. Oral bile acid supplementation has shown benefit in some animal models but has been little stud-ied in EPP patients. Resolution of hepatic complications may also occur spontaneously, especially if another reversible cause of liver dysfunction, such as viral hep-atitis or alcohol, is contributing. Splenectomy may be beneficial when EPP is complicated by hemolysis and splenomegaly. Other therapeutic options include trans-fusions and intravenous hemin to suppress erythroid and hepatic protoporphyrin production, as well as liver transplantation. However, liver disease may recur after transplantation (165).
99.4.9 Dual Porphyrias
Patients with deficiencies of more than one heme bio-synthetic enzyme are classified as having dual porphyria. For example, kindreds with individuals having both VP and familial PCT have been described. Patients with defi-ciencies of both HMB-synthase and URO-decarboxylase may develop symptoms of AIP, PCT, or both. COPRO-oxidase deficiency inherited from one parent and URO-synthase deficiency from both parents was found to cause severe porphyria in an infant. Coexistence of URO- synthase and URO-decarboxylase deficiencies has been described in a patient with features of an erythropoietic porphyria (166). Mutation analysis was not performed on these patients to confirm that the patient actually has mutations in two different genes. This is important, as shown by studies of a patient initially thought to have both VP and AIP but who was found to have a PROTO-oxidase mutation but no HMB-synthase mutation (167). A patient with both sporadic PCT and HCP due to an inherited COPRO-oxidase mutation was identified based on the urinary porphyrin pattern (168). Recently, ALA-dehydratase and COPRO-oxidase gene mutations were confirmed in one patient (169), and HMB-synthase and URO-decarboxylase gene mutations in another (170), as predicted by biochemical findings. These are the first two cases of dual porphyria where mutations in two different genes have been identified.

26 CHAPTER 99 Inherited Porphyrias
ACKNOWLEDGMENTS
This was supported in part by grants from the National Institutes of Health (NIH) including research grants (5 R21 DK073093 and 5 R01 DK026824), a grant (1 U54 DK083909) for the Porphyrias Consortium of the NIH Rare Diseases Clinical Research Network (RDCRN), that includes funding and/or programmatic support from the NIH Office of Rare Disease
Research (ORDR), and a General Clinical Research Center grant (MO1-RR000073) and a Clinical and Translational Science Award (UL1 RR029876-01), both from the National Center for Research Resources, and by a grant from the US Food and Drug Administration Office of Orphan Product Development (R01FD002604).
CHAPTERS TO CROSS-REFERENCE
2. Medicine in a Genetic Context; 3. Nature and Fre-quency of Genetic Disease; 7. Mutations in Human Disease: Nature and Consequences; 8. Mendelian Inher-tiance; 14. Pathogenetics of Disease; 23. Diagnostic Molecular Genetics; 24. Heterozygote Testing and Car-rier Screening; 29. Gene Therapy.
FURTHER READING
1. Anderson, K. E.; Sassa, S.; Bishop, D. F.; Desnick, R. J. Dis-orders of Heme Biosynthesis: X-Linked Sideroblastic Ane-mias and the Porphyrias. In The Metabolic and Molecular Basis of Inherited Disease, 8th ed.; Scriver, C. R.; Beaudet, A. L.; Sly, W. S.; Valle, D., Eds.; McGraw-Hill: New York, 2001; pp 2991–3062.
2. Anderson, K. E.; Bloomer, J. E.; Bonkovsky, H. L.; Kushner, J.; Pierach, C.; Pimstone, N.; Desnick, R. J. Recommendations for the Diagnosis and Treatment of the Acute Porphyrias. Ann. Intern. Med. 2005, 142, 439–450.
3. Badminton, M. N.; Elder, G. H. Molecular Mechanisms of Dominant Expression in Porphyria. J. Inherit. Metab. Dis. 2005, 28, 277–286.
4. Kauppinen, R. Porphyrias. Lancet 2005, 365, 241–252. 5. Schmid, R. The Porphyrias. Semin. Liver. Dis. 1998, 18, 1–101. 6. Stenson, P. D.; Ball, E. V.; Mort, M.; Phillips, A. D.; Shiel, J.
A.; Thomas, N. S.; Abeysinghe, S.; Krawczak, M.; Cooper, D. N. Human Gene Mutation Database (HGMD): 2003 Update. Hum. Mutat. 2003, 21, 577–581.
7. May, B. K.; Dogra, S. C.; Sadlon, T. J.; Bhasker, C. R.; Cox, T. C.; Bottomley, S. S. Molecular Regulation of Heme Biosynthe-sis in Higher Vertebrates. Prog. Nucleic. Acid. Res. Mol. Biol. 1995, 51, 1–51.
8. Cotter, P. D.; Rucknagel, D. L.; Bishop, D. F. X-Linked Sid-eroblastic Anemia: Identification of the Mutation in the Ery-throid-Specific d-Aminolevulinate Synthase Gene (ALAS2) in the Original Family Described by Cooley. Blood 1994, 84, 3915–3924.
9. Bekri, S.; May, A.; Cotter, P. D.; Al-Sabah, A. I.; Guo, X.; Mas-ters, G. S.; Bishop, D. F. A Promoter Mutation in the Erythroid-Specific 5-Aminolevulinate Synthase (ALAS2) Gene Causes X-linked Sideroblastic Anemia. Blood 2003, 102, 698–704.
10. Shoolingin-Jordan, P. M.; Al-Daihan, S.; Alexeev, D.; Bax-ter, R. L.; Bottomley, S. S.; Kahari, I. D.; Roy, I.; Sarwar, M.; Sawyer, L.; Wang, S. F. 5-Aminolevulinic Acid Synthase:
Mechanism, Mutations and Medicine. Biochim. Biophys. Acta. 2003, 1647, 361.
11. Kaya, A. H.; Plewinska, M.; Wong, D. M.; Desnick, R. J.; Wet-mur, J. G. Human d-Aminolevulinate Dehydratase (ALAD) Gene: Structure and Alternative Splicing of the Erythroid and Housekeeping mRNAs. Genomics 1994, 19, 242–248.
12. Doss, M. O.; Stauch, T.; Gross, U.; Renz, M.; Akagi, R.; Doss-Frank, M.; Seelig, H. P.; Sassa, S. The Third Case of Doss Por-phyria (Delta-Amino Levulinic Acid Dehydratase Deficiency)in Germany. J. Inherit. Metab. Dis. 2004, 27, 529–536.
13. Sassa, S. ALAD Porphyria. Semin. Liver. Dis. 1998, 18, 95–101. 14. Akagi, R.; Kato, N.; Inoue, R.; Anderson, K. E.; Jaffe, E. K.;
Sassa, S. Delta-Aminolevulinate Dehydratase (ALAD) Por-phyria: The First Case in North America with Two Novel ALAD Mutations. Mol. Genet. Metab. 2006, 87, 329–336.
15. Schwartz, B. S.; Lee, B. K.; Sewart, W.; Ahn, K. D.; Springer, K.; Kelsey, K. Associations of Delta-Aminolevulinic Acid Dehydratase Genotype with Plant, Exposure Duration, and Blood Lead and Zinc Protopophyrin Levels in Korean Lead Workers. Am. J. Epidemol. 1995, 142, 738–745.
16. Alexander, B. H.; Checkoway, H.; Costa-Mallen, P.; Faust-man, E. M.; Woods, J. S.; Kelsey, K. T.; van Netten, C.; Costa, L. G. Interaction of Blood Lead and Delta-Aminolevulinic Acid Dehydratase Genotype on Markers of Heme Synthesis and Sperm Production in Lead Smelter Workers. Environ. Health. Perspect. 1998, 106, 213–216.
17. Fleming, D. E.; Chettle, D. R.; Wetmur, J. G.; Desnick, R. J.; Robin, J. P.; Boulay, D.; Richard, N. S.; Gordon, C. L.; Webber, C. E. Effect of the Delta-Aminolevulinate Dehydra-tase Polymorphism on the Accumulation of Lead in Bone and Blood in Lead Smelter Workers. Environ. Res. 1998, 77, 49–61.
18. Hu, H.; Wu, M. T.; Cheng, Y.; Sparrow, D.; Weiss, S.; Kelsey, K. The Delta-Aminolevulinic Acid Dehydratase (ALAD) Poly-morphism and Bone and Blood Lead Levels in Community-Exposed Men: The Normative Aging Study. Environ. Health. Perspect. 2001, 109, 827–832.
19. Sithisarankul, P.; Schwartz, B. S.; Lee, B. K.; Kelsey, K. T.; Strick-land, P. T. Aminolevulinic Acid Dehydratase Genotype Medi-ates Plasma Levels of the Neurotoxin, 5-Aminolevulinic Acid, in Lead-Exposed Workers. Am. J. Ind. Med. 1997, 32, 15–20.
20. Wetmur, J. G. Influence of the Common Human d-Aminolev-ulinate Dehydratase Polymorphism on Lead Body Burden. Environ. Health. Perspect. 1994, 102 (Suppl. 3), 215–219.
21. Anderson, P. M.; Reddy, R. M.; Anderson, K. E.; Desnick, R. J. Characterization of the PBG-Deaminase Deficiency in Acute Intermittent Porphyria. I. Immunologic Evidence for Hetero-geneity of the Genetic Defect. J. Clin. Invest. 1981, 68, 1–12.
22. Shoolingin-Jordan, P. M.; Al-Dbass, A.; McNeill, L. A.; Sarwar, M.; Butler, D. Human Porphobilinogen Deaminase Mutations in the Investigation of the Mechanism of Dipyr-romethane Cofactor Assembly and Tetrapyrrole Formation. Biochem. Soc. Trans. 2003, 31, 731–735.
23. Grandchamp, B. Acute Intermittent Porphyria. Semin. Liver. Dis. 1998, 18, 17–24.
24. Brownlie, P. D.; Lambert, R.; Louie, G. V.; Jordan, P. M.; Blundell, T. L.; Warren, M. J.; Cooper, J. B.; Wood, S. P. The Three-Dimensional Structures of Mutants of Porphobilino-gen Deaminase: Toward an Understanding of the Structural Basis of Acute Intermittent Porphyria. Protein. Sci. 1994, 3, 1644–1650.
25. Wood, S.; Lambert, R.; Jordan, M. Molecular Basis of Acute Intermittent Porphyria. Mol. Med. Today 1995, 5, 232–239.
26. Aizencang, G.; Solis, C.; Bishop, D. F.; Warner, C.; Desn-ick, R. J. Human Uroporphyrinogen-III Synthase: Genomic Organization, Alternative Promoters, and Erythroid-Specific Expression. Genomics 2000, 70, 223–231.
27. Mathews, M. A.; Schubert, H. L.; Whitby, F. G.; Alexander, K. J.; Schadick, K.; Bergonia, H. A.; Phillips, J. D.; Hill, C. P.

CHAPTER 99 Inherited Porphyrias 27
Crystal Structure of Human Uroporphyrinogen III Synthase. EMBO. J. 2001, 20, 5832–5839.
28. Desnick, R. J.; Astrin, K. H. Congenital Erythropoietic Por-phyria: Advances in Pathogenesis and Treatment. Br. J. Haematol. 2002, 117, 779–795.
29. Moran-Jimenez, M. J.; Ged, C.; Romana, M.; Enriquez De Salamanca, R.; Taïeb, A.; Topi, G.; D’Alessandro, L.; de Verneuil, H. Uroporphyrinogen Decarboxylase: Complete Human Gene Sequence and Molecular Study of Three Fami-lies with Hepatoerythropoietic Porphyria. Am. J. Hum. Genet. 1996, 58, 712–721.
30. Phillips, J. D.; Whitby, F. G.; Kushner, J. P.; Hill, C. P. Char-acterization and Crystallization of Human Uroporphyrinogen Decarboxylase. Protein. Sci. 1997, 6, 1343–1346.
31. Phillips, J. D.; Parker, T. L.; Schubert, H. L.; Whitby, F. G.; Hill, C. P.; Kushner, J. P. Functional Consequences of Nat-urally Occurring Mutations in Human Uroporphyrinogen Decarboxylase. Blood 2001, 98, 3179–3185.
32. Phillips, J. D.; Whitby, F. G.; Kushner, J. P.; Hill, C. P. Struc-tural Basis for Tetrapyrrole Coordination by Uroporphyrino-gen Decarboxylase. EMBO. J. 2003, 22, 6225–6233.
33. Whitby, F. G.; Phillips, J. D.; Kushner, J. P.; Hill, C. P. Crys-tal Structure of Human Uroporphyrinogen Decarboxylase. EMBO. J. 1998, 17, 2463–2471.
34. Elder, G. H. Porphyria Cutanea Tarda. Semin. Liver. Dis. 1998, 18, 67–70.
35. Medlock, A. E.; Dailey, H. A. Human Coproporphyrinogen Oxidase Is Not a Metalloprotein. J. Biol. Chem. 1996, 271, 32507–32510.
36. Dailey, T. A.; Woodruff, J. H.; Dailey, H. A. Examination of Mitochondrial Protein Targeting of Haem Synthetic Enzymes: In Vivo Identification of Three Functional Haem-Responsive Motifs in 5-Aminolevulinate Synthase. Biochem. J. 2005, 386, 381–386.
37. Delfau-Larue, M. H.; Martasek, P.; Grandchamp, B. Copro-porphyrinogen Oxidase: Gene Organization and Description of a Mutation Leading to Exon 6 Skipping. Hum. Mol. Genet. 1994, 3, 1325–1330.
38. Martasek, P.; Camadro, J. M.; Delfaularue, M. H.; Dumas, J. B.; Montagne, J. J.; de Verneuil, H.; Labbe, P.; Grandchamp, B. Molecular Cloning, Sequencing, and Functional Expression of a cDNA Encoding Human Coproporphyrinogen Oxidase. Proc. Natl. Acad. Sci. U.S.A. 1994, 91, 3024.
39. Lee, D. S.; Flachsova, E.; Bodnarova, M.; Demeler, B.; Martasek, P.; Raman, C. S. Structural Basis of Hereditary Coproporphyria. Proc. Natl. Acad. Sci. U.S.A. 2005, 102, 14232–14237.
40. Martasek, P. Hereditary Coproporphyria. Semin. Liver. Dis. 1998, 18, 25–32.
41. Schmitt, C.; Gouya, L.; Malonova, E.; Lamoril, J.; Camadro, J. M.; Flamme, M.; Rose, C.; Lyoumi, S.; Da Silva, V.; Boi-leau, C., et al. Mutations in Human CPO Gene Predict Clini-cal Expression of Either Hepatic Hereditary Coproporphyria or Erythropoietic Harderoporphyria. Hum. Mol. Genet. 2005, 14, 3089–3098.
42. Doss, M. O.; Gross, U.; Lamoril, J.; Kranl, C.; Jacob, K.; Doss, M.; da Silva, V.; Freesemann, A. G.; Deybach, J. C.; Sepp, N., et al. Compound Heterozygous Hereditary Coproporphyria with Fluorescing Teeth. Ann. Clin. Biochem. 1999, 36, 680–682.
43. Martasek, P.; Nordmann, Y.; Grandchamp, B. Homozygous Hereditary Coproporphyria Caused by an Arginine to Tryp-tophane Substitution in Coproporphyrinogen Oxidase and Common Intragenic Polymorphisms. Hum. Mol. Genet. 1994, 3, 477–480.
44. Dailey, H. A. Purification and Characterization of Membrane Bound Ferrochelatase from Rhodopseudomonas Sphaeroides. J. Biol. Chem. 1982, 257, 14714–14718.
45. Puy, H.; Robreau, A. M.; Rosipal, R.; Nordmann, Y.; Dey-bach, J. C. Protoporphyrinogen Oxidase: Complete Genomic
Sequence and Polymorphisms in the Human Gene. Biochem. Biophys. Res. Commun. 1996, 226, 226–230.
46. Taketani, S.; Inazawa, J.; Abe, T.; Furukawa, T.; Kohno, H.; Tokunaga, R.; Nishimura, K.; Inokuchi, H. The Human Pro-toporphyrinogen Oxidase Gene (PPOX): Organization and Location to Chromosome 1. Genomics 1995, 29, 698–703.
47. Kirsch, R. E.; Meissner, P. N.; Hift, R. J. Variegate Porphyria. Semin. Liver. Dis. 1998, 18, 33–40.
48. Kauppinen, R.; Timonen, K.; von und zu Fraunberg, M.; Laitinen, E.; Ahola, H.; Tenhunen, R.; Taketani, S.; Musta-joki, P. Homozygous Variegate Porphyria: 20 y Follow-Up and Characterization of Molecular Defect. J. Invest. Derma-tol. 2001, 116, 610–613.
49. Palmer, R. A.; Elder, G. H.; Barrett, D. F.; Keohane, S. G. Homozygous Variegate Porphyria: A Compound Heterozy-gote with Novel Mutations in the Protoporphyrinogen Oxi-dase Gene. Br. J. Dermatol. 2001, 144, 866–869.
50. Najahi-Missaoui, W.; Dailey, H. A. Production and Charac-terization of Erythropoietic Protoporphyric Heterodimeric Ferrochelatases. Blood 2005, 106, 1098–1104.
51. Koch, M.; Breithaupt, C.; Kiefersauer, R.; Freigang, J.; Huber, R.; Messerschmidt, A. Crystal Structure of Protoporphyrino-gen IX Oxidase: A Key Enzyme in Haem and Chlorophyll Bio-synthesis. EMBO. J. 2004, 23, 1720–1728.
52. Ferreira, G. C. Mammalian Ferrochelatase: Overexpression in Escherichia Coli as a Soluble Protein, Purification and Char-acterization. J. Biol. Chem. 1994, 269, 4396–4408.
53. Ferreira, G. C.; Franco, R.; Lloyd, S. G.; Pereira, A. S.; Moura, I.; Moura, J. J.; Huynh, B. H. Mammalian Ferrochelatase, A New Addition to the Metalloenzyme Family. J. Biol. Chem. 1994, 269, 7062–7065.
54. Dailey, H. A.; Finnegan, M. G.; Johnson, M. K. Human Ferro-chelatase Is an Iron Sulfur Protein. Biochem. 1994, 33, 403–407.
55. Burden, A. E.; Wu, C.; Dailey, T. A.; Busch, J. L.; Dhawan, I. K.; Rose, J. P.; Wang, B.; Dailey, H. A. Human Ferrochelatase: Crystallization, Characterization of the [2Fe-2S] Cluster and Determination that the Enzyme Is a Homodimer. Biochim. Biophys. Acta. 1999, 1435, 191–197.
56. Wu, C. K.; Dailey, H. A.; Rose, J. P.; Burden, A.; Sellers, V. M.; Wang, B. C. The 2.0 A Structure of Human Ferrochela-tase, the Terminal Enzyme of Heme Biosynthesis. Nat. Struct. Biol. 2001, 8, 156–160.
57. Cox, T. M.; Alexander, G. J.; Sarkany, R. P. Protoporphyria. Semin. Liver. Dis. 1998, 18, 85–93.
58. Gouya, L.; Martin-Schmitt, C.; Robreau, A. M.; Austerlitz, F.; Da Silva, V.; Brun, P.; Simonin, S.; Lyoumi, S.; Grandchamp, B.; Beaumont, C., et al. Contribution of a Common Single-nucleo-tide Polymorphism to the Genetic Predisposition for Erythro-poietic Protoporphyria. Am. J. Hum. Genet. 2006, 78, 2–14.
59. Cable, E. E.; Miller, T. G.; Isom, H. C. Regulation of Heme Metabolism in Rat Hepatocytes and Hepatocyte Cell Lines: Delta-Aminolevulinic Acid Synthase and Heme Oxygenase Are Regulated by Different Heme-Dependent Mechanisms. Arch. Biochem. Biophys. 2000, 384, 280–295.
60. Podvinec, M.; Handschin, C.; Looser, R.; Meyer, U. A. Identification of the Xenosensors Regulating Human 5-Aminolevulinate Synthase. Proc. Natl. Acad. Sci. U.S.A. 2004, 101, 9127–9132.
61. Aizencang, G. I.; Bishop, D. F.; Forrest, D.; Astrin, K. H.; Desnick, R. J. Uroporphyrinogen III Synthase. An Alterna-tive Promoter Controls Erythroid-Specific Expression in the Murine Gene. J. Biol. Chem. 2000, 275, 2295–2304.
62. Ponka, P. Tissue-Specific Regulation of Iron Metabolism and Heme Synthesis: Distinct Control Mechanisms in Erythroid Cells. Blood 1997, 89, 1–25.
63. Bonkovsky, H. L.; Barnard, G. F. Diagnosis of Porphyric Syn-dromes: A Practical Approach in the Era of Molecular Biol-ogy. Semin. Liver. Dis. 1998, 18, 57–65.

28 CHAPTER 99 Inherited Porphyrias
64. Maruno, M.; Furuyama, K.; Akagi, R.; Horie, Y.; Meguro, K.; Garbaczewski, L.; Chiorazzi, N.; Doss, M. O.; Hassoun, A.; Mercelis, R., et al. Highly Heterogeneous Nature of Delta-Aminolevulinate Dehydratase (ALAD) Deficiencies in ALAD Porphyria. Blood 2001, 97, 2972–2978.
65. Akagi, R.; Yasui, Y.; Harper, P.; Sassa, S. A Novel Mutation of Delta-Aminolaevulinate Dehydratase in a Healthy Child with 12% Erythrocyte Enzyme Activity. Br. J. Haematol. 1999, 106, 931–937.
66. Sassa, S.; Akagi, R.; Nishitani, C.; Harigae, H.; Furuyama, K. Late-Onset Porphyrias: What Are They? Cell. Mol. Biol. (Noisy-le-grand). 2002, 48, 97–101.
67. Gross, U.; Sassa, S.; Jacob, K.; Deybach, J. C.; Nordmann, Y.; Frank, M.; Doss, M. O. 5-Aminolevulinic Acid Dehydratase Deficiency Porphyria: A Twenty-Year Clinical and Biochemi-cal Follow-Up. Clin. Chem. 1998, 44, 1892–1896.
68. De Siervi, A.; Mendez, M.; Parera, V. E.; Varela, L.; Batlle, A. M.; Rossetti, M. V. Acute Intermittent Porphyria: Char-acterization of Two Novel Mutations in the Porphobilinogen Deaminase Gene, One Amino Acid Deletion (453-455delAGC) and One Splicing Aceptor Site Mutation (IVS8-1G>T). Hum. Mutat. 1999, 14, 355.
69. von und zu Fraunberg, M.; Pischik, E.; Udd, L.; Kauppinen, R. Clinical and Biochemical Characteristics and Genotype-Phe-notype Correlation in 143 Finnish and Russian Patients with Acute Intermittent Porphyria. Medicine (Baltimore) 2005, 84, 35–47.
70. Chen, C. H.; Astrin, K. H.; Lee, G.; Anderson, K. E.; Desnick, R. J. Acute Intermittent Porphyria: Identification and Expres-sion of Exonic Mutations in the Hydroxymethylbilane Syn-thase Gene: An Initiation Codon Missense Mutation in the Housekeeping Transcript Causes “Variant Acute Intermittent Porphyria” with Normal Expression of the Erythroid-Specific Enzyme. J. Clin. Invest. 1994, 94, 1927–1937.
71. Llewellyn, D. H.; Smyth, S. J.; Elder, G. H.; Hutchesson, A. C.; Rattenbury, J. M.; Smith, M. F. Homozygous Acute Inter-mittent Porphyria: Compound Heterozygosity for Adjacent Base Transitions in the Same Codon of the Porphobilinogen Deaminase Gene. Hum. Genet. 1992, 89, 97–98.
72. Solis, C.; Martinez-Bermejo, A.; Naidich, T. P.; Kaufmann, W. E.; Astrin, K. H.; Bishop, D. F.; Desnick, R. J. Acute Intermit-tent Porphyria: Studies of the Severe Homozygous Dominant Disease Provides Insights into the Neurologic Attacks in Acute Porphyrias. Arch. Neurol. 2004, 61, 1764–1770.
73. Meyer, U. A.; Schuurmans, M. M.; Lindberg, R. L. P. Acute Porphyrias: Pathogenesis of Neurological Manifestations. Semin. Liver. Dis. 1998, 18, 43–52.
74. Lindberg, R. L.; Martini, R.; Baumgartner, M.; Erne, B.; Borg, J.; Zielasek, J.; Ricker, K.; Steck, A.; Toyka, K. V.; Meyer, U. A. Motor Neuropathy in Porphobilinogen Deaminase-Deficient Mice Imitates the Peripheral Neuropa-thy of Human Acute Porphyria. J Clin. Invest. 1999, 103, 1127–1134.
75. Lindberg, R. L.; Porcher, C.; Grandchamp, B.; Ledermann, B.; Bürki, K.; Brandner, S.; Aguzzi, A.; Meyer, U. A. Porphobi-linogen Deaminase Deficiency in Mice Causes a Neuropathy Resembling that of Human Hepatic Porphyria. Nat. Genet. 1996, 12, 195–199.
76. Soonawalla, Z. F.; Orug, T.; Badminton, M. N.; Elder, G. H.; Rhodes, J. M.; Bramhall, S. R.; Elias, E. Liver Transplantation as a Cure for Acute Intermittent Porphyria. Lancet 2004, 363, 705–706.
77. Mustajoki, P.; Heinonen, J. General Anesthesia in “Inducible” Porphyrias. Anesthesiology 1980, 53, 15–20.
78. Handschin, C.; Lin, J.; Rhee, J.; Peyer, A. K.; Chin, S.; Wu, P. H.; Meyer, U. A.; Spiegelman, B. M. Nutritional Regulation of Hepatic Heme Biosynthesis and Porphyria Through PGC-1alpha. Cell 2005, 122, 505–515.
79. Nordmann, Y.; Puy, H. Human Hereditary Hepatic Porphyr-ias. Clin. Chim. Acta. 2002, 325, 17–37.
80. Anderson, K. E. Approaches to Treatment and Prevention of Human Porphyrias. In The Porphyrin Handbook, Medical Aspects of Porphyrins; Kadish, K. M.; Smith, K.; Guilard, R., Eds.; Academic Press: San Diego, 2003; pp 247.
81. Elder, G. H.; Hift, R. J.; Meissner, P. N. The Acute Porphyr-ias. Lancet 1997, 349, 1613–1617.
82. Thadani, H.; Deacon, A.; Peters, T. Diagnosis and Manage-ment of Porphyria. BMJ 2000, 320, 1647–1651.
83. Wahlin, S.; Harper, P.; Sardh, E.; Andersson, C.; Andersson, D. E.; Ericzon, B. G. Combined Liver and Kidney Transplatation in Acute Intermittent Porphyria. Transpl. Int. 2010, 23, e18–e21.
84. Yasuda, M.; Bishop, D. F.; Fowkes, M.; Cheng, S. H.; Gan, L.; Desnick, R. J. AAV8-Mediated Gene Therapy Prevents Induced Biochemical Attacks of Acute Intermittent Porphyria and Improves Neuromotor Function. Mol. Ther. 2010, 18, 17–22.
85. Kauppinen, R.; Mustajoki, P. Prognosis of Acute Porphyria: Occurrence of Acute Attacks, Precipitating Factors, and Asso-ciated Diseases. Medicine (Baltimore) 1992, 71, 1–13.
86. Fritsch, C.; Bolsen, K.; Ruzicka, T.; Goerz, G. Congenital Eryth-ropoietic Porphyria. J. Am. Acad. Dermatol. 1997, 36, 594–610.
87. De Verneuil, H.; Ged, C.; Moreau-Gaudry, F. Congenital Erythropoietic Porphyria. Chapter 87; In Porphyrin Hand-book, Part II; Kadish, K. M.; Smith, K.; Guilard, R., Eds.; Academic Press: San Diego, 2003; pp 43.
88. Solis, C.; Aizencang, G. I.; Astrin, K. H.; Bishop, D. F.; Desn-ick, R. J. Uroporphyrinogen III Synthase Erythroid Promoter Mutations in Adjacent GATA1 and CP2 Elements Cause Con-genital Erythropoietic Porphyria. J. Clin. Invest. 2001, 107, 753–762.
89. Bensidhoum, M.; Larou, M.; Lemeur, M.; Dierich, A.; Costet, P.; Raymond, S.; Daniel, J. Y.; de Verneuil, H.; Ged, C. The Disruption of Mouse Uroporphyrinogen III Synthase (uros) Gene Is Fully Lethal. Transgenics 1998, 2, 275–280.
90. Lazebnik, N.; Lazebnik, R. S. The Prenatal Presentation of Congenital Erythropoietic Porphyria: Report of Two Siblings with Elevated Maternal Serum Alpha-Fetoprotein. Prenat. Diagn. 2004, 24, 282–286.
91. Ged, C.; Moreau-Gaudry, F.; Taine, L.; Hombrados, I.; Calvas, P.; Colombies, P.; De Verneuil, H. Prenatal Diagnosis in Con-genital Erythropoietic Porphyria by Metabolic Measurement and DNA Mutation Analysis. Prenat. Diagn. 1996, 16, 83–86.
92. Laorr, A.; Greenspan, A. Severe Osteopenia in Congenital Erythropoietic Porphyria. Can. Assoc. Radiol. J. 1994, 45, 307–309.
93. Bishop, D. F.; Johansson, A.; Phelps, R.; Shady, A. A.; Ramirez, M. C.; Yasuda, M.; Caro, A.; Desnick, R. J. Uro-porphyrinogen III Synthase Knock-in mice have the Human Congenital Erythropoietic Porphyria Phenotype, Including the Characteristic Light-induced Cutaneous Lesions. Am. J. Hum. Genet. 2006, 78, 645–658.
94. Ged, C.; Mendez, M.; Robert, E.; Lalanne, M.; Lamrissi-Garcia, I.; Costet, P.; Daniel, J. Y.; Dubus, P.; Mazurier, F.; Moreau-Gaudry, F., et al. A Knock-in Mouse Model of Con-genital Erythropoietic Porphyria. Genomics 2006, 87, 84–92.
95. Shoolingin-Jordan, P. M.; Leadbeater, R. Coupled Assay for Uroporphyrinogen III Synthase. Methods Enzymol. 1997, 281, 327–336.
96. Guarini, L.; Piomelli, S.; Poh-Fitzpatrick, M. B. Hydroxyurea in Congenital Erythropoietic Porphyria (letter). N. Engl. J. Med. 1994, 330, 1091–1092.
97. Gorchein, A.; Guo, R.; Lim, C. K.; Raimundo, A.; Pullon, H. W.; Bellingham, A. J. Porphyrins in Urine, Plasma, Erythro-cytes, Bile and Faeces in a Case of Congenital Erythropoietic Porphyria (Gunther’s disease) Treated with Blood Transfu-sion and Iron Chelation: Lack of Benefit from Oral Charcoal. Biomed. Chromatogr. 1998, 12, 350–356.

CHAPTER 99 Inherited Porphyrias 29
98. Dupuis-Girod, S.; Akkari, V.; Ged, C.; Galambrun, C.; Keba-ïli, K.; Deybach, J. C.; Claudy, A.; Geburher, L.; Philippe, N.; de Verneuil, H., et al. Successful Match-Unrelated Donor Bone Marrow Transplantation for Congenital Erythropoi-etic Porphyria (Gunther disease). Eur. J. Pediatr. 2005, 164, 104–107.
99. Shaw, P. H.; Mancini, A. J.; McConnell, J. P.; Brown, D.; Kletzel, M. Treatment of Congenital Erythropoietic Por-phyria in Children by Allogeneic Stem Cell Transplantation: A Case Report and Review of the Literature. Bone Marrow Transplant. 2001, 27, 101–105.
100. Géronimi, F.; Richard, E.; Lamrissi-Garcia, I.; Lalanne, M.; Ged, C.; Redonnet-Vernhet, I.; Moreau-Gaudry, F.; de Ver-neuil, H. Lentivirus-mediated Gene Transfer of Uroporphy-rinogen III Synthase Fully Corrects the Porphyric Phenotype in Human Cells. J. Mol. Med. 2003, 81, 310–320.
101. Kauppinen, R.; Glass, I. A.; Aizencang, G.; Astrin, K. H.; Atweh, G. F.; Desnick, R. J. Congenital Erythropoietic Por-phyria: Prolonged High-level Expression and Correction of the Heme Biosynthetic Defect by Retroviral-Mediated Gene Transfer into Porphyric and Erythroid Cells. Mol. Genet. Metab. 1998, 65, 10–17.
102. Mazurier, F.; Géronimi, F.; Lamrissi-Garcia, I.; Morel, C.; Richard, E.; Ged, C.; Fontanellas, A.; Moreau-Gaudry, F.; Morey, M.; de Verneuil, H. Correction of Deficient cd34(+) Cells from Peripheral Blood after Mobilization in a Patient with Congenital Erythropoietic Porphyria. Mol. Ther. 2001, 3, 411–417.
103. Mazurier, F.; Moreau-Gaudry, F.; Salesse, S.; Barbot, C.; Ged, C.; Reiffers, J.; de Verneuil, H. Gene Transfer of the Uroporphyrinogen III Synthase cDNA into Haematopoi-etic Progenitor Cells in View of a Future Gene Therapy in Congenital Erythropoietic Porphyria. J. Inherit. Metab. Dis. 1997, 20, 247–257.
104. Moreau-Gaudry, F.; Barbot, C.; Mazurier, F.; Mahon, F. X.; Reiffers, J.; Ged, C.; de Verneuil, H. Correction of the Enzyme Deficit of Bone Marrow Cells in Congenital Eryth-ropoietic Porphyria by Retroviral Gene Transfer. Hematol. Cell. Ther. 1996, 38, 217–220.
105. Moreau-Gaudry, F.; Ged, C.; Barbot, C.; Mazurier, F.; Boiron, J. M.; Bensidhoum, M.; Reiffers, J.; de Verneuil, H. Correction of the Enzyme Defect in Cultured Con-genital Erythropoietic Porphyria Disease Cells by Retro-virus-mediated Gene Transfer. Hum. Gene. Ther. 1995, 6, 13–20.
106. Moreau-Gaudry, F.; Mazurier, F.; Bensidhoum, M.; Ged, C.; de Verneuil, H. Metabolic Correction of Congenital Erythro-poietic Porphyria by Retrovirus-Mediated Gene Transfer into Epstein–Barr Virus-Transformed B-Cell Lines. Blood 1995, 85, 1449–1453.
107. Elder, G. H. Porphyria Cutanea Tarda and Related Disor-ders. Chapter 88; In Porphyrin Handbook, Part II; Kadish, K. M.; Smith, K.; Guilard, R., Eds.; Academic Press: San Diego, 2003; pp 67.
108. Thunell, S.; Harper, P. Porphyrins, Porphyrin Metabolism, Porphyrias. III. Diagnosis, Care and Monitoring in Porphyria Cutanea Tarda—Suggestions for a Handling Programme. Scand. J. Clin. Lab. Invest. 2000, 60, 561–579.
109. Moran, M. J.; Fontanellas, A.; Brudieux, E.; Hombrados, I.; de Ledinghen, V.; Couzigou, P.; de Verneuil, H.; De Sala-manca, R. E. Hepatic Uroporphyrinogen Decarboxylase Activity in Porphyria Cutanea Tarda Patients: The Influence of Virus C Infection. Hepatology 1998, 27, 584–589.
110. Armstrong, D. K.; Sharpe, P. C.; Chambers, C. R.; Whatley, S. D.; Roberts, A. G.; Elder, G. H. Hepatoerythropoietic Por-phyria: A Missense Mutation in the UROD Gene Is Associ-ated with Mild Disease and an Unusual Porphyrin Excretion Pattern. Br. J. Dermatol. 2004, 151, 920–923.
111. Mendez, M.; Sorkin, L.; Rossetti, M. V.; Astrin, K. H.; del, C.; Batlle, A. M.; Parera, V. E.; Aizencang, G.; Desnick, R. J. Familial Porphyria Cutanea Tarda: Characterization of Seven Novel Uroporphyrinogen Decarboxylase Mutations and Fre-quency of Common Hemochromatosis Alleles. Am. J. Hum. Genet. 1998, 63, 1363–1375.
112. Roberts, A. G.; Elder, G. H.; De Salamanca, R. E.; Herrero, C.; Lecha, M.; Mascaro, J. M. A Mutation (G281E) of the Human Uroporphyrinogen Decarboxylase Gene Causes Both Hepatoerythropoietic Porphyria and Overt Familial Por-phyria Cutanea Tarda: Biochemical and Genetic Studies on Spanish Patients. J. Invest. Dermatol. 1995, 104, 500–502.
113. Brady, J. J.; Jackson, H. A.; Roberts, A. G.; Morgan, R. R.; Whatley, S. D.; Rowlands, G. L.; Darby, C.; Shudell, E.; Wat-son, R.; Paiker, J., et al. Co-inheritance of Mutations in the Uroporphyrinogen Decarboxylase and Hemochromatosis Genes Accelerates the Onset of Porphyria Cutanea Tarda. J. Invest. Dermatol. 2000, 115, 868–874.
114. Kuhnel, A.; Gross, U.; Doss, M. O. Hereditary Copropor-phyria in Germany: Clinical-Biochemical Studies in 53 Patients. Clin. Biochem. 2000, 33, 465–473.
115. McManus, J. F.; Begley, C. G.; Sassa, S.; Ratnaike, S. Five New Mutations in the Uroporphyrinogen Decarboxylase Gene Identified in Families with Cutaneous Porphyria. Blood 1996, 88, 3589–3600.
116. Mendez, M.; Rossetti, M. V.; Siervi, A. D.; del Carmen Batlle, A. M.; Parera, V. Mutations in Familial Porphyria Cutanea Tarda: Two Novel and Two Previously Described for Hepa-toerythropoietic Porphyria. Hum. Mutat. 2000, 16, 269–270.
117. Christiansen, L.; Bygum, A.; Jensen, A.; Thomsen, K.; Bran-drup, F.; Hørder, M.; Petersen, N. E. Association Between CYP1A2 Polymorphism and Susceptibility to Porphyria Cutanea Tarda. Hum. Genet. 2000, 107, 612–614.
118. Linde, Y.; Harper, P.; Floderus, Y.; Ros, A. M. The Preva-lence of Hepatitis C in Patients with Porphyria Cutanea Tarda in Stockholm, Sweden. Acta. Derm. Venereol. 2005, 85, 164–166.
119. Egger, N. G.; Goeger, D. E.; Payne, D. A.; Miskovsky, E. P.; Weinman, S. A.; Anderson, K. E. Porphyria Cutanea Tarda: Multiplicity of Risk Factors Including HFE Mutations, Hepa-titis C, and Inherited Uroporphyrinogen Decarboxylase Defi-ciency. Dig. Dis. Sci. 2002, 47, 419–426.
120. Rossmann-Ringdahl, I.; Olsson, R. Porphyria Cutanea Tarda in a Swedish Population: Risk Factors and Complications. Acta. Derm. Venereol. 2005, 85, 337–341.
121. Mehrany, K.; Drage, L. A.; Brandhagen, D. J.; Pittelkow, M. R. Association of Porphyria Cutanea Tarda with Hereditary Hemochromatosis. J. Am. Acad. Dermatol. 2004, 51, 205–211.
122. Bonkovsky, H. L.; Poh-Fitzpatrick, M.; Pimstone, N.; Obando, J.; Di Bisceglie, A.; Tattrie, C.; Tortorelli, K.; LeClair, P.; Mercurio, M. G.; Lambrecht, R. W. Porphyria Cutanea Tarda, Hepatitis C, and HFE Gene Mutations in North America. Hepatology 1998, 27, 1661–1669.
123. Bulaj, Z. J.; Phillips, J. D.; Ajioka, R. S.; Franklin, M. R.; Griffen, L. M.; Guinee, D. J.; Edwards, C. Q.; Kushner, J. P. Hemochromatosis Genes and Other Factors Contributing to the Pathogenesis of Porphyria Cutanea Tarda. Blood 2000, 95, 1565–1571.
124. Roberts, A. G.; Whatley, S. D.; Nicklin, S.; Worwood, M.; Pointon, J. J.; Stone, C.; Elder, G. H. The Frequency of Hemochromatosis-Associated Alleles Is Increased in British Patients with Sporadic Porphyria Cutanea Tarda. Hepatol-ogy 1997, 25, 159–161.
125. Toback, A.; Sassa, S.; Poh-Fitzpatrick, M. B.; Schechter, J.; Zaider, E.; Harber, L. C.; Kappas, A. Hepatoerythropoietic Porphyria: Clinical, Biochemical, and Enzymatic Studies in a Three-Generation Family Lineage. N. Engl. J. Med. 1987, 316, 645–650.

30 CHAPTER 99 Inherited Porphyrias
126. Ged, C.; Ozalla, D.; Herrero, C.; Lecha, M.; Mendez, M.; de Verneuil, H.; Mascaro, J. M. Description of a New Mutation in Hepatoerythropoietic Porphyria and Prenatal Exclusion of a Homozygous Fetus. Arch. Dermatol. 2002, 138, 957–960.
127. Aarsand, A. K.; Brun, A.; Boman, H.; Sandberg, S. Differ-entiation Between Sporadic and Familial Porphyria Cutanea Tarda (abstract). Physiol. Res. 2003, 52, 1S.
128. Freesemann, A.; Frank, M.; Sieg, I.; Doss, M. O. Treatment of Porphyria Cutanea Tarda by the Effect of Chloroquine on the Liver. Skin Pharmacol. 1995, 8, 156–161.
129. Lamoril, J.; Puy, H.; Gouya, L.; Rosipal, R.; Da Silva, V.; Grandchamp, B.; Foint, T.; Bader-Meunier, B.; Dommergues, J. P.; Deybach, J. C., et al. Neonatal Hemolytic Anemia Due to Inherited Harderoporphyria: Clinical Characteristics and Molecular Basis. Blood 1998, 91, 1453–1457.
130. Rosipal, R.; Lamoril, J.; Puy, H.; Da Silva, V.; Gouya, L.; De Rooij, F. W.; Te Velde, K.; Nordmann, Y.; Martàsek, P.; Deybach, J. C. Systematic Analysis of Coproporphyrinogen Oxidase Gene Defects in Hereditary Coproporphyria and Mutation Update. Hum. Mutat. 1999, 13, 44–53.
131. Lamoril, J.; Puy, H.; Whatley, S. D.; Martin, C.; Woolf, J. R.; Da Silva, V.; Deybach, J. C.; Elder, G. H. Character-ization of Mutations in the CPO Gene in British Patients Demonstrates Absence of Genotype-Phenotype Correlation and Identifies Relationship Between Hereditary Copropor-phyria and Harderoporphyria. Am. J. Hum. Genet. 2001, 68, 1130–1138.
132. Gouya, L.; Puy, H.; Robreau, A. M.; Lyoumi, S.; Lamoril, J.; Da Silva, V.; Grandchamp, B.; Deybach, J. C. Modulation of Penetrance by the Wild-Type Allele in Dominantly Inherited Erythropoietic Protoporphyria and Acute Hepatic Porphyr-ias. Hum. Genet. 2004, 114, 256–262.
133. Meissner, P. N.; Dailey, T. A.; Hift, R. J.; Ziman, M.; Cor-rigall, A. V.; Roberts, A. G.; Meissner, D. M.; Kirsch, R. E.; Dailey, H. A. A R59W Mutation in Human Protoporphy-rinogen Oxidase Results in Decreased Enzyme Activity and Is Prevalent in South Africans with Variegate Porphyria. Nat. Genet. 1996, 13, 95–97.
134. Gouya, L.; Puy, H.; Robreau, A. M.; Bourgeois, M.; Lamoril, J.; Da Silva, V.; Grandchamp, B.; Deybach, J. C. The Pene-trance of Dominant Erythropoietic Protoporphyria Is Modu-lated by Expression of Wildtype FECH. Nat. Genet. 2002, 30, 27–28.
135. Hift, R. J.; Meissner, D.; Meissner, P. N. A Systematic Study of the Clinical and Biochemical Expression of Variegate Por-phyria in a Large South African Family. Br. J. Dermatol. 2004, 151, 465–471.
136. Meissner, P.; Hift, R. J.; Corrigall, A. Variegate Porphyria. Chapter 89; In Porphyrin Handbook, Part II; Kadish, K. M.; Smith, K.; Guilard, R., Eds.; Academic Press: San Diego, 2003; pp 93.
137. von und zu Fraunberg, M.; Timonen, K.; Mustajoki, P.; Kauppinen, R. Clinical and Biochemical Characteristics and Genotype–Phenotype Correlation in Finnish Variegate Por-phyria Patients. Eur. J. Hum. Genet. 2002, 10, 649–657.
138. Corrigall, A. V.; Hift, R. J.; Davids, L. M.; Hancock, V.; Meissner, D.; Kirsch, R. E.; Meissner, P. N. Homozygous Variegate Porphyria in South Africa: Genotypic Analysis in Two Cases. Mol. Genet. Metab. 2000, 69, 323–330.
139. Frank, J.; McGrath, J.; Lam, H.; Graham, R. M.; Hawk, J. L.; Christiano, A. M. Homozygous Variegate Porphyria: Identifi-cation of Mutations on Both Alleles of the Protoporphyrino-gen Oxidase Gene in a Severely Affected Proband. J. Invest. Dermatol. 1998, 110, 452–455.
140. Poblete-Gutierrez, P.; Wolff, C.; Farias, R.; Frank, J. A Chil-ean Boy with Severe Photosensitivity and Finger Shortening: the First Case of Homozygous Variegate Porphyria in South America. Br. J. Dermatol. 2006, 154, 368–371.
141. Roberts, A. G.; Puy, H.; Dailey, T. A.; Morgan, R. R.; Whatley, S. D.; Dailey, H. A.; Martasek, P.; Nordmann, Y.; Deybach, J. C.; Elder, G. H. Molecular Characterization of Homozygous Variegate Porphyria. Hum. Mol. Genet. 1998, 7, 1921–1925.
142. Whatley, S. D.; Puy, H.; Morgan, R. R.; Robreau, A. M.; Rob-erts, A. G.; Nordmann, Y.; Elder, G. H.; Deybach, J. C. Var-iegate Porphyria in Western Europe: Identification of PPOX Gene Mutations in 104 Families, Extent of Allelic Heteroge-neity, and Absence of Correlation Between Phenotype and Type of Mutation. Am. J. Hum. Genet. 1999, 65, 984–994.
143. Grabczynska, S. A.; McGregor, J. M.; Hawk, J. L. Late Onset Variegate Porphyria. Clin. Exp. Dermatol. 1996, 21, 353–356.
144. Cox, T. M. Protoporphyria. Chapter 90; In Porphyrin Hand-book, Part II; Kadish, K. M.; Smith, K.; Guilard, R., Eds.; Academic Press: San Diego, 2003; pp 121.
145. Whatley, S. D.; Ducamp, S.; Gouya, L.; Grandchamp, B.; Beaumont, C.; Badminton, M. N.; Elder, G. H.; Holme, S. A.; Anstey, A. V.; Parker, M., et al. C-Terminal Deletions in the ALAS2 Gene Lead to Gain of Function and Cause X-Linked Dominant Protoporphyria without Anemia or Iron Overload. Am. J. Hum. Genet. 2008, 83, 408–414.
146. Whatley, S. D.; Mason, N. G.; Holme, S. A.; Anstey, A. V.; Elder, G. H.; Badminton, M. N. Molecular Epidemiology of Erythropoietic Protoporphyria in the UK. Br. J. Dermatol. 2010, 162, 642–646.
147. Rufenacht, U. B.; Gouya, L.; Schneider-Yin, X.; Puy, H.; Schäfer, B. W.; Aquaron, R.; Nordmann, Y.; Minder, E. I.; Deybach, J. C. Systematic Analysis of Molecular Defects in the Ferrochelatase Gene from Patients with Erythropoietic Protoporphyria. Am. J. Hum. Genet. 1998, 62, 1341–1352.
148. Wilson, J.; Edixhoven-Bosdijk, A.; Koole-Lesuis, R.; Kroos, M. J.; de Rooij, F. W. M. A New Variant of Erythropoi-etic Protoporphyria with Normal Ferrochelatase Activity. Physiol. Res. 2003, 52, 29S.
149. Minder, E. I.; Gouya, L.; Schneider-Yin, X.; Deybach, J. C. A Genotype–Phenotype Correlation Between Null-Allele Muta-tions in the Ferrochelatase Gene and Liver Complication in Patients with Erythropoietic Protoporphyria. Cell. Mol. Biol. (Noisy-le-grand). 2002, 48, 91–96.
150. Bloomer, J.; Wang, Y.; Singhal, A.; Risheg, H. Molecular Studies of Liver Disease in Erythropoietic Protoporphyria. J. Clin. Gastroenterol. 2005, 39, S167–S175.
151. Risheg, H.; Chen, F. P.; Bloomer, J. R. Genotypic Determi-nants of Phenotype in North American Patients with Eryth-ropoietic Protoporphyria. Mol. Genet. Metab. 2003, 80, 196–206.
152. Whatley, S. D.; Mason, N. G.; Khan, M.; Zamiri, M.; Bad-minton, M. N.; Missaoui, W. N.; Dailey, T. A.; Dailey, H. A.; Douglas, W. S.; Wainwright, N. J., et al. Autosomal Reces-sive Erythropoietic Protoporphyria in the United Kingdom: Prevalence and Relationship to Liver Disease. J. Med. Genet. 2004, 41, e105.
153. Schoenfeld, N.; Mamet, R.; Minder, E. I.; Schneider-Yin, X. A “Null Allele” Mutation Is Responsible for Erythropoietic Pro-toporphyria in an Israeli Patient Who Underwent Liver Trans-plantation: Relationships Among Biochemical, Clinical, and Genetic Parameters. Blood. Cells. Mol. Dis. 2003, 30, 298–301.
154. Wiman, A.; Floderus, Y.; Harper, P. Novel Mutations and Phenotypic Effect of the Splice Site Modulator IVS3-48C in Nine Swedish Families with Erythropoietic Protoporphyria. J. Hum. Genet. 2003, 48, 70–76.
155. Yasui, Y.; Muranaka, S.; Tahara, T.; Shimizu, R.; Wata-nabe, S.; Horie, Y.; Nanba, E.; Uezato, H.; Takamiyagi, A.; Taketani, S., et al. A New Ferrochelatase Mutation Ombined with Low Expression Alleles in a Japanese Patient with Erythropoietic Protoporphyria. Clin. Sci. (Lond). 2002, 102, 501–506.

CHAPTER 99 Inherited Porphyrias 31
156. Ohgari, Y.; Sawamoto, M.; Yamamoto, M.; Kohno, H.; Taketani, S. Ferrochelatase Consisting of Wild-Type and Mutated Subunits from Patients with a Dominant-Inherited Disease, Erythropoietic Protoporphyria, Is an Active but Unstable Dimer. Hum. Mol. Genet. 2005, 14, 327–334.
157. Abitbol, M.; Bernex, F.; Puy, H.; Jouault, H.; Deybach, J. C.; Guénet, J. L.; Montagutelli, X. A Mouse Model Provides Evi-dence that Genetic Background Modulates Anemia and Liver Injury in Erythropoietic Protoporphyria. Am. J. Physiol. Gas-trointest. Liver. Physiol. 2005, 288, G1208–G1216.
158. Libbrecht, L.; Meerman, L.; Kuipers, F.; Roskams, T.; Des-met, V.; Jansen, P. Liver Pathology and Hepatocarcinogenesis in a Long-Term Mouse Model of Erythropoietic Protopor-phyria. J. Pathol. 2003, 199, 191–200.
159. Han, A. P.; Fleming, M. D.; Chen, J. J. Heme-Regulated eIF2alpha Kinase Modifies the Phenotypic Severity of Murine Models of Erythropoietic Protoporphyria and Beta-thalasse-mia. J. Clin. Invest. 2005, 115, 1562–1570.
160. Fontanellas, A.; Mazurier, F.; Landry, M.; Taine, L.; Morel, C.; Larou, M.; Daniel, J. Y.; Montagutelli, X.; de Salamanca, R. E.; de Verneuil, H. Reversion of Hepatobiliary Alterations by Bone Marrow Transplantation in a Murine Model of Erythropoietic Protoporphyria. Hepatology 2000, 32, 73–81.
161. Pawliuk, R.; Tighe, R.; Wise, R. J.; Mathews-Roth, M. M.; Leboulch, P. Prevention of Murine Erythropoietic Protopor-phyria-Associated Skin Photosensitivity and Liver Disease by Dermal and Hepatic Ferrochelatase. J. Invest. Dermatol. 2005, 124, 256–262.
162. Thunell, S.; Harper, P.; Brun, A. Porphyrins, Porphyrin Metabolism and Porphyrias. IV. Pathophysiology of Erythy-ropoietic Protoporphyria—Diagnosis, Care and Monitoring of the Patient. Scand. J. Clin. Lab. Invest. 2000, 60, 581–604.
163. Murphy, G. M. Diagnosis and Management of the Erythro-poietic Porphyrias. Dermatol. Ther. 2003, 16, 57–64.
164. Spelt, J. M.; de Rooij, F. W.; Wilson, J. H.; Zandbergen, A. A. Vitamin D Deficiency in Patients with Erythropoietic Pro-toporphyria. J. Inherit. Metab. Dis. 2009, [Epub] Jan 10.
165. McGuire, B. M.; Bonkovsky, H. L.; Carithers, R. L., Jr.; Chung, R. T.; Goldstein, L. I.; Lake, J. R.; Lok, A. S.; Potter, C. J.; Rand, E.; Voigt, M. D., et al. Liver Transplantation for Erythropoietic Protoporphyria Liver Disease. Liver. Transpl. 2005, 11, 1590–1596.
166. Freesemann, A. G.; Hofweber, K.; Doss, M. O. Coexistence of Deficiencies of Uroporphyrinogen III Synthase and Decar-boxylase in a Patient with Congenital Erythropoietic Por-phyria and in his Family. Eur. J. Clin. Chem. Clin. Biochem. 1997, 35, 35–39.
167. Weinlich, G.; Doss, M. O.; Sepp, N.; Fritsch, P. Variegate Porphyria with Coexistent Decrease in Porphobilinogen Deaminase Activity. Acta. Derm. Venereol. 2001, 81, 356–359.
168. Doss, M. O.; Gross, U.; Puy, H.; Doss, M.; Kühnel, A.; Jacob, K.; Deybach, J. C.; Nordmann, Y. Coexistence of Hereditary Coproporphyria and Porphyria Cutanea Tarda: A New Form of Dual Porphyria. Med. Klin. (Munich). 2002, 97, 1–5, (German).
169. Akagi, R.; Inoue, R.; Muranaka, S.; Tahara, T.; Taketani, S.; Anderson, K. E.; Phillips, J. D.; Sassa, S. Dual Gene Defects Involving Delta-Aminolaevulinate Dehydratase and Copro-porphyrinogen Oxidase in a Porphyria Patient. Br. J. Haema-tol. 2006, 132, 237–243.
170. Harraway, J. R.; Florkowski, C. M.; Sies, C.; George, P. M. Dual Porphyria with Mutations in Both the UROD and HMBS Genes. Ann. Clin. Biochem. 2006, 43, 80–82.
RELEVANT WEB PAGES
Porphy www.porphyriafoundation.comPore www.porphyria-europe.org

32 CHAPTER 99 Inherited Porphyrias
Biographies
Robert J Desnick, MD, PhD, is Dean for Genetics and Genomics and Professor and Chairman of the Department of Genetics and Genomic Sciences at The Mount Sinai School of Medicine and Physician-in-Chief of the Department of Medical Genetics and Genomics at the Mount Sinai Hospital in New York City. He is board-certified in Clinical, Biochemical, and Molecular Genetics by the American Board of Medical Genetics and is a Fellow of the American Academy of Pediatrics. He has published over 600 research articles and chapters, including nine edited books. He is a founder and Past-President of the Association of Professors of Human and Medi-cal Genetics and is a past Chair of the Association of American Medical Colleges (AAMC). He is an elected member of the American Pediatric Society, American Society for Clinical Investigation, American Association of Physicians, American Academy for the Advancement of Science (Fellow), and the Institute of Medicine of the National Academy of Sciences.
Manisha Balwani, MD, MS, received her MD degree from the University of Bombay and a Master’s degree in Genetics at the University of Pittsburgh. She is trained in Internal Medicine as well as Clinical and Biochemical Genetics and is an Assistant Professor in the Department of Genetics and Genomic Sciences at the Mount Sinai School of Medicine. Dr Balwani is the Co-Director of the Comprehensive Porphyria Diagnostic and Treatment Center at Mount Sinai, which has been designated as one of the five “Centers of Excellence” by the American Porphyria Foundation. She is part of the American Porphyria Foundation’s “Protect the Future” program. She is currently involved in research in the field of Porphyria as well as in clinical trials for development for newer therapies.
Karl E Anderson, MD, is Professor of Preventive Medicine and Community Health, Internal Medicine and Pharmacology and Toxicology at the University of Texas Medical Branch in Galveston, Texas. He is board-certified in Internal Medicine and Gastroenterology and a Fellow of the American College of Physicians. He has published over 200 articles, book chapter and reviews. He is Past-President of the Association for Patient-Oriented Research and an elected member of the American Gastroenterological Association, the American Association for the Study of Liver Diseases, the American Federation for Medical Research, the Southern Society for Clinical Investigation, and the American Association for the Advancement of Science.