Embed Size (px)
DESCRIPTION
Citation preview

In: Recent Advances in Veterinary Anesthesia and Analgesia: Companion Animals, Gleed R.D. and Ludders J.W. (Eds.). International Veterinary Information Service, Ithaca NY (www.ivis.org), Last updated: 14-Nov-2005; A1413.1105
Inhalants Used in Veterinary Anesthesia R. D. Keegan
College of Veterinary Medicine, Washington State University, Pullman, Washington, USA.
Introduction Inhalant anesthetics in use in veterinary anesthesia include nitrous oxide, halothane, isoflurane, sevoflurane, and desflurane. The latter four agents are commonly referred to as "the potent inhalants" as their MAC values (minimal alveolar concentration) are such that they may be used as the sole anesthetic agents during a surgical procedure. Nitrous oxide lacks sufficient potency to be used as a sole anesthetic in healthy, young veterinary patients. It must be pointed out that the clinical use of nitrous oxide is, if not controversial, at least contentious among veterinary anesthesiologists. Many specialists feel that the lack of potency of nitrous oxide renders the drug undesirable as an adjunct to inhalation anesthesia. Nevertheless, this author feels that the drug has a place in many situations encountered in the practice of veterinary anesthesia.
Nitrous Oxide Discovered in 1772, nitrous oxide is the oldest inhalant still in use in anesthesia practice. Although technically a vapor (see discussion earlier in this chapter) nitrous oxide is often referred to as a gaseous anesthetic. In veterinary anesthesia, the use of nitrous oxide has four main indications: 1. A MAC-sparing effect when used in combination with other "potent" inhalants - The MAC of nitrous oxide in the dog
is approximately 200% and in cats it is approximately 250%, concentrations that can not be achieved under normal barometric conditions; thus nitrous oxide may not be used as the sole anesthetic agent to anesthetize a fit, healthy patient. However, since nitrous oxide has anesthetic potency, it is often used as an adjunct drug and administered concomitantly with potent inhalant anesthetics such as halothane or isoflurane. Since the cardiorespiratory depressant effects of nitrous oxide are small compared to those of the potent inhalant anesthetics, the combination of nitrous oxide and a lower inspired concentration of a potent inhalant often provides adequate general anesthesia while minimally depressing the cardiorespiratory systems. The potency of nitrous oxide is such that in order to gain any appreciable benefit from including it in an anesthetic technique, high concentrations must be administered. Clinically useful concentrations of nitrous oxide range from 50% to 70%. Concentrations in excess of 70% are not recommended since the inspired oxygen concentration may decrease to dangerous levels. A good rule of thumb is that 50% nitrous oxide in dogs will reduce the MAC of a potent inhalant by 25%. Thus, anesthetists who frequently use vaporizer settings of 2% for isoflurane may find that 50% nitrous oxide and a vaporizer setting of 1.5% yields a similar depth of anesthesia.
Cats compared to dogs, differ in their response to nitrous oxide. In a nitrous oxide MAC reduction study of cats anesthetized with isoflurane, Imai et al., demonstrated that there are individual cats which do not respond (non-responders) to nitrous oxide [1]; that is, as the fraction of inspired nitrous oxide increased, the MAC of isoflurane did not decrease in a dose dependent manner. In cats that did respond as expected, 70% N2O reduced the MAC of isoflurane by only ~22%, a much smaller decrease than would be expected in dogs. This strongly suggests that cats do not respond to nitrous oxide as do dogs, and that there appears to be a subset of cats in which nitrous oxide does not provide any appreciable MAC sparing effects. These results further support studies demonstrating that the MAC of nitrous oxide in the cat is considerably higher than in the dog.
2. To supplement analgesia during a surgical procedure - Sub-anesthetic concentrations of nitrous oxide are associated with significant analgesia that is attributed to the central release of endogenous opioids, the endorphins and enkephalins [2]. Clinically, nitrous oxide is useful as a supplement to analgesia during painful surgical procedures. If more profound analgesia is required, the addition of a potent injectable opioid such as fentanyl is recommended.
3. To speed induction of inhalant anesthesia via the "second gas effect" - The second gas effect is a phenomenon by

which the rapid uptake by blood of large volumes of a gas from the alveoli acts to enhance the uptake of the remaining alveolar gases. This effect is most pronounced in the early stages of induction and has been used to speed anesthetic induction. The effect is usually seen clinically with concurrent administration of nitrous oxide and a potent inhalant anesthetic such as isoflurane or halothane. It is important to realize, however, that the second gas effect is not unique to nitrous oxide alone, but may occur with other gases provided that: 1) they are administered in high concentrations or large volumes, and 2) the gas in question has sufficient solubility in blood to permit significant uptake. Both properties are necessary. The administration of large volumes creates a large partial pressure gradient which drives the nitrous oxide out of the alveoli and into the blood while its solubility in blood means that the blood has the capacity for the nitrous oxide. The cause then of the second gas effect is the presence of at least 2 gases within the alveoli and the differential, rapid uptake of one of the gases. The factors which control how rapidly uptake occurs from the alveoli to the pulmonary blood are the partial pressure gradient between the alveoli and pulmonary blood and the solubility of the gas in blood. Both factors act to promote uptake; the partial pressure gradient provides the force to drive the gas out of the alveoli and into the blood while the solubility of the gas in blood determines how much anesthetic is transported away from the alveoli. The low potency of nitrous oxide dictates that large volumes must be administered to have a significant clinical effect. A large partial pressure gradient from alveoli to blood is generated and a large uptake of nitrous oxide into the blood results. The potent inhalant left behind becomes a larger proportion of the total volume of gas within the alveoli and thus its concentration and partial pressure increase. The concentration of a substance is expressed as the mass of the solute (mg) divided by the volume of the solvent (ml). Thus an increase in the concentration of a solution may be achieved in two ways: by an increase in the mass of the solute or by a decrease in the volume of the solvent. Since the speed of induction is directly influenced by alveolar inhalant partial pressure, an increased alveolar concentration means a more rapid induction into anesthesia, or, if the patient is awakening prematurely, a more rapid change in anesthetic depth. Using nitrous oxide to take advantage of the second gas effect is particularly beneficial during inhalant face mask inductions in canine patients. During mask inductions, healthy patients often exhibit a period of excitement characterized by uncoordinated struggling, vocalization, and expression of anal sacs, a situation that is best avoided. With experience, the anesthetist readily anticipates such excitement and may begin administering nitrous oxide in advance of the anticipated event. The addition of nitrous oxide acts to concentrate the potent inhalant thus hastening induction of anesthesia and lessening the incidence of untoward excitement.
4. As the sole anesthetic in extremely debilitated patients - although the MAC of nitrous oxide precludes its use as the sole inhalant anesthetic in fit patients, it is possible to use nitrous oxide as the primary inhalant in debilitated patients. Additional sedation and analgesia is provided by administering a potent opioid such as fentanyl or hydromorphone. The advantage of this technique is the cardiovascular stability afforded to the patient. Extremely debilitated patients possess a low, fixed cardiac output and may not tolerate the cardiovascular depression inherent in a technique using moderate concentrations of a potent inhalant. Often a technique that uses 50 - 66% nitrous oxide will allow completion of the surgical or diagnostic procedure without severely depressing cardiovascular function.
Important Considerations in the Use of Nitrous Oxide Owing to the low potency of nitrous oxide, large volumes- an inspired concentration of at least 50%- must be delivered to a patient in order to have any beneficial effect; this requirement is unique amongst all inhalant anesthetics in that no other inhalant anesthetics are administered in such high concentrations. The necessarily high administered concentration of nitrous oxide is responsible for two factors of importance to the anesthetist: 1) a large partial pressure gradient is generated for nitrous oxide, and 2) a lower limit on the patient’s inspired oxygen concentration is imposed.
The limiting effect of nitrous oxide on the inspired oxygen concentration is readily appreciated when one considers the inspired volumes of nitrous oxide the anesthetist often works with. All inspired gases are constrained by atmospheric pressure and their relative proportions must sum to 100%. If the anesthetist sets the nitrous oxide flow meter such that 50% of the total fresh gas flow is nitrous oxide, then the maximum inspired oxygen concentration is 50%. It is often desirable to maintain anesthetized patients on high fractions of inspired oxygen, particularly if the patient has underlying
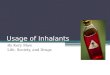
Figure 1. The second gas effect. Alveoli are depicted as square boxes and pulmonary capillaries are depicted below the boxes. The two figures depict an alveoli filled with N2O (blue circles) and a potent inhalant anesthetic (orange circles). In "A", no transfer of gas from alveoli to blood has yet occurred. In "B" the relatively larger partial pressure gradient for N2O drives numerous molecules of N2O into the blood thus increasing the alveolar concentration of the potent inhalant. - To view this image in full size go to the IVIS website at www.ivis.org . -
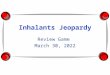
Figure 2. Mass and volume relationships. Box A shows concentration expressed as mass/volume. Concentration may be increased in a number of ways: by increasing the mass contained within the same volume as in B or by keeping the mass constant while decreasing the volume within which it is dissolved as in C. - To view this image in full size go to the IVIS website at www.ivis.org . -

cardiopulmonary dysfunction. In such patients it is advisable to evaluate oxygen exchange through the use of arterial blood gas analysis prior to administering nitrous oxide. Patients exhibiting an impaired ability to oxygenate their blood may become hypoxemic if the inspired fraction of oxygen is markedly decreased below 100%.
Partial pressure gradients are generated whenever a new gas is introduced into the patient’s alveoli. In essence, the partial pressure provides the driving force which transfers the gas from the alveoli to the pulmonary blood and, ultimately to the brain. Most inhalant anesthetics have fairly low MAC values and as a consequence are administered in correspondingly low inspired concentrations. For example, isoflurane has a MAC value of approximately 1.31% in dogs and is commonly administered at inspired concentrations of 1.6 - 2.0%. An inspired concentration of 2% will result in the development of a maximum alveolar-arterial partial pressure gradient of 760 mmHg X 0.02 = 15.2 mm Hg. In comparison, fifty percent nitrous oxide will generate an alveolar-arterial partial pressure gradient of 380 mm Hg. Thus it is apparent that the force driving nitrous oxide into the blood from the alveoli is much greater than the force driving the "potent" inhalants. This comparatively larger partial pressure gradient is responsible for not only the second gas effect described above, but also for two additional phenomena associated with the use of nitrous oxide: diffusion hypoxia and the transfer of nitrous oxide to closed gas spaces.
Diffusion Hypoxia In the previous section we learned that the high concentrations of nitrous oxide administered to patients (made necessary by the high MAC value for nitrous oxide) resulted in the second gas effect. A similar, related phenomenon occurs when the administration of nitrous oxide is discontinued. When the nitrous oxide flow meter is switched off, the concentration of nitrous oxide within the breathing circuit decreases. The partial pressure gradient for nitrous oxide now reverses and the partial pressure within the blood and tissues becomes greater than in the alveoli. Nitrous oxide, following its partial pressure gradient, pours into the alveoli from the blood and dilutes whatever gas is present in the alveoli. If the patient is inspiring room air containing 21% oxygen, the dilution effect may be significant enough to cause hypoxemia. This can be avoided by administering 100% oxygen to the patient for 5 minutes after discontinuing the nitrous oxide.
Transfer of Nitrous Oxide to Closed Gas Spaces The high concentrations of nitrous oxide administered to patients and the differential solubilities of nitrous oxide and nitrogen in blood combine to result in the pooling of nitrous oxide in closed air-containing cavities within a patient’s body. The pooling of nitrous oxide in these spaces may have significant effects on the patient’s cardiac output and/or minute ventilation. Depending upon the condition of the patient and the length of time they are administered nitrous oxide, distension of these pockets may be life threatening. Closed air-containing cavities are normally found throughout the body. Air is normally present to varying degrees in the gut particularly in the rumen and large colon of large animal species. In small animals, abnormal accumulations of nitrogen-containing air are seen with gastric dilation volvulus or pneumothorax. As the tissues surrounding the nitrogen-containing pocket are perfused with blood containing little nitrogen and a significant amount of nitrous oxide, a large partial pressure gradient develops that favors movement of nitrous oxide into the pocket and nitrogen out of the pocket. The much larger partition coefficient of nitrous oxide (0.47) compared with that of nitrogen (0.016) means that the blood will deliver far more nitrous oxide to the pocket than it will remove nitrogen. The net effect is that the volume of the pocket will increase if the walls of the pocket are distensible. If the walls of the gas filled space are rigid as with a facial sinus, the preferential ingress of nitrous oxide causes an increase in pressure within the sinus. The theoretical maximum increase in volume may be estimated from the following formula [3] where M is a multiple of the original volume of a gas-containing space with unlimited compliance.
Thus if 50% nitrous oxide is used the volume of the gas filled space has the potential to increase to two times the original volume; if 80% nitrous oxide is used, then the volume could potentially increase to five times the original volume [3]. The maximal increase in volume or pressure seen with the use of nitrous oxide occurs at equilibrium and is a theoretical maximum that may take several hours to achieve; the process of equilibration is influenced by the nature of the gas originally occupying the gas space and the blood supply to the tissues surrounding the enclosed space. For example, the volume in a segment of gas-filled intestine may be minimally or very slowly affected by the use of nitrous oxide for a short period of time (as when using it only to take advantage of the second gas effect) [3]; the volume of gas in a pneumothorax, however, may change very rapidly because nitrous oxide moves along its concentration gradient not only from blood but also from the lungs [3]. Regardless of the theoretical considerations, many veterinary anesthesiologists choose to avoid the
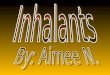
Figure 3. Diffusion hypoxia. When N2O administration is discontinued, the N2O in the blood moves to the alveoli along its partial pressure gradient and effectively dilutes the oxygen present in the alveoli. - To view this image in full size go to the IVIS website at www.ivis.org . -

use of nitrous oxide in patients whenever a closed, gas-filled space exists.
Metabolism and Toxicity The cardiorespiratory effects of nitrous oxide are much less than those of the potent inhalant anesthetics. Although a direct myocardial depressant, the sympathetic stimulant properties of the drug usually result in an increase in cardiac output. Nitrous oxide is an extremely inert substance; the drug is not metabolized to any extent by the patient and is exhaled unchanged. Chronic exposure to nitrous oxide is associated with development of megaloblastic hematopoiesis and polyneuropathy because nitrous oxide oxidizes vitamin B-12 which is an essential cofactor for the enzyme methionone synthetase. With methionine synthetase thus inactivated, serum methionine becomes depleted and results in megaloblastic anemia and leukopenia. Since serum methionine levels typically recover within 3 to 4 days, it may be prudent to avoid repeated use of nitrous oxide within this time frame.
Halothane Introduced into veterinary anesthesia practice in 1956, halothane is still a widely used inhalant anesthetic. Synthesized in an effort to produce a non-flammable inhalant anesthetic, the drug was an attractive alternative to diethyl ether and cyclopropane. Although the fluorinated hydrocarbons are not flammable, significant arrhythmogenic properties limited their future development as inhalant anesthetics. Halothane is a potent drug, having a MAC value in dogs of 0.87% and 1.14% in cats. The vapor pressure of halothane (243 mm Hg at 20°C) is such that it must be administered using a precision vaporizer if precise, predictable concentrations are desired. Clinically useful settings in small animals are 2 - 3% for induction of anesthesia, and 1 - 1.5% for maintenance of anesthesia. The moderate blood solubility of halothane (blood/gas PC = 2.4) translates to a more rapid induction of anesthesia compared with more soluble agents such as methoxyflurane or diethyl ether.
Cardiovascular Effects The cardiovascular effects of halothane may be significant. In a dose dependent manner, halothane decreases blood pressure by decreasing myocardial contractility via direct depression of the myocardium which results in a reduction of cardiac output [4]. As mentioned previously, halothane has arrhythmogenic properties. Studies investigating inhalant anesthetic arrhythmogenicity using the arrhythmogenic dose of epinephrine (ADE) test have shown decreased arrhythmogenic thresholds during administration of halothane. Cardiac arrhythmias during clinical use of halothane are frequently encountered. Most are fairly benign and do not require administration of anti-arrhythmogenic drugs. If halothane associated arrhythmias are worrisome, switching to a less arrhythmogenic inhalant anesthetic such as isoflurane will often reduce or eliminate the arrhythmias. Switching inhalant anesthetics mid-anesthesia may be performed safely provided the anesthetist is mindful of both the solubilities and the potencies of the two inhalant anesthetics. Inhalants having low blood solubility (low PC values) will result in a more rapid induction into and recovery from anesthesia compared with inhalants having high blood solubility (high PC values). Inhalant anesthetics having high potency (low MAC values) require lower alveolar concentrations to induce general anesthesia. These two physical properties of halothane and isoflurane indicate that isoflurane, having lower solubility, will be taken up more rapidly than halothane will be eliminated. Isoflurane is also less potent (higher MAC) than is halothane, thus it might appear that the more rapid effect seen with isoflurane would be counterbalanced by the higher concentrations needed for anesthesia. Clinically it appears that the lower solubility of isoflurane more than compensates for the higher alveolar concentrations necessary, therefore, if a patient is immediately switched from halothane to isoflurane, a deepening of the anesthetic plane is frequently seen. Thus when switching from halothane to isoflurane it is recommended that the administration of halothane be discontinued or at least reduced until the patient displays signs consistent with a lighter anesthetic plane before administering isoflurane. A similar line of reasoning applies when switching from halothane or isoflurane to the less soluble sevoflurane or desflurane. Always decrease administration of the more soluble inhalant before switching to the less soluble agent.
Respiratory Effects Administration of halothane is associated with a dose-dependent respiratory depression that is initially manifested as a decrease in tidal volume; as anesthetic depth increases a decrease in respiratory rate also is seen. Common to all inhalant anesthetics, the respiratory depressing effects of halothane may be at least partially offset by surgical stimulation [5].
CNS Effects Inhalation of halothane results in global depression of the central nervous system. Increasing depth of anesthesia results in reduced EEG activity but unlike with isoflurane a burst suppression pattern is not frequently observed [6]. Halothane decreases cerebral metabolic rate of oxygen utilization and is a potent cerebrovasodilator that results in increased cerebral blood flow (CBF) and intracranial pressure (ICP) [7]. The dilating effect of halothane on the cerebral vasculature may be greatly modified by the patient’s arterial PCO2 tension [8]. Hypoventilation and associated elevations in PaCO2 will greatly exacerbate the increases in ICP while mild hyperventilation (controlled manually or mechanically) - PaCO2 ~ 30 mm Hg - will diminish halothane-induced increases in ICP. Since other inhalant anesthetics do not result in the same magnitude of increase in CBF and ICP at similar MAC

levels [9], halothane is usually not recommended for patients presenting with or suspected of having raised ICP.
Other Effects Of all inhalant anesthetics in veterinary use today, halothane is the least inert and most highly metabolized with 20 - 25% of the anesthetic recovered as metabolites. Although all inhalant anesthetics have the potential to be associated with a hepatocellular injury that is usually manifested as centrilobular necrosis, halothane has been the drug most frequently implicated [10]. While the precise mechanism of hepatic injury remains unknown, a likely cause is the production of reactive metabolites from hepatic biotransformation, especially during periods of regional hepatic hypoxemia or hypoperfusion, together with an autoimmune reaction.
Isoflurane An isomer of the inhalant anesthetic enflurane, isoflurane was introduced into veterinary practice in the 1980's. Similar to the fluorinated hydrocarbon halothane, isoflurane is nonflammable and non-explosive in clinically useful concentrations, but its fluorinated ether structure seems to markedly reduce the potential for cardiac dysrhythmias. Isoflurane is slightly less potent than halothane with a MAC value of 1.31 in dogs and 1.61% in cats. The solubility of isoflurane (Blood:Gas PC = 1.3) is lower than that of halothane and inductions into and recoveries from anesthesia occur more rapidly than with halothane. Isoflurane has a vapor pressure similar to that of halothane (238 mmHg at 20°C) and as such it is recommended that it be administered in a precision vaporizer. Clinically useful settings in small animals are 2 - 4% for induction of anesthesia, and 1 - 2% for maintenance of anesthesia. The current popularity of isoflurane in veterinary practice reflects the drug’s cardiovascular stability, low blood solubility, resistance to hepatic metabolism and attractive price.
Cardiovascular Effects Isoflurane appears to be among the best of the inhalant anesthetics in preserving cardiovascular function. The drug is less likely than is halothane to sensitize the myocardium to the dysrhythmogenic effects of catecholamines. As a consequence, isoflurane is preferred over halothane in patients presenting with pre-existing dysrhythmias. Indeed, in our clinical experience many patients presenting with ventricular premature contractions prior to anesthesia are actually improved under isoflurane anesthesia, that is, the incidence of the ventricular premature contractions is often markedly reduced or eliminated. The exact mechanism of this effect is unknown but may be a result of a decrease in sympathetic nervous system activity and/or a reduction in painful stimuli. Isoflurane is associated with a dose dependant reduction in cardiac output and blood pressure. The effect on cardiac output is less than that seen with halothane although the reduction in blood pressure may be more significant. Reduction of cardiac output appears to be due to a decrease in myocardial contractility and a concomitant but mild decrease in stroke volume. However, isoflurane is associated with an increase in heart rate which compensates for the mild depression of stroke volume and the net result is a slight decrease or no change in cardiac output. Isoflurane is a potent vasodilator and as such reduces systemic vascular resistance which results in depression of mean arterial pressure despite the fact that cardiac output remains essentially unchanged. The mechanism whereby isoflurane causes vasodilation may be related to its ability to activate peripheral opioid receptors by an endogenous opioid peptide possibly related to methionine enkephalin [11].
Respiratory Effects Similar to other inhalant anesthetics, isoflurane depresses ventilation in a dose dependant manner. In anesthetized animals not experiencing surgical stimulation, tidal volume decreases and arterial CO2 tension increases as depth of anesthesia is increased. As the administered dose of isoflurane approaches 2.0 MAC, respiratory frequency decreases and arterial CO2 tension increases [12]. As with all inhalant anesthetics, the effect of surgical stimulation mitigates the respiratory depression caused by isoflurane [5]. This effect is most pronounced during light planes of anesthesia and may be clinically insignificant at very deep levels.
CNS Effects Similar to halothane, administration of isoflurane results in global central nervous system depression. Whereas increasing depth of halothane anesthesia is characterized by an isoelectric EEG pattern, increasing depth of isoflurane anesthesia is associated with a "burst suppression" pattern on the EEG. The burst suppression pattern is commonly seen in dogs at concentrations of 1.8 - 2.0% (1.4 - 1.5 MAC) and is characterized by a period of electrical quiescence interrupted by bursts of activity [13]. Administration of isoflurane is associated with an increase in CBF and therefore in ICP, however the magnitude of increase is much less than for halothane at equi-MAC concentrations. Hyperventilation and the associated reduction in arterial CO2 may be used to limit the isoflurane-associated increase in CBF since the cerebral circulation remains responsive to changes in PaCO2 [14,15]. As the increase in CBF is less for isoflurane compared with halothane and a lowering of the patient’s PaCO2 through the use of judicious hyperventilation is usually quite easily accomplished, isoflurane is generally preferred over halothane for maintenance of inhalant anesthesia in a patient presenting with raised intracranial pressure.
Other Effects Isoflurane is an extremely inert and stable compound. Less than 0.2% of the administered dose is metabolized. As with

halothane, hepatic blood flow is decreased in a dose dependant manner. Despite the potential reduction in hepatic blood flow, post anesthetic serum biochemical tests show minimal changes in hepatocyte integrity or function, presumably reflecting the inertness and lack of metabolism of the drug [16]. The lack of significant effect on hepatic function and the extremely small amount of the drug that undergoes hepatic metabolism has made isoflurane a popular inhalant anesthetic for use in patients presenting with compromised hepatic function.
Sevoflurane Sevoflurane is the newest inhalant anesthetic that has been approved for use in veterinary anesthesia. The drug was initially described in 1975 but not released until the 1990s. Sevoflurane is nonflammable and non-explosive in concentrations used clinically. It has a MAC value of 2.36% in dogs and 2.58% in cats, and a blood:gas partition coefficient of 0.69 making it both less potent and less soluble in blood than either halothane or isoflurane. Typical vaporizer settings are 4 - 5% for induction and 2.5 - 4.0% for maintenance. The lower blood solubility of sevoflurane compared with isoflurane results in more rapid inductions and recoveries, and a more rapid change in anesthetic depth in response to a change in inspired concentration.
Cardiovascular Effects The cardiovascular effects of sevoflurane are comparable to those of isoflurane. Sevoflurane does not markedly increase the sensitivity of the myocardium to circulating catecholamines and thus the potential for developing intraoperative arrhythmias is less for sevoflurane than for halothane [17]. As with all inhalants, sevoflurane depresses cardiac output and blood pressure in a dose dependent manner.
Respiratory Effects The respiratory depressant effects of sevoflurane are similar to those of isoflurane.
CNS Effects The effect of sevoflurane on intracranial hemodynamics appears to be similar to that of isoflurane. In a rabbit model, sevoflurane was associated with changes in ICP, CBF and EEG pattern that were indistinguishable from those seen with isoflurane [18].
Other Effects Approximately 3% of administered sevoflurane may be recovered as sevoflurane metabolites [19]. Sevoflurane is susceptible to degradation both by the patient and within the breathing circuit. Hepatic metabolism of sevoflurane results in the production of free fluoride ions. This discovery caused initial concern, since the older inhalant anesthetic methoxyflurane, had been withdrawn from human anesthesia practice due to documented nephrotoxicity associated with release of fluoride ions during its metabolism. The rate of production of fluoride ions is much less than with methoxyflurane, however, and no reports of nephrotoxicity in humans or animals have been reported. Sevoflurane will decompose in the presence of CO2 absorbants such as soda lime and Baralyme® and produce vinyl ether having nephrotoxic properties. The toxic ether, known as Compound A, is produced when sevoflurane contacts alkaline compounds. Featuring prominently amongst the factors influencing the production of Compound A is the use of dry carbon dioxide absorbant [20,21]. Desiccation of carbon dioxide absorbent can be minimized by disconnecting anesthesia machines from the oxygen source to ensure that gas flow and consequent drying of absorbent does not occur when the equipment is not in use.
Desflurane Desflurane is the newest of the inhalant anesthetics introduced into human anesthesia practice. The chemical structure of desflurane is very similar to that of isoflurane, differing only in the substitution of a fluoride ion for a chloride ion on one of the carbon atoms. This seemingly trivial substitution results in an inhalant anesthetic that is much more inert and much less soluble in blood than its parent, isoflurane. At a blood:gas partition coefficient of 0.42, desflurane is the least soluble of all inhalant anesthetics including nitrous oxide. The low blood solubility means that inductions and recoveries are extremely rapid. In addition, changes in anesthetic depth occur much more rapidly with desflurane than with isoflurane. Desflurane is the least potent of the so called potent inhalant anesthetics (all inhalant anesthetics except nitrous oxide) having a MAC value in dogs of 7.2% and 9.79% in cats. Typical vaporizer settings range from 12 - 18% for induction and 8 - 10% for maintenance.
Desflurane is highly volatile as evidenced by its vapor pressure of 664 mm Hg at 20°C. Since the boiling point of a liquid is defined as the temperature at which the liquid’s vapor pressure equals atmospheric pressure, desflurane begins to boil when the temperature rises above 20°C at sea level; at a lower barometric pressure such as at an altitude of 1000 meters, desflurane boils at 20°C. Its high vapor pressure required developing a vaporizer designed to accurately meter anesthetic at such high vapor pressures. The Ohmeda Tec 6 vaporizer is electrically heated to a constant temperature of 37°C. At this temperature, desflurane is converted to the gaseous phase enabling an electronically controlled pressure regulating valve to

provide precise and controllable output from the vaporizer.
Cardiovascular Effects The cardiovascular effects associated with desflurane are similar to those produced by isoflurane. In contrast to halothane and similar to isoflurane, the myocardium is not sensitized to the arrhythmogenic effects of catecholamines [22]. Similar to all potent inhalant anesthetics, desflurane is a cardiac depressant. It decreases myocardial contractility, cardiac output and blood pressure in a dose related manner while increasing heart rate at all levels of anesthesia [23], effects that are quite similar to those associated with administration of an equipotent concentration of isoflurane. In a dog model of myocardial failure, desflurane was reported to preserve diastolic function to a greater degree than did sevoflurane [24].
Respiratory Effects The respiratory depression associated with administration of desflurane appears to be comparable to that produced by isoflurane. In children, concentrations of desflurane greater than 1 MAC are associated with an increase in respiratory depression that is due mostly to a reduction in tidal volume [25].
CNS Effects Desflurane appears to induce effects on EEG, cerebral vascular resistance (CVR), and CBF that are similar to those associated with isoflurane. In dogs, increasing concentrations of desflurane were associated with decreases in CVR and concomitant increases in CBF [26].
Other Effects Desflurane is the most stable and inert of any potent inhalant anesthetic in use. Replacement of the sole chloride atom on isoflurane with a fluoride ion results in an inhalant anesthetic that is more stable and more resistant to biodegradation; indeed only approximately 0.2% of the drug may be recovered as metabolites [19].
References
1. Imai A, Ilkiw JE, Pypendop BH, et al. Nitrous Oxide does not Consistently Reduce Isoflurane Requirement in Cats. Vet Anaesth Analg 2002; 29(2):98.
2. Cahill FJ, Ellenberger EA, Mueller JL, et al. Antagonism of nitrous oxide antinociception in mice by intrathecally administered antisera to endogenous opioid peptides. J Biomed Sci 2000;7:299-303.
3. Eger EI. Anesthetic Uptake and Action. Baltimore: Williams & Wilkins, 1974; 171-183.
4. Brown BR, Crout JR. A comparative study of the effects of five general anesthetics on myocardial contractility: I. Isometric conditions. Anesthesiology 1971; 34:236-245.
5. France CJ, Plumer MH, Eger EI 2nd, et al. Ventilatory effects of isoflurane (Forane) or halothane when combined with morphine, nitrous oxide and surgery. Br J Anaesth 1974; 46:117-120.
6. Eger EI, Stevens WC, Cromwell TH. The electroencephalogram in man anesthetized with forane. Anesthesiology 1971; 35:504-508.
7. Artru AA. Relationship between cerebral blood volume and CSF pressure during anesthesia with halothane or enflurane in dogs. Anesthesiology 1983; 58:533-539.
8. Smith RB, Aass AA, Nemoto EM. Intraocular and intracranial pressure during respiratory alkalosis and acidosis. Br J Anaesth 1981; 53:967-972.
9. Adams RW, Cucchiara RF, Gronert GA, et al. Isoflurane and cerebrospinal fluid pressure in neurosurgical patients. Anesthesiology 1981; 54:97-99.
10. Brown BR Jr, Gandolfi AJ. Adverse effects of volatile anaesthetics. Br J Anaesth 1987; 59:14-23.
11. Ellenberger EA, Lucas HL, Russo JM, et al. An opioid basis for early-phase isoflurane-induced hypotension in rats. Life Sci 2003; 73:2591-2602.
12. Hodgson DS, Dunlop CI, Chapman PL, et al. Cardiopulmonary effects of anesthesia induced and maintained with isoflurane in cats. Am J Vet Res 1998; 59:182-185.
13. Moore MP, Greene SA, Keegan RD, et al. Quantitative electroencephalography in dogs anesthetized with 2.0% end-tidal concentration of isoflurane anesthesia. Am J Vet Res 1991; 52:551-560.
14. Aladj LJ, Croughwell N, Smith LR, et al. Cerebral blood flow autoregulation is preserved during cardiopulmonary bypass in isoflurane-anesthetized patients. Anesth Analg 1991; 72:48-52.

15. Eger EI. The pharmacology of isoflurane. Br J Anaesth 1984; 56 Suppl 1:71S-99S.
16. Topal A, Gul N, Ilcol Y, et al. Hepatic effects of halothane, isoflurane or sevoflurane anaesthesia in dogs. J Vet Med A Physiol Pathol Clin Med 2003; 50:530-533.
17. Navarro R, Weiskopf RB, Moore MA, et al. Humans anesthetized with sevoflurane or isoflurane have similar arrhythmic response to epinephrine. Anesthesiology 1994; 80:545-549.
18. Scheller MS, Tateishi A, Drummond JC, Z et al. The effects of sevoflurane on cerebral blood flow, cerebral metabolic rate for oxygen, intracranial pressure, and the electroencephalogram are similar to those of isoflurane in the rabbit. Anesthesiology 1988; 68:548-551.
19. Eger EI. New inhaled anesthetics. Anesthesiology 1994; 80:906-922.
20. Fang ZX, Kandel L, Laster MJ, et al. Factors affecting production of compound A from the interaction of sevoflurane with Baralyme and soda lime. Anesth Analg 1996; 82:775-781.
21. Steffey EP, Laster MJ, Ionescu P, et al. Dehydration of Baralyme increases compound A resulting from sevoflurane degradation in a standard anesthetic circuit used to anesthetize swine. Anesth Analg 1997; 85:1382-1386.
22. Weiskopf RB, Eger EI , Holmes MA, et al. Epinephrine-induced premature ventricular contractions and changes in arterial blood pressure and heart rate during I-653, isoflurane, and halothane anesthesia in swine. Anesthesiology 1989; 70:293-298.
23. Weiskopf RB, Holmes MA, Eger EI II, et al. Cardiovascular effects of I-653 in swine. Anesthesiology 1988; 69:303-309.
24. Preckel B, Mullenheim J, Hoff J, et al. Haemodynamic changes during halothane, sevoflurane and desflurane anaesthesia in dogs before and after the induction of severe heart failure. Eur J Anaesthesiol 2004; 21:797-806.
25. Behforouz N, Dubousset AM, Jamali S, et al. Respiratory effects of desflurane anesthesia on spontaneous ventilation in infants and children. Anesth Analg 1998; 87:1052-1055.
26. Lutz LJ, Milde JH, Milde LN. The cerebral functional, metabolic, and hemodynamic effects of desflurane in dogs. Anesthesiology 1990; 73:125-131.
All rights reserved. This document is available on-line at www.ivis.org. Document No. A1413.1105















![Veterinary Anesthesia [Autosaved]](https://img.pdfslide.us/doc/110x75/55cf917a550346f57b8dbe92/veterinary-anesthesia-autosaved.jpg)