Embed Size (px)
Citation preview

E D I T O R I A L
Informed owner consent – how informed?
In this issue, Derek Flaherty raises the question as to
when informed owner consent is required for a
clinical study which compares two established
anaesthetic techniques, and highlights the problems
that anaesthetists, who do not always themselves
meet the owners, have in obtaining such consent.
We thank him for raising this important issue, so
that it can be discussed.
Few people would disagree that some form of owner
consent is needed to allow the use of data from any
patient, as otherwise there would be a breach of
patient (in this case owner) confidentiality. For
retrospective, or even non-randomized prospective
studies, where the anaesthetic technique is specifically
tailored to the individual needs of that animal,
generalized owner consent to use data usually is
acceptable, and can be incorporated into the main
consent form for treatment. However, when a pro-
spective clinical trial uses randomized treatments, the
situation changes, as the choice is no longer individ-
ually assessed on that patient’s needs.
At VAA, we have implemented the statement of
the International Association of Veterinary Editors
(IAVE), a group to which most of the major
veterinary journals belong. The author instructions
for this journal now state:
Manuscripts will be considered for publication
only if the work detailed therein:
1) Follows international, national, and/or institu-
tional guidelines for humane animal treatment;
where national or institutional guidelines do
not exist, international guidelines must be
followed, e.g., National Institutes of Health or
Euroguide;
2) Has been approved by a properly constituted
internal ethics review committee at the insti-
tution or practice at which the studies were
conducted;
3) For studies using client-owned animals (public
or private), demonstrates a high standard (best
practice) of veterinary care and, as relevant,
involves informed client/owner consent
Prior to acceptance of a manuscript, to verify
compliance with the above policies, the authors
must:
1) Attest that legal and ethical requirements have
been met with regards to the humane treat-
ment of animals described in the study;
2) Specify in Materials and methods the ethical
review committee approval process and the
international, national, and/or institutional
guidelines followed;
3) If so requested, provide evidence, such as a
signed animal use form or protocol number, of
compliance with ethical review at the institu-
tion or practice;
4) Provide evidence in Materials and methods that
the principles of reduction, refinement, and
replacement have been met.
As anaesthesiologists we have a difficult time
when it comes to doing clinical research. In the past
many of us have done things that are within the
bounds of normal clinical practice but still represent
a deviation from the usual protocol and have not
asked permission to do this. The above statements
make it clear that this is no longer acceptable and
we need owner permission if we are to collect data
from animals that involves doing something beyond
our normal practice. Since most of us do not have
direct contact with the owner this means gaining
support from the primary clinician and ensuring
that the target population of owners are consistently
asked to sign on to the protocol. We also need
‘informed’ consent, where the conversation with the
owner and the form they sign have to represent
both the expected benefits and complications that
might be associated with the research. The Office for
Human Research Protection (NIH) has a checklist
for an informed consent form that could easily be
321
Veterinary Anaesthesia and Analgesia, 2012, 39, 321–323 doi:10.1111/j.1467-2995.2012.00760.x
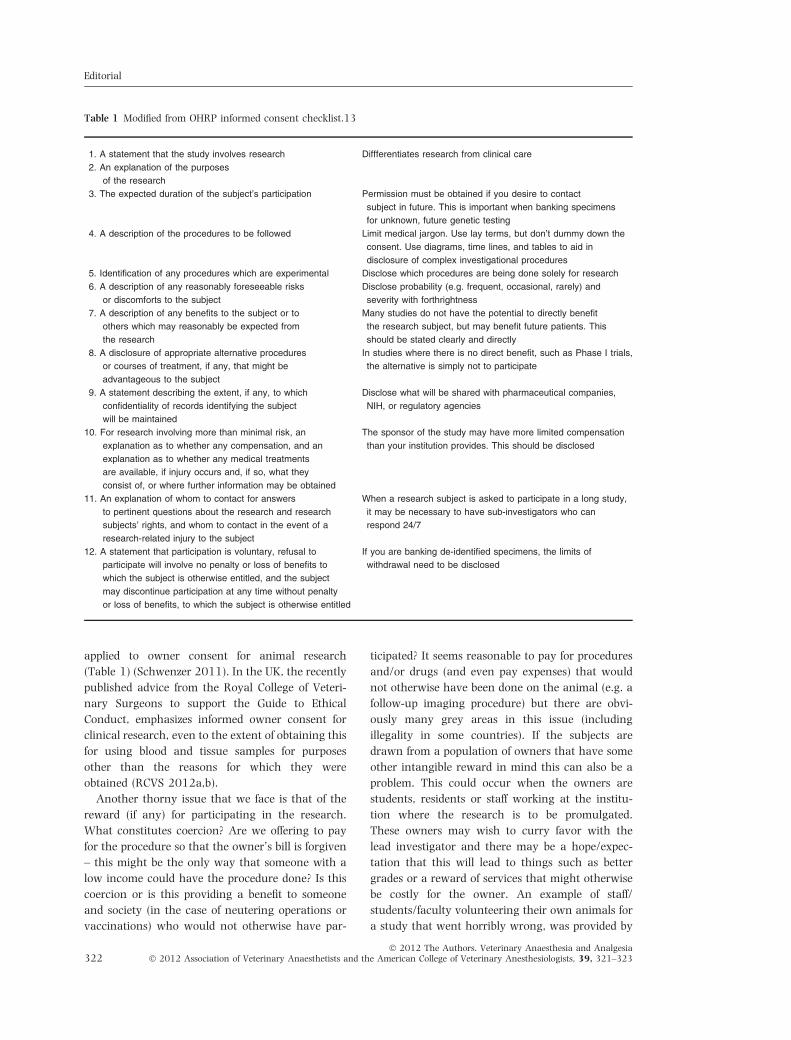
applied to owner consent for animal research
(Table 1) (Schwenzer 2011). In the UK, the recently
published advice from the Royal College of Veteri-
nary Surgeons to support the Guide to Ethical
Conduct, emphasizes informed owner consent for
clinical research, even to the extent of obtaining this
for using blood and tissue samples for purposes
other than the reasons for which they were
obtained (RCVS 2012a,b).
Another thorny issue that we face is that of the
reward (if any) for participating in the research.
What constitutes coercion? Are we offering to pay
for the procedure so that the owner’s bill is forgiven
– this might be the only way that someone with a
low income could have the procedure done? Is this
coercion or is this providing a benefit to someone
and society (in the case of neutering operations or
vaccinations) who would not otherwise have par-
ticipated? It seems reasonable to pay for procedures
and/or drugs (and even pay expenses) that would
not otherwise have been done on the animal (e.g. a
follow-up imaging procedure) but there are obvi-
ously many grey areas in this issue (including
illegality in some countries). If the subjects are
drawn from a population of owners that have some
other intangible reward in mind this can also be a
problem. This could occur when the owners are
students, residents or staff working at the institu-
tion where the research is to be promulgated.
These owners may wish to curry favor with the
lead investigator and there may be a hope/expec-
tation that this will lead to things such as better
grades or a reward of services that might otherwise
be costly for the owner. An example of staff/
students/faculty volunteering their own animals for
a study that went horribly wrong, was provided by
Table 1 Modified from OHRP informed consent checklist.13
1. A statement that the study involves research Diffferentiates research from clinical care
2. An explanation of the purposes
of the research
3. The expected duration of the subject’s participation Permission must be obtained if you desire to contact
subject in future. This is important when banking specimens
for unknown, future genetic testing
4. A description of the procedures to be followed Limit medical jargon. Use lay terms, but don’t dummy down the
consent. Use diagrams, time lines, and tables to aid in
disclosure of complex investigational procedures
5. Identification of any procedures which are experimental Disclose which procedures are being done solely for research
6. A description of any reasonably foreseeable risks
or discomforts to the subject
Disclose probability (e.g. frequent, occasional, rarely) and
severity with forthrightness
7. A description of any benefits to the subject or to
others which may reasonably be expected from
the research
Many studies do not have the potential to directly benefit
the research subject, but may benefit future patients. This
should be stated clearly and directly
8. A disclosure of appropriate alternative procedures
or courses of treatment, if any, that might be
advantageous to the subject
In studies where there is no direct benefit, such as Phase I trials,
the alternative is simply not to participate
9. A statement describing the extent, if any, to which
confidentiality of records identifying the subject
will be maintained
Disclose what will be shared with pharmaceutical companies,
NIH, or regulatory agencies
10. For research involving more than minimal risk, an
explanation as to whether any compensation, and an
explanation as to whether any medical treatments
are available, if injury occurs and, if so, what they
consist of, or where further information may be obtained
The sponsor of the study may have more limited compensation
than your institution provides. This should be disclosed
11. An explanation of whom to contact for answers
to pertinent questions about the research and research
subjects’ rights, and whom to contact in the event of a
research-related injury to the subject
When a research subject is asked to participate in a long study,
it may be necessary to have sub-investigators who can
respond 24/7
12. A statement that participation is voluntary, refusal to
participate will involve no penalty or loss of benefits to
which the subject is otherwise entitled, and the subject
may discontinue participation at any time without penalty
or loss of benefits, to which the subject is otherwise entitled
If you are banking de-identified specimens, the limits of
withdrawal need to be disclosed
Editorial
� 2012 The Authors. Veterinary Anaesthesia and Analgesia322 � 2012 Association of Veterinary Anaesthetists and the American College of Veterinary Anesthesiologists, 39, 321–323

Francis et al. (2007) where human albumin was
administered to six otherwise healthy dogs and two
of them died! It is suggested that investigators who
are looking for such subjects from their local
community do it by posters or impersonal adver-
tisements but that they do not directly solicit the
owners so that there is less likelihood of direct
inducement (Schwenzer 2011). It is interesting
that in studies that look at attitudes to rewards for
altruistic behavior, the application of a monetary
reward to something may decrease the likelihood of
participation (Heffernan 2011).
Journal editors are put in the role of arbiters on
this subject because the rules that govern this issue
vary considerably from country to country and
what may seem to be an acceptable use of animals
in one country is abhorrent or even illegal in
another. Ethics committees in different establish-
ments, even within the same country, may interpret
the rules differently. This is an international journal
and we will try to publish articles that meet the
highest ethical principles. This means that as
authors we have to use high standards in our daily
practice and get informed owner consent if there is
any question that we are deviating from the
excellent care we all try to provide for our subjects
and patients.
To return to Mr Flaherty’s example, his study was
both legal and ethical from the point of view of the
excellent care given to the animals. His ethics
committee considered that it did not need informed
owner consent. If this had been a study using human
subjects, informed patient consent would have been
mandatory. In view of the recently published IAVE
and RCVS guidelines, his ethics committee might
come to a different conclusion today.
Peter J Pascoe & KW Clarke
E-mail: [email protected];
References
Francis AH, Martin LG, Halsorson GJ et al. (2007) Adverse
reactions suggestive of type III hypersensitivity in six
healthy dogs given human albumin. J Am Vet Med
Assoc 230, 873–879.
Heffernan M (2011) Wilful Blindness: Why We Ignore the
Obvious At Our Peril. Walker, New York, NY, USA.
RCVS (2012a) http://www.rcvs.org.uk/advice-and-guid
ance/code-of-professional-conduct-for-veterinary-surgeons/
supporting-guidance/use-and-re-use-of-samples-images-
post-mortems-and-disposal/ Paragraphs 12.1, 12.2, 12.8
RCVS (2012b) http://www.rcvs.org.uk/advice-and-guid
ance/code-of-professional-conduct-for-veterinary-surgeons/
supporting-guidance/recognised-veterinary-practice/
Paragraphs 25.7, 25.18, 25.19, 25.20, 25.21.
Schwenzer KJ (2011) Best practice & research in anaes-
thesiology issue on new approaches in clinical research
ethics in clinical research. Best Pract Res Clin Anaesthiol
25, 569–582.
Editorial
� 2012 The Authors. Veterinary Anaesthesia and Analgesia� 2012 Association of Veterinary Anaesthetists and the American College of Veterinary Anesthesiologists, 39, 321–323 323





























