Embed Size (px)
Citation preview

INFO LINK
Your local pathology providerDelivering quality comprehensive clinical and laboratory services for all your pathology needs
AUTUMN 2010
www.palms.com.au
InsIde thIs Issue
• haemoglobin A1c – A new era
• Lab tests Online
23Issue twenty three
09875 Infolink 23.indd 1 22/4/10 12:04:52 PM

ISSUE TWENTY THREE
09875 Infolink 23.indd 2 22/4/10 12:04:53 PM

I would like to take this opportunity to introduce myself as the Assistant Director, Pathology North, Pacific Laboratory Medicine Services (PaLMS).
The hospital, community and corporate based public pathology model of Pathology North delivers efficiencies across all areas due to economies of scale, access to Consultant Pathologist and Clinical Scientist expertise, and state-of-the-art equipment with advanced technologies.
We offer access to affordable care with our fee policy based on the Government’s Medicare fee schedule. Unlike many of our commercial and corporate pathology competitors, we do not charge individual patients a co-payment or a premium above the Schedule Fee. We continue to accept bulk-billing or Medicare-rebate-only for our patients. We look forward to working with you as your local pathology provider and we welcome your contact and support.
Our feature article is A New Era, Haemoglobin A1c (HbA1c ). Since its identification over 50 years ago HbA1c has come to be essential in the assessment of glycaemic control for all diabetic patients. Even though HbA1c has been used for assessing diabetes control, agreement as to how the assay will be standardised internationally has only recently been decided.
This issue of Infolink provides a timely opportunity to examine HbA1c’s role in the assessment of glycaemic control and the appropriate HbA1c targets for diabetic patients. The circumstance in which an HbA1c assay may give a misleading impression of a patient’s glycaemic control is also a significant issue which will be discussed.
The article identifies that it is essential that the results reported by Australian laboratories can be directly compared with the HbA1c measurements from the international laboratories involved in the studies used to set the guidelines. Given these considerations, it may seem surprising that Australia has had no formal program of HbA1c assay standardisation.
Pathology tests are an integral and vital part of the healthcare chain and PaLMS is thrilled to be working with Lab Tests Online. The Commonwealth Department of Health and Ageing has recognised that the better informed patients are the more they can participate in the management of their health care. They have subsequently funded Lab Tests Online for the past three years. Lab Tests Online can also be useful for doctors personally or by passing the website on to their patients to assist with questions about their tests.
We will be distributing the patient flyer in our collection centres to give patients access to information about the pathology tests they are having.
Welcome to the Autumn 2010 edition of Infolink
1Info Link, PaLMS
Dr. Tom Kennedy
Assistant Director Pathology North Pacific Laboratory Medicine Services (PaLMS) Northern Sydney, Central Coast MBBS (Monash) MBA (Tas) MClinEpid (Newcastle) FRCPA
ISSUE TWENTY THREE
09875 Infolink 23.indd 3 22/4/10 12:04:54 PM

Lab Tests Online (LTO) Australasia is a free, non commercial web site that gives patients and their carers impartial and accurate information about the pathology tests and screenings that underpin their healthcare.
It’s also a very useful tool for healthcare professionals wanting to help guide patients through the maze of often conflicting, confusing and sometimes commercially skewed information on the internet that can sometimes not be supportive of the diagnostic and clinical decisions being made by the doctor.
The material on Lab Tests Online Australasia has been prepared by pathologists and scientists working in diagnostic laboratories and it has been peer reviewed by an editorial board. It has also been reviewed to make sure that it is easy to understand. The site covers a comprehensive range of pathology, and includes some of the less common tests. New material is being added all the time.
Through a series of cross referenced lists of diseases and conditions, and tests and screens it’s easy to find out what tests are used and why; how the sample is taken, what is being tested and what the results mean.
Links are also provided to websites deemed reliable and useful by the editors.
Developed by the Australasian Association of Clinical Biochemists with support from the Royal College of Pathologists of Australasia, all information is specific to Australia and New Zealand and in line with our health systems.
Lab Tests Online was pioneered in America in 2001 and a sister service was started in the UK in 2004. LTO is now Google’s top-ranking US site for health information. It also won the Communicators Award from the International Academy of the Visual Arts (IAVA) in America.
Please note: the information contained in LTOAu is not to be regarded as a substitute for professional medical advice from a GP or specialist doctor. The aim is to help both patient and medical professional by ensuring that the information accessed on-line by the patient is accurate
labtestsonline.org.auPamela Robson Marketing Manager LTO
2 Info Link, PaLMS
You are invited to a presentation and lunch
Labtests OnlineHelping patients and consumers understand their lab tests
Presented by:
dr Andrew st John Dr. Andrew St John is a clinical biochemist, having worked in laboratories in the UK and Australia. Since joining the IVD industry he has worked in Australia, Asia and Europe for various companies
and is now the Regional Business Development Manager for Ortho Clinical Diagnostics in the Asia Pacific region. On behalf of the Australasian Association of Clinical Biochemists he has been
instrumental in establishing an Australian version of Lab Tests Online.
WHEN: 30th June 12:30 pm– 1:45 pm
WHERE: Wallace Freeborn Lecture Theatre, Kolling Institute of Medical Research Royal North Shore Hospital Pacific Hwy, St Leonards
RSVP: Rita Castles – [email protected] or 8425 3126
ISSUE TWENTY THREE
09875 Infolink 23.indd 4 22/4/10 12:04:54 PM

Dr Christopher Farrell graduated from University of New South Wales with MBBS in 2004. He then worked at Bankstown-Lidcombe Hospital as an Intern and Resident Medical Officer (2005 & 2006), completing terms in cardiology, aged care, emergency and intensive care. Dr Farrell commenced working for PaLMS in 2007 as a Clinical Biochemistry Registrar on the Emil von Behring Scholarship and subsequently on a scholarship from Siemens Diagnostics. In 2009 he was awarded membership to the Australiasian Association of Clinical Biochemists and received the 2009 examination prize. While at PaLMS he has spent time in a number of the laboratories including express biochemistry, endocrinology, renal and trace elements. He has found the benefit of working for PaLMS is having access to the latest technology in clinical chemistry.
Phone: 9926 5530 Email: [email protected]
Haemoglobin a1c: a new era Haemoglobin A1c (HbA1c ) has been used for assessing diabetes control for over 30 years1. However, agreement as to how the assay will be standardised internationally has only been reached recently. PaLMS has implemented the changes necessary to bring HbA1c results into line with this international standardisation effort.
This issue of Infolink provides a timely opportunity to examine HbA1c’s role in the assessment of glycaemic control and the appropriate HbA1c targets for diabetic patients. The circumstances in which an HbA1c assay may give a misleading impression of a patient’s glycaemic control is also a significant issue which will be discussed.
In addition, the importance of standardising HbA1c measurements and how standardisation is being achieved will be considered. Understanding a number of relevant points regarding the standardisation process will assist the clinician to draw the maximum information from laboratory reports. Finally, we will examine some of the ways in which HbA1c standardisation is being exploited: the calculation of an average glucose concentration and a possible role in diabetes diagnosis.
Hba1c in tHe assessment of glycaemic control: background
Haemoglobin A1c is formed by the non-enzymatic condensation of glucose with the adult haemoglobin molecule. HbA1c was first identified in 1958 by chromatography of haemoglobin2. In this technique, the glucose attached to the haemoglobin molecule covers a positive charge at one of a number amino acid residues and causes the glycated haemoglobin to move through a negatively charged chromatographic column more rapidly than the non-glycated haemoglobin. Thus HbA1c as first identified represented a mixture of slightly different glycated haemoglobin molecules.
Two main processes govern the dynamics of HbA1c formation. First is the glucose concentration to which the haemoglobin is exposed. The membrane of red blood cells is freely permeable to glucose and therefore the venous glucose concentration provides an accurate indicator of this parameter at any given point in time. Second is the duration over which the haemoglobin experiences this glucose concentration. This parameter is influenced by the lifespan of red cells in vivo. There is no ready laboratory measure of this parameter and the assumption is made that the red cell lifespan is constant between patients. This assumption is valid for the vast majority of patients. However, the assumption does not hold for patients with conditions that alter red cell turnover, as discussed below.
Unsurprisingly, after HbA1c’s identification evidence accumulated relatively rapidly that it was elevated in diabetic patients and that the degree of glycaemic control determined its levels. Moreover, randomised control trial evidence revealed that improving glycaemic control, reflected in a lowering of HbA1c , improved patient outcomes.
Haemoglobin A1c: A New Era
3Info Link, PaLMS
Dr Christopher Farrell
ISSUE TWENTY THREE
09875 Infolink 23.indd 5 22/4/10 12:04:57 PM

4 Info Link, PaLMS
Both the Australian Diabetes Society and the NHMRC have published guidelines for glycaemic targets on the basis of the accumulating evidence 5,11. Both these documents represent a move to a more individualised approach to the setting of treatment targets for diabetics. Indeed, as evidence continues to accrue it is likely that glycaemic targets will become increasingly individualised.
The guidelines reconfirm that HbA1c ≤7.0% remains the general target for both type 1 and 2 diabetes. However, tighter control is recommended for patients with type 2 diabetes of short duration, without cardiovascular disease who do not require insulin therapy. Conversely, a target of ≤8.0% is advised for patients with recurrent severe hypoglycaemic episodes or hypoglycaemic unawareness. The HbA1c targets from the ADS position statement are given in tables 1 and 2.
Hba1c in tHe assessment of glycaemic control: Hba1c targetsTraditional glycaemic targets for type 1 and type 2 diabetic patients have been largely based on data from the Diabetes Control and Complications Trial (DCCT)3 and UK Prospective Diabetes Study (UKPDS)4, respectively. In both these studies, the intensively managed groups had mean HbA1c concentrations of approximately 7.0%. These intensively managed patients had better outcomes in terms of both microvascular complications and, at longer-term follow-up, macrovascular complications.
Significantly, both these trials demonstrated that a period of good glycaemic control had long-lasting benefits for patients. After the conclusion of both the DCCT and UKPDS, all patients were managed to the same glycaemic targets and followed-up for approximately 10 years. These observational studies showed that those who were managed with tight glycaemic control during the primary studies had improved microvascular and macrovascular outcomes some 10 years later 5,6.
Post hoc analysis of data from the DCCT and UKPDS, as well as epidemiological evidence, have suggested that glycaemic control even tighter than that achieved in the DCCT and UKPDS may improve patient outcomes 7,8. These data show that microvascular and macrovascular complications are reduced for each 1% reduction in HbA1c , with no threshold effect. Recently a number of trials have been published which aimed to examine the effect of very tight glycaemic control on outcomes in type 2 diabetes (ACCORD9, ADVANCE10, and VADT11). The results of these trials were mixed and they highlight both significant benefits and risks of very tight glycaemic control. Furthermore, they show that the risk/benefit profile varies between different patient subgroups. The implication, therefore, is that an individualised approach to glycaemic targets is likely to be the optimal strategy for managing patients with diabetes.
ISSUE TWENTY THREE
09875 Infolink 23.indd 6 22/4/10 12:04:57 PM

5Info Link, PaLMS
table 1: recommended glycated haemoglobin (Hba1c) target ranges for adults with type 2 diabetes
HbA1c target Rationale for recommendation
Level of evidence for target
General target ≤ 7.0%* UKPDS demonstrated improved outcomes with median HbA1c of ≤ 7.0%, result supported by NHMRC systematic review.
I
Specific clinical situations:
Diabetes of short duration† and no clinical cardivascular disease
• Requiring lifestyle modification ± metformin
≤ 6.0%* UKPDS showed early treatment of diabetes to be beneficial. In epidemiological studies, the threshold level of HbA1c beyond which increased mortality and cardiovascular events occur, lies between 5.0% and 6.0%. Risk of hypoglycaemia is negligible with lifestyle modification or melformin.
Consensus
• Requiring any antidiabetic agents other than metformin or insulin
≤ 6.5%* UKPDS showed early treatment of diabetes to be beneficial. Risk of hypoglycaemia increases with use of most antidiabetic agents other than metformin, hence we do not recommend a target HbA1c ≤ 6.0% for this group. ADVANCE demonstrated reduced microvascular disease with target HbA1c ≤ 6.5%.
II
• Requiring insulin ≤ 7.0%* UKPDS demonstrated improved outcomes with median HbA1c
II
Pregnancy or planning pregnancy
≤ 6.0%* Observational data (albeit mainly in type 1 diabetes) demostrate a relationship between HbA1c and adverse pregnancy outcomes when HbA1c levels exceed a threshold between 5.0% and 6.0%.
Consensus
Diabetes of longer duration† or clinical cardivascular disease (any therapy)
≤ 7.0%* UKPDS demonstrated improved outcomes with median HbA1c of ≤ 7.0%. ACCORD indicated attempts for even tighter control in people with relatively long duration of diabetes and cardiovascular disease were associated with increased mortality. We therefore do not routinely recommend tighter control in this group.
II
Recurrent severe hypoglycaemia or hypoglycaemia unawareness (any therapy)
≤ 8.0%* Severe hypoglycaemia is associated with significant morbidity and mortality. Risks of tight glycaemic control outweigh the benefits for such patients.
Consensus
Patients with major comorbidities likely to limit life expectancy† (any therapy)
Symptomatic therapy of
hyperglycaemia§
Tight glycaemic control will be of no benefit, as diabetic complications take many years to develop.
Consensus
ACCORD – Action to Control Cardiovascular Risk in Diabetes study: ADVANCE – Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation trial. NHMRC – National Health and Medical Research Council. UKPDS – United Kingdom Prospective Diabetes Study.* Achievement of HbA1c targets must be balanced against risk of severe hypoglycaemia, especially among older people. † In an older adult, Iong duration might be considered to be > 10-20 years, but for a person who develops type 2 diabetes at a
young age, it maybe considerably longer. ‡ Examples of major comorbidities include chronic medical conditions, such as chronic kidney disease stages 4 or 5; heart failure
stage III or IV (New York Heart Association grading); incurable malignancy; and moderate to severe dementia. § Where practical, suggest blood glucose target leve1 <15 mmol/L to help minimise risk of infection.
ISSUE TWENTY THREE
09875 Infolink 23.indd 7 22/4/10 12:04:58 PM

6 Info Link, PaLMS
limitations of Hba1c It is important for clinicians to appreciate circumstances where the HbA1c level may be misleading as to the degree of glycaemic control in a patient. Some of these circumstances are predictable on the basis of the mechanics of the glycation process itself. Other circumstances reflect analytical interferences that are rather unpredictable in terms of which methodologies they affect.
While HbA1c is measured to assess the glycaemic control in a patient, this is only one parameter influencing the HbA1c level. As outlined earlier, the other relevant parameter is the age of the red blood cells. Therefore, any condition that alters the red cell age profile will have a predictable effect on the HbA1c result independent of glycaemic control. Increased red cell breakdown, as in haemolytic conditions, will result in a decrease in HbA1c. Similarly, an increase in red cell production, such as following erythropoietin administration or immediately after treatment of vitamin B12 or folate deficiency. Conversely, conditions that tend to prolong red cell survival will lead to an increase in HbA1c. This may be seen in patients with untreated iron, vitamin B12 or folate deficiency. It is also of significance to note that following a blood transfusion, HbA1c measurements will not reflect the recipient’s glycaemic control until 1-2 months after the transfusion.
Variant haemoglobins, such as HbS, HbC and HbF, may also cause misleading HbA1c results. Some methodologies are affected by these variants and others are not. Whether a particular method suffers interference and whether the effect is to increase or decrease the HbA1c result is not predictable from first principles.
Chronic kidney disease exerts complex influences on HbA1c. Depending on the method used for measurement, there may be a false increase due to interference from carbamylated haemoglobin. Conversely, increased red cell turnover from dialysis and/or erythropoietin administration will tend to decrease HbA1c.
Vitamin C and E have been reported to lower results HbA1c by inhibition of the glycation process. 13,14 However, vitamin C may also cause direct interference with the measurement procedure of some assays and cause artefactually elevated results.
In summary, there are numerous factors that have the potential to influence HbA1c levels independent of glycaemic control and many of these depend on which assay is used for measurement. Therefore, it is advisable to discuss any anomalous HbA1c results with the testing laboratory for guidance on which conditions may be relevant for their particular assay.
table 2: recommended glycated haemoglobin (Hba1c) target ranges for adults with type 1 diabetes
HbA1c target Rationale for recommendation
Level of evidence for target
General target ≤ 7.0%* DCCT/EDIC showed that achieving a mean HbA1c of 7.0% is associated with improved outcomes.
II
Specific clinical situations:
Pregnancy or planning pregnancy
≤ 7.0%*† Better pregnancy outcomes (borderline significance) were achieved for intensive-therapy group of DCCT (mean HbA1c of 7.4%). Observational data demonstrate a relationship between HbA1c and adverse pregnancy outcomes when HbA1c levels exceed a threshold between 5.0% and 6.0%, but there is a heightened risk of hypoglycaemia at such low levels. Therefore, for most women, we recommend a target HbA1c ≤ 7.0%.
II
Recurrent severe hypoglycaemia or hypoglycaemia unawareness
≤ 8.0% Severe hypoglycaemia is associated with significant morbidity and mortality. Risks of tight glycaemic control outweigh the benefits for such patients.
Consensus
Patients with major comorbidities likely to limit life expectancy
Symptomatic therapy of
hyperglycaemia‡
and avoidance of ketosis
Tight glycaemic control will be of no benefit, as diabetic complications take many years to develop.
Consensus
DCCT – Diabetes Control and Complications Trial. EDIC – Epidemiology of Diabetes Interventions and Complications Study.* Achievement of HbA1c targets must be balanced against risk of severe hypoglycaemia. † An HbA1c level of ≤ 6.0% is desirable if it can be achieved safely.‡ Where practical, suggest blood glucose target leve1 <15 mmol/L to help minimise risk of infection.
ISSUE TWENTY THREE
09875 Infolink 23.indd 8 22/4/10 12:04:58 PM

7Info Link, PaLMS
conditions that may alter Hba1c• Haemolysis• Recovery from acute blood loss• Pregnancy• End-stage renal failure• Erythropoietin therapy• Vitamin B12 deficiency• Folate deficiency• Haemoglobin variants• Vitamin C• Vitamin E
tHe need for standardisationThe publication of HbA1c targets for diabetic patients assumes assay standardisation. That is, a patient will get the same HbA1c result regardless of the laboratory performing the analysis. Additionally, it is essential that the results reported by Australian laboratories can be directly compared with the HbA1c measurements from the international laboratories involved in the studies used to set the guidelines.
Given these considerations, it may seem surprising that Australia has had no formal program of HbA1c assay standardisation. However, because many laboratories purchase equipment from manufacturers from the United States, many Australian laboratories were inadvertently subject to the US standardisation program.
The US program is known as the National Glycohemoglobin Standardization Program (NGSP). This program is aimed at standardising HbA1c measurements to the assay used in the DCCT (and UKPDS). This approach is pragmatic but has significant flaws. For instance, the assay in these studies used a cation exchange chromatography method, the same principle as the technique first used to identify HbA1c. This technique measures a number of glycated haemoglobin molecules rather than a single specific molecule. Standardising all methods to measure an impure mixture of molecules is less than ideal.
The International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) took responsibility for establishing a theoretically sound system of standardisation. A consensus document was recently published by the major international diabetes bodies ratifying the system established by the IFCC for international implementation into clinical laboratories. This system ensures that patient results will be comparable regardless of where the assay was performed and that results can be equated with published guidelines and research papers. The way this program is constructed and will be implemented is described below.
How Hba1c is standardisedThe implementation of the IFCC system of standardisation will largely take place behind-the-scenes in clinical laboratories. However, appreciating a few salient points regarding this system will assist with understanding the various report formats that different laboratories may put out in the near future.
The IFCC system is based on the definition of HbA1c as a specific molecular species (the stable adduct of glucose at the N-terminal valine of the ß chain of adult haemoglobin) and the modern ability to specifically measure this molecule alone using mass spectrometry technology. Mass spectrometry can therefore be used to produce solutions of known concentration of HbA1c which can then be used to calibrate routine assays.
HbA1c results produced by IFCC-aligned assays have been showed to be lower than those that are NGSP-aligned. This is expected because the IFCC-based assays are standardised to measure the specific HbA1c molecule, while NGSP-based assays are standardised to measure a mixture of glycated haemoglobins. To help avoid confusion between the 2 systems, the decision was made to use different units for each system. Thus, results produced by each system will be quite different numerically. IFCC-aligned results will be reported in mmol of HbA1c per mol HbA (mmol/mol) while NGSP-aligned results will continue to be reported in the usual percentage units. Table 3 demonstrates how the numbers differ under the two systems.
To enable comparison of patient results with current guidelines, a ‘master equation’ has been established. The equation will be used to convert IFCC-aligned results to NGSP-equivalent results. The NGSP-equivalent results will continue to be reported in percentage units and can be interpreted, as previously, against current management guidelines. In fact, many Australian laboratories, including PaLMS, who have implemented the IFCC standardisation system are only currently reporting the NGSP-equivalent results. Therefore, the re-standardisation process is occurring behind-the-scenes. However, the IFCC, American Diabetes Association, European Association for the Study of Diabetes and the International Diabetes Foundation have all recommended the reporting of mmol/mol IFCC-aligned results in addition to NGSP-equivalent results. It is likely that as clinicians become more familiar with the IFCC system, more Australian laboratories will begin reporting IFCC-aligned results in mmol/mol.
ISSUE TWENTY THREE
09875 Infolink 23.indd 9 22/4/10 12:04:58 PM

8 Info Link, PaLMS
Hba1c derived average glucoseA ‘patient-friendly’ way to present an HbA1c result is as an estimated average glucose. An average glucose result helps the patient to understand the relationship between their level of glycaemic control and their HbA1c result. One of the major impediments to widespread reporting of an HbA1c-derived average glucose has been the lack of adequate standardisation. The establishment of the IFCC standardisation system has paved the way for routine reporting of an estimated average glucose concentration.
The results of the A1c-Derived Average Glucose (ADAG) study were recently published 16. This large study examined relationship between HbA1c and average glucose concentrations. The study included over 500 subjects with type 1 or type 2 diabetes mellitus as well as non-diabetic subjects. Approximately 2700 glucose measurements were made in each subject over a 3 month period and compared with their HbA1c level at the end the 3 months. The study successfully developed an equation relating HbA1c to average glucose concentration (AG = 1.59 x A1c – 2.59). Table 3 illustrates the estimated average glucose results for various levels of HbA1c. This equation was shown to be relatively robust to variations in gender, ethnicity and age. There is consensus that an estimated average glucose should now be reported whenever HbA1c is measured.13
However, there are a number of limitations of the study that must be appreciated when interpreting estimated average glucose results. Firstly, both individuals under the age of 18 years and pregnant women were excluded. Thus, the equation that was developed cannot be used to estimate an average glucose for either of these groups.
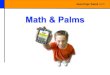
Secondly, the study demonstrated a considerable amount of scatter around the regression equation. The plot of HbA1c versus average glucose concentration from the study in Figure 1 illustrates this scatter. The researchers noted that 90% of HbA1c-derived average glucose results fell within ±15% of the measured average glucose concentration. Table 3 demonstrates how this scatter translates into 95% confidence intervals for any one estimate of average glucose. The amount of scatter present emphasises that the average glucose result is truly an ‘estimate’. Its value lies in helping patients understand their HbA1c results.
However, from the clinician’s point-of-view, appreciating how much scatter is expected from the estimation equation may assist in deciding whether an HbA1c result and a patient’s glucometer readings are discordant.
Finally, it is imperative not to lose sight of the fact that all the limitations of HbA1c assay discussed earlier apply equally to the estimated average glucose concentration. Therefore, changes in red cell turnover as well as analytical interference in HbA1c assays may cause misleading estimated average glucose results.
figure 1: a1c assat and estimated glucose values
table 3
HbA1c -NGSP (%)
HbA1c - IFCC
(mmol/mol)
Average Glucose (mmol/L)
95% Confidence Internal of
Average Glucose Estimation
5
6
7
8
9
10
11
12
31
42
53
64
75
86
97
108
5.4
7.0
8.6
10.2
11.8
13.4
14.9
16.5
4.2 - 6.7
5.5 - 8.5
6.8 - 10.3
8.1 - 12.1
9.4 - 13.9
10.7 - 15.7
12.0 - 17.5
13.3 - 19.3
ISSUE TWENTY THREE
09875 Infolink 23.indd 10 22/4/10 12:04:59 PM

Hba1c and diabetes diagnosisA potential future role for HbA1c is in the diagnosis of diabetes. One of the major barriers to the use of HbA1c for the diagnosis of diabetes has been a lack of standardisation. Now that standardisation has been addressed, HbA1c’s potential utility in diagnosis has been reignited as an issue.
The enthusiasm for using HbA1c for diabetes diagnosis is based on a number of clear practical and technical advantages over the use of glucose-based criteria. Firstly, HbA1c can be collected from non-fasting patients. HbA1c is also relatively unaffected by intercurrent illnesses that may raise glucose concentrations and confound their diagnostic interpretation. Furthermore, HbA1c is at least as tightly correlated as fasting glucose concentration with risk of microvascular complications. From a technical point-of-view, HbA1c is considerably more stable in vitro, exhibits less biological variation and there is better standardisation of assays.
Citing these advantages, an International Expert Committee has recommended the use of HbA1c for diabetes diagnosis. The Committee, with members from the American Diabetes Association, the European Association for the Study of Diabetes and the International Diabetes Federation, has recommended that an HbA1c ≥6.5% be used to define diabetes. A repeat HbA1c would be necessary to confirm the diagnosis unless the patient was symptomatic and had a glucose concentration ≥11.1mmol/L. The 6.5% cut-off was chosen on the basis of the level at which risk of retinopathy begins to increase appreciably.
The Committee also recommended that individuals with HbA1c levels in the range 6.0-6.4% be targeted with interventions aimed at preventing the development of diabetes. However, other risk factors for diabetes should be taken into account when identifying those at increased risk of developing diabetes. These include elevated triglycerides, blood pressure and BMI as well as a family history of diabetes. The use of validated risk assessment tools, such as the Australian Type 2 Diabetes Risk Assessment Tool (AUSDRISK), may help identify those at increased risk.
AUSDRISK is available at http://www.health.gov.au/internet/main/publishing.nsf/Content/C73A9D4A2E9C684ACA257473 0002A31B/$File/Risk_Assessment_Tool.pdf or via a number of online calculators).
Despite international enthusiasm, HbA1c has a number of shortcomings with regard to diabetes diagnosis. A major disadvantage of HbA1c is increased cost compared to glucose measurement; this would preclude its use in many parts of the world. Furthermore, all the limitations of HbA1c measurement relevant to the assessment of glycaemia, as discussed previously, would also confound diabetes diagnosis. Foremost among these are conditions that change red cell turnover and haemoglobinopathies. The state of pregnancy alters red cell turnover and diagnosis of gestational diabetes would have to remain on the basis of glucose measurement. Additionally, the situation may rarely arise in which the onset of type 1 diabetes is so acute that the HbA1c may not have time to reach the diagnostic level despite very high glucose concentrations.
The relative merits of the use of HbA1c in the diagnosis of diabetes will likely lead to debate for some time yet. However, it is likely that HbA1c will have a role in diabetes diagnosis in the near future, either alone or in some combination with glucose.
conclusionSince its identification over 50 years ago HbA1c has come to be essential in the assessment of glycaemic control for all diabetic patients. From an initial one-size-fits-all approach, guidelines are beginning to promote a more individualised approach to the setting of glycaemic targets in diabetic patients. This trend is likely to continue as the evidence-base continues to grow as to which glycaemic targets are optimal for particular groups of patients. Standardisation of HbA1c measurement is essential in enabling an individual’s HbA1c result to be comparable to the published guidelines.
HbA1c also provides an example of how standardisation facilitates the incorporation of research data into routine practice. PaLMS is able to report an HbA1c
-derived average glucose concentration by using the equation developed in the large ADAG study because of the international standardisation of HbA1c measurement. Additionally, the use of a standardised HbA1c measurement for the diagnosis of diabetes provides a likely advance in the identification of this common condition in the near future.
9Info Link, PaLMS
ISSUE TWENTY THREE
09875 Infolink 23.indd 11 22/4/10 12:04:59 PM

10 Info Link, PaLMS
1 John WG. Haemoglobin A1c: Analysis and standardisation. Clin Chem Lab Med 2003; 41: 1199-1212.
2 Allen DW, Schroeder WA, Balog J. Observations on the chromatographic heterogeneity of normal adult and foetal haemoglobins. A study of the effects of crystallisation and chromatography in the heterogeneity and isoleucine content. J Am Chem Soc 1958; 80: 1628-1634.
3 The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329: 977-986.
4 UK Prospective Diabetes Study (UKPDS) Group. Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837-853.
5 Nathan DM, Cleary PA, Backlund JY, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005; 353: 2643-2653.
6 Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008; 359: 1577-1589.
7 Khaw KT, Wareham N, Bingham S, et al. Association of hemoglobin A1c with cardiovascular disease and mortality in adults: The European prospective investigation into cancer in Norfolk. Ann Intern Med 2004; 141: 413-420.
8 Selvin E, Marinopoulos S, Berkenblit G. Meta-analysis: Glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med 2004; 141: 421-431.
9 Gerstein HC, Riddle MC, Kendall DM, et al. Glycemia treatment strategies in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Am J Cardiol 2007; 99:34i-43i.
10 Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) Collaborative Group. Intensive Blood Glucose Control and Vascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2008; 358:2560-2572.
11 Abraira C, Duckworth WC, Moritz T. Glycaemic separation and risk factor control in the Veterans Affairs Diabetes Trial: an interim report. Diabetes Obes Metab 2009 Feb;11:150-156.
12 Colagiuri S, Dickinson S, Girgis S, Colagiuri R. National evidence based guideline for blood glucose control in type 2 diabetes. Diabetes Australia and the NHMRC, Canberra 2009.
13 Davie SJ, Gould BJ & Yudkin JS. Effect of vitamin C on glycosylation of proteins. Diabetes 1992; 41: 167-173
14 Ceriella A, Giugliano D, Quatraro A, et al. Vitamin E reduction of protein glycosylation in diabetes. New prospect for prevention of diabetic complications? Diabetes Care 1991; 14: 68-72
15 The American Diabetes Association, European Association for the Study of Diabetes, International Federation of Clinical Chemistry and Laboratory Medicine, & International Diabetes Association. Consensus statement on the worldwide standardization of the haemoglobin A1c measurement. Diabetes Care2007; 30: 2399-2400.
16 Nathan DM, Kuenen J, Borg R, et al. Translating the A1c assay into estimated average glucose values. Diabetes Care 2008; 31: 1473-1478.
17 The International Expert Committee. International Expert Committee report on the role of the A1c assay in the diagnosis of diabetes. Diabetes Care 2009; 32: 1327-1334.
ISSUE TWENTY THREE
09875 Infolink 23.indd 12 22/4/10 12:04:59 PM

Issue Twenty TwoTrace Elements in Health and Disease PaLMS Toxicology
Issue Twenty OneCytogenetic advances in the detection of prognostic factors in B cell malignancies, Trace Elements in Health and Disease
Issue Twenty Human Papilloma Virus, Expanding Molecular Biology
Issue Nineteen B-type Natriuretic Peptide (BNP)
Issue Eighteen Down Syndrome – Population Screening
Issue Seventeen, Anti-Neutrophil Cytoplasmic Antibodies – ANCA
Issue Sixteen,Changes in the use of RH D immunoglobin products in Australia: Introduction of Antenatal Prophylaxis
Issue Fifteen,Laboratory Diagnosis for Infection with Human Immunodeficieny Virus (HIV)
Issue Fourteen,Hereditary Haemochromatosis Infectious Mononucleosis
Issue Thirteen,ThrombophiliaFaecal Occult Blood Testing
Issue Twelve,Acute Phase ResponseNew Targeted Treatment for CML
Issue Eleven, Laboratory Markers of Bone Metabolism
Issue Ten, Thyroid Function Tests – Dead Easy or Impossible
Issue Nine, Synovial Fluid Analysis in the Investigation of Arthritis
Issue Eight, The Biopsy Diagnosis of Gastritis
Issue Seven, Diabetes Mellitus
Issue Six, New Markers for Coronary Artery Diseases
Issue Five,Laboratory Investigation of the Small, Pale Red Cell: Microcytic, Hypochromic Anaemia
Issue Four, Auto-Antibodies in Connective Tissue Diseases
Issue Three, Laboratory Tests to Detect Allergiv Reactions to Drugs
Issue Two, Investigation of Hypertension
Issue One, Important Concepts in Laboratory Utilisation
Visit the PaLMS Web site at www.palms.com.au to view past issues or contact PaLMS Marketing on (02) 8425 3127 for a copy to be sent to you.
Past Issues
11Info Link, PaLMS
ISSUE TWENTY THREE
09875 Infolink 23.indd 13 22/4/10 12:04:59 PM

Infolink Mailout and Change of DetailsPlease select the relevant box and fill in the details below:
I would like to:
Be included in the Infolink mail out (please fill in details below)
Change my current details (please fill in details below)
Be removed from the Infolink mail out
Name: .............................................................................................................................................................
Telephone: .....................................................................................................................................................
New Details
Title: ...............................................................................................................................................................
Name: .............................................................................................................................................................
Position: .........................................................................................................................................................
Provider Number: ..........................................................................................................................................
Speciality area: ..............................................................................................................................................
Business Name: ..............................................................................................................................................
Address: .........................................................................................................................................................
Phone: ............................................................................................................................................................
Fax: .................................................................................................................................................................
Email: .............................................................................................................................................................
Please photocopy this page and fax to Vicki Johnston,
PaLMS Marketing and Communication Manager (02) 9437 1477
Or send an email: [email protected]
12 Info Link, PaLMS
ISSUE TWENTY THREE
09875 Infolink 23.indd 14 22/4/10 12:05:00 PM

09875 Infolink 23.indd 15 22/4/10 12:05:00 PM

16
[email protected] NO: 09875
Northern SydneyEnquiries 9926 6066 or 1300 30 PaLMS
ChatswoodKatherine Street Medical Centre Unit 235, 1 Katherine Street Chatswood NSW 2067 Ph: (02) 9411 8197 Monday to Friday: 8.00am to 4.30pm
Dee Why Unit 1 "Seascape" 22-26 Fisher Road Dee Why NSW 2099 Ph: (02) 9982 9433 Monday to Friday: 8.30am to 5.00pm
Eastwood / Ryde HospitalDenistone Road, Eastwood Ryde NSW 2122 Ph: (02) 9858 7542 Monday to Friday: 8.00am to 4.30pm Saturday: 9.00am to 12.00 midday
Frenchs ForestBuilding 1, Level 2 Frenchs Forest Road Frenchs Forest NSW 2086 Ph: (02) 9453 0210 Monday to Friday: 8.00am to 4.30pm
Hornsby Ku-ring-gai HospitalAdj. Main Entrance Palmerston Rd Hornsby NSW 2077 Ph: (02) 9477 9537 Monday to Friday: 8.30am to 5.00pm Saturday: 8.30am to 12.00 midday
Manly HospitalWest Wing, Darley Road Manly NSW 2095 Ph: (02) 9976 9686 Monday to Friday: 8.00am to 4.30pm Saturday: 9.00am to12.00 midday
Mona Vale HospitalLevel 2, Coronation Street Mona Vale NSW 2103 Ph: (02) 9998 0278 Monday to Friday: 8.00am to 4.30pm Saturday: 9.00am to 12.00 midday
Neutral BaySuite 3, 5 Waters Road Neutral Bay NSW 2089 Ph: (02) 8969 6157 Monday to Friday: 8.30am to 5.00pm Saturday: 9.00am to 12.00 midday
St Leonards North Shore Private HospitalPaLMS Collection Suite, St Leonards NSW 2065 Ground Floor, Westbourne St Ph: (02) 8425 3066 Monday to Friday: 8.00am to 6.00pm Saturday: 9.00 to 1.00pm
St Leonards Royal North Shore HospitalClinic 13, Outpatient Department, Level 3, Pacific Highway St Leonards NSW 2065 Ph: (02) 9926 7557 Monday to Friday: 8.30am to 5.00pm
Central CoastEnquiries (02) 4230 3375
Gosford Hospital
central coast specialist centre Holden Street Gosford NSW 2250 Ph: (02) 4320 5607 Monday to Thursday: 9.00am to 3.00pm
outpatient department Level 3, Holden Street Gosford Hospital Ph: (02) 4320 3767 Monday to Friday: 8.00am to 4.00pm
Wyong Hospital
Pathology Collection Centre (near Outpatients Clinic) Pacific Highway Wyong NSW 2259 Ph: (02) 4394 7554 Monday to Friday: 8.00am to 2.00pm
For further information visit www.palms.com.au or www.pathologynorth.com.au
PaLMS COLLECTION FACILITIES
09875 Infolink 23.indd 16 22/4/10 12:05:01 PM