Embed Size (px)
Citation preview

6.2: Pandemic Influenza
Priority Medicines for Europe and the World"A Public Health Approach to Innovation"
Background Paper
Preparing for Pandemic Influenza:A Research Agenda for the European
Union During the Interpandemic Period
This chapter has been compiled by David S. Fedson, M.D. in collaboration with the Global Influenza Programme
11 October 2004
6.2-1

6.2: Pandemic Influenza
Table of Contents
1. Executive Summary.....................................................................................32. Background.................................................................................................63. Burden of Disease.......................................................................................8
3.1. The Influenza Virus........................................................................................83.2. Interpandemic Influenza: The Burden of Disease..........................................83.3. Avian Influenza: Increasing the Risk for a Pandemic.....................................93.4. Pandemic Influenza and its Potential Impact on Europe and the World......10
4. Prevention and Control of Influenza.........................................................114.1. The Current Control Strategy and its Effectiveness.....................................11
4.1.1...............................................................................Influenza Vaccination11
4.1.2........................................................................................Antiviral Agents11
4.1.3..................................Use of Vaccines and Antivirals During a Pandemic12
4.1.4.......................................................................Non-Medical Interventions13
4.2. Current Implementation of the Control Strategy.........................................144.2.1. The Interpandemic Use of Influenza Vaccine in Europe and the Rest of the World......................................................................................................144.2.2........The Interpandemic Use of Antivirals in Europe and the Rest of the World............................................................................................................184.2.3.............................................................Affordability of the Interventions
185. Constraints to a Better Control.................................................................19
5.1. Interpandemic Period...................................................................................195.2. Pandemic Period...........................................................................................20
5.2.1...................................................Limitations of the Vaccination Strategy20
5.2.2........................................................Limitations of the Antiviral Strategy21
6. Lessons Learned from Research into Pharmaceutical Interventions.......226.1. Vaccination Strategies.................................................................................226.2. Reverse Genetics..........................................................................................256.3. Existing Research Resource Flows...............................................................26
7. Pipeline of Products..................................................................................277.1. Pipeline for Influenza Vaccines....................................................................277.2. Pipeline for Antiviral Agents........................................................................297.3. About Safety and Efficacy of Products in the Pipeline.................................30
8. Research into New Pharmaceutical Interventions....................................318.1. Vaccines with Broad Spectrum and Long Lasting Immunity........................318.2. Newer Antiviral Agents................................................................................338.3. Other Pharmaceuticals.................................................................................338.4. Institutions and Human Resources..............................................................34
9. Gaps and Opportunities for Pharmaceutical Research.............................349.1. Research to Be Carried Out in 5 Years.........................................................35
9.1.1...................................................................................................Vaccines35
9.1.2........................................................................................Antiviral Agents35
9.1.3.................................................................Non-Pharmaceutical Research36
9.1.4.............................................................................Translational Research38
9.2. Research to be Carried Out in the Longer Term..........................................38
6.2-2

6.2: Pandemic Influenza
9.3. Research in Need for Increased Support.....................................................399.4. The Comparative Advantage of the EU........................................................40
10. References............................................................................................................42
Appendix
6.2-3

6.2: Pandemic Influenza
1. Executive SummaryThe threat of a new influenza pandemic, its potential impact on health and the social and economic life of nations are clearly recognized by World Health Organization and the European Union. The key strategies to prepare for a pandemic have been adopted by the Member States of both organizations. Although all agree that vaccines and antiviral agents will be the only reliable interventions for reducing the morbidity and mortality of a pandemic, current vaccines and antivirals and have several disadvantages and supplies of both will be severely limited.
Annual outbreaks of influenza are due to minor changes in the virus that enable it to evade the immunity humans have developed following previous infection or vaccination. For this reason, the vaccine needs to be reformulated each year and vaccination must be repeated. Occasionally, one or more genes will be replaced by the genes of another (often avian) influenza virus. When this occurs, most people will have little or no immunity to this new virus. If it can be efficiently transmitted from one person to the next, a new pandemic will emerge.
Outbreaks of influenza in animals, especially when they occur simultaneously with annual outbreaks in humans, increase the chance that genes from the two viruses will reassort and produce a new pandemic virus. During the past few years, the world has experienced several outbreaks of avian influenza that have resulted in human infections. These events remind us that the arrival of the next pandemic is just a matter of time.
The impact of the next pandemic will depend on the infectivity and virulence of the pandemic virus. Mortality estimates for the next pandemic have ranged from 2-7 million deaths, and for a 1918-like pandemic could reach 175 to 350 million. Even with the most conservative estimates, millions of people will become seriously ill or die. Compared with the relatively small number of cases of SARS and their focused social and economic impact, one can expect the worldwide impact of the next influenza pandemic to be far greater.
The main strategy for controlling seasonal epidemics of influenza is yearly vaccination of high-risk individuals. Although vaccination is considered cost-effective in developed countries, vaccine uptake remains low in many of these countries. In developing countries, basic information on the burden of disease does not exist, making it difficult for policymakers to justify programmes for influenza prevention and control. Low vaccine uptake is mirrored by the world’s vaccine production capacity. Approximately 300 million doses of the current inactivated trivalent influenza vaccine are produced each year, two-thirds of them by companies located in the European Union. These European companies provide virtually all of the doses of influenza vaccine used in countries that do not have influenza vaccine companies.
Antiviral agents reduce severity and duration of influenza but due to high prices they are little used. As a result, the current supply and production capacity for these agents is severely limited.
These shortcomings in vaccine and antiviral supply will become evident when the next pandemic emerges. It will take several months before full-scale pandemic vaccine production can begin. Because countries with influenza vaccine companies can be expected to delay or prohibit the export of pandemic
6.2-4

6.2: Pandemic Influenza
vaccines until their domestic needs have been met, countries without vaccine production facilities will be unable to obtain supplies of pandemic vaccines. Unlike vaccines, antiviral agents could be stockpiled in advance, but stockpiles will be limited because of their high cost and uncertainty regarding the effectiveness of these agents. Interventions other than vaccines and antivirals might delay transmission of a pandemic virus, but would unlikely interrupt its global transmission.
In order to overcome limitations in the supply of pandemic vaccines, several options have been explored. The results show that compared with current trivalent inactivated vaccines, monovalent pandemic vaccines formulated with a low antigen dosage and including a commonly available adjuvant could increase the number of doses of pandemic vaccine that could be produced by 12- to 24-fold. These findings offer the best hope for producing an adequate supply of pandemic vaccines for Member States of the European Union and for other countries throughout the world.
Reverse genetics provides a rapid and safe alternative to traditional genetic reassortment for preparing seed strains for pandemic vaccine production. However, the use of reverse genetics is constrained by issues regarding intellectual property rights and public concern about the use of ‘genetically modified organisms’. In order to take full advantage of this important technology, these issues must be resolved as soon as possible.
In order to guarantee rapid licensing of pandemic vaccines, the European Medicines Evaluation Agency (EMEA) has issued guidelines for vaccine manufacturers on how to prepare a pandemic vaccine dossier. The dossier is based on a ‘mock-up’ vaccine that could contain the highly pathogenic avian H5N1 influenza strain currently causing widespread disease in Asia. Although a reverse genetics-engineered vaccine seed strain has been offered free-of-charge to all manufacturers, the companies have little or no incentive to invest in costly clinical trials of a vaccine they will never market. In the United States, the NIH is currently providing public funding for such clinical trials. Although the vaccine formulations the NIH will test will not allow for greatly expanded production of pandemic vaccines to meet global demand (they will not be low-dose, adjuvanted preparations), Europeans should recognize that public funding will be necessary if clinical trials of pandemic vaccines are to be undertaken in Europe.
The recent introduction of an intra-nasally administered live-attenuated influenza vaccine in the US (but not yet in Europe) is promising, but this vaccine is unlikely to have much impact on the influenza vaccine market in Europe for several years. A more long-term research strategy should include studies of vaccines targeting one of several highly conserved virus antigens that induce broad spectrum and long-lasting protection.
The EU currently provides modest support for the developing human influenza vaccines: €2.1 million for FLUPAN and €1.76 million for NOVAFLU. The US government has committed a far larger amount (at least $50-100 million, if not more) to this research. However, even in the US investment in pandemic vaccine development is modest compared with investments in developing vaccines for other diseases.
6.2-5

6.2: Pandemic Influenza
In the field of antivirals, there is little commercial investment in research. Public funding to support research on current or new antiviral agents is largely limited to the US.
In the European Union, priorities for pharmaceutical research on influenza vaccines and antiviral agents should focus on short- and long-term research. Moreover, pharmaceutical research should go hand-in-hand with translational research that will provide the basis for implementing programs for using newer vaccines and antivirals.
Short-term research (within the next five years) should focus on evaluating the immunogenicity and safety of low-dose, adjuvanted ‘pandemic-like’ vaccines. Intellectual property rights and regulatory issues related to the use of reverse genetics to prepare seed strains for pandemic vaccine production need to be resolved. The benefits of expanded use of existing vaccines (including live attenuated influenza vaccines) and expanding vaccine manufacturing capacity should be further explored.
For antiviral agents, their effects on reducing serious complications of influenza should be further explored. Studies on the effectiveness of a lower dose and shorter duration of treatment with anti-neuraminidase agents could increase their availability during a pandemic. More important, there is an urgent need for research on newer antiviral agents, some of which might target new virus antigens.
Research is also needed on the possible impact of commonly available medications such as statins on the clinical course of influenza-related illness.
Long-term research should focus on developing broad spectrum vaccines that provide long lasting protection. In addition, the development of new antiviral agents that overcome the disadvantages of current agents is urgently needed. Support for research on the basic immunology of the response to vaccination, the molecular pathophysiology of influenza virus infection and the role of biological response mediators in host defense should go hand-in-hand with research on influenza vaccines and antiviral agents.
The ability of Europeans to respond to the next influenza pandemic will in considerable measure depend on the willingness of the European Union to provide public support for a research agenda on pandemic vaccines and antiviral agents in interpandemic years. Successful implementation of this agenda will allow the European Union to fulfil its obligations to all Europeans and meet its responsibilities to people in other countries throughout the world.
6.2-6
6.2: Pandemic Influenza
2. BackgroundDespite a considerable increase in our knowledge of influenza viruses, major breakthroughs in the prevention and control of annual epidemics and influenza pandemic preparedness have not been made. This is especially worrying as an influenza pandemic becomes more and more likely. The last pandemic occurred more than 35 years ago and the recent years' outbreaks of avian influenza in poultry in Asian countries have heightened global concern that a new human pandemic could follow.1
The World Health Organization (WHO) has historically focused its influenza activities on virological surveillance to support annual vaccine strain selection. Recently, WHO expanded its focus to address new challenges. In May 2002, WHO convened a consultation of influenza experts, virologists, epidemiologists and public health officials. The consensus that was achieved led to the publication of the first Global Agenda on Influenza Surveillance and Control 2.(See Appendix 6.2.2) The Global Agenda responds to the challenges posed by poor understanding of the impact of influenza, especially in developing countries, the long time frame needed to manufacture influenza vaccines, persisting inadequate vaccine coverage in most countries, and the need for surveillance activities to be more closely related to control. It encourages collaboration among all those in the public and private sectors who can contribute to better influenza surveillance and control, and maps out a strategic plan for doing so. The Global Agenda identifies 17 priority activities judged necessary to reduce the burden of epidemics and prepare the world for the next pandemic. They are listed according to four main objectives: (i) strengthen surveillance; (ii) improve knowledge of the health and economic burden of influenza; (iii) increase influenza vaccine usage, and (iv) accelerate national and international action on pandemic preparedness. Each priority activity is further defined in a series of recommended activities for researchers, industry, governments, and WHO. Among the priorities are research on pandemic viruses, vaccines, antiviral agents and other control measures.
The Global Agenda has been widely accepted by scientists all over the world. It gained strong political backing in May 2003 when the World Health Assembly (WHA) adopted a resolution on the “Prevention and Control of Influenza Pandemics and Annual Epidemics”. 3 (See Appendix 6.2.3) In this resolution, Member States acknowledged that influenza affects millions of people worldwide and causes fatal complications in up to 1 million people each year. Many of these deaths could be prevented by increasing the use of existing vaccines, particularly in high-risk groups. Member States expressed concern about “the general lack of national and global preparedness for a future influenza pandemic, especially in view of the recurrence of such pandemics and the high mortality, social disruption, and economic costs they invariably cause, which may now be exacerbated by rapid international travel, the recent worldwide increase in the size of at-risk populations, and the development of resistance to first-line antibacterial drugs.” They recognized the need to improve vaccine formulations, increase manufacturing capacity for vaccines, ensure more equitable access to antiviral drugs, and strengthen disease surveillance as part of national and global pandemic preparedness. The WHA resolution called for Member States ”to support research and development on improved influenza vaccines, particularly concerning their suitability for use in developing countries, in order to develop and produce an influenza vaccine formulation
6.2-7
6.2: Pandemic Influenza
capable of conferring long-lasting and broad protection against all influenza virus strains.” WHO was asked ”to search jointly with other international and national partners, including the private sector, for solutions to reduce the present global shortage of, and inequitable access to, influenza vaccines and antiviral drugs, both for epidemic and global pandemic situations.”
The event that marks the beginning of European planning for the next influenza pandemic was the EU-sponsored conference “Pandemic Preparedness in the Community” that was held in Brussels on 27 November 2001. In its preliminary conclusions, the conference noted:“The next pandemic is imminent. EU Member States are not prepared. Vaccine availability is not secured. Antiviral stocks do not exist and will not be under the current market forces. In the event of a pandemic millions of people could die, economies will be affected and services (medical, civil) could collapse. Members of the public will not excuse authorities, who will be held responsible for not having put in place up-to-date preparedness.”4
In March 2004 the European Commission published a working document on “Community Influenza Pandemic Preparedness and Response Planning”.5 (See Appendix 6.2.1) The document noted that "current vaccine production capacity is not deemed to be sufficient to meet the demands of the Community in the event of a pandemic. Manufacturers’ reserve capacity is not likely to be enough to support a sudden increase in demand. Availability of vaccines or antivirals to populations most at risk may, in critical situations, be further limited by measures imposed by Member State authorities to provide maximum protection to their own population. Measures should, therefore, be considered with a view to ensuring equity of access." The Commission emphasized that research performed during the inter-pandemic period would be vital for preparing an effective pandemic response, noting that "research leading to the development of new vaccine technology should remain a priority and be linked to routine and fast-track licensing procedures for influenza vaccines. Current and emerging anti-viral drug resistance developments in influenza need to be addressed through coordinated research at the European level. Furthermore, in the process of early recognition of the identity and origins of pandemic strain, the role of international scientific cooperation is key. The Commission will therefore continue to develop its collaborative research networks to integrate partners in third countries, as was the case in the past with similar threats, such as Ebola and Lassa fever and more recently SARS. "
Since these reports were published, considerable progress has been made in formulating plans for pandemic preparedness within the European Union and outsite.6 The research components for various Community actions had already been identified in the Community’s 5th and 6th Framework Programmes. Two projects for developing new influenza vaccines are currently being funded and a call was recently issued for proposals for post genomic research in the field of influenza vaccines. In addition, in April 2004 the European Agency for the Evaluation of Medicinal Products (EMEA) published guidelines for developing and registering pandemic influenza vaccines through a procedure that will be based on ‘mock-up’ dossiers for candidate pandemic vaccines submitted by individual vaccine companies.7 Nonetheless, there has been limited progress in developing new interventions to prevent or delay a pandemic and that are accessible by the majority of the world’s population. This can be remedied only through greater investment by the public sector. This need was strongly emphasised in the report of a recent WHO Consultation on “Priority Public Health Interventions Before and During a
6.2-8

6.2: Pandemic Influenza
Pandemic” that was held in March 2004.8 This report can and should be used as an inspiration to all the readers of this document.
3. Burden of Disease 3.1. The Influenza Virus
Influenza viruses are negative-stranded RNA viruses, of which type A is the most pathogenic for humans.9 The influenza virus genome consists of eight RNA segments that code for 10 proteins: two envelope glycoproteins - the hemagglutinin (HA) and neuraminidase (NA) antigens, matrix protein (M1), nucleoprotein (NP), three polymerases (PB1, PB2 and PA), an ion channel protein (M2) and two non-structural proteins (NS1 and NS2). The type A viruses that cause epidemics in man are classified according to their HA (H1, H2 and H3) and NA (N1 and N2) antigens. Point mutations in the HA and less frequently NA antigens lead to the antigenic drift characteristic of interpandemic yearly epidemics. Sudden substitutions of whole genes from one subtype to another, by mixing human and animal influenza viruses in animal hosts, lead to the antigenic shifts that uniquely characterize new pandemics.
3.2. Interpandemic Influenza: The Burden of Disease
Influenza affects people of all ages in all parts of the world, and each year 5 to 20% will develop symptomatic illness Error: Reference source not found. Epidemics of varying degrees of severity occur each winter. Although difficult to assess, these annual epidemics are thought to result in between three and five million cases of severe illness and up to 1,000,000 deaths worldwide. Most deaths associated with influenza in industrialized countries occur among people over 65 years of age.
Although most cases of influenza are self-limited, they are responsible for an enormous amount of work absenteeism, additional medical care and economic loss. In England and Wales, for example, hospital admissions for influenza-related conditions have caused major problems for health service delivery each winter, especially for older people,10 and this experience is duplicated in other countries.11 Moreover, in England and Wales, an estimated 6200 to almost 30,000 people died of influenza-related illnesses during each of the epidemics between 1975 and 1989,12 an experience common to other countries where influenza morality has been studied.13 In the United States, estimates put the economic costs of annual influenza epidemics at several billion dollars per year.14 There have been few studies of the health and economic burden of influenza in tropical and developing countries. However, a recent report from Hong Kong for the period 1998-2001 documented rates of excess influenza-related hospital admissions for pneumonia, chronic obstructive pulmonary disease and heart failure that were comparable to those reported in developed countries.15 In the developing countries of Madagascar and the Democratic Republic of Congo, recent outbreaks have been extensive and case-fatality rates have been 3-4%, rates similar to those experienced in developed countries during the 1918 pandemic. The mortality impact of these outbreaks has been especially severe in children.
In developed countries, infection rates are higher in children than in any other age group, and children are the principle disseminators of influenza throughout communities. Influenza is a major cause of acute otitis media 16 and in children < 2 years of age hospitalization rates approach those seen in elderly adults.17
6.2-9

6.2: Pandemic Influenza
Several studies from European countries have documented the impact of childhood influenza on ambulatory care visits 18 19 20and hospitalizations.21 22 23
24Recently, attention has been drawn to influenza-associated complications such as febrile seizures and acute influenza-associated encephalopathy, a condition that is either fatal or causes serious neurological sequelae in more that half of cases.25 Influenza is also an important cause of respiratory illness and hospitalization for acute cardiopulmonary conditions in pregnant women, although adverse effects on perinatal outcomes have not been noted.26
In most European countries there are no estimates of excess influenza-associated mortality nor are there measures of influenza’s impact on the economic life of communities and nations. Several studies have documented aspects of the burden of influenza in European children, but compared with other countries, less is known about rates of hospitalization, specific complications such as acute encephalopathy, and the effects of influenza on pregnant women and perinatal outcomes. Accurate assessment of the health and economic impact of influenza in different populations will enable policy-makers to set priorities and justify budgets for programs for influenza prevention and control.
3.3. Avian Influenza: Increasing the Risk for a Pandemic
Avian influenza viruses do not normally infect species other than birds and pigs. However, in 1997, avian H5N1 influenza appeared in the poultry markets of Hong Kong and infection spread to 18 people, six of whom died 27. Little, if any, inter-human spread was recorded. Human cases of H5N1 influenza reappeared in 1999 and again in early 2003. In late 2003 and early 2004, an unprecedented outbreak of avian H5N1 influenza swept through poultry flocks in many countries in East and Southeast Asia. Again, human cases of H5N1 infection occurred, and this time 24 (68%) of the 34 people who were infected died.28
Avian influenza has persisted in poultry flocks in several of the counties affected, and in August 2004 three additional fatal cases of human H5N1 influenza were reported from Vietnam.29 Europeans have also had recent experience with avian influenza. In early 2003 a highly pathogenic avian influenza H7N7 outbreak affected commercial poultry farms in The Netherlands and infection was transmitted to humans. As a result, more than 400 poultry workers and their family members developed conjunctivitis and influenza-like illness and one person, a previously healthy veterinarian, died.30 This is not the only documented instance of the transmission of an avian influenza virus to mammals. In the early 1980s, an H7N7 avian virus infected seals on Cape Cod in New England, and within two months 25% had died.31
The persistence of highly pathogenic avian influenza viruses in poultry flocks in Asian countries provides continuing opportunities for the direct infection of humans. As more humans become infected, the likelihood increases that humans might be concurrently infected with human and avian influenza strains. One of these persons could serve as the “mixing vessel” for the emergence of a novel influenza virus subtype possessing the genetic phenotype that permits efficient person-to-person transmission, the essential requirement for a new pandemic virus32. Another possible and alarming scenario, and different from the “mixing vessel” mechanism, is that of an avian virus mutating at a critical site to allow for a stronger binding of the virus to cells in the human respiratory tract and
6.2-10

6.2: Pandemic Influenza
therefore speeding up viral replication and facilitating a more efficient man-to-man transmission
The World Health Organization and infectious disease experts throughout the world are concerned that events such as the recent avian influenza outbreaks in Asia could lead to a new human influenza pandemic.Error: Reference source not found 33
3.4. Pandemic Influenza and its Potential Impact on Europe and the World
The influenza pandemic of 1918 was one of the most significant disease outbreaks in all of recorded history.34 Within a two-year period, it killed an estimated 50-100 million people worldwide, far more than died in World War I.35
Two later pandemics - Asian influenza in 1957-59 and Hong Kong influenza in 1968 - were much milder, but nonetheless caused widespread social disruption and substantial excess mortality.Error: Reference source not found
No one can know with certainty how severe the next pandemic will be. Several years ago, a respected influenza expert cautioned against what he called ‘influenza extrapolitis’; that is, the assumption that the next pandemic will be as severe as the one in 1918.36 Epidemiological models from the Centers for Disease Control and Prevention, Atlanta, USA project that today a pandemic could result in 2 to 7.4 million deaths worldwide. In high income countries that account for 15% of the world’s population, epidemiological models project a demand for 134–233 million outpatient visits and 1.5–5.2 million hospital admissions.37 Many regard these estimates as very conservative and believe that the burden of pandemic disease will be more severe, especially in developing countries.
If the next pandemic is as severe as the one in 1918, the situation could be much worse. Given the more than 3-fold increase in the world’s population since 1918, a reappearance of a 1918-like pandemic could also kill as many as 175 to 350 million people. This is more than the number of people killed in all wars and by the most murderous governments throughout the 20th Century.38 These people would die not in 100 years but in 1 or 2.
In early 2004, 68% of the human cases of avian H5N1 influenza seen in Vietnam and Thailand died. The case-fatality rate was far worse than what was seen in 1918. If a pandemic virus with this degree of virulence were to acquire the transmission characteristics of a usual pandemic influenza virus, the health consequences for human populations everywhere could be catastrophic. No country will be spared.
In addition to their consequences for health, influenza outbreaks can have a huge impact on the social and economic life. Recent experience with SARS has shown that an emerging disease that causes a small number of cases in a region can rapidly spread to distant countries and create anxiety in the community. Medical facilities can be easily overwhelmed, and anxiety can quickly disrupt community life. Compared with the SARS experience, a severe influenza pandemic can be expected to be far worse. Widespread illness may result in significant shortages of personnel who provide essential community services and public fear may put immense political pressure on decision makers. Thus, in making plans for responding to the next pandemic, it would be prudent to
6.2-11
6.2: Pandemic Influenza
anticipate the ‘worst case scenario’, remembering that, “the only thing more difficult than planning for an emergency is having to explain why you didn't".39
4. Prevention and Control of Influenza4.1. The Current Control Strategy and its Effectiveness
4.1.1. Influenza VaccinationInfluenza vaccines are the mainstay of influenza prevention and control.Error:Reference source not found The trivalent inactivated vaccines currently available are immunogenic and safe. Following vaccination, serological responses to the hemagglutinin (HA) antigen of the influenza virus correlate well with clinical protection.40 Vaccination also stimulates an increase in anti-neuraminidase antibodies,41 42 and these antibodies protect against both influenza itself43 and secondary bacterial pneumonia [J. McCullers, personal communication, 16 June 2004]. Provided there is a close match between the vaccine virus and the virus causing disease, the protective efficacy of vaccination is up to about 70% against disease and even more so against adult hospitalizations and death.44 In addition to being clinically effective, influenza vaccination has also been shown to be cost-effective in European countries.45
Vaccination of children is also clinically effective46 and high levels of coverage among schoolchildren induce herd immunity and prevent deaths in older adults.47 Pregnant women are at increased risk of hospitalization for influenza-related illness,48 and vaccination during pregnancy has the potential to benefit not only mothers themselves but also their newborn infants.49
There are relatively few European studies on the effectiveness of influenza vaccination preventing influenza-associated hospitalizations and death in adults, children and pregnant women.
WHO recommends the use of influenza vaccine in nationally defined risk groups.50 People at risk include residents of institutions for the elderly or the disabled, persons (> 6 months of age) with chronic cardiovascular, pulmonary, metabolic or renal disease, persons who are immunocompromised and individuals who are above a nationally defined age limit irrespective of their medical risk status (most countries define the age limit as ≥ 65 years). The WHA resolution on influenza in 2003 recommended that Member States undertake the following:Error: Reference source not found
where national influenza vaccination policies exist: increase vaccination coverage of all high-risk groups, including the elderly and persons with underlying chronic disease, and establish appropriate strategies for doing so, with the goal of attaining vaccination coverage in the elderly population of at least 50% by 2006 and 75% by 2010;
where no national influenza vaccination policies exist: assess the health and economic impact of annual influenza epidemics as a basis for developing and implementing influenza prevention policies within the context of other national health priorities.
4.1.2.Antiviral Agents Currently, four antivirals have proven efficacy in treatment and prophylaxis of influenza A infections: two M2 inhibitors (amantadine and rimantadine) and two neuraminidase inhibitors (zanamivir and oseltamivir).Error: Reference sourcenot found The therapeutic efficacy of all of these agents was established in clinical trials conducted in adults and children who received treatment within
6.2-12

6.2: Pandemic Influenza
two days of the onset of the symptoms. There are few data on their efficacy in high-risk individuals.Error: Reference source not found Antivirals reduce virus shedding and thus infectivity of treated infected persons.
Early treatment with M2 inhibitors reduces the duration of symptoms and the time to recovery by one to two days. When M2 inhibitors are used in treatment, antiviral resistance develops rapidly, limiting their use. Moreover, the avian H5N1 viruses isolated in Asia have not been inhibited by these agents. All influenza type A and B viruses, including the avian viruses, are sensitive to the anti-neuraminidase agents oseltamivir and zanamivir. Zanamivir is administered by inhaler and its use has been limited. Oseltamivir has been more widely used, and when given within the first 48 hours of the onset of symptoms, it shortens the course of clinical illness, reduces antibiotic use and reduces rates of pneumonia and hospital admissions.51 Thus far, antiviral resistance has not become an important clinical problem with oseltamivir.Error: Reference sourcenot found, 52
There are no European data on the effectiveness of neuraminidase inhibitors in preventing influenza-associated hospitalizations and death in adults, children and pregnant women.
4.1.3.Use of Vaccines and Antivirals During a PandemicInfluenza vaccines and antiviral agents are the two essential components of a comprehensive pandemic response. Other components include adequate supplies of antibiotics and other resources for providing hospital and outpatient care to populations affected by the pandemic. Most countries will have limited or inadequate resources to manage a pandemic. Given this, national authorities must address the question of which citizens should be given priority for receiving the limited supplies of pandemic vaccines and antiviral agents.
Considerations for establishing priority groups for vaccination will be different for each country, not only because of differences in vaccine availability and resources but also because of differences in population structure and the organization of essential services. Decisions as to who should be included in priority groups will depend on the primary goals of the vaccination programs. Possible target groups for pandemic vaccination include the following:53 (See Appendix 6.2.4)
Essential service providers including health care workers (to maintain essential services)
Groups at high risk of death and severe complications (to prevent or reduce death and hospital admissions)
Persons without risk factors or complications (to prevent or reduce morbidity).
Options for the use of antiviral agents will depend on their availability, the size of the target groups and the specific goals to be achieved. The main options include:Error: Reference source not found
Long term prophylaxis (prevention) of defined populations for the duration of a wave of pandemic activity (minimum of 4 weeks)
Prophylaxis during outbreaks in closed institutions (usually lasting about 2 weeks)
6.2-13

6.2: Pandemic Influenza
Protection of individuals for the period between vaccination and the development of protection, ranging from 2–6 weeks depending on whether one or two doses of vaccine is recommended
Prophylaxis of individuals following exposure to pandemic influenza (approximately one week per course)
Treatment of ill persons for whom treatment can be initiated within the first 48 hours of illness
Treatment of exposed persons for whom influenza vaccination is contraindicated
In general, prophylaxis is more likely that treatment to prevent serious complications from influenza because it prevents influenza virus infection itself. However, early treatment represents a more efficient use of resources than prophylaxis, which requires a prohibitively large stockpile.Error: Referencesource not found Vaccination should still be the primary method of prophylaxis.
4.1.4.Non-Medical Interventions In the early stages of a pandemic, antiviral agents will be in very short supply and vaccines will not be available for many months. During this period other non-medical interventions could delay the national and international spread of the pandemic. This strategy of ‘buying time' was discussed during the WHO Consultation on”Priority Public Health Interventions Before and During an Influenza Pandemic” that was held in March 2004.Error: Reference source notfound
A wide range of non-medical interventions – from personal hygiene and wearing masks to quarantine and screening travellers – could potentially limit the transmission of the pandemic virus. Although many of these interventions were tested during the response to the SARS outbreak, their use under the very different conditions of an influenza pandemic has not been systematically evaluated. Their effectiveness will depend on the transmissibility of the virus, its virulence, its attack rate in different age groups, the duration of virus shedding, and the susceptibility of the virus to antiviral agents. In addition to their effectiveness, the choice of non-medical interventions will be driven by their availability, cost, ease of implementation and likelihood of acceptance by the public. Mathematical modelling suggests that early detection of the first chains of human-to-human transmission might provide a unique opportunity to prevent or at least delay further virus transmission. Because the window of opportunity will close quickly, prior guidance on the most appropriate interventions will be particularly important.
More than 30 non-medical public health interventions for controlling a pandemic have been suggested. It is unlikely that any single measure would have a meaningful impact on its own. However, as all regions of the world are unlikely to be affected simultaneously during the first wave of infection, opportunities for preventing the spread of the pandemic virus to these regions will probably remain open even after the pandemic has begun. During this phase, simple measures such as hand washing, the use of masks and voluntary quarantine for symptomatic persons could help reduce transmission. Travel-related measures such as exit screening of persons departing from affected areas might limit or delay international spread. Knowing that a pandemic has emerged, the general public will probably be strongly motivated to adopt personal preventive behaviours, even though some of them might have limited effectiveness. Some behaviours such as avoiding travel to affected areas will probably be followed regardless of official recommendations. In all instances, implementing these
6.2-14

6.2: Pandemic Influenza
measures may require changing public health laws at both national and international levels.
Once efficient and sustained human-to-human transmission is established in a region, containment of the virus will become virtually impossible and opportunities for averting the pandemic or appreciably slowing its spread will end. Thus non-medical interventions may be important 'additional control measures', but by themselves they will not be able to stop or control a pandemic.
4.2. Current Implementation of the Control Strategy
4.2.1.The Interpandemic Use of Influenza Vaccine in Europe and the Rest of the World
Supplies of influenza vaccine for the next pandemic will be critically dependent on the levels of vaccine use during the interpandemic period. Thus, planning for pandemic vaccine supply requires an ongoing understanding of the global epidemiology of influenza vaccination54.
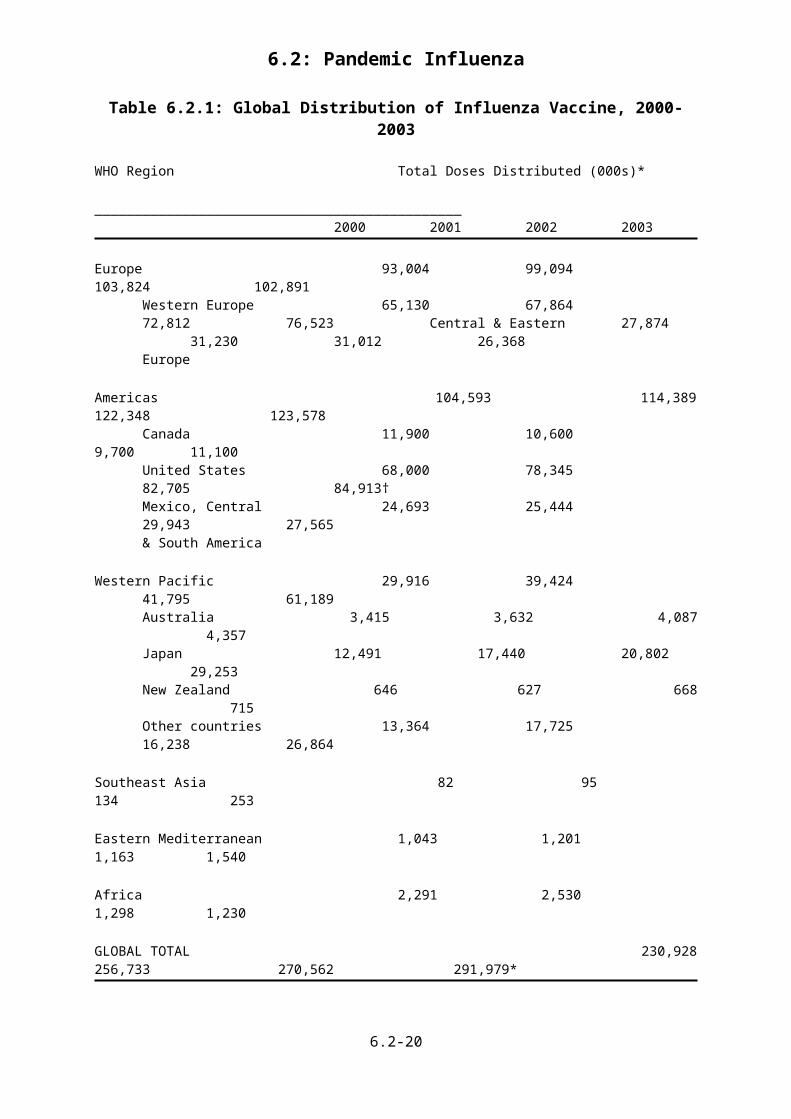
An overview of the global production and distribution of influenza vaccines during the interpandemic period has been provided by the Influenza Vaccine Supply (IVS) International Task Force. The IVS Task Force is sponsored by the International Federation of Pharmaceutical Manufacturers Associations (IFPMA). Its report for the period 2000-2003 was recently submitted to WHO (see Table 6.2.1). In 2000, 230 million doses of influenza vaccine were distributed worldwide, 162 million (70%) of which were distributed in Canada, the U.S., Western Europe, Australasia and Japan. In 2004, vaccine distribution increased to 292 million doses, of which 207 million (71%) were used in these same countries. During this four-year period, vaccine distribution increased 18% in Western Europe, 20% in Canada and the US, 25% in Australasia and 134% in Japan. For the rest of the world, vaccine distribution increased from 69 million doses to 85 million doses, a 23% increase. For these other countries, the use of influenza vaccine was largely limited to four countries in South America (Argentina, Brazil, Chile and Uruguay), several countries in Central Europe (especially Hungary and Poland), Russia and South Korea. Compared with 1994, when approximately 135 million doses of influenza vaccine were distributed worldwide, the level of vaccine distribution ten years later had more than doubled.
6.2-15

6.2: Pandemic Influenza
Table 6.2.1: Global Distribution of Influenza Vaccine, 2000-2003
WHO Region Total Doses Distributed (000s)* ______________________________________________
2000 2001 2002 2003
Europe 93,004 99,094 103,824 102,891
Western Europe 65,130 67,864 72,81276,523 Central & Eastern 27,874 31,230 31,01226,368 Europe
Americas 104,593 114,389 122,348 123,578
Canada 11,900 10,600 9,70011,100United States 68,000 78,345 82,705 84,913†Mexico, Central 24,693 25,444 29,94327,565& South America
Western Pacific 29,916 39,424 41,79561,189Australia 3,415 3,632 4,087 4,357Japan 12,491 17,440 20,802 29,253New Zealand 646 627 668 715Other countries 13,364 17,725 16,23826,864
Southeast Asia 82 95 134 253
Eastern Mediterranean 1,043 1,201 1,163 1,540
Africa 2,291 2,530 1,298 1,230
GLOBAL TOTAL 230,928 256,733 270,562 291,979*
*Individual reports on the numbers of doses of influenza vaccine distributed each year were submitted by all IVS Task Force companies: Aventis Pasteur, Aventis Pasteur MSD, Berna Biotech, Ltd., Chiron/Powderject, CSL Limited, GSK Biological, Medimmune, Inc., Shire Biologicals, Solvay Pharmaceuticals B.V. and Wyeth Vaccines. The Association of Japanese Biologicals Manufacturers reported data on behalf of four Japanese vaccine companies. In addition, data were gathered from non-IVS Task Force companies located in Hungary, the Russian Federation and Romania. The Task Force was unable to obtain information on doses produced and distributed in other counties. The data were reported for calendar years according to WHO Regions. For some regions, additional information was obtained on vaccine distribution in countries within the regions.
†The data for the United States in 2003 do not include doses of cold-adapted, live-attenuated trivalent influenza vaccine distributed by Medimmune. In 2003, Medimmune produced ~4-5 million doses of CAIV-T and distributed ~830,000 doses, but only ~250,000 doses were actually sold.
Almost all of the world’s influenza vaccine is produced in nine countries. Five of these countries are EU Member States - France, Germany, Italy, The
6.2-16

6.2: Pandemic Influenza
Netherlands and the UK. The other four countries are Australia, Canada, Japan, and the US. (In Europe, a Swiss company markets influenza vaccine, but it obtains its bulk virus from a vaccine company located in Australia.) In 2003, these nine countries had only 12% of the world’s population, yet they produced ~95% of the world’s influenza vaccine. Almost none of the doses produced in Canada, Japan and the US were exported to other countries, and all of the 13.8 million doses produced in Hungary, Romania and Russia were used domestically.
In 2003, companies located in five EU countries produced 190 million doses of influenza vaccine, 65% of the world’s supply. The EU companies produced 85% of the 93 million doses used in countries outside Western Europe, Canada, the US, Australasia and Japan.
The IVS Task Force survey has provided an accurate summary of influenza vaccine production and the distribution of vaccine to different regions of the world. However, the survey cannot provide country-specific information on vaccine distribution for more than a few countries. Recently, the Macroepidemiology of Influenza Vaccination (MIV) Study Group was established to provide this information. Individual investigators in each country now submit data on the total number of doses of vaccine distributed each year. The data are reported as rates of vaccine distribution per 1000 total population. Information has been gathered from 40 countries and the results for 2002 are shown in Figure 6.2.1 (MIV Study Group, unpublished observations). The largest user of influenza vaccine was Canada, primarily because its largest province (Ontario) has a universal influenza vaccination program. The Republic of Korea ranked third, in part because a vigorous vaccination program was undertaken in the wake of the SARS outbreak in early 2003. Countries within the European Union showed varying levels of vaccine use, with those in Western Europe generally having higher levels than the new Member States of Central and Eastern Europe. However, Russia and Hungary had higher levels of vaccine use that did several Western European countries, and a few countries in South America used more vaccine that did some European countries.
6.2-17

6.2: Pandemic Influenza
Figure 6.2.1: Rates of Influenza Vaccine Distribution in 40 Countries in 20021
Number of doses distributed per 1000 total population
All EU Member States and almost all other developed and rapidly developing countries have national recommendations to vaccinate elderly people and others with high-risk medical conditions.55 Nonetheless, ten-fold variations in vaccine use are still seen within the EU. Factors that contribute to these variations include different levels of understanding of the health and economic 1 Member States of the European Union are shown in solid bars; non-EU countries are shown in the hatched bars. No data were obtained for Cyprus, Estonia and Malta.
6.2-18

6.2: Pandemic Influenza
consequences of influenza, the presence or absence of public programs for vaccine delivery and vaccination reimbursement, and the views of small groups of policy makers. In addition, a number of underlying cultural factors are important.
The data provided by the IVS Task Force and the MIV Study Group document a reality of enormous logistical and political importance for the Member States of the European Union. Most countries in the EU and virtually all non vaccine-producing countries in the rest of the world are critically dependent on supplies of interpandemic influenza vaccines produced in only five EU countries. This dependence will directly affect the availability of supplies of pandemic vaccines for the other 20 EU Member States and for all other countries that do not have influenza vaccine companies of their own.
4.2.2.The Interpandemic Use of Antivirals in Europe and the Rest of the World
There is very little epidemiological information available on the use of antiviral agents worldwide. The M2 inhibitors have several disadvantages, have not been heavily marketed and have fallen out of favour. The anti-neuraminidase agents, particularly oseltamivir, have received more attention and are the only agents that would be effective against the avian H5N1 viruses. Only one company located in Switzerland produces oseltamivir, although it is considering building one or more additional production sites in other countries. The time needed to increase production capacity in the current facility is at least 9-12 months, if not longer.
There are no publicly available data on the distribution of oseltamavir in EU countries or in the rest of the world. However, the EU and global production capacity for this agent is extremely limited. In 2003, approximately 7 million oseltamivir ‘treatments’ (one treatment is a five-day course for an individual patient) were distributed by the manufacturer (Brown P, Roche Pharmaceuticals, personal communication, 17 June 2004). Approximately half of the treatments were used in Japan. The total number of ‘treatments’ was similar to the population of the country where oseltamivir is produced. In the event of a pandemic, the export of oseltamivir might be prohibited, and consequently supplies will be available only in countries that have stockpiled oseltamivir (at great expense) in advance.
Greater and more diversified manufacturing capacity for anti-neuraminidase agents is needed, as are new and less expensive antiviral agents.
4.2.3. Affordability of the InterventionsSeveral years ago, influenza vaccines were sold in developed countries at relatively low prices, but recent supply constraints and expanding markets have been accompanied by increased prices. In Western Europe, the current (2004) retail price to health care providers is € 5-16 per dose [Bertrand Verwee, personal communication, 18 August 2004]. In 2000, the total cost of vaccinating an individual in three Western European countries was €15-30.Error: Referencesource not found Despite recent price increases, the value of influenza vaccination is still regarded as very high, even though annual revaccination is required. Cost-effectiveness analyses for three Western European countries show that vaccinating elderly persons is highly cost-effective and in some instances may even be cost saving.Error: Reference source not found
6.2-19
6.2: Pandemic Influenza
There is little public knowledge about vaccine prices and the costs of vaccination programs in the newer Member States of the EU and in the rest of the world. In most developing countries the cost of the vaccine probably puts influenza vaccination outside the range of affordability for public vaccination programs. Nonetheless, the increase in vaccine use documented for many rapidly developing countries indicates that for large segments of the populations in these countries, influenza vaccines are considered affordable.
Antiviral agents are considerably more expensive than influenza vaccines. Little is known about their current prices in all EU countries. However, in 2000 the cost of a five-day course of anti-neuraminidase treatment ranged from € 30-40 in three Western European countries, and a 4-week course of chemoprophylaxis cost € 130-215.Error: Reference source not found Chemoprophylaxis was 30-50 times more expensive than vaccination, although properly timed treatment of symptomatic patients was reasonably cost-effective. Greater use of antivirals would eventually have the effect of reducing their price, but it is unknown to what level prices would drop. In the event of a pandemic, anti-neuraminidase agents could be stockpiled in bulk and formulated for use when a pandemic threat is declared. Nonetheless, the basic cost of the bulk drug for a five-day treatment course would be at least € 7 and the cost of its formulation, distribution and administration would add greatly to the total cost per person.
The current costs of antiviral agents represent a major obstacle to their supply and will severely limit their use in the control of pandemic influenza.
5. Constraints to Better Control5.1. Interpandemic Period
Despite the effectiveness of global influenza surveillance, national and international responses to influenza suffer from several weaknesses that could have severe consequences for public health in the event of a pandemic. Recent WHO-sponsored consultations have identified several areas of concern.Error:Reference source not found,Error: Reference source not found
There is an urgent need for better understanding of the occurrence, epidemiology, and health and economic burden of influenza in developing countries. Surveillance and control activities in these countries receive little support, and as a result the WHO surveillance network has important geographical gaps. Health officials in these countries have little available evidence for concluding that influenza is a significant health problem and that policies for its control should be adopted.
Some countries in the European Union have made considerable progress in increasing influenza vaccination coverage, particularly when operational targets have been set. However, knowledge about the benefits of influenza vaccination has not been translated into effective vaccination programs in most Member States. At present, only ~50 countries, mainly in the industrialized world, have policies for influenza vaccination. Despite numerous studies demonstrating the safety and effectiveness of vaccines, only 10–20% of people in high-risk groups in these countries are vaccinated. Vaccination coverage rates in developing countries are
6.2-20

6.2: Pandemic Influenza
minimal. In addition, vaccination rates among health care workers in direct contact with the elderly high-risk group are low, despite strong evidence that health care workers contribute to outbreaks in institutions caring for the elderly and are highly susceptible to infection themselves.
No currently available influenza vaccines confer protection against all strains of the three influenza virus subtypes that cause human disease. Because each subtype exhibits frequent antigenic drift, the vaccine formulation must be adjusted each year. This change requires re-licensing of the vaccine and repeat vaccination. Thus stockpiling influenza vaccine is not an option. In addition, influenza vaccine continues to be moderately expensive for people who live in developed countries and its price is out of reach for most of those who live in developing countries.
Greater efforts are needed to implement current recommendations for influenza vaccination in order to reach coverage levels specified by the World Health Assembly in its resolution on influenza. Research on novel vaccines, vaccine delivery methods and production technologies is needed to overcome the limitations of current influenza vaccines.
5.2. Pandemic Period
5.2.1.Limitations of the Vaccination StrategyIf a new pandemic virus emerges within the next few years, several potential limitations in the supply of pandemic vaccines immediately become apparent.Error: Reference source not found Pandemic vaccine production will be totally dependent on the capacities of the existing vaccine companies in the EU and the rest of the world. All of these companies currently produce their vaccines in embryonated eggs.56 If the interpandemic use of vaccine increases in the next few years, the production capacities of vaccine companies will increase in parallel, but the incremental increase year-on-year will not be large. One new EU-based company is scheduled to enter the market within the next 2-3 years and it plans to market 40-50 million doses of cell culture-produced inactivated influenza vaccine each year. None of the other EU-based companies is expected to have an appreciable capacity to produce cell culture vaccines within the next five years; it usually takes five or more years to build and obtain regulatory approval for a new vaccine production facility. Given that five EU-based companies produced 190 million doses of trivalent vaccine in 2003 (Table 6.2.1) and that an additional 40-50 million doses will soon be added, the overall capacity of EU-based companies for pandemic vaccine production within the next five years is unlikely to exceed the equivalent of ~250 million doses of trivalent vaccine each year.
Because the pandemic vaccine will almost certainly contain only the pandemic vaccine virus (it will be a monovalent vaccine), it is possible that up to 750 million doses of same-strength (15 µg HA) monovalent pandemic vaccine could be produced within the EU. However, most if not all people will not have been previously infected with a virus like the pandemic virus. Because they will be immunologically naïve, they will require two doses of vaccine to be fully protectedError: Reference source not found. Moreover, in many if not most countries, public health authorities will want to vaccinate everyone in their populations.Error: Reference source not found,,Error: Reference source not found This means that in the 25 EU countries, only 375 million people could be vaccinated with a ‘same strength’ monovalent vaccine, well under the total EU population of 450 million. Further, when a pandemic virus appears, government leaders in the five countries that have vaccine companies could be tempted to ‘nationalize’ their
6.2-21

6.2: Pandemic Influenza
vaccine production facilities, citing national emergencies, to ensure that there is enough vaccine to vaccinate their own populations.
If a pandemic vaccine is formulated to contain 15 µg HA, 100 million people in the 20 EU countries without vaccine companies will have to wait several months or more for supplies of pandemic vaccines. Countries outside the EU that have traditionally been supplied with interpandemic vaccines by EU-based companies might not be able to obtain any supplies of pandemic vaccines.
5.2.2.Limitations of the Antiviral StrategyOne or more antiviral agents currently in use will likely be effective in the prophylaxis and treatment of illness caused by a new pandemic virus. Important differences between the M2 inhibitors and the neuraminidase inhibitors will require careful definition of their respective roles in pandemic control. However, supplies of these agents will quickly be exhausted in the first few weeks of the pandemic. Because these agents are relatively stable over time, they could be stockpiled. However, for most countries the cost of stockpiling will be a significant burden.
All countries will need to consider the complementary use of vaccines and antiviral agents in planning for various phases of pandemic control. Vaccination will remain the primary means of prevention once vaccines become available. Antivirals will have to be used in special situations.Error: Reference source notfound Countries will be able to meet their pandemic requirements only if they make plans for obtaining supplies of antivirals in advance. Manufacturers require regular estimates of demand on which to base production plans, and the current market-based system has limited or no surge capacity to respond to a sudden increase in demand. There is currently no global estimate of the future demand for antiviral agents, and a global distribution system for what will inevitably be limited supplies does not exist. Moreover, the issue of liability for adverse reactions to antiviral treatment has not been addressed.
In the event of a pandemic, supplies of antiviral agents will be available only to countries that have stockpiled them (at great expense) in advance. Greater and more diversified manufacturing capacity for anti-neuraminidase agents is needed, as are new and different antiviral agents.
6.2-22

6.2: Pandemic Influenza
6. Lessons Learned from Research into Pharmaceutical Interventions
6.1. Vaccination Strategies
Within the past few years, several groups of European investigators have carefully explored a promising strategy for developing ‘pandemic-like’ vaccines that (1) induce protective levels of antibodies when two doses are given to immunologically naïve subjects, and (2) could be produced in abundant supply by vaccine companies using their existing facilities Error: Reference source notfound. The strategy is based on using a lower dose of HA antigen and including an adjuvant. The initial studies were conducted using a proprietary MF59 adjuvant 57 58 59 60, but later studies have used a simple alum adjuvant of the kind widely available and used by all vaccine companies that produce childhood vaccines.61, 62 Vaccines against H2, H5 and H9 ‘pandemic-like’ viruses have been tested. Both adjuvanted and non-adjuvanted vaccines have been produced using both whole virus and subunit virus preparations. The vaccines have been formulated with HA concentrations as low as 1.875 µg per dose.Error:Reference source not found, 61 A single injection of one these low-dose vaccines primes the immune system and a second dose, usually given 3 weeks later, leads to the development of protective levels of antibodies when measured after another 3 weeks.
How low the HA content of a pandemic vaccine can be set is uncertain, but an ‘antigen sparing’ strategy has critical implications for the amounts of vaccine that could be produced at any given time during the course of a pandemic vaccination program. For example, if the world’s vaccine companies were told to produce a monovalent alum-adjuvanted whole virus pandemic vaccine with an HA content of 1.875 µg (i.e., 8-fold less than normal strength), they could theoretically produce approximately 36 times more vaccine than normal. If normally they would produce 130 million doses in a 6-month period, they would be able to produce 4.68 billion doses of pandemic vaccine (130 x 3 x 1.5 x 8; see pandemic supply model in Figure 6.2.2). This would be enough to vaccinate 2.34 billion people (2 doses), almost one-third the world’s population. These estimates are hypothetical and they assume that the pandemic virus would have similar growth/yield characteristics as current vaccine strains, that the production facilities would be available, and that the immunogenic properties of the pandemic virus would be similar to those of the H2, H5 and H9 viruses already tested. Nevertheless, this amount of vaccine would probably exceed the vaccine delivery capacities of all of the world's health care systems. One should also consider the option of using a single low-dose priming strategy without a second dose. A one-dose strategy might be sufficient to reduce the frequency of severe illness and death when the pandemic virus hits an unprotected population. The clinical efficacy of these strategies could not be tested in man, but could be evaluated using appropriate animal models.
The low-dose, alum-adjuvanted vaccine strategy is central to the thinking of all EU vaccine companies. Most European and WHO experts consider it to be the most promising approach for guaranteeing adequate supplies of pandemic vaccines for all EU Member States and for all other countries that will depend on EU companies for supplies of pandemic vaccines.
6.2-23

6.2: Pandemic Influenza
Figure 6.2.2: Pandemic Vaccine Supply Model for Global Production
0
1000
2000
3000
4000
5000
Trivalent 0 0 10 50 90 130 170 210Monovalent 0 0 30 150 270 390 510 630Whole virus 0 0 45 225 405 585 765 945Adjuv. (8x) 0 0 360 1800 3240 4680 6120 7560
1 2 3 4 5 6 7 8
million D
* months **doses / month
**
*
2 doses for 2.3 billion people2 doses for 2.3 billion people
0
1000
2000
3000
4000
5000
Trivalent 0 0 10 50 90 130 170 210Monovalent 0 0 30 150 270 390 510 630Whole virus 0 0 45 225 405 585 765 945Adjuv. (8x) 0 0 360 1800 3240 4680 6120 7560
1 2 3 4 5 6 7 8
million D
* months **doses / month
**
*
2 doses for 2.3 billion people2 doses for 2.3 billion people
○ = ten million doses per week, ● = 30 million doses per week, = 45 million doses per week and = 360 million doses per week. Source: N
Hehme et al. GSK, Germany.
6.2-24

6.2: Pandemic Influenza
Box 1: The US Approach to Developing a Pandemic Vaccine: Lessons for the EU
In June 2004, the National Institutes of Health (NIH) in the US awarded contracts to Aventis Pasteur (US) and Chiron Vaccines (UK) to produce pilot lots of monovalent H5N1 'pandemic-like' vaccines. These vaccines will be formulated at two dosage strengths - 15 µg and 45 µg of HA antigen (standard and high-dose, respectively) - in order to comply with FDA requirements for currently licensed influenza vaccines. They will be tested in the NIH Vaccine Trial and Evaluation Units. Public funding will support the full costs of this project.
The US currently has a domestic influenza vaccine production capacity of approximately 50 million doses of trivalent vaccine per year. According to the NIH strategy, 50 million doses of domestically produced trivalent inactivated vaccine would be equivalent to 150 million doses of standard-dose (15 µg HA) monovalent pandemic vaccine and 50 million doses of high-dose (45 µg HA) vaccine. For the US to be able to offer two doses of standard-dose pandemic vaccine to each person (assume 300 million x 2 = 600 million vaccinations), domestic production of trivalent vaccine would have to increase four-fold (and for a high-dose pandemic vaccine up to 12-fold) to reach the equivalent of 600 million doses of trivalent vaccine per year. To expect such an expansion of domestic vaccine production capacity within the next five years is not realistic.
The current NIH strategy for developing an H5N1 ’pandemic-like' vaccine appears to be based on (1) the goal of determining the optimal dose of HA antigen for an individual rather than an acceptably immunogenic dose for a population, and (2) the assumption that a new pandemic virus will not emerge for five or more years. The US government hopes to increase domestic capacity for producing influenza vaccines by accelerating the introduction of cell culture vaccine production and expanding the supply of embryonated eggs, but these effort are almost certain to be of limited success within the next five years.
From a global perspective, it would be more beneficial for pandemic vaccine development to focus on ensuring that the largest possible supply of pandemic vaccine can be made available as quickly as possible. A short-term development strategy should be based on existing egg-based production capacity. Its goal should be to determine the lowest amount of HA antigen that can be included in an adjuvanted vaccine that will be acceptably immunogenic when given in a two-dose schedule to a population. This alternative strategy would respond to the needs of people in vaccine producing countries and would provide millions of doses of pandemic vaccine for people in other countries.
Europeans can learn two lessons from the current US approach to developing pandemic vaccines. First, vaccine development should focus on vaccines that are acceptably immunogenic for populations and that can be produced in existing production facilities. Most European vaccine experts already accept this strategy. Second, public funding is driving the development of pandemic vaccines in the US. Current evidence suggests that Europeans have yet to appreciate that public funding will be essential for pandemic vaccine development in Europe.
6.2-25

6.2: Pandemic Influenza
6.2. Reverse Genetics
There is a possibility that the next influenza pandemic could be caused by a highly pathogenic avian virus.Error: Reference source not found, Error: Reference source
not found, Error: Reference source not found In the first eight years following the 1997 outbreak of H5N1 avian influenza in Hong Kong, no commercially viable human H5N1 vaccine could be produced. Since the early 1970s, vaccine reference strains have been prepared using the technique of genetic reassortment. With this technique, embryonated eggs are co-infected with an influenza virus considered most likely to cause epidemic disease and a high-growth strain of influenza A/PR8 virus. Following subsequent cloning, a progeny genetic reassortant virus is isolated that has two genes coding for the surface (HA and NA) antigens of the epidemic virus and six genes derived from the A/PR8 virus that are associated with high growth.
Genetic reassortants have been essential to the success of influenza vaccine production for more than 30 years, but they have disadvantages. The time needed to isolate a genetic reassortant suitable for commercial vaccine production can take many weeks. The reassortants do not always grow efficiently in egg-based production systems. Importantly, this technology cannot be used with highly pathogenic avian viruses because the resulting reassortants are highly pathogenic for embryonated eggs and may be capable of human infection. These reasons explain why no commercially viable seed strain for human H5N1 vaccine production has yet been prepared using genetic reassortment.
Within the past two years, reference strains suitable for producing human 'pandemic' influenza vaccines have been prepared in several laboratories using the techniques of reverse genetics (RG).Error: Reference source not found, Error:
Reference source not found, Error: Reference source not found, Error: Reference source not found Using this technique, the polybasic amino acids associated with H5N1 virulence are removed from the HA cleavage site. Plasmids containing the genes for the avian virus HA and NA antigens are then cloned and transfected into Vero cells along with plasmids containing the six A/PR8 genes. The progeny virus is rescued from cell culture, purified, propagated in embryonated eggs and tested for stability and pathogenicity. The methods for preparing RG-engineered viruses are straightforward, the results are predictable and the process can take as little as 10-20 days. Moreover, when used with avian viruses, the resultant RG-engineered reference strains can be used as seed strains for egg-based vaccine production.
Reverse genetics has been used to prepare reference strains using human isolates of H5N1 viruses obtained during the 2003 and 2004 outbreaks of avian influenza. WHO has been instrumental in developing guidelines for safety testing of these reassortants and has provided advice on risk assessment for vaccine manufacturers intending to use them63 .
It is important that virologists working in WHO-affiliated laboratories and in vaccine companies gain more experience with reverse genetics-engineered influenza viruses. This will ensure that the time between the isolation of a new pandemic virus and the beginning of full-scale vaccine production is minimized.
6.2-26

6.2: Pandemic Influenza
6.3. Existing Research Resource Flows
Two projects for influenza vaccine development have been funded by the EU. The 4-year FLUPAN project (€ 2,100,000) was begun in January 2001. Its goal has been to develop better methods to rapidly detect the emergence a pandemic virus in animals and its spread in man, and to more rapidly produce a safe and effective vaccine. The major focus of the research has been to use reverse genetics to produce reference strains of vaccine viruses (mostly avian viruses) to produce pilot lots of vaccines in cell culture systems and to evaluate the immunogenicity and safety of these vaccines in Phase I/II clinical trials. The investigators have also produced libraries of reagents for the production and standardization of several avian and swine virus vaccines and explored the use of genetically modified mammalian cells that express influenza virus proteins for future use in diagnostic tests. The 3-year NOVAFLU project (€ 1,765,000) was begun in autumn 2002. Its goal is to develop more effective strategies for vaccination against interpandemic and pandemic influenza. The investigators are developing better strategies for vaccine strain selection, exploring alternative approaches for vaccine production in cell culture systems, considering several novel vaccine candidates and evaluating animal model systems of influenza virus infection to establish better laboratory correlates of clinical protection.
The EU Framework programme is currently open (until the 16 th of November 2004) again for new research proposals exploring post-genomic approaches to a pandemic vaccine. Studies should focus on the development of a system that allows for rapid design of safe and efficient vaccines and scale-up of production and should address the development of improved adjuvants, standardisation of animal models and strategies for multi-centre clinical vaccine evaluation in man.
The EU is also funding the VIRGIL project to monitor and evaluate the evolution of resistance to antiviral agents in Europe.
In the U.S., the National Institute of Allergy and Infectious Disease (NIAID) at the NIH supports activities for developing and testing effective countermeasures against pandemic influenza that range from basic and applied research to partnerships with industry. Current NIAID projects include developing a library of reference viruses and producing and distributing reagents for vaccine standardization, research and surveillance. NIAID also supports the production and clinical evaluation of different types of pandemic influenza vaccines to assess their safety and age-related immunogenicity. Inactivated and live-attenuated egg-based and non-egg based vaccines (e.g., DNA and recombinant protein vaccines) are also being evaluated.
6.2-27

6.2: Pandemic Influenza
Recent NIAID activities include:
Evaluation of a recombinant mono-component (HA only) H5 vaccine in Phase I/II clinical trials (1997 H5 strain)
Grant award to Aventis Pasteur to produce an inactivated cell culture-based H7 influenza vaccine
Evaluation of a Phase I inactivated subunit H9N2 vaccine (serology in process)
Award of contracts to Aventis Pasteur and Chiron to pilot lots of an inactivated 2004 H5N1 vaccine (both companies are licensed in the U.S.)
Award a contract to Chiron (Sienna, Italy) to evaluate an MF59 adjuvanted inactivated H9N2 influenza vaccine
Support for the development and testing of improved inactivated influenza vaccines and new production technologies include the development of cell culture-based vaccine technologies, broadly cross-protective influenza vaccines and the improvement of inactivated vaccines by assessing the role of adjuvants, alternate delivery systems and dose range. Recent accomplishments include the production and clinical evaluation of the first trivalent baculovirus-expressed influenza vaccine in a phase II clinical trail and phase I/II clinical trials to enhance the effectiveness of inactivated influenza vaccines for the elderly.
NIAID also supports the development of new antiviral drugs against influenza. Activities range from basic research to identify new drug targets, in vitro and in vivo antiviral screening programs, and the preclinical and clinical evaluation of new drugs.
The resources currently committed to this NIAID research program (excluding extramural funding) are in the range of US$ 50-100 million. Additional funding might become available under the $ 5.4 billion Bioshield program.
There is little knowledge of funding levels for influenza research that is supported by individual EU governments and by non-governmental organizations. Currently the world's largest source of non-governmental funding for all vaccine-related research is the Bill and Melinda Gates Foundation in the US. The foundation has yet to fund research devoted to influenza prevention and control.
7. Pipeline of Products7.1. Pipeline for Influenza Vaccines
The most important new influenza vaccine product introduced in recent years, has been Medimmune’s intranasal cold-adapted live-attenuated influenza vaccine (LAIV; FluMist). Clinical trials have shown very promising clinical efficacy in children and younger adults against infection with homotypic and heterotypic influenza viruses.64 The LAIV product was launched in the US in 2003-2004, but sales were far lower than had been planned for or anticipated. Major reasons for this failure were the vaccine’s very high price, the limited age group (5 to 49 years) for which it was licensed, and the inconvenience of handling a product that must be stored frozen. In future years, the company will market its LAIV product at a lower price. Additional safety data will lead to recommendations for using it in children less than 5 years of age. A fully liquid non-frozen preparation will also be forthcoming. Medimmune’s LAIV is not yet being used in EU countries, but will probably be introduced within the next few
6.2-28

6.2: Pandemic Influenza
years. However, it is unlikely that it will command a substantial share of the European influenza vaccine market for many years to come.
All European vaccine companies are seriously considering investments in cell culture vaccine production systems, and several have built facilities that are already licensed or will be licensed within the next few years. It is widely believed that one advantage of cell culture production will be to free manufacturers from their dependence on supplies of embryonated eggs.Error:Reference source not found,65 In addition, it is believed that cell culture systems will allow companies to rapidly increase vaccine production when confronted with a sudden increase in demand, as will occur with a pandemic. Whether this anticipated ‘surge capacity’ will materialize remains an open question. Nonetheless, there can be little doubt that companies with a commercial need to increase their vaccine production capacity will do so by building cell culture facilities. It will take many years, however, before cell culture-produced vaccines command a substantial share of the European or global influenza vaccine market. Vaccines produced in embryonated eggs are likely to be the mainstay of influenza prevention for at least the rest of this decade, if not longer.
Two European vaccine companies are collaborating on the development of a virosomal influenza vaccine.66 Clinical trials have shown that this vaccine is safe and immunogenic, and applications for registration are pending in at least two countries.
In the US, a new influenza vaccine is being developed by a biotechnology company using a recombinant baculovirus-expressed HA antigen that is prepared in insect cell culture .67 In an early clinical trial, two doses of a monovalent H5 HA-containing vaccine were poorly immunogenic at relatively high doses (90 µg HA), but recent unpublished Phase II (b) dose-ranging studies of two doses of a trivalent HA vaccine (15, 45 and 135 µg for each HA) are said to be more encouraging. Questions that still must be addressed are the immunogenicity of only one dose, the possible need for an adjuvant, the effect that the absence of an NA antigen will have on its acceptability for registration and the cost of its production relative to egg-derived vaccines.
As mentioned earlier, several vaccine companies have been making preparations for producing clinical lots of H5N1 and other 'pandemic-like' vaccines. However, progress has been limited due to biosafety requirements, uncertainties regarding intellectual property rights for the reverse genetics-engineered H5N1 reference strains and lack of public funds to support the clinical trials.
An overview of some of the products in company pipelines is shown in Table 6.2.2.
6.2-29

6.2: Pandemic Influenza
Table 6.2.2: Overview of Pipeline Products2
2 Table contains information published on internet. The contents have not been checked with the companies and may be incomplete.1 Webby RJ, Webster RC. Are we ready for pandemic influenza? Science 2003; 302: 1519-22.2 World Health Organization. Global Agenda on Influenza Surveillance and Control. http://www.who.int/csr/disease/influenza/csrinfluenzaglobalagenda/en/3 Fifty-Sixth World Health Assembly. Prevention and control of influenza pandemics and annual epidemics. WHA 56.19, 28 May 2003.4 Pandemic preparedness in the community: influenza and other health threats. Preliminary conclusions and recommendations. Conference Brussels, 27 November 2001.5 European Commission. Commission Working Document on Community Influenza Pandemic Preparedness and Response Planning. Brussels, 26.03.2004, COM(2004) 201 final. 6 See http://www.who.int/csr/disease/influenza/nationalpandemic/en/ for and overview of published national pandemic preparedness plans. Two examples of pandemic preparedness plans (for Canada and the US) are included in the annexes of this report.
7 Committee for Proprietary Medicinal Products (CPMP). Guideline on dossier structure and content for pandemic influenza vaccines marketing authorisation applications. EMEA/CPMP/VEG 47107/03 [http://www.emea.eu.int/pdf/human/veg/4710703en.pdf].8 World Health Organization. WHO Consultation on priority public health interventions before and during an influenza pandemic. Geneva, Switzerland, 16-18 March 2004. WHO/CDS/CSR/RMD/2004.99 Nicholson KG, Wood JM, Zambon M. Influenza. Lancet 2003; 362: 1733-45.55 van Essen GA, Palache AM, Forleo E, Fedson DS. Influenza vaccination in 2000: recommendations and vaccine use in 50 developed and rapidly developing countries. Vaccine 2003; 21: 1780-5.64 Kemble G, Greenberg H. Novel generation of influenza vaccines. Vaccine 2003; 21: 1789-95.10 Fleming D, Harcourt S, Smith G. Influenza and adult hospital admissions for respiratory conditions in England 1989-2001. Commun Dis Public Health 2003; 6: 231-7.11 Scuffham PA. Estimating influenza-related hospital admissions in older people from GP consultation data. Vaccine 2004; 22: 2853-62.12 Nicholson KG. Impact of influenza and respiratory syncytial virus on mortality in England and Wales from January 1975 to December 1980. Epidemiol Infect 1996: 116: 51-63.13 Reichert TA, Simonsen L, Sharma A, Pardo SA, Fedson DS, Miller MA. Influenza and the winter increase in mortality in the United States, 1959-1999. Am J Epidemiol 2004; 160: 492-502.
6.2-30
Company Sort of product/ development StageAventis Alternative delivery system (intradermal) Phase 1 finished
Cell culture Long termChiron Cell culture
MF59 adjuvanted subunit egg grown H5N3 vaccine
Phase 2 Phase 1 research
Protein Science FluBlok - recombinant HA
Rec H5 HA vaccine
Phase 3 fall this yearPhase 1 research
Recombinant Neuraminidase (Additive) Phase 2 finishedZymetx ViraZYme: technology to be used for
diagnostics and antiviral development Antivirals: animal testing
Shire Cell cultureBaxter Cell culture Approved in NLCrucell Cell culture Commercial
agreement with Aventis
Solvay Cell culture Approved in NLVirosomal influenza vaccine (with Berna) Under approval
in NL and CHBernaBiotech Virosomal influenza vaccine (with Solvay) Under approval
in NL and CHGSK Subunit vaccine
Low dose subunit/whole virus alum adjuvanted H2N2 and H9N2 vaccines
Phase 1 Phase 1 research
Biota / Sankyo Long acting neuraminidase inhibitors See textEU vaccine manufacturers
Pandemic ‘mock-up’ vaccines for EU licensing (ie H5, H7, H9 or H2 vaccines)
Planning stage
6.2: Pandemic Influenza
7.2. Pipeline for Antiviral Agents
Little is know about pharmaceutical company pipelines for new antiviral agents. Interest in their development may have waned as a result of the commercial difficulties experienced by companies that have already introduced anti-neuraminidase agents. One company has essentially withdrawn from the market and another has discontinued its development program. However, one pharmaceutical company in Japan recently reported results of a Phase I study of a long-acting neuraminidase inhibitor administered by inhalation.68 Experimental studies showed complete protection of experimentally infected mice when treated 7 days before infection, and Phase I studies in man showed that this agent’s active metabolite could be detected in urine up to 6 days after the
14 Schoenbaum SC. Economic impact of influenza. The individual's perspective. Am J Med. 1987; 82 (6A): 26-30.15Yap FHY, Ho P-L, Lam K-F, et al. Excess hospital admissions for pneumonia, chronic obstructive pulmonary disease, and heart failure during influenza seasons in Hong Kong. J Med Virol 2004; 73: 617-23. 16 Neuzil KM, Zhu Y, Griffin MR, et al. Burden of interpandemic influenza in children younger than 5 years: a 25-year prospective study. J Infect Dis 2002; 185: 147-52.17 Neuzil KM, Mellen BG, Wright PF, Mitchel EFJr, Griffin MR. The effect of influenza on hospitalizations, outpatient visits and courses of antibiotics in children. N Engl J Med 2000; 342: 225-31.18 Heikkinen T, Ziegler T, Peltola V, et al. Incidence of influenza in Finnish children. Pediatr Infect Dis J 2003; 22: S204-6.19 Principi N, Esposito S, Marchisio P, Gasparini R, Crovari P. Socioeconomic impact of influenza on healthy children and their families. Pediatr Infect Dis J 2003; 22: S207-10.20 Aymard M, Valette M, Luciani J, et al. Burden of influenza in children: preliminary data from a pilot survey network on community diseases. Pediatr Infect Dis J 2003; 22: S211-4.21 Forster J. Influenza in children: the German perspective. Pediatr Infect Dis J 2003; 22: S215-7.22 Ploin D, Liberas S, Thouvenot D, et al. Influenza burden in children newborn to eleven months of age in a pediatric emergency department during the peak of an influenza epidemic. Pediatr Infect Dis J 2003; 22: S218-22.23 Laundy M, Ajayi-Obe E, Hawrami K, Aitken C, Breuer J, Booy R. Influenza A community-acquired pneumonia in East London infants and young children. Pediatr Infect Dis J 2003; 22: S223-7.24 Nicholson KG, McNally T, Silverman M, Simons P, Zambon MC. Influenza-related hospitalisations among young children in Leicestershire. Pediatr Infect Dis J 2003; 22: S228-30.25 Togashi T, Matsuzono Y, Narita M, Morishima T. Influenza-associated acute encephalopathy in Japanese children in 1994-2002. Virus Res 2004: 103: 75-8.26 Hartert TV, Neuzil KM, Shintani AK, et al. Maternal morbidity and perinatal outcomes among pregnant women with respiratory hospitalizations during influenza season. Am J Obstet Gynecol 2003; 189: 1705-12.27 Claas ECJ, Osterhaus ADME, van Beek R, et al. Human influenza A H5N1 virus related to a highly pathogenic avian influenza virus. Lancet 1998; 351: 472-7.28 World Health Organization. Avian influenza – Current evaluation of risks to humans from H5N1 following recent reports. Wkly Epidemiol Rec 2004;79 (29): 265-27229 World Health Organization. Avian influenza - update Viet Nam. http://www.who.int/csr/don/2004_08_18/en/.
6.2-31

6.2: Pandemic Influenza
inhalation of one dose. The commercial dimensions of this company’s development program are unknown. Given its simplicity of administration and its long-lasting activity, this and/or other similar antiviral agents could have widespread applicability for the control of pandemic influenza.
7.3. The Safety and Efficacy of Products in the Pipeline
Currently available influenza vaccines have a well-established record of safety. Nonetheless, concerns about safety are always present. The swine influenza vaccine used in the US in 1976 was associated with an increase in the occurrence of Guillain–Barre syndrome, although vaccines used since then have been essentially free of this association.69 More recently, an inactivated vaccine produced by a Canadian company was associated with cases of an ocular complication that was traced to a correctible change in the vaccine’s manufacturing process.70 Also, an intranasally administered inactivated vaccine produced by a European company was quickly withdrawn from the market because it was associated with Bell’s palsy.71 The adverse effect was attributed to the adjuvant used in the vaccine, and the vaccine has not been reintroduced into the market. There have been extensive safety studies of Medimmune’s LAIV and no serious adverse events have yet been noted. The acute and long-term safety of vaccines still under development is not known. As with all other vaccines, rare and delayed complications of vaccination cannot be known without careful post-marketing surveillance and evaluation of suspected adverse events.
Concerns have been raised about the safety of workers involved in vaccine production. One relates to the safety of using a reverse genetics-engineered vaccine strain in commercial vaccine production facilities. A risk assessment sponsored by WHO provides reassurance on this issueError: Reference sourcenot found.
In Europe, the EMEA has published its Note for Guidance on dossier structure and content for pandemic influenza vaccines marketing authorization applications.Error: Reference source not found (See appendices 6.2.5 and 6.2.6) 30 Koopmans M, Wilbrink B, Conyn M, et al. Transmission of H7N7 avian influenza virus to human beings during a large outbreak in commercial poultry farms in the Netherlands. Lancet 2004; 363: 587-93.31 Geraci JR, St. Auban DJ, Barker IK, et al. Mass mortality of harbor seals: pneumonia associated with influenza A virus. Science 1982; 215: 1129-31.32 Li KS, Guan Y, Wang J, et al. Genesis of a highly pathogenic and potentially pandemic H5N1 influenza virus in eastern Asia. Nature 2004; 430: 209 - 13.36 Dowdle WR. Striking the balance. In: Osterhaus ADME, Cox N, Hampson AW (eds). Options for the control of influenza IV. Amsterdam: Excerpta Medica 2001, pp 3-7.37 Meltzer M. Preliminary global estimates of the impact of the next influenza pandemic. Presentation prepared for the WHO Consultation on priority public health interventions before and during an influenza pandemic, 16-18 March 2004.38 Emmott B. 20:21 vision. The lessons of the 20th Century for the 21st. London: Penguin Books, 2003, p 9.39 Henry B. Canadian Conference on Counter-Terrorism and Public Health. Toronto: Oct 29-Nov 1, 2003.
46 Ruben F. Inactivated influenza virus vaccines in children. Clin Infect Dis 2004; 38: 678-88.
6.2-32

6.2: Pandemic Influenza
The document addresses the quality requirements, the non-clinical safety and immunological requirements and the clinical requirement for ‘mock-up’ pandemic vaccines. Because there will be no time to conduct clinical trials of a true pandemic vaccine, immunogenicity and safety data should be obtained for 'mock-up vaccines' that are developed and tested during the interpandemic period. These vaccines must include viral antigen(s) to which humans are immunologically naïve. Assuming the true pandemic vaccine is similar to and is produced in the same way as the ‘mock-up’ vaccines, clinical data from the core pandemic dossier can be extrapolated to the true pandemic vaccine and it can be quickly registered.
With few if any influenza antiviral agents in the pipelines of pharmaceutical companies, there is no information on their safety.
47 Reichert TA, Sugaya N, Fedson DS, et al. The Japanese experience with vaccinating schoolchildren against influenza. N Engl J Med 2001; 344: 889-96.48 Neuzil KM, Reed GW, Mitchel EF, Simonsen L, Griffin MR. Impact of influenza on acute cardiopulmonary hospitalizations in pregnant women. Am J Epidemiol 1998; 148: 1094-102.49 Englund JA. Maternal immunization with inactivated influenza vaccine: rationale and experience. Vaccine 2003; 21: 4360-4.53 World Health Organization. WHO guidelines on the use of vaccines and antivirals during influenza pandemics. WHO/CDS/CSR/RMD/2004.8.54 Fedson DS. Pandemic influenza and the global vaccine supply. Clin Infect Dis 2003; 36: 1552-61.63 World Health Organization. Production of pilot lots of inactivated influenza vaccine in response to a pandemic threat: an interim biosafety risk assessment. Wkly Epidemiol Rec 2003; 78 (47): 405-8.
6.2-33

6.2: Pandemic Influenza
8. Research into New Pharmaceutical Interventions8.1. Vaccines with Broad Spectrum and Long Lasting Immunity
In February 2004, WHO held a meeting on the “Development of Influenza Vaccines with Broad Spectrum and Long-lasting Immune Responses”72. The goal of this meeting was to identify critical scientific issues and gaps in knowledge that must be addressed in order to accelerate the development of new influenza vaccines that induce broad spectrum and long-lasting immunity. A broadly protective vaccine that is affordable in developing countries could be important in light of the avian influenza outbreak in Asia and concern that a virus from this avian reservoir might acquire the capacity for human-to-human transmission and result in a pandemic.
Vaccine TypeA broad spectrum influenza vaccine would offer protection against infections caused by divergent influenza virus types and subtypes and would also protect against infection caused by an antigenically new virus characteristic of a pandemic. It would not need to be updated each year because it would offer equal protection against infection with antigenically drifted virus strains not perfectly matched (by HA and NA) with current inactivated influenza vaccines. This would make the manufacturing process more flexible and less time constrained. If the vaccine were also able to induce long-lasting immunity, the current yearly vaccination strategy could be revised to one that would be easier to implement in developing countries.
Currently available inactivated influenza vaccines cannot be used to protect children less than 6 months of age and are less than optimally protective in older adults. They must also be reformulated and re-administered each year. However, they do induce a certain degree of heterotypic immunity to infection with variants related to the vaccine virus. Increasing the dose of HA correlates with an increasing magnitude, duration and cross-reactivity of anti-HA antibodies and these antibodies correlate with protection against disease. Increased levels of antibody to the NA antigen also reduce the intensity of infection and limit its transmission to others. Given the importance of these two antibodies, improvements in existing inactivated vaccines could be important. By inducing better antibody responses to these two antigens, an improved inactivated vaccine could contribute to better heterotypic immunity and provide longer-lasting protection against infection caused by antigenic variants within a subtype.
In addition to anti-HA and NA antibodies, cytotoxic lymphocytes (CTL) also help to reduce the intensity and duration of viral shedding. Several invariant antigens (M1, NP, and possibly others) induce CTL responses, and antibody to the invariant M2 protein may also have an important role in protection. Vaccines 66 de Bruijn IA, Nauta J, Gerez L, Palache AM. Virosomal influenza vaccine: a safe and effective influenza vaccine with high efficacy in elderly and subjects with low pre-vaccination antibody titers. Virus Res 2004; 103: 139-45.67 Treanor JJ, Wilkinson BE, Masseoud F, et al. Safety and immunogenicity of a recombinant hemagglutinin vaccine for H5 influenza in humans. Vaccine 2001; 1732-7.68 Yamashita M. R-118958, a unique anti-influenza agent showing high efficacy for both prophylaxis and treatment after a single administration: from the in vitro stage to phase I study (abstract S5-2). Options for the control of influenza V. Okinawa, Japan, 7-11 October 2003, p 37.
6.2-34

6.2: Pandemic Influenza
containing these invariant antigens could induce long-lasting immunity and provide in advance significant protection against a yet-to-emerge pandemic virus.
6.2-35
6.2: Pandemic Influenza
Delivery Options and AdjuvantsMany of the disadvantages of current inactivated influenza vaccines could be overcome by mucosal delivery.Error: Reference source not found Intranasal administration of influenza virus seems promising because administration of antigens to the mucosa is required for optimal IgA antibody responses. This route stimulates both mucosal and systemic immune responses. Mucosal vaccine delivery could facilitate vaccine use, especially in developing countries. However, several obstacles stand in the way, including the need to develop an optimal delivery system, overcoming concern about inducing immune tolerance, achieving a proper balance between IgA and IgG antibodies, and defining the need for adjuvants to improve antibody responses. Despite a recent setback, the potential value of mucosal vaccination is sufficient reason to continue research on this approach to vaccine delivery.
Several adjuvants are available for improving immune responses to vaccines.Error: Reference source not found The choice of adjuvant depends on the proposed antigen, the type of immune response required and the target population for vaccination. Virosomal vaccines containing IL–2 or CpG as an adjuvant have induced enhanced immune responses in clinical trials. In mice, cationic liposomes containing antigens are highly immunogenic without added adjuvants. ISCOMS can induce TH1 and TH2 responses and have induced long-lasting immunity and increased immune responses in both young and elderly subjects.
Several potential new conjugated vaccines prepared with the ectodomain of the influenza M2 protein have induced homotypic and heterotypic immunity to infection by antigenic variants within a subtype and by different influenza A subtypes73. Preclinical studies of this ‘universal’ influenza A vaccine in experimental animal models of infection have been promising.74
DNA vaccines that induce antibody responses to surface antigens have been shown in animal models to induce homologous protection, while DNA vaccines against conserved internal proteins (NP, M1) induce broad, heterotypic protection against infections by influenza A viruses of different subtypes.Error:Reference source not found
Influenza virus infections can induce both broad spectrum and long-lasting immunity against reinfection with an influenza virus within a subtype. This suggests that live-attenuated influenza vaccines (LAIV) could induce similar protection and that this would be due to immunity to viral components other than the hemagglutinin 75. In mice, ferrets and humans, LAIV have induced potent protection against both homotypic and antigenically drifted viruses. Children benefit from LAIV but evidence for the superiority of LAIV over inactivated vaccines in adults is mixed.
Regulatory IssuesSeveral difficult regulatory issues will have to be addressed before a new vaccine that promises to induce cross-protective and long-lasting immunity can be licensed. Regulatory authorities must be convinced that laboratory correlates of immunity provide reliable evidence of protection. It is unlikely that a clinical trial to demonstrate true long-lasting protection (e.g., more than five years) would be undertaken. Consequently, regulatory officials will probably have to accept evidence of heterotypic protection over fewer years, as was shown in the clinical trials of live-attenuated influenza vaccine.
6.2-36
6.2: Pandemic Influenza
More important will be the decision on whether to regard a new cross-protective vaccine as a replacement for or as a supplement to the current inactivated influenza vaccines. If regarded as a replacement vaccine, licensure will likely depend on a Phase III clinical efficacy trial. A placebo-controlled trial could be conducted in healthy younger adults in whom serious consequences of infection in the placebo group would not be expected. Such a trial would not be able to determine whether the new vaccine would prevent hospitalization and death. A placebo-controlled trial in older adults could not be justified because infections would have to occur in the placebo group to demonstrate the efficacy of the new vaccine, and they could be severe or fatal. (None of the evidence for the effectiveness of current inactivated vaccines in preventing hospitalisation and death has come from placebo-controlled trials conducted in community-dwelling older adults.Error: Reference source not found If evidence of efficacy were to be required in older, high-risk individuals, the clinical trial would have to be structured to demonstrate non-inferiority of the new vaccine compared with the inactivated vaccine. Such a trial would be large, costly and difficult to justify. A placebo-controlled clinical trial in high-risk individuals might be possible if the trial were conducted in a developing country where there is little chance the inactivated vaccine could be introduced.
If a new vaccine is to be regarded as a supplemental vaccine, a clinical trial designed to demonstrate a significant degree of incremental improvement over the current inactivated vaccine alone would also be large and costly. If laboratory correlates of protection were convincing, such a vaccine might be licensed and incremental and (more important) long-lasting protection demonstrated in long-term observational studies. Currently there is no consensus on how a candidate vaccine that promises broad spectrum and long-lasting protection is to be evaluated, but sooner or later this question will have to be addressed.
8.2. Newer Antiviral Agents One new approach to the treatment of influenza focuses on short interfering RNAs (siRNAs). RNA interference has been shown to suppress influenza virus replication in vitro. In experimental influenza infection in mice, siRNAs specific for highly conserved regions of the nucleoproein (NP) of acidic polymerase molecules inhibit virus replication in the lungs and protect against lethal challenge.76, 77 Protection is not mediated by interferon. Importantly, siRNA protects against lethal challenge with highly pathogenic H5 and H7 avian influenza A viruses.
Another possible approach to antiviral treatment and prophylaxis involves the NS1 protein. H5N1 influenza is lethal because the NS1 protein makes the virus resistant to the antiviral effects of interferons and tumor necrosis factor alpha.78,
79 The NS1 protein could be evaluated as a target for newer antiviral agents.
8.3. Other Pharmaceuticals
Few laboratory and clinical investigators are currently studying the molecular pathophysiology of influenza virus infection and the role of the innate immune system in the response to infection 80. Yet such understanding could help us develop new ways of reducing the morbidity and mortality caused by interpandemic and pandemic influenza. Recent studies suggest that the biological basis for severe influenza in humans is associated with virus-induced cyotokine dysregulation81. Avian H5N1 influenza viruses are potent inducers of
6.2-37

6.2: Pandemic Influenza
proinflammatory cytokines (e.g., TNF-alpha and interferon beta). High serum concentrations of the chemokines interferon induced protein-10 (IP-10) and monokine induced by interferon gamma (MIG) have also been reported in patients with H5N1 disease.
In addition to these laboratory findings, epidemiologists recognize that influenza is associated with an increased risk of hospitalizations for cardiovascular and cerebrovascular diseases. Observational studies have documented reductions in hospitalization for congestive heart failure, recurrent myocardial infarction and stroke following influenza vaccination.Error: Reference source not found Given these findings, new advances in the understanding of cardiovascular treatments could have important implications for the prophylaxis and therapy of interpandemic and pandemic influenza.
Much attention has been given recently to the positive effects of high intensity statin treatment for coronary heart disease. These effects seem to be due to their anti-inflammatory effects rather than their effects on low-density cholesterol lipoproteins. Whether prophylaxis and/or treatment with statins or other commonly available therapeutic agents that affect the innate immune system could modify the clinical course of human influenza is unknown. However, in the event of a pandemic, antiviral agents will be largely unavailable and vaccine supplies will be delayed. In these circumstances, it will be essential to know whether commonly used treatments could affect, positively or negatively, the clinical course of pandemic virus infection.
8.4. Institutions and Human Resources
In the last seven years, most of the European research on pandemic influenza vaccines has been conducted by a few groups of dedicated investigators using funds obtained from either commercial sources or national governments. The budgets for these projects have been limited. Most of the world’s influenza vaccine is produced in the European Union and a regulatory framework for pandemic vaccine development has been created by the EMEA. There are adequate numbers of European investigators and institutions to continue work on improving existing influenza vaccines and developing new vaccines and antiviral agents. However, if they are to be successful, they will have to have adequate and stable funding for their research.
9. Gaps and Opportunities for Pharmaceutical ResearchThe primary objectives of supporting new pharmaceutical research in the field of influenza is to reduce the burden of yearly epidemics, to be better prepared to limit the health and socioeconomic burden of the next pandemic and to ensure equal access to vaccines and antiviral agents used in prevention and control. These objectives cannot be met by pharmaceutical research alone. The success of these interventions will also depend greater on understanding of the burden of disease and the health and economic benefits of these interventions.
Reducing the burden of pandemic influenza will not be possible by medical interventions alone. In the early weeks after a pandemic virus emerges, non-medical interventions may be are the only interventions affordable in most countries. Slowing the spread of a pandemic will depend on the available infrastructure for surveillance and early warning and possibilities for the quick determination of the causative agent. Although there are many research
6.2-38

6.2: Pandemic Influenza
opportunities in this area, this chapter has focused on medical interventions only.
The research agenda outlined below is divided into studies that should be carried out over the next five years and studies that should be carried out over a longer period. A sharp distinction cannot be drawn between the two. Because we do not know when the next pandemic will occur, it is essential that both short- and long-term research be conducted simultaneously. The three most important priorities in this research agenda are outlined in bold.
9.1. Research to Be Carried Out in 5 Years 9.1.1.VaccinesThe research agenda for vaccine development is based on the identified gaps in current knowledge, as outlined earlier.
Evaluate different types of monovalent inactivated influenza vaccines (whole virus/split and subunit, adjuvanted/non-adjuvanted, and egg-derived/ cell culture derived) and different vaccination schedules (one/two doses, different dose ranges) using vaccines directed against different hemagglutinin (HA) subtypes considered to have pandemic potential, especially H5N1, H7N7, H9N2 and H2N2. To ensure the most economical use of limited vaccine supplies, the evaluation of a low-dose priming strategy should be emphasized.
Evaluate the safety and effectiveness of using reverse genetics to prepare reference strains of these ‘pandemic-like’ viruses that can be used as seed strains by vaccine companies in Europe and elsewhere to produce pilot lots of ‘pandemic-like’ vaccines.
Continue to prepare libraries of reagents specific for a range of potential ‘pandemic-like’ viruses that can be used to test a future pandemic virus ahead of the time when specific reagents directed against the pandemic virus become available.
Evaluate new methods of vaccination, including mucosal and "needle free" vaccine delivery methods, that might offer improved immunogenicity and be more suitable for mass vaccination programs.
Explore the use of different adjuvants and other new approaches (e.g., higher doses of HA antigen) to improving the antibody response to inactivated influenza vaccines among elderly persons and those with immunocompromise.
Evaluate the role of maternal vaccination and the transplacental transfer of neutralizing antibody in protecting newborn infants against influenza.
9.1.2.Antiviral AgentsThe research agenda for antiviral agents is based on identified gaps in knowledge as identified earlier.
Determine the minimally effective dose and duration for antiviral therapy using anti-neuraminidase and other antiviral agents.
Determine whether use antiviral treatment reduces the occurrence of serious consequences of influenza, such as hospital admission for pneumonia and other influenza-related complications.
Evaluate the comparative effectiveness of the M2 inhibitors and neuraminadase inhibitors and the importance of antiviral resistance when they are used in treatment and prophylaxis.
6.2-39

6.2: Pandemic Influenza
Determine the minimally effective dosages and side effects of antiviral agents when used in selected high-risk populations, such as infants, pregnant women, immunocompromised persons, and elderly persons with underlying disease.
Develop long-acting anti-neuraminidase agents that can be easily administered and are much less expensive to produce.
Further explore the mechanisms of antiviral resistance to both classes of antiviral agents and assess the biological consequences of resistance for transmissibility and virulence.
Develop new and improved antiviral agents directed at the M2 and NA antigens and explore possibilities for developing other classes of antiviral agents directed at other targets such as the NS1 and HA antigens
9.1.3.Non-Pharmaceutical ResearchThe research agenda for non-pharmaceutical research is based on identified gaps in basic knowledge of the immune response to vaccination, the molecular pathophysiology of influenza virus infection and the role of the innate immune system in the host response to infection.
Continue to explore how different components of the innate and adaptive immune systems confer protection against influenza following vaccination, giving special attention to factors that determine heterotypic and heterosubtypic protection and the contributions of CTL –based immunity.
Evaluate the molecular response to influenza virus infection in cell culture systems and the role of cytokines and other biological response mediators in determining the outcome of infection. Evaluate also these responses in experimental infections in mice, ferrets and primates.
Explore the effects of commonly available pharmaceutical agents that are known to affect biological response mediators on the response to influenza virus infection both in vitro and in vivo.
6.2-40

6.2: Pandemic Influenza
Box 2: Reverse Genetics, Intellectual Property and Influenza Vaccination
Reverse genetics (RG) is a promising technique for the rapid and safe production of influenza vaccine seed strains. The practical advantages of reverse genetics over genetic reassortment are well known. However, there is one essential difference between the two techniques: reverse genetics is associated with patents. The intellectual property (IP) rights for RG are held by at least two academic institutions and one pharmaceutical company, all three of which are located in the United States. The patent holders have agreed that RG can be used to prepare reference strains for research purposes. However, if RG-engineered seed strains are to be used for commercial vaccine production, patent holders expect to be paid royalties.
The recent award of NIH contracts to Aventis Pasteur and Chiron to prepare pilot lots of H5N1 vaccine for clinical testing highlights several problems related to intellectual property rights for reverse genetics. If we were now facing a true H5N1 pandemic threat, an H5N1 pandemic vaccine would be needed, but most vaccine companies would be uncertain about the precise ownership of the IP rights for the RG-engineered seed strains they would be called upon to use. A few companies have probably already undertaken their own RG patent analyses, but no one should expect them to disclose their findings. The US Department of Health and Human Services recently conducted a patent search of its own and has formulated its future policy options, but they are not publicly known. Even if they were, the US patent rights would apply only to the US, since patent rights in Europe and Japan are independent of those in the US. The status of European patents is not publicly known.
In the absence of knowing who owns the intellectual property for RG, it will be difficult for a vaccine company to enter into negotiations on royalty payments for pandemic vaccine production. If one company attempts to open negotiations with only one patent holder, litigation by the other patent holders could follow. Moreover, if presented with a pandemic threat, the governments of countries with vaccine companies would probably exercise compulsory use licenses. Royalty payments for using RG would be determined by governments and would not be negotiated between patent holders and patent users. Even if there were no problems with RG-IP, companies with no previous experience using RG-engineered viruses might have difficulty obtaining regulatory approval for the using them in their production facilities.
A strong argument can be made for resolving RG-IP ownership before the next pandemic threat appears Error: Reference source not found,82. This would allow companies to determine whether using RG-engineered seed strains would offer advantages for vaccine production when compared with genetic reassortants. Companies would have time to respond to regulatory requirements to upgrade their production facilities. Since some European countries regard RG-engineered viruses as ‘genetically modified organisms’, there would be time for European vaccine companies to resolve uncertainties over GMO issues with national regulatory authorities and with the public. Royalty payments could be negotiated with the RG patent holders, avoiding litigation. However, several obstacles still stand in the way.
Experts in intellectual property describe the influenza RG-IP issue as a classic example of market failure. Unless the public sector provides a framework for RG-IP negotiations during interpandemic years, companies will not be prepared to produce pandemic vaccines using RG-engineered reference strains. Moreover, because IP issues are governed by national patent laws, any negotiating framework that is established must be international in scope. The need for an international solution has been acknowledged by WHOError: Reference source not found, but WHO can address the technical but not the IP issues related to RG.
Because of its importance to the European and global supply of pandemic vaccine, efforts must be undertaken immediately to solve the intellectual property issues related to reverse genetics. An international solution is not readily apparent. Political and technical support might be sought not only from EU Member States but also from other institutions such as the Organization for Economic Cooperation and Development (almost all countries with vaccine companies are OECD Member States). The technical support of the World Intellectual Property Organization and the WIPO Arbitration and Mediation Center could be especially helpful 83. Whatever process is chosen, achieving a solution to the problem of intellectual property for reverse genetics represents an important criterion for judging the world’s ability to achieve ‘good governance’ for global public health. 84 9.1.4.Translational ResearchThe research agenda for translational research is based on gaps identified in current knowledge.
6.2-41

6.2: Pandemic Influenza
Remove obstacles to the use of reverse genetics to prepare seed strains for producing ‘pandemic-like’ vaccines and accelerate the introduction of this technology into the production of interpandemic vaccines. These obstacles include the status of intellectual property rights, regulatory requirements (e.g., biosafety) for using these viruses in vaccine production facilities and the acceptability of using these ‘genetically modified organisms’ by regulatory authorities and the public.
Conduct burden of disease studies in several EU Member States to determine the impact of interpandemic influenza on influenza-related hospitalizations and death. Special attention should be given to the elderly, young children and pregnant women.
Conduct yearly observational studies (case-control studies) in several EU Member States on the effectiveness of influenza vaccination in reducing the occurrence of influenza-related complications and death, following an internationally designed WHO protocol for such studies.
Explore the legal and political issues regarding liability for adverse events associated with pandemic vaccination.
Undertake case-control studies during the next influenza season (or during past influenza seasons where appropriate administrative databases exist) to determine whether common treatments for cardiovascular and cerebrovascular diseases are associated with reductions or increases in all influenza-related hospitalizations and deaths, not just those associated with underlying cardiovascular or cerebrovascular diseases. In addition, analyse the databases of large prospective randomized controlled trials of cardiovascular therapies to determine whether subjects in the treatment groups experience reductions or increases in influenza-related events that are independent of the effects of influenza vaccination.
Undertake studies of influenza virus infection in experimental animals to determine whether treatment with commonly available medications that affect the innate immune system alter clinical illness and/or virus shedding. Special attention should be given to the effects of treatment on the development of secondary bacterial pneumonia.
Undertake in vitro cell culture studies to determine whether specific treatments before or shortly after infection with influenza viruses affect the subsequent production of proinflammatory cytokines and other biological response mediators.
9.2. Research to be Carried Out in the Longer Term
The long-term research agenda for vaccines, antiviral agents and non-pharmaceutical research is based on identified gaps in current knowledge.
Continue to explore the potential for developing and clinically testing influenza vaccines that provide heterotypic (broad spectrum) and long-lasting protection, including vaccines directed at the ectodomain of the M2 protein and other conserved influenza proteins.
Conduct clinical studies comparing the efficacy of LAIV and IIV vaccines in children and adults, including assessments of potential correlates of immunity other than serum anti-HA antibody and of the value of each type of vaccine for induction of heterotypic immunity in the different age groups85.
Reassess efficacy and safety of DNA-based influenza vaccines using adjuvants and new delivery systems. These vaccines have shown efficacy
6.2-42

6.2: Pandemic Influenza
in pre-clinical studies and are an attractive alternative to the current vaccines because large-scale production of DNA vaccines would be easy, fast and inexpensive.
Continue to evaluate the short and long-term occurrence of adverse events following influenza vaccination and antiviral treatment.
9.3. Research in Need of Increased Support
Most of the elements of the pharmaceutical and translational research agenda outlined above are not included in or likely to be included in pharmaceutical research traditionally carried out by companies. Therefore, implementing this research strategy will require financial support from public sources.
The current pipeline for new vaccine and antiviral agents is limited because there are few incentives for companies to develop a wider variety of new products. Several factors are responsible for this:
No one knows when the next pandemic will occur. It is not commercially attractive for a company to invest in the development of a product that may never be sold or a technique that is of limited use during the interpandemic period.
Even if a potential pandemic vaccine could be of use in the interpandemic period (for example, vaccinating poultry workers in Southeast Asia with an H5N1 vaccine), it would probably not be affordable in countries at greatest risk.
The current inactivated interpandemic vaccine needs to be re-administered every year. Replacing the current vaccine with a long
73 Fiers W, De Filette M, Birkett A, Neirynck S, Jou WM. A “universal” human influenza A vaccine. Virus Res 2004; 103: 173-6.74 Fan F, Liang XP, Horton MS, et al. Preclinical study of influenza virus A M2 peptide conjugate vaccines in mice, ferrets, and rhesus monkeys. Vaccine 2004; to be published.75 Horimoto T, Takada A, Iwatsuki-Horimoto K, Kawaoka Y. A protective immune response in mice to viral components other than hemagglutinin in a live influenza A virus vaccine model. Vaccine 2004; 22: 2244-7.76 Ge Q, Filip L, Bai A, Nguyen T, Eisen HN, Chen J. Inhibition of influenza virus production in virus-infected mice by RNA interference. Proc Natl Acad Sci USA 2004; 101: 8676-81.77 Tompkins SM, Lo CY, Tumpey TM, Epstein SL. Protection against lethal influenza virus challenge by RNA interference in vivo. Proc Natl Acad Sci USA 2004; 101: 8682-6.78 Geiss GK, Salvatore M, Tumpey TM, et al. Cellular transcriptional profiling in influenza A virus-infected lung epithelial cells: the role of the non-structural NS1 protein in the evasion of the host innate defense and its potential contribution to pandemic influenza. Proc Natl Acad Sci USA 2002; 99: 10736-10741.79 Seo SH, Hoffmann E, Webster RG. The NS1 gene of H5N1 influenza viruses circumvents the host anti-viral cytokine responses. Virus Res 2004; 103: 107-13.80 Hayden FG, Fritz R, Lobo C, Alvord W, Strober W, Straus SE. Local and systemic cytokine responses during experimental human influenza A virus infection. Relation to symptom formation and host defense. J Clin Invest 1998; 101: 643-9.81 Julkunen I, Sareneva T, Pirhonen J, Ronni T, Melen K, Matikainen S. Molecular pathogenesis of influenza A virus infections and virus-induced regulation of cytokine gene expression. Cytokine Growth Factor Rev 2001; 12: 171-80.83 see http://www.wipo.int.
6.2-43
6.2: Pandemic Influenza
lasting vaccine would dramatically decrease profits for the current manufacturers.
Currently one antiviral agent is superior to other antivirals regarding its effectiveness and limited development of antiviral resistance. However, since there is only one manufacturer and potentially a very great demand, this company has little incentive to look for alternative (cheaper) ways to make its product affordable to larger populations.
There may be limited interest on the part of other pharmaceutical companies to explore the possible impact of existing products or new antiviral agents because the profits expected from their sale during the interpandemic period may be limited.
However, several factors might serve as positive incentives to drive the research agenda:
With an increasing interest in vaccinating children, the development of influenza vaccines that are more easily administered could be commercially attractive.
There is increasing interest in using reverse genetics during the interpandemic period. This technique might increase a company’s capacity to produce vaccine, reducing production costs and increasing profit margins. In 2003, the circulating A/Fujian strain could not be included in the Northern Hemisphere’s trivalent vaccine because a high-growth genetic reassortant seed strain that could be used for vaccine production was unavailable. However, an A/Fujian-containing seed strain was produced using reverse genetics. This experience should serve as a stimulus to solve intellectual property rights issues for reverse genetics during the interpandemic period.
All of the research gaps that have been identified meet the requirements for public support by the European Union.
9.4. The Comparative Advantage of the EU
Most of the world’s largest influenza vaccine companies are located in the EU and there is a global dependence on the influenza vaccines produced in the EU. This constitutes a compelling argument for EU support for the research agenda described in this proposal. The research will require a level of public funding beyond that which can be expected from individual EU Member States. Such support will bring added value to the EU because it:
Specifically addresses gaps in knowledge within Europe, Responds to European legislation, and Should result in findings that will benefit to all Member States within the
European Union
Currently, most of the public support for developing pandemic vaccines and antiviral agents is being provided by the US government. There may be additional (political) arguments for obtaining public support for this research
84Fidler DP. Germs, governance, and global health in the wake of SARS. J Clin Invest 2004; 113: 799-804 85 Brown F, Haaheim LR, Wood JM, Schild GC (eds): Laboratory Correlates of Immunity to Influenza - A Reassessment. Dev Biol. Basel: Karger, 2003, vol 115.
6.2-44
6.2: Pandemic Influenza
agenda in order to ensure that European citizens also benefit from the progress being made.
Among the many topics outlined in the research agenda above, three should be given highest priority:
Evaluate different types of monovalent inactivated influenza vaccines (whole virus/split and subunit, adjuvanted/non-adjuvanted, and egg-derived/ cell culture derived) and different vaccination schedules (one/two doses, different dose ranges) using vaccines directed against different hemagglutinin (HA) subtypes considered to have pandemic potential, especially H5N1, H7N7, H9N2 and H2N2. In particular, to ensure the most economic use of a limited vaccine supply, a low-dose priming strategy should be investigated.
Continue to explore the potential for developing influenza vaccines that provide heterotypic (broad spectrum) and long-lasting protection, including vaccines directed at the ectodomain of the M2 protein and other conserved influenza proteins.
Develop new and improved antiviral agents directed at the M2 and NA antigens and explore possibilities for developing other classes of antiviral agents directed at other targets such as the NS1 and HA antigens.
Public funding provided by the European Union to support this research agenda will ensure that Member States are better able to conduct programs for the prevention and control of interpandemic and pandemic influenza. By supporting this research, the European Union will fulfil its responsibilities for maintaining the health and economic wellbeing of all Europeans and contribute to the health and wellbeing of people in other countries throughout the world.
6.2-45
6.2: Pandemic Influenza
10. References
34 Nguyen-Van-Tam JS, Hampson AW. The epidemiology and clinical impact of pandemic influenza. Vaccine 2003; 21: 1762-8.35 Johnson NPAS, Mueller J. Updating the accounts: global mortality of the 1918-1920 “Spanish” influenza pandemic. Bull Hist Med 2002; 76: 105-15.40 Hannoun C, Megas F, Piercy J. Immunogenicity and protective efficacy of influenza vaccination. Virus Res 2004; 103: 133-8.41 Kilbourne ED, Couch RB, Kasel JA, et al. Purified influenza A virus N2 neuraminidase vaccine is immunogenic and non-toxic in humans. Vaccine 1995; 13: 1799-803.42 Brydak LB, Machala, Mysliwska J, Mysliwski A, Trzonkowski P. Immune response to influenza vaccination in an elderly population. J Clin Immunol 2003; 23: 214-22.43 Kilbourne ED, Pokorny BA, Johansson B, Brett I, Milev Y, Matthews JT. Protection of mice with recombinant influenza virus neuraminidase. J Infect Dis 2004; 189: 459-61.44 Nichol KL. The efficacy, effectiveness and cost-effectiveness of inactivated influenza virus vaccines. Vaccine 2003; 21: 1769-75.45 Scuffham PA, West PA. Economic evaluation of strategies for the control and management of influenza in Europe. Vaccine 2002; 21: 2562-78.50 World Health Organization. Recommendations for the use of inactivated influenza vaccines and other preventive measures. Wkly Epidemiol Rec 2000; 75 (35):281-288.51 Kaiser L, Wat C, Mills T, Mahoney P, Ward P, Hayden F. Impact of oseltamivir treatment on influenza-related lower respiratory tract complications and hospitalizations. Arch Intern Med 2003; 163: 1667-72.56 Gerdil C. The annual production cycle for influenza vaccine. Vaccine 2003; 21: 1776-79.33 I Stephenson, KG Nicholson, JM Word, MC Zambon, JM Katz. Confronting the avian influenza threat: vaccine development for a potential pandemic. The Lancet 2004; 4: 499-509.52 Neuraminidase Inhibitors Susceptibility Network. NISN Statement on antiviral resistance in influenza viruses. Wkly Epidemiol Rec 2004 (33): 306-308.57 Nicholson KG, Colegate AE, Podda A, et al. Safety and antigenicity of non-adjuvanted and MF59-adjuvanted influenza A/Duck/Singapore/97 (H5N3) vaccine: a randomized trial of two potential vaccines against H5N1 influenza. Lancet 2001; 357: 1937-43.58 Wood JM. Developing vaccines against pandemic influenza. Phil Trans R Soc Lond B Biol Sci 2001; 356: 1953-60.59 Stephenson I, Nicholson KG, Colegate A, et al. Boosting immunity to influenza H5N1 with MF59-adjuvanted H5N3 A/Duck/Singapore/97 vaccine in a primed human population. Vaccine 2003; 21: 1687-93.60 Stephenson I, Wood JM, Nicholson KG, Charlett A, Zambon MC. Detection of anti-H5 responses in human sera by HI using horse erythrocytes following MF59-adjuvanted
6.2-46
6.2: Pandemic Influenza
influenza A/Duck/Singapore/97 vaccine. Virus Res 2004; 103: 91-5.61 Hehme N, Engelmann H, Kunzel W, Neumeier E. Sanger R. Pandemic preparedness: lessons learnt from H2N2 and H9N2 candidate vaccines. Med Microbiol Immunol (Berl) 2002; 191: 203-8.62 Hehme N, Engelmann H, Kuenzel W, Neumeier E, Saenger R. Immunogenicity of a monovalent, aluminum-adjuvanted influenza whole virus vaccine for pandemic use. Virus Res 2004; 103: 163-71.65 Medema JK, Zoellner YF, Ryan J, Palache AM. Modelling pandemic preparedness scenarios: health economic implications of enhanced pandemic vaccine supply. Virus Res 2004; 103: 9-15.69 Lasky T, Terracciano CJ, Magder L, et al. The Guillain-Barre syndrome and the 1992-1993 and 1993-1994 influenza vaccines. N Engl J Med 1998; 339: 1797-1802.70 National Advisory Committee on Immunization (NACI). Supplementary statement for the 2002-2003 influenza season: update on Oculo-Respiratory Syndrome in association with influenza vaccination. , Can Commun Dis Report 2002; 28 (September 1): ACS-6.71 Mutsch M, Zhou W, Rhodes P et al. Use of the inactivated intranasal influenza vaccine and the risk of Bell’s Palsy in Switzerland. N Engl J Med 2004; 350: 896-903.72 Cassetti C, Couch R, Wood J, Pervikov Y. Report of meeting on the development of influenza vaccines with broad spectrum and long-lasting immune responses. Geneva: World Health Organization, 26-27 February 2004. Submitted for publication. 82 Fedson DS. Pandemic flu vaccine trials and reverse genetics: foundation for effective response to next pandemic. Ensuring an adequate global supply of influenza vaccine. Infect Dis News 2003, December, pp. 4
6.2-47





























