Embed Size (px)
Citation preview
Influencing CareThe Nova Scotia
P.I.E.C.E.S. StoryAlzheimer Society Manitoba, 2008 Conference
Joanne Collins RSW Challenging Behaviour Program
Nova Scotia Department Of Health
Today’s Purpose
To provide:• Overview Nova Scotia Challenging
Behaviour Program• Highlight critical factors in program
design• Highlight using the P.I.E.C.E.S.
approach to support an integrated model of care

Beginnings….• Sector identified the need for improved
services to enhance capacity in care provision particularly complex behaviours
• Department of Health responded and established the Challenging Behaviour Working Group in May 2002
• Working Group had representation from LTC, Home Care, Mental Health and DoH
• Defined Challenging Behaviour and developed an Approach to Care
• Completed majority of tasks in January 2003

Challenging, or complex behaviours, as a result of dementia or mental illness can include:
• Agitation & restlessness
• Anxiety• Apathy/failure to
participate; withdrawn/crying
• Defensive behaviour• Hearing & seeing
things that do not exist• Impulsivity • Intrusiveness
• Hoarding and/or rummaging
• Inappropriate sexual behaviour
• Resistance to care• Suspicious/accusing
others• Vocally disruptive
behaviour• Wandering

Behavioural and Psychological Symptoms of Dementia (BPSD)
BPSD left untreated has been associated with caregiver burnout, nursing home placement, poor management of co-morbid conditions and excess health care costs.
Steel, Cohen, Mansfield, Ballard

Challenges of Challenging Behaviour
• BPSD significantly impacts quality of life of both the person and caregivers (Finkel SJ)
• Caregivers consistently rate BPSD as the most stressful aspect of caring (Jarriot PN)
• Is the primary factor for deciding to institutionalize (Steel C, Balestreri)
• Approximately 50% of people with Severe Dementia Alzheimers Type experience psychosis, 90% behavioural issues, 7-10% severe (Rabins, Zimmer)

Readiness For Change
Opportunity
Policy Advocate
s
Structural Flexible
Organizations
Changes
Sabattier10 Years

Challenging Behaviour Program
Client
In House Resource Consultant (IHRC)
P.I.E.C.E.S Clinical Resource Consultnat(PCRC)
Resource Support & Augmentation
Stabilization Service
LTC Facilities
HC AgenciesFamily
Care-givers
Staff Education & Training
Continuing Care

Education and Training
• Enhance capacity at the organization level in providing service to the older adults with complex cognitive/mental health issues and associated behaviours.
• Target group – Nursing Homes, Home Support Agencies, Nursing Agencies, and Continuing Care Offices
• Develops the In-house Resource Consultant role

P.I.E.C.E.S. Clinical Resource Consultants
• Provide case based consultation to IHRC• Educators, coaches, consultants and
assist in program development • Facilitate Local Learning Networks• Link to community-based resources and
external stakeholders• Promotes linkages between care givers
and specialized resources • Ensures a comprehensive assessment is
conducted pre/post admission to stabilization service

Resource Support and Augmentation
• Temporary short term funding.
• Alternative short term care provision and intervention to stabilize challenging behaviour
• PCRC play a supportive role with requesting agencies and Continuing Care District Offices

Stabilization Service
• Target Population – Client/Residents who have not benefited from interventions targeting complex cognitive/mental health issues and associated behaviours.
• Goal – Assess, stabilize and develop a care plan that will permit the client/resident to be discharged back to the community.
• Access through the PCRC

Program Design
• Step I Gaining multi-Organization and Communities of Interest
Support• Step II Engaging the Learners• Step III Education Program• Step IV Support• Step V Maturation from Education to
Practice• Step VI Putting the P.I.E.C.E.S. together at
the Systems Level

Program DesignStep I : Gaining Multilevel Organizational/
Communities of Interest and Support
Organization Support
Academic
Institutions
Service Organization
Communities of Interest
Consumers
Provincial
Gov.
Target
Learning
Org’s
Chambers
Program Design
Step II: Engaging the Learners
• Education Program• Engage Senior Leaders• Selecting the learners to fulfill the In- House Resource consultant role “Peer/Opinion Leaders”

The P.I.E.C.E.S. Model
Putting the P.I.E.C.E.S Together

PPhysical, IIntellectual, EEmotional,
CCapabilities, EEnvironment, SSocial, and are the cornerstones of the
philosophy and care of the P.I.E.C.E.SP.I.E.C.E.S.. Education
Initiative.
Putting the P.I.E.C.E.S. ...together
What is P.I.E.C.E.S.?What is P.I.E.C.E.S.?• A practical, effective approach to
change and continuous improvement• Best practices in learning &
development • Performance improvement foundation• Provides approach to understanding &
enhancing care• Framework, systematic• Team, Dialogue
PPhysical, IIntellectual, EEmotional, CCapabilities, EEnvironmental, SSocial

The P.I.E.C.E.S. Model Provides
Common vision and set of values
Common language and knowledge for communicating across the system
Common yet comprehensive approach for thinking through problems

P.I.E.C.E.S.P.I.E.C.E.S.A Model for Changing PracticeA Model for Changing Practice
++
Form foundation for a common vision,Form foundation for a common vision, common language and a common approachcommon language and a common approach
P.I.E.C.E.S. Enabler Program for Senior LeadersP.I.E.C.E.S. Enabler Program for Senior Leaders
P.I.E.C.E.S. Education Programs for Professional StaffP.I.E.C.E.S. Education Programs for Professional Staff
Foundation for Practice ChangeFoundation for Practice Change
==
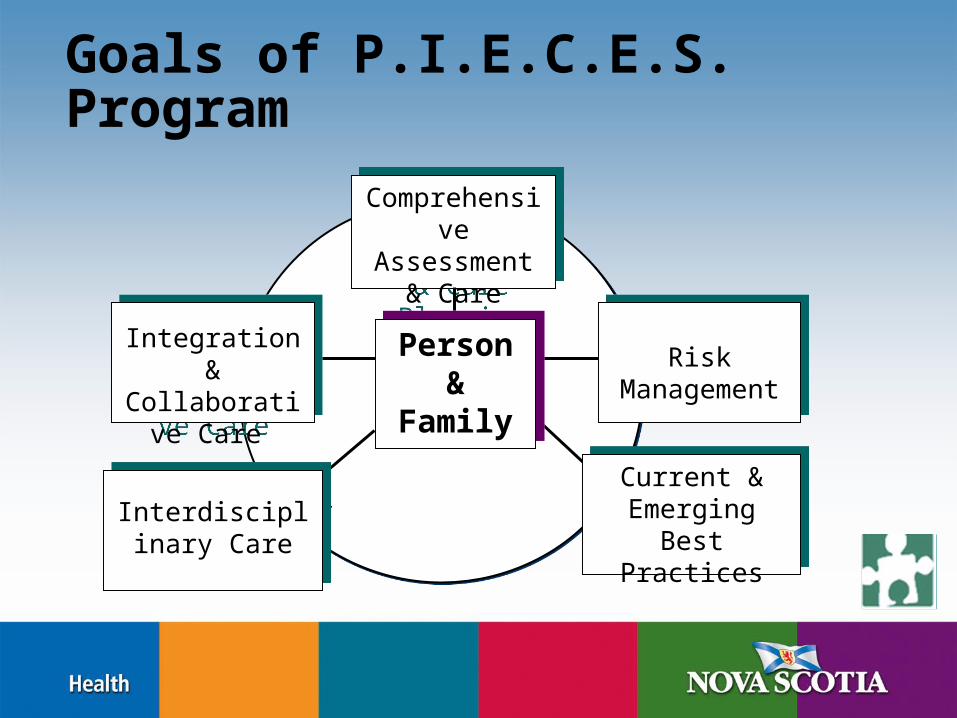
Goals of P.I.E.C.E.S. Program
Comprehensive
Assessment & Care
Planning
Comprehensive
Assessment & Care
PlanningPerson &
Family
Person &
Family
InterdisciplinaryCare
Interdisciplinary Care
Interdisciplinary Care
Current & Emerging Best
Practices
Current & Emerging Best
Practices
Risk Management
Risk Management
Integration & Collaborative
Care
Integration & Collaborative
Care

Enabler Program for Senior Leaders
• 8 hour program• Target audience:
those in a position to supervise regulated and/or unregulated staff but not involved in direct care (I.e Administrator, DOC)
those in a position to support learners/In-house Resource (I.e
Educators)

The 40-hour P.I.E.C.E.S. Program
Prepares the In-house Resource Prepares the In-house Resource Person Person …… to serve as a resource to others in the organization by:
• promoting a common language, common values, and common way method of thinking through complex problems
• modeling P.I.E.C.E.S. competencies
• developing P.I.E.C.E.S. competencies in others.

Step III The Education
• Curriculum development
• 3 staged vis-à-vis Dave Davis
• Importance of Job Aids
• Templates and Tools, Practicality
• Reinforcement and Meta Learning

Enabler Program Objectives
• Familiarize participants with the P.I.E.C.E.S. framework, approach, assessment tools and screening guides taught in the 40-hour program.
• Introduce a practical tool to improve observations of the “Team” and teach the importance of knowledge exchange regarding the client/resident
• Identify clinical and educational coaching and senior leadership support strategies to support the in-house resource role and others in transferring learning to practice change

The Enabler Program Includes Strategies to…….
• Flag gaps between current practice and best practice
• Select the most appropriate candidates and develop an implementation plan
• Explore current approaches to learning and development and performance improvement
• Support change efforts • Engage team in collaborative improvement
efforts

The 40-hour P.I.E.C.E.S. Program
• Part 1: 18-hour intensive program of core curriculum
• Part 2: Practical application of skills from Part 1
• Part 3: 12-hour consolidation program
• Part 4: Post-program support

Core Competencies1. Detect or flag what has changed
2. Use the 3-Q P.I.E.C.E.S.3-Q P.I.E.C.E.S. template
3. Be familiar with tools
4. Plan care with others
5. Evaluate care and goals
6. Coach others using U-First collaborative care tool

3-Question Template
Q. 1Q. 1 What has changed? Avoid assumptions; think atypical.
Q. 2Q. 2 What are the RISKS and possible causes?Think P.I.E.C.E.S.
Q. 3Q. 3 What is the action?InvestigationsInteractions Information

Collaborative Care Tool U-FIRST!
PI
E
CE
S
Understanding Flag
Interact
Reflect and Report
Support
Tools and Techniques
• Abilities: Lawton
• Behavior: DOS, Cohen
• Cognition: CAM, Clock, Folstein
• Distress Caregiver PIECES revisited
• Emotional, Depression/Mood; Psychosis (7D)

Performance Objectives
• 4 objectives which describe outcomes in terms of “on-the-job” performance
• Measurable
• Achievable over one year

Evaluation Strategies
• Pre-program assessment
• After 3-day and 2-day session
• In-class work and observation
• On-the-job performance demonstration
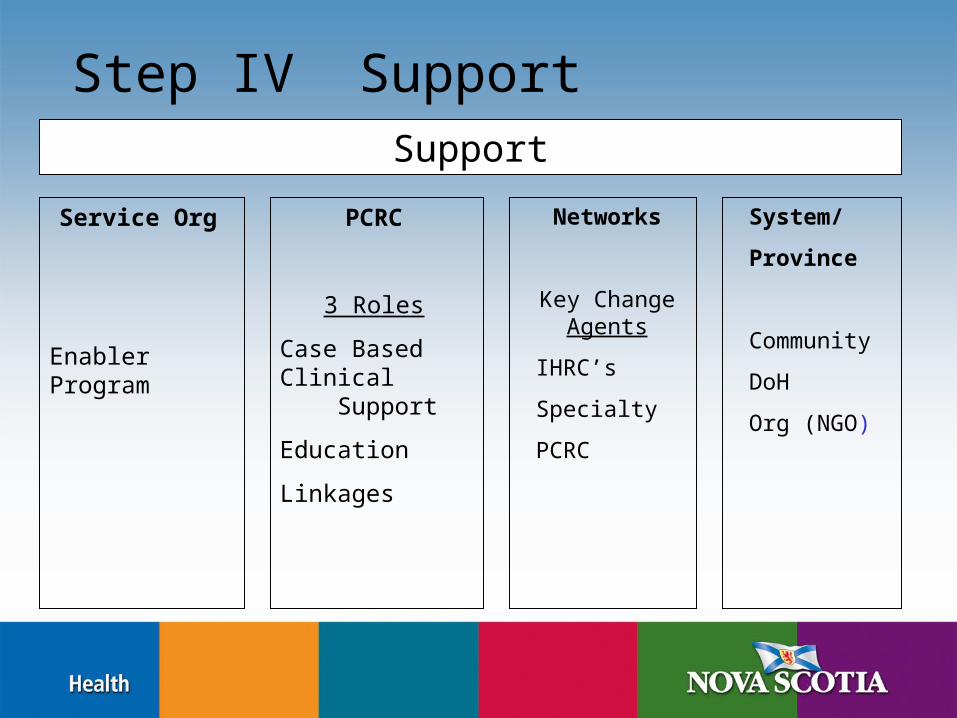
Step IV SupportSupport
Service Org
Enabler Program
PCRC
3 Roles
Case Based Clinical Support
Education
Linkages
Networks
Key Change Agents
IHRC’s
Specialty
PCRC
System/
Province
Community
DoH
Org (NGO)
To change systems we:
• Assess the potential for change
• Get the whole system in the room
• Focus on the future
• Structure tasks people can do themselves
Marvin Weisbord

Commitment From Enablers
• Leadership support is critical to success
• Support the In-house Resource role
• Promote application and integration of new learning into day to day practice
• Strengthen learner skills

What have we learned?
Elements for success of In-house Elements for success of In-house Resource roleResource role
Right person(s) selected; peer leaderSupport from Senior Leadership, care teamClinical P.I.E.C.E.S. Resource Consultants Development of Local Learning Networks

Through P.I.E.C.E.S.P.I.E.C.E.S. Education Collaborative Care is enhanced:
Individual Team Organization System
Training canchange
individual behaviours
Increased collaboration& results at
the team level
Visionlinked to teamand individual
outcomes
Part of a larger program
to support system change
Accountability to front line

P.I.E.C.E.S. Clinical Resource Consultants
• Capacity to catch and promote the vision
• Clinical background – knowledge of Alzheimer’s Disease and other dementia’s
• Coach
• Ability to establish and foster collaborative and consultative relationships at the individual, team, organization and system levels
• Networking and Team Building
• Champion

Elements for Success in the System
• Translatable and transferable
• Framework
• Multi-level awareness and support
• Intersectoral Community Stakeholder Group
• Telepsychiatry
• Importance of Local Resources
• Ongoing Learning Support
• Evaluation

Benefits of the P.I.E.C.E. S. Model
• Increased capacity among continuing care providers.
• A common vision, approach (framework) and language.
• A vehicle to link people, ideas and resources at the
- Clinical- Service Coordination- Systems Level

Step V• Maturation from Education to day-to-day
practice
Step VI• Putting the P.I.E.C.E.S. together at a
systems levelFrom……….
Education to Knowledge
to
Translation and Exchange

Thank You
Questions? Comments !





























