Embed Size (px)
Citation preview

1695
Prognosis of functional outcome after ischemic stroke is influenced by a variety of factors already assessable in
the acute phase and within the first days after symptom onset. In clinical trials, stroke outcome is most commonly rated by the modified Rankin Scale (mRS)1 because of the valid-ity and rapid application of this rating scale and its ability to discriminate clinically relevant levels of disability and recov-ery.2–4 Brain imaging in the early phase after stroke onset pro-vides valuable information related to individual functional recovery.5,6 In particular, structural MRI identifies injured brain regions and allows for assessment of extent and loca-tion, both known to influence and predict functional outcome measured by the mRS.3 However, infarct volume from early
MRI correlates only moderately with the mRS at later time points,7,8 indicating that additional factors, such as lesion loca-tion, influence functional outcome. It is therefore of major interest to elucidate the relationship between early lesion pat-terns and functional impairment in the later course of stroke.
Clinical impact of lesion locations can be inferred from voxel-based lesion symptom mapping (VLSM). This statisti-cal method examines effects of brain lesions on behavioral scores on a voxel-by-voxel base. Therefore, a statistical test is conducted for each voxel to detect differences in a behav-ioral score based on the presence or absence of injury.9 VLSM produces statistical results that map structural lesions to a behavioral scale. In patients with chronic stroke, it has been
Background and Purpose—In the early days after ischemic stroke, information on structural brain damage from MRI supports prognosis of functional outcome. It is rated widely by the modified Rankin Scale that correlates only moderately with lesion volume. We therefore aimed to elucidate the influence of lesion location from early MRI (days 2–3) on functional outcome after 1 month using voxel-based lesion symptom mapping.
Methods—We analyzed clinical and MRI data of patients from a prospective European multicenter stroke imaging study (I-KNOW). Lesions were delineated on fluid-attenuated inversion recovery images on days 2 to 3 after stroke onset. We generated statistic maps of lesion contribution related to clinical outcome (modified Rankin Scale) after 1 month using voxel-based lesion symptom mapping.
Results—Lesion maps of 101 patients with middle cerebral artery infarctions were included for analysis (right-sided stroke, 47%). Mean age was 67 years, median admission National Institutes of Health Stroke Scale was 11. Mean infarct volumes were comparable between both sides (left, 37.5 mL; right, 43.7 mL). Voxel-based lesion symptom mapping revealed areas with high influence on higher modified Rankin Scale in regions involving the corona radiata, internal capsule, and insula. In addition, asymmetrically distributed impact patterns were found involving the right inferior temporal gyrus and left superior temporal gyrus.
Conclusions—In this group of patients with stroke, characteristic lesion patterns in areas of motor control and areas involved in lateralized brain functions on early MRI were found to influence functional outcome. Our data provide a novel map of the impact of lesion localization on functional stroke outcome as measured by the modified Rankin Scale. (Stroke. 2014;45:1695-1702.)
Key Words: magnetic resonance imaging ◼ stroke
Influence of Stroke Infarct Location on Functional Outcome Measured by the Modified Rankin Scale
Bastian Cheng, MD; Nils Daniel Forkert, PhD; Melissa Zavaglia, PhD; Claus C. Hilgetag, PhD; Amir Golsari, MD; Susanne Siemonsen, MD; Jens Fiehler, MD; Salvador Pedraza, MD;
Josep Puig, MD; Tae-Hee Cho, MD, PhD; Josef Alawneh, PhD; Jean-Claude Baron, MD, ScD; Leif Ostergaard, MD, PhD; Christian Gerloff, MD; Götz Thomalla, MD
Received February 13, 2014; final revision received March 26, 2014; accepted March 31, 2014.From the Department of Neurology (B.C., A.G., C.G., G.T.), Department of Computational Neuroscience (N.D.F., M.Z., C.H.), and Department of
Neuroradiology (S.S., J.F.), University Medical Center Hamburg-Eppendorf, Hamburg, Germany; Department of Radiology (IDI), Girona Biomedical Research Institute (IDIBGI), Hospital Universitari de Girona Dr Josep Trueta, Girona, Spain (S.P., J.P.); Department of Neurology, Hospices Civils de Lyon, Lyon, France (T.-H.C.); Centre de Psychiatrie & Neurosciences, Inserm U894, Centre Hospitalier Sainte Anne, Sorbonne Paris Cité, Paris, France (J.-C.B.); Department of Clinical Neurosciences, University of Cambridge, Addenbrooke’s Hospital, Cambridge, United Kingdom (J.A., J.-C.B.); and Department of Neuroradiology, Aarhus University Hospital and Center of Functionally Integrative Neuroscience/MINDLab, Aarhus University, Aarhus, Denmark (L.O.).
The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA. 114.005152/-/DC1.
Correspondence to Bastian Cheng, MD, Klinik und Poliklinik für Neurologie, Kopf- und Neurozentrum, Universitätsklinikum Hamburg-Eppendorf, Martinistr 52, 20246 Hamburg, Germany. E-mail [email protected]
© 2014 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.114.005152
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
pril 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
pril 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
pril 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
pril 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on A
pril 12, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

1696 Stroke June 2014
applied to identify areas critical for motor recovery,10 spatial neglects,11 and language comprehension.12
In this study, we examined stroke lesion pattern from early MRI (days 2–3) to identify lesion locations that influ-ence clinical outcome measured by the mRS after 1 month. We hypothesized that (1) brain areas linked to physical dis-ability will show a strong association with higher mRS values (ie, worse clinical outcome) and (2) different lesion locations would characterize individual contribution to functional out-come depending on hemisphere side.
MethodsPatients and Clinical AssessmentWe analyzed MRI and clinical data from the I-KNOW database (http://www.i-know-stroke.eu). I-KNOW was an European multicenter study aiming at collecting a large sample of patients with anterior circulation stroke, who underwent both admission and follow-up MRI to derive maps of infarct prediction based on clinical and imaging variables. In I-KNOW, patients with first-ever stroke and a National Institutes of Health Stroke Scale (NIHSS) >4, MRI ≤12 hours of witnessed stroke onset, and either conservative or intravenous thrombolytic treatment were included. Among other clinical parameters, patient age, sex, side of ischemic lesion, severity of neurological deficit on admission as-sessed by the NIHSS, and functional deficit (measured by the mRS) before stroke and after 1 month were recorded.
The mRS consists of 7 grades rated as follows: 0, no symptoms at all; 1, no significant disability: despite symptoms, able to perform all usual duties and activities; 2, slight disability: unable to perform all previous activities but able to look after own affairs without as-sistance; 3, moderate disability: requiring some help but able to walk without assistance; 4, moderately severe disability: unable to walk without assistance and unable to attend to own bodily needs without assistance; 5, severe disability: bedridden, incontinent, and requiring constant nursing care and attention; and 6, death.
In addition to the original inclusion criteria, we selected only pa-tients without previous functional deficits (mRS before stroke, 0), MRI data on days 2 to 3, and mRS after 1 month. The study was ap-proved by the local ethics committees and institutional review boards (University Centre Hamburg-Eppendorf, Germany).
Imaging DataFluid-attenuated inversion recovery (FLAIR) and diffusion-weighted imaging data were acquired on 1.5 magnets according to the I-KNOW imaging protocol. Data were acquired at days 2 to 3 after stroke onset. Typical imaging parameters for FLAIR se-quences were echo time, 100 ms; repetition time, 8000 ms; in-version time, 2300 ms; field of view, 250; and slice thickness, 5 mm. For diffusion-weighted imaging: b value, 1000 s/mm2; echo time, 100 ms; repetition time, 5000 ms; field of view, 250; and slice thickness, 3 mm. Stroke lesions were segmented on FLAIR im-aging data using an in-house developed software tool for the analysis of stroke image sequences (AnToNIa, Analysis Tool for Neuro Image Data)13: first, a rough region of interest (ROI) surrounding the FLAIR lesion was drawn manually with a generous margin at each affected slice. The single ROIs were then combined to a volume of interest and refined by manually applying and adjusting a lower threshold of FLAIR signal intensity. Voxel exhibiting signal intensities below this threshold were rejected from the initial lesion volume of inter-est. Accuracy of lesion delineation was inspected visually at each slice, and the corresponding diffusion-weighted imaging images were consulted for confirming plausibility and extent of infarct ROI. If required, manual correction was performed. It has been shown that FLAIR images provide high sensitivity for acute cerebral infarcts with high interobserver and intertechnique reproducibility for the detection of ischemic lesions.14–16 Lesion volumes were calculated for each re-fined volume of interest. After this, the FLAIR data set of each patient was registered to the standard Montreal Neurological Institute (MNI)17
brain atlas. Therefore, the individual optimal affine transformation of each FLAIR data set to the reference atlas was calculated using the mutual information metric and linear interpolation. The resulting affine transformation was then used to align the segmented FLAIR lesion in the MNI atlas space using a nearest-neighbor interpolation.
For VLSM, we used the nonparametric mapping toolbox included in the MRIcron software package18 (MRIcron, Version 6.6.2013). All lesion volume of interest (n=101) were flipped onto the left hemisphere to increase statistical power identifying lesion pattern with significant contribution to functional outcome independent of lesioned hemisphere. Lesion overlap was calculated to create a color-coded overlay map of injured voxel across all patients to provide an overview of all lesioned brain areas and areas with highest lesion frequency. We then performed a group comparison for each voxel (lesioned or nonlesioned) using the mRS as dependent variable and the Brunner and Munzel Rank order test implemented in the nonparametric mapping toolbox.18 This test provides a Z score map where higher values indicate higher impact on (worse) recovery. To correct for multiple comparisons, we used a permutation-based familywise error (FWE) correction with 2000 per-mutations. Only voxel affected in ≥10 individuals (10%) were tested. A FWE correction threshold of 5% was applied. In the resulting figures, the color range indicates Z scores resulting from Brunner–Munzel test-ing corrected for multiple comparison.
In a second step, we investigated hemisphere-specific influences. Therefore, the Brunner and Munzel Rank order test was calculated for each hemisphere so that 2 separate tests were performed for right- and left-sided lesions (n=47 right and n=54 left). Accounting for the lower sample size and exploratory nature of this analysis, we choose a false discovery rate (FDR) of 1% (0.01) to correct for FWEs. Although the FDR is a more liberal method then conventional FWE correction, this threshold ensures that false-positive results do not exceed >1% of all true-positive results.
Resulting statistical maps were processed using imaging tools of the Functional MRI of the Brain Software Library (FMRIB Software Library; http://www.fmrib.ox.ac.uk/fsl).19 Therefore, Z score maps were masked with anatomic ROIs provided by the Harvard-Oxford Cortical Structural Atlas20 and Johns Hopkins University International
Table 1. Baseline Characteristics of Included Patients (n=101)
Left Hemisphere Stroke
Right Hemisphere Stroke P Value
Frequency, n 54 47 …
Mean age, y (95% CI) 70 (67–72) 64 (60–68) 0.023
Mean NIHSS at admission (95% CI)
12.1 (10.5–13.7) 10.8 (9.1–12.4) 0.33
Median NIHSS at admission (IQR)
11 (9) 11 (9) …
FLAIR lesion volume at days 2–3 (95% CI)
37.7 (23.6–51.7) 43.2 (27.6–58.9) 0.89
Mean mRS at day 30 (95% CI) 2.1 (1.6–2.6) 2.1 (1.7–2.5) 0.85
Median mRS at day 30 (IQR) 2 (4) 2 (2) …
Frequency of mRS subscores, n
0 15 6 …
1 11 14 …
2 9 10 …
3 4 8 …
4 9 7 …
5 6 2 …
6 0 0 …
P values are shown resulting from group comparisons between patients with left- and right-hemispheric stroke lesions. CI indicates confidence interval; FLAIR, fluid-attenuated inversion recovery; IQR, interquartile range; mRS, modified Rankin Scale; and NIHSS, National Institutes of Health Stroke Scale.
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

Cheng et al Impact of Stroke Location on Functional Outcome 1697
Consortium of Brain Mapping Diffusion Tensor Imaging (JHU ICBM-DTI)-81 White Matter Labels21 implemented in FMRIB Software Library. Median, minimum, and maximum Z score values were cal-culated in each anatomic ROI and voxel coordinates of peak values located automatically using imaging tools implemented in FMRIB Software Library.
Statistical AnalysisClinical data were described with mean and 95% confidence intervals for continuous data and numbers and percentage for categorical data. Group comparison of clinical and imaging data between patients with right- and left-hemispheric stroke was performed using an indepen-dent t test or Wilcoxon rank-sum test as appropriate. Correlation of lesion volumes with clinical outcome (mRS) was analyzed using Spearman ρ correlation coefficient. Statistical analysis was done us-ing SPSS version 20.0 (IBM Co, Somers, NY).
ResultsPatient CharacteristicsOf 168 patients included in the I-KNOW database, 67 patients were excluded from analysis because of MRI data of insuf-ficient quality or missing data at days 2 to 3. In total, clinical and MRI data of 101 patients were analyzed. Details of clini-cal data are given in Table 1.
The right hemisphere was affected in 47 patients (47%). Mean values of individual NIHSS items on admission are shown in Figure I and Table I in the online-only Data Supplement according to affected hemisphere. Baseline
characteristics depending on lesion side are shown in Table 1. In group comparison, mean age was higher in patients with left-sided infarction (P=0.023). There were no significant dif-ferences between groups as to clinical impairment measured by the NIHSS at admission or mRS after 1 month. Lesion vol-umes were comparable between both sides (left side, 37.7 mL; 95% confidence interval, 23.6–51.7 mL and right side, 43.2 mL; 95% confidence interval, 27.6–58.9 mL). Overall mean lesion volume on days 2 to 3 was 40.1 mL (95% confidence interval, 30–50.1). Lesion volume on days 2 to 3 correlated moderately with functional outcome after 1 month as mea-sured by the mRS (r=0.624; P<0.001).
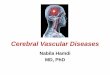
Voxel-Based Lesion Symptom MappingColor-coded overlays of FLAIR stroke lesion distribution on days 2 to 3 of all patients after flipping onto the left hemi-sphere (n=101) are shown in Figure 1. Highest frequency of injury was observed in the deep territory of the middle cere-bral artery (MCA) with lesion distribution concentrating at the striatocapsular region and insula and decreasing toward the borders of the MCA territory.
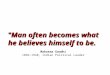
Results of VLSM are shown in Figure 2 by color-coded overlays. A permutation FWE correction (threshold=0.05) resulted in a Z score value of 4.8. Z values and anatomic MNI coordinates of voxels with highest Z score values are given in Table 2. A full list of minimal, maximal, mean, and median Z
Figure 1. Overlay lesion plot of stroke lesions on days 2 to 3 after stroke onset. Data from all patients (n=101) are shown. All lesions are flipped onto the left hemisphere. The color bar indicates number of overlapping lesions. Overlays are thresholded to show lesions present in >10 (10%) patients as included in the voxel-based lesion symptom map-ping analysis. Montreal Neurological Institute coor-dinates of each transverse section (z axis) are given.
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

1698 Stroke June 2014
score values of all template ROIs is provided in Table II in the online-only Data Supplement. Mapping of the mRS revealed significant contribution of brain regions comprising the motor pathway, namely the posterior limb of the internal capsule and corona radiata. Moreover, injury involving the insular and oper-cular cortex was associated strongly with higher mRS values.
Results of VLSM for each separate hemisphere (right, n=47; left, n=54) are shown in Figure 3. Lesion overlays for both hemispheres are shown in Figure II in the online-only Data Supplement. A FDR correction (threshold=0.01) resulted in Z score values of 3.1 (right hemisphere) and 2.7 (left hemisphere). On visual inspection, VLSM showed lateralized influences of stroke lesions on the mRS reflected by mean and maximal z
values (Table III in the online-only Data Supplement). In the right hemisphere, this asymmetry was prominent in the inferior parietal lobe, specifically in the angular gyrus (MNI coordi-nates of peak value, 54, −52, 26; Z score, 3.9). In the left hemi-sphere, a cluster of injured voxel in the middle and superior temporal gyrus influenced mRS values (MNI coordinates of peak value, −48, −34, 2; Z score, 3.54). See also Figure 4 for an annotated version of the VLSM map.
DiscussionUsing VLSM, we examined the influence of lesion localization from early MRI on functional outcome as assessed by the mRS after 1 month. We studied a representative group of patients
Table 2. Anatomic Coordinates of Maximal Z Score Values Resulting From Voxel-Based Lesion Symptom Mapping in Selected Regions Identified by the Harvard-Oxford Cortical Structural Atlas and JHU ICBM-DTI-81 White Matter Labels
Region MNI Coordinates Max Z Score Mean Z Score Median Z Score SD
Central opercular cortex −54, −4, 12 8.0 4.4 4.4 1.1
Corona radiata (posterior part) −26, −28, 22 7.1 4.3 3.9 1.3
Corona radiata (superior part) −24, −18, 3 8.2 4.2 4.0 1.0
Capsula externa −32, −4, 4 8.0 4.1 4.2 1.3
Capsula interna (posterior limb) −26, −26, 18 6.9 3.6 3.5 0.7
Insular cortex −40, −12, 8 7.2 3.3 3.2 1.4
All coordinates are given in MNI space. Mean, median, and SD of Z scores in selected regions are shown. Familywise error correction (0.05) resulted in a threshold for Z score of 4.8. JHU ICBM-DTI indicates Johns Hopkins University International Consortium of Brain Mapping Diffusion Tensor Imaging; and MNI, Montreal Neurological Institute.
Figure 2. Voxel-wise statistical analysis of fluid-attenuated inversion recovery lesion impact (days 2–3) on functional outcome (modified Rankin Scale [mRS]) after 1 month. Analysis of all patients (n=101) with lesions flipped onto the left hemisphere. The color range indicates Z scores resulting from Brunner–Munzel testing corrected for multiple comparison by permutation familywise error (FWE) correction with a threshold of 1% (0.01). Higher Z scores (red) indicate areas asso-ciated with worse clinical outcome (mRS). Montreal Neurological Institute coordi-nates of each transverse section (z axis) are given. FWE correction (0.05) resulted in a threshold for Z score of 4.8.
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

Cheng et al Impact of Stroke Location on Functional Outcome 1699
with moderate to severe stroke reflected by a mean NIHSS score of 11. Lesions were distributed throughout the MCA territory showing a typical distribution overlap pattern simi-lar to previous observation.22 Our results illustrate the complex
relationship between spatial pattern of injury and functional deficits in patients with stroke. In addition to the known impact of lesion volume on functional outcome, we present a novel map linking structural brain damage with the mRS.
Figure 3. Voxel-based lesion symptom mapping of lesion impact on modified Rankin Scale (mRS) cal-culated separately for each hemisphere (right side, n=47; left side, n=54). The color range indicates Z scores resulting from Brunner–Munzel test thres-holded at 1% (0.01) false discovery rate. Higher Z scores (red) indicate areas associated with worse clinical outcome (mRS). Montreal Neurological Insti-tute coordinates of each transverse section (z axis) are given. Note that the false discovery rate correc-tion (threshold=0.01) resulted in a Z score values of 3.1 (right hemisphere) and 2.7 (left hemisphere).
Figure 4. Annotated statistical maps as shown in Figure 3. The color range indicates Z scores result-ing from voxel-based lesion symptom mapping sep-arately in each hemisphere thresholded at 1% false discovery rate. Anatomic structures are identified according to International Consortium of Brain Map-ping Diffusion Tensor Imaging (ICBM-DTI)-81 white matter labels and Harvard-Oxford Cortical Structural Atlas. Higher Z scores (red) indicate areas associ-ated with worse clinical outcome (modified Rankin Scale). Montreal Neurological Institute coordinates (z axis) are given. COC indicates central opercular cortex; IPC, inferior parietal cortex; MTC, middle temporal cortex; and STC, superior temporal cortex.
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

1700 Stroke June 2014
Assessment of lesion symptom maps yielded 2 main find-ings: first, injury to areas of the corticospinal tract related to higher functional impairment as measured by the mRS. In our group, patients recovered less well depending on damage to the corona radiata (and lack thereof, see Figure 2). These intui-tive findings are in line with previous studies mapping corti-cospinal tract lesions to motor impairment and motor function recovery in patients with ischemic stroke.23–27 Using a similar methodological approach, Lo et al10 identified areas in the corona radiata critical for motor function recovery measured by the Arm Motor Ability Test. The mRS broadly assesses the degree of disability or dependence in the daily activities, which strongly depend on intact motor functions.4 Results from valid-ity studies show that specific clinical impairments, such as limb weakness, contribute significantly to short- and long-term disability measured by the mRS.28 This aspect of our findings is, therefore, plausible and highlights the clinical meaning of the mRS from a structural and anatomic perspective.
A considerably high impact on functional outcome was also found at the insula and surrounding opercular cortex. There are several aspects to this finding: insular lesions are common in nonlacunar strokes and have found in up to half of all patients with MCA infarcts.29 This is also the case in our group of patients as shown by the overlap map of lesion distribution (Figure 1). Moreover, insular involvement often occurs in proximal occlusion of MCA causing large infarct volumes and damage to the lenticulostriate subcortical terri-tory of the MCA, both of which result in severe motor deficits and low functional outcome.30 However, the exact means by which damage to the insula influences clinical outcome is not known. In recent years, a variety of clinical deficits are being attributed to insular injury, including speech and language, hand-and-eye motor movement, space and body perception, and cardiovascular regulation.31 Impairment of some of these functions has also been shown in patients with ischemic stroke.32–34 Insular lesion influence on clinical outcome mea-sured by the mRS is, however, less clear and interpretation of our results have to remain speculative in this regard.
The second finding of our study illustrates the distinct influ-ence of brain lesions depending on hemisphere side. Although lesion symptom mapping patterns seem fairly evenly distrib-uted in the striatocapsular regions in both hemispheres, asym-metrical patterns were detected involving the right inferior parietal lobe and left superior/middle temporal lobe (Figures 3 and 4). About the right hemisphere, one might speculate that damage to the inferior parietal lobule leads to neglect, which in turn disturbs a wide range of activities of daily living captured by the mRS. In our group, half of all patients with right-sided infarctions (n=24; 51%) showed clinical signs of neglect on admission measured by the NIHSS (item extinc-tion and inattention >0 points; Figure 1). The right inferior parietal lobe is anatomically and functionally linked to frontal and temporal areas creating a perisylvian neural network pro-posed to represent the anatomic basis for functions involving spatial orientation and exploration.35 Furthermore, damage to the right inferior parietal lobe was associated with visual–spatial components of neglect in a VLSM study of 80 patients with right hemisphere stroke.36 From a clinical point of view, neglect strongly influences functional outcome after stroke by
either interfering with correct processing of external stimuli37 or in its negative effect on motor rehabilitation,38 which is also reflected by higher mRS scores.
With regard to the left hemisphere, an additional asym-metrical lesion pattern was apparent in the superior and middle temporal cortex (Figures 3 and 4). In analogy to the common functional right-sided lateralization of neglect, these findings in the left hemisphere could point to the influence of aphasia on functional rehabilitation. Both, the superior and middle temporal gyrus, have been found to facilitate auditory language comprehension39 and have been highlighted as criti-cal regions in patients with poststroke aphasia by VLSM and voxel-based morphometry.40 Global aphasia has been dem-onstrated previously to represent a significant risk factor for higher mRS values.41
Left-to-right asymmetry in lesion impact maps underscores that the mRS as a global disability scale is weighted toward functions of the dominant hemisphere. A similar result has been found accounting for functional deficits measured by the NIHSS.42 Previous studies have reported an impact of hemi-sphere side on clinical characteristics at baseline, treatment outcome, and functional recovery of patients with stroke.43–45 However, studies of clinical outcome comparing patients with right- or left-sided lesions have been inconclusive possibly because of selection bias introduced at different time points starting from symptom recognition to selection for rehabilita-tion admission.46 Our findings highlight the fact that impact of structural lesions on recovery involves specific brain regions depending on hemisphere side. Thus, we extend previous findings by providing localized maps that add to information gained by clinical examination (clinical score) or basic imag-ing (stroke lesion side and volume).
We have studied findings from a representative group of moderately to severely affected patients with stroke. However, exclusion of mildly affected patients (NIHSS <4) limits inter-pretation of our results. An additional selection bias is intro-duced by inclusion of patients with MRI examinations that might not have been tolerated by patients with severe clini-cal deficits. Similarly, patients with posterior territory stroke, especially patients with isolated visual field defects, are not represented in our results.
Lesion mapping can identify brain areas that are critical for clinical functions. However, it is not possible to infer causality. In our work, we used FDR to correct for multiple comparisons from VLSM separated by hemisphere side. This liberal cor-rection controls the rate of false alarms to true hits, as previ-ously applied in lesion analysis.9,47 Given the large number of brain voxels and the fact of cross-dependency with regard to function, FDR correction seems a reasonable approach for an exploratory analysis without dramatically increasing the rate of false-positive results. In addition, our analysis is limited by the lack of factors that have been shown to predict functional outcome after stroke, most notably the initial NIHSS, patient age, and lesion volume. We have chosen FLAIR imaging for lesion delineation in accordance with previous VLSM stud-ies in stroke population at similar time points.11,48 Although accuracy of lesion localization and extent was checked in cor-responding diffusion-weighted imaging datasets, we cannot exclude a confounding influence of FLAIR hyperintensities
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

Cheng et al Impact of Stroke Location on Functional Outcome 1701
resulting from pre-existing white matter lesions. Finally, we acknowledge the arbitrary and limited nature of clinical scores selected in this study. Although the mRS is currently the most commonly used outcome scale in clinical stroke studies, selec-tion of other available outcome measures (NIHSS, Barthel Index, and Glasgow Outcome Scale) will most likely result in different results and should be examined in future studies.
ConclusionsOur study provides a novel atlas of structural lesion impact on functional outcome after stroke using early MRI at days 2 to 3 after stroke onset. Lesion-symptom maps demonstrate spe-cific influence of motor pathway injury on the mRS and reflect lateralized functions such as neglect and aphasia. Our results provide insight into the impact of structural brain injury on functional outcome as captured by the mRS as the most com-monly used outcome rating scale in clinical stroke research.
Sources of FundingThis work was supported by the Deutsche Forschungsgemeinschaft (DFG), Sonderforschungsbereich (SFB) 936, Project C2 and by the European Union (EU) Grant I-KNOW (027294). Dr Hilgetag re-ceived research grant from the DFG, SFB 936, Project A1 (no com-pensation). Dr Gerloff received research grant from the DFG, SFB 936, Project C1 (no compensation) and the EU, Seventh Framework Project WAKE-UP, Grant No. 278276 (no compensation). Dr Thomalla received research grant from the EU, Seventh Framework Project WAKE-UP, Grant No. 278276 (no compensation).
DisclosuresNone.
References 1. Rankin J. Cerebral vascular accidents in patients over the age of 60. III.
Diagnosis and treatment. Scott Med J. 1957;2:254–268. 2. Sulter G, Steen C, De Keyser J. Use of the Barthel index and modified
Rankin scale in acute stroke trials. Stroke. 1999;30:1538–1541. 3. Banks JL, Marotta CA. Outcomes validity and reliability of the modified
Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38:1091–1096.
4. de Haan R, Limburg M, Bossuyt P, van der Meulen J, Aaronson N. The clinical meaning of Rankin ‘handicap’ grades after stroke. Stroke. 1995;26:2027–2030.
5. Gale SD, Pearson CM. Neuroimaging predictors of stroke out-come: implications for neurorehabilitation. NeuroRehabilitation. 2012;31:331–344.
6. Farr TD, Wegener S. Use of magnetic resonance imaging to predict outcome after stroke: a review of experimental and clinical evidence. J Cereb Blood Flow Metab. 2010;30:703–717.
7. Schiemanck SK, Post MW, Kwakkel G, Witkamp TD, Kappelle LJ, Prevo AJ. Ischemic lesion volume correlates with long-term functional outcome and quality of life of middle cerebral artery stroke survivors. Restor Neurol Neurosci. 2005;23:257–263.
8. Lev MH, Segal AZ, Farkas J, Hossain ST, Putman C, Hunter GJ, et al. Utility of perfusion-weighted CT imaging in acute middle cerebral artery stroke treated with intra-arterial thrombolysis: prediction of final infarct volume and clinical outcome. Stroke. 2001;32:2021–2028.
9. Bates E, Wilson SM, Saygin AP, Dick F, Sereno MI, Knight RT, et al. Voxel-based lesion-symptom mapping. Nat Neurosci. 2003;6:448–450.
10. Lo R, Gitelman D, Levy R, Hulvershorn J, Parrish T. Identification of critical areas for motor function recovery in chronic stroke subjects using voxel-based lesion symptom mapping. Neuroimage. 2010;49:9–18.
11. Karnath HO, Rennig J, Johannsen L, Rorden C. The anatomy under-lying acute versus chronic spatial neglect: a longitudinal study. Brain. 2011;134(pt 3):903–912.
12. Magnusdottir S, Fillmore P, den Ouden DB, Hjaltason H, Rorden C, Kjartansson O, et al. Damage to left anterior temporal cortex predicts
impairment of complex syntactic processing: a lesion-symptom mapping study. Hum Brain Mapp. 2013;34:2715–2723.
13. Cheng B, Brinkmann M, Forkert ND, Treszl A, Ebinger M, Köhrmann M, et al; STIR and VISTA Imaging Investigators. Quantitative measure-ments of relative fluid-attenuated inversion recovery (FLAIR) signal intensities in acute stroke for the prediction of time from symptom onset. J Cereb Blood Flow Metab. 2013;33:76–84.
14. Brant-Zawadzki M, Atkinson D, Detrick M, Bradley WG, Scidmore G. Fluid-attenuated inversion recovery (FLAIR) for assessment of cerebral infarction. Initial clinical experience in 50 patients. Stroke. 1996;27:1187–1191.
15. Neumann AB, Jonsdottir KY, Mouridsen K, Hjort N, Gyldensted C, Bizzi A, et al. Interrater agreement for final infarct MRI lesion delinea-tion. Stroke. 2009;40:3768–3771.
16. Noguchi K, Ogawa T, Inugami A, Fujita H, Hatazawa J, Shimosegawa E, et al. MRI of acute cerebral infarction: a comparison of FLAIR and T2-weighted fast spin-echo imaging. Neuroradiology. 1997;39:406–410.
17. Mazziotta J, Toga A, Evans A, Fox P, Lancaster J, Zilles K, et al. A four-dimensional probabilistic atlas of the human brain. J Am Med Inform Assoc. 2001;8:401–430.
18. Rorden C, Karnath HO, Bonilha L. Improving lesion-symptom mapping. J Cogn Neurosci. 2007;19:1081–1088.
19. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-Berg H, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004;23(suppl 1):S208–S219.
20. Desikan RS, Ségonne F, Fischl B, Quinn BT, Dickerson BC, Blacker D, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. 2006;31:968–980.
21. Mori S, Wakana S, Nagae-Poetscher LM, van Zijl PC. MRI Atlas of Human White Matter. Amsterdam, The Netherlands: Elsevier; 2005.
22. Cheng B, Golsari A, Fiehler J, Rosenkranz M, Gerloff C, Thomalla G. Dynamics of regional distribution of ischemic lesions in middle cere-bral artery trunk occlusion relates to collateral circulation. J Cereb Blood Flow Metab. 2011;31:36–40.
23. Zhu LL, Lindenberg R, Alexander MP, Schlaug G. Lesion load of the corticospinal tract predicts motor impairment in chronic stroke. Stroke. 2010;41:910–915.
24. Dawes H, Enzinger C, Johansen-Berg H, Bogdanovic M, Guy C, Collett J, et al. Walking performance and its recovery in chronic stroke in rela-tion to extent of lesion overlap with the descending motor tract. Exp Brain Res. 2008;186:325–333.
25. Thomalla G, Glauche V, Koch MA, Beaulieu C, Weiller C, Röther J. Diffusion tensor imaging detects early Wallerian degeneration of the pyramidal tract after ischemic stroke. Neuroimage. 2004;22:1767–1774.
26. Lindenberg R, Renga V, Zhu LL, Betzler F, Alsop D, Schlaug G. Structural integrity of corticospinal motor fibers predicts motor impair-ment in chronic stroke. Neurology. 2010;74:280–287.
27. Puig J, Pedraza S, Blasco G, Daunis-I-Estadella J, Prados F, Remollo S, et al. Acute damage to the posterior limb of the internal capsule on diffu-sion tensor tractography as an early imaging predictor of motor outcome after stroke. Am J Neuroradiol. 2011;32:857–863.
28. Appelros P, Nydevik I, Viitanen M. Poor outcome after first-ever stroke: predictors for death, dependency, and recurrent stroke within the first year. Stroke. 2003;34:122–126.
29. Fink JN, Selim MH, Kumar S, Voetsch B, Fong WC, Caplan LR. Insular cortex infarction in acute middle cerebral artery territory stroke: predictor of stroke severity and vascular lesion. Arch Neurol. 2005;62:1081–1085.
30. De Freitas GR, De H Christoph D, Bogousslavsky J. Topographic clas-sification of ischemic stroke. Handb Clin Neurol. 2009;93:425–452.
31. Ibañez A, Gleichgerrcht E, Manes F. Clinical effects of insular damage in humans. Brain Struct Funct. 2010;214:397–410.
32. Rousseaux M, Honoré J, Vuilleumier P, Saj A. Neuroanatomy of space, body, and posture perception in patients with right hemisphere stroke. Neurology. 2013;81:1291–1297.
33. Cereda C, Ghika J, Maeder P, Bogousslavsky J. Strokes restricted to the insular cortex. Neurology. 2002;59:1950–1955.
34. Christensen H, Boysen G, Christensen AF, Johannesen HH. Insular lesions, ECG abnormalities, and outcome in acute stroke. J Neurol Neurosurg Psychiatry. 2005;76:269–271.
35. Karnath HO. A right perisylvian neural network for human spatial orient-ing. In: Gazzaniga MS, ed. The Cognitive Neurosciences IV. Cambridge, MA: MIT Press; 2009:259–268.
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

1702 Stroke June 2014
36. Verdon V, Schwartz S, Lovblad KO, Hauert CA, Vuilleumier P. Neuroanatomy of hemispatial neglect and its functional components: a study using voxel-based lesion-symptom mapping. Brain. 2010;133(pt 3):880–894.
37. Maxton C, Dineen RA, Padamsey RC, Munshi SK. Don’t neglect ‘neglect’—an update on post stroke neglect. Int J Clin Pract. 2013;67:369–378.
38. Punt TD, Riddoch MJ. Motor neglect: implications for movement and rehabilitation following stroke. Disabil Rehabil. 2006;28:857–864.
39. Hickok G, Poeppel D. The cortical organization of speech processing. Nat Rev Neurosci. 2007;8:393–402.
40. Geva S, Baron JC, Jones PS, Price CJ, Warburton EA. A comparison of VLSM and VBM in a cohort of patients with post-stroke aphasia. Neuroimage Clin. 2012;1:37–47.
41. Paciaroni M, Arnold P, Van Melle G, Bogousslavsky J. Severe dis-ability at hospital discharge in ischemic stroke survivors. Eur Neurol. 2000;43:30–34.
42. Menezes NM, Ay H, Wang Zhu M, Lopez CJ, Singhal AB, Karonen JO, et al. The real estate factor: quantifying the impact of infarct location on stroke severity. Stroke. 2007;38:194–197.
43. Foerch C, Misselwitz B, Sitzer M, Berger K, Steinmetz H, Neumann-Haefelin T; Arbeitsgruppe Schlaganfall Hessen. Difference in recogni-tion of right and left hemispheric stroke. Lancet. 2005;366:392–393.
44. Di Legge S, Fang J, Saposnik G, Hachinski V. The impact of lesion side on acute stroke treatment. Neurology. 2005;65:81–86.
45. Aszalós Z, Barsi P, Vitrai J, Nagy Z. Lateralization as a factor in the prognosis of middle cerebral artery territorial infarct. Eur Neurol. 2002;48:141–145.
46. Fink JN, Frampton CM, Lyden P, Lees KR; Virtual International Stroke Trials Archive Investigators. Does hemispheric lateralization influ-ence functional and cardiovascular outcomes after stroke? An analysis of placebo-treated patients from prospective acute stroke trials. Stroke. 2008;39:3335–3340.
47. Rorden C, Karnath HO. Using human brain lesions to infer func-tion: a relic from a past era in the fMRI age? Nat Rev Neurosci. 2004;5:813–819.
48. Karnath HO, Fruhmann Berger M, Küker W, Rorden C. The anatomy of spatial neglect based on voxelwise statistical analysis: a study of 140 patients. Cereb Cortex. 2004;14:1164–1172.
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

Jean-Claude Baron, Leif Ostergaard, Christian Gerloff and Götz ThomallaSusanne Siemonsen, Jens Fiehler, Salvador Pedraza, Josep Puig, Tae-Hee Cho, Josef Alawneh,
Bastian Cheng, Nils Daniel Forkert, Melissa Zavaglia, Claus C. Hilgetag, Amir Golsari,Rankin Scale
Influence of Stroke Infarct Location on Functional Outcome Measured by the Modified
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.114.005152
2014;45:1695-1702; originally published online April 29, 2014;Stroke.
http://stroke.ahajournals.org/content/45/6/1695World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2014/04/29/STROKEAHA.114.005152.DC1Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on April 12, 2018
http://stroke.ahajournals.org/D
ownloaded from

SUPPLEMENTAL MATERIAL
Influence of stroke infarct location on functional outcome
measured by the modified Rankin scale

Figure I: Pyramid plot showing mean NIHSS values on admission (per test item) depending on injured hemisphere. LOC refers to level of consciousness test items (patient’s alertness, answers of verbal questions and response to simple commands)

NIHSS test item left right left right
Mean SD Mean SD Median IQR Median IQR
LOC responsiveness 0.15 0.36 0.13 0.40 0 0 0 0 LOC questions 1.26 0.94 0.26 0.61 2 2 0 0 LOC commands 0.65 0.80 0.15 0.47 0 1 0 0 horizontal eye movements 0.33 0.58 0.60 0.74 0 1 0 1 visual field test 0.65 0.91 0.72 0.90 0 2 0 2 facial palsy 1.28 0.79 1.49 0.80 1 1 2 1 motor arm right 2.20 1.64 0.04 0.29 2 3 0 0 motor arm left 0.00 0.00 2.23 1.48 0 0 2 3 motor leg right 1.81 1.65 0.02 0.15 2 3 0 0 motor leg left 0.00 0.00 1.74 1.52 0 0 2 3 limb ataxia 0.04 0.19 0.15 0.42 0 0 0 0 sensory 0.63 0.68 1.02 0.79 1 1 1 2 language 1.76 1.03 0.23 0.63 2 2 0 0 speech 0.60 0.79 0.83 0.70 0 1 1 1 extinction / inattention 0.04 0.19 0.85 0.91 0 0 1 2
Table I: NIHSS values on admission (per test item) depending on injured hemisphere. Mean, median and standard deviation of NIHSS values are shown. LOC refers to level of consciousness test items (patient’s alertness, answers of verbal questions and response to simple commands)

Figure II: Overlay lesion plot of FLAIR lesions on day 2hemishpere (right: n=47, left: n:54). MNI coordinates of each second transverse section (z
: Overlay lesion plot of FLAIR lesions on day 2-3 after stroke onset shown for each hemishpere (right: n=47, left: n:54). The colorbar indicates number of overlapping lesions. MNI coordinates of each second transverse section (z-axis) are given.
3 after stroke onset shown for each The colorbar indicates number of overlapping lesions.

Region
Mean
z-score
Median
z-score
Minimum
z-score
Maximum
z-score
SD
Central Opercular Cortex 4.41 4.38 0.00 8.04 1.06
Heschl's Gyrus 4.34 4.30 0.00 8.41 1.08
Posterior corona radiata 4.28 3.89 0.00 7.09 1.28
Parietal Operculum Cortex 4.21 3.92 0.00 7.80 0.92
Uncinate fasciculus 4.19 4.23 0.00 6.13 0.94
Superior corona radiata 4.19 3.96 0.00 8.18 0.95
External capsule 4.09 4.22 0.00 8.04 1.33
Planum Temporale 4.01 3.89 0.00 7.57 0.79
Superior longitudinal fasciculus 3.78 3.72 -0.18 8.11 1.15
Superior fronto-occipital fasciculus 3.68 3.61 0.00 4.81 0.46
Planum Polare 3.63 3.54 0.00 7.25 0.71
Posterior limb of internal capsule 3.62 3.54 0.00 6.97 0.72
Retrolenticular part of internal capsule 3.57 3.51 0.00 7.39 1.04
Superior Temporal Gyrus. posterior division 3.36 3.54 0.00 5.39 0.55
Insular Cortex 3.34 3.21 0.00 7.20 1.38
Supramarginal Gyrus anterior division 3.28 3.39 0.00 5.65 0.51
Middle Temporal Gyrus. posterior division 3.25 3.39 0.00 3.89 0.49
Superior Temporal Gyrus. anterior division 3.20 3.17 0.00 3.89 0.41
PostcentralGyrus 3.13 3.22 0.00 5.98 0.53
Temporal Pole 3.11 3.17 0.00 4.28 0.47
Middle Temporal Gyrus. anterior division 3.11 3.17 0.00 3.72 0.32
Body of corpus callosum 3.03 3.17 0.00 4.37 0.79
Precentral Gyrus 3.00 2.90 0.00 8.67 0.89
Anterior limb of internal capsule 2.85 2.77 0.00 5.13 0.79
Superior Parietal Lobule 2.79 2.75 0.00 3.62 0.58
Cerebral peduncle 2.75 2.75 0.00 2.75 0.00
Supramarginal Gyrus posterior division 2.74 2.72 0.00 4.86 0.54
Fornix (cres) / Stria terminalis 2.70 2.53 0.00 4.92 0.78

Middle Temporal Gyrus temporooccipital part 2.58 2.47 0.00 3.72 0.57
Sagittal stratum 2.58 2.62 0.00 4.73 0.65
Angular Gyrus 2.48 2.54 0.00 4.17 0.69
Frontal Orbital Cortex 2.34 2.47 0.00 3.89 0.81
Anterior corona radiata 2.27 2.26 0.00 4.54 0.66
Frontal Operculum Cortex 2.06 2.00 0.00 4.69 0.86
Inferior Frontal Gyrus. pars opercularis 2.01 1.99 -0.20 4.60 0.73
Inferior Frontal Gyrus. pars triangularis 1.81 1.90 0.00 2.77 0.49
Posterior thalamic radiation 1.78 1.94 0.00 2.19 0.34
Lateral Occipital Cortex. superior division 1.76 1.92 -0.56 3.39 0.76
Genu of corpus callosum 1.69 1.69 0.00 1.69 0.00
Lateral Occipital Cortex. inferior division 1.68 1.69 0.00 2.47 0.46
Middle Frontal Gyrus 1.49 1.46 -0.18 3.72 0.66
Table II: Results from VLSM of all patients (n=101). Mean, median, minimum, maximum and standard deviation (SD) of z-scores according to template regions from anatomical atlases Harvard-Oxford Cortical Structural Atlas and JHU ICBM-DTI-81 White Matter Labels. Regions are sorted by highest mean z-values in descending order.

Left hemisphere Right hemisphere
Region Mean
z-score
Median
z-score
Minimum
z-score
Maximum
z-score
SD Mean
z-score
Median
z-score
Minimum
z-score
Maximum
z-score
SD
Middle Temporal Gyrus. anterior division 3.48 3.48 0.00 3.48 0.87 2.10 2.08 0.00 3.17 0.47
Superior Temporal Gyrus. anterior division 3.25 3.48 0.00 3.54 0.59 1.91 1.92 0.00 3.48 0.52
Body of corpus callosum 3.22 3.48 0.00 3.89 0.00 1.38 1.54 0.00 3.26 0.51
External capsule 3.22 3.23 0.00 6.00 0.70 2.28 2.16 -0.32 5.29 0.77
Superior corona radiata 3.11 3.11 0.00 5.59 1.16 2.36 2.32 0.00 4.49 0.61
Superior fronto-occipital fasciculus 3.06 2.90 0.00 3.89 1.03 1.58 1.61 0.00 3.26 1.15
Uncinate fasciculus 3.03 3.16 0.00 3.91 0.59 2.17 2.15 0.00 3.55 0.56
Posterior corona radiata 2.95 3.35 -0.34 3.89 0.57 2.02 2.02 0.00 3.54 0.74
Temporal Pole 2.86 3.48 0.00 3.72 0.75 1.65 1.49 0.00 3.17 0.55
Parietal Operculum Cortex 2.81 2.82 0.00 3.89 0.77 2.59 2.57 0.00 4.44 0.51
Heschl's Gyrus 2.80 2.94 0.00 4.48 0.82 2.90 2.95 0.00 4.75 0.56
Retrolenticular part of internal capsule 2.80 2.90 -0.16 4.60 0.49 1.75 1.64 0.00 3.19 0.46
Planum Temporale 2.79 2.83 0.00 3.89 0.68 2.54 2.56 0.00 3.89 0.55
Posterior limb of internal capsule 2.78 2.82 0.00 5.15 0.53 2.04 2.07 0.00 4.07 0.67

Central Opercular Cortex 2.78 2.83 0.00 4.16 0.72 2.67 2.79 0.00 5.08 0.75
Planum Polare 2.76 2.88 0.00 3.89 0.58 2.28 2.23 0.00 3.89 0.58
Supramarginal Gyrus, anterior division 2.66 2.74 0.00 3.89 0.63 1.72 1.70 0.00 3.17 0.45
Cerebral peduncle 2.61 2.66 0.00 3.43 0.49 1.64 1.64 0.00 1.64 0.47
Superior Temporal Gyrus. posterior division 2.48 2.53 0.00 3.72 0.55 2.35 2.32 -0.05 3.89 0.00
Middle Temporal Gyrus. posterior division 2.46 2.93 0.00 3.54 0.92 2.28 2.08 0.00 3.89 0.67
Postcentral Gyrus 2.44 2.36 0.00 3.89 0.66 1.75 1.70 -0.18 3.89 0.64
Superior longitudinal fasciculus 2.42 2.62 -0.81 3.89 0.40 2.16 2.10 0.00 3.89 0.61
Anterior limb of internal capsule 2.26 2.32 0.00 3.94 0.64 1.36 1.31 -0.21 3.09 0.60
Insular Cortex 2.23 2.14 -0.47 5.79 1.11 2.18 2.07 -0.44 5.81 1.05
Fornix / Stria terminalis 2.12 2.13 0.00 3.39 0.60 1.30 1.27 0.00 2.73 0.68
Sagittal stratum 2.06 2.04 0.00 3.89 0.65 1.28 1.32 0.00 2.40 0.49
Precentral Gyrus 2.01 1.81 0.00 3.89 0.82 1.76 1.85 -0.48 3.89 0.95
Supramarginal Gyrus, posterior division 1.76 1.62 -0.05 3.89 0.78 2.03 2.10 -0.45 3.89 0.72
Frontal Orbital Cortex 1.70 1.90 0.00 3.48 0.67 1.04 1.24 -0.99 2.98 0.75
Middle Temporal Gyrus, temporooccipital part 1.53 1.24 0.00 3.19 0.00 2.06 2.03 0.00 3.72 0.53
Genu of corpus callosum 1.44 1.44 0.00 1.44 0.77 0.73 0.63 0.00 1.94 0.73
Frontal Operculum Cortex 1.32 1.36 -0.47 3.39 0.65 1.26 1.32 -1.15 3.04 0.86
Angular Gyrus 1.26 1.26 -0.81 3.04 0.85 2.29 2.24 0.00 3.89 0.53

Inferior Frontal Gyrus. pars opercularis 1.15 1.03 -0.87 3.16 0.65 1.54 1.65 -0.08 2.99 0.63
Superior Parietal Lobule 1.15 0.95 0.00 1.69 0.33 1.49 1.36 0.00 3.62 0.45
Inferior Frontal Gyrus. pars triangularis 0.99 0.79 0.00 2.15 0.66 1.17 0.99 -0.05 2.57 1.12
Temporal Fusiform Cortex. posterior division 0.90 0.90 0.00 0.90 0.00 0.00 0.00 0.00 0.00 0.00
Lateral Occipital Cortex. superior division 0.82 0.92 -0.81 2.42 0.52 2.09 2.08 -0.87 3.89 0.68
Middle Frontal Gyrus 0.63 0.68 -1.18 2.82 0.66 1.76 1.77 0.00 3.48 0.55
Lateral Occipital Cortex. inferior division 0.52 0.47 -0.05 1.07 0.28 1.72 2.03 -0.36 3.72 0.94
Posterior thalamic radiation 0.43 0.07 -0.67 2.50 0.88 1.49 1.36 0.00 3.62 0.34
Frontal Pole 0.00 0.00 0.00 0.00 0.00 0.13 0.13 0.00 0.13 0.00
Superior Frontal Gyrus 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Inferior Temporal Gyrus, anterior division 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Inferior Temporal Gyrus, posterior division 0.00 0.00 0.00 0.00 0.00 1.78 2.03 0.00 2.56 0.52
Inferior Temporal Gyrus, temporooccipital part 0.00 0.00 0.00 0.00 0.00 1.38 1.42 0.00 2.08 0.42
Table III: Results from VLSM calculated for each hemisphere (right: n=47 patients. left: n=54 patients). Mean, median, minimum, maximum and standard deviation (SD) of z-scores according to template regions from anatomical atlases Harvard-Oxford Cortical Structural Atlas and JHU ICBM-DTI-81 White Matter Labels. Regions are sorted by highest mean z-values (left hemisphere) in descending order.